Back to Journals » Research and Reports in Tropical Medicine » Volume 10
Mapping and monitoring for a lymphatic filariasis elimination program: a systematic review
Authors Srividya A, Subramanian S ![]() , Jambulingam P, Vijayakumar B
, Jambulingam P, Vijayakumar B ![]() , Dinesh Raja J
, Dinesh Raja J ![]()
Received 12 October 2018
Accepted for publication 2 April 2019
Published 27 May 2019 Volume 2019:10 Pages 43—90
DOI https://doi.org/10.2147/RRTM.S134186
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mario Rodríguez-Pérez
Adinarayanan Srividya, Swaminathan Subramanian, Purushothaman Jambulingam, Balakrishnan Vijayakumar, Jeyapal Dinesh Raja
Division of Epidemiology, Biostatistics and Operations Research, ICMR – Vector Control Research Centre, Puducherry, India
Abstract: Lymphatic filariasis (LF) is targeted for elimination by the year 2020. The Global Programme for Elimination of LF (GPELF) aims to achieve elimination by interrupting transmission through annual mass drug administration (MDA) of albendazole with ivermectin or diethylcarbamazine. The program has successfully eliminated the disease in 11 of the 72 endemic countries, putting in enormous efforts on systematic planning and implementation of the strategy. Mapping areas endemic for LF is a pre-requisite for implementing MDA, monitoring and evaluation are the components of programme implementation. This review was undertaken to assess how the mapping and impact monitoring activities have evolved to become more robust over the years and steered the LF elimination programme towards its goal. The findings showed that the WHO recommended mapping strategy aided 17 countries to delimit, plan and implement MDA in only those areas endemic for LF thereby saving resources. Availability of serological tools for detecting infection in humans (antigen/antibody assays) and molecular xenomonitoring (MX) in vectors greatly facilitated programme monitoring and evaluation in endemic countries. Results of this review are discussed on how these existing mapping and monitoring procedures can be used for re-mapping of unsurveyed and uncertain areas to ensure there is no resurgence during post-MDA surveillance. Further the appropriateness of the tests (Microfilaria (Mf)/antigenemia (Ag)/antibody(Ab) surveys in humans or MX of vectors for infection) used currently for post-MDA surveillance and their role in the development of a monitoring and evaluation strategy for the recently WHO recommended triple drug regimen in MDA for accelerated LF elimination are discussed.
Keywords: lymphatic filariasis, mass drug administration, mapping, monitoring, elimination, xenomonitoring, TAS (transmission-assessment survey)
Introduction
Lymphatic filariasis (LF) is one of the neglected tropical diseases (NTD) caused by three species of filarial worm: Wuchereria bancrofti, Brugia malayi, and Brugia timori. As of 1997, the disease was prevalent in 72 tropical and sub-tropical countries of the world.1 In 1997, the World Health Assembly2 declared elimination of LF as a public health problem. Subsequently, the World Health Organization (WHO) launched the Global Programme to Eliminate Lymphatic Filariasis (GPELF) in 2000 to achieve elimination by 2020.3 The elimination program has two components 1) interruption of transmission; and 2) morbidity management and disability prevention. For interruption of transmission, the strategy is annual single dose mass drug administration (MDA) of albendazole in combination with diethylcarbamazine (DEC) or ivermectin (IVM) to the LF endemic population. The program encompasses the following sequence of steps:4 1) map LF endemic areas (>1% of antigenemia (Ag), among 50–100 individuals (>15 years), from two communities of an endemic district);5 2) deliver MDA for a minimum of 5 years with an effective coverage of 65%; 3) conduct a transmission-assessment survey (TAS);4 4) conduct post-MDA surveillance; 5) develop a dossier that documents the achievement of elimination targets; and 6) independent validation of the claim that elimination criteria have been achieved.
Mapping the areas endemic for LF is the pre-requisite for the countries to plan and implement the elimination program. The next step is to implement MDA in endemic areas for a minimum of 5 years with an effective coverage of 65%. The program is to be monitored every 6 months post-MDA by assessing filarial infection (microfilaria [Mf]/Ag) in sentinel and spot check sites. If the prevalence of Mf in all the sentinel and in the randomly selected spot check sites are <1%, TAS is conducted to decide on stopping or continuing MDA. The TAS’s decision to stop or continue MDA is based on a pre-determined number of Ag positives below which transmission is expected to be interrupted and hence MDA can be stopped, if not MDA is continued for another two rounds. TAS is repeated twice at 2–3 year intervals (post-MDA surveillance) to assess if transmission interruption is sustained after cessation of MDA following TAS 1. After successfully passing all the three TASs, a dossier is submitted to the WHO, which validates the claim of elimination made by the country and once validated, WHO acknowledges LF elimination in that country. As of 2017, 51 of the 72 LF endemic countries have fully implemented MDA, and WHO acknowledged after post-MDA validation in 11 countries, that LF is no longer a public health problem.6
As GPELF is nearing its end game in many endemic countries it would be useful to do a comprehensive assessment of the mapping and monitoring activities used so far and to see how they been improvised to help in upscaling and assessing the impact of the program. Such a review would also be helpful to provide an insight on the methods that could be used in future for 1) remapping areas that are unsurveyed and not under MDA and areas bordering endemic districts; and 2) in identifying the appropriate sensitive tool that would detect ongoing transmission during post-MDA surveillance or validation phase. With this background, a systematic review of the literature on use of mapping and monitoring methods for LF elimination is undertaken.
Search criteria
All published articles in national and international peer-reviewed journals were searched. Searches were made in PUBMED MEDLINE database with key words like “lymphatic filariasis” in combination with “monitoring,” “mapping,” “infection,” “disease,” “MDA,” “antigeneamia,” “antibody,” “ICT,” “FTS,” “Wb123," “Mf” (or “microfilaria”), “vector infection,” and “xenomonitoring” using Boolean operators like “and” and “or.” Attempts were made to download the full articles and the back reference lists in these articles were searched for additional studies.
Eligibility criteria
For a study to be eligible for the review it should either have carried out mapping or monitored/measured impact evaluation with respect to MDA or both in terms of filarial infection (Mf/Ag/Ab) in humans or disease in humans or infection in vectors.
Results
The studies in this review were from the regions of Africa, Americas, Western Pacific, East Mediterranean and South-east Asia (as specified by WHO). The countries included from the African region were Benin, Botswana, Burkina Faso, Cameroon, Central African Republic, Côte d’Ivoire, Democratic Republic of the Congo, Ethiopia, Ghana, Malawi, Mozambique, Nigeria, Republic of the Congo, Rwanda, Senegal, Seychelles, Sierra Leone, Togo, Uganda, United Republic of Tanzania and Zambia; the studies in the American region were from Brazil and Haiti; the Western Pacific included studies from Papua New Guinea, Samoa, and American Samoa; Egypt and Sudan were the two countries from the East Mediterranean. The countries included from South East Asia were Bangladesh, India, Indonesia, Myanmar, Nepal, Sri Lanka, and Thailand. While in the African and East Mediterranean countries, where bancroftian filariasis is co-endemic with onchocerciasis (oncho), ivermectin plus albendazole were used for MDA, in the rest of the regions, where bancroftian filariasis is the only predominant form, DEC plus albendazole are being used.
Up until 2018, a total of 138 papers had been published on mapping, and or monitoring of LF. Of these, 541,7–59 were not eligible (as per the inclusion criteria) and therefore were excluded from subsequent review (Figure 1). A total of 84 studies were eligible for this review. Of these, 43 were on mapping alone, 36 on monitoring alone and five both on mapping and monitoring aspects of LF.
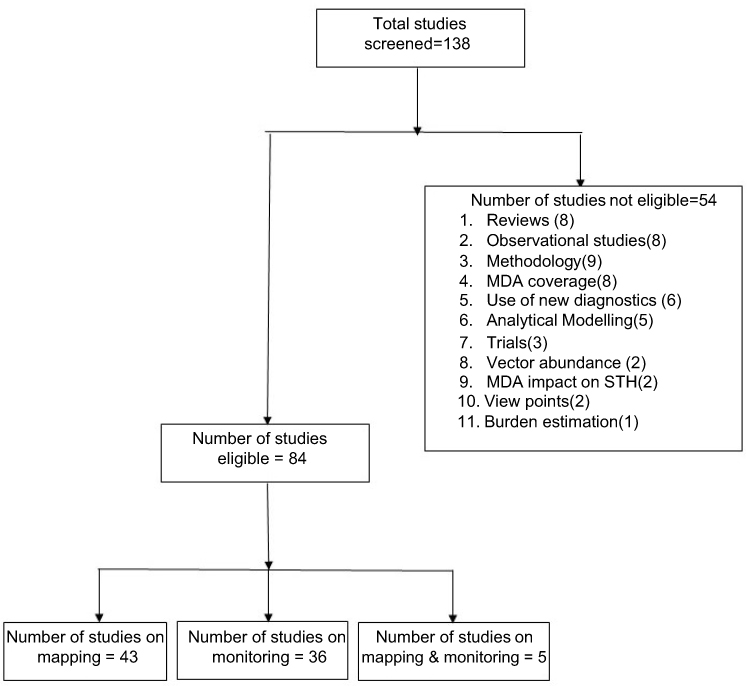 | Figure 1 Selection of studies for the review. |
The results of this review on mapping and monitoring of LF are presented in accordance with different phases of the program (pre-MDA, during MDA and post-MDA). While one would expect mapping to be undertaken mostly prior to implementation of MDA, it was observed that mapping was also done in the during- and post-MDA phases. As for monitoring, the studies included in this review assessed only the impact of MDA and not on coverage or compliance aspects of MDA.
Mapping
The majority (86%; 37/43) of the studies on mapping were conducted prior to implementation of MDA, mainly to delimit areas that required MDA. Of these 37 studies, 23 (62%) were from Africa, 5 (14%) from South East Asia, 6(16%) from the Americas and 3 (8%) from the Eastern Mediterranean region.
The WHO mapping guidelines5 for LF endemic areas (preferably an implementation unit (IU)/district) recommended a two stage sampling method of examining 50–100 individuals aged >15 years (conveniently sampled) for filarial antigen from two communities purposively selected from the IU/district. If the Ag prevalence is found to be ≥1%, the IU/district is considered for MDA.
Pre-MDA
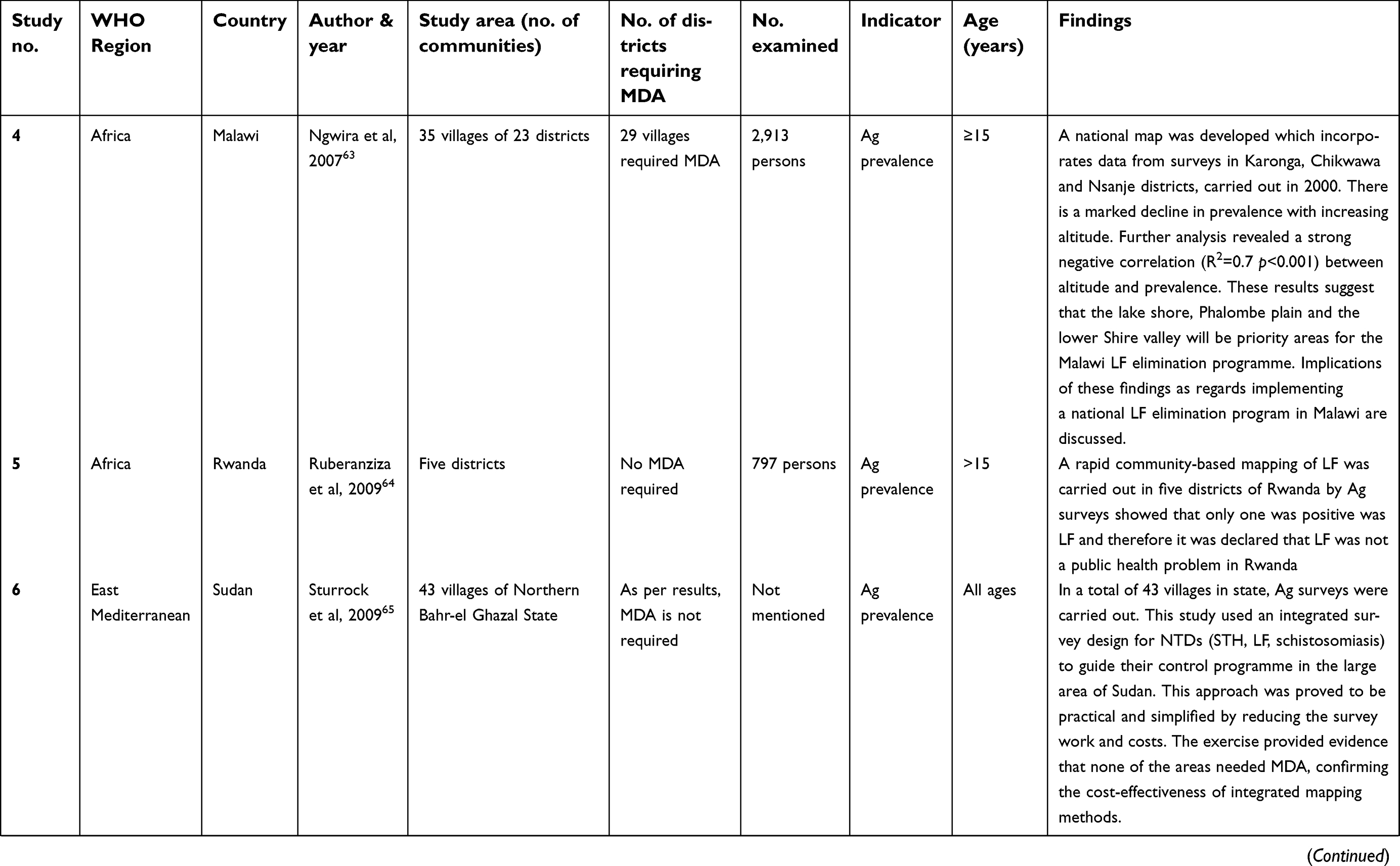
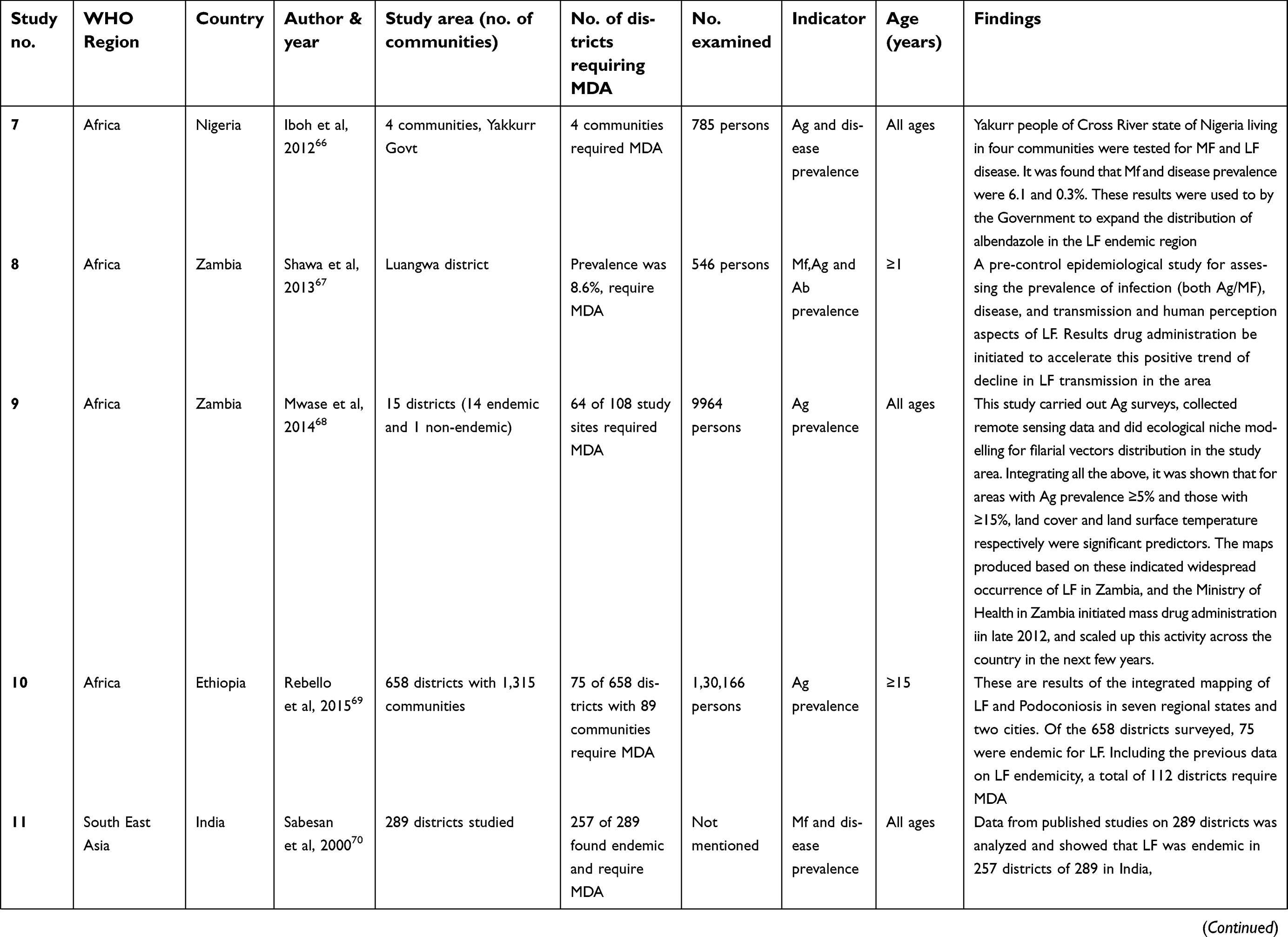
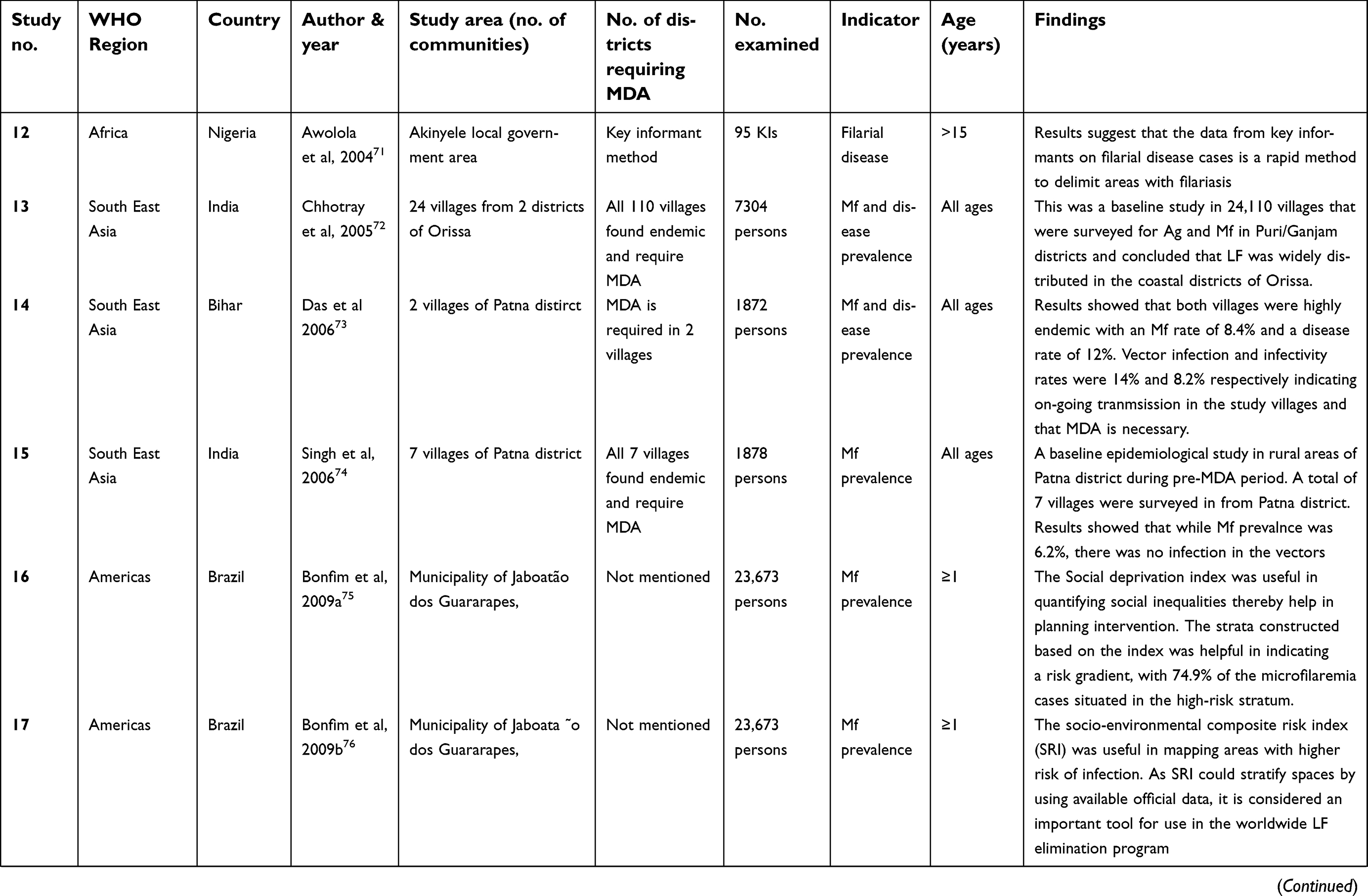
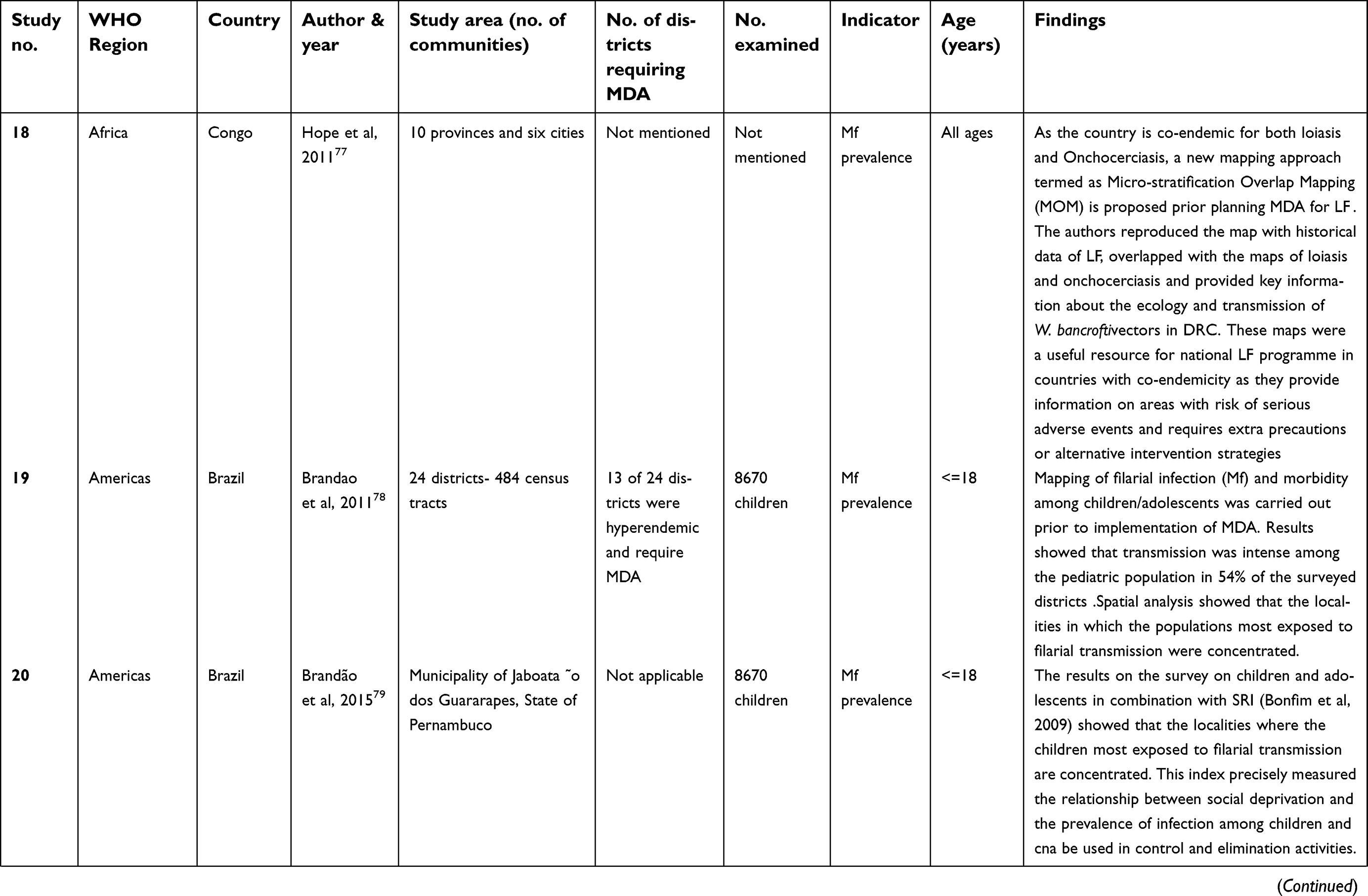
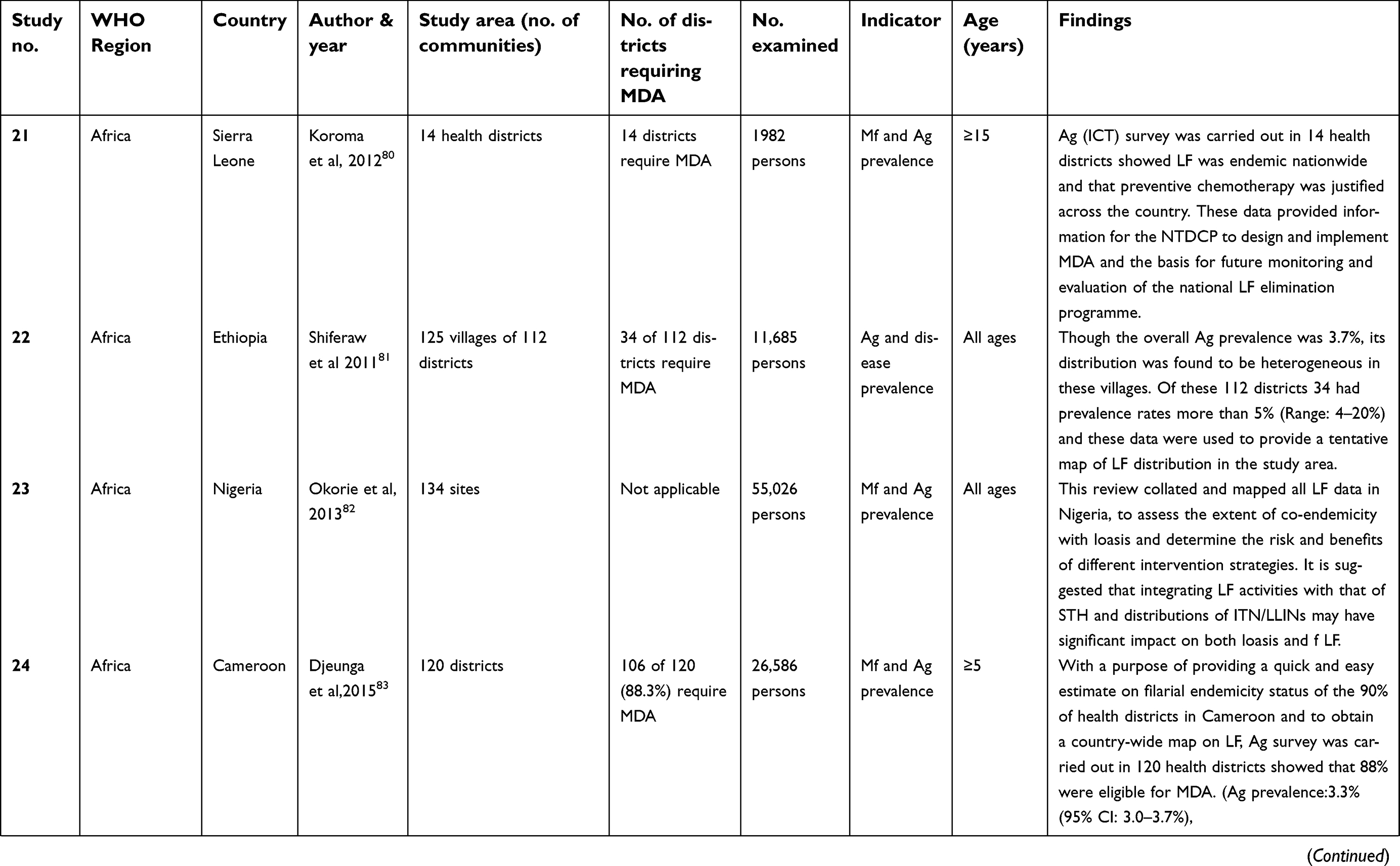
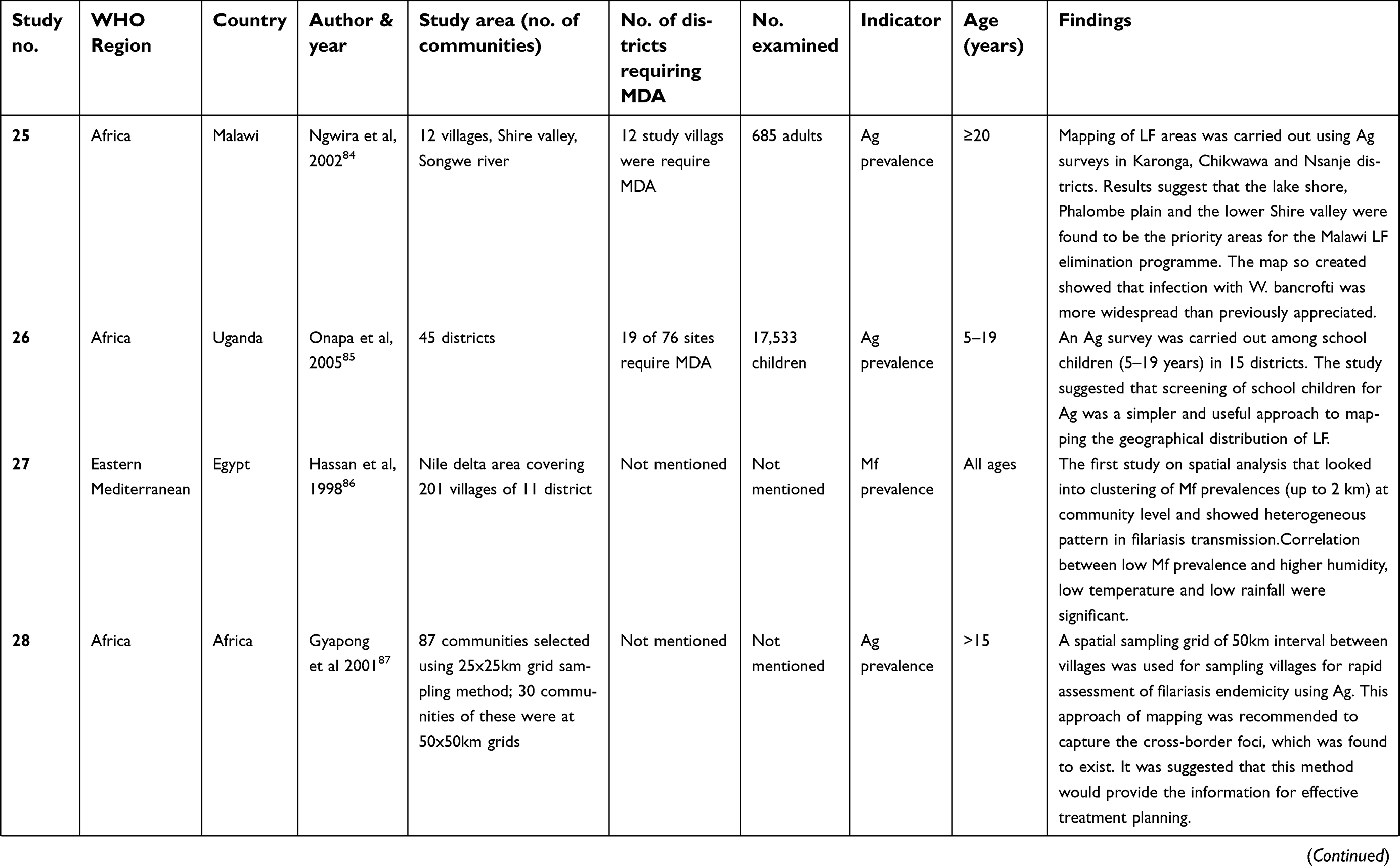
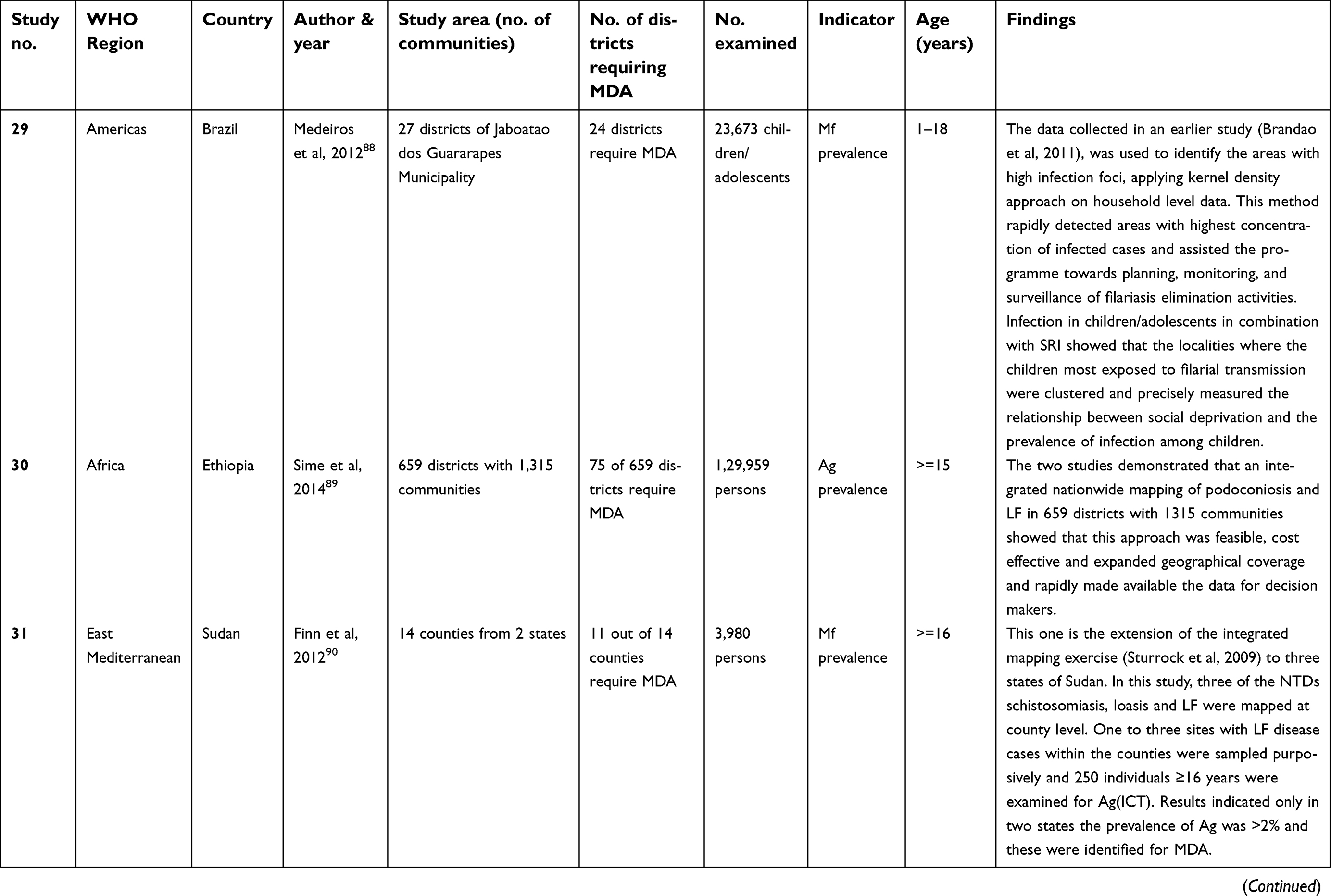
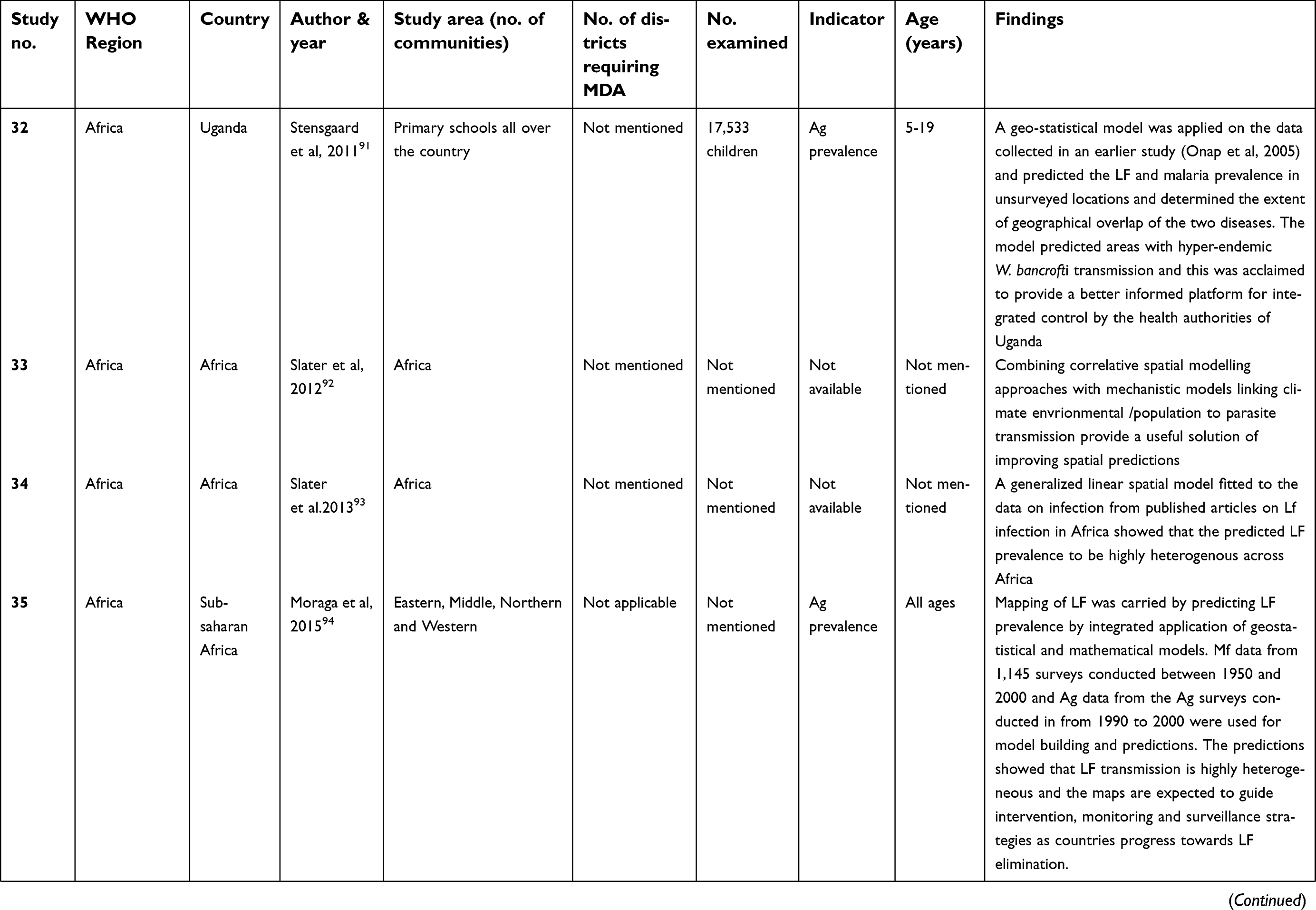
The details of the pre-MDA mapping studies that were carried out to assess if MDA is required are given in Table 1. The review showed that most African countries used the WHO recommended mapping method for delimiting areas requiring MDA.60–68 The surveys were conducted among adults and or children aged 5–15 years across the studies spanning over countries. In addition to these surveys, a few studies used Mf surveys (current and historic data), key informant techniques69-78 for assessing LF endemicity. In four studies, Mf, Ag and or disease surveys were used to map areas requiring MDA.79–82
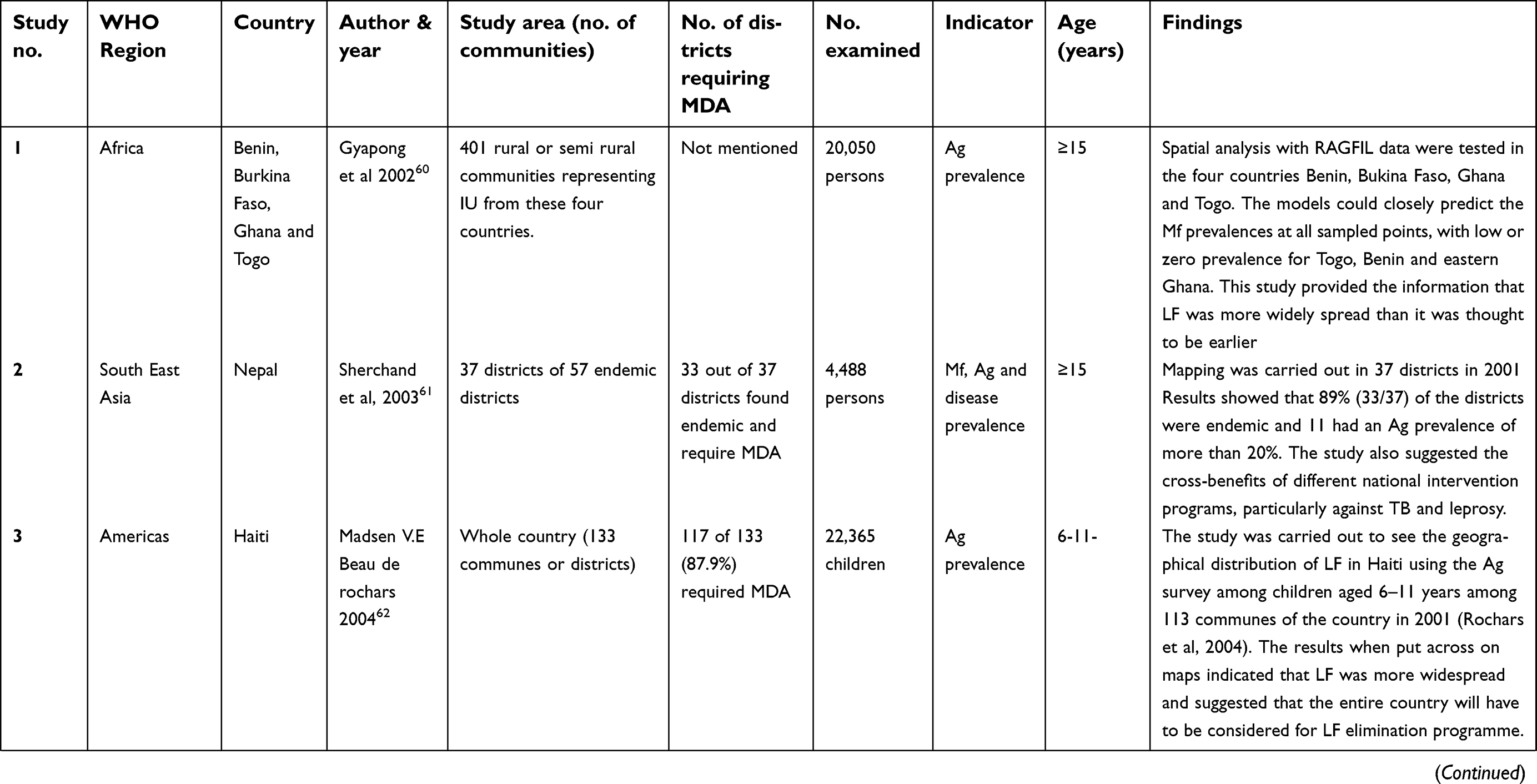 | Table 1 Details of the studies on mapping prior to MDA |
 | Table 1 (Continued). |
 | Table 1 (Continued). |
 | Table 1 (Continued). |
 | Table 1 (Continued). |
 | Table 1 (Continued). |
 | Table 1 (Continued). |
 | Table 1 (Continued). |
 | Table 1 (Continued). |
 | Table 1 (Continued). |
In Rwanda, mapping showed that there was only one Ag positive case in all five districts that were surveyed and this helped in declaring that LF was not a public health problem and therefore MDA was deferred thereby saving money and other humane efforts.63
In the countries of the African region, starting with rapid assessment procedures (Ag survey and key informant interviews on LF symptoms) for delimiting areas endemic for LF, the progress made on mapping of LF has been tremendous. A few studies mapped the distribution of LF61,62,66,83,84 using Mf and or Ag surveys and showed that the LF was more widely spread than it was previously thought in those countries. Few studies went further to carry out spatial analysis of the filarial prevalence data collected for mapping through a spatial sampling grid with 50 km distance between sampled locations and predicted LF prevalence at 25 km distance.60,77,85–87
Studies that carried out mapping of LF in Oncho co-endemic area helped the program to produce LF distribution maps80,82 with areas having Ag rates >1% and recommended inclusion of albendazole with the monotherapy of ivermectin to aid elimination of LF in these areas.65 Subsequently, as the countries in the African region were known to be co-endemic for NTDs like loasis, soil transmitted helminthic diseases, schistosomiasis and podoconiosis, attempts were made to map all these under one roof and this paved the way for an integrated mapping approach to understand the extent of distribution of diseases, and implementing control programs. Integrated mapping of LF with podoconiosis led to efficient use of resources and helped in rapidly delimiting large geographical areas. This approach was popular among the health staff in Ethiopia.68,88 A large NTD survey integrating mapping for LF, schistosomiasis and STH in three states of Sudan89 established that an estimated population of 1.2 and 1.4 million individuals were eligible for regular MDA with preventive chemotherapy (PCT) to treat STH and schistosomiasis respectively, and that 1.3 million individuals residing in Central- and Eastern Equatoria required MDA for LF. This integrated mapping approach cut costs and saved time with the same man-power efforts.64 Yet another approach called Micro stratification overlapped mapping (MOM) in Congo76 helped the program authorities to take extra precautions in handling serious adverse events that may take place due to co-endemicity of LF and loasis. In Nigeria, a similar approach using historical data helped in producing a series of maps to assist in maximizing existing interventions, cost effective usage of resources as the LF elimination programme scaled up.81
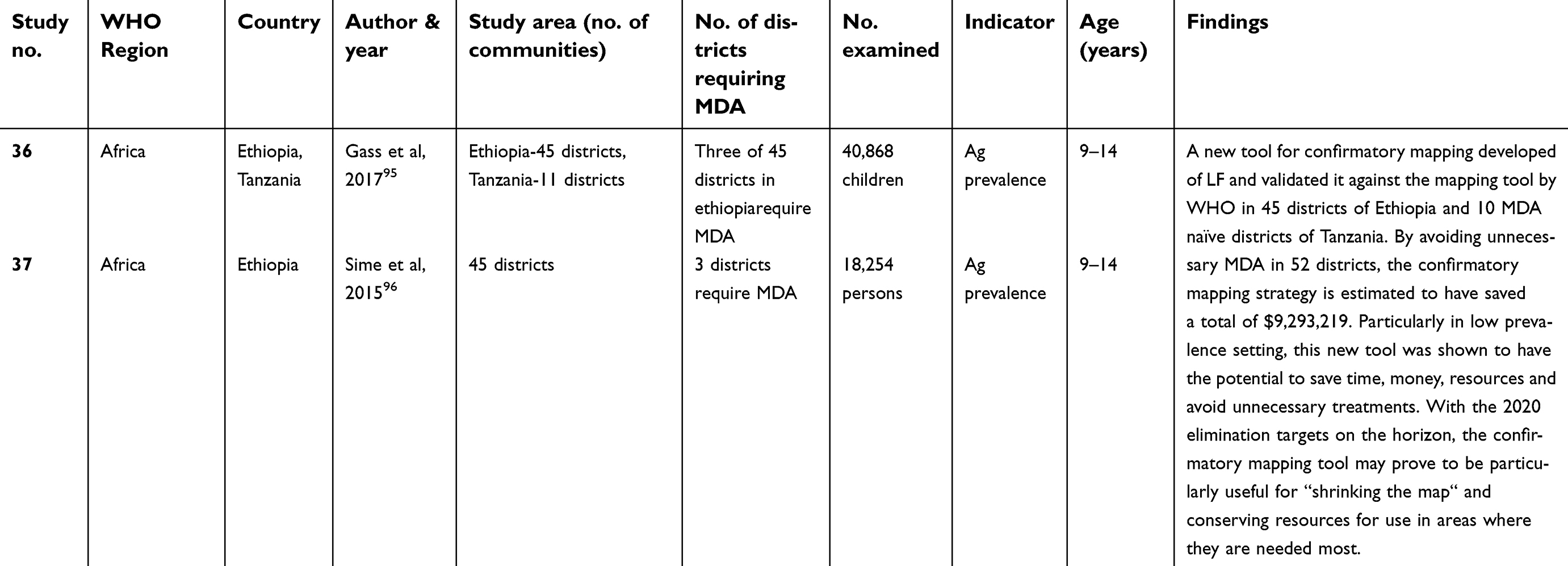
Countries such as Ghana, Uganda and India used the historical data (Mf, Ag), for predicting LF prevalence in the uncertain and un-surveyed areas using geo-statistical models67,69,90–93 and showed the heterogeneous distribution of LF for the respective countries, indicating the possibility on the risk of occurrence of LF even in the probably non-endemic areas. Three studies from India used Mf prevalence to identify districts for MDA.71–73 Mapping data along with social deprivation index (SDI) and socio-environmental composite risk index (SRI) were used in Haiti to specifically map LF risk in urban areas74,75,78 and to see clustering of infection. Two studies tested a confirmatory mapping tool against the WHO recommended mapping strategy mainly to assess whether those areas in Ethiopia and Tanzania94,95 with uncertain endemicity (one Ag positive among 200 adults; 45 in Ethiopia and 11 in Tanzania) needed to be included for MDA. This tool tested a sample of 320 children aged 9–14 years, from 30 schools selected based on probability proportional to estimated population size in a Woreda (a district) to find areas requiring MDA. The results showed that while only 3 out of 45 in Ethiopia and none of the 11 from Tanzania required MDA, thereby saving time and the resources by preventing MDA in areas where there was no evidence of transmission.
During MDA
Mapping during MDA (Table 2) was useful in re-assessing the geographic limits of LF and identifying new LF endemic areas that were either not surveyed, or classified as uncertain or non-endemic earlier.96–98 It was observed that in India, 113 of the 190 districts, which were not surveyed earlier and not included for MDA, were identified to be having varying risk of transmission. As the elimination goal is nearing, the National Vector-Borne Disease Control Programme (NVBDCP) is in the process of validating these findings before bringing these districts under MDA net. Mf and entomological surveys conducted in the sentinel villages of the Gampha district of Sri Lanka after 5 rounds of MDA showed ongoing transmission99 and recommended continuation of further rounds of MDA. In another study in Malawi that had already undergone 5 rounds of MDA for LF elimination is co-endemic for oncho and malaria, it was felt that the intervention programmes against these diseases could have impacted the transmission of LF. Therefore, to identify the high-risk areas of LF, a multiple intervention score map (MISM), that is based on weighted sum of individual intervention scores was used. This score was useful in identifying areas with high and low coverage of LF impacting interventions. It was shown that those areas with low coverage with high baseline LF prevalence were identified and considered to be with high risk of transmission or re-emergence.100 Another study101 attempted morbidity mapping to estimate lymphedema burden in Malawi after 5 rounds of MDA, observed that as there was no standardized method for collection of morbidity data, the morbidity burden due to LF could be grossly underestimated.
 | Table 2 Details of the studies on mapping LF during and post-MDA |
Monitoring
A total of 36 studies have monitored filarial infection during the period of MDA implementation and also during post-MDA surveillance. Of them, 19 were during MDA implementation, 15 during post-MDA, one study reported monitoring of both pre-MDA and during MDA, and another study about monitoring in all the three phases, (pre, during and post MDA) of elimination programme.
During MDA
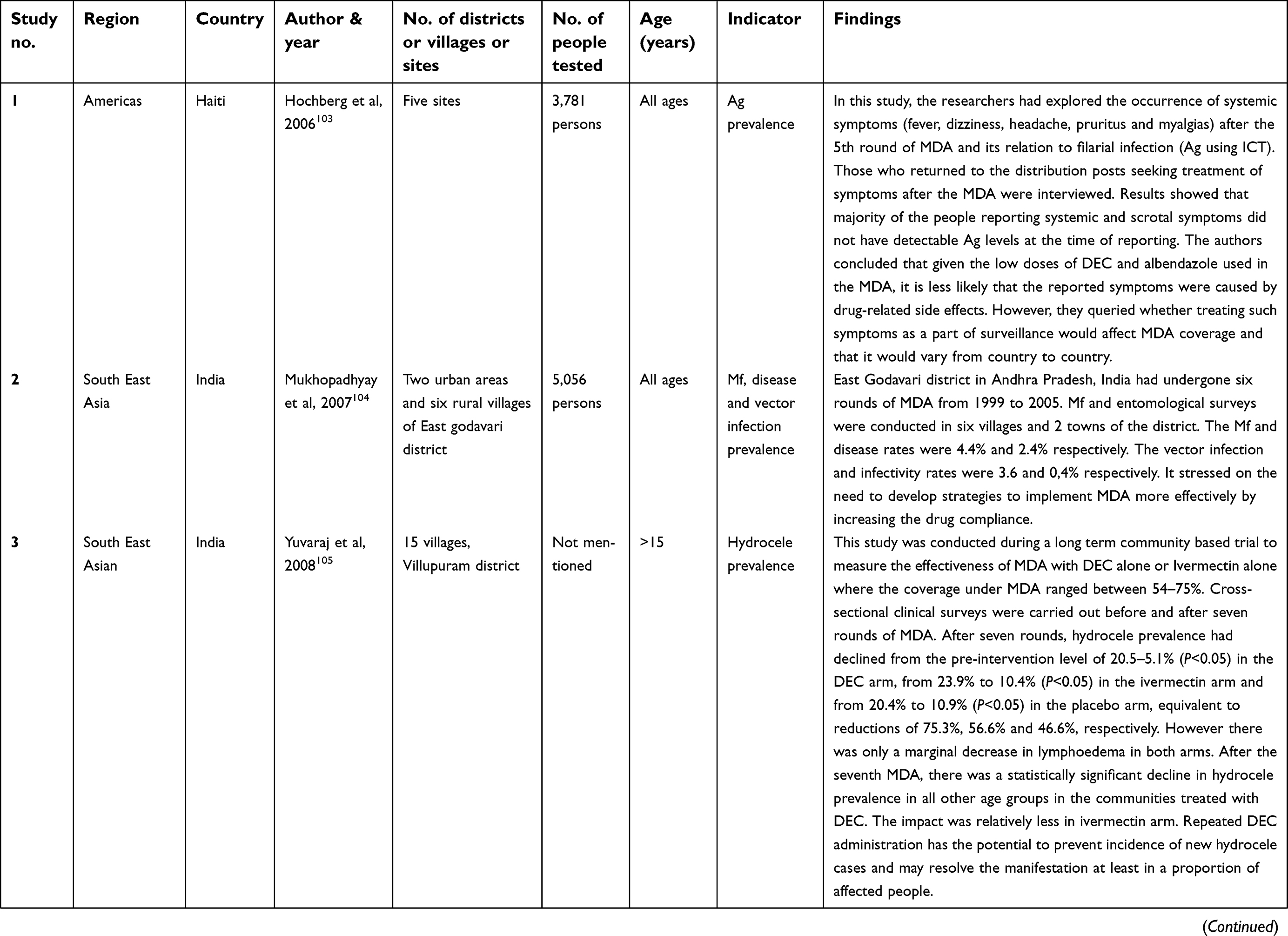
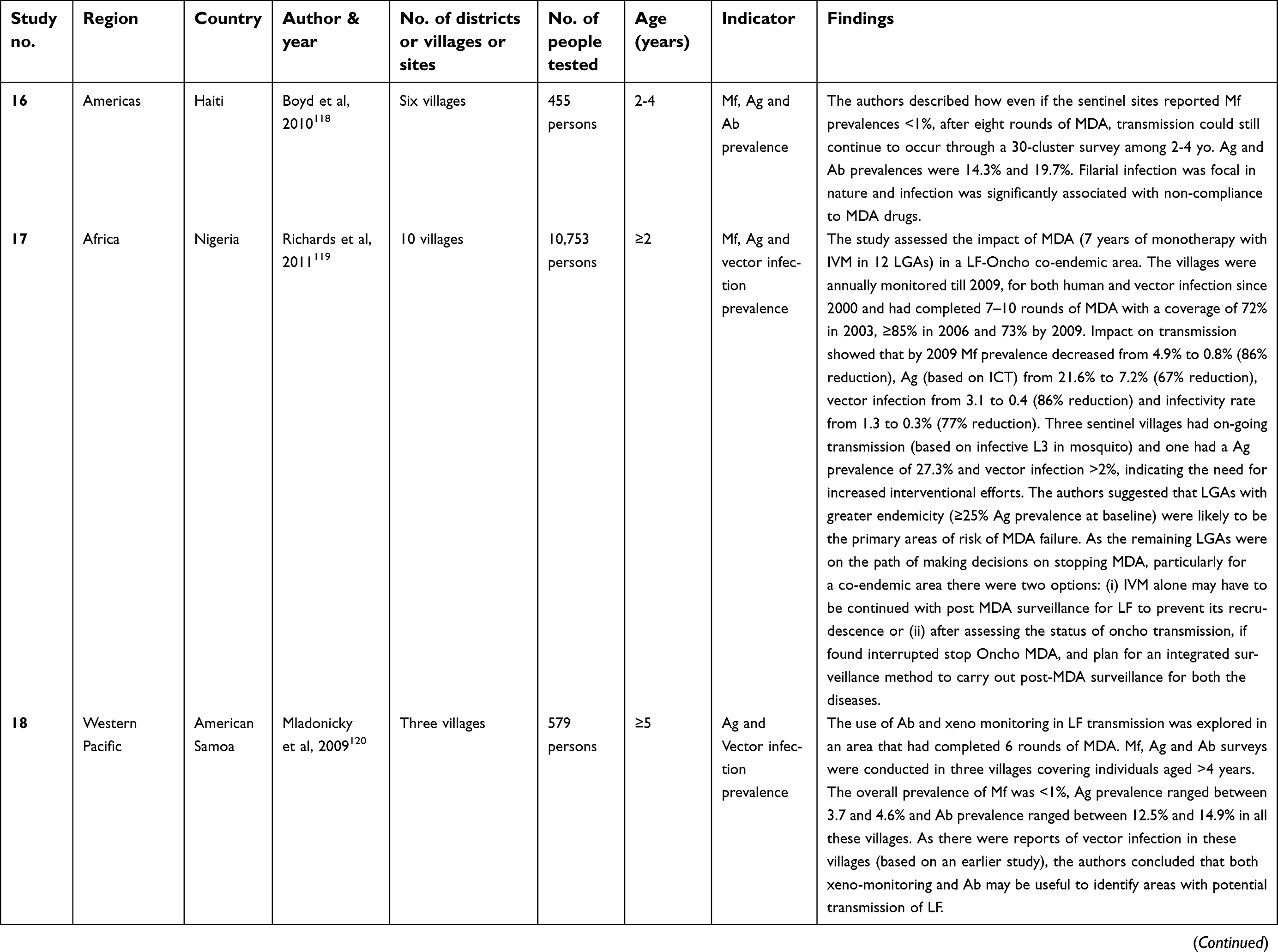
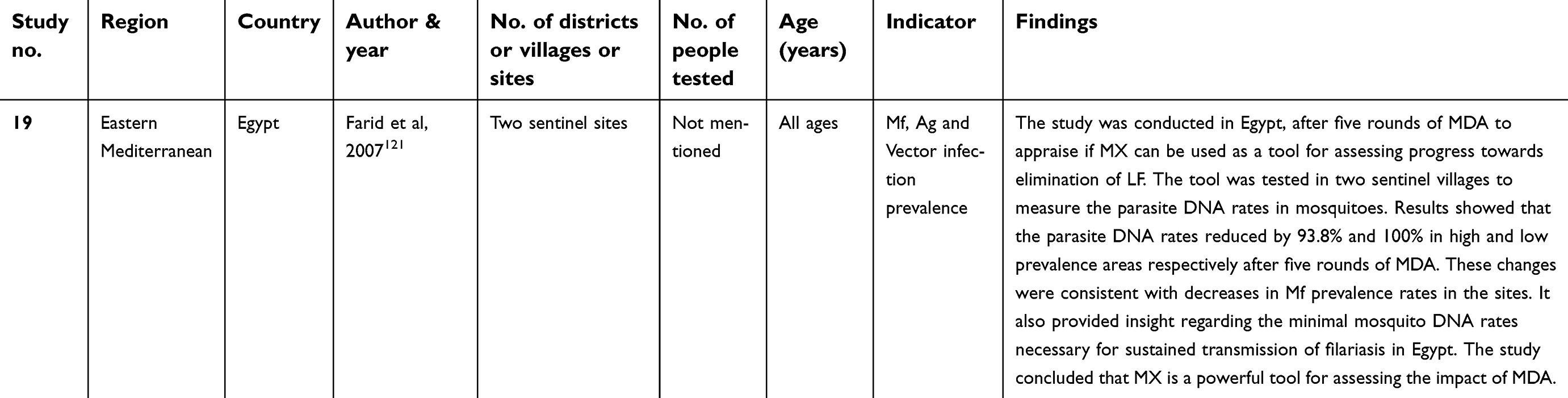
Of the 19 studies conducted during MDA phase, 6, 7, 3, 2 and 1 were from African, Southeast Asian, Western Pacific, Americas and eastern Mediterranean regions respectively (Table 3). In eleven studies, the impact of MDA had been measured in terms of reduction in Mf Ag or Ab or filarial disease prevalence102-112 in humans. Seven studies, two from India,113,114 two from Tanzania,115,116 one each from Haiti,117 Nigeria,118 Samoa,119 and Egypt120 monitored infection (xenomonitoring/dissection) in vectors in addition to infection in humans (MF/Ag/Ab).
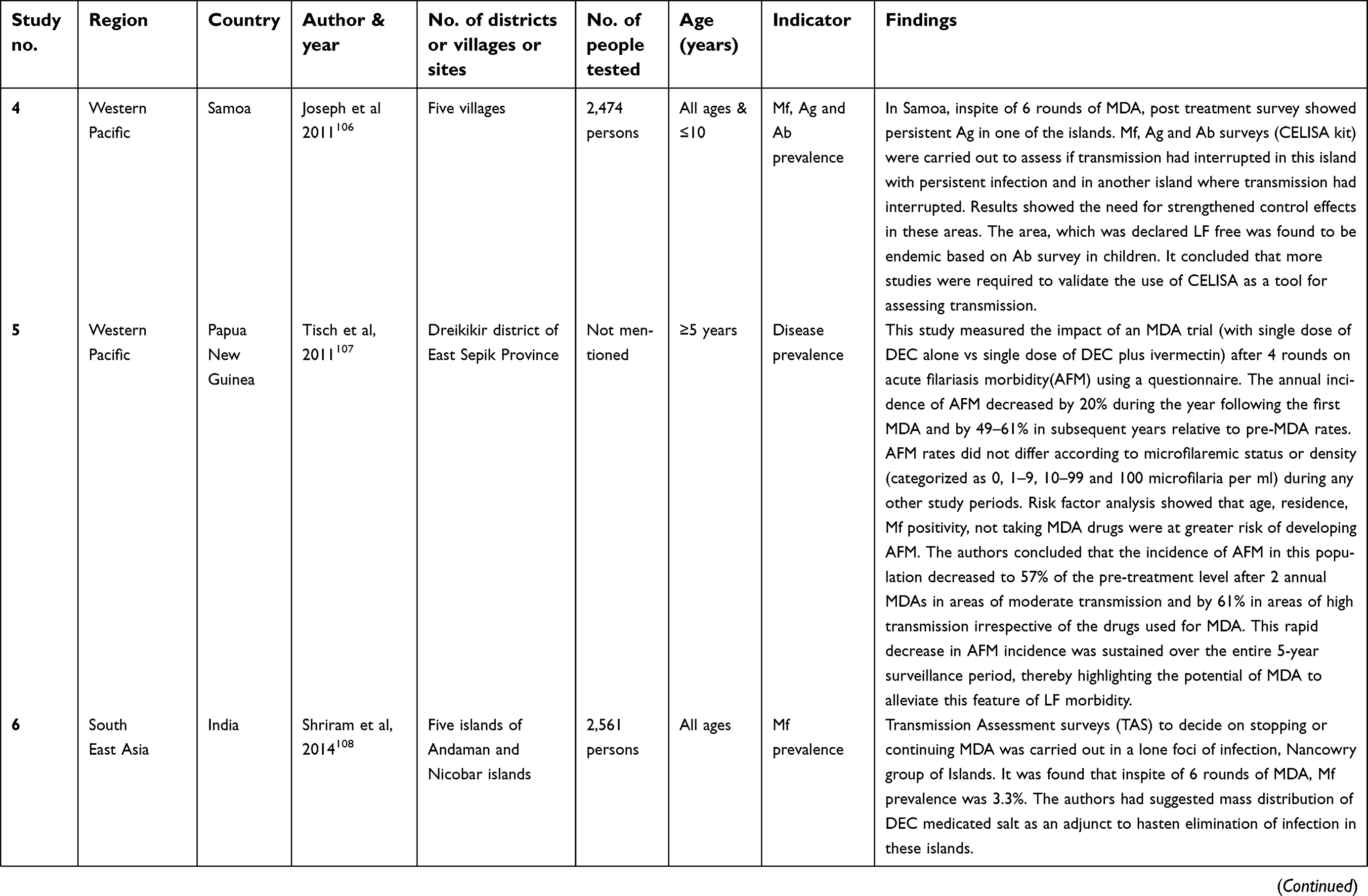
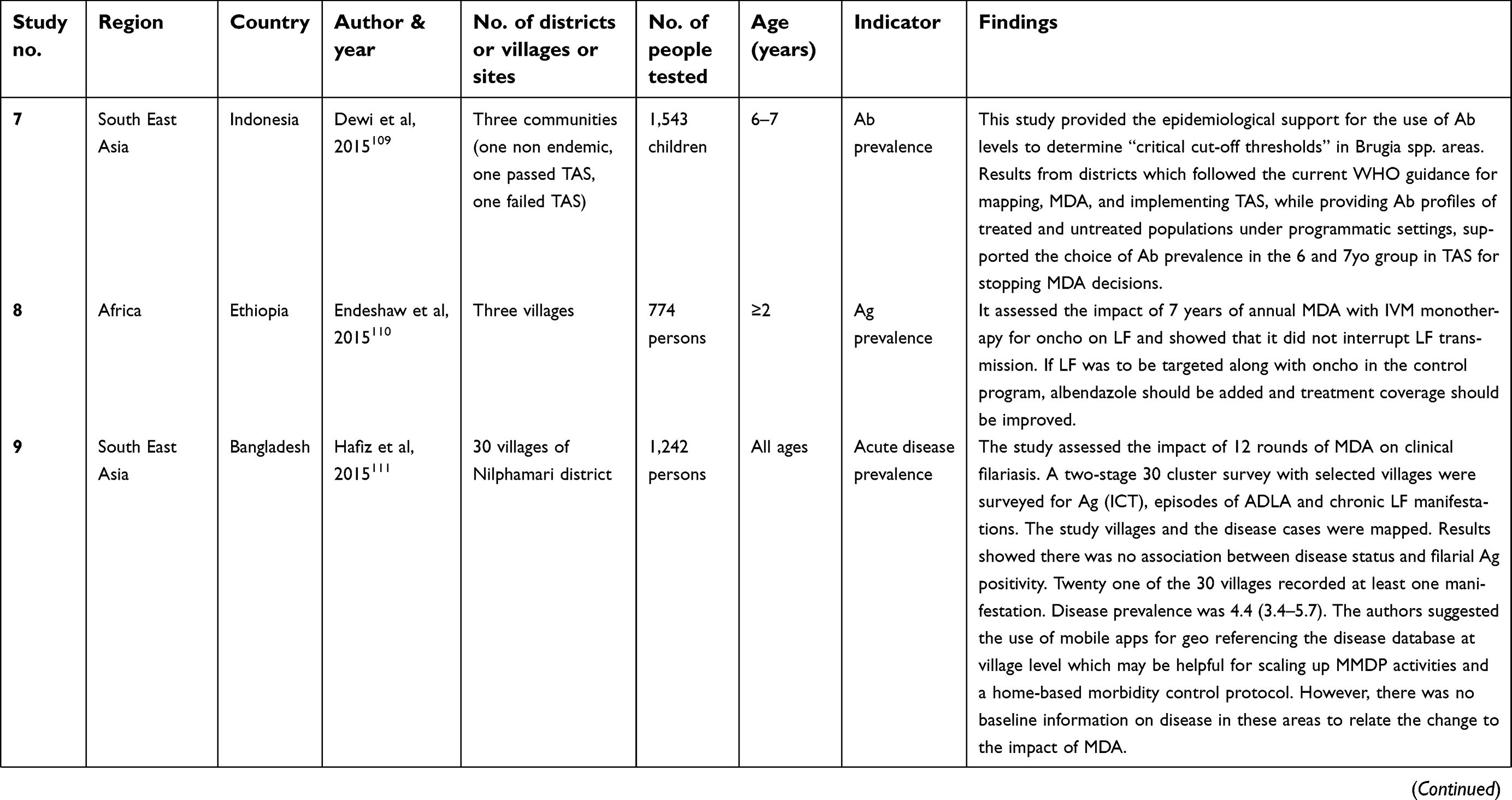
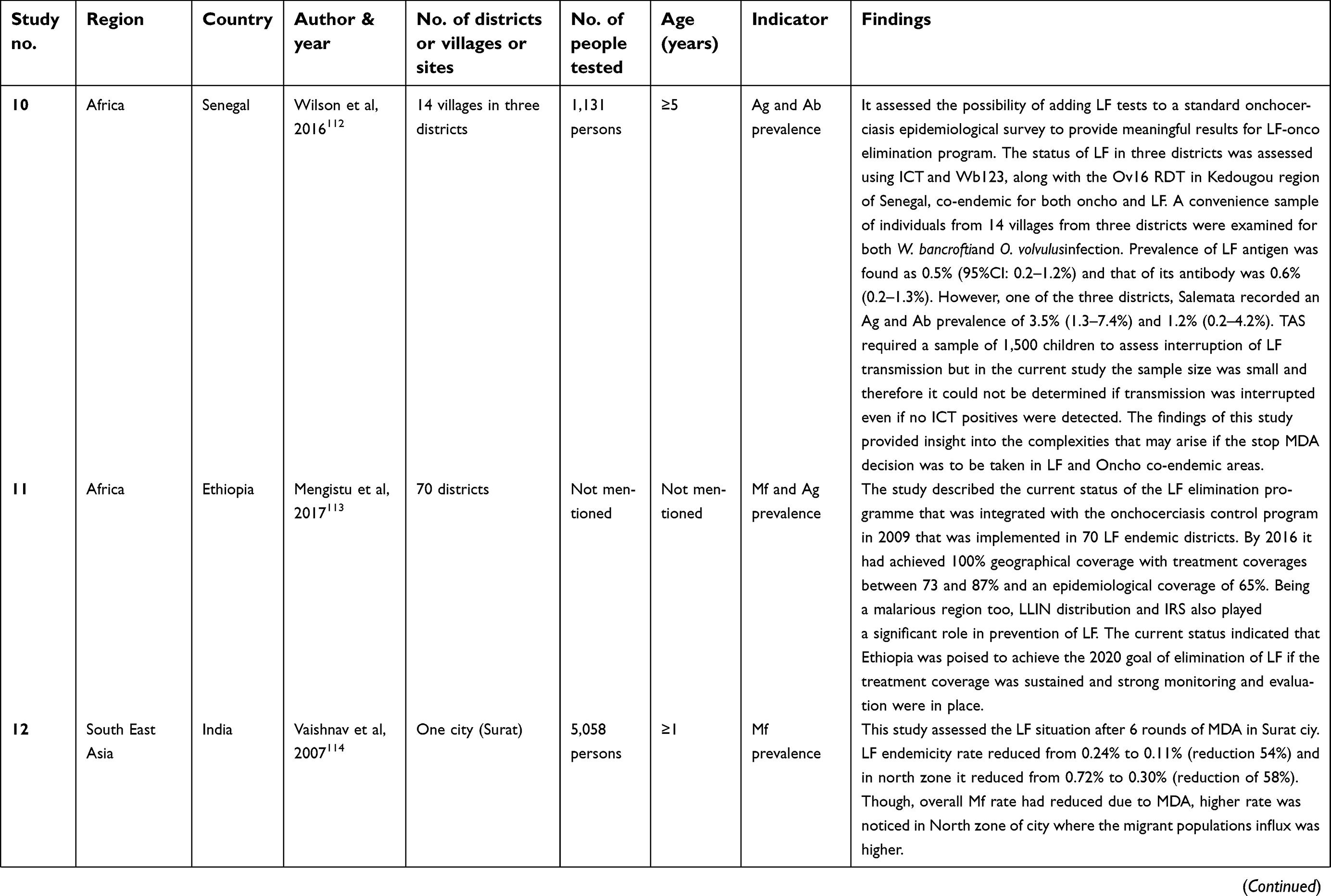
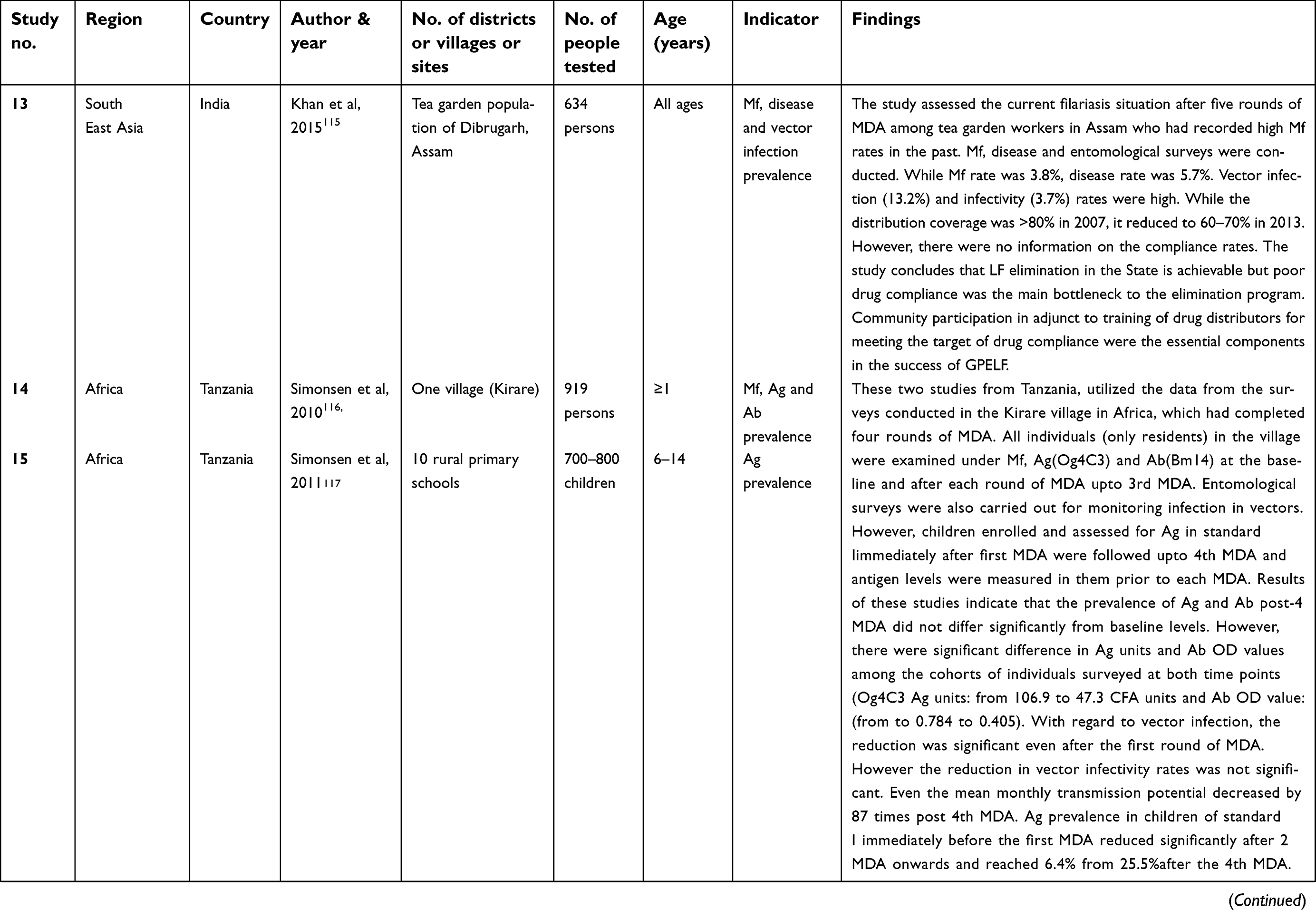
 | Table 3 Details of the studies in which monitoring was done during MDA |
 | Table 3 (Continued). |
 | Table 3 (Continued). |
 | Table 3 (Continued). |
 | Table 3 (Continued). |
 | Table 3 (Continued). |
 | Table 3 (Continued). |
Studies in the African,118 East Mediterranean,120 and South East Asian107,114,117 regions which used human and vector infection indicators have concluded that 4–6 rounds of MDA may not be sufficient to interrupt transmission. While the study from Nigeria118 concluded that additional interventions (like more frequent MDA treatments and insecticidal bed nets) were necessary particularly for those sentinel villages that had baseline Ag prevalence >25%, systematic non-compliance to MDA was the reason for on-going transmission in Haiti which led to two additional MDA rounds.117 The studies that had used vector infection prevalence in addition to Mf/Ag/Ab117,119,120 have suggested that MX is a powerful tool in assessing the impact of MDA and that both Ab in humans and the MX tool could be used to measure on-going transmission.
Few studies that had measured Ab prevalence alone or in addition to Mf/Ag in children105,108,115,116 indicated that measuring Ab in children is a better indicator to assess interruption of transmission as it also measures exposure to infective bites in addition to infection with adult worms. It was suggested that measuring Ab instead of Ag alone may be helpful in identifying areas with residual infections.105
Studies that used disease prevalence to measure the impact of MDA104,106,110 suggested that 10 rounds of MDA had helped in reducing the overall disease prevalence to low levels. A study from Papua New Guinea showed that after four rounds of MDA, the acute filarial morbidity reduced significantly from the pre-treatment levels and that the reduction was higher in those areas that had higher transmission indices compared to those with lower figures.106 In a community trial from India, it was found that seven rounds of MDA with DEC alone prevented incidence of new hydrocele cases and resolved the manifestation in a proportion of already affected individuals in addition to reducing the levels of Mf and transmission indices in the communities.104 Assessment of occurrence of systemic symptoms102 following a 5th round of MDA and providing free symptomatic treatment was expected to motivate people to report symptoms and seek care. However, the authors concluded that from a programmatic perspective, treatment of these systemic symptoms might not be necessary, because most of the individuals surveyed did not report these symptoms as a barrier to participating in future MDA.
Few studies have reported only the current situation of LF (Mf/Ag/Ab/disease) after six to seven rounds of MDA103,104,110,112–114 in the endemic areas and found that Mf prevalence were still above the 1% threshold. To interrupt the on-going transmission in spite of several rounds of MDA, these studies recommend the need for additional efforts by program authorities to improve the coverage of the program and better monitoring and evaluation procedures.
One study assessed the possibility of integrating antibody testing for LF and oncho, which has highlighted the complexities that may arise in making a decision on stopping MDA particularly in LF-oncho co-endemic areas of Africa.111 Another study109 observed that 7 years of monotherapy with ivermectin has not reduced Mf prevalence in a oncho-LF co-endemic area and therefore to achieve significant reduction, the authors suggested that albendazole be added to the program particularly in LF endemic areas. In another oncho-LF co-endemic area118 the study showed that while Mf and Ag rates were reduced by 83% and 67%, the mosquito infection and infectivity rates were reduced by 86% and 76% compared to the baseline. As this was a LF-oncho co-endemic area, regarding the decision of stopping MDA, it was suggested that if LF transmission was found to be interrupted, albendazole could be stopped and the MDA could continue only with ivermectin with simultaneous post-MDA surveillance for LF for resurgence. If it is found that oncho transmission also has been interrupted, an integrated surveillance can be planned for post-MDA surveillance.
Post-MDA
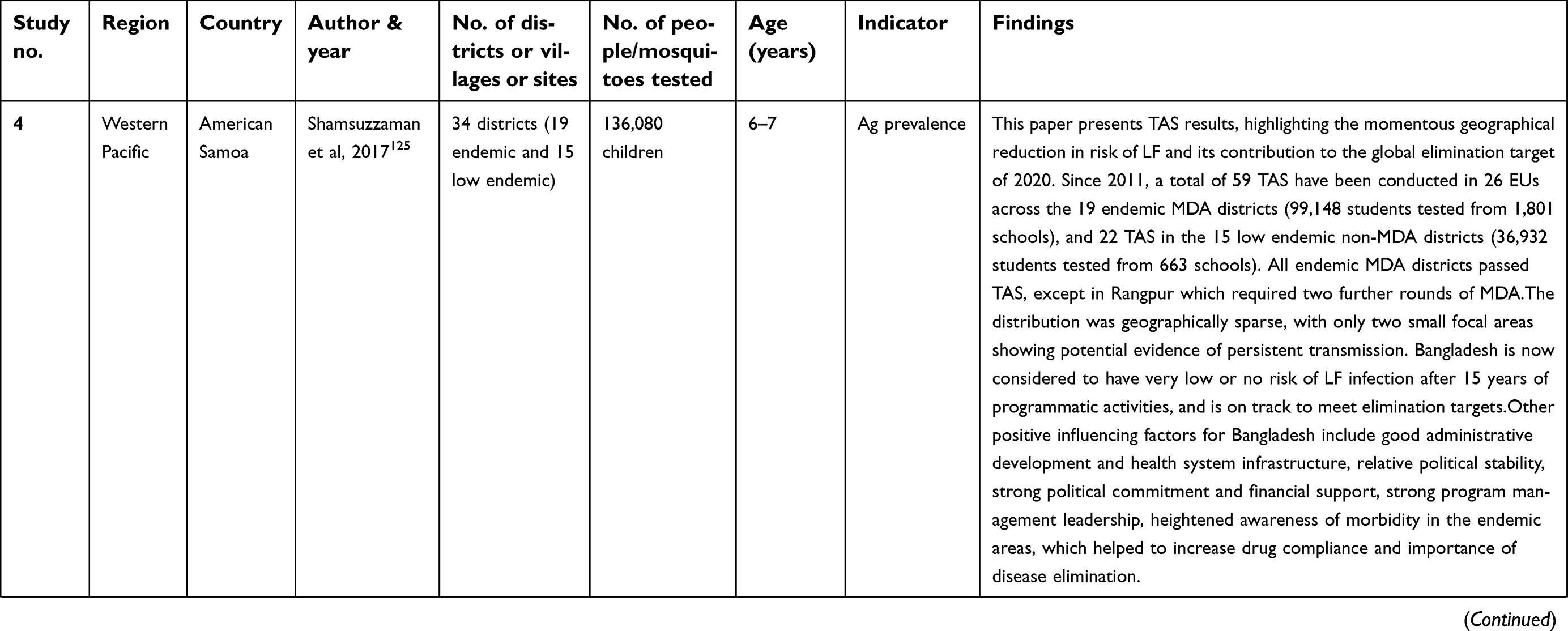
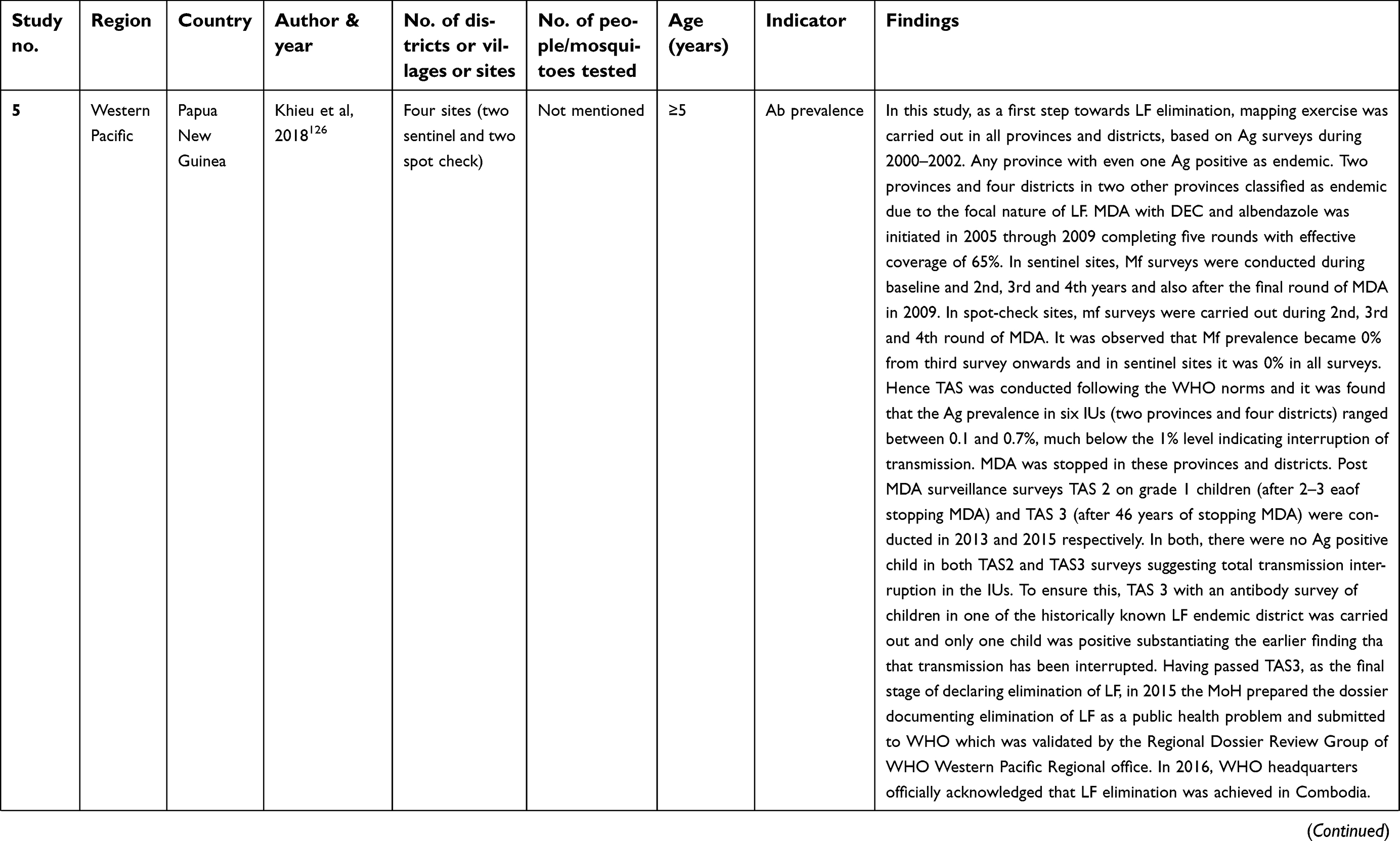
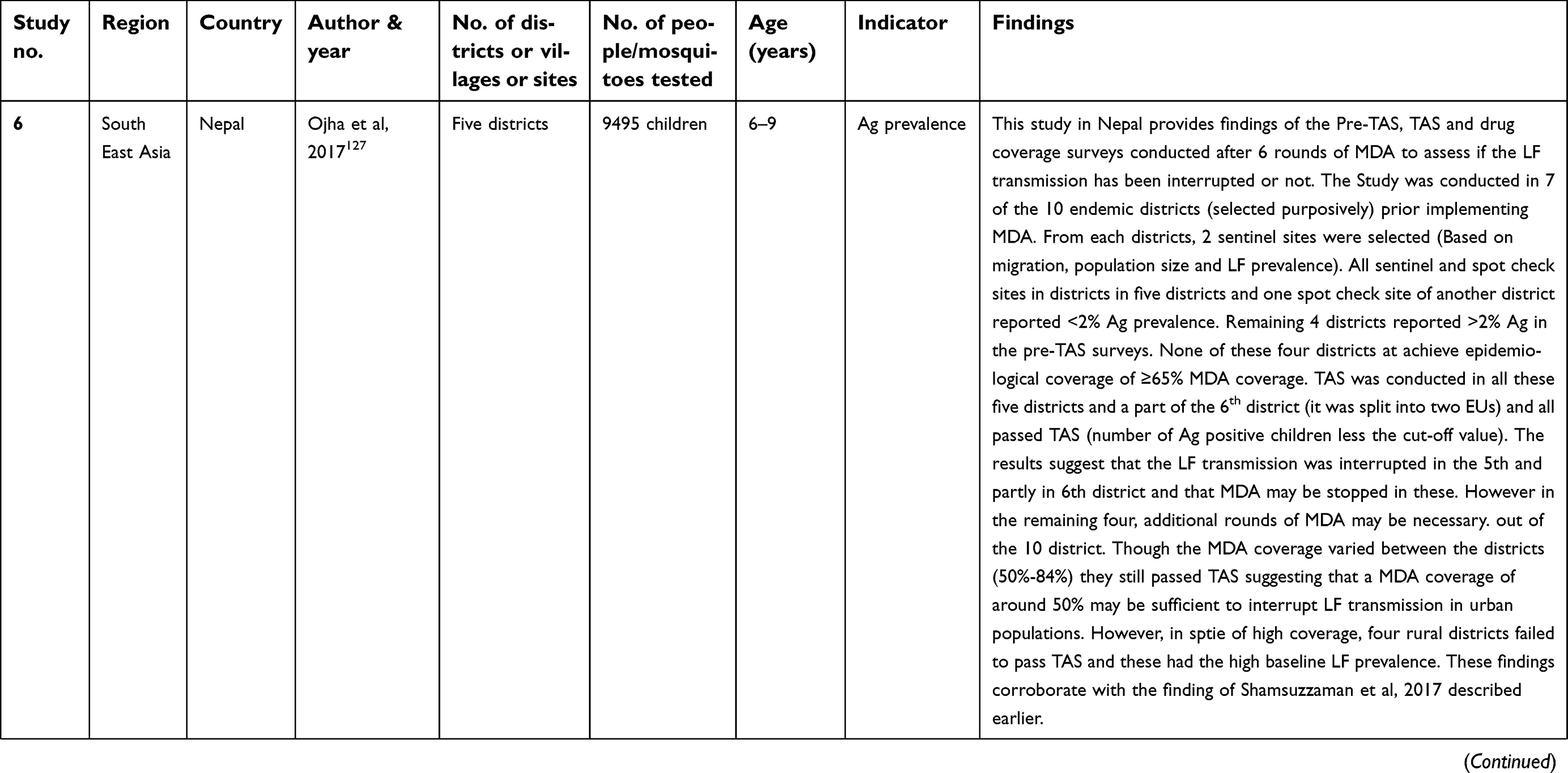
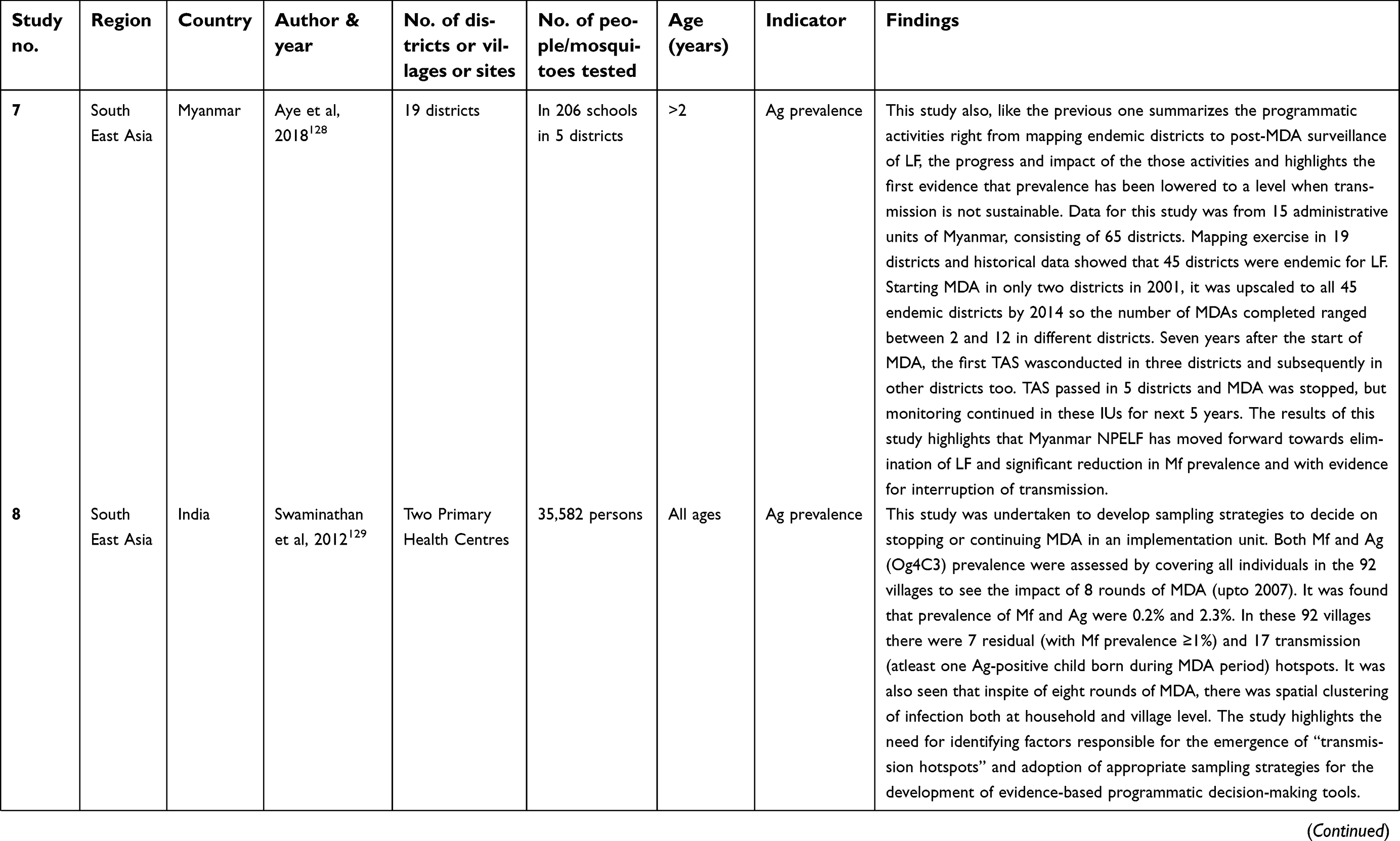
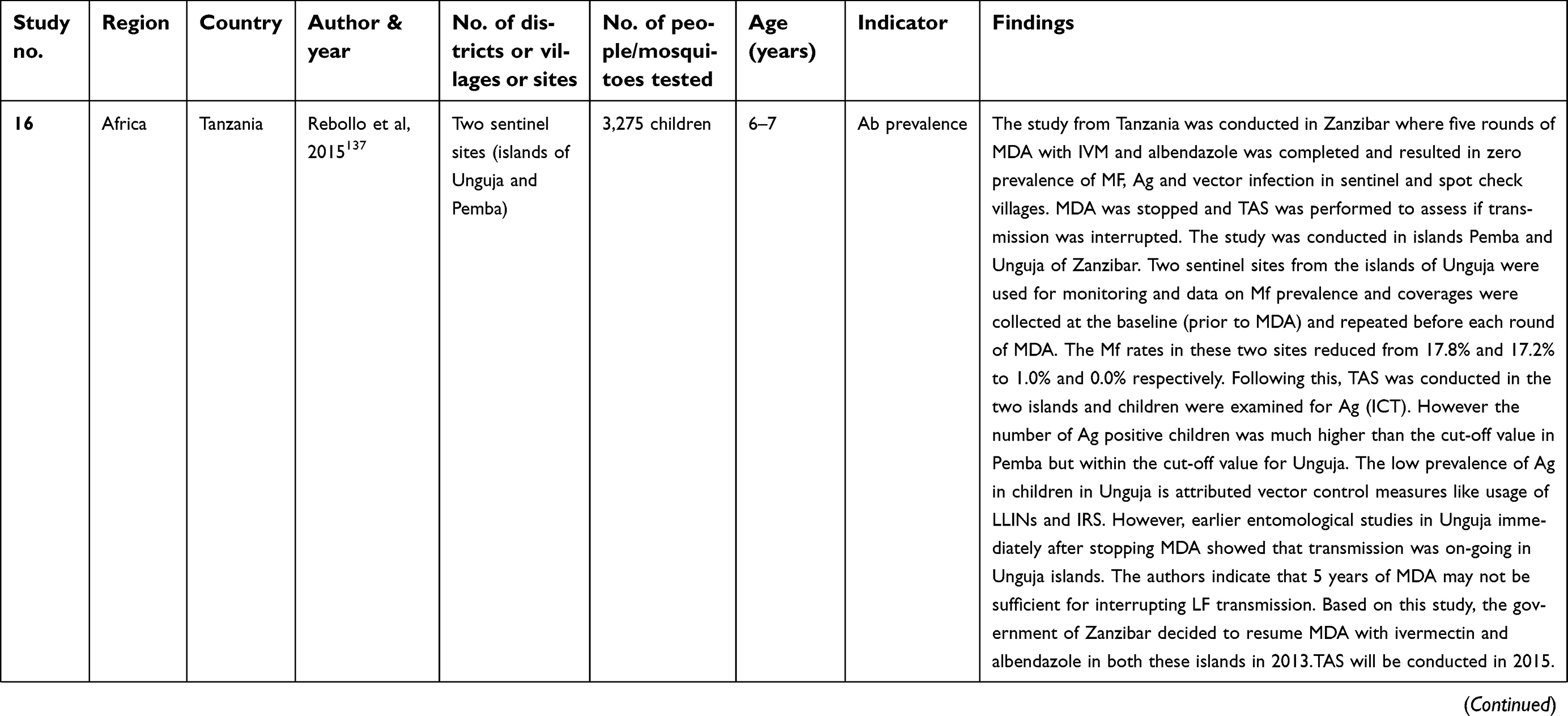
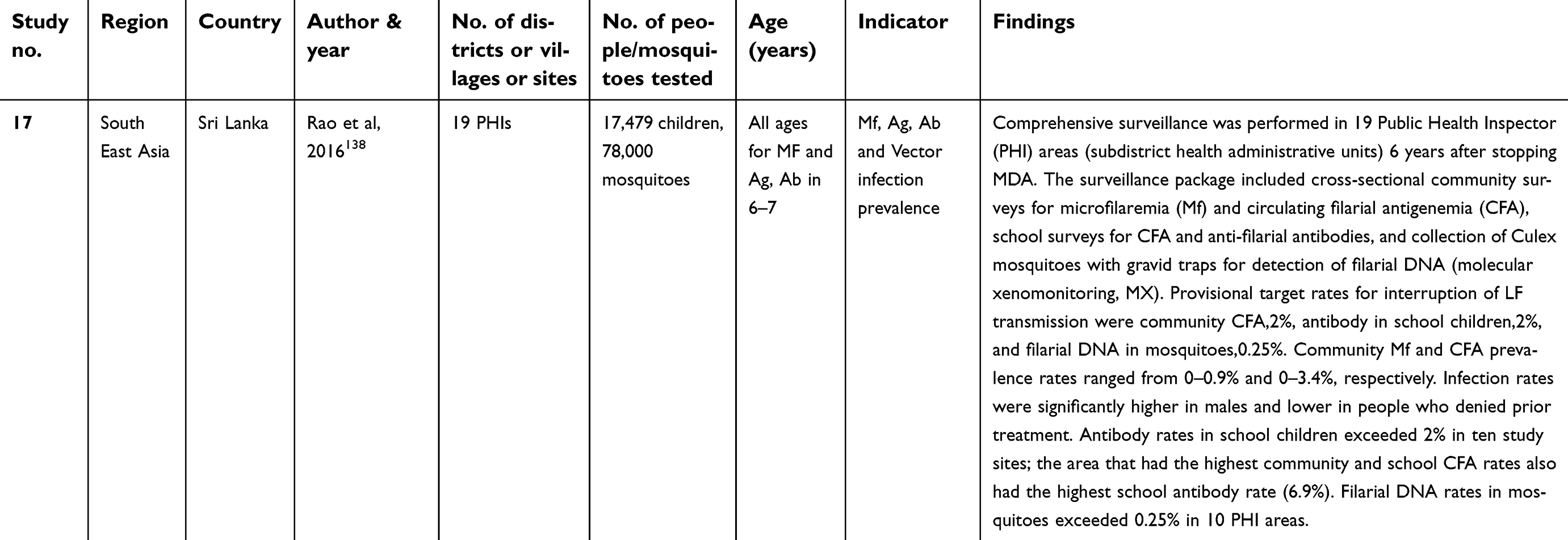
A total of 17 studies (eleven from South East Asia, three from Western Pacific, two from Africa and one from American regions) have reported the findings during the post-MDA monitoring phase. Of these, one additionally monitored pre-MDA period and another study monitored pre-, during- and post-MDA periods. These studies highlighted the importance of monitoring during different phases of MDA (Table 4).
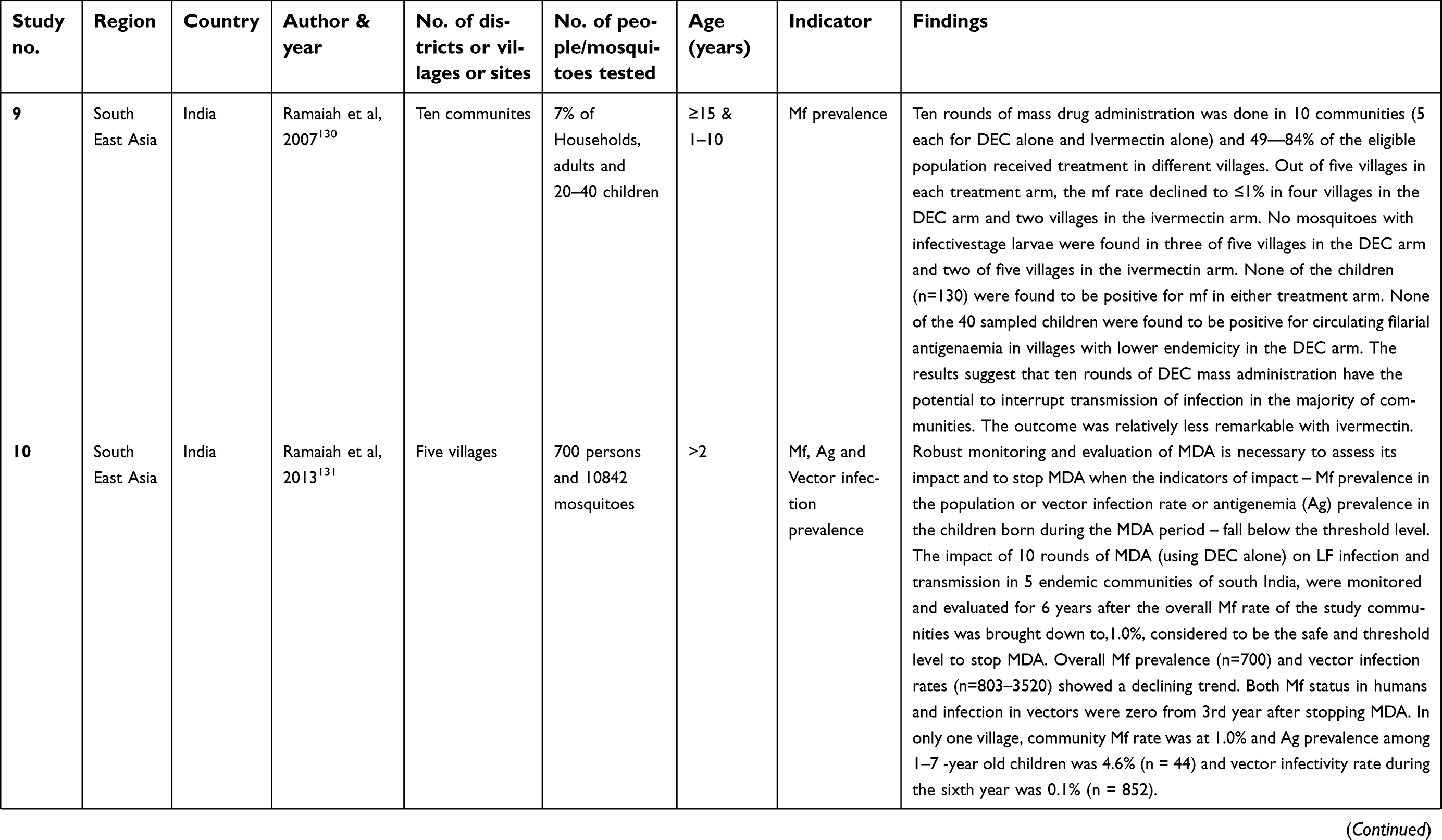
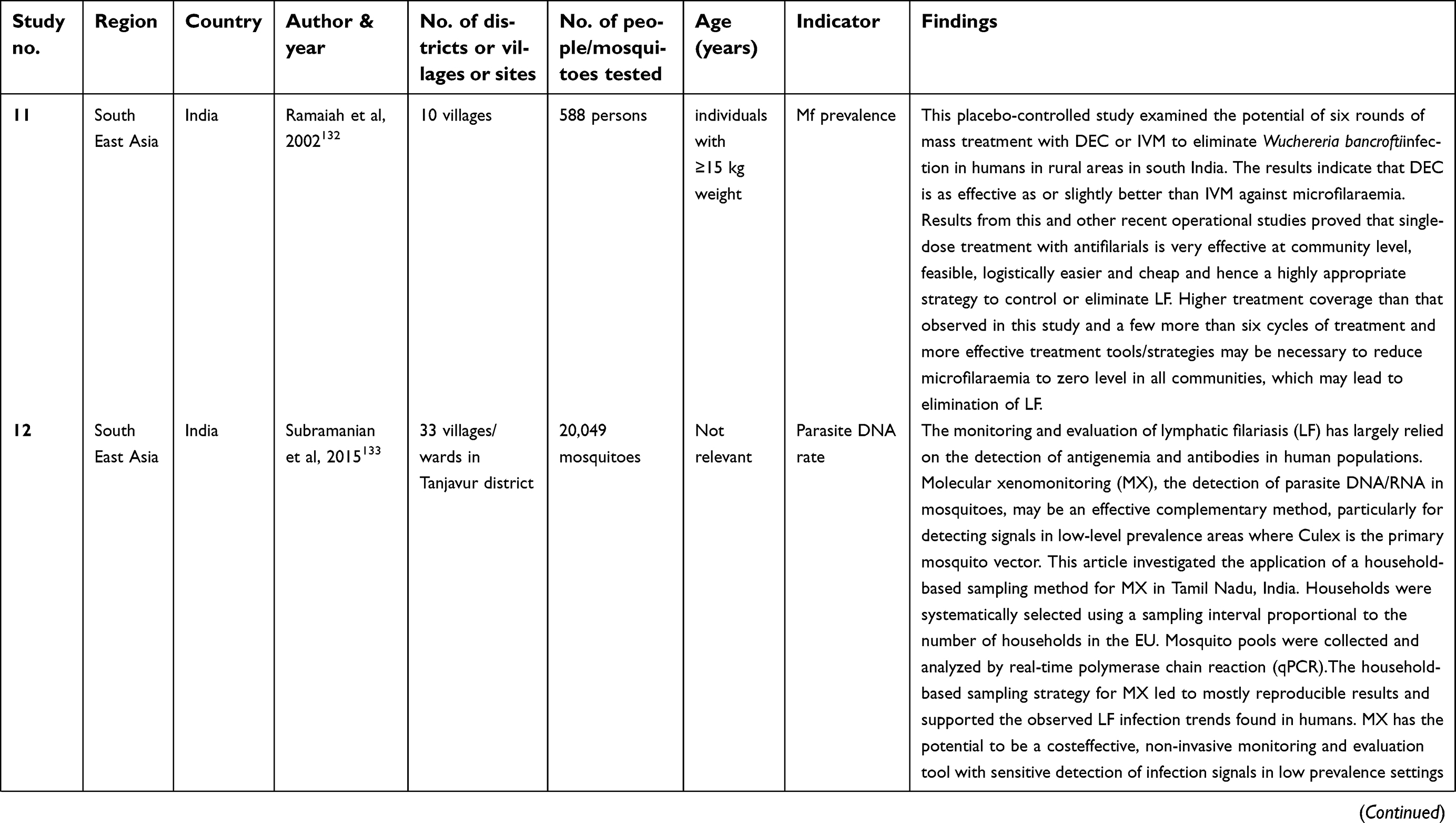
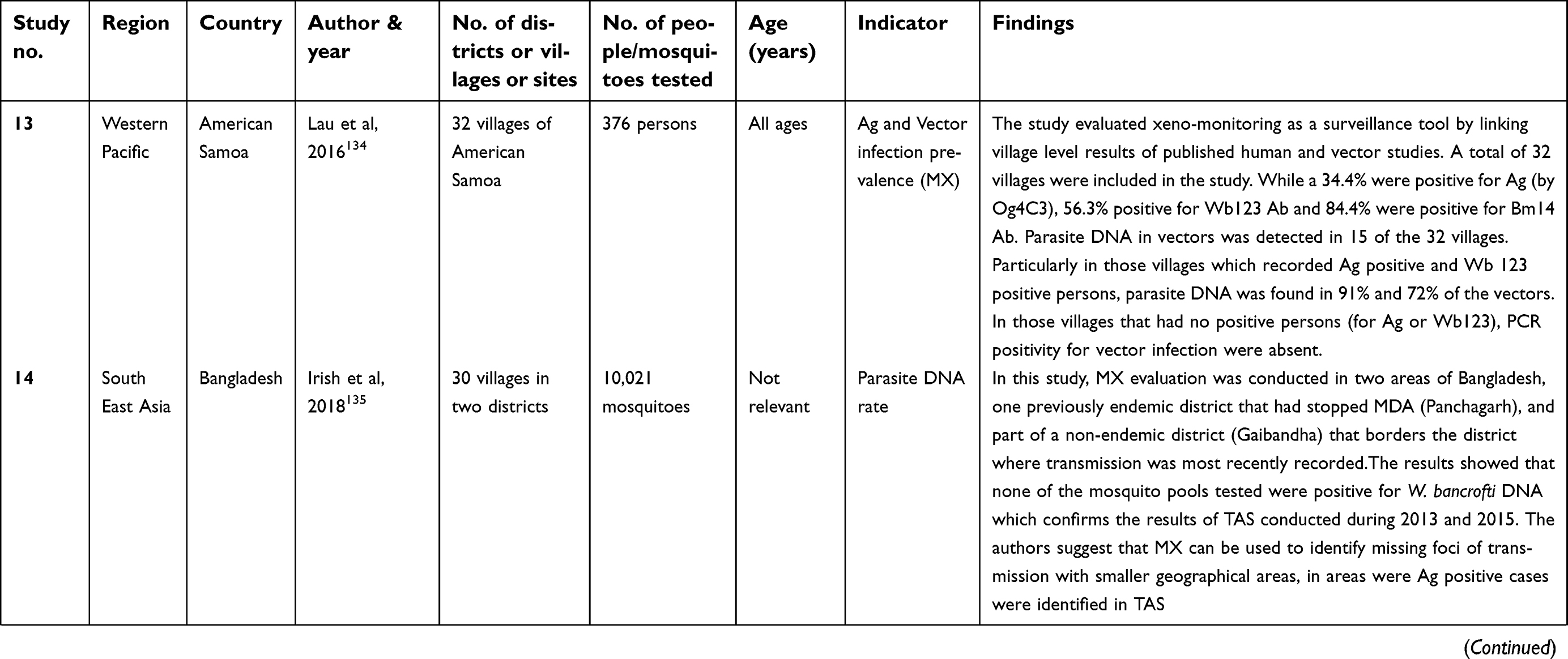
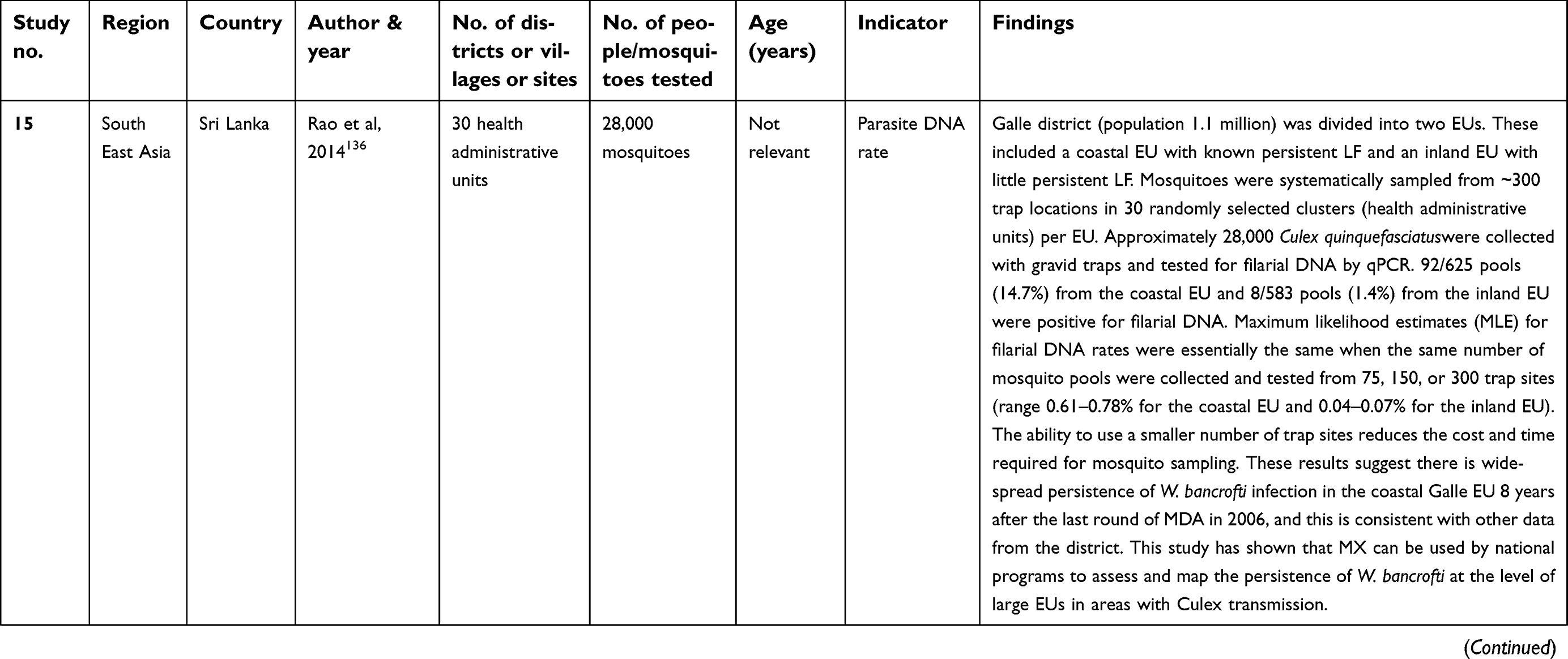
 | Table 4 Details of the studies where monitoring was done post-MDA |
 | Table 4 (Continued). |
 | Table 4 (Continued). |
 | Table 4 (Continued). |
 | Table 4 (Continued). |
 | Table 4 (Continued). |
 | Table 4 (Continued). |
 | Table 4 (Continued). |
 | Table 4 (Continued). |
 | Table 4 (Continued). |
 | Table 4 (Continued). |
 | Table 4 (Continued). |
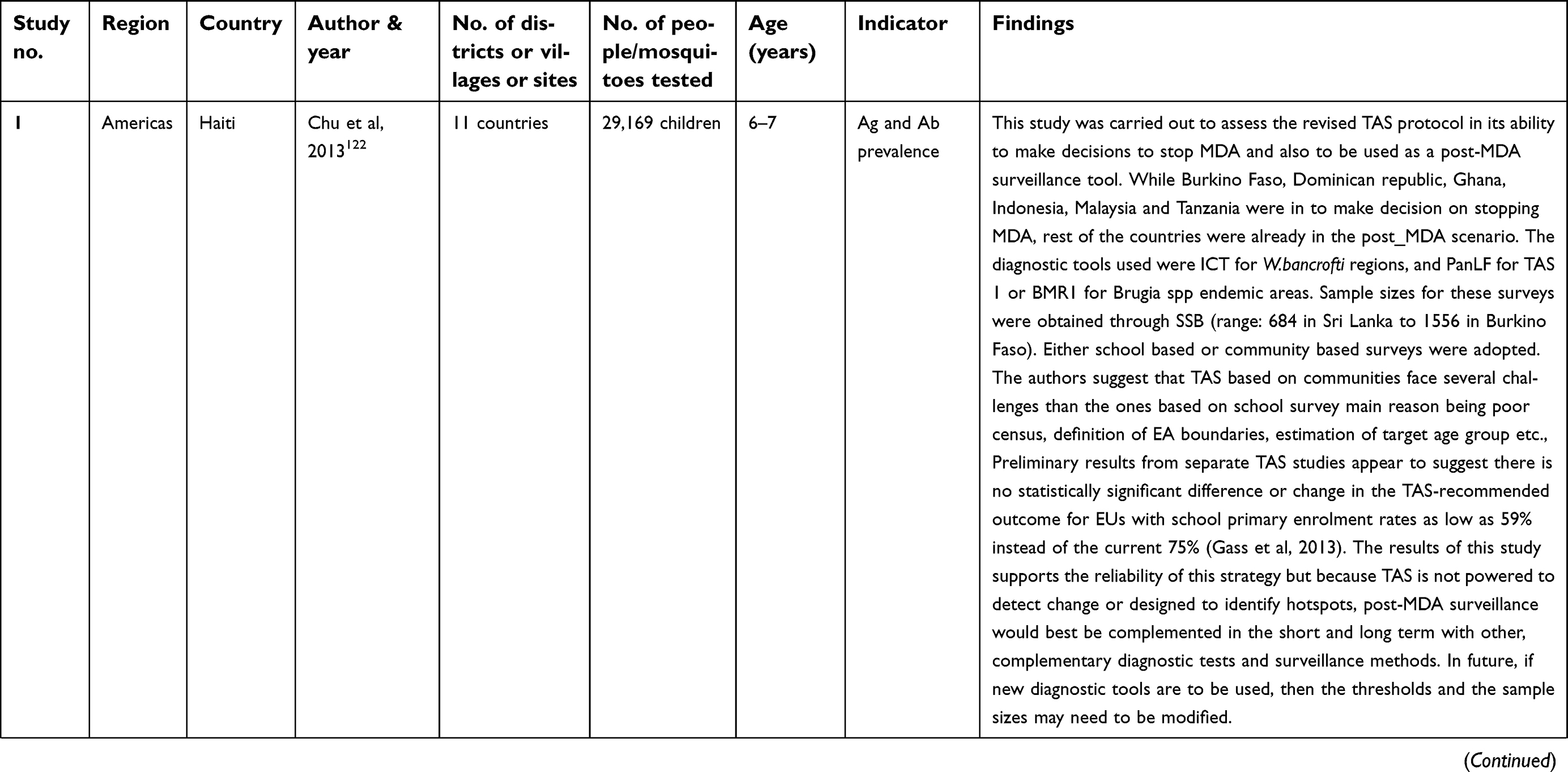
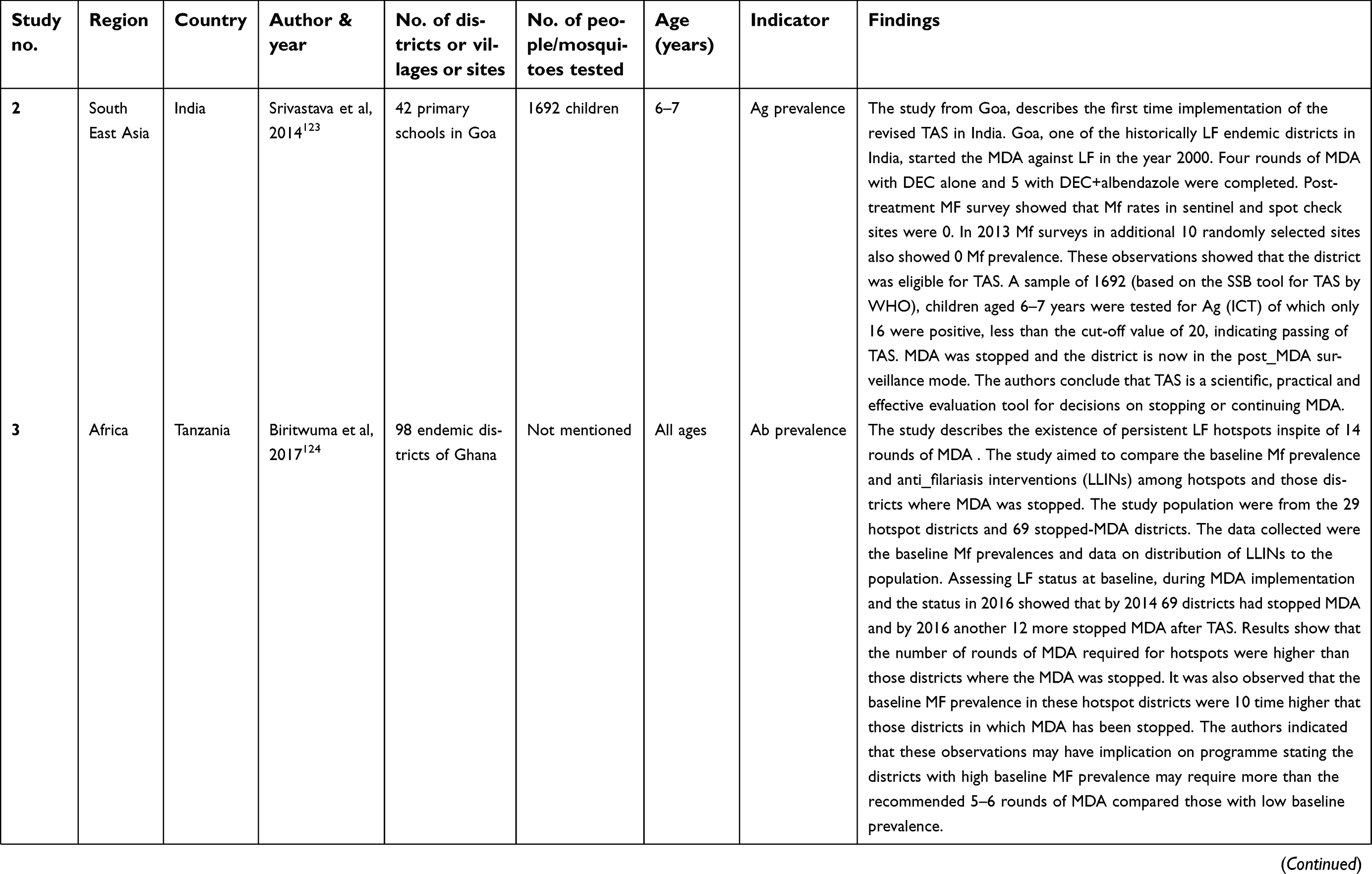
As seen in pre- and during-MDA phases, studies in the post-MDA phase have also used Ag/Ab and vector infection indicators to monitor the LF situation. In a multi-country study (consisting of eleven countries) Chu et al.121 reported that TAS protocol is a reliable strategy (either school- or community-based) to assess interruption of transmission. Similar observation was made in India122 who reported the first successful TAS in Goa in India after nine rounds of MDA, mentioning that TAS is a scientific, practical, and effective evaluation tool for stopping MDA. The authors emphasized the importance of focal survey to identify the source of infection in communities with antigen-positive children to prevent resurgence in an area declared free from MDA.
A study from Ghana reported the existence of hotspots, despite 14 years of MDA, and attributed the persistence of hotspots to its high baseline Mf prevalence123 and reported that more than the standard five to six rounds of MDAs, say up to 14 rounds were required to interrupt transmission. Another study124 summarized the current situation of LF in Bangladesh through TAS conducted in 19 districts (which had undergone 5–12 rounds of MDA) and 15 low endemic districts (not given MDA). The results showed a significant reduction in prevalence of geographical distribution of infection across Bangladesh and attributed this to factors like good administrative development and health system infrastructure, relative political stability, strong political commitment and financial support, strong program management leadership and heightened awareness of morbidity in the endemic areas. The authors also suggested that districts that required more rounds of MDA had higher baseline Mf prevalence. Post-MDA surveillance in Cambodia125 showed that all the endemic districts had undergone five rounds of MDA with >65% coverage and had passed even TAS 3 and is currently in the final stage of declaring LF elimination. The authors have attributed this success to the commitment of the government and effective implementation of MDA, monitoring and evaluation, and surveillance activities. MDA was successfully implemented even in forested and remote endemic areas through advocacy, sensitization of various departments, active participation of provincial- and central-level program personnel in MDA activities, and financial and related support from partners and stakeholders. In Nepal126 it was shown that interruption of transmission was established in five of the ten endemic districts and in one EU of another district following successful TAS after six rounds of MDA, in-spite of not achieving the optimum coverage of 65% in three districts. In the remaining districts, MDA continued as they had a higher baseline Mf prevalence as reported in Bangladesh.124
In Myanmar127 the program initiated in one district in 2001 was up-scaled to 42 of the 45 endemic districts by 2014. This slow progress in upscaling was attributed to lack of funding, resources (eg training of basic health staff, advocacy materials), continued problems in procuring adequate quantities of DEC, as well as security-related issues. In spite of this, five districts declared interruption of transmission with two passing TAS 1 after 6–10 rounds of MDA and three districts that had passed TAS 2 after undergoing five rounds. In this study also, a predictive modeling approach showed that the decline in Mf prevalence was associated with the number of MDAs and initial Mf prevalence as observed in the above studies.
The PHC area in Thanjavur district, Tamil Nadu, India,128 reported low levels of infection (community Mf and Ag prev-0.2%,and 2.3%, and Ag prevalence in 2–8 years old children was 0.12%) after eight rounds of MDA with spatially clustered infection both at household and community level. Based on this study MDA was stopped in this area. Results of a long-term community trial that evaluated the effectiveness of ten rounds of DEC or ivermectin alone in ten villages of the Villupuram district of Tamilnadu, India129-131 concluded that ten rounds of MDA with DEC alone would be able to interrupt transmission of LF and achieve the objective of LF elimination.129 Subsequent post-MDA study130 in the same area indicated that 6 years of post-MDA monitoring and evaluation was adequate to discern the status of transmission interruption and for making an appropriate decision on certifying LF elimination.
Few studies have also evaluated the use of MX for confirming the findings of TAS and, also as a post-MDA surveillance tool. In a study from India, Ag-prevalence in children and vector infection indicators were used to assess the LF situation in one of the evaluation areas that stopped MDA (after 8 rounds).128,132 The estimated vector infection rate based on xenomonitoring corroborated with the decision based on human infection for stopping MDA in this evaluation unit, suggesting that xenomonitoring could be a potential alternative to post-MDA surveillance or validation. Further, vector infection prevalence was reported to be higher in communities which were transmission hotspots (with Ag positive children). Similar observations were made in American Samoa133 that detected parasite DNA in vector mosquitoes in the communities where Ag-positive persons were detected. In Bangladesh, one study134 reported MX evaluation for transmission interruption in two areas; one previously endemic district that had stopped MDA (Panchagarh), and another part of a non-endemic district that reported transmission. In a study from Sri Lanka, in addition to TAS, a comprehensive surveillance (a package included cross-sectional community surveys for Mf and Ag, school surveys for Ag and Ab, besides xenomonitoring) was carried out to assess the LF situation 6 years after cessation of MDA in 19 Public Health Inspector (PHI) areas of the eleven EUs in eight districts.135 The prevalence of infection in vector exceeded the provisional threshold of 0.25% in 10 of the 19 PHIs where the school- and community-based Ag- and Ab surveys reported <2% Ag and >2% Ab prevalence. Based on the results, the authors recommended use of antibody and MX testing as tools to complement TAS for post-MDA surveillance. Similarly, a study from Tanzania showed that in areas that had passed TAS, MX provided evidence of on-going transmission and this led to re-initiation of MDA for another two rounds in those areas. In a subsequent study from Sri Lanka,136 MX indicated ongoing transmission (filarial DNA prevalence of 0.63% greater than the provisional threshold of 0.25%135) in a coastal district 8 years post-MDA, although Mf prevalence (0.2%) was much lower than the threshold for stopping MDA (1%) proving xenomonitoring is more sensitive than TAS and Mf-survey.
Mapping and monitoring
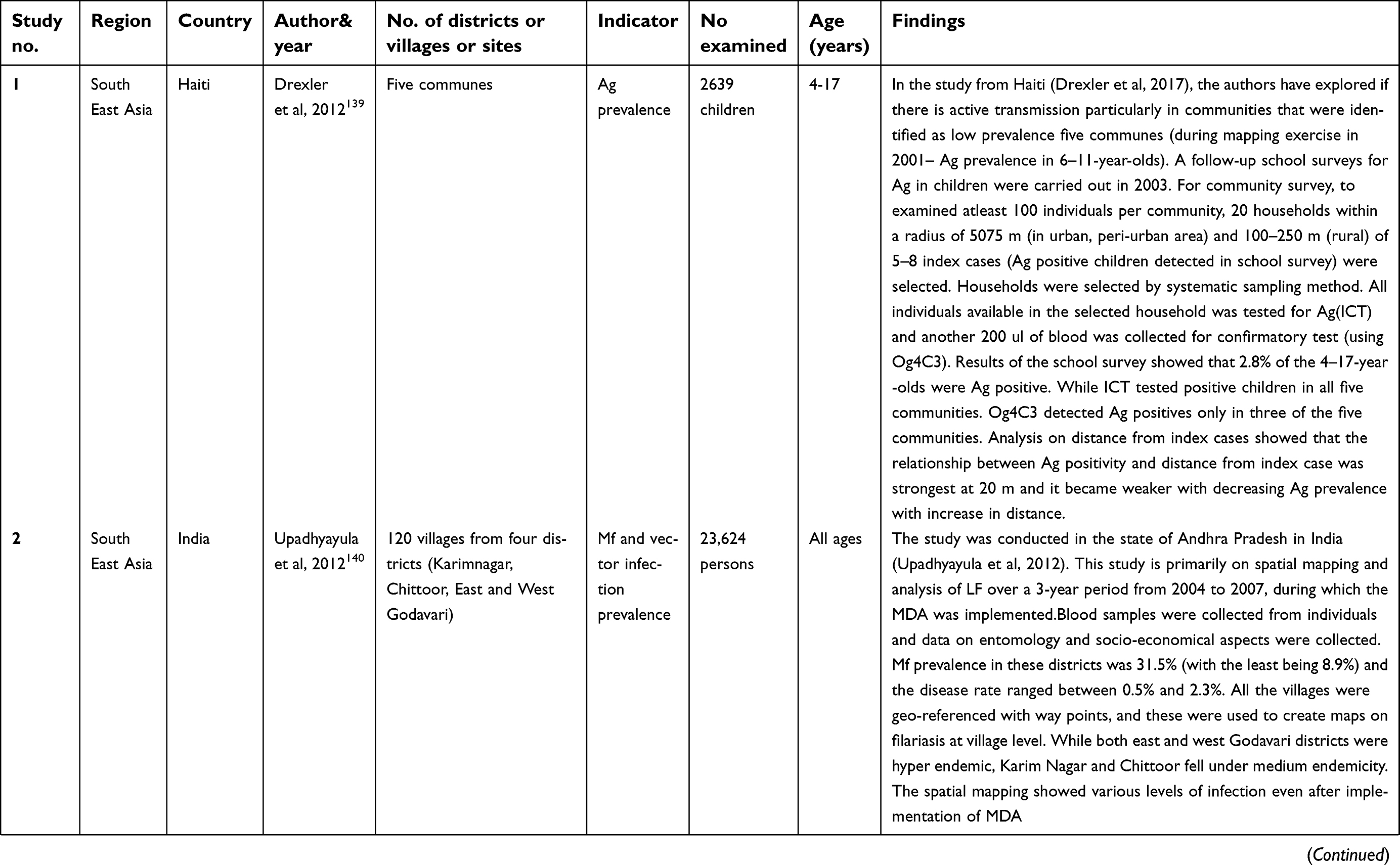
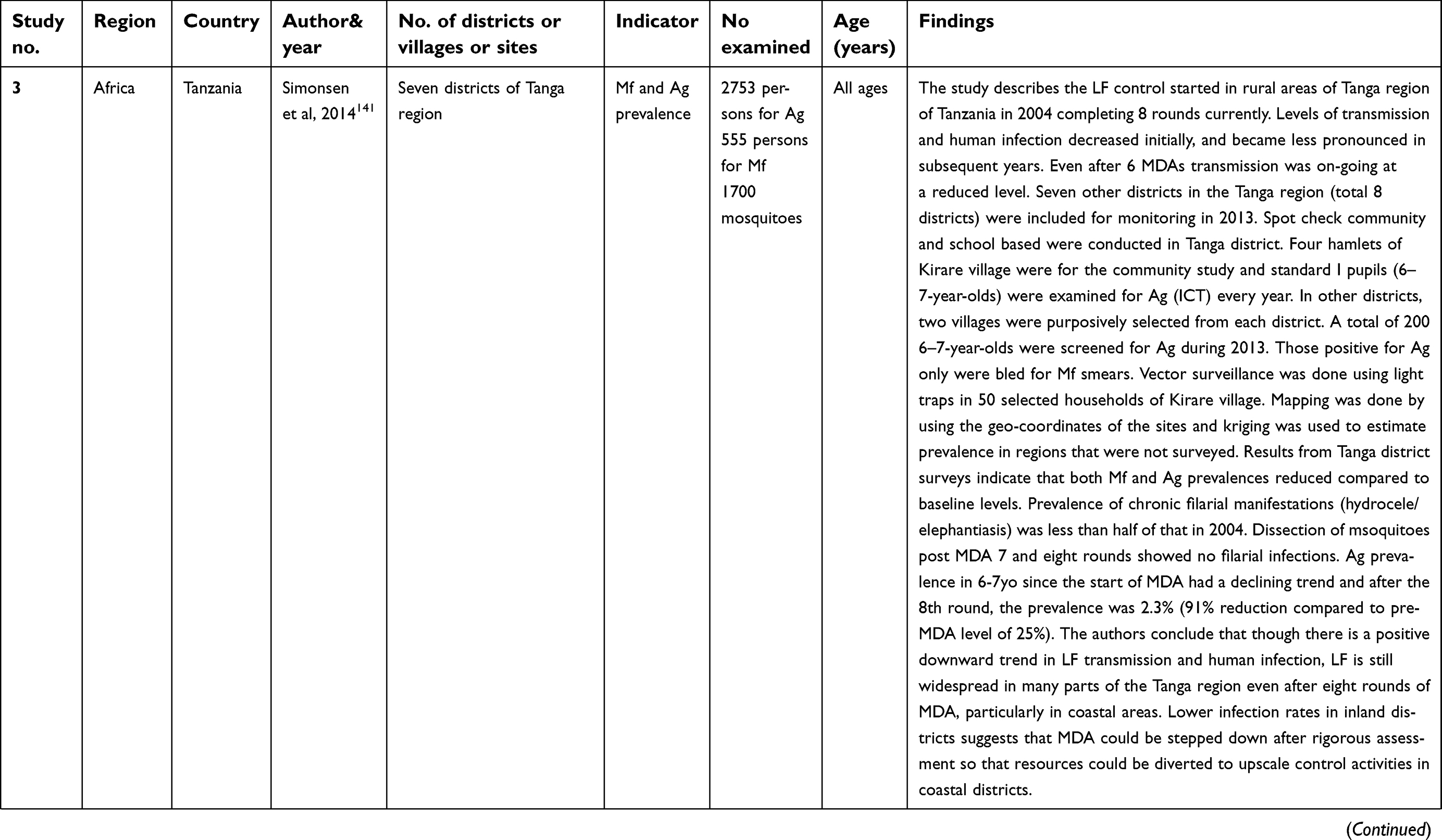
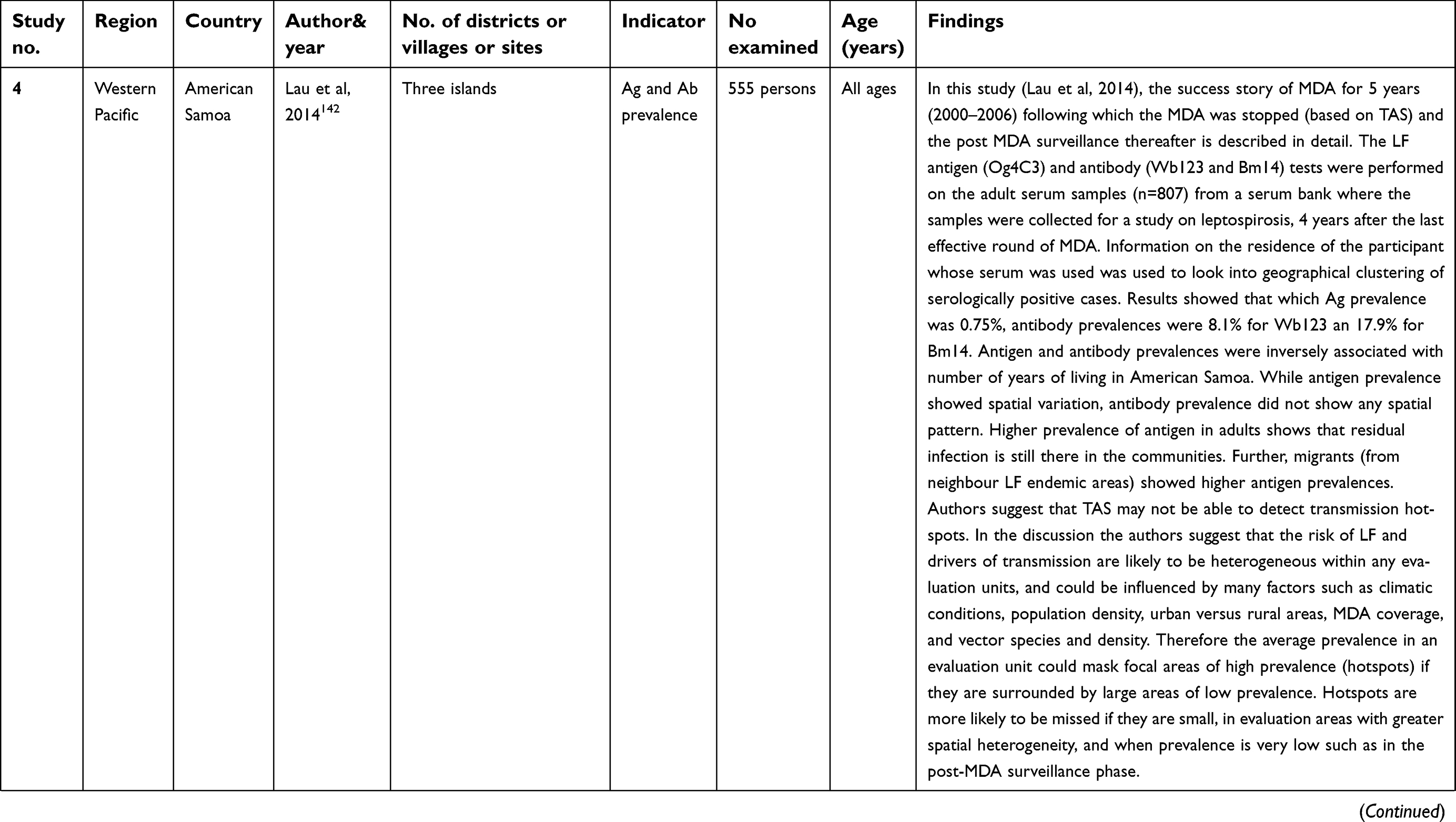
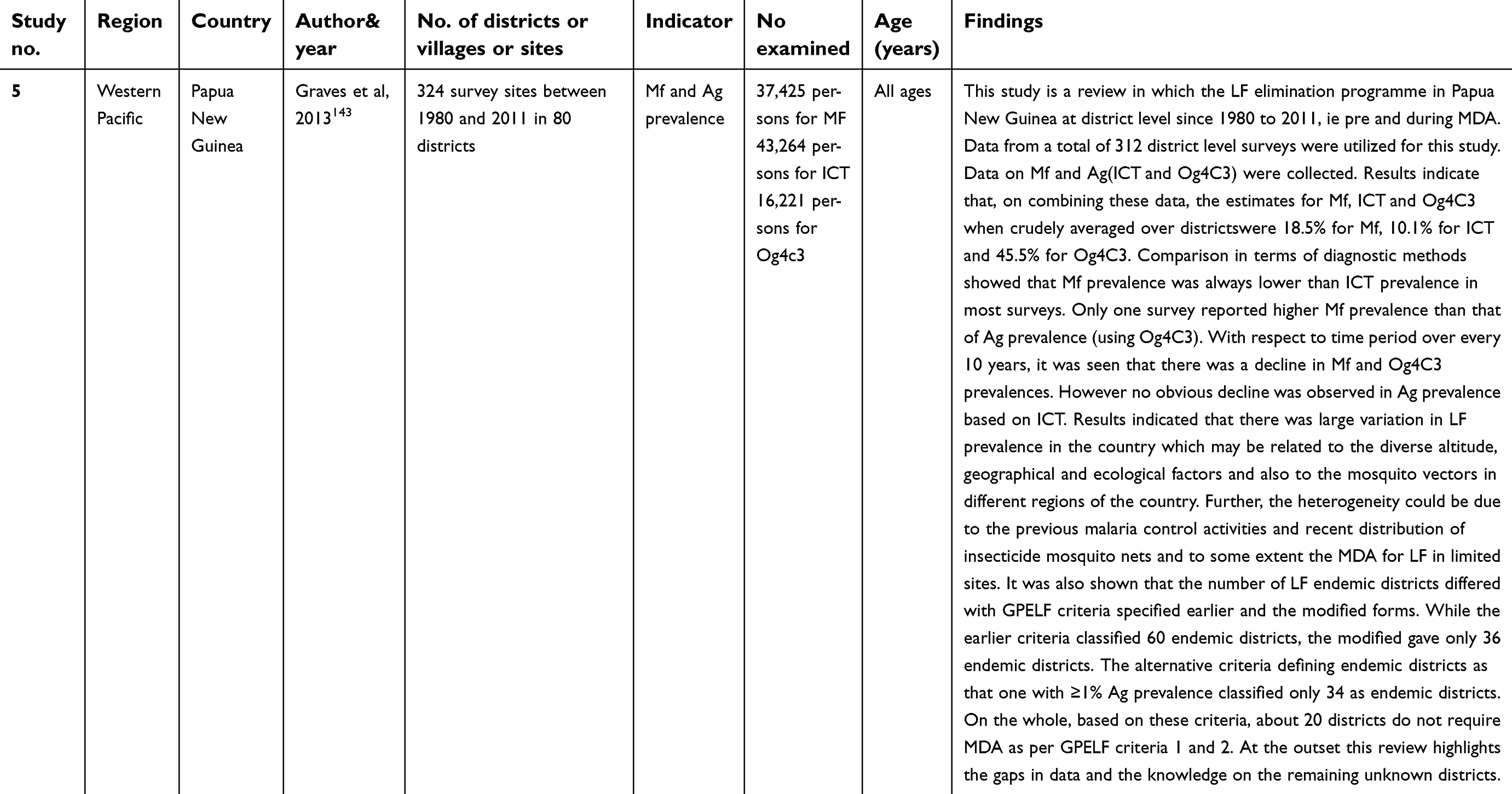
Five studies reported on mapping and monitoring together (Table 5) during MDA (four studies) and post-MDA phase (one study).
 | Table 5 Details of the studies that carried out both mapping and monitoring |
 | Table 5 (Continued). |
 | Table 5 (Continued). |
 | Table 5 (Continued). |
In Haiti, of the five districts that were mapped as low endemic based on Ag survey prior to MDA,137 transmission was on-going during MDA in three districts and a possibility of spatial dependency up to a distance of 20 m from an index case (an Ag-positive child). Spatial mapping of Mf prevalence (overall 31.5%, least 8.5%) after three rounds of MDA in four endemic districts of Andhra Pradesh in India showed spatial heterogeneity with non-interruption of transmission.138
A study in Tanzania139 showed that even after six rounds of MDA, transmission was on-going but at a lower level. However, the Ag prevalence in 6–7-year-olds had started showing a declining trend. One study,140 using samples from a serum bank assessed the prevalence of LF Ag and Ab, 4 years after stopping MDA. They reported that while Ag prevalence was very low (0.8%), Ab prevalence (8.1%) was high as expected. It was seen that while Ag prevalence showed spatial variation, Ab prevalence did not. Another study141 from Papua New Guinea that reviewed the district level distribution of MDA during 1980–2011, reported that targeting of districts by level of prevalence will strengthen the control program, facilitate monitoring of the disease trend and increase the likelihood of reaching the target of LF elimination by 2020.
Discussion
This review on mapping and monitoring of LF is based on 84 studies from 32 countries representing all WHO regions except the European region over two decades between 1997 and 2018. Most African countries followed the mapping protocol for delimitation in addition to historical data. Countries from other regions used WHO mapping strategy and other methods like the Key informant technique,70 physical examination by health workers for chronic symptoms of filariasis, disease prevalence and Mf prevalence for mapping LF. The review has shown how the WHO mapping strategy that initially used convenience sampling design evolved to become a more robust 30-cluster-based design in line with the confirmatory mapping tool94,95 to delimit areas requiring MDA. This confirmatory mapping tool tested Ag among older children aged 9–14 years in 30 randomly selected schools and was proved to be more effective in low-prevalence settings. Though this tool is similar to the LF-TAS, the sample size requirement is only one-fourth of that of TAS and covers older children and is currently termed as “Mini-TAS.” In the current scenario, where most LF endemic countries have completed at least five rounds of MDA, it is proposed to use this for re-mapping in uncertain and naive areas bordering the endemic districts or the unsurveyed areas that have the risk of LF transmission to help the country program to bring in or exclude those areas from the MDA net. However, the challenge will be to choose the appropriate test (Ag/Ab surveys in humans or MX for vector infection) for re-mapping to identify new transmission hotspots if any, and prevent resurgence during post-MDA surveillance.
This review has highlighted how mapping helped in implementing the elimination program only in the areas known to be endemic for LF thereby preventing MDA in areas where the LF was non-endemic. Mf and Ag surveys were used in prioritizing areas requiring MDA and these data were subsequently used to visualize the extent of LF distribution. Accounting for the spatial component in these data with appropriate spatial models, LF prevalence was predicted up to a distance of 25–50 km around the surveyed locations to provide additional information on risk of LF to the program authorities to act upon.60,90,93,96–98 Such data also provided scientific evidence on the clustering nature of LF around a transmission/residual foci which again could be used to extend MDA or other supplementary interventions in those neighboring areas. In addition, mapping data collected over time from different countries were also useful for modeling the trends of LF prevalence accounting for the effect of climate change on parasite transmission.91,92
The mapping initiative for LF also paved the way to integrate mapping of all NTDs (LF, podoconiosis, schistosomiasis, loasis and STH) which was proven to be cost effective and feasible while covering a large geographical area.64,88,89,100,142 However, it could be logistically intensive and methodologically difficult due to the difference in the tests used and the target groups to be covered. As this is one of the important activities under the WHO road map143 for implementing interventions against NTDs, the challenges for the endemic countries would be in terms of strong in-country leadership, man power and resources to conduct the surveys and application to capture the data to make it cost effective and feasible.
One of the reasons for the success of this large scale elimination program is attributed to the strong in-built component of monitoring and evaluation during- and post-MDA. The review has shown that impact of MDA is generally measured in terms of Mf and Ag prevalence in humans. However, in recent times Ab prevalence in humans and MX for assessing parasite DNA in vectors are being used for the purpose in view of their high sensitivity in detecting exposure/transmission. It was observed that the WHO recommended strategy of 5–6 rounds of MDA was not sufficient in interrupting transmission103,107,109,111,114,118,119,123 suggesting the requirement of additional interventions like frequent MDA treatments, distribution of insecticide treated nets and other localized vector control measures.118 Additional efforts warranting improved MDA coverage and adequate monitoring by the implementing authorities were recommended. Non-interruption of transmission and persistence of hotspots in spite of several rounds of MDA (up to 12 rounds) were found to be significantly associated with high baseline prevalence of Mf or Ag118,123,124 and systematic non-compliance to MDA.117 These imply that the number of rounds required to reach the threshold of <1% Mf prevalence (or 2% Ag prevalence) cannot be generalized for all endemic areas. The success stories in Bangladesh124 and Cambodia125 indicated that in addition to the adequate MDA coverage, the reasons for success of the elimination program in a country is driven by 1) the commitment of the government and effective implementation of MDA even in remote areas; 2i) active participation of provincial- and central-level program personnel; 3) adequate financial and related support from stakeholders and partners; and 4) a rigorous monitoring and evaluation plan and post-MDA surveillance activities. The impact of MDA on LF disease, both chronic and acute forms were promising with not only reduction in the disease prevalence following 5–8 rounds of MDA but also in preventing new cases of hydrocele, thereby indirectly achieving the MMDP goals too.104,106
In LF-oncho co-endemic areas, impact assessment surveys during MDA showed that several rounds of MDA with monotherapy of Ivermectin alone, 100, 107, 113 could not interrupt LF transmission and inclusion of albendazole in the subsequent rounds helped in reducing the Mf and Ag prevalence in humans and vector infection and infectivity rates significantly, respectively.109,111 However, the decision on stopping MDA in such areas would imply stopping albendazole but continuing with ivermectin alone along with post-MDA surveillance to ensure there is no resurgence of the disease.
TAS, the decision-making tool for stopping or continuing MDA was adjudged to be a robust, scientific and reliable tool based on the results from 12 countries,121 including India,122 based on a single EU. Detection of filaria parasite DNA in vectors in areas with Ag-positive children, showed that the results of TAS and MX corroborate with each other, when the decision to continue MDA is to be made. However in a few countries, it was also shown that assessing the impact of MDA on transmission interruption was more accurate if Ag tests in TAS are complemented with Ab tests during post-MDA surveillance as they provide additional evidence of on-going transmission/exposure in the community, particularly in children.105,115,116,132,134 In some instances, even when both Ag (TAS) and Ab tests indicated interruption of transmission, vector infection prevalence through MX was found to be well above the provisional threshold level of 0.5% (indicating on-going transmission) suggesting that TAS may not be a sensitive tool in assessing complete interruption of transmission,133,135,136,142 particularly during post-MDA surveillance. In view of this, it was recommended MX/Ab surveys may be used as a complementary tool for TAS to assess transmission, particularly during post-MDA surveillance and validation phases.133,135,136,142 These observations suggest that though TAS is a powerful tool while making decisions on stopping MDA or not, it may or may not be very sensitive particularly during the post-MDA surveillance and validation phases when the transmission levels are very low. Therefore MX, a sensitive tool in detecting on-going transmission may also be done alongside so that there is added support to the results by TAS. However, implementing MX under programmatic mode will be a major challenge as the expertise and the facilities for running the molecular assays need to be made available at all implementation unit levels.
Currently, in order to eliminate LF in hard core areas with persisting transmission, WHO has recommended the use of triple drug regimen (IDA, Ivermectin + Diethylcarbamazine + Albendazole) for MDA towards accelerated elimination of LF by 2020.6 While the monitoring and impact evaluation methods are in place for the existing LF elimination strategy of MDA with two drug regimens (DA, DEC + Albendazole),4 the challenge will be to develop an appropriate monitoring and evaluation (M & E) strategy, as this strategy is expected to interrupt transmission with 2–3 rounds of MDA in the endemic areas. In addition to the appropriate indicators sensitive enough to measure the human infection levels and or vector infection/infectivity levels, the target population need to be examined and the diagnostic to be used in humans for assessing transmission interruption needs to be identified.
Conclusions
The review has highlighted the necessity of mapping for LF before a massive intervention program is to be implemented in large geographical area as it helps in identifying only those areas that require the intervention, thereby saving resources and man-power. If the area is endemic for other NTDs as well, an integrated mapping approach would be cost effective as well as feasible. For example in India, if an area is prone for dengue, chikungunya and LF, serological or MX surveys with appropriate test kits/devices with good sampling designs can be used to carry out integrated mapping of these diseases at the same time sharing the man-power and other resources.144 However, to include this as a part of a national program, a substantial investment has to be made in providing the infrastructure and training to personnel to carry out serological and MX surveys for the NTDs prevalent in the area. The review compared the performance of both serological (Ag/Ab) and molecular tools in assessing the status of LF transmission and highlighted that MX could play a major role in the context of M & E for LF. As most endemic countries under GPELF are progressing towards post-MDA surveillance, validation and elimination phases, M & E component needs to be revised/strengthened with appropriate tools either Ag complemented with Ab or MX for verifying the absence of transmission, assessing the risk of resurgence, identifying hotspots, particularly in the context of introduction of IDA as MDA for accelerated elimination.
With this holistic approach, national programs should take advantage of the existing serological tools and MX and incorporate them wherever necessary in their integrated vector management program to control, monitor and eliminate all vector borne diseases. And wherever possible both mapping of diseases and monitoring of interventions should adopt an integrated approach, to assess the current situation with minimum resources.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Michael E, Bundy DAP. Global mapping of lymphatic filariasis. Parasitol Today. 1997;13(12):472–476.
2.
3.
4.
5. WHO. Operational Guidelines for Rapid Mapping of Bancroftian Filariasis in Africa. WHO/CDS/CPE/CEE/2000.9 [press release]. Geneva: World Health Organization. 2000.
6.
7. Babu BV. A rapid method to assess the coverage of the mass drug administration of diethylcarbamazine in the program to eliminate lymphatic filariasis in India. Southeast Asian J Trop Med Public Health. 2005;36(1):44–45.
8. Bhumiratana A, Pechgit P, Koyadun S, Siriaut C, Yongyuth P. Imported bancroftian filariasis: diethylcarbamazine response and benzimidazole susceptibility of Wuchereria bancrofti in dynamic cross-border migrant population targeted by the National Program to Eliminate Lymphatic Filariasis in South Thailand. Acta Trop. 2010;113(2):121–128. doi:10.1016/j.actatropica.2009.10.004
9. Boakye DA, Baidoo HA, Glah E, Brown C, Appawu M, Wilson MD. Monitoring lymphatic filariasis interventions: adult mosquito sampling, and improved PCR-based pool screening method for Wuchereria bancrofti infection in Anopheles mosquitoes. Filaria J. 2007;6:13. doi:10.1186/1475-2883-6-13
10. Cano J, Rebollo MP, Golding N, et al. The global distribution and transmission limits of lymphatic filariasis: past and present. Parasit Vectors. 2014;7:466. doi:10.1186/1756-3305-7-23
11. Carme B. Mapping of lymphatic filariasis: “to be (in English) or not to be”. Med Trop (Mars). 2010;70(5–6):425–427.
12. Carme B. Rapid assessment procedure for loiasis and mapping lymphatic filariasis: two perfect illustrations of “to be in English or not to be”. PLoS Negl Trop Dis. 2012;6(12):e1863. doi:10.1371/journal.pntd.0001863
13. Chesnais CB, Vlaminck J, Kunyu-Shako B, et al. Measurement of circulating filarial antigen levels in human blood with a point-of-care test strip and a portable spectrodensitometer. Am J Trop Med Hyg. 2016;94(6):1324–1329. doi:10.4269/ajtmh.15-0916
14. De Rochars MB, Direny AN, Roberts JM, et al. Community-wide reduction in prevalence and intensity of intestinal helminths as a collateral benefit of lymphatic filariasis elimination programs. Am J Trop Med Hyg. 2004;71(4):466–470.
15. Dunyo SK, Appawu M, Nkrumah FK, Baffoe-Wilmot A, Pedersen EM, Simonsen PE. Lymphatic filariasis on the coast of Ghana. Trans R Soc Trop Med Hyg. 1996;90(6):634–638.
16. Eigege A, Richards FO
17. El Setouhy M, Ramzy RM. Lymphatic filariasis in the Eastern Mediterranean Region: current status and prospects for elimination. East Mediterr Health J. 2003;9(4):534–541.
18. Fontes G, Rocha EM, Brito AC, Antunes CM. Lymphatic filariasis in Brazilian urban area (Maceio, Alagoas). Mem Inst Oswaldo Cruz. 1998;93(6):705–710.
19. Freeman AR, Lammie PJ, Houston R, et al. A community-based trial for the control of lymphatic filariasis and iodine deficiency using salt fortified with diethylcarbamazine and iodine. Am J Trop Med Hyg. 2001;65(6):865–871.
20. Gbakima AA, Appawu MA, Dadzie S, et al. Lymphatic filariasis in Ghana: establishing the potential for an urban cycle of transmission. Trop Med Int Health. 2005;10(4):387–392. doi:10.1111/j.1365-3156.2005.01389.x
21. Gunawardena S, Gunawardena NK, Kahathuduwa G, et al. Integrated school-based surveillance for soil-transmitted helminth infections and lymphatic filariasis in Gampaha district, Sri Lanka. Am J Trop Med Hyg. 2014;90(4):661–666. doi:10.4269/ajtmh.13-0641
22. Gyapong JO, Adjei S, Gyapong M, Asamoah G. Rapid community diagnosis of lymphatic filariasis. Acta Trop. 1996;61(1):65–74.
23. Gyapong JO, Adjei S, Sackey SO. Descriptive epidemiology of lymphatic filariasis in Ghana. Trans R Soc Trop Med Hyg. 1996;90(1):26–30.
24. Gyapong JO, Owusu IO, da-Costa Vroom FB, Mensah EO, Gyapong M. Elimination of lymphatic filariasis: current perspectives on mass drug administration. Res Rep Trop Med. 2018;9:25–33. doi:10.2147/RRTM.S125204
25. Gyapong JO, Webber RH, Morris J, Bennett S. Prevalence of hydrocele as a rapid diagnostic index for lymphatic filariasis. Trans R Soc Trop Med Hyg. 1998;92(1):40–43.
26. Harb M, Faris R, Gad AM, Hafez ON, Ramzy R, Buck AA. The resurgence of lymphatic filariasis in the Nile delta. Bull World Health Organ. 1993;71(1):49–54.
27. Harris JR, Wiegand RE. Detecting infection hotspots: modeling the surveillance challenge for elimination of lymphatic filariasis. PLoS Negl Trop Dis. 2017;11(5):e0005610. doi:10.1371/journal.pntd.0005610
28. Hodges MH, Smith SJ, Fussum D, et al. High coverage of mass drug administration for lymphatic filariasis in rural and non-rural settings in the Western Area, Sierra Leone. Parasit Vectors. 2010;3:120. doi:10.1186/1756-3305-3-22
29. Hodges MH, Sonnie M, Turay H, Conteh A, MacCarthy F, Sesay S. Maintaining effective mass drug administration for lymphatic filariasis through in-process monitoring in Sierra Leone. Parasit Vectors. 2010;5:232. doi:10.1186/1756-3305-5-232
30. Houston R. Salt fortified with diethylcarbamazine (DEC) as an effective intervention for lymphatic filariasis, with lessons learned from salt iodization programmes. Parasitology. 2000;121(Suppl):S161–S173.
31. Koudou BG, de Souza DK, Biritwum NK, et al. Elimination of lymphatic filariasis in west African urban areas: is implementation of mass drug administration necessary? Lancet Infect Dis. 2018;18(6):e214–e20. doi:10.1016/S1473-3099(18)30069-0
32. Leang R, Socheat D, Bin B, Bunkea T, Odermatt P. Assessment of disease and infection of lymphatic filariasis in Northeastern Cambodia. Trop Med Int Health. 2004;9(10):1115–1120. doi:10.1111/j.1365-3156.2004.01311.x
33. Lenhart A, Eigege A, Kal A, et al. Contributions of different mosquito species to the transmission of lymphatic filariasis in central Nigeria: implications for monitoring infection by PCR in mosquito pools. Filaria J. 2007;6:14. doi:10.1186/1475-2883-6-14
34. Lindsay SW, Thomas CJ. Mapping and estimating the population at risk from lymphatic filariasis in Africa. Trans R Soc Trop Med Hyg. 2000;94(1):37–45.
35. Mandal NN, Bal MS, Das MK, Achary KG, Kar SK. Lymphatic filariasis in children: age dependent prevalence in an area of India endemic for Wuchereria bancrofti infection. Trop Biomed. 2010;27(1):41–46.
36. Manhenje I, Galán-Puchades MT, Fuentes MV. Socio-environmental variables and transmission risk of lymphatic filariasis in central and northern Mozambique. Geospat Health. 2013;7(2):391–398. doi:10.4081/gh.2013.96
37. Melrose W, Rahmah N. Use of Brugia Rapid dipstick and ICT test to map distribution of lymphatic filariasis in the Democratic Republic of Timor-Leste. Southeast Asian J Trop Med Public Health. 2006;37(1):22–25.
38. Meyrowitsch DW, Nguyen DT, Hoang TH, Nguyen TD, Michael E. A review of the present status of lymphatic filariasis in Vietnam. Acta Trop. 1998;70(3):335–347.
39. Modi A, Gamit S, Jesalpura BS, Kurien G, Kosambiya JK. Reaching endpoints for lymphatic filariasis elimination- results from mass drug administration and nocturnal blood surveys, South Gujarat, India. PLoS Negl Trop Dis. 2017;11(4):e0005476. doi:10.1371/journal.pntd.0005476
40. Mohammad A, Hussain AKS, Swain S, Kadam S, Sanghamitra P. Mass drug administration for lymphatic filariasis elimination in a coastal state of India: a study on barriers to coverage and compliance. Infect Dis Poverty. 2014;3: 31–38
41. Mohammed KA, Molyneux DH, Albonico M, Rio F. Progress towards eliminating lymphatic filariasis in Zanzibar: a model programme. Trends Parasitol. 2006;22(7):340–344. doi:10.1016/j.pt.2006.05.010
42. Molyneux DH. Filaria control and elimination: diagnostic, monitoring and surveillance needs. Trans R Soc Trop Med Hyg. 2009;103(4):338–341. doi:10.1016/j.trstmh.2008.12.016
43. Msyamboza K, Ngwira B, Banda R, Mkwanda S, Brabin B. Sentinel surveillance of lymphatic filariasis, schistosomiasis soil transmitted helminths and malaria in rural southern Malawi. Malawi Med J. 2010;22(1):12–14.
44. Joseph N, Subba SH, Jain A, Unnikrishnan B, Nagaraj K, Kotian SM. Awareness of health personnel about lymphatic filariasis and mass drug administration in Karnataka state of South India. Australas Med J. 2011;4(2):87–93. doi:10.4066/AMJ.2011.533
45. Odermatt P, Leang R, Bin B, Bunkea T, Socheat D. Prevention of lymphatic filariasis with insecticide-treated bednets in Cambodia. Ann Trop Med Parasitol. 2008;102(2):135–142. doi:10.1179/136485908X252313
46. Pani SP, Srividya A, Krishnamoorthy K, Das PK, Dhanda V. Rapid assessment procedures (RAP) for lymphatic filariasis. Natl Med J India. 1997;10(1):19–22.
47. Pelletreau S, Nyaku M, Dembele M, et al. The field-testing of a novel integrated mapping protocol for neglected tropical diseases. PLoS Negl Trop Dis. 2011;5(11):e1380. doi:10.1371/journal.pntd.0001370
48. Pichon G, Merlin M, Fagneaux G, Riviere F, Laigret J. [Studies of the numerical distribution of microfilariae in foci of lymphatic filariasis (author‘s transl)]. Tropenmed Parasitol. 1980;31(2):165–180.
49. Adhikari RK, Sherchand JB, Mishra SR, Ranabhat K, Wagle RR. Awareness and coverage of mass drug administration for elimination of lymphatic filariasis: a community based cross sectional study in Nepal. J Community Health. 2015;40(1):30–40. doi:10.1007/s10900-014-9891-1
50. Rebollo MP, Bockarie MJ. Shrinking the lymphatic filariasis map: update on diagnostic tools for mapping and transmission monitoring. Parasitology. 2014;141(14):1912–1917. doi:10.1017/S0031182014001231
51. Schneider MC, Aguilera XP, Barbosa da Silva Junior J, et al. Elimination of neglected diseases in latin america and the Caribbean: a mapping of selected diseases. PLoS Negl Trop Dis. 2011;5(2):e964. doi:10.1371/journal.pntd.0001370
52. Singh S, Raina VK, Bora D, Dhariwal AC, Lal S. Lymphatic filariasis in Bilaspur district, Chhattisgarh. J Commun Dis. 2005;37(2):125–130.
53. Srividya A, Michael E, Palaniyandi M, Pani SP, Das PK. A geostatistical analysis of the geographic distribution of lymphatic filariasis prevalence in southern India. Am J Trop Med Hyg. 2002;67(5):480–489.
54. Steel C, Golden A, Kubofcik J, et al. Rapid Wuchereria bancrofti-specific antigen Wb123-based IgG4 immunoassays as tools for surveillance following mass drug administration programs on lymphatic filariasis. Clin Vaccine Immunol. 2013;20(8):1155–1161. doi:10.1128/CVI.00252-13
55. Sukhvir S, Bora D, Dhariwal AC, Pawan D, Shiv L. Epidemiological, clinical and entomological observations on lymphatic filariasis in urban Puri, Orissa. J Commun Dis. 2008;40(2):161–165.
56. Terranella A, Eigiege A, Gontor I, et al. Urban lymphatic filariasis in central Nigeria. Ann Trop Med Parasitol. 2006;100(2):163–172. doi:10.1179/136485906X86266
57. Triteeraprapab S, Karnjanopas K, Porksakorn C, Sai-Ngam A, Yentakam S, Loymak S. Lymphatic filariasis caused by Brugia malayi in an endemic area of Narathiwat Province, southern of Thailand. J Med Assoc Thai. 2001;84(Suppl 1):S182–8.
58. Wynd S, Carron J, Selve B, Leggat PA, Melrose W, Durrheim DN. Qualitative analysis of the impact of a lymphatic filariasis elimination programme using mass drug administration on Misima Island, Papua New Guinea. Filaria J. 2007;6:1. doi:10.1186/1475-2883-6-1
59. Yousrya M, Abdel-Hamid MIS, Kenawy M. Geographical distribution and relative abundance of culicine mosquitoes in relation to transmission of lymphatic filariasis in El Menoufia Governorate, Egypt. J Egypt Soc Parasitol. 2011;41(1):109–118.
60. Gyapong JO, Kyelem D, Kleinschmidt I, et al. The use of spatial analysis in mapping the distribution of bancroftian filariasis in four West African countries. Ann Trop Med Parasitol. 2002;96(7):695–705. doi:10.1179/000349802125001735
61. Sherchand JB, Obsomer V, Thakur GD, Hommel M. Mapping of lymphatic filariasis in Nepal. Filaria J. 2003;2(1):7. doi:10.1186/1475-2883-2-7
62. Ngwira BM, Tambala P, Perez AM, Bowie C, Molyneux DH. The geographical distribution of lymphatic filariasis infection in Malawi. Filaria J. 2007;6:12. doi:10.1186/1475-2883-6-12
63. Ruberanziza E, Mupfasoni D, Karibushi B, et al. Mapping of lymphatic filariasis in Rwanda. J Lymphoedema. 2009;4(1):20–23.
64. Sturrock HJ, Picon D, Sabasio A, et al. Integrated mapping of neglected tropical diseases: epidemiological findings and control implications for northern Bahr-el-Ghazal State, Southern Sudan. PLoS Negl Trop Dis. 2009;3(10):e537. doi:10.1371/journal.pntd.0000537
65. Iboh CI, Okon OE, Opara KN, Asor JE, Etim SE. Lymphatic filariasis among the Yakurr people of Cross River State, Nigeria. Parasit Vectors. 2012;5:203. doi:10.1186/1756-3305-5-123
66. Shawa ST, Mwase ET, Pedersen EM, Simonsen PE. Lymphatic filariasis in Luangwa District, South-East Zambia. Parasit Vectors. 2013;6(1):299. doi:10.1186/1756-3305-6-299
67. Mwase ET, Stensgaard AS, Nsakashalo-Senkwe M, et al. Mapping the geographical distribution of lymphatic filariasis in Zambia. PLoS Negl Trop Dis. 2014;8(2):e2714. doi:10.1371/journal.pntd.0002714
68. Rebollo MP, Sime H, Assefa A, et al. Shrinking the lymphatic filariasis map of Ethiopia: reassessing the population at risk through nationwide mapping. PLoS Negl Trop Dis. 2015;9(11):e0004172. doi:10.1371/journal.pntd.0004172
69. Sabesan S, Palaniyandi M, Das PK, Michael E. Mapping of lymphatic filariasis in India. Ann Trop Med Parasitol. 2000;94(6):591–606.
70. Awolola TS, Manafa OU, Idowu ET, Adedoyin JA, Adeney AK. Epidemiological mapping of lymphatic filariasis in southern Nigeria. Preliminary sury of Akinyele local govenment area. Afr J Clin Exp Microbiol. 2004;5(3):231–234.
71. Chhotray GP, Ranjit MR, Khuntia HK, Acharya AS. Precontrol observations on lymphatic filariasis & geo-helminthiases in two coastal districts of rural Orrisa. Indian J Med Res. 2005;122(5):388–394.
72. Das VN, Siddiqui NA, Kumar N, et al. A pilot study on the status of lymphatic filariasis in a rural community of Bihar. J Commun Dis. 2006;38(2):169–175.
73. Singh S, Bora D, Dhariwal AC, Singh R, Lal S. Lymphatic filariasis in rural areas of Patna District, Bihar. A challenge ahead. J Commun Dis. 2006;38(2):160–163.
74. Bonfim C, Aguiar-Santos AM, Pedroza D
75. Bonfim C, Netto MJ, Pedroza D, Portugal JL, Medeiros Z. A socioenvironmental composite index as a tool for identifying urban areas at risk of lymphatic filariasis. Trop Med Int Health. 2009;14(8):877–884. doi:10.1111/j.1365-3156.2009.02317.x
76. Kelly-Hope LA, Thomas BC, Bockarie MJ, Molyneux DH. Lymphatic filariasis in the Democratic Republic of Congo; micro-stratification overlap mapping (MOM) as a prerequisite for control and surveillance. Parasit Vectors. 2011;4:178. doi:10.1186/1756-3305-4-178
77. Brandao E, Bonfim C, Cabral D, et al. Mapping of Wuchereria bancrofti infection in children and adolescents in an endemic area of Brazil. Acta Trop. 2011;120(1–2):151–154. doi:10.1016/j.actatropica.2011.06.004
78. Brandao E, Bonfim C, Alves A, et al. Lymphatic filariasis among children and adolescents: spatial identification via socio-environmental indicators to define priority areas for elimination. Int Health. 2015;7(5):324–331. doi:10.1093/inthealth/ihv053
79. Koroma JB, Bangura MM, Hodges MH, Bah MS, Zhang Y, Bockarie MJ. Lymphatic filariasis mapping by immunochromatographic test cards and baseline microfilaria survey prior to mass drug administration in Sierra Leone. Parasit Vectors. 2012;5:10. doi:10.1186/1756-3305-5-123
80. Shiferaw W, Kebede T, Graves PM, et al. Lymphatic filariasis in western Ethiopia with special emphasis on prevalence of Wuchereria bancrofti antigenaemia in and around onchocerciasis endemic areas. Trans R Soc Trop Med Hyg. 2012;106(2):117–127. doi:10.1016/j.trstmh.2011.10.006
81. Okorie PN, Ademowo GO, Saka Y, et al. Lymphatic filariasis in Nigeria; micro-stratification overlap mapping (MOM) as a prerequisite for cost-effective resource utilization in control and surveillance. PLoS Negl Trop Dis. 2013;7(9):e2416. doi:10.1371/journal.pntd.0002416
82. Nana-Djeunga HC, Tchatchueng-Mbougua JB, Bopda J, et al. Mapping of bancroftian filariasis in cameroon: prospects for elimination. PLoS Negl Trop Dis. 2015;9(9):e0004001. doi:10.1371/journal.pntd.0004001
83. Ngwira BM, Jabu CH, Kanyongoloka H, et al. Lymphatic filariasis in the Karonga district of northern Malawi: a prevalence survey. Ann Trop Med Parasitol. 2002;96(2):137–144. doi:10.1179/0003498302125000411
84. Onapa AW, Simonsen PE, Baehr I, Pedersen EM. Rapid assessment of the geographical distribution of lymphatic filariasis in Uganda, by screening of schoolchildren for circulating filarial antigens. Ann Trop Med Parasitol. 2005;99(2):141–153. doi:10.1179/136485905X19829
85. Hassan AN, Dister S, Beck L. Spatial analysis of lymphatic filariasis distribution in the Nile Delta in relation to some environmental variables using geographic information system technology. J Egypt Soc Parasitol. 1998;28(1):119–131.
86. Gyapong JO, Remme JH. The use of grid sampling methodology for rapid assessment of the distribution of bancroftian filariasis. Trans R Soc Trop Med Hyg. 2001;95(6):681–686.
87. Medeiros Z, Bonfim C, Brandao E, et al. Using kernel density estimates to investigate lymphatic filariasis in northeast Brazil. Pathog Glob Health. 2012;106(2):113–117. doi:10.1179/2047773212Y.0000000008
88. Sime H, Deribe K, Assefa A, et al. Integrated mapping of lymphatic filariasis and podoconiosis: lessons learnt from Ethiopia. Parasit Vectors. 2014;7:397. doi:10.1186/1756-3305-7-23
89. Finn TP, Stewart BT, Reid HL, et al. Integrated rapid mapping of neglected tropical diseases in three States of South Sudan: survey findings and treatment needs. PLoS One. 2012;7(12):e52789. doi:10.1371/journal.pone.0052789
90. Stensgaard AS, Vounatsou P, Onapa AW, et al. Bayesian geostatistical modelling of malaria and lymphatic filariasis infections in Uganda: predictors of risk and geographical patterns of co-endemicity. Malar J. 2011;10:298. doi:10.1186/1475-2875-10-330
91. Slater H, Michael E. Predicting the current and future potential distributions of lymphatic filariasis in Africa using maximum entropy ecological niche modelling. PLoS One. 2012;7(2):e32202. doi:10.1371/journal.pone.0032202
92. Slater H, Michael E. Mapping, bayesian geostatistical analysis and spatial prediction of lymphatic filariasis prevalence in Africa. PLoS One. 2013;8(8):e71574. doi:10.1371/journal.pone.0071574
93. Moraga P, Cano J, Baggaley RF, et al. Modelling the distribution and transmission intensity of lymphatic filariasis in sub-Saharan Africa prior to scaling up interventions: integrated use of geostatistical and mathematical modelling. Parasit Vectors. 2015;8:560. doi:10.1186/s13071-015-1166-x
94. Gass KM, Sime H, Mwingira UJ, et al. The rationale and cost-effectiveness of a confirmatory mapping tool for lymphatic filariasis: examples from Ethiopia and Tanzania. PLoS Negl Trop Dis. 2017;11(10):e0005944. doi:10.1371/journal.pntd.0005944
95. Sime H, Gass KM, Mekasha S, et al. Results of a confirmatory mapping tool for Lymphatic filariasis endemicity classification in areas where transmission was uncertain in Ethiopia. PLoS Negl Trop Dis. 2018;12(3):e0006325. doi:10.1371/journal.pntd.0006325
96. Sabesan S, Raju KH, Subramanian S, Srivastava PK, Jambulingam P. Lymphatic filariasis transmission risk map of India, based on a geo-environmental risk model. Vector Borne Zoonotic Dis. 2013;13(9):657–665. doi:10.1089/vbz.2012.1238
97. Dhimal M, Gautam I, Kress A, Muller R, Kuch U. Spatio-temporal distribution of dengue and lymphatic filariasis vectors along an altitudinal transect in Central Nepal. PLoS Negl Trop Dis. 2014;8(7):e3035. doi:10.1371/journal.pntd.0003035
98. Chand G, Kaushal LS, Choudhari NK, Singh N. Mapping is a prerequisite for elimination of filariasis and effective targeting of filarial ‘hot spots‘. Pathog Glob Health. 2016;110(4–5):157–163. doi:10.1080/20477724.2016.1205302
99. Wijegunawardana ND, Gunawardene YI, Manamperi A, Senarathne H, Abeyewickreme W. Geographic information system (GIS) mapping of lymphatic filariasis endemic areas of Gampaha District, Sri Lanka based on epidemiological and entomological screening. Southeast Asian J Trop Med Public Health. 2012;43(3):557–566.
100. Stanton MC, Mkwanda S, Mzilahowa T, Bockarie MJ, Kelly-Hope LA. Quantifying filariasis and malaria control activities in relation to lymphatic filariasis elimination: a multiple intervention score map (MISM) for Malawi. Trop Med Int Health. 2014;19(2):224–235. doi:10.1111/tmi.12266
101. Smith EL, Mkwanda SZ, Martindale S, Kelly-Hope LA, Stanton MC. Lymphatic filariasis morbidity mapping: a comprehensive examination of lymphoedema burden in Chikwawa district, Malawi. Trans R Soc Trop Med Hyg. 2014;108(12):751–758. doi:10.1093/trstmh/tru150
102. Hochberg N, Michel MC, Lammie PJ, et al. Symptoms reported after mass drug administration for lymphatic filariasis in Leogane, Haiti. Am J Trop Med Hyg. 2006;75(5):928–932.
103. Mukhopadhyay AK, Patnaik SK, Babu PS. Status of lymphatic filariasis in parts of east Godavari district of Andhra Pradesh, India. J Vector Borne Dis. 2007;44(1):72–74.
104. Yuvaraj J, Pani SP, Vanamail P, Ramaiah KD, Das PK. Impact of seven rounds of mass administration of diethylcarbamazine and ivermectin on prevalence of chronic lymphatic filariasis in south India. Trop Med Int Health. 2008;13(5):737–742. doi:10.1111/j.1365-3156.2008.02044.x
105. Joseph H, Maiava F, Naseri T, Silva U, Lammie P, Melrose W. Epidemiological assessment of continuing transmission of lymphatic filariasis in Samoa. Ann Trop Med Parasitol. 2011;105(8):567–578. doi:10.1179/2047773211Y.0000000008
106. Tisch DJ, Alexander ND, Kiniboro B, et al. Reduction in acute filariasis morbidity during a mass drug administration trial to eliminate lymphatic filariasis in Papua New Guinea. PLoS Negl Trop Dis. 2011;5(7):e1241. doi:10.1371/journal.pntd.0001370
107. Shriram AN, Krishnamoorthy K, Sivan A, Saha BP, Kumaraswami V, Vijayachari P. Impact of MDA and the prospects of elimination of the lone focus of diurnally sub periodic lymphatic filariasis in Nicobar Islands, India. Acta Trop. 2014;133:93–97. doi:10.1016/j.actatropica.2014.02.004
108. Dewi RM, Tuti S, Ganefa S, et al. Brugia Rapid antibody responses in communities of Indonesia in relation to the results of ‘transmission assessment surveys‘ (TAS) for the lymphatic filariasis elimination program. Parasit Vectors. 2015;8:499. doi:10.1186/s13071-015-1093-x
109. Endeshaw T, Taye A, Tadesse Z, et al. Presence of Wuchereria bancrofti microfilaremia despite 7 years of annual ivermectin monotherapy mass drug administration for onchocerciasis control: a study in north-west Ethiopia. Pathog Glob Health. 2015;109(7):344–351. doi:10.1080/20477724.2015.1103501
110. Hafiz I, Graves P, Haq R, Flora MS, Kelly-Hope LA. Clinical case estimates of lymphatic filariasis in an endemic district of Bangladesh after a decade of mass drug administration. Trans R Soc Trop Med Hyg. 2015;109(11):700–709. doi:10.1093/trstmh/trv084
111. Wilson NO, Badara Ly A, Cama VA, et al. Evaluation of lymphatic filariasis and onchocerciasis in three Senegalese Districts treated for onchocerciasis with ivermectin. PLoS Negl Trop Dis. 2016;10(12):e0005198. doi:10.1371/journal.pntd.0005198
112. Mengistu B, Deribe K, Kebede F, et al. The national programme to eliminate lymphatic filariasis from Ethiopia. Ethiop Med J. 2017;55(Suppl 1):45–54.
113. Vaishnav KG, Desai HS, Srivastava PK, et al. Impact of mass drug administration on elimination of lymphatic filariasis in Surat city, India. J Commun Dis. 2012;44(4):251–259.
114. Khan AM, Dutta P, Sarmah CK, et al. Prevalence of lymphatic filariasis in a tea garden worker population of Dibrugarh (Assam), India after six rounds of mass drug administration. J Vector Borne Dis. 2015;52(4):314–320.
115. Simonsen PE, Pedersen EM, Rwegoshora RT, Malecela MN, Derua YA, Magesa SM. Lymphatic filariasis control in Tanzania: effect of repeated mass drug administration with ivermectin and albendazole on infection and transmission. PLoS Negl Trop Dis. 2010;4(6):e696. doi:10.1371/journal.pntd.0000696
116. Simonsen PE, Magesa SM, Derua YA, Rwegoshora RT, Malecela MN, Pedersen EM. Monitoring lymphatic filariasis control in Tanzania: effect of repeated mass drug administration on circulating filarial antigen prevalence in young schoolchildren. Int Health. 2011;3(3):182–187. doi:10.1016/j.inhe.2011.06.009
117. Boyd A, Won KY, McClintock SK, et al. A community-based study of factors associated with continuing transmission of lymphatic filariasis in Leogane, Haiti. PLoS Negl Trop Dis. 2010;4(3):e640. doi:10.1371/journal.pntd.0000640
118. Richards FO, Eigege A, Miri ES, et al. Epidemiological and entomological evaluations after six years or more of mass drug administration for lymphatic filariasis elimination in Nigeria. PLoS Negl Trop Dis. 2011;5(10):e1346. doi:10.1371/journal.pntd.0001370
119. Mladonicky JM, King JD, Liang JL, et al. Assessing transmission of lymphatic filariasis using parasitologic, serologic, and entomologic tools after mass drug administration in American Samoa. Am J Trop Med Hyg. 2009;80(5):769–773.
120. Farid HA, Morsy ZS, Helmy H, Ramzy RM, El Setouhy M, Weil GJ. A critical appraisal of molecular xenomonitoring as a tool for assessing progress toward elimination of lymphatic filariasis. Am J Trop Med Hyg. 2007;77(4):593–600.
121. Chu BK, Deming M, Biritwum NK, et al. Transmission assessment surveys (TAS) to define endpoints for lymphatic filariasis mass drug administration: a multicenter evaluation. PLoS Negl Trop Dis. 2013;7(12):e2584. doi:10.1371/journal.pntd.0002584
122. Srivastava PKK, Sachin G, Sunita P, et al. Elimination of lymphatic filariasis in Goa: first successful transmission assessment survey in India. J Commun Dis. 2014;46(2):7–16.
123. Biritwum NK, Garshong B, Alomatu B, de Souza DK, Gyapong M, Kyelem D. Improving drug delivery strategies for lymphatic filariasis elimination in urban areas in Ghana. PLoS Negl Trop Dis. 2017;11(5):e0005619. doi:10.1371/journal.pntd.0005619
124. Shamsuzzaman AK, Haq R, Karim MJ, et al. The significant scale up and success of transmission assessment surveys ‘TAS‘ for endgame surveillance of lymphatic filariasis in Bangladesh: one step closer to the elimination goal of 2020. PLoS Negl Trop Dis. 2017;11(1):e0005340. doi:10.1371/journal.pntd.0005340
125. Khieu V, Or V, Tep C, et al. How elimination of lymphatic filariasis as a public health problem in the Kingdom of Cambodia was achieved. Infect Dis Poverty. 2018;7(1):15. doi:10.1186/s40249-018-0394-7
126. Ojha CR, Joshi B, Kc KP, et al. Impact of mass drug administration for elimination of lymphatic filariasis in Nepal. PLoS Negl Trop Dis. 2017;11(7):e0005788. doi:10.1371/journal.pntd.0005788
127. Aye NN, Lin Z, Lon KN, et al. Mapping and modelling the impact of mass drug adminstration on filariasis prevalence in Myanmar. Infect Dis Poverty. 2018;7(1):56. doi:10.1186/s40249-018-0420-9
128. Swaminathan S, Perumal V, Adinarayanan S, Kaliannagounder K, Rengachari R, Purushothaman J. Epidemiological assessment of eight rounds of mass drug administration for lymphatic filariasis in India: implications for monitoring and evaluation. PLoS Negl Trop Dis. 2012;6(11):e1926. doi:10.1371/journal.pntd.0001926
129. Ramaiah KD, Das PK, Vanamail P, Pani SP. Impact of 10 years of diethylcarbamazine and ivermectin mass administration on infection and transmission of lymphatic filariasis. Trans R Soc Trop Med Hyg. 2007;101(6):555–563. doi:10.1016/j.trstmh.2006.12.004
130. Ramaiah KD, Vanamail P. Surveillance of lymphatic filariasis after stopping ten years of mass drug administration in rural communities in south India. Trans R Soc Trop Med Hyg. 2013;107(5):293–300. doi:10.1093/trstmh/trt011
131. Ramaiah KD, Vanamail P, Pani SP, Yuvaraj J, Das PK. The effect of six rounds of single dose mass treatment with diethylcarbamazine or ivermectin on Wuchereria bancrofti infection and its implications for lymphatic filariasis elimination. Trop Med Int Health. 2002;7(9):767–774.
132. Subramanian S, Jambulingam P, Chu BK, et al. Application of a household-based molecular xenomonitoring strategy to evaluate the lymphatic filariasis elimination program in Tamil Nadu, India. PLoS Negl Trop Dis. 2017;11(4):e0005519. doi:10.1371/journal.pntd.0005519
133. Lau CL, Won KY, Lammie PJ, Graves PM. Lymphatic filariasis elimination in American Samoa: evaluation of Molecular Xenomonitoring as a surveillance tool in the Endgame. PLoS Negl Trop Dis. 2016;10(11):e0005108. doi:10.1371/journal.pntd.0005108
134. Irish SR, Al-Amin HM, Paulin HN, et al. Molecular xenomonitoring for Wuchereria bancrofti in Culex quinquefasciatus in two districts in Bangladesh supports transmission assessment survey findings. PLoS Negl Trop Dis. 2018;12(7):e0006574. doi:10.1371/journal.pntd.0006574
135. Rao RU, Nagodavithana KC, Samarasekera SD, et al. A comprehensive assessment of lymphatic filariasis in Sri Lanka six years after cessation of mass drug administration. PLoS Negl Trop Dis. 2014;8(11):e3281. doi:10.1371/journal.pntd.0003281
136. Rao RU, Samarasekera SD, Nagodavithana KC, et al. Programmatic use of Molecular Xenomonitoring at the level of evaluation units to assess persistence of lymphatic filariasis in Sri Lanka. PLoS Negl Trop Dis. 2016;10(5):e0004722. doi:10.1371/journal.pntd.0004722
137. Drexler N, Washington CH, Lovegrove M, et al. Secondary mapping of lymphatic filariasis in Haiti-definition of transmission foci in low-prevalence settings. PLoS Negl Trop Dis. 2012;6(10):e1807. doi:10.1371/journal.pntd.0001807
138. Upadhyayula SM, Mutheneni SR, Kumaraswamy S, Kadiri MR, Pabbisetty SK, Yellepeddi VS. Filaria monitoring visualization system: a geographical information system-based application to manage lymphatic filariasis in Andhra Pradesh, India. Vector Borne Zoonotic Dis. 2012;12(5):418–427. doi:10.1089/vbz.2011.0713
139. Simonsen PE, Derua YA, Magesa SM, et al. Lymphatic filariasis control in Tanga Region, Tanzania: status after eight rounds of mass drug administration. Parasit Vectors. 2014;7:507. doi:10.1186/1756-3305-7-23
140. Lau CL, Won KY, Becker L, et al. Seroprevalence and spatial epidemiology of lymphatic filariasis in American Samoa after successful mass drug administration. PLoS Negl Trop Dis. 2014;8(11):e3297. doi:10.1371/journal.pntd.0003297
141. Graves PM, Makita L, Susapu M, et al. Lymphatic filariasis in Papua New Guinea: distribution at district level and impact of mass drug administration, 1980 to 2011. Parasit Vectors. 2013;6:7. doi:10.1186/1756-3305-6-7
142. Rebollo MP, Mohammed KA, Thomas B, et al. Cessation of mass drug administration for lymphatic filariasis in Zanzibar in 2006: was transmission interrupted? PLoS Negl Trop Dis. 2015;9(3):e0003669. doi:10.1371/journal.pntd.0003669
143.
144. Ramesh A, Cameron M, Spence K, et al. Development of an urban molecular xenomonitoring system for lymphatic filariasis in the Recife Metropolitan Region, Brazil. PLoS Negl Trop Dis. 2018;12(10):e0006816. doi:10.1371/journal.pntd.0006816
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.