Back to Journals » Clinical Ophthalmology » Volume 19
Markedly Lower Rates of Age-Related Macular Degeneration in Malta Compared to European Countries: Results from The Malta Eye Study, Indicating Possible Divergent Genetic Ancestry?
Authors Agius D ![]() , Mamo JJ, Calleja N, Cassar D, Marku X
, Mamo JJ, Calleja N, Cassar D, Marku X ![]() , Nappa MC, Zammit M
, Nappa MC, Zammit M ![]() , Pace ME, Carbonaro F
, Pace ME, Carbonaro F
Received 15 July 2025
Accepted for publication 6 October 2025
Published 27 October 2025 Volume 2025:19 Pages 3961—3971
DOI https://doi.org/10.2147/OPTH.S551852
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
David Agius,1,2 Julian J Mamo,3 Neville Calleja,3 Daniel Cassar,2 Xeniya Marku,2 Maria Christina Nappa,4 Michaela Zammit,4 Maria Elena Pace,5 Francis Carbonaro1,2,6
1Department of Surgery, University of Malta, Msida, Malta; 2Department of Ophthalmology, Mater Dei Hospital, Msida, Malta; 3Department of Public Health, University of Malta, Msida, Malta; 4Department of Medicine, Mater Dei Hospital, Msida, Malta; 5Medical School, University of Malta, Msida, Malta; 6Department of Twin Research, King’s College, London, UK
Correspondence: David Agius, Ophthalmology Outpatients, Mater Dei Hospital, Triq id-Donaturi tad-Demm, Msida, MSD 2090, Malta, Email [email protected]
Purpose: To estimate the prevalence of age-related macular degeneration (ARMD) in a nationally representative sample of older adults from Malta, evaluate associations with established risk factors, and compare rates with those reported in other European populations, where substantial variation has been observed.
Patients and Methods: A population-based cross-sectional study was conducted involving 1794 participants aged 50– 80 years from Malta (1% of the represented population), recruited as part of The Malta Eye Study. Standardized ophthalmic examinations were performed, including retinal imaging graded for ARMD according to Age-Related Eye Disease Study criteria and optical coherence tomography scans. Data on demographics, medical history, behavioural risk factors, and ocular characteristics were collected via structured questionnaires. Associations were assessed using multivariable logistic regression. DNA samples were also collected for future genetic analyses.
Results: The overall prevalence of ARMD was 6.5% (95% CI 5.4– 7.8%), with early ARMD accounting for 5.6% (95% CI 4.6– 6.7%) and late ARMD for 0.4% (95% CI 0.2– 0.8%). Multivariate analysis showed that ARMD prevalence increased significantly with age (OR per year 1.08; 95% CI 1.05– 1.11, p< 0.001) and in the male sex (OR 1.57; 95% CI 1.01– 2.44, p=0.043). The other traditional ARMD risk factors did not show significant associations in this cohort. Compared to other European populations, ARMD prevalence was notably lower.
Conclusion: This study reports a relatively low prevalence of ARMD compared to other European settings, with age and male sex emerging as the only significant risk factors. The absence of association with other traditional risk factors may reflect underlying genetic differences or distinct gene–environment interactions. As DNA samples were collected, further investigation incorporating genetic data is warranted to better understand ARMD susceptibility in this population.
Plain Language Summary: This study looked at how common age-related macular degeneration (ARMD) is in Malta and what factors might increase the chances of developing it.
Why was this study done?
ARMD is a leading cause of vision loss in older adults across Europe, where many studies report high rates of disease. Malta has some of the highest European rates of risk factors linked to ARMD, such as obesity and ultraviolet (UV) exposure. Smoking rates in Malta are similar to other European countries. Despite this, little is known about prevalence of ARMD in Malta.
What did the researchers do and find?
We examined a large, representative group of adults aged 50 and older living in Malta. We checked for signs of ARMD and collected information about their age, gender, medical history, and lifestyle.We found that 6.5% of people had ARMD, which is lower than reported in other European countries.Only older age and being male were clearly linked to ARMD.Other factors often thought to increase ARMD risk, like smoking, diabetes, high blood pressure, or obesity, were not strongly linked in our study.
What do these results mean?
Lower ARMD rates in Malta may be due to unique genetic or environmental factors. We collected DNA samples to support future research. Our findings suggest ARMD risk varies more between populations than previously thought, highlighting the need for further study in Mediterranean countries.
Keywords: macular degeneration, prevalence, risk factors, ageing, population-based study, gene–environment interaction
Introduction
Age-related macular degeneration (ARMD) is the most common maculopathy causing visual impairment in those aged over 75 years.1–3 It begins with drusen (lipofuscin deposits) and may progress to central vision loss through dry (retinal pigment epithelial dysfunction, geographic atrophy) or wet (neovascularization, fluid, hemorrhage, scarring) forms.4
Globally, ARMD affects 8.69% of individuals aged 45–85, with early and late stages affecting 8.01% and 0.37%, respectively.5 In the United States (≥40 years), prevalence is 11.64% for early and 0.94% for late ARMD,6 while in Europe (≥60 years), it is 25.3% and 2.41%, respectively.7
Meta-analyses highlighted older age, smoking, prior cataract surgery, and family history as key ARMD risk factors (OR ≥ 1.5).8 Recent data added male sex, hypertension, cardiovascular disease, and diabetes.9 Age remains the strongest non-modifiable risk, with prevalence rising sharply after 75 years.5 Rates are highest in Northern Europeans.10,11 Early ARMD is less common in Asians (6.8%) and Africans (7.1%) compared with Europeans (11.2%), late ARMD is less common in Africans (0.3% vs 0.5% in Europeans), and overall (“any”) ARMD is lower in Asians (7.4%) and Africans (7.5%) than in Europeans (12.3%).5 Modifiable behavioral risks include smoking, which triples ARMD risk,12 low physical activity,13 and Western diets,14 while Mediterranean eating patterns, olive oil consumption,15 and exercise16,17 are protective. Obesity nearly doubles the odds of late ARMD.18 Sunlight exposure has also been associated with risk in multiple studies.19–22 Hyperopia is a possible ocular risk23,24 while cataract surgery has been associated with ARMD,8,25–30 though recent evidence remains conflicting.31,32
Genetic susceptibility contributes substantially to ARMD risk at the population level. Variants in CFH and ARMS2/HTRA1, related to complement regulation and oxidative stress, were among the earliest identified.33 A landmark genome-wide association study by the International ARMD Genomics Consortium identified 34 risk loci,34 later expanded to 63 through further analyses,35–37 implicating key pathways such as inflammation, lipid metabolism, and extracellular matrix regulation. Differences in genetic architecture between populations help explain variation in ARMD prevalence, while gene–environment interactions further shape individual and population risk.38 Smoking and obesity, in particular, have been shown to markedly increase ARMD risk in individuals carrying high-risk variants, especially in CFH and ARMS2.39 The development of polygenic risk scores supports early risk stratification and may guide both personalized lifestyle interventions and public health strategies targeting high-risk groups.40–42
Malta, a small Southern European island-state with a growing, ageing population of 563,443,43 has the highest overweight/obesity prevalence in the EU (69.75%; 95% CI: 68.32–71.18%), a trend rising over three decades.44 It also ranks second in Europe for UV radiation, with 8.2 average daily sunshine hours and a mean annual temperature of 19.5°C.45,46 Smoking rates in Malta are similar to other European countries.47 Given that obesity, UV exposure and smoking are established ARMD risk factors, these may influence its prevalence in Malta. A 1959 Maltese blindness report noted no ARMD cases,48 while a 1989 study found a 0.4% prevalence of senile macular degeneration in those aged 40+.49
The Malta Eye Study (TMES) is a population-based, cross-sectional study assessing the prevalence of visual impairment and common eye diseases in Maltese adults aged 50–80. This paper focuses on ARMD, presenting its prevalence and associated risk factors in Malta, and evaluating how these patterns align with established European estimates.
Materials and Methods
TMES methodology, including sample size derivation, is detailed elsewhere.50 The study adhered to The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist,51(Supplementary Table 1).
Ethical Clearance and Permissions
Ethical approval was granted by the University of Malta Faculty Research Ethics Committee (FRECMDS_1819_94) before data collection in 2019. The study followed the Declaration of Helsinki52 and General Data Protection Regulation (GDPR)53 guidelines, with hospital and Data Protection Officer approvals. Informed consent was obtained, and data were pseudonymized.
Study Population
A random sample of 4006 individuals aged 50–80 years, stratified by age, sex, and locality, obtained from the Malta Electoral Register, was invited for an ophthalmic assessment between September 2021 and July 2024. Chi-square and binomial tests assessed age-sex subgroup representativity and weights (Population proportion / Sample proportion) adjusted the sample to census data for ages 50–80.
Ophthalmic Assessment
The individuals were examined at Mater Dei Hospital between September 2021 and May 2024 and at Gozo General Hospital between June 2024 and July 2024.
The assessment involved visual acuity tests and autorefraction using the Visionix device (Visionix),54 subjective refraction, anthropometric (weight, height) and clinical (blood pressure and capillary blood glucose) measurements, Goldmann tonometry, a slit lamp based anterior segment and dilated posterior segment indirect (90D) examination, fundus photography and swept-source optical coherence tomography (OCT) scanning of the macula and disc. The questionnaire included themes related to sociodemographic status, medical and ocular history.
Definitions Used
The presence and severity of ARMD were classified according to the Age-Related Eye Disease Study (AREDS) criteria.55 Category 1 indicated no drusen or <15 small drusen (<63 µm) in both eyes. Category 2 included ≥15 small drusen (<63 µm), <20 intermediate drusen (63–124 µm), or pigmentary abnormalities in at least one eye. Category 3 was defined by the presence of large drusen (≥125 µm), ≥20 intermediate drusen (63–124 µm), or non-central geographic atrophy in at least one eye. Category 4 indicated advanced ARMD, or visual acuity worse than 20/32 attributable to lesions of non-advanced ARMD (eg, central large drusen) in one eye only.
For analysis, ARMD status was grouped as: no ARMD (Category 1), early ARMD (Categories 2 and 3), and late ARMD (Category 4), based on the more severely affected eye. Grading was performed by a single observer (DA) using both direct fundus examination and retinal images. As a quality control measure, a single-blinded validation was conducted by an independent reviewer (FC), who graded fundus images post hoc for a subsample of 74 participants (148 eyes). The validation sample was selected to detect an expected agreement of κ = 0.9 with a precision of ±0.1, with a 50% prevalence of ARMD in the subset (sample size based on Shoukri et al’s formula).56 The resulting inter-rater agreement for the presence or absence of ARMD was substantial (κ = 0.7).
Statistical Analysis
Statistical analyses were done using IBM SPSS Statistics v23 (IBM Corp.).57 Demographic variables (age, sex, district) were compared with national census data58 for representativeness. Descriptive statistics were used to provide prevalence estimates with 95% confidence intervals. Categorical predictors of ARMD were tested with Chi-square or Fisher’s exact tests. Significant univariate predictors (p<0.05) were included in backward stepwise binary logistic regression models on the basis of the Wald test, with absence of ARMD as reference. The models’ final steps were presented. Missing data, being minimal, were handled by listwise deletion, assumed missing completely at random, with no imputation.
Results
A total of 1794 individuals were assessed between September 2021 and July 2024, yielding a turnout of 44.8%. Sample representativity was evaluated against the national census,58 showing good alignment for age, sex, and district when considered separately. However, there was an underrepresentation of males (p<0.001) and females (p=0.009) aged 50–59 in Northern Harbor, and of females aged 50–59 in Gozo (p=0.004). To correct this, weighting based on national census58 data was applied. Missing data were minimal: 0.4% for most questionnaire items, 0.2% for VI classification, 8.1% for education (post-assessment), and 4.8% for autorefraction.
Prevalence of Age-Related Macular Degeneration
The prevalence of any ARMD in either eye was 6.5% (95% CI 5.4–7.8%) in TMES, and when taking into consideration the worst stage in the affected eye, category 2 ARMD was present in 5.6% (95% CI 4.6–6.7%), category 3 ARMD occurred in 0.6% (95% CI 0.3–1.1%) while category 4 ARMD affected 0.4% (95% CI 0.2–0.8%) (Table 1).
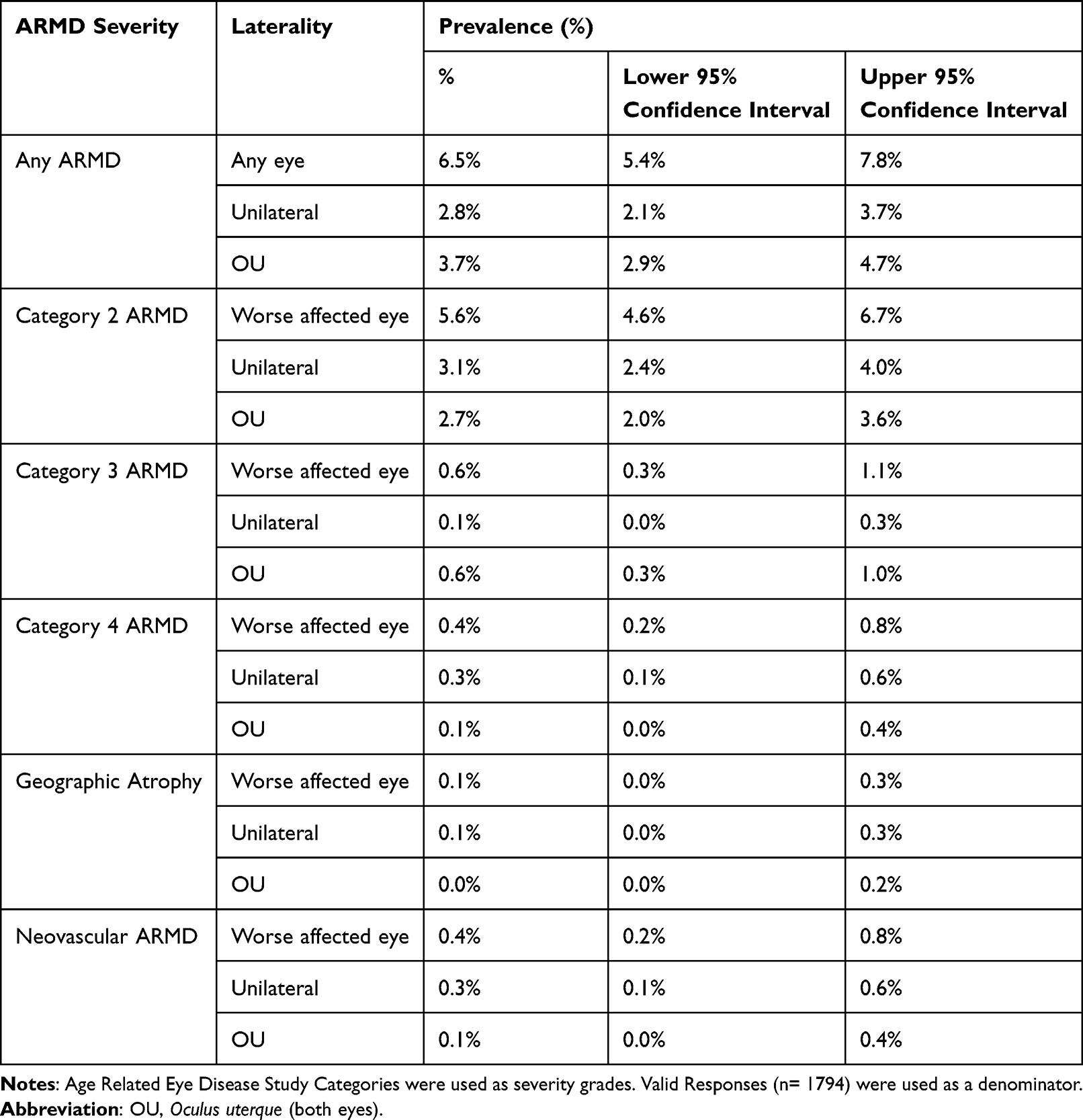 |
Table 1 Prevalence of Age-Related Macular Degeneration (ARMD) Among the Census-Adjusted TMES Population |
A comparison of the age-standardized prevalence of ARMD in individuals aged 60+ between TMES and the latest European ARMD meta-analysis7 showed significantly lower prevalence rates of both early and late ARMD in each age group within TMES, with the differences increasing with age (Figures 1 and 2).
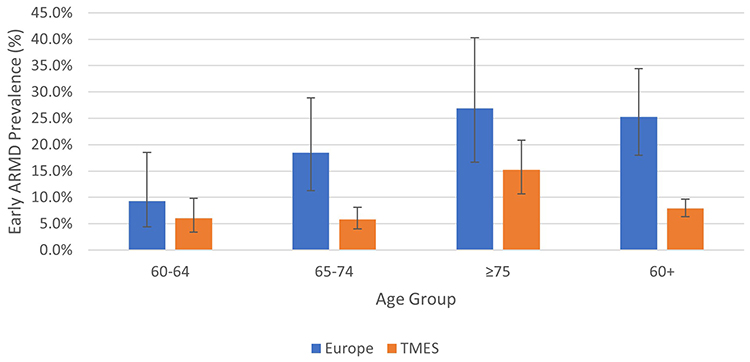 |
Figure 1 Comparison of Age-Standardized Prevalence Rates (with 95% confidence interval bars) of Early (Categories 2 and 3) Age-Related Macular Degeneration (ARMD) between European data7 and that in TMES. |
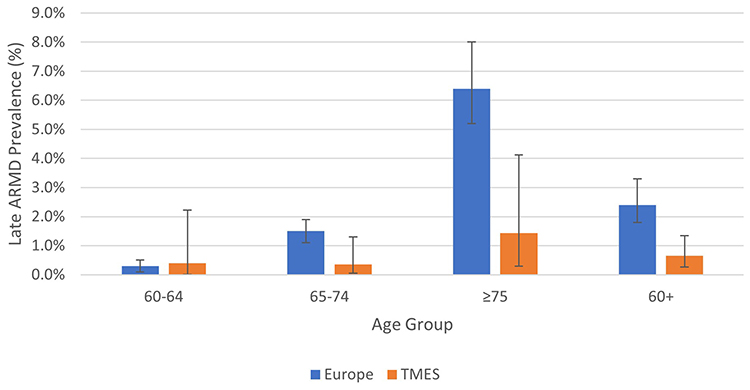 |
Figure 2 Comparison of Age-Standardized Prevalence Rates (with 95% confidence interval bars) of Late (Category 4) Age-Related Macular Degeneration (ARMD) between European data7 and that in TMES. |
Age Related Macular Degeneration by Age and Sex
The prevalence of any ARMD and bilateral ARMD increased by age group and was higher among males overall, especially from 60 years and over (Figures 3–5). Similar trends were observed for early and intermediate ARMD in the worse affected eye. Advanced ARMD, including both geographic atrophy and neovascular ARMD, increased with age but had no sex preference.
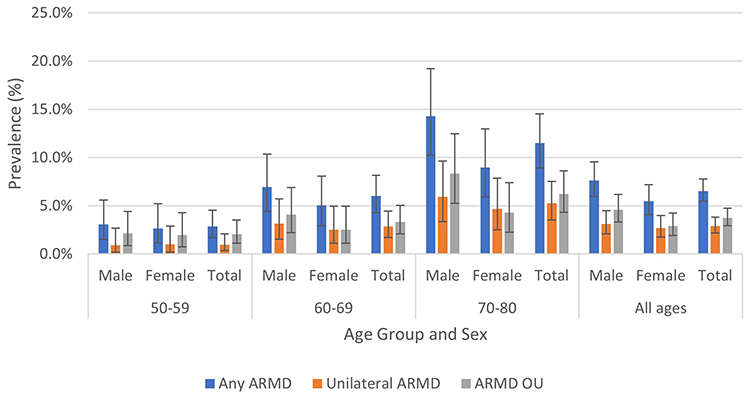 |
Figure 3 The prevalence of age-related macular degeneration (ARMD) laterality (with 95% confidence interval bars) by age group and sex among the census-adjusted TMES population. ARMD OU: Bilateral ARMD. |
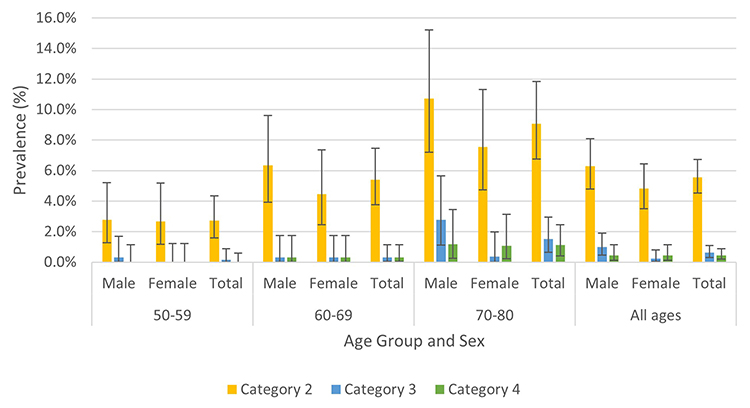 |
Figure 4 The prevalence of age-related macular degeneration (ARMD) severity in the worse affected eye (with 95% confidence interval bars) by age group and sex among the census-adjusted TMES population. |
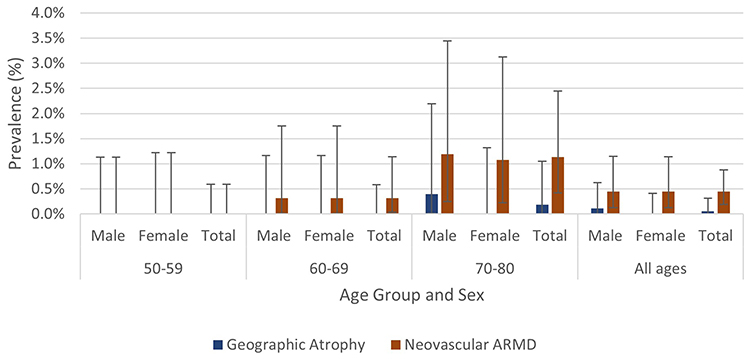 |
Figure 5 The prevalence of geographic atrophy and neovascular age-related macular degeneration (ARMD) (with 95% confidence interval bars) by age group and sex among the census-adjusted TMES population. |
Predictors of Age-Related Macular Degeneration
Due to the relatively small number of ARMD cases (n = 117), only predictors of any ARMD were analyzed. Stepwise multivariate logistic regression modelling was employed, which led to the exclusion of several predictors that were initially significant in univariate analysis (Supplementary Table 2), including education level, employment status, sunglasses wear, antiplatelet use, astigmatism, and corneal arcus. Sex was included in the model, especially in view of its theoretical relevance. After adjusting for age and sex, increasing age remained significantly associated with ARMD (OR per year 1.08 95% CI 1.05–1.11, p<0.001) and male sex was independently associated with greater risk (OR: 1.57 95% CI 1.01–2.44, p=0.043).
Discussion
Comparison with Previous Local Rates
Since the previous study did not provide defining criteria for “senile macular degeneration”, the earlier reported prevalence of 0.4% cannot be meaningfully compared with current data.49 This is really the first comprehensive, cross sectional prevalence study, on a large sample of the population, using a random sample of 1% of the population, stratified for age, sex and locality.
Comparison with European Data
ARMD prevalence was notably lower among the TMES cohort (Figures 1 and 2). Although age groups and ARMD categories were matched to those used in the literature, comparisons should be interpreted with caution. TMES had an upper age limit of 80 years, unlike the European meta-analysis,7 which included older participants. Additionally, the meta-analysis combined studies with varying grading methods, and its reported categories, early/intermediate and late ARMD, correspond to AREDS stages 2/3 and 4, which TMES used.
One possible explanation for the lower prevalence observed in Malta is a difference in genetic susceptibility. The Maltese population may have a lower frequency of high-risk alleles, such as CFH Y402H and ARMS2/HTRA1 A69S, or a higher frequency of protective variants. This genetic background could also contribute to the lack of significant associations between ARMD and modifiable risk factors such as smoking (p = 0.430) or obesity in the TMES cohort. Notably, even when high-risk variants are present, recent evidence suggests that their effect sizes vary by ancestry and these risk variants have been shown to confer weaker effects in individuals with non-European ancestry.59
The genetic structure of the Maltese population is distinct from that of Central and Northern Europe. Studies have shown close genetic affinity with Sicilians and Southern Italians,60 along with traces of Near Eastern ancestry.61,62 This distinct ancestry may modulate both the expression of risk alleles and their interaction with environmental exposures, potentially attenuating the risk conferred by smoking or obesity.
In Salandra, Basilicata (Southern Italy), the prevalence of ARMD among individuals aged 60–89 years was notably lower than in other European populations, with advanced ARMD observed in only 1.1% and early changes, defined as drusen larger than 50 μm and more than 10 in number, reported in 4.5%.63 In contrast, a citation reported ARMD prevalence of 22.3% among adults aged 40+ in the Sicilian town of Casteldaccia.64 Although the original source is not readily accessible, the findings highlight the need for caution when comparing regional prevalence estimates, as factors such as local environmental exposures, dietary habits, and methodological differences between studies may significantly influence outcomes, regardless of underlying genetic similarities.
Sardinians, unlike Sicilians, have a distinct genetic ancestry closely aligned with Early European Farmers.61 They had a relatively low ARMD prevalence, 6.9% for early and 0.7% for late ARMD among individuals aged 50+, and their genetic predisposition by the CFH Y402H allele and ARMS2/HTRA1 polymorphisms were low.65 In contrast, Northeast Italy reported a much higher prevalence of 62.7% (95% CI: 59.4–66.0%) among individuals aged 60–80 years.66 Northeast Italy differs genetically from Sardinia and Malta, reflecting more Central European ancestry, and is also less traditionally Mediterranean in climate and diet. These combined genetic and lifestyle differences likely contribute to the higher ARMD prevalence observed there. These examples imply complex interplay between genetics, ancestry and environmental factors in determining ARMD.
The Mediterranean diet and olive oil consumption are known for their protective effects against ARMD.67,68 Although dietary habits were not assessed in this cohort, it is possible that protective dietary factors, such as adherence to a Mediterranean diet, were present within the TMES population.
Geographic location, including proximity to the equator and higher solar insolation, has been linked to lower ARMD prevalence, potentially due to the role of vitamin D. Higher early ARMD rates were found in predominantly white populations while higher late ARMD rates were found in areas with lower insolation, with whites being more susceptible in these regions.38 Higher insolation may help explain Malta’s lower ARMD rates compared to Northern Europe. In Crete, a prevalence of 6.1% (95% CI: 4.4–8.2%) was reported in individuals aged 50–79, with higher rates associated with increased altitude.64 Malta’s relatively low elevation may be another factor contributing to its lower ARMD prevalence.
Since Malta is a relatively small country, easy access to ophthalmic care and timely AREDS supplementation, may help reduce progression to late-stage ARMD, especially among older adults.
The lower ARMD prevalence among the Maltese population as opposed to Europeans warrants further investigation on specific genetic variants, and their interaction with environmental exposures. Although genetic analysis was beyond the scope of this project, DNA samples were collected from over 1400 TMES participants, and genetic data obtained from TMES controls and individuals with known ARMD, particularly those in the older age groups, may help explain these striking differences. This remains a promising area for investigation.
Associations of ARMD
Interestingly, data from TMES indicate that several well-established risk factors for AMD, beyond age and sex, such as smoking, UV exposure, obesity, hypertension, cardiovascular disease, diabetes, dementia, and pseudophakia,9,12,18,21,26,69,70 were not significantly associated with ARMD in this population. Upon stratifying systemic diseases such as diabetes and hypertension by their level of control, as determined by clinic blood pressure readings, the type of medications used to treat diabetes, and by clinic capillary blood glucose readings, no significant differences in ARMD rates were observed between individuals without these conditions, those with poorly controlled disease, and those with well-controlled disease.
There may be protective genetic or environmental factors specific to the Maltese population that mitigate the impact of traditional risk factors. Nonetheless, the lack of observed associations may also reflect the relatively low prevalence of ARMD in the cohort, potentially limiting the statistical power to detect significant relationships. Future studies with larger sample sizes and longitudinal or case–control designs are needed to better explore these factors.
While pseudophakia has been linked to ARMD in earlier studies,26,30 the higher ARMD rates observed among pseudophakic individuals in this cohort were not statistically significant. In this context, pseudophakia may instead reflect access to cataract surgery and overall better eye care, possibly acting as a protective confounder rather than a true risk factor, aligning with current evidence.31,32,71
Strengths and Limitations
The strengths of this study include its large, representative, population-based and clinician-led design, with all examinations performed by the same validated specialist. This approach eliminated inter-observer variability and ensured intra-observer consistency, thereby enhancing the validity and robustness of the findings. Furthermore, the use of pupil-dilated indirect fundoscopy and swept-source OCT enabled comprehensive and high-quality ARMD assessment. Turnout matched similar local studies,18 but the 44.8% response rate may have introduced nonresponse ad selection bias. Participants were invited to clinics rather than examined through domiciliary visits, which may have potentially discouraged attendance of older individuals who might have had visual problems, including ARMD, potentially leading to underestimation of its prevalence. While domiciliary assessments could have reduced this bias, they were not feasible in this study due to resource limitations. Additionally, we did not assess dietary patterns or AREDS supplementation, which may influence ARMD risk, and thus these factors could not be evaluated in our analyses. The low prevalence of ARMD limited the power of risk factor analyses, including those for severity subgroups. Finally, the cross-sectional design restricted causal inference due to potential biases, confounding factors, and the inability to establish temporal relationships.
Conclusion
In this study, we report a significantly lower prevalence of ARMD compared to other European populations, with most traditional risk factors, except age and male sex, not showing significant associations. While our findings suggest a lower prevalence of ARMD in the Maltese population, further research into genetic and environmental factors may help explain these patterns, considering the cross-sectional design, modest response rate, and potential selection bias. These differences may be partly explained by underlying genetic variation or distinct gene–environment interactions. As DNA samples were collected, future analyses incorporating genetic data are recommended to explore these hypotheses further and enhance understanding of ARMD risk in this population.
Abbreviations
AREDS, Age-Related Eye Disease Study; ARMD, Age-Related Macular Degeneration; DNA, Deoxyribonucleic acid; GDPR, General Data Protection Regulation; OCT, Optical Coherence Tomography; OU, Oculus uterque (both eyes); STROBE, The Strengthening of the Reporting of Observational Studies in Epidemiology Statement; TMES, The Malta Eye Study; UV, Ultraviolet.
Acknowledgments
We thank our funding bodies; the Malta Community Chest Fund and Research Innovation, Development Fund, Tertiary Education Scholarship Scheme, Prohealth Ltd (Malta), and Class Optical. We thank the management at the Mater Dei and Gozo General Hospitals for their study support. We also acknowledge the support of Mr. Nicolai Schembri and Mr. Christian Attard for IT services, Mr. Stefan Attard for the invitation design, and Dr. George Farrugia for translation services. We thank Dr. John Cachia for sharing his past research experience and to all staff, volunteers, and assistants involved in data collection. Special thanks to Mrs. Marilyn Grech for her vital logistical support throughout this study.
Funding
Funding for Dr David Agius: The Malta Community Chest Fund (MCCF), coordinated by the University of Malta’s Research, Innovation and Development Trust (RIDT), provided funding amounting to EUR 132,000. This covered equipment, publication and conference costs, and a stipend to Dr. David Agius under a University of Malta Scholarship agreement (30/01/2019, agreement 20190304). Tertiary Education Scholarship Scheme (TESS) funded Dr. Agius’s tuition. Prohealth Ltd (Malta) provided stationery and postage. Class Optical supplied participant gifts. None of the funders were involved in the study’s design, data, or manuscript decisions. The other authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
None of the authors has any proprietary interests or conflicts of interest related to this submission.
References
1. Klein R, Klein BEK, Linton KLP. Prevalence of age-related maculopathy: the beaver dam eye study. Ophthalmology. 1992;99(6):933–943. doi:10.1016/S0161-6420(92)31871-8
2. Mitchell P, Smith W, Attebo K, Wang JJ. Prevalence of age-related maculopathy in Australia: the Blue Mountains Eye Study. Ophthalmology. 1995;102(10):1450–1460. doi:10.1016/S0161-6420(95)30846-9
3. Klaver CC, Assink JJ, van Leeuwen R, et al. Incidence and progression rates of age-related maculopathy: the Rotterdam Study. Invest Ophthalmol Vis Sci. 2001;42(10):2237–2241.
4. Young RW. Pathophysiology of age-related macular degeneration. Surv Ophthalmol. 1987;31(5):291–306. doi:10.1016/0039-6257(87)90115-9
5. Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014;2(2):e106–e116. doi:10.1016/S2214-109X(13)70145-1
6. Rein DB, Wittenborn JS, Burke-Conte Z, et al. Prevalence of age-related macular degeneration in the US in 2019. JAMA Ophthalmol. 2022;140(12):1202. doi:10.1001/jamaophthalmol.2022.4401
7. Li JQ, Welchowski T, Schmid M, Mauschitz MM, Holz FG, Finger RP. Prevalence and incidence of age-related macular degeneration in Europe: a systematic review and meta-analysis. Br J Ophthalmol. 2020;104(8):1077–1084. doi:10.1136/BJOPHTHALMOL-2019-314422
8. Chakravarthy U, Wong TY, Fletcher A, et al. Clinical risk factors for age-related macular degeneration: a systematic review and meta-analysis. BMC Ophthalmol. 2010;10(1):1–13. doi:10.1186/1471-2415-10-31/FIGURES/14
9. Babaker R, Alzimami L, Al Ameer A, et al. Risk factors for age-related macular degeneration: updated systematic review and meta-analysis. Medicine. 2025;104(8):e41599. doi:10.1097/MD.0000000000041599
10. Colijn JM, Buitendijk GHS, Prokofyeva E, et al. Prevalence of age-related macular degeneration in Europe: the past and the future. Ophthalmology. 2017;124(12):1753–1763. doi:10.1016/J.OPHTHA.2017.05.035
11. Erke MG, Bertelsen G, Peto T, Sjolie AK, Lindekleiv H, Njolstad I. Prevalence of age-related macular degeneration in elderly Caucasians: the Tromsø Eye Study. Ophthalmology. 2012;119(9):1737–1743. doi:10.1016/j.ophtha.2012.03.016
12. Smith W, Assink J, Klein R, et al. Risk factors for age-related macular degeneration: pooled findings from three continents. Ophthalmology. 2001;108(4):697–704. doi:10.1016/S0161-6420(00)00580-7
13. Mauschitz MM, Schmitz MT, Verzijden T, et al. Physical activity, incidence, and progression of age-related macular degeneration: a multicohort study. Am J Ophthalmol. 2022;236:99–106. doi:10.1016/j.ajo.2021.10.008
14. Chiu CJ, Chang ML, Zhang FF, et al. The relationship of major American dietary patterns to age-related macular degeneration. Am J Ophthalmol. 2014;158(1):118–127.e1. doi:10.1016/J.AJO.2014.04.016
15. Merle BMJ, Cougnard-Grégoire A, Delyfer MN, et al. Mediterranean diet and incidence of advanced age-related macular degeneration: the EYE-RISK Consortium. Ophthalmology. 2019;126(3):381–390. doi:10.1016/j.ophtha.2018.08.006
16. Knudtson MD, Klein R, Klein BEK. Physical activity and the 15-year cumulative incidence of age-related macular degeneration: the Beaver Dam Eye Study. Br J Ophthalmol. 2006;90(12):1461–1463. doi:10.1136/BJO.2006.103796
17. McGuinness MB, Karahalios A, Simpson JA, et al. Past physical activity and age-related macular degeneration: the Melbourne Collaborative Cohort Study. Br J Ophthalmol. 2016;100(10):1353–1358. doi:10.1136/BJOPHTHALMOL-2015-307663
18. Milton RC, Clemons TE, Klien R, Seddon JM, Ferris FL. Risk factors for the incidence of advanced age-related macular degeneration in the Age-Related Eye Disease Study (AREDS): AREDS report no. 19. Ophthalmology. 2005;112(4):533–539.e1. doi:10.1016/j.ophtha.2004.10.047
19. Cruickshanks KJ, Klein R, Klein BEK. Sunlight and age-related macular degeneration: the Beaver Dam Eye Study. Arch Ophthalmol. 1993;111(4):514–518. doi:10.1001/ARCHOPHT.1993.01090040106042
20. Tomany SC, Cruickshanks KJ, Klein R, Klein BEK, Knudtson MD. Sunlight and the 10-year incidence of age-related maculopathy: the Beaver Dam Eye Study. Arch Ophthalmol. 2004;122(5):750–757. doi:10.1001/ARCHOPHT.122.5.750
21. Fletcher AE, Bentham GC, Agnew M, et al. Sunlight exposure, antioxidants, and age-related macular degeneration. Arch Ophthalmol. 2008;126(10):1396–1403. doi:10.1001/ARCHOPHT.126.10.1396
22. Hirakawa M, Tanaka M, Tanaka Y, et al. Age-related maculopathy and sunlight exposure evaluated by objective measurement. Br J Ophthalmol. 2008;92(5):630–634. doi:10.1136/BJO.2007.130575
23. Ikram MK, Van Leeuwen R, Vingerling JR, Hofman A, De Jong PTVM. Relationship between refraction and prevalent as well as incident age-related maculopathy: the Rotterdam Study. Invest Ophthalmol Vis Sci. 2003;44(9):3778–3782. doi:10.1167/IOVS.03-0120
24. Pan CW, Ikram MK, Cheung CY, et al. Refractive errors and age-related macular degeneration: a systematic review and meta-analysis. Ophthalmology. 2013;120(10):2058–2065. doi:10.1016/J.OPHTHA.2013.03.028
25. Klein BEK, Howard KP, Lee KE, Iyengar SK, Sivakumaran TA, Klein R. The relationship of cataract and cataract extraction to age-related macular degeneration: the Beaver Dam Eye Study. Ophthalmology. 2012;119(8):1628. doi:10.1016/J.OPHTHA.2012.01.050
26. Krishnaiah S, Das T, Nirmalan PK, et al. Risk factors for age-related macular degeneration: findings from the Andhra Pradesh eye disease study in South India. Invest Ophthalmol Vis Sci. 2005;46(12):4442–4449. doi:10.1167/IOVS.05-0853
27. Cugati S, Mitchell P, Rochtchina E, et al. Cataract surgery and the 10–year incidence of age–related macular degeneration: the Blue Mountains Eye Study. Invest Ophthalmol Vis Sci. 2006;47(13):1130.
28. Ho L, Boekhoorn SS, van Duijn CM, et al. Cataract surgery and the risk of aging macula disorder: the Rotterdam study. Invest Ophthalmol Vis Sci. 2008;49(11):4795–4800. doi:10.1167/IOVS.08-2066
29. Bikbov MM, Kazakbaeva GM, Iakupova EM, et al. Prevalence of age-related macular degeneration and retinal pseudodrusen in an elderly population. The Ural very old study. Graefes Arch Clin Exp Ophthalmol. 2024;263(2):291–304. doi:10.1007/S00417-024-06644-1
30. Klein R, Klein BEK, Jemen SC, Cruichshanks KJ. The relationship of ocular factors to the incidence and progression of age-related maculopathy. Arch Ophthalmol. 1998;116(4):506–513. doi:10.1001/ARCHOPHT.116.4.506
31. Hanhart J, Wiener R, Totah H, Brosh K, Zadok D. Pseudophakia as a surprising protective factor in neovascular age-related macular degeneration. J Fr Ophtalmol. 2023;46(5):527–535. doi:10.1016/J.JFO.2022.11.015
32. Sutter FKP, Menghini M, Barthelmes D, et al. Is pseudophakia a risk factor for neovascular age-related macular degeneration? Invest Ophthalmol Vis Sci. 2007;48(4):1472–1475. doi:10.1167/IOVS.06-0766
33. Fritsche LG, Loenhardt T, Janssen A, et al. Age-related macular degeneration is associated with an unstable ARMS2 (LOC387715) mRNA. Nat Genet. 2008;40(7):892–896. doi:10.1038/NG.170
34. Fritsche LG, Igl W, Bailey JNC, et al. A large genome-wide association study of age-related macular degeneration highlights contributions of rare and common variants. Nat Genet. 2016;48(2):134. doi:10.1038/NG.3448
35. Winkler TW, Brandl C, Grassmann F, et al. Investigating the modulation of genetic effects on late AMD by age and sex: lessons learned and two additional loci. PLoS One. 2018;13(3):e0194321. doi:10.1371/JOURNAL.PONE.0194321
36. Han X, Gharahkhani P, Mitchell P, Liew G, Hewitt AW, MacGregor S. Genome-wide meta-analysis identifies novel loci associated with age-related macular degeneration. J Hum Genet. 2020;65(8):657–665. doi:10.1038/S10038-020-0750-X
37. He W, Han X, Ong JS, et al. Genome-wide meta-analysis identifies risk loci and improves disease prediction of age-related macular degeneration. Ophthalmology. 2024;131(1):16–29. doi:10.1016/J.OPHTHA.2023.08.023
38. Reibaldi M, Longo A, Pulvirenti A, et al. Geo-epidemiology of age-related macular degeneration: new clues into the pathogenesis. Am J Ophthalmol. 2016;161:78–93.e2. doi:10.1016/J.AJO.2015.09.031/ASSET/644F9114-0630-4075-8F61-147986007C7B/MAIN.ASSETS/GR9.SML
39. Seddon JM, Francis PJ, George S, Schultz DW, Rosner B, Klein ML. Association of CFH Y402H and LOC387715 A69S with progression of age-related macular degeneration. JAMA. 2007;297(16):1793–1800. doi:10.1001/JAMA.297.16.1793
40. Grunin M, Triffon D, Beykin G, et al. Genome wide association study and genomic risk prediction of age related macular degeneration in Israel. Sci Rep. 2024;14(1):1–9. doi:10.1038/s41598-024-63065-0
41. Tang F, Hogg RE, Higgins BE, Wright DM, Smyth L, Sivaprasad S. Impact of polygenic risk scores on retinal microstructures in early and intermediate age-related macular degeneration: the Northern Ireland Sensory Aging Study. Eye. 2025;1–9. doi:10.1038/s41433-025-03844-9
42. Yu C, Robman L, He W, et al. Predictive performance of an updated polygenic risk score for age-related macular degeneration. Ophthalmology. 2024;131(8):880–891. doi:10.1016/j.ophtha.2024.01.033
43. NSO. NSO Malta | world Population Day: 11 July 2024 - NSO Malta. National Statistics Office; 2024. Available from: https://nso.gov.mt/world-population-day-11-july-2024/.
44. Cuschieri S, Vassallo J, Calleja N, et al. Prevalence of obesity in Malta. Obes Sci Pract. 2016;2(4):466–470. doi:10.1002/osp4.77
45. Galdies C. The state of the climate 2022 - A multidecadal report and assessment of Malta’s climate. 2022.
46. World Health Organisation. Exposure to solar ultraviolet (UV) radiation - Data by country. World Health Organisation; 2004. Available from: https://apps.who.int/gho/data/view.main.35300.
47. Eurostat. Tobacco Consumption Statistics - Statistics Explained - Eurostat. 2022. Available from: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Tobacco_consumption_statistics.
48. Damato FJ. Incidence and causes of blindness in the Maltese Islands: a survey based on the examination of 638 blind persons. Br J Ophthalmol. 1960;44(3):164–171. doi:10.1136/BJO.44.3.164
49. Cachia J, Soler R, Blagojevic M, Agius Muscat H. Prevalance Study of Glaucoma in Malta and Gozo. Vol IV. 1992. Available from: http://www.um.edu.mt/library/e-articles/mmj/mmj040120.pdf.
50. Agius D, Mamo J, Hammond C, Calleja N, Carbonaro F. The Study Design and Methodology of the Malta Eye Study (TMES), an ophthalmic epidemiology study. South East Eur J Public Health. 2024. doi:10.52710/seejph.498
51. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
52. The World Medical Association. Declaration of Helsinki – ethical Principles for Medical Research Involving Human Subjects. 1964. Available from: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/.
53. European Parliament and Council. General Data Protection Regulation (GDPR) compliance guidelines. 2016. Available from: https://gdpr.eu/.
54. Gordon-Shaag A, Piñero DP, Kahloun C, et al. Validation of refraction and anterior segment parameters by a new multi-diagnostic platform (VX120). J Optom. 2018;11(4):242–251. doi:10.1016/J.OPTOM.2017.12.003
55. Ardourel JE. Risk factors associated with age-related macular degeneration: a case-control study in the age-related eye disease study: age-related eye disease study report number 3. Ophthalmology. 2000;107(12):2224–2232. doi:10.1016/S0161-6420(00)00409-7
56. Shoukri MM, Asyali MH, Donner A. Sample size requirements for the design of reliability study: review and new results. Stat Methods Med Res. 2016;13(4):251–271. doi:10.1191/0962280204SM365RA
57. IBM Corp. IBM SPSS statistics for windows, version 23.0. 2015.
58. NSO. Census of population and housing 2021: final report: population, migration and other social characteristics volume 1. 2023. Available from: https://nso.gov.mt/events/census-of-population-and-housing-2021-final-report-population-migration-and-other-social-characteristics/.
59. Gorman BR, Voloudakis G, Igo RP, et al. Genome-wide association analyses identify distinct genetic architectures for age-related macular degeneration across ancestries. Nat Genet. 2024;56(12):2659–2671. doi:10.1038/S41588-024-01764-0
60. Caruana J. Population genetics of Western Mediterranean Islands - Malta: a case study - research explorer The University of Manchester. The University of Manchester; 2013. Available from: https://research.manchester.ac.uk/en/studentTheses/population-genetics-of-western-mediterranean-islands-malta-a-case?utm_source=chatgpt.com.
61. Lazaridis I, Patterson N, Mittnik A, et al. Ancient human genomes suggest three ancestral populations for present-day Europeans. Nature. 2014;513(7518):409–413. doi:10.1038/NATURE13673
62. Capelli C, Redhead N, Romano V, et al. Population structure in the Mediterranean basin: a Y chromosome perspective. Ann Hum Genet. 2006;70(2):207–225. doi:10.1111/J.1529-8817.2005.00224.X
63. Pagliarini S, Moramarco A, Wonnald RPL, et al. Age-related macular disease in rural southern Italy. Arch Ophthalmol. 1997;115(5):616–622. doi:10.1001/ARCHOPHT.1997.01100150618007
64. Kozobolis VP, Detorakis ET, Tsilimbaris MK, Vlachonikolis LG, Tsambarlakis LC, Palliharis LG. Correlation between age-related macular degeneration and pseudoexfoliation syndrome in the population of Crete (Greece). Arch Ophthalmol. 1999;117(5):664–669. doi:10.1001/ARCHOPHT.117.5.664
65. Serra R. Age-related macular degeneration analysis from SardiNIA project. Università degli studi di Sassari; 2022. Available from: https://tesidottorato.depositolegale.it/static/PDF/web/viewer.jsp.
66. Piermarocchi S, Segato T, Scopa P, et al. The prevalence of age-related macular degeneration in Italy (PAMDI) study: report 1. Ophthalmic Epidemiol. 2011;18(3):129–136. doi:10.3109/09286586.2011.574334
67. Barreto P, Farinha C, Coimbra R, et al. Interaction between genetics and the adherence to the Mediterranean diet: the risk for age-related macular degeneration. Coimbra Eye Study Report 8. Eye Vision. 2023;10(1):1–13. doi:10.1186/S40662-023-00355-0/FIGURES/4
68. Chong EWT, Robman LD, Simpson JA, et al. Fat consumption and its association with age-related macular degeneration. Arch Ophthalmol. 2009;127(5):674–680. doi:10.1001/ARCHOPHTHALMOL.2009.60
69. Rahmati M, Smith L, Lee H, et al. Associations between vision impairment and eye diseases with dementia, dementia subtypes and cognitive impairment: an umbrella review. Ageing Res Rev. 2024;101:102523. doi:10.1016/J.ARR.2024.102523
70. Tsai HR, Lo RY, Liang KH, et al. Risk of subsequent dementia or Alzheimer disease among patients with age-related macular degeneration: a systematic review and meta-analysis. Am J Ophthalmol. 2023;247:161–169. doi:10.1016/J.AJO.2022.11.005
71. Rim TH, Lee CS, Lee SC, Kim S, Kim SS. Association between previous cataract surgery and age-related macular degeneration. Semin Ophthalmol. 2017;32(4):466–473. doi:10.3109/08820538.2015.1119861
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.