Back to Journals » International Journal of Women's Health » Volume 12
Mandatory Waiting Periods Before Abortion and Sterilization: Theory and Practice
Authors Rowlands S ![]() , Thomas K
, Thomas K
Received 8 April 2020
Accepted for publication 14 July 2020
Published 31 July 2020 Volume 2020:12 Pages 577—586
DOI https://doi.org/10.2147/IJWH.S257178
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Sam Rowlands,1 Kevin Thomas2
1Department of Medical Sciences and Public Health, Faculty of Health and Social Sciences, Bournemouth University, Bournemouth, UK; 2Department of Psychology, Faculty of Science and Technology, Bournemouth University, Bournemouth, UK
Correspondence: Sam Rowlands R506, Royal London House, Christchurch Road, Bournemouth BH1 3LT, UK
Tel +44 1202 962782
Email [email protected]
Abstract: Some laws insist on a fixed, compulsory waiting period between the time of obtaining consent and when abortions or sterilizations are carried out. Waiting periods are designed to allow for reflection on the decision and to minimize regret. In fact, the cognitive processing needed for these important decisions takes place relatively rapidly. Clinicians are used to handling cases individually and tailoring care appropriately, including giving more time for decision-making. Psychological considerations in relation to the role of emotion in decision-making, eg, regret, raise the possibility that waiting periods could have a detrimental impact on the emotional wellbeing of those concerned which might interfere with decision-making. Having an extended period of time to consider how much regret one might feel as a consequence of the decision one is faced with may make a person revisit a stable decision. In abortion care, waiting periods often result in an extra appointment being needed, delays in securing a procedure and personal distress for the applicant. Some women end up being beyond the gestational limit for abortion. Those requesting sterilization in a situation of active conflict in their relationship will do well to postpone a decision on sterilization. Otherwise, applicants for sterilization should not be forced to wait. Forced waiting undermines people’s agency and autonomous decision-making ability. Low-income groups are particularly disadvantaged. It may be discriminatory when applied to marginalized groups. Concern about the validity of consent is best addressed by protective clinical guidelines rather than through rigid legislation. Waiting periods breach reproductive rights. Policymakers and politicians in countries that have waiting periods in sexual and reproductive health regulation should review relevant laws and policies and bring them into line with scientific and ethical evidence and international human rights law.
Keywords: mandatory, waiting period, psychology, decision-making, abortion, sterilization
Introduction
Waiting (cooling-off or reflection) periods are time-periods during which a person can work through their decision-making process before committing to a final decision. They are designed to be “breathing spaces” during which no external pressure is applied, thus allowing for reflection and deliberation on what might otherwise be a hurried decision and the possibility of a change of mind.
Cooling-off periods apply in the sphere of consumer protection/rights. They allow for the consumer who might be being pressured/coerced into a purchase or has signed up to what will be a legally binding contract to reflect on their decision. During this statutory time-period (15 days in the European Union), they can take advice from someone they trust and, if they regret their decision, obtain a refund/cancel a signed contract.
This paper examines waiting periods in relation to abortion and sterilization. Imposed waiting times directly affect clinical practice and service delivery. With regard to abortion, more complex decision-making in second and third trimesters is not included in this paper. For most individuals globally, sterilization is considered to be permanent; access to reversal would be beyond their reach. The purpose of this paper is to explore how decisions are made and to determine whether waiting periods have beneficial or adverse effects on those making decisions about their reproductive lives.
The scope of this paper extends from psychological judgment and decision-making theory through enacted laws to the practical effects that waiting periods have on individuals and finally to human rights. No attempt is made to tackle the complexities of the social context in which decisions are made1 nor ethical implications in any depth.
Within this paper the term woman is used. However, it is important to acknowledge that it is not only people who identify as women who need access to reproductive health services in order to maintain their health and wellbeing. Delivery of healthcare must therefore be appropriate, inclusive and sensitive to the needs of those individuals whose gender identity does not align with the sex they were assigned at birth.
Decision-Making
The Process and Its Timing
Decisions about serious matters like sterilization and abortion are not taken lightly2 without some kind of deliberation on the part of those concerned. Indeed, people in such situations engage in substantial cognitive processing of their situation — eg, weighing-up the pros and cons of the options open to them3 — before they arrive at a decision. However, the majority of women surveyed in a study by Ashton reported deciding to have an abortion shortly after discovering they were pregnant,4 suggesting that the decision-making process is quite quick. This rapidity does not preclude some quite detailed in-depth cognitive processing which has been shown to be engaged in, even under time pressure constraints.5 If decision-making about abortion and sterilization proceeds rapidly, it can mean that consulting a healthcare practitioner occurs after the decision has been made. Indeed, a sizeable majority of women sampled reported having made a decision to opt for abortion before seeing a doctor.6 It has been shown that women considering having an abortion report consulting approximately six other people, including friends, partners and medical professionals, before making their decision.4 Thus, talking to others such as family members7,8 seems to be an important factor in the decision-making process with respect to abortion. There is much more literature on decision-making before abortion than there is for sterilization. Although much of what is included below on decision-making probably applies to sterilization as well, the focus will be on how it applies to abortion.
There is extensive study and literature on how medical decisions are made in clinical consultations. Various frameworks for decision-making in medicine have been proposed. Healthcare professionals are now encouraged to involve patients more, facilitate their decision-making and share the decision(s) made.9–11 However, there appears to be nothing in these models about timing for patients — only time-pressures for clinicians.
The Role of Emotion
Given the nature of abortion, how people feel when faced with such challenging circumstances might well influence their decision-making. Indeed, studies have reported that women faced with an unintended pregnancy experience a range of emotions,12 typically negative, eg, shame and anger but also sometimes mixed with positive feelings, eg, pride and joy.13 Thus, there is a large emotional element to the process of deciding whether to have an abortion.
Psychological research suggests that decision-making in various domains such as gambling on horse races14 is influenced by emotion. For example, experiencing a positive emotional state has been found to result in less risky choices being made in gambling tasks because of not wanting to experience the negative feelings associated with losing money.15 Similarly, decision-making has been shown to differ across discrete negative emotions, with riskier decisions being associated with anger and risk-averse decisions with fear and sadness.16 Moreover, the same life events are perceived as entailing greater risk by research participants induced to feel angry than those induced to feel sad or fearful.17 Given the variety of emotions experienced by people making a decision about abortion,13 such psychological research can potentially enhance our understanding of the subject.
It is important to note, though, that risk is conceptualised in the psychological decision-making literature as essentially entailing winning or losing something and so is not the same as in the medical sphere where risk is typically viewed as the threat to health or life that medical procedures entail.18 Moreover, in the psychological literature, risk is viewed as not only applying to the decision-making activity under consideration — eg, a gambling task — but also having the potential to impact upon other areas of decision-makers’ lives.17 An example would be the risk to one’s financial lifestyle of losing a large amount of money due to taking a chance on a long-shot bet in a gambling activity.17 Thus, in the context of abortion, the psychological literature on decision-making is relevant. The risk might be perceived as the longer-term impact of having an abortion on one’s lifestyle, eg, having to put one’s career on hold due to having a child resulting from an unintended pregnancy.
Regret
Another factor that has been shown to influence decision-making is the negative emotion of regret.19 Regret can occur not only once decisions have been made and acted upon20 but also in advance of decision-making. The latter is termed “anticipated regret”, which involves trying to avoid experiencing regret as a consequence of the decision.21 This anticipated regret effect has been found in health settings ranging from organ donation decision-making to risk-taking in sexual behavior.22 For example, O’Carroll et al found that decisions to register as organ donors were more likely among non-donors who rated the extent to which they might later regret not becoming a donor relative to non-donors who were not asked about anticipated regret.23 Similarly, Bakker et al, using a longitudinal methodology, found that anticipated regret was positively associated with the actual use of condoms among university students.24 Thus, anticipated regret can influence actual health behaviors as well as decisions about future health behaviors, demonstrating its potential applicability to decisions about abortion.
The psychological literature also suggests that the wish to avoid experiencing regret can influence future decision-making.20 In the course of participants reading a scenario about parents deciding whether or not to have their child vaccinated, Reb and Connolly found that parents who collated relevant information and consulted expert sources were judged to experience less anticipated regret about their decision than those parents who made a quick decision.21 Reb and Connolly suggest that the greater deliberation afforded by collating information and consulting sources provides time to rationalize and justify the decision being made, which can ameliorate feelings of regret that might be experienced as a consequence of the decision.
Two factors have been found to influence the link between post-decisional regret and future decision-making: whether people acted or not in the decision-making situation25 and the extent to which the decision-making situation was perceived to be under their control.26 People report experiencing greater regret following both situations in which the outcome was precipitated by action rather than inaction and also those perceived to be under their control – ie, situational controllability. For example, Feldman and Albarracín25 found that observer participants reported greater regret among savers who had switched their investment to a higher-paying fund which subsequently did not yield as large a dividend as their original investment, as opposed to savers who stuck with the original investment fund. This “action effect” has been replicated several times with different stimuli.21 It is attributed to it being easier to imagine alternatives to actions rather than things that have not been done.27 Given the importance and emotionally-charged nature of abortion,12,13 decision-making could be influenced by situational controllability and considerations about whether to act or not act, resulting in differential feelings of regret that could permeate choices if similar situations are encountered in the future.
Consent
In healthcare, clinicians routinely build in time for patients to make decisions, with flexibility to tailor the length of time to the individual. The informed consent process may or may not overlap with decision-making; it ensures that a person is competent to make a particular decision, that there has been provision of relevant information and an opportunity for a full discussion about it and that the decision is being freely made, without any pressure or coercion.28–30 For anyone whose decision is not certain, more time may be needed. Mandatory waiting periods generally start after seeing the clinician who is going to carry out the procedure for the first time. Essentially, they impose an extension of the consent process. Enforced waiting periods are inflexible, not tailored to individual needs and keep people waiting who do not need extra time. The potential and actual effects caused by mandatory waiting are dealt with under the headings below.
Abortion
Abortion is often perceived as a difficult solution to a disturbing problem; the pregnancy is not necessarily regarded as unwanted.12 Many women have rehearsed the scenario of a positive pregnancy test before it happens to them.6,12 Only a minority of women are unsure about their decision by the time they present to medical services.31 Such women can be supported, counseled and given more time,32 although decisions about abortion are always taken with the “ticking clock” of advancing gestation in mind.
Waiting periods in abortion laws are generally associated with paternalistic influence.33 They imply that the decision to have an abortion carries huge moral weight — while this may be true for some people, it is not the case for everyone.34 In the USA, they are one small part of concerted efforts by social conservatives to restrict access to abortion by multiple means.35 The declared paternalistic argument is that waiting periods help women to make more reasoned decisions about their unintended pregnancy or, to put it another way, to prevent women making “rash” decisions that they will later regret.36 However, a longitudinal study showed that only 1% of women regretted their abortion five years later; throughout follow-up, relief was the predominant emotion.37 What is often underplayed is that waiting periods create significant delays.35 Literature searching for this paper did not reveal any negative effects in countries that do not have waiting periods in their abortion laws and so have more rapid access.
Waiting periods for abortion are common only in Europe and the USA (see Table 1). There are none at all in Oceania. Early examples of use of this requirement are French Law No. 75–17 in 1975 and Italian Law No. 194 in 1978, largely modelled on the French law. The French 7-day waiting period was in place for 41 years. Law No. 18.987 of 2012 in Uruguay stipulates a 5-day waiting period,38 which 70% of women seeking abortion in that country find unnecessary.39 Such retrogressive requirements contravene World Health Organization Safe Abortion Guidelines40 and jeopardise compliance with international human rights standards (see below).
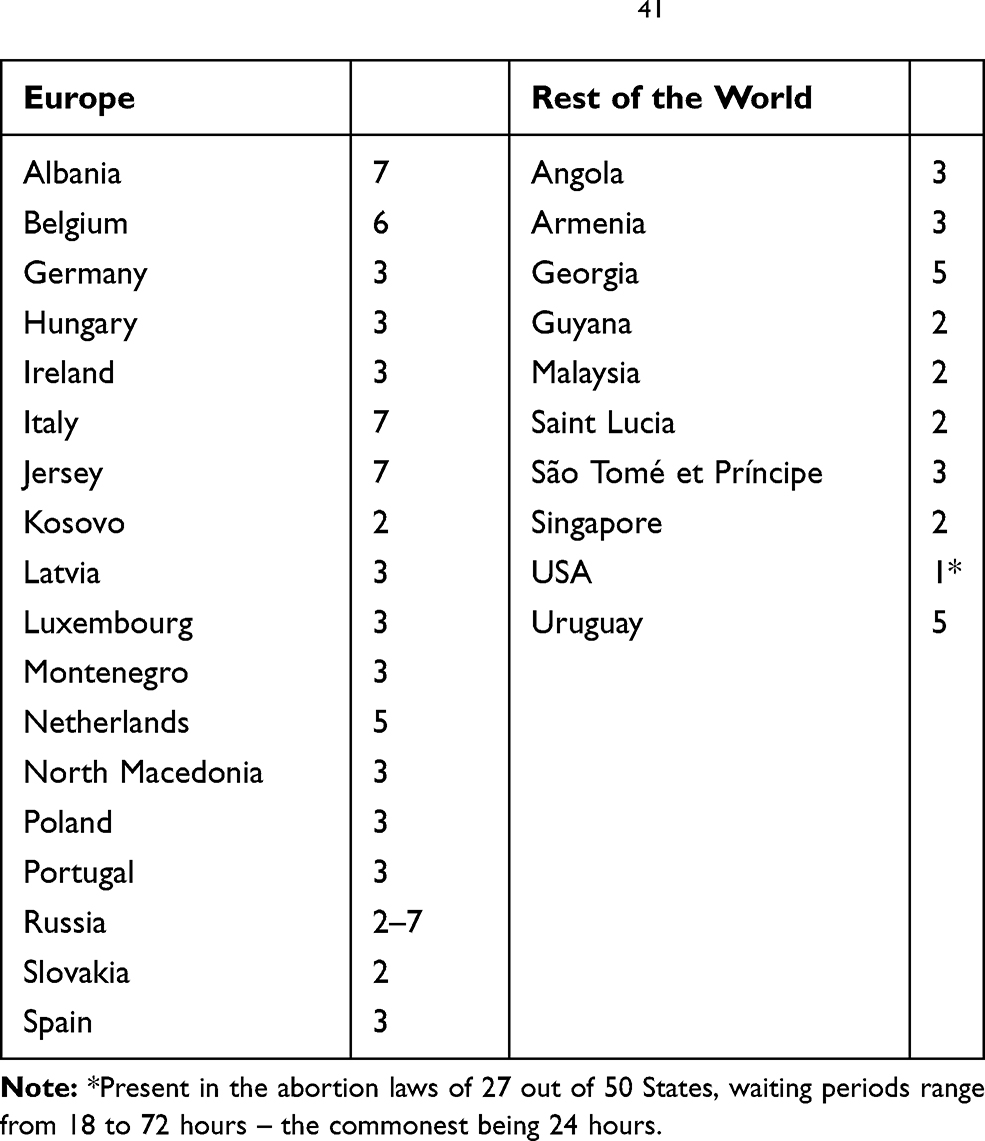 |
Table 1 Jurisdictions in Which There are Mandatory Waiting Periods for Abortion (Times are in Days)41 |
Between 1978 and 1981 — when it was struck down by the US Supreme Court — a restrictive ordinance on the delivery of abortion services in the City of Akron, Ohio operated, including a 24-hour waiting period.42 Similar laws passed at US State and local government levels have on occasions been declared unconstitutional. These collections of “informed consent” requirements were considered by the US Courts to impede the fundamental right of a woman to make the highly personal choice about whether or not to terminate a pregnancy.42 Since the Akron case, US courts have determined that “health regulations that have the purpose or effect of presenting a substantial obstacle to a woman seeking an abortion impose an undue burden”.35,43
Fourteen US State abortion laws involve an extra trip to the facility44,45 with associated travel and expense46 — in some jurisdictions, a remote consultation by telephone or some other communication medium suffices. Waiting periods generally sit alongside biased counseling laws which are ethically problematic according to every account of informed consent.47 The strictest States insist that a physician does the counselling and some even that the selfsame physician performs the procedure. This creates complex logistical problems, particularly when physicians are coming to a facility from out of State.35
In Europe, 18 jurisdictions have waiting periods built into their abortion laws (see Table 1). Ireland was the most recent country to follow this practice by including a 3-day waiting period in its Health (Regulation of Termination of Pregnancy) Act 2018.
Although Australia has never had waiting periods in abortion laws, there is clearly a strong wish in the country that it stays that way. The Victorian Law Reform Commission recommended that “any new abortion law should not contain a compulsory delay”.48 The South Australia Law Reform Institute concluded in its report on abortion that “the notion of waiting periods is inappropriate and objectionable”.49
There is a wide array of evidence on the emotional harm and practical difficulties caused by waiting periods for abortion. In the early years of US abortion provision after Roe v. Wade, 70% of 332 women interviewed in Tennessee thought that the waiting period they were experiencing was not beneficial.50 The women in this survey reported that during the wait they suffered from nausea/vomiting and mental anguish, needed to lie/make excuses for their absence and incurred extra transport and childcare costs. A more recent study in Tennessee found also that enforced waiting creates general stress for the pregnant woman and those supporting her.46 Almost one third (31%) of women in Texas reported that the waiting period there had a negative effect on their emotional wellbeing.51 Reported practical difficulties created by waiting periods include: time off work with associated loss of income, time taken and logistics of traveling, childcare needed and loss of privacy for those keeping their abortion a secret.46,52,53 In a jurisdiction with a 24-hour waiting period, 40% of women could not in fact re-attend within a week or more.54 Low-income women tend to be impacted on all fronts to a greater extent than those who are better off.53–55
Waiting periods cause delays in accessing abortion;56 abortions at higher gestations have greater morbidity and mortality.57 Waiting periods can push women into the second trimester58 or beyond legal gestational limits for abortion, denying them legitimate healthcare and in some cases forcing them into unsafe abortion or to travel to another jurisdiction.59 Detailed studies from two US States illustrate these points. Mississippi introduced a waiting period of 24 hours in 1992; this was interpreted to mean that women must attend twice in person.60 The impact of this law was lower in-State abortion rates, more abortions performed in the second trimester and more out-of-State abortions to Mississippi residents.60–63 An evaluation of the introduction of the Tennessee 48-hour waiting period in 2015 showed an increase of the proportion of second-trimester abortions in residents, from 6.6% before to 9.4% afterwards.45
A majority of women in a study in Utah were certain of their decision to have an abortion when they presented for their abortion “information visit” and their certainty was resolute despite the information visit and a 72-hour waiting period.64 The small minority whose certainty changed were conflicted before the beginning of the information visit. Roberts et al concluded that individualized counseling for the minority who are conflicted when they first attend seems more appropriate than universal requirements that create unnecessary hardships for women, the vast majority of whom have made their decision by the time they present for abortion.
Forced waiting undermines women’s agency and autonomous decision-making ability. Cook et al believe that waiting periods stereotype women contemplating abortion as impetuous, emotional and unreflective about the implications of the choices they make for their health and family wellbeing.65 These scholars also consider that such mandatory components of abortion law contribute to women’s internalization of infantilizing sexist stereotypes such that they are not fully capable of making difficult moral decisions. Such effects run contrary to the prohibition of discrimination against women enshrined in international human rights law and standards. The Irish Council for Civil Liberties, for instance, found the 2018 abortion law in Ireland to be non-rights compliant.66
Sterilization
Mandatory waiting periods for sterilization are not as common as for abortion. Waiting for a sterilization is not quite as time-sensitive as for abortion but, as decisions are often made during pregnancy, there is still the ticking-clock element for some. There has been very little research done looking for adverse effects of waiting periods on those undergoing sterilization. There appear to be no surveys of people’s views on having a compulsory wait for the operation. The only adverse effects documented have been on women who are denied postpartum sterilization because of imposed waiting periods (see below).
When they are asked to look back, women who have undergone postpartum sterilization describe an iterative decision-making process running throughout their reproductive lives.67 Most participants in this study reported being 100% certain of their decision for sterilization in the second or third trimester of pregnancy.67
The subject of sterilization needs to be set in the context of historical and continuing coercion. These abuses have often targeted marginalized groups and there has been a pervasive bias towards sterilizing women.68 Waiting periods for those considering sterilization have generally been introduced with good intentions as part of a comprehensive package with an emphasis on best practice around consent. As with abortion, the informed consent process prior to sterilization is crucial. Although someone who is uncertain of their decision may need more time, insisting that all people have an extended period between giving consent and undergoing the operation denies them prompt access to their chosen method of fertility control.
A few countries have felt it necessary to mandate a waiting period before people undergo sterilisation for the purpose of fertility control. The duration of these waiting periods is quite arbitrary. In Brazil since 1996, Law No. 9263 has regulated the practice of sterilization, stipulating a 60-day waiting period before the operation can be performed.69 This, together with a lower age limit of 25 years and two living children, was designed to minimize the chance of subsequent regret. France put a “precautionary” 4-month waiting period into its law when sterilization was legalized in 2001. In two countries, waiting periods were introduced in the wake of years of coercion. Peru set a 72-hour waiting requirement, brought in as part of a 1998 informed consent provision in guidelines introduced towards the end of the excesses of the Fujimori regime.70,71 In 2004, the Slovak Ministry of Health introduced a 72-hour waiting period following widespread targeting of Roma women for sterilization.72
In the USA, as part of 1978 guidance designed to prevent coercion, Medicaid-funded female sterilization cannot be carried out until 30 days after consent has been taken.73,74 This waiting period has been shown to work against individual autonomy, by causing delays and obstructing access to care, and to be discriminatory when applied to marginalized groups.75–77 The 1978 guidance was written with the admirable intention of protecting marginalized groups from coerced sterilization but has been shown in practice to be a barrier to access to permanent fertility control for the very same groups. Low-income women have their desire for postpartum sterilization disproportionately impeded by the waiting period.78
Discussion
The psychological literature tends to suggest that particular attention should be paid to those making decisions who are experiencing intense negative emotions such as fear or anger.17 This indicates that there may be special cases needing careful counseling. With respect to an unintended pregnancy, a woman being subjected to intimate partner violence or reproductive control might be more prone to making a decision under pressure and in haste. Nevertheless, her overwhelming priorities are going to be lack of support, her own safety and risks to a newborn child, should she choose to continue the pregnancy to term.79 With respect to sterilization, those involved in an active conflict in their relationship might do well to postpone a decision on sterilization.80 A 5-year cumulative probability study showed that women who reported substantial conflict with their husbands/partners before sterilization were significantly more likely to seek reversal.81
The psychological literature on counterfactual thinking82 indicates that the experience of previous abortions, with an element of regret in some cases, might modify subsequent behaviour. When thinking about pregnancy options, the choice that maximises a woman’s wellbeing, however, is not inevitably the choice that leaves her with no regrets.83 In practice it appears that women tend to treat pregnancies as unique life events.84,85 A previous abortion demystifies the process but does not appear to play a significant role in decision-making.84
The work of Reb and Connolly21 hints at anticipated regret— and arguably actual, experienced regret — possibly being reduced when people have greater time to make a decision. However, it must be borne in mind that Reb and Connolly21 examined participants’ perceptions of other people’s decision-making rather than their own decision-making, which limits the generalisability of the findings.21 Moreover, the “child vaccination decision” scenario Reb and Connolly used differed in terms of whether or not topic-relevant information was acquired by the depicted parents rather than the amount of time available to them to make their decision. Thus, further research that examines the effect of the passage of time on the role of anticipated — and actual — regret in people’s own decision-making is required to explore whether Reb and Connolly’s findings apply beyond scenario-reading research tasks to major life decisions like abortion.
Psychological studies about the regret people experience from comparing alternative courses of action19 may, however, speak more directly to the impact of the passage of time on decision-making about abortion. Moreover, in light of research into “counterfactual thinking”,82 — ie, mentally generating alternative, competing scenarios of the decision outcome — on balance, it is likely that the presence of waiting periods in sexual and reproductive health (SRH) will have a detrimental impact on the emotional wellbeing of those concerned which in turn may influence their decision-making. That is, having an extended period of time to possibly change their mind about their decision to have an abortion by thinking counterfactually86 about their situation may result in people having negative feelings such as anxiety at the prospect of making a decision that might be regretted in the long-run.87 In sum, it seems prudent to put greater emphasis on the impact of waiting periods on people’s emotional functioning rather than focus overly on the supposed benefit of having longer for their decision-making and their wider cognitive functioning.47 Having extended time to consider how much regret one might feel as a consequence of the decision one is faced with may make a person revisit a stable decision.
Waiting periods have been used sporadically in abortion laws/policies and to a lesser extent for sterilization. Originally, those drafting abortion laws may have been cautious due to lack of experience of such laws in action. We surmise that more recent inclusions of waiting periods may be linked to a general upsurge in anti-genderist feeling among religious fundamentalists. However, changes to a more secular society in Ireland are an exception to this trend. Waiting periods fundamentally disrespect and interfere with reproductive autonomy. They shame women as unreliable decision-makers about their own fertility.88 According to a US federal appeals court judgment, waiting period laws contradict the basic notion that “women, like all humans, are intellectual creatures with the ability to reason, consider, ponder and challenge their own ideas”.89
In contrast to financial cooling-off periods which can protect people from losing money, mandatory waiting periods in healthcare do not have health advantages. There is nothing to support the concept of blanket waiting periods between obtaining consent and the procedure for either abortion or sterilization. Such legislation applies an impersonal negative stereotype on women’s decision-making capacity. Clinicians are well-versed in treating their patients as individuals and judging when more time is needed for decision-making.90 Displacing them from exercising their judgment interferes with their ability to balance the need for deliberation and the time pressure of increasing gestation, when this applies. Fixed waiting times, by definition, result in delays to access, which in the context of abortion has particularly serious implications. Women who have made their decision want their abortion procedure as soon as possible; they find it distressing to be kept waiting.12,91,92 Adding to existing causes of delay93 is unhelpful and can be harmful. Waiting periods disproportionately affect low-income women in jurisdictions that do not have a national health service or a universal benefits system.94 Waiting periods have also been shown to fragment delivery of abortion care.95
Waiting periods in SRH contravene international human rights law which stipulates that States must remove, and refrain from enacting, laws and policies that create barriers in access to SRH services. The Committee on the Elimination of Discrimination Against Women (CEDAW) has specifically mentioned in its Country Reports on Slovakia, Hungary and Russia that waiting period requirements should be removed.59 The Committee on Economic, Social and Cultural Rights recommends in its General Comment No. 22,96 at paragraph 41, that laws and policies which act as barriers to access to SRH, such as waiting periods, should be repealed or States should refrain from enacting them in the first place. They are also universally unpopular with women undergoing abortion.39,46,50-53
Concern about the validity of consent for sterilization is best addressed by ensuring that there are adequate, protective clinical guidelines in place rather than through rigid legislation. Concerns about shorter intervals between consent and sterilization are largely misplaced. Regret is mainly associated with timing procedures at younger ages or close to a pregnancy.97 Only one study has ever shown an association between shorter consent-procedure interval and regret.98 In this Danish study, the median interval was one month in those who regretted their decision compared to three months in those who did not.98 The range of waiting times extended to 25 months, so this association is more to do with how long the study participants sat on a waiting list for their sterilization than being operated upon before they had had time to make their decision.
Also, it can be reasonably argued that the truly autonomous29 person ought to be permitted to make a decision that they might later regret, provided of course that the consent is valid.99 There is no reason to think that priority should be given to a person’s possible future wishes over and above their present wishes.
Countries making laws and policies in the area of SRH should take care with their drafting but also look at the evidence for the possible consequences of the individual clauses. States that have introduced such conditions should review them and the effects they are having on the quality of healthcare. In 2015, Catherine Coutelle, a deputy in the French National Assembly, proposed an amendment to the law, calling the waiting period “infantilizing and stigmatizing”;100 as a result, the waiting period requirement for abortion was removed in 2016. The stipulation that Ireland’s Health (Regulation of Termination of Pregnancy) Act 2018 be reviewed at the 3-year mark101 provides a window of opportunity to remedy adverse effects relating to access102 and to repeal section 12(3). Policymakers and politicians in all other countries that have waiting periods in SRH regulation should review relevant laws and policies and bring them into line with scientific and ethical evidence and international human rights law.
Acknowledgments
We thank Dr Jeffrey Wale, Senior Lecturer in Law at Bournemouth University, for comments on an earlier draft of the manuscript. We are also grateful to the two anonymous reviewers for their helpful comments. All errors remain our own.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bruch E, Feinberg F. Decision-making processes in social context. Annu Rev Sociol. 2017;43(1):207–227. doi:10.1146/annurev-soc-060116-053622
2. McLean SAM. Abortion law: is consensual reform possible? in: McLean SAM, editor. Medical Law and Ethics. Abingdon: Routledge; 2018:249–266.
3. Kahneman D, Tversky A. The psychology of preferences. Sci Am. 1982;246(1):160–173. doi:10.1038/scientificamerican0182-160
4. Ashton J. Patterns of discussion and decision-making amongst abortion patients. J Biosoc Sci. 1980;12(3):247–259. doi:10.1017/s0021932000012797
5. Evans JSBT, Curtis-Holmes J. Rapid responding increases belief bias: evidence for the dual-process theory of reasoning. Think Reason. 2005;11(4):382–389. doi:10.1080/13546780542000005
6. Rowlands S. The decision to opt for abortion. J Fam Plann Reprod Health Care. 2008;34(3):175–180. doi:10.1783/147118908784734765
7. Lee E, Clements S, Ingham R, et al. A Matter of Choice? Explaining National Variation in Teenage Abortion and Motherhood. York: Joseph Rowntree Foundation; 2004.
8. Ekstrand M, Tydén T, Darj E, et al. An illusion of power: qualitative perspectives on abortion decision-making among teenage women in Sweden. Perspect Sex Reprod Health. 2009;41(3):173–180. doi:10.1363/4117309
9. Entwistle VA, Cribb A, Watt IS. Shared decision-making: enhancing the clinical relevance. JRSM. 2012;105(10):416–421. doi:10.1258/2Fjrsm.2012.120039
10. NICE. Shared Decision Making. London: National Institute for Health and Care Excellence; 2020. Available from: https://www.nice.org.uk/about/what-we-do/our-programmes/nice-guidance/nice-guidelines/shared-decision-making.
11. Yahanda AT, Mozersky J. What’s the role of time in shared decision making? AMA J Ethics. 2020;22(5):E416–422. doi:10.1001/amajethics.2020.416
12. Freeman EW. Abortion: subjective attitudes and feelings. Fam Plann Perspect. 1978;10(3):150–155. doi:10.2307/2134301
13. Kero A. Psychosocial factors in women requesting abortion. In: Rowlands S, editor. Abortion Care. Cambridge: Cambridge University Press; 2014:34–41.
14. Cahir C, Thomas K. Asymmetric effects of positive and negative affect on decision making. Psychol Rep. 2010;106(1):193–204. doi:10.2466/PR0.106.1.193-204
15. Isen AM, Geva N. The influence of positive affect on acceptable level of risk: the person with a large canoe has a large worry. Organ Behav Hum Decis Process. 1987;39(2):145–154. doi:10.1016/0749-5978(87)90034-3
16. Lerner JS, Tiedens LZ. Portrait of the angry decision maker: how appraisal tendencies shape anger’s influence on cognition. J Behavioral Decision Making. 2006;19(2):115–137. doi:10.1002/bdm.515
17. Lerner JS, Keltner D. Fear, anger, and risk. J Personality Soc Psychol. 2001;81(1):146–159. doi:10.1037//0022-3514.81.1.146
18. RCOG. Understanding How Risk is Discussed in Healthcare. London: Royal College of Obstetricians and Gynaecologists; 2015.
19. Connolly T, Zeelenberg M. Regret in decision-making. Curr Dir Psychol Sci. 2002;11(6):212–216. doi:10.1111/1467-8721.00203
20. Pieters R, Zeelenberg M. On bad decisions and deciding badly: when intention–behavior inconsistency is regrettable. Organ Behav Hum Decis Process. 2005;97(1):18–30. doi:10.1016/j.obhdp.2005.01.003
21. Reb J, Connolly T. The effects of action, normality, and decision carefulness on anticipated regret: evidence for a broad mediating role of decision justifiability. Cogn Emot. 2010;24(8):1405–1420. doi:10.1080/02699930903512168
22. Richard R, van der Pligt J, de Vries N. Anticipated regret and time perspective: changing sexual risk-taking behavior. J Behavioral Decision Making. 1996;9(3):185–199. doi:10.1002/(SICI)1099-0771(199609)9:3<185::AID-BDM228>3.0.CO;2-5
23. O’Carroll RE, Dryden J, Hamilton-Barclay T, et al. Anticipated regret and organ donor registration - a pilot study. Health Psychol. 2011;30(5):661–664. doi:10.1037/a0024182
24. Bakker AB, Buunk BP, Manstead ASR. The moderating role of self-efficacy beliefs in the relationship between anticipated feelings of regret and condom use. J Applied Social Psychol. 1997;27(22):2001–2014. doi:10.1111/j.1559-1816.1997.tb01637.x
25. Feldman G, Albarracín D. Norm theory and the action-effect: the role of social norms in regret following action and inaction. J Experiment Soc Psychol. 2017;69:111–120. doi:10.1016/j.jesp.2016.07.009
26. Roese NJ, Olson JM. Outcome controllability and counterfactual thinking. Pers Soc Psychol Bull. 1995;21(6):620–628. doi:10.1177/0146167295216008
27. Kahneman D, Miller DT. Norm theory: comparing reality to its alternatives. Psychol Review. 1986;93(2):136–153. doi:10.1037/0033-295X.93.2.136
28. Beauchamp TL, Childress JF. Principles of Biomedical Ethics.
29. McLean SAM. Autonomy, Consent and the Law. Abingdon: Routledge-Cavendish; 2010.
30. Chan SW, Tulloch E, Cooper ES, et al. Montgomery and informed consent: where are we now? BMJ. 2017;357:j2224. doi:10.1136/bmj.j2224
31. Foster DG, Gould H, Taylor J, et al. Attitudes and decision making among women seeking abortions in one U.S. clinic. Perspect Sex Reprod Health. 2012;44(2):117–124. doi:10.1363/4411712
32. Kjelsvik M, Sekse RJT, Moi AL, et al. Women’s experiences when unsure about whether or not to have an abortion in the first trimester. Health Care Women Int. 2018;39(7):784–807. doi:10.1080/07399332.2018.1465945
33. Mayans I, Vaca M. The paternalistic argument against abortion. Hypatia. 2018;33(1):22–39. doi:10.1111/hypa.12385
34. O’Shaughnessy A. A race against the ‘body clock’: abortion and the temporal politics of the ‘waiting period’: reproductive Sociology Research Group; 2019 Available from: http://www.reprosoc.com/blog/2019/11/20/a-race-against-the-body-clock-abortion-and-the-temporal-politics-of-the-waiting-period. A
35. Cohen DS, Joffe C. Obstacle Course: The Everyday Struggle to Get an Abortion in America. Oakland: University of California Press; 2020.
36. Klick J. Mandatory waiting periods for abortions and female mental health. Health Matrix. 2006;16(1):183–208.
37. Rocca CH, Samari G, Foster DG, et al. Emotions and decision rightness over five years following an abortion: an examination of decision difficulty and abortion. Soc Sci Med. 2020. doi:10.1016/j.socscimed.2019.112704
38. Pizzarossa LB. Legal barriers to access abortion services through a human rights lens: the Uruguayan experience. Reprod Health Matters. 2018;26(52):151–158. doi:10.1080/09688080.2017.1422664
39. Makleff S, Labandera A, Chiribao F, et al. Experience obtaining legal abortion in Uruguay: knowledge, attitudes, and stigma among abortion clients. BMC Women’s Health. 2019;19(1):155. doi:10.1186/s12905-019-0855-6
40. WHO. Safe Abortion: Technical and Policy Guidance for Health Systems.
41. WHO. Global Abortion Policies Database. Geneva: World Health Organization; 2018. Available from: https://abortion-policies.srhr.org.
42. Thomas TA. Back to the future of regulating abortion in the first term. Wisconsin J Law Gender Soc. 2014;29(1):47–86.
43. Anonymous. Whole Woman’s Health v. Hellerstedt. Harv Law Rev. 2016;130:397–406.
44. Anonymous. Counseling and Waiting Periods for Abortion. New York: Guttmacher Institute; 2020. Available from: https://www.guttmacher.org/state-policy/explore/counseling-and-waiting-periods-abortion.
45. Lindo JM, Pineda-Torres M. New evidence on the effects of mandatory waiting periods for abortion. Working Papers. Cambridge, MA: National Bureau of Economic Research; 2019.
46. Rouland RS, Ely GE, Caron A. Abortion patient experiences of the forty-eight-hour waiting period policy in Tennessee. J Appalachian Studies. 2019;25(1):87–104. doi:10.5406/jappastud.25.1.0087
47. Vandewalker I. Abortion and informed consent: how biased counseling laws mandate violations of medical ethics. Michigan J Gender Law. 2012;19(1):1–70.
48. VLRC. Law of Abortion: Final Report. Melbourne: Victorian Law Reform Commission; 2008.
49. Williams J, Plater D, Brunacci A, et al. Abortion: A Review of South Australian Law and Practice. Adelaide: South Australian Law Reform Institute; 2019.
50. Lupfer M, Silber BG. How patients view mandatory waiting periods for abortion. Fam Plann Perspect. 1981;13(2):75–79. doi:10.2307/2134696
51. Texas Policy Evaluation Project. Impact of Abortion Restrictions in Texas Austin. University of Texas, Ibis Reproductive Health, University of Alabama; 2013. Available from: https://liberalarts.utexas.edu/txpep/_files/pdf/TxPEP-ResearchBrief-ImpactofAbortionRestrictions.pdf.
52. Sanders JN, Conway H, Jacobson J, et al. The longest wait: examining the impact of Utah’s 72-hour waiting period for abortion. Women’s Health Issues. 2016;26(5):483–487. doi:10.1016/j.whi.2016.06.004
53. Karasek D, Roberts SCM, Weitz TA. Abortion patients’ experience and perceptions of waiting periods: survey evidence before Arizona’s two-visit 24-hour mandatory waiting period law. Women’s Health Issues. 2016;26(1):60–66. doi:10.1016/j.whi.2015.10.004
54. White K, Turan JM, Grossman D. Travel for abortion services in Alabama and delays in obtaining care. Women’s Health Issues. 2017;27(5):523–529. doi:10.1016/j.whi.2017.04.002
55. Roberts SC, Turok DK, Belusa E, et al. Utah’s 72-hour waiting period for abortion: experiences among a clinic-based sample of women. Perspect Sex Reprod Health. 2016;48(4):179–187. doi:10.1363/48e8216
56. Jones RK, Jerman J. Time to Appointment and Delays in Accessing Care Among U.S. Abortion Patients. New York: Guttmacher Institute;2016. Available from: https://www.guttmacher.org/report/delays-in-accessing-care-among-us-abortion-patients.
57. Zane S, Creanga AA, Berg CJ, et al. Abortion-related mortality in the United States: 1998–2010. Obstet Gynecol. 2015;126(2):258–265. doi:10.1097/AOG.0000000000000945
58. Bitler M, Zavodny M. The effect of abortion restrictions on the timing of abortions. J Health Economics. 2001;20(6):1011–1032. doi:10.1016/s0167-6296(01)00106-0
59. Hoctor L, Lamačková A. Mandatory waiting periods and biased abortion counseling in Central and Eastern Europe. Int J Gynecol Obstet. 2017;139(2):253–258. doi:10.1002/ijgo.12288
60. Joyce T, Henshaw SK, Skatrud JD. The impact of Mississippi’s mandatory delay law on abortions and births. JAMA. 1997;278(8):653–658. doi:10.1001/jama.1997.03550080063040
61. Joyce T, Kaestner R. The impact of Mississippi’s mandatory delay law on the timing of abortion. Fam Plann Perspect. 2000;32(1):4–13. doi:10.2307/2648143
62. Joyce T, Kaestner R. The impact of mandatory waiting periods and parental consent laws on the timing of abortion and State of occurrence among adolescents in Mississippi and South Carolina. J Policy Anal Manage. 2001;20(2):263–282. doi:10.1002/pam.2025
63. Althaus FA, Henshaw SK. The effects of mandatory delay laws on abortion patients and providers. Fam Plann Perspect. 1994;26(5):
64. Roberts SCM, Turok DK, Belusa E, et al. Do 72-hour waiting periods and two-visit requirements for abortion affect women’s certainty? A prospective cohort study. Women’s Health Issues. 2017;27(4):400–406. doi:10.1016/j.whi.2017.02.009
65. Cook RJ. Stigmatized meanings of criminal abortion law. In: Cook RJ, Erdman JN, Dickens BM, editors. Abortion Law in Transnational Perspective. Philadelphia: University of Pennsylvania Press; 2014:347–369.
66. Anonymous. ICCL Says 3-Day Abortion Waiting Period Not Rights-Compliant. Dublin: Irish Council for Civil Liberties; 2018. Available from: https://www.iccl.ie/equality/3-day-abortion-waiting-period-not-rights-compliant/.
67. Foley O, Janiak E, Dutton C. Women’s decision making for postpartum sterilization: does the Medicaid waiting period add value? Contraception. 2018;98(4):312–316. doi:10.1016/j.contraception.2018.07.004
68. Rowlands S, Amy J-J. Involuntary sterilisation: we still need to guard against it. BMJ Sex Reprod Health. 2018;44(4):239–241. doi:10.1136/bmjsrh-2018-200119
69. Soares LC, Brollo JLA. Family planning in Brazil: why not tubal sterilisation during childbirth? J Med Ethics. 2013;39(11):710–712. doi:10.1136/medethics-2012-101142
70. León FR. Peru: Providers’ Compliance with Quality of Care Norms. New York: Population Council; 1999.
71. Serra AM. (Forced) Sterilization in Peru: power and narrative configurations. Rev Antropol Iberoamericana. 2017;12(1):31–52. doi:10.11156/aibr.120103e
72. Zampas C, Barot S, Bukovska B. Body and Soul: Forced Sterilization and Other Assaults on Roma Reproductive Freedom in Slovakia. New York: Center for Reproductive Rights/Poradna; 2003.
73. Rowlands S, Wale J. Sterilisations at delivery or after childbirth: addressing continuing abuses in the consent process. Glob Public Health. 2019;14(8):1153–1166. doi:10.1080/17441692.2019.1583265
74. Amy J-J, Rowlands S. Legalised non-consensual sterilisation - Eugenics put into practice before 1945, and the aftermath. Part 1: USA, Japan, Canada and Mexico. Eur J Contracept Reprod Health Care. 2018;23(2):121–129. doi:10.1080/13625187.2018.1450973
75. Borrero S, Zite N, Creinin MD. Federally funded sterilization: time to rethink policy? AJPH. 2012;102(10):1822–1825. doi:10.2105/2FAJPH.2012.300850
76. Moaddab A, McCullough LB, Chervanak FA, et al. Health care justice and its implications for current policy of a mandatory waiting period for elective tubal sterilization. AJOG. 2015;212(6):736–739. doi:10.1016/j.ajog.2015.03.049
77. Batra P, Rodriguez K, Cheney AM. Using deliberative and qualitative methods to recommend revisions to the Medicaid sterilization waiting period. Women’s Health Issues. 2020;30(4):260–267. doi:10.1016/j.whi.2020.04.001
78. Potter JE, White K, Hopkins K, et al. Frustrated demand for sterilization among low-income Latinas in El Paso, Texas. Perspect Sex Reprod Health. 2012;44(4):228–235. doi:10.1363/4422812
79. Côté I, Lapierre S. Abortion and domestic violence: women’s decision-making process. Affilia. 2014;29(3):285–297. doi:10.1177/2F0886109913519791
80. ACOG. Sterilization of Women: Ethical Issues and Considerations. Committee Opinion No. 695. Washington DC: American College of Obstetricians and Gynecologists; 2017.
81. Jamieson DJ, Kaufman SC, Costello C, et al. A comparison of women’s regret after vasectomy versus tubal sterilization. Obstet Gynecol. 2002;99(6):1073–1079. doi:10.1016/s0029-7844(02)01981-6
82. Smallman R, Roese NJ. Counterfactual thinking facilitates behavioral intentions. J Experiment Soc Psychol. 2009;45(4):845–852. doi:10.1016/j.jesp.2009.03.002
83. Greasley K. Abortion and regret. J Med Ethics. 2012;38(12):705–711. doi:10.1136/medethics-2012-100522
84. LaRoche KJ, Foster AM. Exploring Canadian women’s multiple abortion experiences: implications for reducing stigma and improving patient-centred care. Women’s Health Issues. 2018;28(4):327–332. doi:10.1016/j.whi.2018.04.002
85. Weitz TA, Kimport K. A need to expand our thinking about “repeat” abortions. Contraception. 2012;85(4):408–412. doi:10.1016/j.contraception.2011.09.003
86. Roese NJ. Counterfactual thinking. Psychol Bull. 1997;121(1):133–148. doi:10.1037/0033-2909.121.1.133
87. Gilovich T, Medvec VH. The experience of regret: what, when, and why. Psychol Review. 1995;102(2):379–395. doi:10.1037/0033-295x.102.2.379
88. Olund E. Repealing a ‘legacy of shame’: press coverage of emotional geographies of secrecy and shame in Ireland’s abortion debate. In: Browne K, Calkin S, editors. After Repeal: Rethinking Abortion Politics. London: Zed Books; 2020:174–188.
89. Court of Appeals for the 7th Circuit. Planned Parenthood of Indiana and Kentucky v. Commissioner of the Indiana State Department of Health; 2018.
90. Montomery K. How Doctors Think: Clinical Judgment and the Practice. New York: Oxford University Press; 2006.
91. Wiebe ER, Sandhu S. Access to abortion: what women want from abortion services. J Obstet Gynaecol Can. 2008;30(4):327–331. doi:10.1016/S1701-2163(16)32801-8
92. Steinberg JR, Tschann JM, Furgerson D, et al. Psychosocial factors and pre-abortion psychological health: the significance of stigma. Soc Sci Med. 2016;150:67–75. doi:10.1016/j.socscimed.2015.12.007
93. Foster DG, Jackson RA, Cosby K, et al. Predictors of delay in each step leading to an abortion. Contraception. 2008;77(4):289–293. doi:10.1016/j.contraception.2007.10.010
94. Shepherd L, Turner HD. The over-medicalization and corrupted medicalization of abortion and its effect on women living in poverty. J Law Med Ethics. 2018;46(3):672–679. doi:10.1177/1073110518804222
95. Donnelly M, Murray C. Abortion care in Ireland: developing legal and ethical frameworks for conscientious provision. Int J Gynecol Obstet. 2020;148(1):127–132. doi:10.1002/ijgo.13025
96. General comment No. 22 (2016) on the right to sexual and reproductive health (article 12 of the International Covenant on Economic, Social and Cultural Rights): United Nations, 2016.
97. Clinical Effectiveness Unit. Male and Female Sterilisation. London: Faculty of Sexual and Reproductive Healthcare; 2014.
98. Thranov I, Kjersgaard AG, Rasmussen OV, et al. Regret among 547 Danish sterilized women. Scand J Soc Med. 1988;16(1):41–48. doi:10.1177/140349488801600107
99. McQueen P. Autonomy, age and sterilisation requests. J Med Ethics. 2017;43(5):310–313. doi:10.1136/medethics-2016-103664
100. Béguin F, Dupont G. IVG: Le délai de réflexion supprimé. Le Monde; March 19, 2015.
101. Reddy LM, Nolan A. Bill Digest: Health (Regulation of Termination of Pregnancy) Bill. Vol. 2018. Dublin: Houses of the Oireachtas; 2018.
102. Carnegie A, Roth R. From the grassroots to the Oireachtas. Health & Human Rights J. 2019;21(2):109–120.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.