Back to Journals » International Journal of Women's Health » Volume 18
Managing Vaginismus with Assisted Dilatation Multidisciplinary Protocol – Retrospective Cohort Study from Indonesia’s Largest Dedicated Centre
Authors Wicaksono RA, Gunawan E ![]() , Fitriansari S, Pacik PT, Tjandraprawira KD
, Fitriansari S, Pacik PT, Tjandraprawira KD
Received 16 December 2025
Accepted for publication 4 March 2026
Published 11 March 2026 Volume 2026:18 580236
DOI https://doi.org/10.2147/IJWH.S580236
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Vinay Kumar
Robbi Asri Wicaksono,1 Elvine Gunawan,2,3 Santy Fitriansari,1 Peter T Pacik,4 Kevin Dominique Tjandraprawira1
1Department of Obstetrics and Gynecology, Limijati Women and Children Hospital, Bandung, Indonesia; 2Department of Psychiatry, Limijati Women and Children Hospital, Bandung, Indonesia; 3Doctoral Program in Medical Science, Faculty of Medicine, Universitas Padjadjaran, Bandung, Indonesia; 4Retired Scholar, Dunbarton, New Hampshire, USA
Correspondence: Robbi Asri Wicaksono, Department of Obstetrics and Gynecology, Limijati Women and Children Hospital, Jalan LLRE Martadinata No. 39, Bandung, 40115, Indonesia, Email [email protected]
Background: Vaginismus is a gynecologic disorder with persistent vaginal spasm whenever any penetration is attempted. This leads to a failure of penetration. Vaginismus’ true prevalence is unknown and reporting heavily biased. A similar condition is happening in Indonesia, where our facility treats > 200 new cases/year. No standardized vaginismus treatment protocol is available internationally, so this retrospective study evaluates our multidisciplinary assisted dilatation protocol and the obstetric outcomes of our patients.
Methods: This is a retrospective cohort study of all patients presenting with vaginismus undergoing assisted dilatation between 01/01/2022 and 31/12/2023. Diagnosis is through the presence of vaginal muscle spasms precluding penetration and/or severe penetrative pain, as confirmed by history and physical examination. We included all patients undergoing assisted dilatation in this timeframe. We employed a standardised multidisciplinary approach involving gynaecologist, psychiatrist and specialist nurses. It combines botulinum toxin A injections, dilator exercises and psychiatric medications. Patients are followed up 6– 8 weeks post-dilatation and their obstetric outcomes are recorded through an online questionnaire.
Results: We included 513 patients. 85.4% (438/513) presented due to failure of penetration. The average age at consultation was 30.39 ± 4.75 years. Most patients came from the island of Java (76.8%; 394/513), were undergraduates (83.3%; 309/371) and worked in the private sector (49.5%; 254/513). The median duration of vaginismus prior to presenting for treatment was 36 months (range 1– 252 months). 45.8% (235/315) had experienced medical trauma previously, 46.6% (239/513) had marital trauma and 56.7% (291/513) had social trauma. 61.2% (314/513) attended follow-up and 89.4% (281/314) achieved penetration post-discharge. 23.7% (52/219) displayed involuntary movements during follow-up examination. Patients required a median of 4 weeks to achieve penetration and most achieved penetration at 1st attempt. 51% (159/312) reported pregnancy post-procedure with 85.1% (120/141) achieving it spontaneously. 9.2% (13/141) experienced splash pregnancies. 88% (102/116) of pregnancies were term but 94.2% (98/104) opted for caesarean section.
Conclusion: Our assisted dilatation protocol, emphasizing on both multidisciplinary and multimodal approach, may be offered for standardized vaginismus treatment.
Keywords: vaginismus, assisted dilatation, multidisciplinary, botulinum toxin
Introduction
Vaginismus is a gynaecologic disorder with persistent vaginal closure when any form of penetration is attempted, whether by a penis, finger, tampon or speculum.1,2 This often makes vaginal penetration during intercourse extremely difficult if not impossible.1 Additionally, this condition precludes transvaginal gynaecological examination.3 Unfortunately, vaginismus is often retreated to the silent corners of discussion, which makes its true prevalence practically unknown.3 A Danish study put vaginismus prevalence at less than 1% of general female population.1 Studies ranging from Africa to the Middle East have put the prevalence at a wider range, between 7 and 68%.1,4–7 As such, the true prevalence may remain unknown as guilt, shame and secrecy continue to confine vaginismus into the dark.1
Vaginismus’ etiology is still debated, and vaginismus remains a taboo for many couples in many parts of the world. Many healthcare professionals also struggle to discuss vaginismus openly.8 They have cited lack of training and communication skills to engage in vaginismus treatment.8 A similar situation is present in Indonesia, where the authors are based. The Indonesian population is mostly a conservative country with strong religious backgrounds shaping the general mindset of the population, including on family ideals and sexual practices.9,10 There is a strong emphasis on married couples to reach the family ideal of having offspring(s) of their own and so, sexual issues including infertility and penetration difficulties tend to be sidelined.10–12 Despite the presence of a dedicated support group (Vaginismus Indonesia at www.vaginismusindonesia.com), vaginismus has persisted as a cultural taboo, which has not helped in determining its disease burden.
Vaginismus management is a challenge due to a lack of standardized protocol internationally. A variety of treatments, including pelvic floor physiotherapy, vaginal dilators, muscle relaxants (eg. nitroglycerin ointment and botulinum toxin), and cognitive behavioral therapy has been offered with varying levels of efficacy.13 The latest review highlighted the many options of treatment but the lack of gold-standard management recommendation.14 Trials often struggle with small number of patients, as highlighted by the relatively small number of total patients (863 total patients) across 18 studies, averaging <50 patients per study.14 Additionally, vaginismus is associated with adverse obstetrical outcomes as vaginismus patients have a significantly increased rates of elective caesarean sections upon maternal requests, thereby exposing them to potential complications during and after the surgery.15
Our facility has spearheaded vaginismus care in Indonesia since starting the nation’s first vaginismus-dedicated clinic in 2017.16 We have consistently cared for >200 new vaginismus patients per year, including during the COVID-19 pandemic. At our facility, we have adopted a multidisciplinary approach for vaginismus treatment, in which a dedicated team of consultant gynecologist, consultant psychiatrist, anesthesiologist and specialist nurses are involved. Such approach is necessary as vaginismus patients often present with a psychiatric/mental health comorbidity alongside their gynaecological complaint. Thus, in this retrospective research, we are evaluating our own protocol and would like to present our results, in the hope of other centers adopting a similar holistic approach for the benefit of vaginismus patients. This study, emphasizing a multidisciplinary and multimodal approach, is aimed to evaluate the clinical and obstetric outcomes of patients following our assisted dilatation protocol for vaginismus at Indonesia’s largest dedicated center.
Materials and Methods
This is a retrospective cohort study involving all patients undergoing assisted dilatation for vaginismus at a private women and children’s hospital in Bandung, Indonesia. We recruited all patients presenting with vaginismus that underwent assisted dilatation between 1 January 2022 and 31 December 2023. We opted for total sampling of patients as it was feasible. We also included patients that might have presented earlier than 1 January 2022 for their initial consultation but only opted for the procedure within the study timeframe. We followed patients after their discharge on their follow-up visit(s) to the hospital and should they not present themselves again, we provided an online questionnaire for them to fill, with details on their current state, any symptoms and subsequent reproductive history. Our exclusion criteria:
In our hospital, we have introduced a management protocol for vaginismus called assisted dilatation procedure. This protocol is a modification of Pacik et al’s original multimodal protocol.17–19 Assisted dilatation procedure is a sequence of multidisciplinary medical procedures with the objective of producing adequate self-vaginal dilatation that is worthwhile, humane, trauma-free and progress in vaginal penetration that is trouble-free. This procedure mimics the mechanical stretching of vagina, providing exposure and understanding to the patient of what a successful vaginal penetration should be like.20 In addition, it has a psychological benefit of lessening post-traumatic stress disorder (PTSD) and phobias due to vaginismus.21 For this reason, we have instituted the involvement of a consultant psychiatrist who is deeply concerned with vaginismus from the very beginning of care, as we often encounter vaginismus patients with co-existing mental health disorders from their experience with vaginismus. The protocol up to the procedure is as follows:
- Presenting patient with signs and symptoms of vaginismus is seen by the consultant gynecologist. Diagnosis is based on characteristic patient history of involuntary vaginal spasms, precluding penetration or causing severe vaginal pain, confirmed through physical examination.
- After the diagnosis is confirmed, a reflex consultation with the consultant psychiatrist is offered for an assessment of their quality of life (QoL), mental health condition, trauma-triggering events and pain-related trauma, marital wellbeing and sexual wellbeing. Should the patient refuse such consultation, it is noted down in the patient electronic case notes.
- The patient is offered a treatment with assisted dilatation usually at the following day. If the patient agrees, then she is admitted to the gynaecology ward and started on psychiatric medications consisting of anti-depressant (serotonin selective reuptake inhibitors) and anti-psychotic medications at low dosages.
- On the day of the procedure, patient is transported to the operating theatre.
- Patient is given TIVA (total intravenous anaesthesia) before being positioned to lithotomy.
- After positioning to lithotomy, any involuntary movements on the patient’s buttocks, thighs, legs and hands are noted. If such involuntary movements are noted, an increase in the TIVA dose will be administered by the anaesthetist in charge.
- The combination of anaesthetic drugs is at the discretion of the anaesthetist. For pre-induction, generally midazolam is used. For induction and maintenance, any of the following drugs may be used singly or in combination: propofol, sodium thiopenthal, fentanyl or sevoflurane.
- The procedure is started by inserting a speculum into the vagina to allow for inspection of the vagina and the cervix.
- Type A Botulinum toxin is then injected for a total dose of 100 IU. 50 IU of botulinum toxin is injected into the right bulbospongiosus muscle at 7–9 o’clock direction. Another 50 IU of botulinum toxin is injected into the left bulbospongiosus muscle at 3–5 o’clock direction.
- A injection of local anaesthetic mixture composed of bupivacaine and epinephrine is given to the right and left lateral walls of the vagina. This is to ensure that the patient wakes up with minimal pain and is comfortable with the largest possible dilator inside her vagina. Injections on the anterior and posterior walls of the vagina are avoided to prevent incontinence.
- Progressive dilatation is carried out by inserting the largest possible dilator according to the vagina’s capacity (#6 or #7), accompanied by digital evaluation.
- Procedure is concluded by a bimanual examination and continuous dilator application.
- The patient is transferred to the recovery room where her vital signs are monitored continuously.
- After patient fully regains her consciousness, re-evaluation is carried out. In the absence of complicating factors, eg. excessive hemorrhage, patient is transferred back to the gynaecology ward.
The following protocol concerns the patient in the gynaecology ward and her subsequent follow-up visits:
- Patient is transferred to a private room in the gynaecology ward. In our facility, vaginismus patients are treated in private en-suite rooms.
- With the nurse’s assistance, patient is asked to remove the dilator from her vagina and requested to urinate.
- Patient is guided to perform self-dilatation under the supervision of the consultant gynaecologist (RAW). She will independently hold, control, insert, remove, and rotate the dilator, without any physical intervention from anyone including the consultant gynaecologist. The supervision provided is mediated only through verbal instructions and encouragement without any physical intervention.
- Throughout this process, the consultant gynaecologist performs a continuous assessment of the patient’s overall condition, ie. anxiety, eye contact, involuntary physical movements, mechanical process of dilatation, the patient’s ability to control and coordinate her limbs, the patient’s concentration, initiative and ability to follow instructions.
- Once adequate self-dilatation is achieved, patient is considered able to continue dilatation. She is provided a guided checklist for continuing self-dilatation for the next 24 hours. During her self-dilatation, patient is asked to perform the procedure by herself, without the intrusion or the assistance of her partner and/or nursing staff.
- In general, patients are admitted for at least 24 hours after starting the self-dilatation procedure. However, if required from the consultant’s assessment, the patient’s stay may be extended for another day.
- Patient is provided with another consultation with the consultant psychiatric whilst in the ward. Top up dosages of psychiatric medication (eg. Selective serotonin reuptake inhibitors/SSRIs or D2-antagonists) are provided at the clinician’s discretion.
- Patient is provided with information on continuing her practice at home after discharge, the dos and don’ts and the expected follow-up appointment at the gynaecology clinic.
- After discharge, there are no limits to the patient’s physical activity. Patient is expected to resume daily activities without any hindrance.
- Patient is asked to continue gradual dilatation practice according to the provided module, up to 2 times per day, preferably in the morning and the evening.
- After 6–8 weeks post-procedure completion, patient is expected to come for a follow-up appointment for a direct observation. During follow-up appointment, patient history is taken, including her adherence to dilatation schedule, adherence to medication and other complaints. Patient is asked for her consent to undergo gynaecologic examination, in the form of digital vaginal examination, speculum exam and transvaginal ultrasound. During this exam, any involuntary bodily movements are documented, if present. If vaginal muscle spasm and/or involuntary movement are still present, the examination is immediately halted and the patient is informed to attend another follow-up.
- After her gynaecologic follow-up appointment, patient is offered a reflex consultation on the same day to the psychiatric clinic, in which she will undergo a follow-up assessment. Further follow-ups, if required, are discussed and agreed with the consultant psychiatrist.
- If no further visits are deemed necessary, patient is then discharged from care.
The patients undergoing assisted dilatation between 1 January 2022 and 31 December 2023 are identified through their medical records and case notes. Between March and April 2025, the consultant gynaecologist personally sent the patients an online questionnaire to fill in, asking about their current conditions and reproductive history. The customised questionnaire included questions asking for presenting complaint, the number of weeks and attempts required to achieve sexual penetration (if successful) and details of any pregnancy after discharge. This questionnaire was not to validate the vaginismus diagnosis and/or accompanying mental health conditions as they were considered completely treated upon discharged. This questionnaire included a written consent form which the patients were specifically asked to complete prior to agreeing to proceed with the questionnaire. Thus, all patients responding to the questionnaire had specifically provided a written consent and acknowledged the use of their data for the purposes of this study. Patients that did not respond to our request were recorded. However, we did not send another request to non-responding patients for reasons discussed later in Discussion. Patient data are collected and tabulated into a customized Microsoft Excel spreadsheet with their data anonymized, coded and standardized. We collected data on the following variables: chief complaint, age at consultation (female patient and male spouse), origin, educational background, employment status, median duration of vaginismus, patient history, psychiatric history, follow-up attendance, number of weeks to penetration, number of attempts to penetration, and details surrounding any pregnancy after treatment (type of pregnancy, outcome and delivery method). A flowchart (Figure 1) depicting the stages of patient care and the study performed is presented below.
 |
Figure 1 Flowchart of Vaginismus Management. |
Statistical analysis is performed as required. Numerical data are presented in mean ± standard deviations for parametric data with median (range) presented for non-parametric data. Percentages are presented followed by their numerators and denominators in brackets. Descriptive statistical calculations are carried out on all variables. Further statistical analysis is carried out for number of weeks to penetration and number of attempts of penetration. Kolmogorov–Smirnov test is used to assess data normality. They are analysed by Student’s t-test when parametric and Mann–Whitney U-test when non-parametric. A p-value of <0.05 is considered statistically significant. Statistical analysis is carried out using IBM SPSS for Mac version 30. Spreadsheets are made on Microsoft Excel as part of the Office365 suite for Mac.
This study complies with the Declaration of Helsinki and received its ethical clearance from the Research Ethics Committee of the Faculty of Medicine of Universitas Padjadjaran, Indonesia, with the registration number of 1276/UN6/KEP/EC/2024.
Results
There were 513 patients included in this study, of which 54.4% (277/513) were in 2022 and 45.6% (234/513) were in 2023 (Table 1). 10.6% (513/4838) of new patients presenting to our hospital were vaginismus patients across 2022–2023. 85.4% (438/513) of patients presented due to failure of penetration in intercourse, whilst 14.6% (75/513) reported difficult and/or painful penetration. The overall average age at consultation for the female patient was 30.39 ± 4.75 (median 30, range 19–53) and 12.7% (65/513) presented above 35 years old. The male partner’s (where available) average at consultation was 31.82 ± 5.46 (median 31).
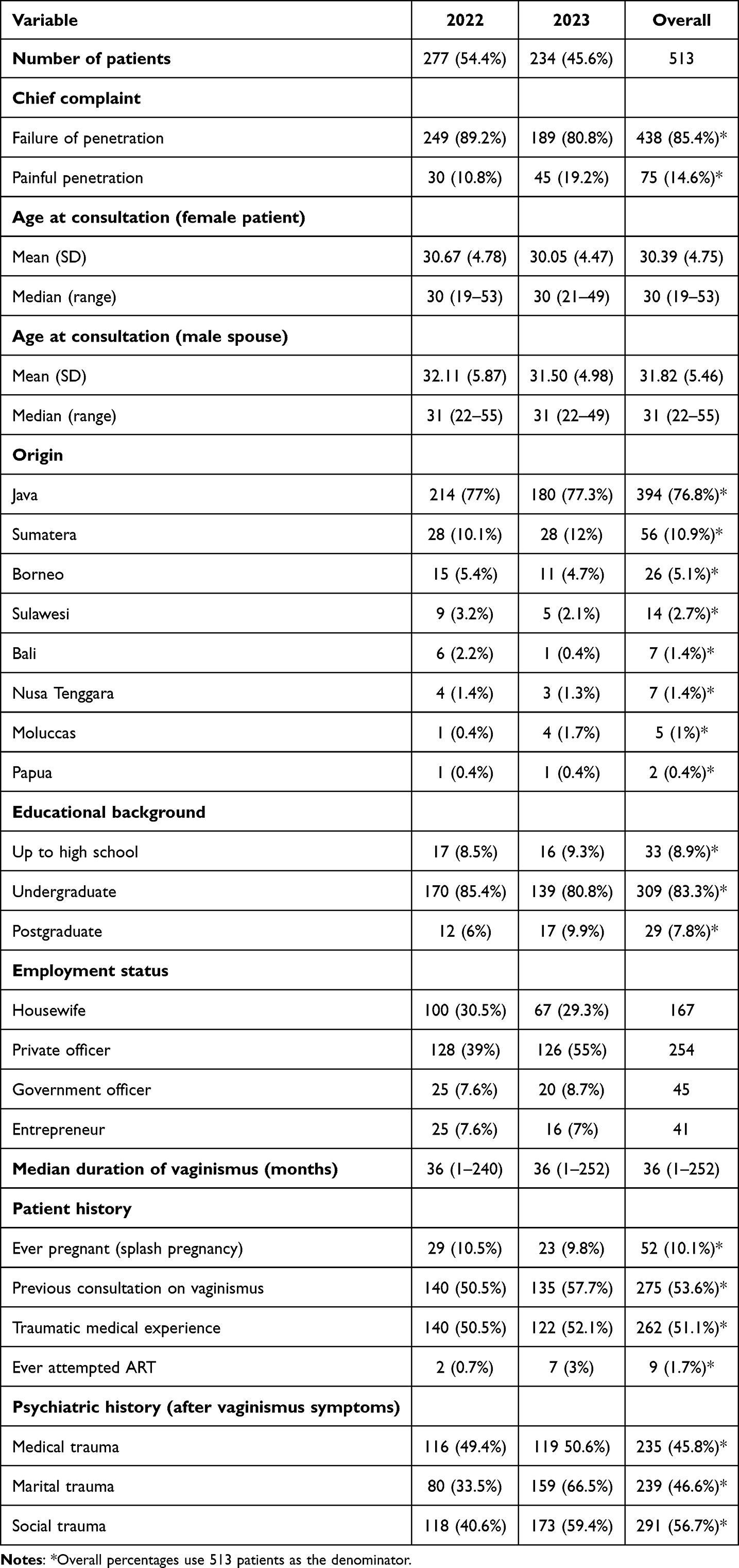 |
Table 1 Patient Demographics |
In both years, whilst most patients came from the island of Java at 76.8% (394/513) we had patients coming from all parts of Indonesia, the furthest being from Papua. Undergraduates formed the majority of patients at 83.3% (309/371) and most patients worked in the private sector at 49.5% (254/513).
The median duration of vaginismus prior to presenting for treatment was 36 months (range 1–252 months). Up to 1 in 10 (52/513) had been pregnant previously. More than half, at 53.6% (275/513), had had previous consultations regarding vaginismus with other health professionals prior to coming to our clinic and unfortunately, 51.1% (262/513) had experienced some degree of traumatic medical experience with health professionals. Nine patients (1.7%, 9/513) had attempted assisted reproductive technology (ART) previously.
Upon consultation with the consultant psychiatrist, 45.8% (235/513) disclosed that they had experienced medical trauma whilst seeking help for their vaginismus. 46.6% (239/513) of patients reported that they had experienced marital trauma before the procedure. More than half, at 56.7% (291/513) had experienced social trauma before the procedure, and they had reported having received neither diagnosis from mental health professionals nor treatment for mental health conditions.
Most patients at 99.4% (510/513) required/underwent the procedure once whilst 0.6% (3/513) underwent a second procedure. The three patients underwent their first procedure in 2022 and had a repeat procedure in 2023.
Upon discharge, overall, 61.2% (314/513) attended follow-up visit post-procedure at 6–8 weeks post-discharge (Table 2). 89.4% (281/314) reported penetration post-discharge when questioned at follow-up. 79.4% (174/219) achieved gynecological examination. 78.5% (172/219) said they adhered to the self-dilatation protocol. 23.7% (52/219) still exhibited involuntary movement when examined at follow-up visit.
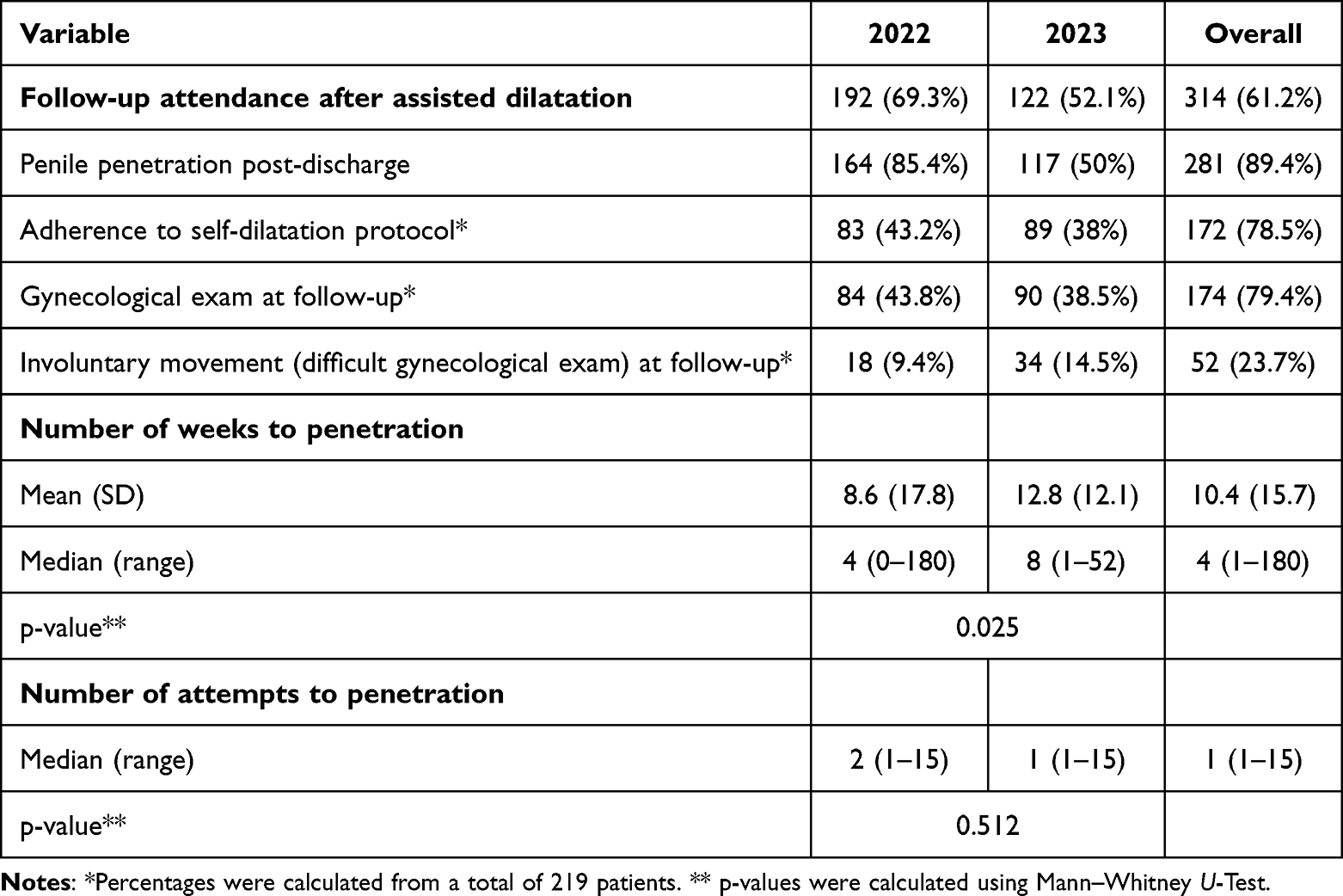 |
Table 2 Patient Follow-Up Post-Assisted Dilatation |
Due to not all patients having attended follow-up, we sent out an online questionnaire to all patients in March–April 2025 to all patients undergoing assisted dilatation procedure in 2022–2023. 60.8% (312/513) filled the online questionnaire and 91% (284/312) patients had reported continuous penetration after being discharged from follow-up. The mean number of weeks for 1st penetration to occur is 10.4 ± 15.7 weeks, whilst median was 4 weeks, range 1–180 weeks. There was a statistically significant difference in the median number of weeks required between 2022 and 2023 with p = 0.025 (Mann–Whitney U-Test). The self-reported median number of penetrations attempts before achieving complete penetration at intercourse was 1 attempt, range 1–15 attempts. There was not a statistically significant difference between the number of attempts across both years with p = 0.512 (Mann–Whitney U-Test).
In this questionnaire, we also surveyed the obstetric outcomes of patients (Table 3) and we got 312 responses. However, not all responses were completely filled. 51% (159/312) of patients reported that they had achieved pregnancy. However, not all patients disclosed of their method of conception. Among those who did, 85.1% (120/141) conceived spontaneously, 5.7% (8/141) conceived through assisted reproductive technology and 9.2% (13/141) had splash pregnancies. Splash pregnancies are pregnancies that occur without penile penetration into the vagina. One hundred and sixteen patients reported the pregnancy outcomes, with 88% (102/116) achieving term delivery. Most patients at 94.2% (98/104) delivered by caesarean section.
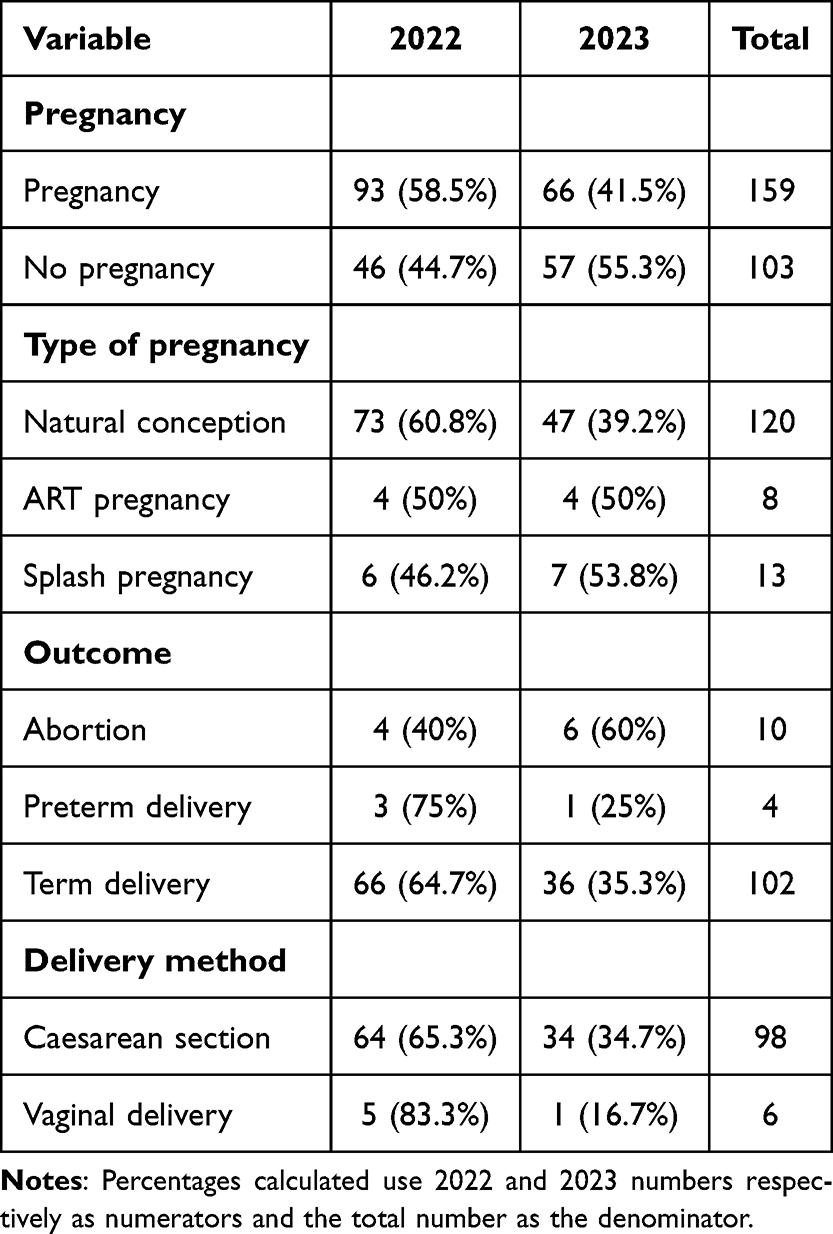 |
Table 3 Obstetric Outcomes of Surveyed Vaginismus Patients |
Discussion
Vaginismus is a gynaecologic disorder with involuntary and persistent vaginal closure when any form of penetration is attempted, whether by a penis, finger, tampon or speculum.22 In the latest International Classification of Diseases (ICD) 11th edition, it is now classified under sexual pain-penetration disorder, which is different from ICD-10, which classified it under pain and other conditions associated with the female genital organs (ie. vagina) and menstrual cycle.23,24 In the latest edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), the diagnoses of vaginismus and dyspareunia have been collapsed into a single diagnostic entity called “genito-pelvic pain/penetration disorder” due to their substantial clinical overlap and the absence of reliable discriminatory markers.13,22,25–27 GPPPD manifests through four core symptom dimensions (Criterion A), encompassing persistent or recurrent difficulties with vaginal penetration during intercourse, genito-pelvic pain during penetration or attempts thereof, marked fear of pain associated with vaginal penetration, and notable tension or tightening of the pelvic floor during attempted vaginal penetration.13,25–27
Principal Findings
Vaginismus’ etiology remains unknown and often called idiopathic, and it is not limited to a particular group. It affects all kinds of people from every tribe and language, across difference levels of educational attainment and socioeconomic status, as demonstrated by our data. We found that our patients originated from all regions of Indonesia, despite our hospital’s location in the island of Java, Indonesia’s most populous island. We also found that most patients in our cohort were undergraduates. This may be explained by the socio-economic profile our patients presenting to our private hospital, which tend to come from middle-class to upper-class background. Furthermore, in this study, we only included patients that underwent surgery at our facility and as vaginismus is not covered by the national health insurance scheme of Indonesia, the out-of-pocket expenses for this surgery might have excluded a lot of patients from undergoing the procedure. Interestingly, the same observation has been reported elsewhere in Iran and Turkey. Their studies also had a similar weakness, as they only reviewed patients presenting to their clinic and another reason might have been that undergraduates and/or postgraduates were more meticulous regarding their sexual health and would be better equipped to enquire of their conditions.28
Patients often presented to our facility after a protracted duration of vaginismus. The median duration was 36 months, considerably longer than the timeframe for infertility diagnosis. Low awareness, both from the public and medical community, may prevent women from seeking help early and getting the appropriate diagnosis and treatment at a timely manner.29–31 Lack of spousal support, unfavorable interpersonal relationship with a spouse and in some communities, patriarchy, form the first barrier to seeking help.31,32 Additionally, the healthcare system is still predominantly androcentric, and women’s concerns of painful sex are often dismissed as normal and given generic and inappropriate advice to “relax” during sexual intercourse.17,30 Such unsympathetic response may stem from the physician’s lack of confidence and reluctance in initiating discussion of sexual matters.2 This contributes to women receiving misinformation and prevents them from seeking further help.30,31
Our data seem to corroborate this argument. More than half of our patients had sought consultations with other health professionals prior to presenting to our facility and 51% of patients had also reported a traumatic medical experience. Such traumas may stem from verbal abuse from the health professionals.30 Whilst not formally recorded by our consultant gynaecologist (RAW), patients often reported of condescending remarks from their previous gynecologist, eerily similar to a previous study by Pacik et al17 Worst still, patients also reported of physical abuse through inappropriate and painful vaginal examinations.30
Review of Literature on Vaginismus and Pain
Painful experiences shape future prognosis. The prolonged experience of pain, ie. at least 3 months, contribute to stress, anxiety, depression, and interference in normal everyday function. Post-traumatic stress disorder and chronic pain, eg. in vaginismus, often coexist.33 They show a bidirectional relationship due to shared neural mechanisms and the fear-avoidance model. The development of chronic pain and PTSD is called the Triple Vulnerability Model. The model suggests that there are three integrated vulnerabilities that need to be present for one to develop a disorder: biological vulnerabilities, generalized psychological vulnerabilities, and specific psychological vulnerabilities.33,34
Vaginismus experience inevitably caused a lot of psychosocial traumas for the patient and their partner.35 The most common problem is mental health problem, sexual problems, unconsummated marriage, infertility, and extramarital affairs.27,36–38 Couple with longer vaginismus period possibly have higher level of catastrophic moments and phobia, negative self-image cognition, and self-stigma.1,27 The health-related stigma and discrimination in vaginismus cases are harmful and affect the help-seeking behavior.39,40 This is most evident amongst our patients. By their own admission, 45.8% (235/513) disclosed that they had experienced medical trauma from their vaginismus symptoms; 46.6% (239/513) had experienced marital trauma before the procedure; and 56.7% (291/513) had experienced social trauma. Thus, a trauma-informed care is a prerequisite for health professionals managing vaginismus patients, to avoid any form of re-victimization and the addition of new traumas to patients.41,42
Psychological trauma from self-guilt and facing the shame co-occur with chronic pain during sexual activities, causing life-impairing distress.43,44 Excessive dread of pain during the penetration trial is a common symptom that can induce trauma in patients, leading to phobic disorder.45 Involuntary spasm of the pelvic floor, which receive neural input from both the autonomic nervous systems sympathetic and parasympathetic systems, may be part of the wider defense reaction of the body to stress.27 Most cases showed the involuntary response, such as closing the thighs, elevating the buttocks, avoiding intimate moments, stiffness in the thighs, and trembling. All this response was the automatic body response to prevent the penetration moment, the fear-avoidance moment. This condition also happens during vaginal examination.45 This further underlines the urgency and the necessity of psychological treatment for vaginismus patients, as the primary goal is not penetration per se, but rather to support the patient in her journey to recovery.
Another example of PTSD amongst vaginismus patients is the somewhat muted response towards the online questionnaire we distributed. Whilst 60.8% (312/513) filled the online questionnaire, we noticed that many entries were filled partially and even, sparsely. Some patients only put in their names and dates of birth but then discontinued the questionnaire. Other examples were “blank entries”, in which the patients had clicked the link provided but not going past the introduction page of the questionnaire. It is our suspicion that this questionnaire was an act of “revisiting the trauma” for some patients, and such experience was too overwhelming as it re-triggered the immense emotional pain that they had been through.43–45
Clinical Results and Implications
Botulinum toxin was used to aid vaginal dilatation.18,19 There are several suggested mechanisms to how botulinum toxin ameliorates pain in vaginismus patients.46 Vaginismus is associated with muscle overactivity and spasm, and botulinum toxin may block acetylcholine release at the neuromuscular junctions.46 With reduced muscle spasm, gradually, there is an easing of muscular pain and ability to achieve assisted vaginal dilatation.46 The effects of botulinum toxin are not instantaneous and so, to provide more immediate pain relief, we added local anaesthetic drugs (eg. bupivacaine and epinephrine). However, we observe that the stepwise dilatation using dilators is the primary contributor to the progressive reduction of vaginal spasms, aided by botulinum toxin and local anaesthetics.
Our results regarding penetration post-procedure are in line with other studies. Our patients reported that >90% achieved continuous penetration after hospital discharge. This is better than the previous results from Pacik et al with 71% of patients achieving pain-free penetration after procedure.18 The use of sensate focus technique during the initial self-dilatation by the patient in the ward could contribute to the positive outcome. The sensate focus technique, originally described by Masters and Johnson, consists of “a series of structured instructions for touching activities to help couples overcome anxiety and increase comfort with physical intimacy.”47–49 The consultant gynaecologist (RAW) was present in the same room during the first supervised session of self-dilatation and would give verbal instructions alongside empathetic reassurances without direct physical intervention. Further instructions for the patient and her partner were provided to overcome anxiety and be more comfortable with the dilatation process. This technique, similar to Jindal’s report, was effective in allowing patients adhere to the self-dilatation protocol, resume intimacy with their partner and eventually succeeding in gynaecological examination at follow-up.47
Our data will add more data to the suggested efficacy of combining botulinum toxin injection, vaginal dilator therapy and psychiatric support for managing vaginismus. A recent meta-analysis highlighted the challenges of managing vaginismus, as over 10-year period between 2015–2025, various studies only managed to recruit 863 patients.14 Our results agree with the meta-analysis reporting that combined psychosexual interventions had the biggest success rate (86%), followed by botulinum toxin injection (85%), cognitive behavioral therapy (82%) and finally vaginal dilator therapy (78%).14
We are aware of the somewhat low follow-up attendance at only 61%. Whilst travel costs might have been prohibitive for some couples, others might not have attended the follow-up visit due to fears and associated denial. This is a possible attrition bias, and this is a limitation for our study. It is worth noting that whilst almost 90% reported penetration post-discharge, less than 80% could achieve vaginal exam. About 23% of patients still had involuntary movements when they were examined at the follow-up visit. This could suggest that some patients had experienced such complex deep-lasting traumas that were not easily cured with a single assisted dilatation procedure.
A notable finding was the median number of weeks to penetration at 4 weeks. It allowed a significant time for patients to be confident in achieving self-dilatation, free of trauma, which in turn gave them the added confidence and, finally, impetus to attempt sexual penetration with their partner. This is reflected by the patients’ own admission of achieving penetration in their first attempt. Whilst there may be a recall bias, we suspect minimal recall bias here as achieving full penetration would have been a significant milestone.
Our findings on obstetric outcomes are in line with published results elsewhere. Most patients achieved conception naturally through sexual intercourse, and this is similar to a meta-analysis by Baril et al15 This is somewhat expected, as their barrier to conception is the lack of sexual penetration. Once this issue is resolved, most patients could conceive as their reproductive organs were functioning normally. Most patients managed to reach term gestation, similar to Baril et al’s results15 Finally, most patients opted for caesarean section. Unfortunately, there are no data on why they opted for caesarean section as they were from out of town and chose to deliver at their respective hospitals. We also did not include a question on why they had caesarean section in the questionnaire as it would have introduced another possible source of response bias. This high caesarean section rate is similar to other studies with Baril et al reporting that up to one-quarter of all caesarean sections amongst vaginismus patients are done upon maternal request.15 This may reflect the fear of experiencing the pain of childbirth and the associated vulvovaginal traumas/tears among these women.15 Furthermore, caesarean section can be performed on the basis of preventing secondary vaginismus in the future.50 Secondary vaginismus can reach up to 30% according to an Indian study.50
We continue in our efforts to further enlighten the general Indonesian public on vaginismus. Our consultant gynaecologist, RAW, received a national award from the Indonesian museum of world records (Museum Rekor Dunia Indonesia) for his contributions in vaginismus and the support group Vaginismus Indonesia continues to present talks and seminars on the topic.16
Strengths and Limitations
This study has several strengths. Firstly, ours is the largest hospital by number in treating vaginismus patients in Indonesia, and to our knowledge, in Southeast Asia. This is highlighted by a recent meta-analysis that only managed to combine 863 patients across 18 studies, highlighting the need for large-scale studies on vaginismus.14 Secondly, we have established a clear protocol with multidisciplinary team approach in patient treatments. Prior to launching our vaginismus service, we initiated a compulsory training for the nursing staff, administrative staff and even our security team to enable them in providing a compassionate service with minimal prejudice from beginning to end. Fourthly, this is the largest audit of vaginismus patients to date from Indonesia. Our experience in managing vaginismus patients amidst our country’s religious background with conservative principles and family values may provide a new insight on holistic vaginismus management.
However, this study has several limitations too. Firstly, this was a retrospective audit and it lacked a comparison group, thereby limiting causal inference. Secondly, it suffers from various biases, ie. recall bias, attrition bias and selection bias, which might hamper its adoption in other health facilities. Thirdly, several aspects in the patient data were filled incorrectly and/or missing so for some variables, the analysis could not involve all patients. Fourthly, the questionnaire only had a 60% response. Whilst this was satisfactory considering we only distributed the questionnaire once, we also suspect that some patients refused or were hesitant in answering the questionnaire due to fears of re-traumatization. Finally, we do not have the data on why patients were offered caesarean section for their delivery. More proper research is thus needed, in which prospective patients are explicitly informed about a future questionnaire and then asked for their consent to fill in the questionnaire when requested. We are also modifying our protocol as we suggest necessary improvements in the timeframe where patients are allowed to attempt vaginal penetration. We hope to publish our results in the future.
Conclusion
Vaginismus is a disease with complex condition with multiple consequences in biological, psychological and socio-cultural domains. Co-existing mental health disorders due to protracted duration of vaginismus suggest that a comprehensive simultaneous assisted dilatation procedure and psychiatric treatment along with strong patient commitments towards cure are required for improving clinical outcomes. More research is necessary to evaluate the lasting effect of our protocol, the general long-term outcomes and the adoption of our protocol for other centers of vaginismus care.
Data Sharing Statement
Anonymized data are available from the authors upon written request.
Ethics Approval
Approved by the Research Ethics Committee of Universitas Padjadjaran, registration number: 1276/UN6.KEP/EC/2024.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pithavadian R, Chalmers J, Dune T. The experiences of women seeking help for vaginismus and its impact on their sense of self: an integrative review. Womens Health. 2023;19:17455057231199383. doi:10.1177/17455057231199383
2. Buster JE. Managing female sexual dysfunction. Fertil Steril. 2013;100(4):905–14. doi:10.1016/j.fertnstert.2013.08.026
3. Tetik S, Yalçınkaya Alkar YAÖ. Vaginismus, dyspareunia and abuse history: a systematic review and meta-analysis. J Sex Med. 2021;18(9):1555–1570. doi:10.1016/j.jsxm.2021.07.004
4. Velayati A, Jahanian Sadatmahalleh S, Ziaei S, Kazemnejad A. The role of personal factors in quality of life among Iranian women with vaginismus: a path analysis. Health Qual Life Outcomes. 2021;19(1):166. doi:10.1186/s12955-021-01799-5
5. Laskowska A, Gronowski P. 267 vaginismus: an overview. J Sexual Med. 2022;19(Supplement_2):S228–S229. doi:10.1016/j.jsxm.2022.03.520
6. Amidu N, Owiredu WK, Woode E, et al. Incidence of sexual dysfunction: a prospective survey in Ghanaian females. Reprod Biol Endocrinol. 2010;8(1):106. doi:10.1186/1477-7827-8-106
7. Oksuz E, Malhan S. Prevalence and risk factors for female sexual dysfunction in Turkish women. J Urol. 2006;175(2):654–658. doi:10.1016/s0022-5347(05)00149-7
8. Bulgurcu RA, Sahin BM. ‘I feel like i’m hitting a wall or there’s a narrow tunnel’: a qualitative study based on online forum posts by women with vaginismus. Scand J Caring Sci. 2025;39(2):e70056. doi:10.1111/scs.70056
9. Lamba A, Mohajir N, Rahman S. A review of the psychosocial factors that contribute to sexuality, female sexual dysfunction, and sexual pain among Muslim women. Sex Med Rev. 2023;11(3):156–173. doi:10.1093/sxmrev/qead019
10. Bennett LR. Infertility, womanhood and motherhood in contemporary indonesia: understanding gener discrimination in the realm of biomedical fertility care. Intersectionsc. 2012;(28). doi:10.25911/5F8H-1Y66
11. Kapoor I. Family planning encompasses sexuality -- an Asian perspective. Planned Parenthood Challenges. 1993;(2):8–10.
12. Bennett LR, Wiweko B, Bell L, et al. Reproductive knowledge and patient education needs among Indonesian women infertility patients attending three fertility clinics. Patient Educ Couns. 2015;98(3):364–369. doi:10.1016/j.pec.2014.11.016
13. Chalmers KJ. Clinical assessment and management of vaginismus. Aust J Gen Pract. 2024;53(1–2):37–41. doi:10.31128/ajgp/06-23-6870
14. Zulfikaroglu E. Vaginismus treatment: a systematic review and meta-analysis of contemporary therapeutic approaches. J Sexual Med. 2025;23(1). doi:10.1093/jsxmed/qdaf295
15. Baril S, Marion A, Abenhaim HA. Obstetric outcomes in women with vulvodynia and vaginismus: a systematic review. Arch Gynecol Obstet. 2024;311(1):1–11. doi:10.1007/s00404-024-07871-x
16. MURI. Dokter Penggiat Vaginismus Pertama di Indonesia. Museum Rekor Dunia - Indonesia. 2018. Available from: https://muri.org/Website/Rekor_detail/dokterpenggiatvaginismuspertamadiindonesia.
17. Pacik PT. Understanding and treating vaginismus: a multimodal approach. Inturogynecol J. 2014;25(12):1613–1620. doi:10.1007/s00192-014-2421-y
18. Pacik PT, Geletta S. Vaginismus treatment: clinical trials follow up 241 patients. Sex Med. 2017;5(2):e114–e123. doi:10.1016/j.esxm.2017.02.002
19. Werner MA, Ford T, Pacik PT, Ferrara M, Marcus BS. Botox for the treatment of vaginismus: a case report. J Womens Health Care. 2014;03. doi:10.4172/2167-0420.1000150
20. Sarelius I, Pohl U. Control of muscle blood flow during exercise: local factors and integrative mechanisms. Acta Physiol. 2010;199(4):349–365. doi:10.1111/j.1748-1716.2010.02129.x
21. ter Kuile MM, van Lankveld JJDM, de Groot E, Melles R, Neffs J, Zandbergen M. Cognitive-behavioral therapy for women with lifelong vaginismus: process and prognostic factors. Behav Res Ther. 2007;45(2):359–373. doi:10.1016/j.brat.2006.03.013
22. Association AP. Diagnostic and Statistical Manual of Mental Disorders.
23. Organization WH. International Statistical Classification of Diseases and Related Health Problems.
24. Reed GM, Drescher J, Krueger RB, et al. Disorders related to sexuality and gender identity in the ICD-11: revising the ICD-10 classification based on current scientific evidence, best clinical practices, and human rights considerations. World Psychiatry. 2016;15(3):205–221. doi:10.1002/wps.20354
25. Cosgriff L, Ramanathan A, Iglesia CB. Pelvic floor disorders and sexual function: a review. Obstet Gynecol Clin North Am. 2024;51(2):241–257. doi:10.1016/j.ogc.2024.02.001
26. Zarski A-C, Baumeister H, Kählke F. DSM-5 genito-pelvic pain/penetration disorder: prevalence, comorbidities, and associated factors in university students. Int J Clin Health Psychol. 2025;25(1):100529. doi:10.1016/j.ijchp.2024.100529
27. McEvoy M, McElvaney R, Glover R. Understanding vaginismus: a biopsychosocial perspective. Sexual and Relationship Therapy. 2024;39(3):680–701. doi:10.1080/14681994.2021.2007233
28. Akhavan-Taghavi MH, Asghari-Moghaddam MA, Froutan SK, Jadid-Milani M. Vaginismus in Iran: a single center report of 7 years experience. Nephro Urol Monthly. 2015;7(6):e30077. doi:10.5812/numonthly.30077
29. Pacik PT, Babb CR, Polio A, Nelson CE, Goekeler CE, Holmes LN. Case series: redefining severe grade 5 vaginismus. Sexual Med. 2019;7(4):489–497. doi:10.1016/j.esxm.2019.07.006
30. Pithavadian R, Dune T, Chalmers J, Ramanathan V. The interrelationship between women’s help-seeking experiences for vaginismus and their sense of self: a qualitative study and abductive analysis. Health Psych Behav Med. 2024;12(1):2396134. doi:10.1080/21642850.2024.2396134
31. Maasoumi R, Sabetghadam S, Keramat A, Aghayan SS. Help-seeking challenges for female sexual concerns: a qualitative study from Iran. BMC Health Serv Res. 2023;23(1):713. doi:10.1186/s12913-023-09719-7
32. Rodríguez-García-de-Cortázar A, González-Calo I, Gómez-Bueno C. What is the patriarchy doing in our bed? Violent sexual-affective experiences among youth. Sex Res Soc Policy. 2025;22(1):424–434. doi:10.1007/s13178-024-00956-x
33. Kind S, Otis JD. The interaction between chronic pain and PTSD. Curr Pain Headache Rep. 2019;23(12):91. doi:10.1007/s11916-019-0828-3
34. Jeng C-J. The pathophysiology and etiology of vaginismus. Taiwanese J Obstetrics Gynecol. 2004;43(1):10–15. doi:10.1016/S1028-4559(09)60047-4
35. Fulton J, Snyder H, Chalif J, Delwiche K, Chambers LM. Evidence and best practices for trauma-informed care in gynecologic oncology patients. Int J Gynecol Cancer. 2024;34(7):1077–1088. doi:10.1136/ijgc-2024-005300
36. Michetti PM, Silvaggi M, Fabrizi A, Tartaglia N, Rossi R, Simonelli C. Unconsummated marriage: can it still be considered a consequence of vaginismus? Int J Impot Res. 2014;26(1):28–30. doi:10.1038/ijir.2013.24
37. Maseroli E, Scavello I, Rastrelli G, et al. Outcome of medical and psychosexual interventions for vaginismus: a systematic review and meta-analysis. J Sex Med. 2018;15(12):1752–1764. doi:10.1016/j.jsxm.2018.10.003
38. Krishnappa P, Manfredi C, Jayaramaiah S, et al. Unconsummated marriage: a systematic review of etiological factors and clinical management. J Sexual Med. 2023;21(1):20–28. doi:10.1093/jsxmed/qdad146
39. Hussein J, Ferguson L. Eliminating stigma and discrimination in sexual and reproductive health care: a public health imperative. Sexual Reproduct Health Matters. 2019;27(3):1–5. doi:10.1080/26410397.2019.1697103
40. Rai SS, Peters RMH, Syurina EV, Irwanto I, Naniche D, Zweekhorst MBM. Intersectionality and health-related stigma: insights from experiences of people living with stigmatized health conditions in Indonesia. Int J Equity Health. 2020;19(1):206. doi:10.1186/s12939-020-01318-w
41. Lees BF, Stewart TP, Rash JK, Baron SR, Lindau ST, Kushner DM. Abuse, cancer and sexual dysfunction in women: a potentially vicious cycle. Gynecol Oncol. 2018;150(1):166–172. doi:10.1016/j.ygyno.2018.04.002
42. ACOG. Caring for patients who have experienced trauma: ACOG committee opinion, number 825. Obstet Gynecol. 2021;137(4).doi:10.1097/AOG.0000000000004326
43. Nanavaty N, Thompson CG, Meagher MW, McCord C, Mathur VA. Traumatic life experience and pain sensitization: meta-analysis of laboratory findings. Clin J Pain. 2023;39(1):15–28. doi:10.1097/ajp.0000000000001082
44. Hooten WM. Chronic pain and mental health disorders: shared neural mechanisms, epidemiology, and treatment. Mayo Clin Proc. 2016;91(7):955–970. doi:10.1016/j.mayocp.2016.04.029
45. Raveendran AV, Rajini P. Vaginismus: diagnostic challenges and proposed diagnostic criteria. Balkan Med J. 2024;41(1):80–82. doi:10.4274/balkanmedj.galenos.2023.2022-9-62
46. Karp BI, Stratton P. Applications of botulinum toxin to the female pelvic floor: botulinum toxin for genito-pelvic pain penetration disorder and chronic pelvic pain in women. Toxicon. 2023;230:107162. doi:10.1016/j.toxicon.2023.107162
47. Jindal UN, Jindal S. Use by gynecologists of a modified sensate focus technique to treat vaginismus causing infertility. Fertil Steril. 2010;94(6):2393–2395. doi:10.1016/j.fertnstert.2010.03.071
48. Weiner L, Avery-Clark C. Sensate focus: clarifying the masters and Johnson’s model. Sexual Relationship Therapy. 2014;29(3):307–319. doi:10.1080/14681994.2014.892920
49. Linschoten M, Weiner L, Avery-Clark C. Sensate focus: a critical literature review. Sexual Relationship Therapy. 2016;31(2):230–247. doi:10.1080/14681994.2015.1127909
50. Bulbuli A, Kokate V. Prevalence of vaginismus in reproductive age group: observational study. J South Asian Federation Obstet Gynaecol. 2024;16(2):198–201. doi:10.5005/jp-journals-10006-2395
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.