Back to Journals » International Medical Case Reports Journal » Volume 18
Marcus-Gunn Jaw-Winking Phenomenon: A Case Report on Rare Oculofacial Synkinesis
Authors Alharthe AFH, Alghreeb HM, ALBalawi HB, ALAli NM
Received 3 February 2025
Accepted for publication 1 August 2025
Published 18 August 2025 Volume 2025:18 Pages 1053—1056
DOI https://doi.org/10.2147/IMCRJ.S520496
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Supplementary video of “Marcus-Gunn jaw-winking phenomenon” [520496].
Views: 3671
Amjad Fiusal H Alharthe,1 Hagar Mohammad Alghreeb,2 Hani B ALBalawi,1 Naif M ALAli1
1Division of Ophthalmology, Department of Surgery, Faculty of Medicine, University of Tabuk, Tabuk, Saudi Arabia; 2Department of Ophthalmology, Neem Medical Center, Tabuk, Kingdom of Saudi Arabia
Correspondence: Naif M ALAli, Email [email protected]
Abstract: The Marcus-Gunn jaw-winking phenomenon (MGJWP) is an uncommon congenital oculofacial synkinesis resulting from abnormal innervation between the fifth cranial nerve (trigeminal, CN V) and the third cranial nerve (oculomotor, CN III). This case report presents a 5-month-old girl with characteristic left eyelid elevation during suckling movements, highlighting the importance of clinical observation in early diagnosis. The condition was confirmed based on clinical findings, with no associated neurological or structural abnormalities. Management involved observation and follow-up to monitor potential complications such as strabismus or anisometropia. MGJWP remains an essential consideration in cases of unusual eyelid movement, emphasizing the role of multidisciplinary consultation for comprehensive care.
Keywords: Marcus-Gunn jaw-winking phenomenon, congenital synkinesis, oculomotor nerve, trigeminal nerve, eyelid movement
Introduction
After pseudo-inferior oblique overaction and Duane’s retraction syndrome (DRS), Marcus-Gunn jaw-winking phenomenon (MGJWP), also called trigeminal-oculomotor synkinesis, is one of the most prevalent forms of congenital abnormal ocular innervation.1 Robert Marcus Gunn initially documented the condition more than 130 years ago in a woman who had upper eyelid contractions while chewing and unilateral blepharoptosis.1 This results from an aberrant connection between the mandibular division of the trigeminal nerve and the superior division of the oculomotor nerve, which innervates the levator palpebrae superioris muscle.2 The pterygoid muscle is engaged in a variety of activities, such as smiling, swallowing, eating, and shifting the jaw to the side, which can lead to this condition, which is almost usually intermittent.2 Although some forms can develop as a result of infections, trauma, surgery, or pontine tumors, the disorder is congenital.3 Strabismus occurs as complication of the phenomenon in 50–60% cases while 5–25% for anisometropia, and 30–60% of patients have Amblyopia.4
Case Presentation
A 5-month-old full-term girl was brought to a private outpatient clinic due to involuntary movement of her left eyelid, observed by the parents since she was one month old. The eyelid movement was noted to occur consistently during bottle feeding, particularly during sucking motions (Figures 1) (Video S1).
 |
Figure 1 Showing involuntary movement of left eyelid while sucking. |
The parents are consanguineous, but there is no family history of similar conditions. Examination findings are repetitive elevation of the left eyelid was consistently triggered by sucking movements. Full extra-ocular movement was observed in both eyes. No ptosis was noted in the primary position. Corneas were clear, and the conjunctiva was quiet. Fundus examination revealed no abnormalities, and pupils were normal. Normal cover test results. Cycloplegic Refraction: right eye (OD): +3.50 −1.50 × 140 and Left eye (OS): +2.25 −2.25 × 180. Normal physical and neurological findings. Marcus Gunn jaw-winking phenomenon was evident during near accommodation and suckling movements. Observation and follow-up by an ophthalmologist were advised to monitor the condition and ensure no progression or associated complications.
Discussion
Marcus Gunn phenomenon is sporadic, however familial instances with abnormal autosomal dominant inheritance were reported, suggesting a genetic aspect in a few instances.1 Each time the jaw moves, It is defined by the rapid upward movement of one upper eyelid in a fast-rising movement. Parents or guardians often notice the synkinetic movement when their children are young, which helps in making a diagnosis. However, some cases go unrecognized until the child reaches puberty.4 It occurs in 4 to 6% of people who were born with ptosis.5 The most common causes of a raised lid are chewing or sucking, although other causes include smiling, yawning, sternocleidomastoid contraction, tongue protrusion, Valsalva maneuver, inhalation, and lateral mandibular movement.1 It is almost always unilateral, typically affects the left side, and is accompanied with ipsilateral superior rectus muscular under action in around 80% of the cases.5 There are two hypotheses regarding explanation of this phenomenon the first one is “release hypothesis”, which holds that abnormal links between the oculomotor nucleus and the neighboring trigeminal mesencephalic nucleus are a remnant of a primal reflex that vanished throughout evolutionary development.1 Synkinetic lid and jaw movement results from the release and activation of this basic reflex due to prenatal trauma or other unidentified reasons.1 According to the second one, MGJWP results from a brainstem structural anomaly that causes trigeminal motor axons to LPS to be neurally misdirected.1 The differential diagnosis of Marcus Gunn phenomenon includes congenital ptosis, blepharophimosis syndrome, third nerve palsy, and Duane retraction syndrome (Table 1). It is crucial to make an accurate diagnosis using the patient’s medical history, pupillary examination, and extraocular movements.6 They can result from a variety of factors, including inflammation, ischemia, trauma, and space-occupying lesions like tumors and aneurysms.7 One category of congenital cranial dysinnervation disorder is Duane Retraction Syndrome (DRS). It is distinguished by the absence of normal nerve innervation, which can be seen using sophisticated imaging methods that show either the abducens nerve is absent or hypoplastic. The lateral rectus muscle, which is innervated by an atypical offshoot of the oculomotor nerve, also experiences misinnervation in DRS.8 Blepharophimosis, ptosis, epicanthus inversus, and telecanthus are the four orbito-palpebral abnormalities that make up the rare autosomal dominant genetic disorder known as Blepharophimosis-Ptosis-Epicanthus Inversus Syndrome. The diagnosis requires a complete history and examination, including observation of jaw movement, extraocular muscle testing, and facial features while Neuroimaging or genetic analysis may be indicated based on clinical presentation.9 It should be mentioned that due to the possibility of related disorders and secondary complications like strabismus which occur in 50–60% and anisometropia, which occur in 5–25% of cases, patients with a MGS should be referred as soon as possible for consultation in pediatric neurology and ophthalmology.3 Surgical intervention and observation are two possible treatment options.10 An observational strategy with frequent follow-up and monitoring is advised if the symptoms are steady and not impairing their ability to function.11 Surgical correction may be considered in extreme situations or if the patient is experiencing severe psychological or social distress.10 If amblyopia is present, it should be treated with occlusion therapy and correction of anisometropia before beginning any lid surgical intervention. Four to Six months clinic visiting is recommended and frequent photographs are helpful in monitoring the patients. Additionally, due to the possibility of pressure by the ptotic lid, astigmatism should be checked with every clinic visit. Attempting to address ptosis without simultaneously correcting the jaw winking may lead to an intensification of the abnormal movement of the eyelid, which could be deemed cosmetically unacceptable According to Dillman and Anderson, Eliminating a minor part of the levator muscle situated above Whitnall’s ligament is adequate to entirely impair its function without resulting in considerable dissection or harm to the eyelid.12 Beard and others have supported bilateral frontalis suspension and bilateral levator muscle excision. With this method, the wink is virtually eliminated, and the symmetry is improved.13 If the postoperative result is considered disappointed, further surgery on the opposite side may be offered. Kersten et al suggest performing unilateral levator muscle excision and frontalis sling solely on the side that is affected.14 The Marcus Gunn Phenomenon, a rare congenital condition, is often underdiagnosed. Pediatricians should remain vigilant and recommend routine eye examinations to detect associated abnormalities. Early recognition ensures timely intervention and better outcomes for affected children. The case report limitations are absence of long-term follow-up of the patient to assess the outcomes and potential late complications like amblyopia, strabismus, anisometropia, psychosocial challenges. Additionally, the case report reveals a negative family history but does not explore the genetic analysis.
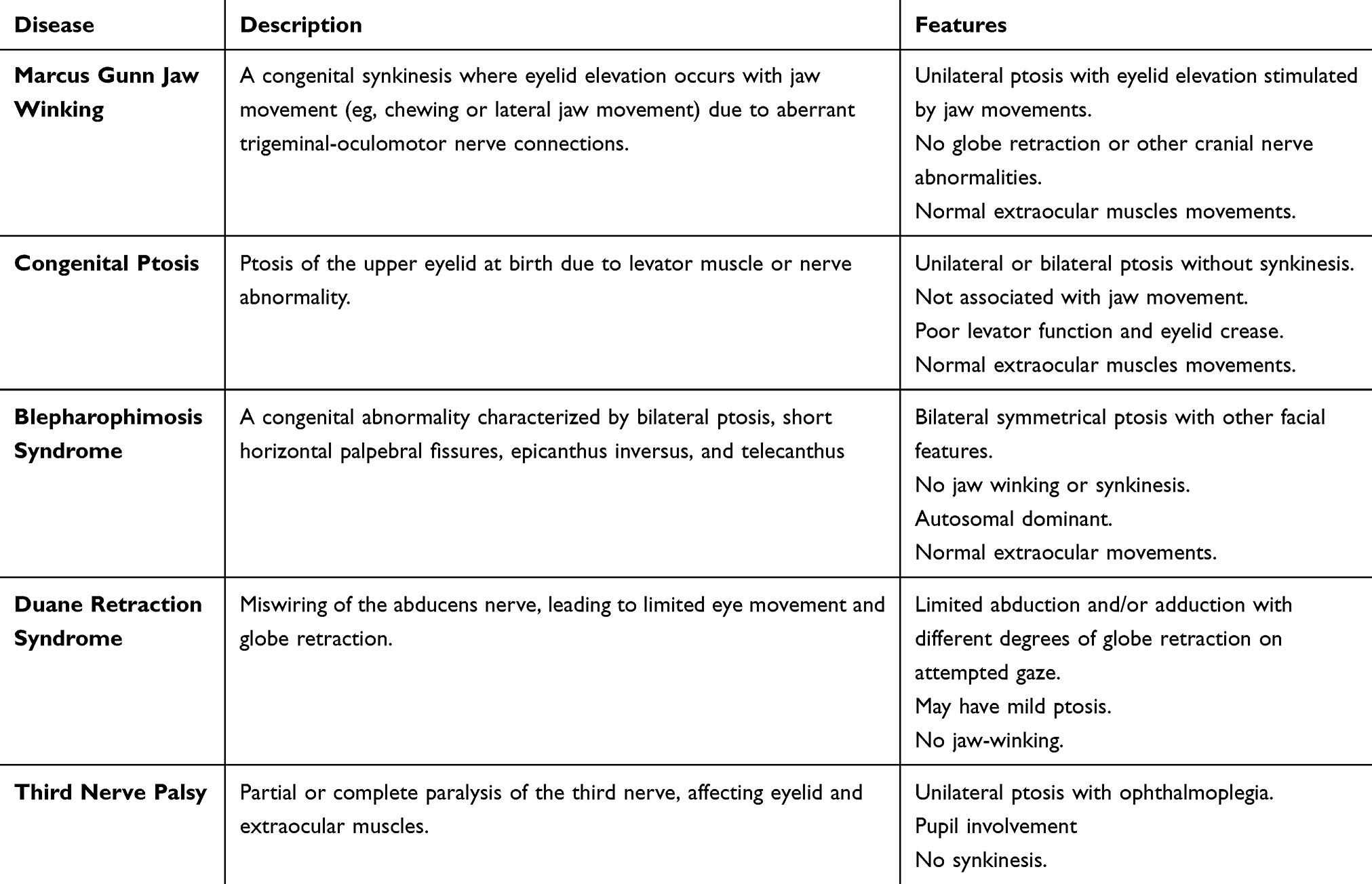 |
Table 1 Differential Diagnosis of MGJW with Distinguishing Features |
Conclusion
Marcus-Gunn jaw-winking phenomenon is a congenital condition that can significantly impact ocular function and patient quality of life. Early diagnosis is pivotal in preventing secondary complications such as strabismus and anisometropia, which are frequently associated with this condition. This case underscores the importance of detailed clinical evaluation and long-term follow-up to ensure optimal management. Regular follow-up is important since complications can develop over time and may not be obvious at the initial presentation. It is critical to monitor the visual development including binocular vision and refractive errors of the patient to prevent complications as amblyopia. Multidisciplinary collaboration among ophthalmologists, neurologists, and pediatricians is crucial for addressing patient-specific needs and monitoring for potential complications.
Institutional Approval
Waived as case report without any intervention.
Consent for Publication
Written informed consent was obtained from parents for case publication and any accompanying images.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alam MS, Nishanth S, Ramasubramanian S, Swaminathan M, Mukherjee B. The rare phenomenon of Marcus-Gunn jaw winking without ptosis: report of 14 cases and review of the literature. Indian J Ophthalmol. 2020;68(6):1132–1135. doi:10.4103/ijo.IJO_1099_19
2. Sano K. Trigemino-oculomotor synkinesis. Neurology. 1959;9(5):332–335.
3. Barreira C, Barreira R. Marcus Gunn syndrome in primary care: a case report. Cureus. 2023;15(8):e43738. doi:10.7759/cureus.43738
4. Ziga N, Biscevic A, Pjano MA, Pidro A. Marcus Gunn Jaw-Winking syndrome: a case report. Med arch. 2019;73(4):282–284. doi:10.5455/medarh.2019.73.282-284
5. Pandey M, Baduni N, Jain A, Sanwal MK, Vajifdar H. Abnormal oculocardiac reflex in two patients with Marcus Gunn syndrome. J Anaesthesiol Clin Pharmacol. 2011;27(3):398–399. doi:10.4103/0970-9185.83693
6. Schroeder RM, Stunkel L, Gowder MTA, et al. Misdiagnosis of third nerve palsy. J Neuroophthalmol. 2022;42(1):121–125. doi:10.1097/WNO.0000000000001010
7. Hörner R, Kassubek J, Dreyhaupt J, Ludolph AC. The spectrum and differential diagnosis of acquired ocular motor nerve palsies: a clinical study of 502 patients. J Neurol. 2022;269(4):2140–2148. doi:10.1007/s00415-021-10761-w
8. Khorrami-Nejad M, Akbari MR, Masoomian B, Mahmood HA, Daneshvar K, Majdi A. Astigmatism in Duane retraction syndrome. BMC Ophthalmol. 2025;25(1):15. doi:10.1186/s12886-025-03855-w
9. Nabih O, Arab L, El Maaloum L, Allali B, El Kettani A. Bilateral cataract in a child with blepharophimosis-ptosis-epicanthus inversus syndrome: a surgical challenge. Int J Surg Case Rep. 2022;92:106845. doi:10.1016/j.ijscr.2022.106845
10. Sathish S, Subramani M, Patel P, Hirani N, Arjunan P. Marcus Gunn Jaw-Winking syndrome: a case report. Acta Marisiensis Seria Medica. 2023;69(4):302–304. doi:10.2478/amma-2023-0040
11. Kirkham TH. Familial Marcus Gunn phenomenon. Br J Ophthalmol. 1969;53(4):282–283. doi:10.1136/bjo.53.4.282
12. Dillman DB, Anderson RL. Levator myomectomy in synkinetic ptosis. Arch Ophthalmol. 1984;102(3):422–423. doi:10.1001/archopht.1984.01040030340033
13. Beard C. A new treatment for severe unilateral congenital ptosis and for ptosis with jaw winking. Am J Ophthalmol. 1965;59:252–258. doi:10.1016/0002-9394(65)94789-6
14. Kersten RC, Bernardini FP, Khouri L, et al. Unilateral frontalis sling for the surgical correction of unilateral poor-function ptosis. Ophthal Plast Reconstr Surg. 2005;21(6):
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.