Back to Journals » Psychology Research and Behavior Management » Volume 19
Mapping the Cognitive Constructs Assessed by the Allen Cognitive Level Screen: A Scoping Review
Authors Liu GH ![]() , Pordage L
, Pordage L ![]() , Pan TC, Chou LW
, Pan TC, Chou LW ![]() , Ma WF
, Ma WF
Received 5 January 2026
Accepted for publication 26 March 2026
Published 9 April 2026 Volume 2026:19 593468
DOI https://doi.org/10.2147/PRBM.S593468
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Igor Elman
Guang-Hsing Liu,1,2 Loren Pordage,3 Tzu-Chi Pan,4 Li-Wei Chou,5– 7,* Wei-Fen Ma8,9,*
1Ph.D. Program in Healthcare Science, Division in Rehabilitation Science, China Medical University, Taichung, Taiwan; 2Department of Psychiatry, China Medical University Hospital, Taichung, Taiwan; 3ACDMweb, Sydney, Australia; 4Office of the Superintendent, Evergreen General Hospital, Taoyuan, Taiwan; 5Department of Physical Medicine and Rehabilitation, China Medical University Hospital, Taichung, Taiwan; 6Department of Physical Therapy and Graduate Institute of Rehabilitation Science, China Medical University, Taichung, Taiwan; 7Department of Physical Medicine and Rehabilitation, Asia University Hospital, Asia University, Taichung, Taiwan; 8Department of Nursing, China Medical University Hospital, Taichung, Taiwan; 9School of Nursing, China Medical University, Taichung, Taiwan
*These authors contributed equally to this work
Correspondence: Li-Wei Chou, Department of Physical Medicine and Rehabilitation, China Medical University Hospital, No. 2 Yuh-Der Road, Taichung, 404332, Taiwan, Tel +886-4-22052121 ext. 12601, Email [email protected] Wei-Fen Ma, School of Nursing, China Medical University, No. 100, Sec. 1, Jingmao Road, Beitun Dist, Taichung, 406040, Taiwan, Tel +886-4-22053366 ext. 7107, Email [email protected]
Purpose: Despite widespread clinical use for over four decades, the precise cognitive constructs assessed by the Allen Cognitive Level Screen (ACLS) remain unresolved. This scoping review examines quantitative relationships between ACLS scores and standardized cognitive assessments to clarify which cognitive abilities the ACLS captures and inform its integration alongside traditional cognitive evaluations.
Methods: Following Arksey and O’Malley’s framework, we searched five databases (PubMed, Embase, Web of Science, CINAHL, PsycINFO) from inception through December 2025. Studies were included if they reported empirical data from clinical populations, used any ACLS version, included standardized cognitive measures, and reported correlation analyses. Two independent reviewers screened 222 records. Cognitive measures were classified into nine domains based on Lezak’s neuropsychological taxonomy. Correlation strength was categorized according to Cohen’s conventions: weak (r < 0.30), moderate (0.30 ≤ r < 0.50), or strong (r ≥ 0.50).
Results: Twenty-four studies, encompassing 1951 participants across six diagnostic groups, met the inclusion criteria. Of 117 quantitative relationships examined, 73.5% were statistically significant. The ACLS showed the strongest associations with global cognition, social cognition, and executive function, with significance rates ranging from 81.5% to 94.7%. Associations were comparatively weaker across memory, visuospatial, and orientation domains, ranging from 33.3% to 50.0%. Correlation patterns varied across populations and ACLS versions, with only one study examining the current ACLS-6.
Conclusion: The ACLS demonstrates reliable associations with integrated cognitive processes, particularly global functioning, executive abilities, and attention-processing capacities, rather than discrete cognitive components. These findings suggest the ACLS may reflect observable patterns of sensorimotor information processing during purposeful activity. Clinicians should therefore interpret ACLS results as a complement to, rather than a substitute for, traditional domain-specific cognitive assessments, particularly when precise differentiation of cognitive deficits is required for treatment planning. Critical gaps in structural validity research and ACLS-6 which currently constrain definitive conclusions regarding the instrument’s construct validity.
Keywords: Allen cognitive level screen, neuropsychological testing, performance-based assessment, functional cognition
Introduction
Cognition encompasses the mental processes through which individuals acquire, process, store, and utilize information to guide behavior.1 In clinical psychology and psychiatric practice, cognitive assessment serves critical functions including establishing diagnosis, predicting functional outcomes, and informing treatment plan.2 Laboratory-based neuropsychological assessments have established distinctive cognitive profiles across clinical populations. Individuals with schizophrenia spectrum disorders typically demonstrate executive dysfunction and working memory impairments,3 dementia involves progressive memory and visuospatial deterioration,4 substance use disorders associate with compromised executive control,5 and cerebrovascular accidents affect domain-specific functions in approximately 80% of survivors.6
However, mounting evidence reveals a persistent dissociation between neuropsychological test performance and everyday functional abilities, what researchers term the “capacity-performance gap”.7,8 This reflects the fundamental difference between measuring discrete cognitive capacities in controlled conditions versus evaluating integrated performance in naturalistic contexts.9 Clients may perform adequately on standardized tests yet struggle with daily activities, while others with substantial test deficits demonstrate surprising functional competence through compensatory strategies. Multiple factors moderate this translation, including motivation, emotional regulation, environmental support, task familiarity, and metacognitive awareness.8 This unpredictability challenges practitioners to develop targeted occupation-based interventions, allocate support services, and make informed placement decisions.
Recognition of the limitations has driven occupational therapy’s emphasis on functional cognition, cognitive processes as they manifest within meaningful activities.10,11 Rather than quantifying isolated capacities, occupational therapy employs “top-down” assessment methodologies prioritizing observation of actual task performance.12 This approach directly addresses: “What can this person actually accomplish in daily life?” For multidisciplinary teams, functional cognitive assessment bridges the gap between neuropsychological data and intervention planning, providing actionable information about task demands, environmental modifications, and support requirements.
The Allen Cognitive Level Screen (ACLS), grounded in the Allen Cognitive Disabilities Model (ACDM) pioneered by Claudia Kay Allen in the late 1960s, represents one of the earliest systematic attempts to integrate cognitive assessment with functional task analysis.13–15 The ACLS employs performance-based methods using leather-lacing and additional activities to observe how individuals process sensorimotor information during tasks. ACLS is a series of standardized craft-based tasks that observe the sensorimotor information processing system, specifically how a person attends to sensory cues (Input), processes cues (Throughput), and executes voluntary motor actions (Output). Earlier versions (ACLS-1 through ACLS-5) relied on leather-lacing stitches of increasing complexity; ACLS-6 introduced additional tasks at each level to provide complementary ways to demonstrate performance.14
The ACLS is administered by trained occupational therapists, who observe and score the individual’s performance on standardized stitching tasks corresponding to Levels 3 through 5 of the Allen Cognitive Level (ACL) scale: the running stitch reflects Level 3, characterized by the processing of linear information through repetitive motor responses; the whip stitch corresponds to Level 4, requiring the processing of classification information through goal-directed behavior and imitation of demonstrated procedures; and the single cordovan stitch aligns with Level 5, demanding the processing of tangible information through independent problem-solving and perception of surface and spatial relationships. (Table 1) The resulting ACL score assists occupational therapists in determining the level of environmental support or caregiver assistance an individual may require in daily living.14,15
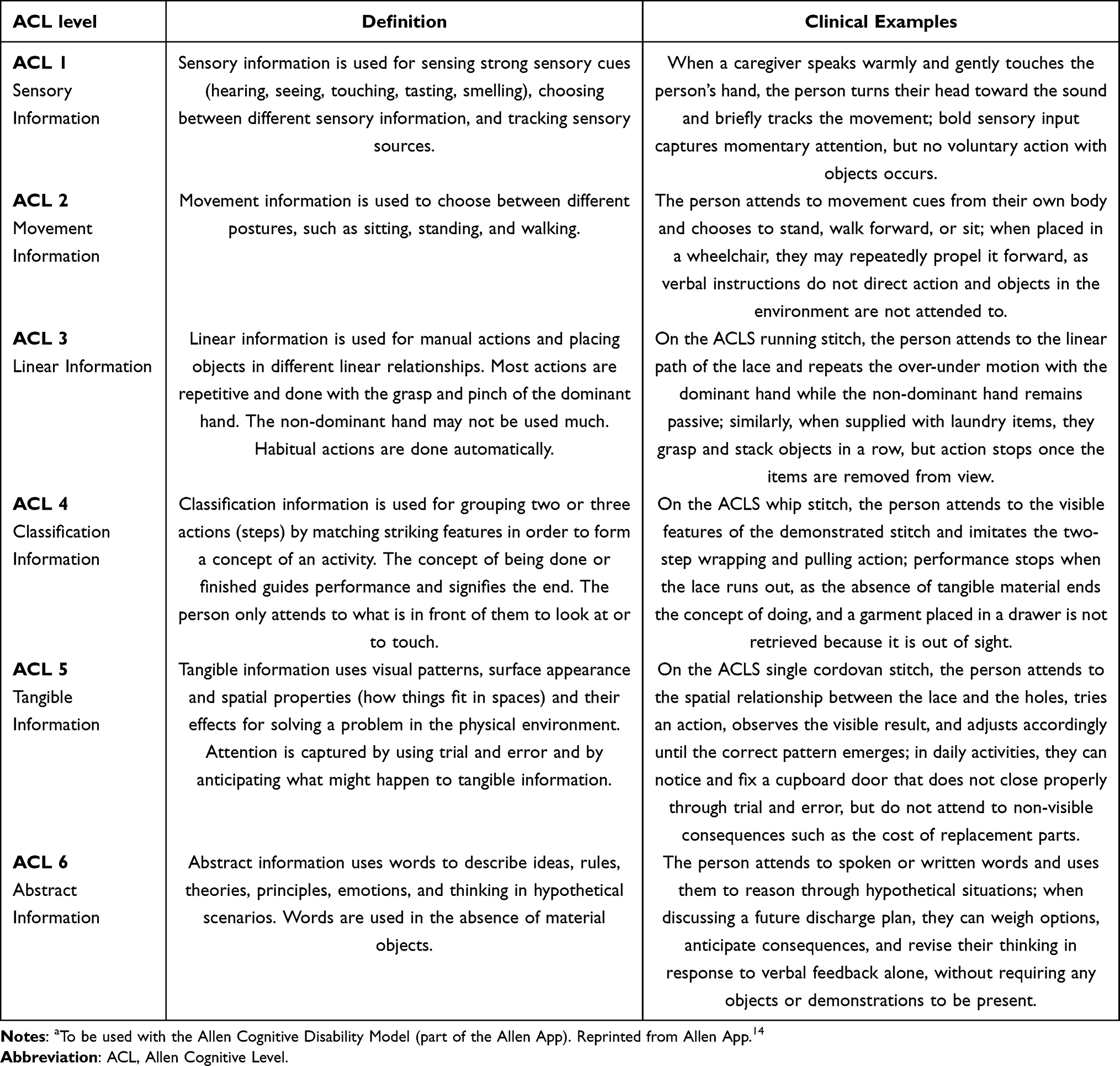 |
Table 1 Allen Cognitive Levelsa |
The ACLS has been extensively utilized across mental health, geriatric, and neurological settings. A recent U.S. national survey of occupational therapy practitioners revealed the ACLS (15.2%) as the most widely used standardized functional cognitive measure when evaluating cognition in adults.16 Clinicians use ACL scores to match task demands to cognitive capacity, design environmental modifications, and establish realistic goals. The ACLS has evolved considerably over four decades. Initially questioned regarding face validity issue, like whether leather-lacing could predict generalized competence,13 the assessment was reconceptualized to evaluate “capacity to learn other visuomotor tasks”,17 then broadened to measure “best ability to function”,18 and ultimately refined to focus on “functional cognition”.14,19 The current version, ACLS-6, positions the assessment as observing “effects caused by aroused attention in several actions” while indicating “quality of information processing and global functional ability”.14
Despite widespread clinical adoption, fundamental questions remain unresolved regarding what the ACLS actually measures. The ACDM proposes that function reflects the brain’s information-processing capabilities, as observed when tasks engage attention through sensorimotor cues,14 yet empirical validation of this theoretical foundation remains limited. A recent scoping review found ACLS scores correlate strongly with functional capacity (89% of tasks) but less consistently with real-world adaptive performance (64% of activities),20 suggesting that the cognitive dimensions captured by the ACLS may differ across levels of functional performance, with its precise measurement construct warranting further investigation.
Critically, it remains unclear which specific cognitive domains the ACLS taps, and whether these craft-based tasks accurately reflect what individuals can do in daily life. This scoping review therefore examines published research on correlations between ACLS scores and cognitive domain assessments to clarify what cognitive abilities the ACLS measures. By synthesizing evidence across diverse populations, cognitive measures, and ACLS versions, this review aims to strengthen the theoretical foundation of functional cognitive assessment and provide practical guidance for clinicians integrating the ACLS into comprehensive evaluations.
Materials and Methods
Design
Scoping reviews are effective when research is still in development. Given variation in cognitive measure across studies, we required a more comprehensive approach. This method enables us to map what’s out there and identify the types of evidence that exist.21 We followed Arksey and O’Malley’s framework to examine peer-reviewed literature on relationships between the ACLS and cognitive assessments.
Stage 1: Identifying the Research Question
Our primary question was:
What is known from published, peer-reviewed literature about quantitative relationships between scores on the ACLS (and its variants) and performance on measures of cognitive function across different populations?
Stage 2: Identifying Relevant Studies
We searched five databases (PubMed, Embase, Web of Science, CINAHL, and PsycINFO) from inception through December 2025 using the following search term: (“Allen Cogn*”). Database-specific syntax was applied accordingly. The Allen Cognitive Network Bibliography helped identify potentially missed literature. Manual searches of developer Claudia Kay Allen’s publications revealed two studies that were embedded within the Loewenstein Occupational Therapy Cognitive Assessment (LOTCA) psychometric research.22,23
Stage 3: Study Selection
We followed a systematic screening process with two independent reviewers (G.-H. Liu and T.-C Pan). As shown in Figure 1. First, we screened all titles and abstracts against our eligibility criteria. The study selection process included the removal of duplicates. Studies moved to full-text review if they appeared to meet inclusion criteria or if eligibility was unclear from the abstract. During full-text review, we documented reasons for exclusion. Disagreements were resolved through discussion, with a third reviewer available for consultation if consensus could not be reached.
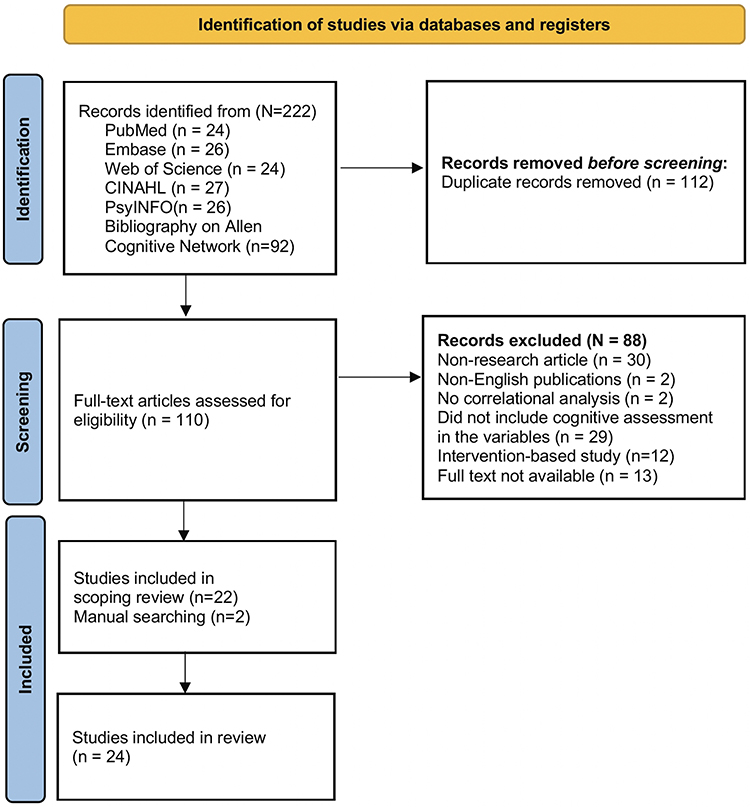 |
Figure 1 Study Selection PRISMA Diagram. |
Our inclusion criteria required studies to: (a) be published in peer-reviewed journals in English, (b) include participants from clinical populations, (c) report empirical data using any ACLS version, as each version represents a refinement of the same underlying cognitive disabilities model and measures the same six-level cognitive continuum,14,15 and (d) include at least one standardized cognitive measure. We excluded studies that focused solely on functional outcomes without cognitive measurement. Conference abstracts, and dissertations sources were also excluded.
After full-text assessment of 110 articles, 88 were excluded for the following reasons: non-research articles (n = 30), studies that did not include cognitive assessment in the variables (n = 29), full text not available (n = 13), intervention-based studies (n = 12), non-English publications (n = 2), and studies with no correlational analysis (n = 2). Combined with two additional studies identified through manual searching, a total of 24 studies were included in this scoping review.
This broad inclusion of diverse clinical populations and multiple instrument versions was intentional, aligning with the scoping review’s objective to comprehensively map the available evidence and identify cross-cutting patterns across the tool’s 40-year development.
Stage 4: Charting the Data
Data extraction captured study characteristics including authors, year, participant demographics, setting, ACLS version used, and ACLS scores. Cognitive measures were extracted and classified into nine domains mapped onto Lezak’s neuropsychological taxonomy1 and functional cognition concepts.10 Statistical results were categorized by correlation strength following Cohen’s conventions:24 weak (r < 0.30), moderate (r = 0.30–0.50), or strong (r ≥ 0.50). Crucially, we accounted for the directionality of scoring. For cognitive assessments where lower scores indicate better performance (eg., TMT-B, error counts), a negative correlation with the ACLS (where higher scores indicate better function) represents a positive convergent validity. These inverse relationships were interpreted as supporting the association between the constructs.
Global cognition captures overall cognitive performance across multiple functions. Since brain function is too complex to be represented by a single score, this domain encompasses composite performance. Measures included the Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), Intelligence Quotient (IQ) scores, and LOTCA Total Score.
Executive function involves the abilities needed for independent, purposive behavior, basically volition, planning, purposive action, and effective performance. We included the Wisconsin Card Sorting Test (WCST), Trail Making Test Part B (TMT-B), verbal fluency tasks, Prefrontal Symptom Inventory (PSI), LOTCA Thinking Operations, and various measures of abstraction.
Attention/processing speed/working memory combines related but distinct abilities. Attention involves becoming receptive to stimuli; processing speed refers to how quickly we perform mental and motor responses; working memory temporarily stores and processes information to guide behavior. This domain included the Symbol Digit Modalities Test (SDMT), Continuous Performance Test (CPT), Digit Symbol, TMT Part A (TMT-A), digit span tasks, reaction time measures, and LOTCA Execution time.
Memory/learning covers retention and acquisition of information. Memory involves retaining and recalling previous experiences, while learning represents acquiring and storing new information. We examined verbal learning tasks, including the Hopkins Verbal Learning Test (HVLT), the Rey Auditory Verbal Learning Test (RAVLT), the Logical Memory test, and the Perceptual Memory Task (PMT) factors.
Verbal and language encompass functions that process verbal and symbolic information. Core impairments include difficulties with comprehending and formulating verbal messages. Measures included Verbal IQ, vocabulary tests, and the Boston Naming Test (BNT).
Visuospatial/perceptual involves integrating sensory impressions and processing complex visual patterns that cannot be easily verbalized. We included Picture Arrangement, Picture Completion, the Hooper Visual Organization Test (HVOT), and LOTCA visual and spatial perception subscales.
Visual-motor constructional/psychomotor skills encompass building and assembling activities where spatial form is important, as well as motor response speed. Measures included Block Design, Object Assembly, the Beery-Buktenica Developmental Test of Visual-Motor Integration (VMI), LOTCA visuomotor organization and motor praxis, and Finger Tapping.
Social cognition involves the abilities necessary for effective interaction, including practical judgment and appropriate social conduct. We examined the Social Interaction Test (SIT), the Problem-Solving Verbal Reaction to Everyday Problematic Situations (PVRS), the Cartoon Intention Inference Task (CIIT), and the Social Behavior Sequencing Task (SBST).
Functional cognition refers to cognitive abilities as they manifest in daily tasks, examining an individual’s capacity to perform essential tasks given their overall abilities, rather than just specific skills in isolation. Measures included the Assessment of Motor and Process Skills (AMPS), Executive Function Performance Test (EFPT), and Allen Diagnostic Module (ADM). Orientation simply refers to awareness of person, place, and time, assessed through the LOTCA Orientation subscale.
Stage 5: Collating, Summarizing, and Reporting Results
We synthesized data both numerically and thematically, calculating the proportion of significant findings for each cognitive domain to identify patterns across studies.
Results
Study Characteristics
Twenty-four studies published between 1988 to 2023 included 1,951 participants across six diagnostic groups (Table 2). Outpatient psychotic spectrum disorders formed the largest group (7 studies, 635 participants), followed by inpatient psychotic spectrum disorders (5 studies, 420 participants), elderly/neurocognitive disorders (4 studies, 372 participants), substance use disorders (3 studies, 332 participants), neurological disorders (4 studies, 168 participants), and youth (1 study, 24 emotionally disturbed boys). Research was conducted in the United States (n=8), Spain (n=4), Israel (n=3), Taiwan (n=3), South Korea (n=2), Australia (n=1), Hong Kong (n=1), Netherland (n=1), and Turkey (n=1). Sample sizes ranged from 24 to 232 participants. A notable finding regarding assessment versioning emerged: studies were predominantly conducted using older ACLS versions, specifically ACLS-3 (n=10, 41.7%) and ACLS-5 (n=10, 41.7%), with only minimal representation of ACLS-2 (n=3, 12.5%) and the current version, ACLS-6 (n=1, 4.2%).
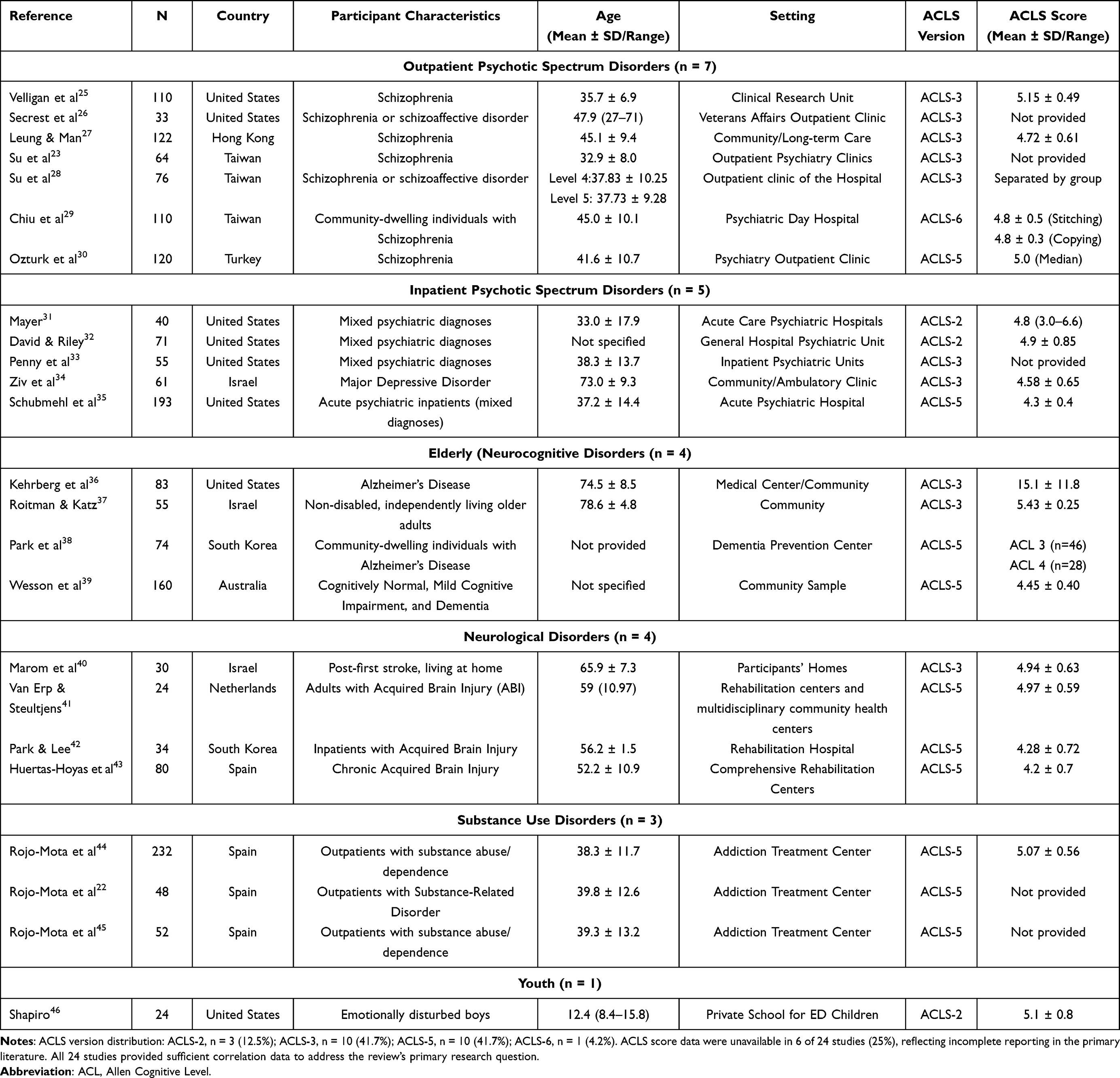 |
Table 2 Overview of Studies in the Scoping Review |
Patterns of Correlations Across Cognitive Domains
Of 117 quantitative relationships examined between ACLS scores and cognitive measures, 86 were statistically significant (73.5%). Figure 2 presents the proportion of significant findings and distribution of effect sizes across cognitive domains. Detailed correlation data for all specific measures are provided in Supplementary Table S1.
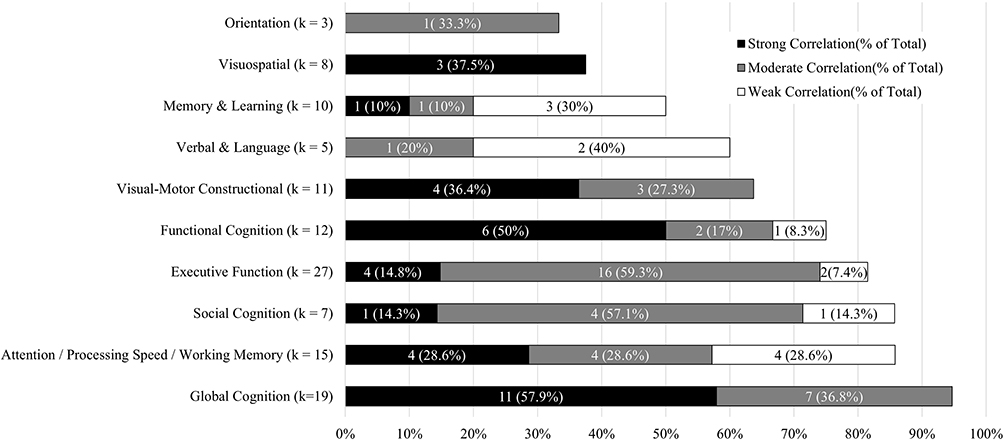 |
Figure 2 Horizontal bars represent the percentage of statistically significant correlations for each cognitive domain. Bar length indicates the proportion of significant findings, while grayscale shading within bars shows the distribution of effect sizes among significant correlations. Dark gray segments represent strong correlations (r ≥ 0.50), medium gray represents moderate correlations (0.30 ≤ r < 0.50), and light gray represents weak correlations (r < 0.30). Numbers adjacent to bars show the percentage of significant correlations and the ratio of significant to total correlations examined (in parentheses). Sample sizes (k = number of correlations) are displayed below each domain name. The dashed vertical line at 50% and the dotted line at 75% serve as reference thresholds. Domains are listed in order from highest to lowest proportion of significant findings. |
Global cognition showed the highest proportion of significant correlations at 94.7% (18/19), with predominantly strong effects (n = 11) and moderate effects (n = 7). The MMSE demonstrated strong correlations in six studies25,27,29,36,38,40 and moderate correlations in three.33,43,44 The MoCA showed one strong29 and two moderate correlations.38,44 Performance IQ, Full Scale IQ,31 and LOTCA Total Score showed predominantly strong to moderate associations across studies.22,23
Social cognition achieved 85.7% significant relationships (6/7), with predominantly moderate effects (n = 4), one strong effect, and one weak effect. Significant associations emerged across the SIT,33 PVRS,34 CIIT, and SBST.42
Attention, processing speed, and working memory demonstrated 85.7% (12/15) significant relationships, with balanced distribution across strong (n = 4), moderate (n = 4), and weak (n = 4) effects. The SDMT32 and Digit Symbol31 showed strong correlations, while working memory measures including digit span tasks31 and Digits Backward25 demonstrated varied but generally positive patterns. TMT-A showed population-dependent directional patterns.35,39
Executive function reached 81.5% significant relationships (22/27), with predominantly moderate effects (n = 16), some strong effects (n = 4), and weak effects (n = 2). The WCST showed robust associations, with Categories Completed demonstrating strong to moderate positive correlations26,29,30 and Perseverative Errors showing strong to moderate negative correlations.29,31,32 TMT-B, verbal fluency measures,35,39 and LOTCA Thinking Operations22,23 also showed significant associations, though patterns varied by population.
Functional cognition achieved 75% (9/12) significant relationships, with predominantly strong effects (n = 6), moderate effects (n = 2), and one weak effect. The AMPS Process Score showed consistently strong correlations across three studies,39,40,43 while the Motor Score was strong in two studies35,40 and weak in one.39 In EFPT, specifically showing moderate correlations in the sequencing and judgment subscale; conversely, the initiation and organization subscales failed to reach statistical significance.45
Visual-motor constructional and psychomotor abilities reached 63.7% (7/11) significant relationships, with strong effects (n = 4) outnumbering moderate effects (n = 3). Block Design showed strong correlations in psychiatric inpatients31 and moderate in older adults,39 though patterns were inconsistent in other groups.35 Object Assembly,31 VMI,46 and LOTCA Visuomotor Organization demonstrated significant associations,23 but these correlations were not significant among individuals with substance use disorders.22
Verbal and language abilities achieved 60% (3/5) significant relationships, with predominantly weak effects (n = 2) and one moderate effect. Verbal IQ showed moderate correlation in adults,31 but not in youth.46 Vocabulary measures showed weak32,39 or non-significant31 associations.
Memory and learning demonstrated 50% (5/10) significant relationships, with one strong, one moderate, and three weak effects. Verbal learning tasks showed a strong correlation in schizophrenia27,31 and a weak correlation in older adults.39 Logical Memory showed moderate correlation,39 while PMT factors were non-significant.46
Visuospatial and perceptual abilities showed 37.5% (3/8) significant relationships, with all significant correlations demonstrating strong effects (n = 3). Picture Arrangement31 and HVOT27 showed strong correlations, as did LOTCA Visual Perception in substance use disorders,22 though the latter was non-significant in other populations.22,42
Orientation had the lowest proportion at 33.3% (1/3), with moderate correlation in brain injury42 but non-significant findings in schizophrenia23 and substance use disorders.22
Two studies employed group comparison approaches. One study found that individuals with schizophrenia at ACL Level 5 (n=41) demonstrated significantly higher performance than those at Level 4 (n=35) on processing speed, verbal recall, and working memory, with discriminant analysis correctly classifying 78% of participants.28 Another study reported descriptively higher ACLS scores in the anticipatory awareness group (n=11, M=5.17±0.66) compared to the emergent awareness group (n=13, M=4.77±0.48) among individuals with acquired brain injury, though statistical significance was not reported.41
Only one included study examined the latest ACLS-6, in which only the stitching and copying tasks have established psychometric support, with both showing comparable correlations with the MMSE, MoCA, and WCST.29 Other ACLS-6 tasks remain unvalidated.
Discussion
This scoping review synthesized evidence from 24 studies examining relationships between ACLS scores and standardized cognitive assessments across 1,951 participants. The findings provide compelling evidence that the ACLS measures integrated cognition rather than discrete cognitive components. Strong correlations with global cognition (94.7%), social cognition (85.7%), executive function (81.5%), and attention/processing speed/working memory (85.7%) support the criterion-related validity of the ACLS as a measure of generalized cognitive capacity. Variable relationships with memory and learning (50.0%) and visuospatial abilities (37.5%) reflect construct boundaries rather than measurement limitations.
What the ACLS Measures?
The ACDM is grounded in the premise that cognition is fundamentally embodied and observable through action. This perspective draws from Soviet psychology, particularly Vygotsky’s mediation theory and Leontyev’s activity theory, which conceptualize cognition as sensorimotor information processing guiding purposeful action.47,48 Consistent with Vygotsky’s emphasis on potential over existing abilities, the ACLS aligns with the concept of “learning potential” as a mediator between basic neurocognition and functional outcomes.49 Wilson’s embodied cognition framework further supports this view, articulating that sensorimotor mechanisms can operate “off-line” to support abstract thought.50 The ACDM’s hierarchical levels, from sensory information (Level 1) through abstract symbolic information (Level 6), reflect this spectrum, representing qualitatively distinct patterns of attention to environmental cues.47
What the ACDM assesses corresponds to “functional cognition”:
the observable performance of everyday activities resulting from a dynamic interaction between motor abilities, activity demands and the task environment, which is guided by cognitive abilities.51
Recent research confirmed that functional cognition is a unique construct, distinct from fluid and crystallized cognition, with this distinctiveness reflecting cognitive skills rather than motor demands.52
These frameworks converge on the proposition that cognition is best understood through purposeful, tool-mediated action in context. The ACLS operationalizes this proposition by eliciting observable motor responses to a standardized craft task, capturing the integrated product of sensorimotor processing, attentional regulation, and learning potential (best ability to function), which is precisely what functional cognition frameworks define as clinically meaningful cognitive performance.
Criterion-Related Validity Within ACLS and Other Cognitive Measurement
Across 117 correlations examined, 86 (73.5%) demonstrated statistical significance, though the strength and consistency of these relationships varied systematically across cognitive domains. The strong associations with global cognition (predominantly strong effects, n = 11 out of 18 significant correlations), executive function (predominantly moderate effects, n = 16 out of 22), and attention/processing speed/working memory (balanced across strong, moderate, and weak effects) demonstrate criterion-related validity despite epistemological differences in what is being measured. These correlations indicate that individuals who categorize higher-quality sensorimotor information during ACLS performance also tend to perform well on traditional cognitive tests that measure internal processing efficiency and capacity.
However, these associations reflect convergence between different ontological lenses rather than measuring identical constructs. Traditional neuropsychological assessments conceptualize cognition as internal information-processing mechanisms,1 yielding quantitative scores that reflect cognitive capacity. The ACLS conceptualizes cognition as observable performance modes categorizing sensorimotor information quality, yielding ordinal classifications of how people engage with tasks.14 Both capture aspects of general cognitive functioning, explaining the strong correlations with global measures, but through different frameworks.
The high proportion of moderate effect sizes in executive function (16/22) lends support to this interpretation. Executive processes, as measured through psychological tests such as the WCST assess internal regulatory mechanisms, including set-shifting, inhibition, and working memory updating.53 ACLS performance appears to be associated with the integrated application of these processes as they manifest in sustained attention to sensorimotor information during complex stitching task. The consistent moderate associations suggest systematic relationships between internal executive capacities and observable attention to information quality, while the absence of extremely strong correlations indicates these are related but distinct phenomena.
The balanced distribution of effect sizes in attention/processing speed/working memory (4 strong, 4 moderate, 4 weak among 12 significant correlations) reflects different attentional demands. Traditional attention tests often measure speed of response or sustained vigilance to decontextualized stimuli, while ACLS requires sustained attention to the quality of sensorimotor information arising from object manipulation. Both involve attentional resources, but the nature of what is attended to differs.
The weaker and more variable patterns with memory and learning (50.0% significant, with 3 weak effects among 5 significant correlations) and visuospatial abilities (37.5% significant, though all significant correlations were strong) are often interpreted as discriminant validity. However, this interpretation may be misleading. These patterns more accurately reflect epistemological boundaries. Memory tests assess encoding, storage, and retrieval of information,54 while ACLS assesses moment-to-moment categorization of currently available sensorimotor information. Visuospatial tests assess mental manipulation of spatial representations.55
ACLS as a Functional Cognition
The strong associations with functional cognition measures (75.0% significant, predominantly strong effects) suggest that the ACLS assesses cognitive abilities as they naturally operate during purposeful activity. However, high correlations with ADM measures may reflect shared ACDM theoretical foundations rather than independent validation, as both assessments were developed by the same research team. AMPS correlations likely capture similar integrated cognitive-motor demands,10 whereas ACLS showed selective EFPT correlations only with sequencing and judgment/safety components, possibly because EFPT relies more heavily on executive processing and amount of assistance provided,45 which differs from ACLS theoretical assumptions.
A recent scoping review found evidence supporting the ACLS’s predictive and concurrent validity as a measure of functional performance.20 This supports the interpretation that the ACLS related to functional performance, yet also raises a broader question about ecological validity. Some researchers argued that this concept “is ill-formed, lacks specificity, and falls short of addressing the problem of generalizability”.56 Brunswik originally defined ecological validity as the correlation between proximal sensory cues and distal environmental variables,57 whereas contemporary researchers often conflate it with whether assessments appear “realistic.” Within the ACLS context, ecological validity concerns the correlation between performance on leather-lacing tasks (proximal cues) and actual capabilities in daily occupational activities (distal variables), essentially a question of task equivalence.
However, the current ACLS manual positioned the ACLS as a screening tool and a means for learning the ACDM, not as a comprehensive measure of real-world functioning.14 The Routine Task Inventory (RTI) was designed to capture actual occupational performance. Therefore, validation studies should prioritize the RTI to establish whether ACDM-based assessments validity to predict daily functioning across diverse activity contexts.
Existing validity evidence for the ACLS has predominantly relied on criterion-related and convergent approaches, such as correlations with neuropsychological tests and functional measures.25,39 Criterion-related evidence alone is insufficient and must be situated within a broader construct validity framework, including the structural aspect, appraising whether the scoring structure faithfully reflects the internal structure of the construct domain.58 The COSMIN taxonomy further operationalized this concept, defining structural validity as “the degree to which the scores of an instrument are an adequate reflection of the dimensionality of the construct to be measured”.59,60 To date, whether the ACLS’s hierarchical scoring structure empirically corresponds to the theoretical cognitive levels it purports to measure remains insufficiently examined.
The research gap also noted by recent systematic review.58 The theoretical model proposes a hierarchical structure where each level represents a qualitatively distinct mode of categorizing sensorimotor information, with higher levels subsuming lower-level capabilities.14 This structure has never been empirically verified through item response theory or confirmatory factor analysis. Austin’s Rasch analysis of the Canvas Placemats and Key Fob provided preliminary construct are valid within the 3.0–5.0 range of ADM tasks,60 and one study identified distinct cognitive profiles between Levels 4 and 5 with 78% classification accuracy,28 suggesting levels represent qualitative differences.
ACLS-6 Evidence Gap and Task Complementarity
Only one included study examined the latest ACLS-6 version; most employed earlier versions. The ACLS-6, published in 2016, introduced additional tasks at each level between Levels 1 and 5 to provide complementary ways of demonstrating performance within a level.14 Current evidence supports the psychometric properties of the stitching and copying tasks. Tasks differ in form but theoretically assess the same underlying quality of sensorimotor information categorization. This assumption of task equivalence within levels requires empirical verification. However, clinicians should exercise caution when interpreting ACLS-6 scores, and generating ACLS-6 validity studies should be an urgent research priority.
Methodological Considerations
Methods designed for ordinal data should be considered in future research, particularly when samples cluster at certain levels or when measures show ceiling or floor effects. Treating the ordinal scale as an interval scale can reduce correlations and obscure non-linear relationships.61 For example, one study found non-significant correlations with LOTCA-II visual perceptual/spatial subscales when participants reached ceiling scores,23 and orientation scores in substance use disorder populations averaged 7.73/8.22 As a wide-range cognitive screening tool, the ACLS’s criterion validity reflects the association between sample ACLS range and cognitive performance, not merely task-to-instrument correspondence.
Additionally, task-specific demands may also explain some null or weak associations. The ACLS leather-lacing tasks primarily engage visual attention, fine motor coordination, and sequential problem-solving. Cognitive domains such as verbal memory, orientation, or visuospatial perception may show weaker correlations not because they are unrelated to functional cognition, but because the task format does not sufficiently engage those specific processes.
Self-report measures consistently show weaker or non-significant correlations compared to objective assessments. One study found PSI executive subscales to be non-significant, except for attention, reflecting differences between subjective self-perception and objective performance.44 Self-report accuracy is compromised by limited insight and defensive mechanisms, particularly in populations with cognitive impairment.62
Age-related cognitive maturation also influences ACLS-cognition relationships. Full Scale IQ showed moderate positive correlations in adult samples31,32 but was non-significant in emotionally disturbed boys,46 reflecting ongoing crystallization of verbal abilities during childhood. Performance IQ demonstrated strong positive correlations across both populations,31,46 consistent with frontal lobe maturation during late childhood affecting attention control and strategy deployment. Simple span tasks may show stronger associations than complex cognitive tasks at this developmental stage due to limited elaborative rehearsal strategies.63 However, the results are based on a single study with a small sample (n = 24) and should be interpreted with caution.
Study Limitations
This scoping review has several limitations. We did not conduct quality assessment of included studies, following standard scoping review methodology that prioritizes breadth of evidence synthesis over critical appraisal.64 However, this means we cannot comment on the methodological rigor of included studies or weight findings by study quality. We also limited our search to English-language publications, potentially missing relevant evidence published in other languages. The wide range of sample sizes across included studies (range: 24–232) may affect the stability of reported correlation coefficients, and findings from smaller samples (n < 30) should be interpreted with caution. Descriptive ACLS score data were also unavailable in 25% of included studies, reflecting incomplete reporting in the primary literature rather than a gap in the review’s analytical scope.
The descriptive synthesis approach, while appropriate for scoping reviews, precludes quantitative meta-analysis that could provide more precise estimates of relationships across studies. Finally, the high heterogeneity in diagnostic groups and ACLS versions reflects the clinical breadth of the field but constrains the direct generalizability of a universal cognitive profile. Nevertheless, this diversity is essential for identifying critical research gaps, such as the relative lack of validation for the current ACLS-6 compared to earlier iterations.
Implications for Practice and Future Research
Current evidence demonstrates that ACLS scores relate systematically to diverse cognitive performances, providing criterion-related validity evidence despite epistemological differences in how cognition is conceptualized. The ACLS’s distinctive contribution lies in assessing categorization of the quality of sensorimotor information that arouses attention and guides observable action, with ACL scores representing qualitative, ordinal hierarchies of performance modes rather than quantitative measurements of internal capacity.
Clinicians can interpret ACLS scores as reflecting observable performance modes under standardized conditions that relate to general cognitive functioning, executive processes, and attentional capacities. However, the assessment should complement rather than replace a comprehensive evaluation. When interpreting ACLS findings in relation to daily activities, clinicians should recognize that actual performance depends on the complex interaction of capacity (can do), environmental factors (may do), and volition (will do), compounded by the dynamic nature of cognition across different times and contexts. Discrepancies between ACLS scores and daily functioning may reflect this multifaceted nature of real-world performance rather than assessment invalidity.20
The recommendation to attend to qualitative differences between levels is grounded in both the theoretical structure of the ACDM and available empirical evidence. Specifically, Su et al28 demonstrated distinct cognitive profiles between ACL Levels 4 and 5, with discriminant analysis correctly classifying 78% of participants, providing direct evidence that adjacent levels represent qualitatively different patterns of cognitive functioning. However, no study to date has empirically verified the full hierarchical continuity across all ACL levels, nor has the scoring structure been examined through item response theory or confirmatory factor analysis. In the absence of structural validity evidence supporting the interpretation of fine-grained numeric differences within levels, we believe it is more defensible to recommend that clinicians focus on between-level qualitative distinctions, where empirical support does exist. That means, given the ordinal scale structure and absence of structural validity evidence, clinicians should focus on qualitative differences between levels rather than interpreting small numeric changes within levels as clinically meaningful.28
Future research should address several priorities, with structural validity testing being the most pressing. Specifically, it remains to be examined whether ACL levels function as theorized qualitative categories, and whether appropriate analytical frameworks for hierarchical, ordinal performance modes can empirically support this assumption. Closely related is the question of ACLS-6 task equivalence, namely, whether the additional tasks introduced within each level demonstrate comparable patterns that support complementarity and interchangeability. Beyond psychometric concerns, future work should also investigate how performance under standardized conditions relates to functioning in naturalistic contexts, where environmental and volitional factors play a significant role. Methodological advances should employ ordinal analytical approaches and longitudinal designs to capture the dynamic nature of ACL across time and contexts.
Conclusions
The ACLS demonstrates criterion-related validity through systematic relationships with cognitive assessments across diverse populations, while measuring a different construct. Rather than quantifying internal cognitive capacities, the ACLS assesses observable categorization of sensorimotor information quality that guides action. These well-supported findings are particularly evident in the strong convergence with global cognition, social cognition, executive function, and attention supports the interpretation that ACL is related to general cognitive capacity. In contrast, variable patterns with memory, visuospatial abilities, and orientation reflect epistemological boundaries and should be interpreted with greater caution, given the more limited and inconsistent evidence available. Several areas remain preliminary and warrant further investigation before firm conclusions can be drawn. Structural validity research, examination of the properties of ACLS-6 tasks, and investigation of how standardized performance relates to dynamic real-world functioning currently lack sufficient evidence and represent essential directions for advancing the evidence base supporting this theoretically distinctive approach to cognitive assessment.
Data Sharing Statement
The datasets generated and analyzed during the present study are available from the corresponding author (Dr. Li-Wei Chou, [email protected]) on reasonable request.
Acknowledgments
This research was supported by China Medical University Hospital, Taiwan (DMR-114-114). The authors express their gratitude for this financial support, which made this study possible.
Author Contributions
Wei-Fen Ma and Li-Wei Chou contributed equally to this work. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Loren Pordage is a Director of ACDMweb, a for-profit company created by Claudia Allen in 2014 to continue the development of the Allen Cognitive Disability Model through further research and education. Dr. Pordage provided consultation on the Allen Cognitive Disability Model for this study without fee. The authors report no other conflicts of interest in this work.
References
1. Lezak MD, Howieson DB, Bigler ED, Tranel D. Neuropsychological Assessment.
2. Harvey PD. Clinical applications of neuropsychological assessment. Dialogues Clin Neurosci. 2012;14(1):91–16. doi:10.31887/DCNS.2012.14.1/pharvey
3. Joshi YB, Thomas ML, Braff DL, et al. Anticholinergic medication burden-associated cognitive impairment in schizophrenia. Am J Psychiatry. 2021;178(9):838–846. doi:10.1176/appi.ajp.2020.20081212
4. Cipriani G, Danti S, Picchi L, Nuti A, Di Fiorino M. Daily functioning and dementia. Dement Neuropsychol. 2020;14(2):93–102. doi:10.1590/1980-57642020dn14-020001
5. Verdejo-Garcia A, Lorenzetti V, Manning V, et al. A roadmap for integrating neuroscience into addiction treatment: a consensus of the neuroscience interest group of the international society of addiction medicine. Front Psychiatry. 2019;10:877. doi:10.3389/fpsyt.2019.00877
6. Stolwyk RJ, Mihaljcic T, Wong DK, Chapman JE, Rogers JM, Özkara Ç. Post-stroke cognitive impairment: epidemiology, risk factors, and management. J Neurol. 2024;271(2):723–741. doi:10.1007/s00415-023-12072-8
7. Chaytor N, Schmitter-Edgecombe M. The ecological validity of neuropsychological tests: a review of the literature on everyday cognitive skills. Neuropsychol Rev. 2003;13(4):181–197. doi:10.1023/B:NERV.0000009483.91468.fb
8. Manchester D, Priestley N, Jackson H. The assessment of executive functions: coming out of the office. Brain Inj. 2004;18(11):1067–1081. doi:10.1080/02699050410001672387
9. Burgess PW, Alderman N, Evans J, Emslie H, Wilson BA. The case for the development and use of “ecologically valid” measures of executive function in experimental and clinical neuropsychology. J Int Neuropsychol Soc. 2006;12(2):194–209. doi:10.1017/S1355617706060310
10. Giles GM, Edwards DF, Baum C, et al. Health policy perspectives: making functional cognition a professional priority. Am J Occup Ther. 2020;74(1):7401090010. doi:10.5014/ajot.2020.741002
11. Wolf TJ, Edwards DF, Giles GM. Functional Cognition and Occupational Therapy: A Practical Approach to Treating Individuals with Cognitive Loss. Bethesda (MD): AOTA Press; 2019.
12. Brown T, Chien CW. Top-down or bottom-up occupational therapy assessment: which way do we go? Br J Occup Ther. 2010;73(3):95. doi:10.4276/030802210X12682330090334
13. Allen CK. Occupational Therapy for Psychiatric Diseases: Measurement and Management of Cognitive Disabilities. Boston: Little, Brown; 1985.
14. Allen CK. Allen App: The Allen Cognitive Disability Model.
15. Earhart CA, McCraith DB, Riska-Williams L. Manual for Version 5 of the Allen Cognitive Level Screen.
16. Boone AE, Marks TS, Wolf TJ, Giles GM, Farrar-Edwards D. A national survey of occupational therapy practitioners’ evaluation of cognition in adults. Am J Occup Ther. 2025;79(5):7905205110. doi:10.5014/ajot.2025.051113
17. Allen CK, Earhart CA, Blue T. Occupational Therapy Treatment Goals for the Physically and Cognitively Disabled. Rockville (MD): American Occupational Therapy Association; 1992.
18. Allen CK. Allen Cognitive Level Test Manual and Kit. Colchester (CT): S&S Worldwide; 2000.
19. Allen CK, Austin SL, David SK, Earhart CA, McCraith DB, Riska-Williams L. Manual for the Allen Cognitive Level Screen-5 (ACLS-5) and Large Allen Cognitive Level Screen-5. Camarillo (CA): ACLS and LACLS Committee; 2007:LACLS–5.
20. Stewart K, Hancock N, Chapparo C, Stancliffe RJ. Functional performance and the Allen cognitive level screen for adults with mental illness: a scoping review. Am J Occup Ther. 2022;76(2):7602205150. doi:10.5014/ajot.2022.045757
21. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
22. Rojo-Mota G, Pedrero-Pérez EJ, Ruiz-Sánchez de León JM, Llanero-Luque M, Puerta-García C. Loewenstein occupational therapy cognitive assessment to evaluate people with addictions. Occup Ther Int. 2017;2017:2750328. doi:10.1155/2017/2750328
23. Su CY, Chen WL, Tsai PC, Tsai CY, Su WL. Psychometric properties of the loewenstein occupational therapy cognitive assessment-second edition in taiwanese persons with schizophrenia. Am J Occup Ther. 2007;61(1):108–118. doi:10.5014/ajot.61.1.108
24. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
25. Velligan DI, Bow-Thomas CC, Mahurin R, Miller A, Dassori A, Erdely F. Concurrent and predictive validity of the Allen cognitive levels assessment. Psychiatry Res. 1998;80(3):287–298. doi:10.1016/S0165-1781(98)00078-X
26. Secrest L, Wood AE, Tapp A. A comparison of the Allen cognitive level test and the wisconsin card sorting test in adults with schizophrenia. Am J Occup Ther. 2000;54(2):129–133. doi:10.5014/ajot.54.2.129
27. Leung DP, Man DW. The concurrent validity of the cognitive assessment scale for Chinese patients with schizophrenia. OTJR. 2007;17(2):69–73.
28. Su CY, Tsai PC, Su WL, Tang TC, Tsai AYJ. Cognitive profile difference between Allen cognitive levels 4 and 5 in schizophrenia. Am J Occup Ther. 2011;65(4):453–461. doi:10.5014/ajot.2011.000711
29. Chiu LY, Lee SC, Chiu EC. Psychometric properties of two tasks in the Allen cognitive level screen-sixth edition for community-dwelling people living with schizophrenia. Am J Occup Ther. 2022;76(5):7605205100. doi:10.5014/ajot.2022.049133
30. Ozturk LK, Bumin G, Ozturk E, Akyurek G. Investigation of the validity and reliability of the Turkish adaptation of Allen cognitive level Screen-5 (ACLS-5) with individuals with schizophrenia. Occup Ther Ment Health. 2023;39(4):419–435. doi:10.1080/0164212X.2022.2135671
31. Mayer MA. Analysis of information processing and cognitive disability theory. Am J Occup Ther. 1988;42(3):176–183. doi:10.5014/ajot.42.3.176
32. David SK, Riley WT. The relationship of the Allen cognitive level test to cognitive abilities and psychopathology. Am J Occup Ther. 1990;44(6):493–497. doi:10.5014/ajot.44.6.493
33. Penny NH, Mueser KT, North CT. The Allen cognitive level test and social competence in adult psychiatric patients. Am J Occup Ther. 1995;49(5):420–427. doi:10.5014/ajot.49.5.420
34. Ziv N, Roitman DM, Katz N. Problem solving, sense of coherence and instrumental ADL of elderly people with depression and normal control group. Occup Ther Int. 1999;6(4):243–256. doi:10.1002/oti.100
35. Schubmehl S, Barkin SH, Cort D. The role of executive functions and psychiatric symptom severity in the Allen cognitive levels. Psychiatry Res. 2018;259:169–175. doi:10.1016/j.psychres.2017.10.023
36. Kehrberg KL, Kuskowski MA, Mortimer JA, Shoberg TD. Validating the use of an enlarged, easier-to-see Allen cognitive level test in geriatrics. Phys Occup Ther Geriatr. 1992;10(3):1–14. doi:10.1080/J148v10n03_01
37. Roitman DM, Katz N. Predictive validity of the Large Allen Cognitive Levels Test (LACL) using the Allen Diagnostic Module (ADM) in an aged, non-disabled population. Phys Occup Ther Geriatr. 1996;14(4):43–59. doi:10.1080/J148v14n04_03
38. Park KY, Park SY, Jeong WM, Park SH, Hwang YJ, Youn JC. An analysis of clinical features in individuals with Alzheimer’s dementia living in the community using the Allen cognitive levels. Indian J Sci Technol. 2016;9(25):1–7.
39. Wesson J, Clemson L, Crawford JD, Kochan NA, Brodaty H, Reppermund S. Measurement of functional cognition and complex everyday activities in older adults with mild cognitive impairment and mild dementia: validity of the large Allen’s cognitive level screen. Am J Geriatr Psychiatry. 2017;25(5):471–482. doi:10.1016/j.jagp.2016.11.021
40. Marom B, Jarus T, Josman N. The relationship between the Assessment of Motor and Process Skills (AMPS) and the Large Allen Cognitive Level (LACL) Test in clients with stroke. Phys Occup Ther Geriatr. 2006;24(4):33–50. doi:10.1080/J148v24n04_03
41. Van Erp JB, Steultjens EM. Cognitive level and awareness in adults with acquired brain injury: preliminary findings. Ir J Occup Ther. 2020;67(3):267–272.
42. Park MO, Lee SH. Relationship between basic neurological cognition and social cognition among Allen cognitive disability levels of acquired brain injury. Healthcare. 2020;8(4):412. doi:10.3390/healthcare8040412
43. Huertas-Hoyas E, Rojo-Mota G, Carretero-Serrano Y, Rodriguez-Berrocal JL, Martín-Prades B, Máximo-Bocanegra N. Clinical validation of the Allen’s cognitive level screen in acquired brain injury. Brain Inj. 2022;36(6):775–781. doi:10.1080/02699052.2022.2065031
44. Rojo-Mota G, Pedrero-Pérez EJ, Huertas-Hoyas E, Merritt B, Mackenzie D. Allen cognitive level screen for the classification of subjects treated for addiction. Scand J Occup Ther. 2016;24(4):290–298. doi:10.3109/11038128.2016.1161071
45. Rojo-Mota G, Pedrero-Pérez EJ, Verdugo-Cuartero I, Huertas-Hoyas E, Carretero-Serrano Y, Rodriguez-Berrocal JL. Reliability and validity of the spanish version of the Executive Function Performance Test (EFPT) in assessing people in treatment for substance addiction. Am J Occup Ther. 2021;75(2):7502205080. doi:10.5014/ajot.2020.041897
46. Shapiro MB. Application of the Allen cognitive level test in assessing cognitive level functioning of emotionally disturbed boys. Am J Occup Ther. 1992;46(6):514–520. doi:10.5014/ajot.46.6.514
47. Allen CK. Activity: occupational therapy’s treatment method. Am J Occup Ther. 1987;41(9):563–575. doi:10.5014/ajot.41.9.563
48. Kozulin A. The concept of activity in soviet psychology: vygotsky, his disciples and critics. Am Psychol. 1986;41(3):264–274. doi:10.1037/0003-066X.41.3.264
49. Green MF, Kern RS, Braff DL, Mintz J. Neurocognitive deficits and functional outcome in schizophrenia: are we measuring the “right stuff”? Schizophr Bull. 2000;26(1):119–136. doi:10.1093/oxfordjournals.schbul.a033430
50. Wilson M. Six views of embodied cognition. Psychon Bull Rev. 2002;9(4):625–636. doi:10.3758/BF03196322
51. Wesson J, Clemson L, Brodaty H, Reppermund S. Estimating functional cognition in older adults using observational assessments of task performance in complex everyday activities: a systematic review and evaluation of measurement properties. Neurosci Biobehav Rev. 2016;68:335–360. doi:10.1016/j.neubiorev.2016.05.024
52. Baum CM, Lau SC, Heinemann AW, Connor LT. Functional cognition: distinct from fluid and crystallized cognition? Am J Occup Ther. 2023;77(3):7703205020. doi:10.5014/ajot.2023.050010
53. Nyhus E, Barceló F. The wisconsin card sorting test and the cognitive assessment of prefrontal executive functions: a critical update. Brain Cogn. 2009;71(3):437–451. doi:10.1016/j.bandc.2009.03.005
54. Tulving E. How many memory systems are there? Am Psychol. 1985;40(4):385–398. doi:10.1037/0003-066X.40.4.385
55. Goodale MA, Milner AD. Separate visual pathways for perception and action. Trends Neurosci. 1992;15(1):20–25. doi:10.1016/0166-2236(92)90344-8
56. Holleman GA, Hooge IT, Kemner C, Hessels RS. The ‘real-world approach’ and its problems: a critique of the term ecological validity. Front Psychol. 2020;11:721. doi:10.3389/fpsyg.2020.00721
57. Brunswik E. Systematic and representative design of psychological experiments: with results in physical and social perception. In: Neyman J, ed.
58. Lee Y, Randolph SB, Kim MY, et al. Performance-based assessments of functional cognition in adults, part 2—psychometric properties: a systematic review. Am J Occup Ther. 2025;79(4):7904205140. doi:10.5014/ajot.2025.050949
59. Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, Bouter LM, de Vet HCW. The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J Clin Epidemiol. 2010;63 (7). doi:10.1016/j.jclinepi.2010.02.006 737–745
60. Austin SA. Hierarchies of Abilities and Activity Demands in Allen Diagnostic Module 2nd Ed.: A Validity Study [dissertation]. Chicago: University of Illinois at Chicago; 2009.
61. Liddell TM, Kruschke JK. Analyzing ordinal data with metric models: what could possibly go wrong? J Exp Soc Psychol. 2018;79:328–348. doi:10.1016/j.jesp.2018.08.009
62. Carrigan N, Barkus E. A systematic review of the relationship between psychological disorders or substance use and self-reported cognitive failures. Cogn Neuropsychiatry. 2016;21(6):539–564. doi:10.1080/13546805.2016.1250620
63. Cowan N, Fristoe NM, Elliott EM, Brunner RP, Saults JS. Scope of attention, control of attention, and intelligence in children and adults. Mem Cognit. 2006;34(8):1754–1768. doi:10.3758/BF03195936
64. Munn Z, Peters MD, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18:143. doi:10.1186/s12874-018-0611-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.