Back to Journals » Psychology Research and Behavior Management » Volume 15
Managing Transference and Countertransference in Cognitive Behavioral Supervision: Theoretical Framework and Clinical Application
Authors Prasko J ![]() , Ociskova M
, Ociskova M ![]() , Vanek J
, Vanek J ![]() , Burkauskas J, Slepecky M, Bite I, Krone I
, Burkauskas J, Slepecky M, Bite I, Krone I ![]() , Sollar T
, Sollar T ![]() , Juskiene A
, Juskiene A
Received 8 April 2022
Accepted for publication 10 July 2022
Published 11 August 2022 Volume 2022:15 Pages 2129—2155
DOI https://doi.org/10.2147/PRBM.S369294
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Jan Prasko,1– 4 Marie Ociskova,1 Jakub Vanek,1 Julius Burkauskas,5 Milos Slepecky,2 Ieva Bite,6 Ilona Krone,7 Tomas Sollar,2 Alicja Juskiene5
1Department of Psychiatry, Faculty of Medicine, Palacky University, University Hospital Olomouc, Olomouc, Czech Republic; 2Department of Psychological Sciences, Faculty of Social Science and Health Care, Constantine the Philosopher University, Nitra, Slovak Republic; 3Department of Psychotherapy, Institute for Postgraduate Training in Health Care, Prague, Czech Republic; 4Rehabilitation Hospital Jessenia Inc, Akeso Holding, Beroun, Czech Republic; 5Laboratory of Behavioral Medicine, Neuroscience Institute, Lithuanian University of Health Sciences, Kaunas, Lithuania; 6University of Latvia, Latvian Association of CBT, Riga, Latvia; 7Riga’s Stradins University, Latvian Association of CBT, Riga, Latvia
Correspondence: Jan Prasko, Department of Psychiatry, Faculty of Medicine, Palacky University in Olomouc, University Hospital, I. P. Pavlova 6, Olomouc, 775 20, Czech Republic, Tel +420 603 414 930, Email [email protected]
Abstract: Dysfunctional patterns, beliefs, and assumptions that affect a patient’s perception of other people often affect their perceptions and behaviours towards the therapist. This tendency has been traditionally called transference for its psychoanalytical roots and presents an important factor to monitor and process. In supervision, it is important to put the patient’s transference in the context of the conceptualization of the case. Countertransference occurs when the therapist responds complementary to the patient’s transference based on their own dysfunctional beliefs or assumptions. Transference and countertransference provide useful insights into the inner world of the patient, therapist, and supervisor. Guided discovery is one of the most common approaches used by a supervisor and a supervisee to map all types and directions of transference and countertransference. Other options to map transference and countertransference are imagery and role-playing techniques.
Keywords: supervision, cognitive behavioral therapy, therapeutic relationship, supervisory relationship, transference, countertransference
Introduction
Comparing current and past experiences is automatic and mostly unconscious.1 Thus, transference and countertransference reactions present valuable sources of information about the individual’s inner world, either a patient, a therapist or a supervisor2,3,4,56. Examining the supervisee’s countertransference is a crucial but delicate part of the supervision process.5 However, transference and countertransference alone do not yet provide sufficient insight into the inner world of the patient, therapist, and supervisor. However, their careful identification and elaboration can be a useful source of clinical information and help remove barriers to treatment.
Sigmund Freud introduced the history of the early development of countertransference in 1909, as described by Stefana (2015).6 In the original psychoanalytic construction, transference was understood as one of the numerous forms of resistance and difficulty forming a required trusting relationship between therapist and patient.7 The concept of transference has gradually become an essential tool of analysis, through which it has undergone profound changes in definition and clinical use. The transference was recognised as a central element of the psychoanalytic process.9 Now classical psychoanalysis recognizes transference as an essential component of the therapeutic relationship.10 The basic tasks of supervision consist of clarifying the mutual expectations of the supervisee and the supervisor, creating a credible supervisory relationship as a basis for countertransference analysis, and examining “parallel processes” between the supervisor and the supervisee.11 Examining the supervisee’s countertransference is a necessary but delicate part of the supervision process.5 From the psychoanalytic perspective, the therapeutic relationship is the sum of the real relationship between two people, the working alliance, transference and countertransference,12,13 Levy and Scala 2012).7,70 Watkins (2011)14 and Gelso (2017)13 explored a tripartite model of the therapeutic relationship. This model postulates that a therapeutic relationship contains a working alliance, a real relationship, and transference and countertransference formation. Although the model seems theoretically and empirically feasible, further research is needed to improve the model further. In transference, the patients project to the therapist’s thoughts and feelings, originating from their experiences with important individuals they met earlier, especially in childhood and their mother and father (Gutheil and Gabbard 1998).10,71
Some psychotherapists believe that the difference between psychodynamic psychotherapy and cognitive behavioural therapy (CBT) lies mainly in the emphasis or lack of attention on transference.15 This is one of the most common misconceptions about CBT.15–18 However, CBT usually does not analyse the therapeutic relationship when solving uncomplicated problems and disorders (Beck 1995).2,19,17
When the patient trusts the therapist and actively engages in the therapy, the therapist acts as a supporting expert who accompanies the patient in the individual steps of the therapy and encourages them in their independent implementation.20 The patient does not depend on the therapist but only seeks a colleague to discuss the steps performed on their own. The relationship is straightforward. In more complex cases, including patients with personality disorders, the therapeutic relationship becomes an important therapeutic focus (Beck 1995;17 Zanarini 2009;2,72 McCracken and Gutiérrez-Martínez 2011).73
When we look at the history of CBT perspectives of transference and countertransference, we can recognise it from the beginning of cognitive therapy. Beck mentions transference as a “schematic response” in his publications as early as the 1970s.21 Although transference and countertransference were described early in CBT, they were not of clinical interest in initial, especially short-term therapies, unless they provided an example for the guided discovery of core beliefs or conditional rules triggered in the therapeutic relationship.2,22,23 In cognitive-analytical therapy (CAT), transference and countertransference are conceptualized as the organization of an individual’s experiences and behaviours throughout patterns composed of self-confirming sequences, including cognitive, emotional, and interpersonal processes based on previous experience.24 Individuals play roles and seek or provoke reciprocal reactions from others. CBT therapists have also pointed out how a patient relates to a therapist may reflect on their past emotional bonding difficulties, previous relationship patterns, and learned maladaptive emotion processing. Previously learned cognitive and emotional processes can lead to blocks in therapy.25
Nevertheless, specific difficulties in dealing with the disruption of the therapeutic relationship due to transference or countertransference have rarely been discussed.26 A deeper interest in theoretical and clinical views on transference and countertransference appeared at the turn of the millennium. From a socio-cognitive approach, it is important to recognise the therapeutic relationship as a co-construction so that what the patient brings and what the therapist brings are important for the way the relationship pattern is formed.27 According to their model, transference supposes that internal representations of important persons are in memory and could be activated by related signals in any context. Once the transference is activated, the individual looks at the other person through the glasses of the earlier representations of important persons. Leahy (2007)28 portrays a therapeutic relationship as an interactive game in which the therapist and the patient follow their previously learned rules and use them to expect the other to behave and adapt their behaviour accordingly. Previously developed relationship patterns and expressions of emotions significantly impact building and developing a therapeutic relationship. Eg, s therapist with unrealistic standards may unintentionally authorise a negative belief in a patient’s relationships. Understanding transference and countertransference allows the therapist to overcome the pitfalls of the therapeutic relationship and the blocks in therapy. It also helps the therapist better understand how the patient’s interpersonal world is reflected in the current relationship in therapy.28 Leahy (2007) states that the transference relationship consists of intrapersonal and interpersonal processes between the patient and the therapist. These processes include personal schemas about the self, others, and the world entering a therapeutic relationship. These patterns that make up the transference relationship can be recognised through guided questioning and Socratic dialogues and corrected by working with thoughts and schemas. To recognise countertransference, the therapist needs to apply the same procedures to themselves and train in self-reflection in a therapeutic situation.29 In his monograph, Newman (2013)23 also emphasises the importance of CBT therapists using CBT methods and strategies for themselves and using CBT methods considerably in coping with barriers in a therapeutic relationship, despite the patient’s self-understanding and understanding. Cartwright (2011)30 inspects the transference and countertransference from various perspectives, including attachment, the socio-cognitive perspective, the perspective of cognitive analytical therapy, and schema therapy. According to the author, countertransference reactions of therapists can offer insight into the experience of patients, especially their ways of relating to others and how others reciprocally react to them. Therefore, therapists can profit from understanding countertransference through reflective practice and supervision.
Hayes et al (2018)31 dealt with the definition and empirical research evaluating the relationship of countertransference to the effectiveness of psychotherapy. The authors presented three meta-analyses. The first showed that countertransference responses are inversely related to psychotherapy results, and the second supported the view that approaches to countertransference management can significantly reduce countertransference responses. Finally, a third meta-analysis showed that successful countertransference management is associated with better therapy outcomes.
Stefana et al (2020)32 conducted a systematic review of quantitative research on the relationship between the personality pathology of the patient and the cognitive, emotional, and behavioural responses of the psychotherapists in individual psychotherapy. Significant relationships between therapist responses and specific personality traits or disorders have been found. In general, eccentric and odd patients evoke feelings of detachment and disconnection in the therapist; patients with emotional dysregulation cause anxiety and feelings of incompetence, and anxious and withdrawn patients cause sympathy and concern. Relatively small studies sample and methodological discrepancies across studies limit the clear conclusions and propose the necessity for further research. This review suggests that patients who share similar personality disorders or symptoms tend to elicit similar cognitive, emotional, and behavioral responses in therapists.
A therapeutic relationship identifies the patient’s automatic thoughts, dysfunctional assumptions, and core beliefs, especially when dysfunctional beliefs about the therapist’s relationship trigger during a session (Beck 1995;17 Spinhoven et al 2007;74 Rivera and Darke 2012).75 If the transference relates to the patient’s relationship problems or lack of self-acceptance or presents an obstacle in the therapy, it is necessary to help the patient discover and gradually process it (Linehan and Kehrer 1993;76 Williams 1997;77 Spinhoven et al 2007).78
From a humanistic perspective, Rogers (1965)33 distinguish transference attitudes and a transference relationship between a client towards a therapist. In typical cases, clients’ attitudes toward their therapists are mild and of reality, rather than a transference in the psychoanalytical interpretation of transferring infantile attitudes to a present relationship where they are inappropriate. For example, the client may feel annoyed in early interviews that he does not receive the guidance he expected or leaves therapy with gratitude to the therapist for providing him with the opportunity to work things out for himself. Even though transference attitudes exist in many clients in non-directive therapy, these do not develop into a transference neurosis or a transference relationship that becomes central for psychoanalytical treatment. This is a consequence of a client-centred therapist’s different handling of clients’ transference attitudes than the psychoanalytical interpretation of transference. The client-centred therapist handles these attitudes just as he would handle similar attitudes directed toward others or any other client’s attitude – “he endeavours to understand and accept.33
In an existentialistic psychotherapeutic perspective, interpreting a client’s reaction as transference (with the implication that s/he was driven to respond as s/he did by echoes of the past within their unconscious) is perceived as a devaluation of a client’s capacity to choose or as reducing a client’s responsibility. The existential definition of transference places more emphasis on the client’s capacity to choose,34 which means that earlier dynamics and displaced feelings cannot completely explain a client’s motivation as they are also “motivated by more contemporary reasons why s/he is choosing to act in that manner to a real person in that room at that minute” (ref).
This paper describes case studies to provide more understanding and practical ideas about transference and countertransference in CBT supervision. The main focus is on approaches and techniques that effectively use transference in supervision. Illustrative supervision cases accompany the theoretical framework.
Patient Transference to the Therapist in Cbt Supervision
Transference within the therapy can be understood as reactions to the patient’s emotional, cognitive, and physical experiences, which can be seen in the responses to the therapist, but which are more related to the patient’s attitudes than to the therapist’s behaviour.2,35,36 These reactions are related to what the patient consciously and unconsciously expects from the therapist, and these expectations reflect their experience with important people in their life,26,36 (Levy and Scala 2012).70 Transference occurs when a patient’s previous experience with other people and with a therapist overlap.37 The patient’s transference reactions allow the therapist to recognize their likely behaviour toward important people in their life.28,38 The patient may respond to the therapist’s personality traits, appearance, style, or behaviour which may remind them of a significant person in the past. Dysfunctional patterns, beliefs, and assumptions that affect patients’ perceptions of other people often affect their therapist’s perception and behaviour.2 This is particularly significant when treating patients whose relationships have been painful, complicated or if they have been abandoned in childhood.39
Transference can also be abused in favour of the therapist at the patient’s expense, and this crossing of boundaries can occur unconsciously or consciously.40,41 The patient is usually unaware of it during psychotherapy if it is not interpreted or revealed to them during the work with the therapist. In treatment, transference can be beneficial, mainly if slightly positive, as it increases the patient’s assurance in the therapist and the likelihood of a cure,35,42,43 (Singer and Conway 2011;79 Nordgren et al 2013).80 Conversely, excessively positive and negative transference can block or slow down the therapeutic process, especially if it is not recognized and processed36 (Prasko et al in review process).
Manifestations of Patient’s Transference to the Therapist
Various signals manifest transference, eg, sudden change of expression, posture, looking away, quick transition to a new topic, admiring glances, avoiding important issues, stalling, pauses in the middle of the speech, clenched fists, knocking of feet, not wanting to say the automatic thoughts, etc.2,22 When asked by the therapist what is going on in their head or what they are experiencing, the patient may say: “It does not matter!” Mapping these reactions provides insight into the patient’s past and present relationships outside of therapy.
The development of strong transference is triggered by an unreadable therapist who behaves neutrally, says nothing about themselves and presents presenting without emotional involvement. The patient can freely transfer to the therapist the feelings they have learned with important people (Breuer and Freud 1895).44,81 A self-disclosure, warm and empathetic atmosphere, leadership for cooperation and an emphasis on patient autonomy can limit the potential for transference.2,37
The therapist should pay attention to any negative or positive reactions but not intentionally provoke them. The patient’s automatic thoughts and feelings about the therapist and their activity can provide a valuable opportunity to test automatic thoughts.17,45 Idealized transference usually develops at the beginning of the therapy, while negative transference usually occurs later. A therapist’s tendency to devaluate is one of the biggest challenges when managing resistance in patients who provoke aggressive or helpless reactions in therapists. When these situations occur, the therapist has a dual role, and they must tolerate the transference sufficiently to not react in a countertransference manner. In addition, from this vulnerable position, the therapist needs to help the patient understand the significance and consequences of the therapist’s devaluation.46
The patient forms the therapeutic relationship through many attitudes and expectations, which are shaped by:
- relationship with the therapist as a representative of authority, a system depending on personal experience with authorities, experience with previous therapists,
- the patient’s relationship to themselves (how much they trust themselves, their ability to manage, to have value, to control their experience and to respond to stress, and how much they label themselves);
- relationship to the therapist according to their actual behaviour (how the therapist behaves and how they act on him);
- concerns over therapy results and how therapy suits them;
- relation to the therapist in the context of societal attitudes, including myths about therapy and therapists;
- relationship with the therapist according to their reputation (what patient heard about a therapist before);
- the relationship to the whole system and the environment where the therapy occurs.
All of the above aspects may change dynamically during therapy39 (Adshead 2003;82 Hayes et al 2013).83 The transference relationship can work in conjunction with therapy to help achieve its goals, limit, disrupt, or block the entire therapy process36,42 (Høglend et al 2011).7,84
If a strong transference develops, it is an important task for the therapist to behave authentically and at the same time with an understanding of the patient’s behaviour (Table 1). One of the most important tasks is to avoid complementary behaviour, such as not reacting to the patient’s aggression by counter-aggression, not providing relief from the patient’s excessive loyalty, etc. This complementary behaviour is usually dictated by countertransference.2,47
 |  |  |
Table 1 Types of Patients Transference and Possible Responses of the Therapist |
Supervision of the Patient’s Transference to the Therapist
Automatic thoughts and feelings associated with therapist-patient interactions can provide valuable opportunities for testing and modifying dysfunctional automatic thoughts.17,45 A rapid leaving of the emotions expressed to the therapist or therapy and insufficient attention to this opportunity to understand the patient further are among therapeutic leadership mistakes.22 Tactics and timing are important when examining transference responses. Focusing on transference allows the patient and therapist to realize the difference between reality and fantasy in a therapy session2,40 directly. However, in short therapy, the therapist’s analyses of transference with the patient may be confusing.
In supervision, it is important to put the patient’s transference responses in context with the conceptualization of the case. Supervision helps the therapist realize that the patient’s transference response is taking place and understand how the type of transference relates to the patient’s previous experiences. Transference work allows the identification and modification of core schemes and conditional beliefs (Beck 1995,17 Nordgren et al 2013),80 early maladaptive schemes45 and modes.48 An explicit discussion of the patient’s relationship with the supervising therapist is compelling if it is accurate and the facts from the therapy are analysed.
The Use of Psychoeducation When Working with the Transference of the Patient to the Therapist
The supervisor’s education about transference and countertransference can increase the therapist’s awareness of what is happening to the patient during the therapeutic sessions. The supervisor asks the supervisee what types of transference or countertransference they know and then whether what is happening in the patient’s session is described.
Supervisors can discuss typical questions that help the therapist understand the transference reactions (Box 1).
 |
Box 1 Typical Questions That Help the Therapist to Map the Patient’s Transference |
Use of Guided Discovery to Map Patient Transference to Therapists
Guided discovery is one of the most common approaches that a supervisor and a supervisee use to map the transference of a patient to a therapist. Based on the description of what is happening in the therapy, the supervisor determines whether the therapist is aware of the patient’s transference. If not, the supervisor asks if there may be any connection between the patient’s behaviour towards the therapist and their behaviour towards important people in life. Another supervisor’s question is whether the therapist perceives from the patient’s conceptualization why a particular patient treats the therapist in a certain way and how their core schemes and conditional beliefs influence behaviour in a therapeutic session.2
Using Imagery to Map Patient Transference to Therapists
Imagery will allow the therapist to return to a specific situation in therapy during the supervision session (Box 2). One possibility is to imagine how the patient looked or behaved in a certain situation, and this can help the therapist reveal what could happen to the patient. Another possibility is to ask the therapist to imagine that they are a patient and what is happening in a particular situation. The connection of the imagery with the patient’s story increases the therapist’s understanding of why the transference occurs.
 |
Box 2 Case Vignette - Using Imagination in Supervision to Mentalize the Patient’s Feelings |
Use of Role-Playing to Map Patient Transference to a Therapist
Role-playing, where the therapist and the supervisor play a significant situation in the therapy, often reveals countertransference reactions. In the beginning, the supervisor may ask the supervisee to describe a specific situation from the therapy session in which they did not feel well. Then they play this situation together – the therapist plays themself, and the supervisor plays the patient. The supervisor then requests a role change and plays what the therapist said or did while the therapist is in the patient’s role (Box 3).
 |
Box 3 Case Vignette - Example of Using Role-Playing During Supervision |
Therapist’s Countertransference to Patient in Cbt Supervision
The supervisor-supervisee relationship (supervisory relationship) is based on similar laws as a therapeutic relationship,19,49,50 (Henry et al 1993).85 The supervisory relationship largely reflects the therapist-patient relationship. Still, more emphasis is placed on equality between the two and the independence and autonomy of the supervisee from the beginning of the supervision process51 (Prasko et al in review process). Countertransference occurs when the therapist responds in a complementary manner to the patient’s transference.52 Countertransference cannot be avoided despite procedures in the treatment and frequent emphasis on therapeutic techniques. Transference and countertransference are important sources of information about the inner world of the patient and the therapist. The therapist needs to recognize, understand, label, and express emotions to understand countertransference.22 Self-reflection is one of the basic competencies of a psychotherapist.2,43 The therapist should not underestimate their reactions to the patient but rather formulate them honestly and deal with them.
Manifestations of the Therapist’s Countertransference to the Patient
Countertransference is characterized by the thoughts, feelings, emotions and attitudes that the patient evoked in the therapist. The classical concept defined countertransference as the therapist’s uncontrolled response to the patient, arising from the therapist’s response to the patient’s transference or from one’s unresolved conflicts. Countertransference has been seen as an obstacle to treatment that needs to be eliminated.3 However, countertransference is present in every therapeutic relationship. In addition, the therapist’s reactions to the patient can be a valuable source of information about what reactions the patient can elicit in the people around them. The therapist needs to distinguish their countertransference from the patient’s transference related to unresolved conflicts (Box 4). This can usually be distinguished by a therapist who has gone through a process of self-knowledge and minimized their own “blind spots”.36
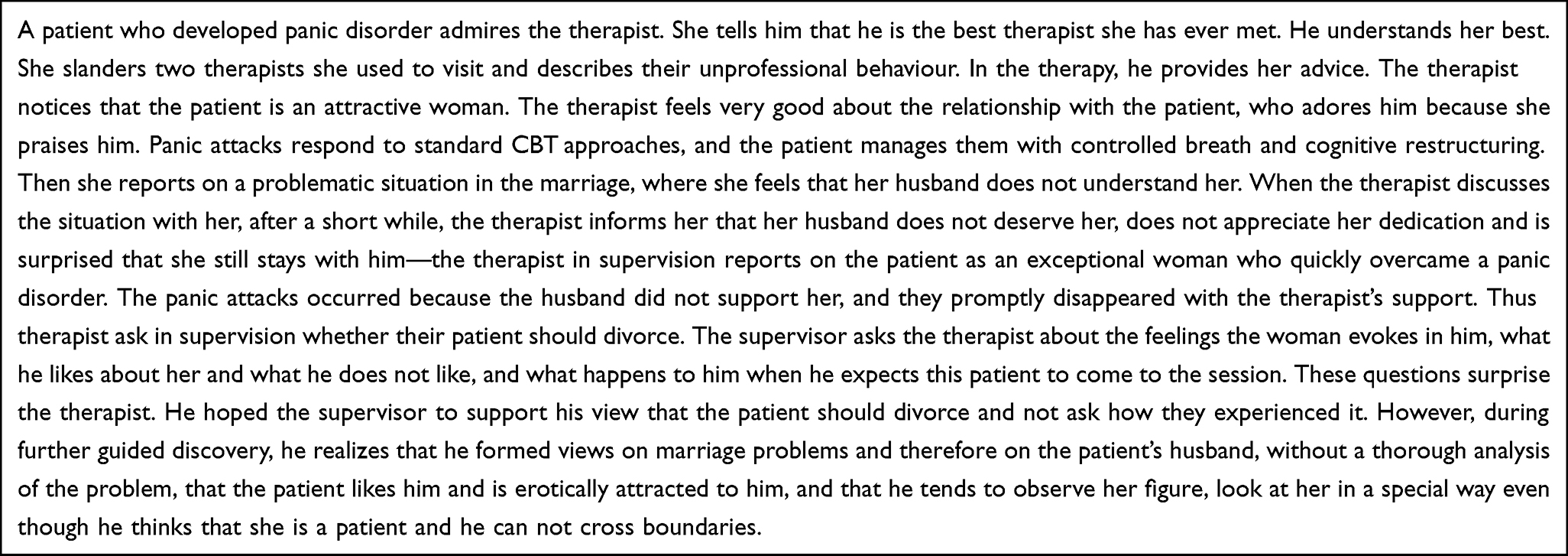 |
Box 4 Case Vignette - Patient Admires the Therapist Who Developed Countertransference |
If the reactions to the patient are intensive, and the therapist does not understand them, it is often a transference to the patient. However, in the literature, countertransference and transference to the patient are not differentiated because they may look similar. Only the internal sources are different. Therapeutic responses to the patient may stem from many sources, including cultural values, the therapist’s view of their professional role and unique learning history, and interactions with the patient’s problematic behaviour.3,52 During countertransference, the therapist may be subject to various automatic thoughts with typical cognitive errors: “This patient is hysterical.” (Labelling); “He only wants secondary profits.” (Mind-reading); “He’ll never get better.” (Negative forecasts); “It’s not improving at all.” (All or nothing thinking); “It’s my fault that the patient is no better.” (All or nothing); “He should do his homework.” “I have to try harder.” “It won’t get better.” (Excessive generalization). According to Hadley (1980),86 the therapist’s hostile “countertransference” to the patient can be expressed in various ways:
- Lack of respect for the patient’s suffering
- An obstacle to the establishment of a working alliance
- Failure to allow the patient to experience a choice between options
- Aggressive attacks on patient defences
- Feelings of disappointment over the patient and their progress
- Slandering the patient in front of other therapists.
Betan et al (2005)53 studied a national random sample of 181 psychiatrists and clinical psychologists in the United States. Each completed a battery of tools on a randomly selected patient in their care, including Axis II symptom measurements and a Countertransference Questionnaire, designed to assess physicians’ cognitive, affective, and behavioural responses when interacting with a particular patient. Factor analysis of the countertransference questionnaire yielded eight clinically and conceptually coherent factors that were independent of clinicians’ theoretical orientation: (1) overwhelmed/disorganized; (2) helpless/inadequate; (3) positive; (4) special/excessive; (5) sexualized; (6) disconnected; (7) parental/protective; and (8) critical/abusive.
Eight factors were associated predictably with personality disorder patients. Countertransference patterns have been systematically associated with patients’ personality difficulties across therapeutic approaches. Therapists may use diagnostic and therapeutic responses to the patient, regardless of therapeutic orientation.53 Robert Leahy (2003)39 described typical countertransference problems, which include: feelings of guilt or fear due to a patient’s anger; lack of strength in collecting fees or enforcing rules; excessive session extension; Catastrophization of the patient’s hospitalization options; inhibition in obtaining a sexual history; uncertainty when the patient is sexually attractive, inability to set boundaries for sexually provocative or hostile patients, etc.
Some patient problems, such as feelings of abandonment, addiction, tendency to devalue oneself or others, great difficulty, sexual interest, abuse, feelings of victimization or betrayal, or trends to exploit others, can arouse these problems in the therapist’s feelings and vulnerabilities.39
The individual schemes of the therapist significantly affect the countertransference. In addition, some patients activate certain schemes more often than others.Leahy (2003)39 describes common problematic therapists’ schemes:
Unrealistic Standards
Therapists with anankastic or perfectionist traits repeatedly perceive patients as irresponsible, self-reliant, and lazy. A therapist with unrealistic standards believes that emphasizing “rationality” and insisting on discovering the consequences can help patients. Therapists-perfectionists may try to compensate for their underlying incompetence by requiring perfect performance from themselves and the patient. The therapist might feel that therapy is simply an opportunity to show that they are more intelligent or perfect than the patient. A typical sequence of automatic thinking might be, “My patient isn’t getting better.” “I’m not doing my job well enough.” “Turns out I can’t do it.” “I failed.” “I must not fail.”
Abandonment
A therapist with an abandonment scheme will fear that the patient will leave the therapy if confronted with something painful, emotionally strong or adverse. They then interpret the premature termination of therapy by the patient as a personal failure. Therapists’ abandonment can manifest themselves in various ways that reflect countertransference: on the one hand, through excessive care about the patient or, on the other hand, by avoiding a meaningful therapeutic relationship so that they do not become too attached themselves and then experience disappointment. Excessive care takes the form of trying to protect the patient from any problem, taking over responsibility for the patient, and solving problems. Therapists who avoid attachment often focus on superficial techniques rather than more meaningful personal matters. This type of therapist avoids difficult topics, exposure to traumatic events, working with mourning, or using exposure techniques. They often say that the patient is not yet ready for more emotionally demanding situations in therapy. They usually accept late patient arrivals, missed meetings or a lack of interest in therapy and accept them as mistakes. They consider the patient’s resistance to be their failure.
Speciality, Superiority
The narcissistic therapist sees therapy as an opportunity to show their special talents. Therapy can begin by raising great hopes, telling the patient that they have finally found the “right therapist.” Emphasizing themselves as special, perfect therapists can lead to the patient falling by the wayside. The therapist’s goal is to show that they are the best. This type of therapist feels entitled to the patient’s admiration. They may encourage the patient to break the boundaries, or the therapist may break the boundaries themselves in some cases. When the patient does not improve quickly, the narcissistic therapist gradually becomes bored, angry, or punishing. They can label a patient as “borderline, histrionic, paranoid, hypochondriac … ” Rather than empathizing with the patient’s understandable frustration of lack of progress. The therapist may accuse them of lacking a desire to improve. The first step to changing the narcissistic perspective is asking: “What would my life look like if I were in this patient’s skin?”. The narcissistic therapist needs personal therapy.
The Need for Approval and Consent
Approval-seeking therapists express empathy all the time. They want the patient to feel good despite what happens and never be angry with the therapist. Many patients appreciate the commitment and empathy of such a therapist. This therapist does not ask about substance abuse, anger, resentment, sexual dysfunction or self-harm, finding these topics too stressful. They fear the patient’s negative reaction. Patients may miss sessions, be late, and do no homework, but a therapist with a high need for approval does not want to cause a “conflict” and tries to excuse the patient’s maladaptive behaviour. Eg, the therapist found it difficult to decide on hospitalization for a suicidal patient because they feared the patient would be angry with them. The patient’s anger is difficult to tolerate. Therefore, the therapist’s behaviour has to be adapted at any cost. They see the patient’s disapproval as a sign of the therapist’s failure. “If a patient gets angry at me, it means I’ve failed.”
Avoidance of Personal Problems
In some cases, focusing on the patient’s issues may allow the therapist to avoid their emotional issues or enable the therapist to pass on their conflicts to the patient.39 Some people are attracted to the profession of therapists because it gives them a sense of competence, superiority and obvious effectiveness (Box 5). This illusion of competence can allow the therapist to unknowingly pursue goals other than the patient’s, such as satisfying the need for power or control or separating, intellectualizing, and isolating oneself from one’s problems.
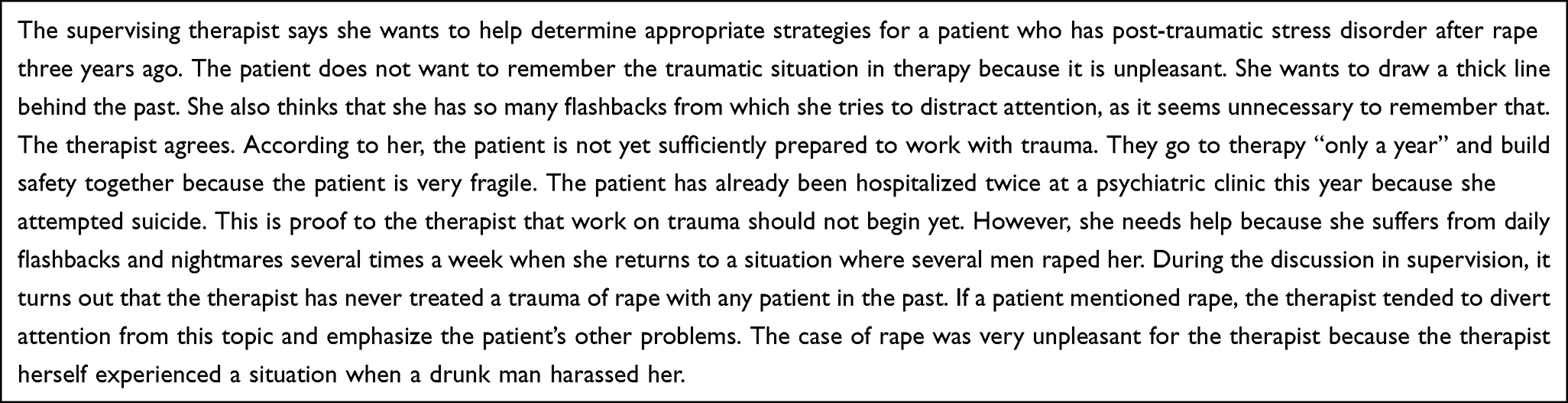 |
Box 5 Case Vignette - Countertransference Induced by Therapist´s Own Negative Experience |
Supervision of the Therapist’s Countertransference to the Patient
The first step in managing countertransference is to realize that the therapist feeling toward the patient is significant, either positively or negatively. During therapy, the therapist must try to help the patient and, at the same time, monitor their reactions to the patient.2 Recognizing countertransference helps the therapist identify how they are likely to respond to the patient’s behaviour.39 The supervisor encourages a therapist to use cognitive behavioural strategies, awareness of their physical feelings and subtle mood swings as stimuli that point to automatic thoughts. They also need to focus on their feelings and thoughts or behaviours. Any changes in the therapist’s typical behaviour can signal the emotional response and be related to automatic thoughts. These include commanding, excessive pressing, indecisiveness, altered tone of voice, excessive thinking about the patient outside the meeting, mood swings when realizing that the patient will come to the session, avoiding answering e-mail, or problems ending the session and treatment in general.
They must pay special attention to recognizing emotional reactions to the patient, both positive and negative (Box 6). It is an opportunity to ask themselves how much the patient is processing corresponds to their own previous experience or pre-existing opinions.
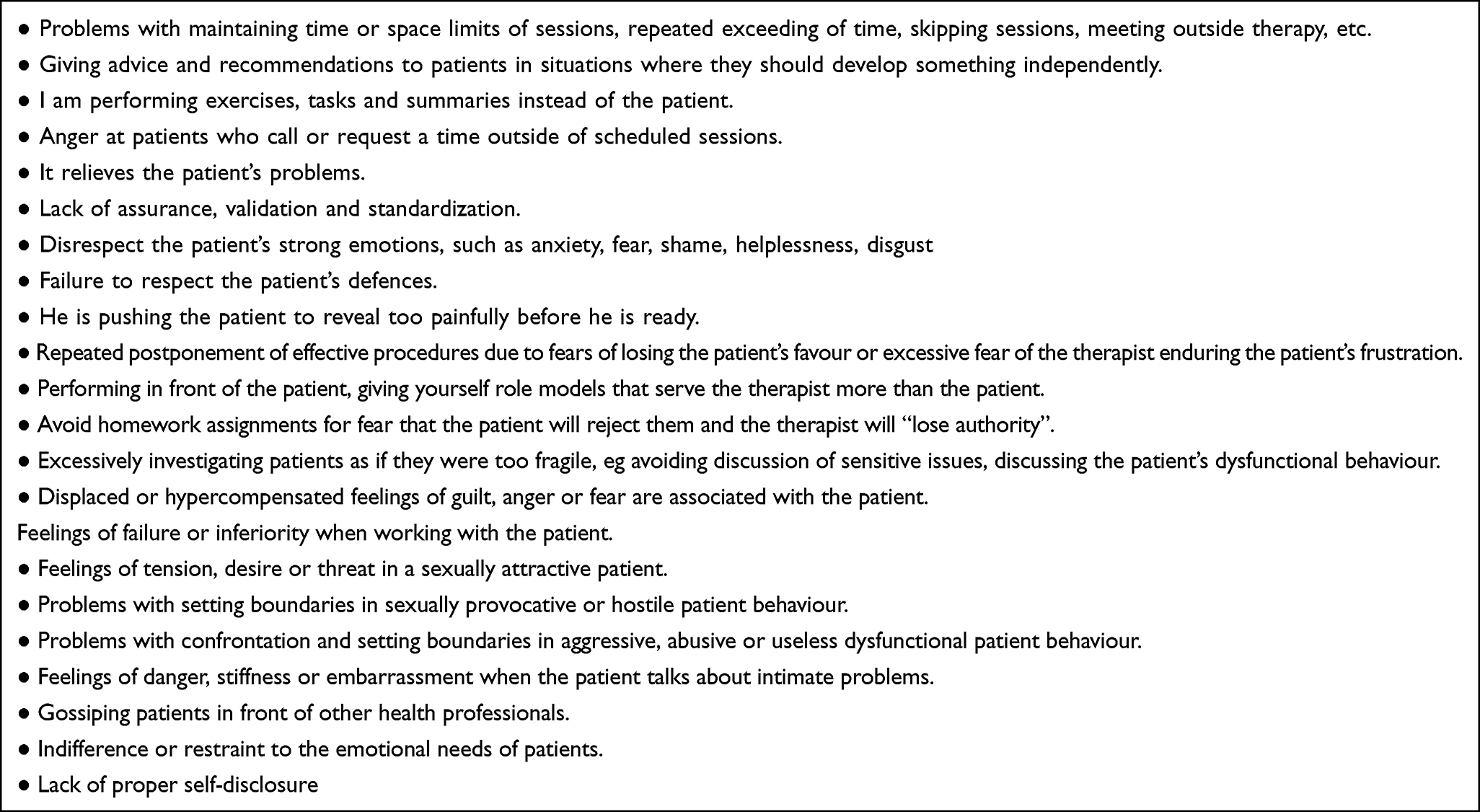 |
Box 6 Examples of Typical Countertransference Problems |
The Use of Education When Working with the Therapist’s Countertransference to the Patient
Education about countertransference is one of the topics in psychotherapeutic training. However, it may be important to supervise novices to educate them about countertransference or refer them to the literature about it (Table 2). The problem for beginners in therapy is that they frequently think that every countertransference is negative and is therefore ashamed to talk about it or immediately displace signals about its presence.54,55 The supervisor should inform that countertransference is a natural part of the therapy (Table 2). Recognizing it, mapping it and correcting it for the patient’s benefit is one of the basic competencies of an experienced psychotherapist.53 The supervisor could tell the therapist about the basic types of countertransference and ask them if it happened to them with a patient and their cognition, emotional reactions, and behaviour (Prasko et al 2020).87 The supervisor then focuses on the specific supervised patient, and the therapist is asked to consider whether any countertransference with the patient is being experienced.2
 |
Table 2 Examples of the Countertransference and Possible Strategies for a Change |
The therapist’s transference reactions can inform us what is happening in the patient’s therapy process. At the critical points in developing transference and countertransference and their interactions, therapeutic recognition and dealing with countertransference problems become crucial to treatment.4
Use of Guided Discovery to Map a Therapist’s Countertransference to a Patient
Psychotherapy and supervision intend to understand both sides and include this understanding in joint action. Self-reflection is advised in therapy and supervision.2 An important goal of supervision is to increase the therapist’s self-reflection to use it automatically during therapy. Self-reflection is enhanced by updating (in the imagination, role-playing) a specific situation with the patient.56,57 To increase the ability to see problematic conditions directly in the session, the supervisee is sometimes given the homework to record the situation with the patient where they feel dissatisfied with the patient, themselves or both of them. A therapist who is unaware of or suppresses any of their feelings cannot understand what is happening between them and the patient.
Through guided discovery, imagination, or role-playing, the supervisor can help the supervisee recognize what is happening in the therapist-patient relationship, both from the therapist’s and the patient’s point of view. The most common approach to discovering the context is guided inductive questioning, during which the supervisee can realize what may not have been considered previously.57 The patient’s understanding may deepen and change significantly.
Cognitive Restructuring to Help with the Therapist’s Countertransference to a Patient
Supervision allows the therapist to delve deeper into the patient’s thoughts, emotions and reactions and seek and process countertransference reactions that potentially block therapy. Eg, the therapist may feel frustrated, angry, anxious or threatened by the patient’s demands, or maybe convinced that the patient is lazy or stupid, is not doing homework on purpose, is undergoing therapy due to secondary gains, or that therapy is impossible (Box 7). Alternatively, the therapist talks about the patient in superlatives, admires them, feels sorry about them excessively, and identifies with their maladaptive attitudes. When questioning therapists’ automatic thoughts, the supervisor helps them and identifies with their patient-centred strings and then tests those thoughts.2
 |
Box 7 Case Vignette - Countertransference with the Complaining Patient |
To examine countertransference, the therapist needs to be aware of their core patterns towards themselves, other types of beliefs, and problems with important people in their life that they have had or have currently and who are involved in creating or maintaining these patterns. Personal therapy is suitable for processing difficult problems, and it is important to understand what schemes are triggered when working with the patient or what important people in their own life can be evoked in supervision. The supervisor can use guided discoveries, role-playing or imagination to make the therapist aware.
Inductive questions focused on countertransference are listed in the following table (Box 8).
 |
Box 8 Supervisor’s Questions for Countertransference |
The way therapists respond to a patient’s situation may require cognitive restructuring, which can help reduce negative emotions with the patient or change their behaviour toward the patient to maintain an appropriate focus on therapeutic goals and objectives.22 The supervisor helps the therapist face concerns that their emotions signify therapy failure. Instead, the supervisor teaches them to focus on what precedes the emotional state in the patient’s behaviour and how it relates to the therapeutic setting.
Cognitive restructuring, one of the common strategies when working with patients, is also used in supervision. However, guiding a therapist through cognitive restructuring can sometimes be difficult because it can make the supervisee feel like the supervisor is treating them as a patient. However, in situations where the therapist is blinded by a one-sided view of the problem or overestimates the difficulties experienced in the case with the patient, or obvious cognitive errors are apparent, cognitive restructuring is appropriate. However, the supervisor must directly jump to what they, as a therapist, would do. As the most common form of cognitive restructuring in supervision, Socratic dialogue is based on the assumption that individuals will change their beliefs more quickly and competently when they find mistakes in their thinking through guided discovery.58 It is much more effective than criticism. Cognitive restructuring can be especially helpful when the therapist feels hopeless or unaware of the transference. When using cognitive restructuring in supervision, it is advisable to normalize the process.43 An uncertain supervisor can try humorously: “Let us try something you do regularly with patients and take a look at the pros and cons. Can we try?” Cognitive restructuring can help, especially when the therapist feels in a hopeless situation or when they are not aware of the transference (Table 3).
 |
Table 3 An Example of Cognitive Restructuring of a Situation Where the Therapist is Angry with the Patient |
Supervision also helps the therapist deal with negative feelings about the patient or themself in a therapeutic situation, understand the broader context of therapy, overcome therapeutic blocks, and encourage more self-care.
Using Imagination to Map a Therapist’s Countertransference to a Patient
Imagination is a means of supervision that allows the return to a specific situation in therapy during a supervision session and the imagining of another solution. It is possible to imagine how the patient looked or behaved in a certain situation and remind the therapist about their emotions. It is possible to imagine the patient’s reaction, including remembering the emotional state and physical symptoms in therapy.2 With the help of imagery rescripting, it is possible to return to a previous situation with similar emotions in the past, rescript this situation with a better end and return with emotions from the rescribed situation to the situation with the patient and solve it another way (Box 9).
 |
Box 9 Case Vignette - Stay a While with the Feelings to Understand Countertransference |
Use of Role-Playing to Map a Therapist’s Countertransference to a Patient
Role-playing can be a good method to map a therapist’s countertransference to a patient, as it presents in the therapy session. The supervisor usually asks the therapist to describe a particular therapy situation where the therapist feels powerful positive or negative emotions. Supervisor then asks the therapist to play with the patient, and the supervisor plays the described behaviour of the therapist. The supervisor asks how the therapist, in the role of the patient, felt what they experienced and what they realized. This is followed by a change of roles, where the therapist plays themself, and the supervisor plays the role of the patient. This allows the therapist to experience the therapeutic situation from both sides and return the therapist to the part of the role play where they perceived that the therapist was experiencing the strongest emotions. The supervisor asks the therapist if they remember a situation where similar emotions were experienced, with whom it happened, and what they felt towards the person. The supervisor asks how the therapist would like to deal with this past situation to feel good or help them feel good (this is also possible in the imagery – imagery rescripting). Then they play a new reformulated situation again. The supervisor asks about the feelings after playing the rescripted situation. With these emotions, the therapist then returns to the situation with the patient and tries to replay it in a new way.
Use of Problem-Solving to Process the Therapist’s Countertransference to the Patient
What to do with the patient’s transference to the therapist or the therapist’s countertransference to the patient is a regular part of the supervision of the therapeutic relationship. First, it is necessary to define the problem they got into with the patient in a therapeutic relationship and then establish the therapist’s goal. The goal should be, if possible, specifically descriptive, realistic and manageable in the foreseeable future. The supervisee could use the following brainstormed strategies to ensure that transference or countertransference does not block therapeutic work. Evaluating individual strategies according to whether they are appropriate is work that the supervisor should do. They then discuss the final plan created together. In subsequent sessions, they evaluate how the plan was feasible and worked.
Use of Homework to Process the Therapist’s Countertransference to the Patient
Homework may include reading what types of transference and countertransference exist and writing examples of patients with whom the supervisee identifies the transference and countertransference. These may be cases they became aware of in the past and became mindful of transference and countertransference during supervision.
Keeping a record of automatic thoughts that occurred to the supervisee during therapy and finding a more adaptive response may also be a homework assignment. Paying attention to these countertransference reactions at home provides the therapist with the opportunity to recognize and manage them. This reduces the risk of complementary behaviour.45
Therapist’s Transference to Supervisor
The supervision relationship is based on analogous principles to the therapeutic relationship, emphasizing independence, responsibility, and self-sufficiency.59 The source of every development is the spirit of safety, acceptance and appreciation.60,61 As in the therapeutic relationship, transference and countertransference also arise in the supervisory relationship. During the therapeutic maturation of the supervisee, the intensity of supervision increases.54 The onset of supervision is usually associated with a certain dependence on the supervisor, but the supervisor can reduce this by self-opening and thus create a cooperating alliance of two partners.48,62
Manifestations of the Therapist’s Transference to the Supervisor
Manifestations of the therapist’s transference to the supervisor are similar to those described for the patient’s transference to the therapist. The transference relationship between the supervisor and the supervisee in CBT supervision is not encouraged.43 Nevertheless, we can expect a similar development in the supervision process as in all other relationships. Defence mechanisms, resistance, transference, and countertransference emerge and tend to evolve, and they must be reflected in the supervisory relationship as the therapist learns to deal with them.36,63
Supervision of the Therapist’s Transference to the Supervisor
Many methods help develop an awareness of the therapist’s transference to the supervisor. The therapist’s transference relationship with the supervisor can be tested in the here and now experience in a supervisory relationship. The supervisor must first ask themselves if they see the therapist’s transference as a natural and productive phenomenon (eg, a submissive relationship with the novice supervisor) or if there are potential negative effects of the transference (becomes dependent on the supervisor, relies on the supervisor asking the responsibility for the patient to the supervisor).48 The supervisor also needs to consider whether the therapist’s transference interferes with the cooperation in supervision, whether it blocks it or harms how the therapist performs the therapy.41 Adaptive correction of the transference relationship, when the therapist tests dysfunctional expectations from the supervisor in the reality of the supervisory relationship, usually changes the view of oneself, increases self-acceptance and changes the relationship with other people, especially authorities and loved ones (increased trust and cooperation) (Sareen and Skakum 2005).88 Interpersonal maladaptive thoughts, such as “others reject incompetent people” and core beliefs about the self, for example, “I am incompetent”, can be corrected when working with the transference of a supervisee,39 Rabinovich and Kacen 2009)89
Use of Education to Map the Therapist’s Transference to the Supervisor
First of all, the therapist must realize that transference is a natural phenomenon in supervision and does not need to be feared; on the contrary, it can help understand the therapy itself and supervision and provide a deeper understanding of one’s personality.4 The supervisor advises the therapist on the literature about transference and countertransference. Then they ask the therapist about experiencing some moments in supervision that reminds them of other life situations - for example, when the supervisee reacted in the last supervisory session with a sudden mood change.
Use of Guided Discovery to Map the Transference of a Therapist to a Supervisor
Guided discovery is one of the most common approaches by supervisors and supervisees to map transference and countertransference both in therapy and in supervision sessions.56,59 Guided discovery helps shape and modulate the supervisory relationship by creating an atmosphere of security, acceptance, understanding and appreciation.57,64,65
Supervisor Countertransference to the Therapist
Unconscious countertransference reactions in supervision can lead to serious doubts about the supervisor, limit supervisees’ self-confidence and discourage them from working with patients, or, conversely, exacerbate their intractable problems in dealing with patients.4,50 Analogously, as a therapist may have significant power over the patient, the supervisor may have uncontrolled power over the supervisee (Box 10). Therefore, the supervisor must recognize and process their countertransference responses during supervision.9
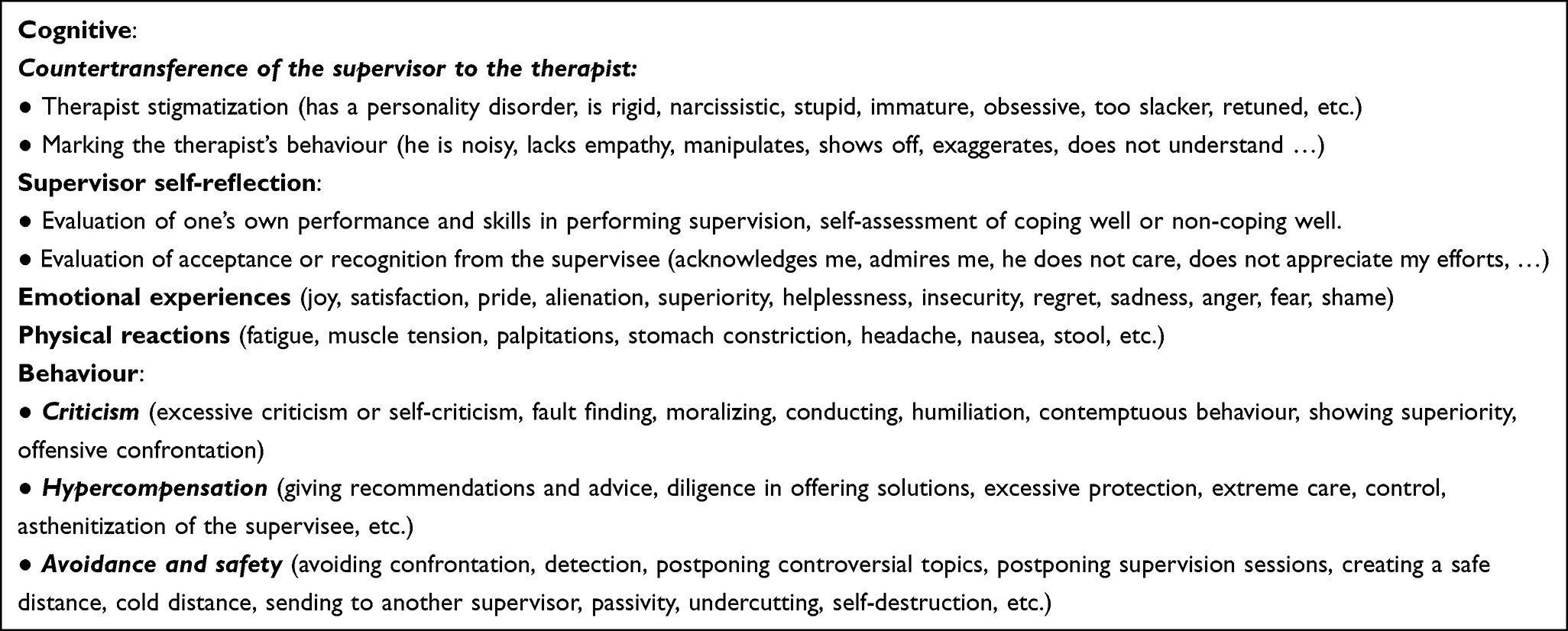 |
Box 10 Examples of Countertransference Reactions in Supervision |
Manifestations of Countertransference of the Supervisor to the Therapist
The supervisor may notice the countertransference reaction primarily in their behaviour towards the supervisee and in emotions, thoughts, and physical symptoms. Often the bodily responses experienced by the supervisor point to emotional motives that they may not be fully aware of at the moment or distract from them because they are uncomfortable for some reason.50,66 Muscle tension, stomach contraction, shortness of breath, headache, and change in tone of voice may indicate changes in emotions and thoughts concerning the supervisee. Other manifestations, such as feelings of unsafety, urgency, too many instructions, reluctance to supervise, prolonging sessions or, conversely, shortening, may also be typical manifestations of countertransference reactions.50,67 Countertransference is either a reaction to the behaviour of the supervised therapist or can be influenced by the supervisor’s core beliefs and conditional rules. In this context. Leahy (2003)39 described the following schemes:
Unreasonable Standards
Some supervisors need everything to be perfect and look into the therapist for mistakes, not to see what they are doing. Supervisors with anankastic features see supervisees as ill-prepared, unreliable, untrained, irresponsible, or lazy. They also think that showing their anxiety, admitting mistakes, and expressing their own emotions can be threatening or devastating.4 They emphasize “logical”, “constructive”, or “rational” thinking, detailed analysis, and protocol tracking accuracy. They tend to have difficulty showing understanding, kindness, warmth and empathy for the supervisee. They often refer to theory, evidence-based approaches, and studies, speak little about themselves and have problems expressing personal perspective or self-reflection. In supervision, they try to find mistakes by the supervisee, have catastrophic comments, and use moralistic remarks. The perfectionist supervisor often unknowingly tries to compensate for their unsafety by controlling and demanding perfect presentation from themselves or the supervisee.
In some cases, the sequence of automatic thoughts may look like this: “How can she make such mistakes!”, “What the hell do they teach her in that training?” “She’s not preparing for supervision at all!”
Abandonment
A supervisor who does not sufficiently work with their abandonment scheme in their personal therapy may still be concerned that they may discourage the supervisee. They are afraid that the supervisee will criticize them, saying that the supervision does not help them. They are so scared to indicate that it is necessary to look for a different strategy when working with the patient because they fear that the supervisee will not like them and leave them. Premature termination of supervision is considered a personal refusal of the supervisor. Under the influence of their abandonment scheme, the supervisor can behave in various ways that reflect this scheme: for example, they can over-care for the supervisee, explain too much, and apologize, but on the other hand, they can avoid making a meaningful contract. Extreme care can protect the supervisee from any difficulties, giving advice, putting off negative feedback, or a preferential solution to the supervisee’s problems that they have in common with the supervisor. Such a supervisor avoids more difficult topics and anxiety-provoking interventions. They often react painfully to the supervisee’s different views, omitting supervision sessions or lacking interest in supervision. The supervisee’s disagreement is often perceived as a personal rejection.
The Need for Exceptionality
A supervisor with narcissistic personality traits sees supervision as a chance to show exceptional talent. They are convinced that they understand everything and have to teach the supervisee, and they often do not realize they are showing off. Supervision of a complex case may begin with grandiose remarks that it is clear how to treat such a patient because the supervisor had many similar patients and cured them all beautifully, even though most therapists had failed before. They can also tell the supervisee that they have finally found a “true supervisor” who will help them solve everything. The supervisor is very happy to advise and knows the solution to all problems. In such cases, the supervisee feels pressured to cooperate with and admire the supervisor, encouraging them to make surprising interventions. Changing the narcissistic perspective is difficult because it tends always to see mistakes in others.
Excessive Need for Acceptance
A “likeable” supervisor is usually friendly and empathetic. The supervisor is constantly trying to please, and they believe that the supervisee should feel good no matter what happens. Supervisees generally appreciate the warmth and empathy of such a supervisor because they never express negative emotions and do not confront shortcomings. This type of supervisor usually avoids questions about the supervisee’s negative emotions, and as these topics upset the supervisor, they become unacceptable The supervisee may be late, not doing homework, or skipping scheduled sessions, but the supervisor with an excessive need for acceptance does not want to “provoke a conflict” and tolerates it all. If the therapist fails in the therapy, the supervisor tends to accuse them of their inability to lead the therapist well enough in supervision. Their attitude tells them that “if a therapist fails, it is my failure.”
As the supervisor recognizes their emotional responses to the supervisee, they may consider how the therapist can partially respond to patients. They can talk about a parallel process, where the patient evokes similar reactions in the therapist, and the therapist may induce this in the supervisor.
Supervisor’s Transference to the Patient
The therapist’s narrative may trigger a supervisor transference to the patient. The supervisor can then create artificial explanations of the patient’s behaviour based on inadequate information, label the patient, be angry with them, or create inadequate interpretations about the patient’s behaviour, eg, say that the patient is manipulated or that they are a typical patient with social welfare tendencies.
Possibilities of Working with the Supervisor’s Countertransference to the Therapist
Awareness of One’s Own Countertransference to the Therapist
The first stage of countertransference is when the supervisor realizes that their feelings toward the supervisee are positive or negative.56,67,68 It is advisable to take some time outside the supervision setting to answer a few questions patiently (Box 11).
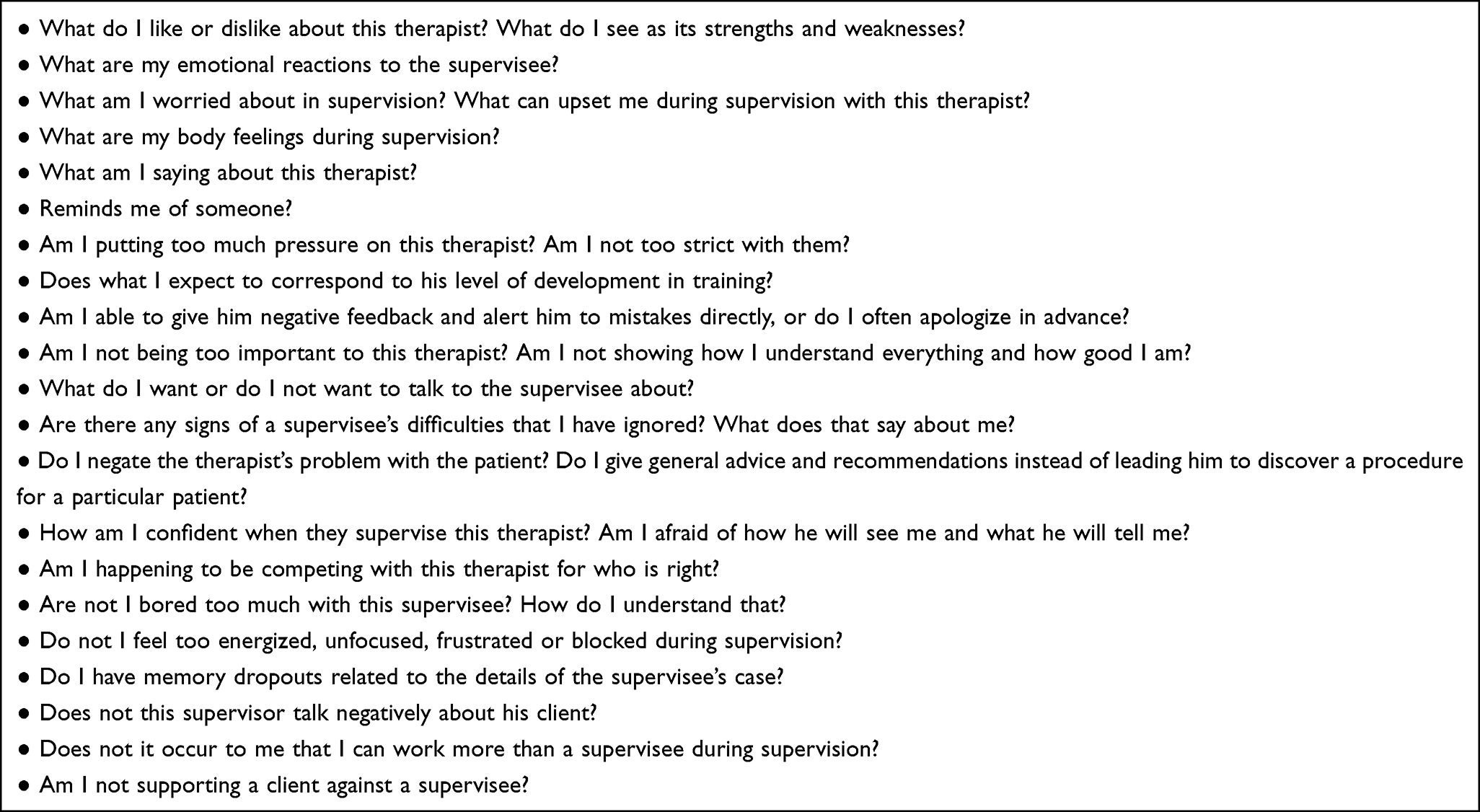 |
Box 11 Questions for Self-Reflection About Countertransference |
Recognizing countertransference in supervision requires the supervisor to be constantly aware of their thoughts and attitudes, which influence how they respond to the supervisee’s behaviour.67,68 It is advisable to write down a self-reflective awareness. Rather than suppressing one’s own emotions, the CBT supervisor is led to pay attention to them and consider how they appear in the supervision and what thoughts and attitudes they are tied to.
Another phase may be looking for discussion with another supervisor to help investigate in-depth and potentially resolve the cause of strong countertransference. To evaluate countertransference, the supervisor may inspect the life difficulties they experience. Have they experienced abandonment or rejection during life? Then the supervisor might examine to what extent similar feelings appear in interaction with the therapist. Does it occur that they permanently have to be “right”? Then it is necessary to realize whether he repeatedly “defeats” the supervisee in their debates since this would decrease their self-confidence. Are they too anxious about failing or being criticized in their life because they think that failures or successes are related to their value as a person?
Cognitive Restructuring of the Supervisor
The supervisor’s work with thoughts related to supervision may result in cognitive restructuring to reduce negative or excessively positive feelings. It is valuable to challenge any fear of making a supervision mistake and recognize what preceded these worries (Table 4). The supervisor’s responses may come from numerous sources, including cultural values and attitudes, their professional role and individual life experiences, including training, or may be activated by contact with the supervisee and their behaviour.3
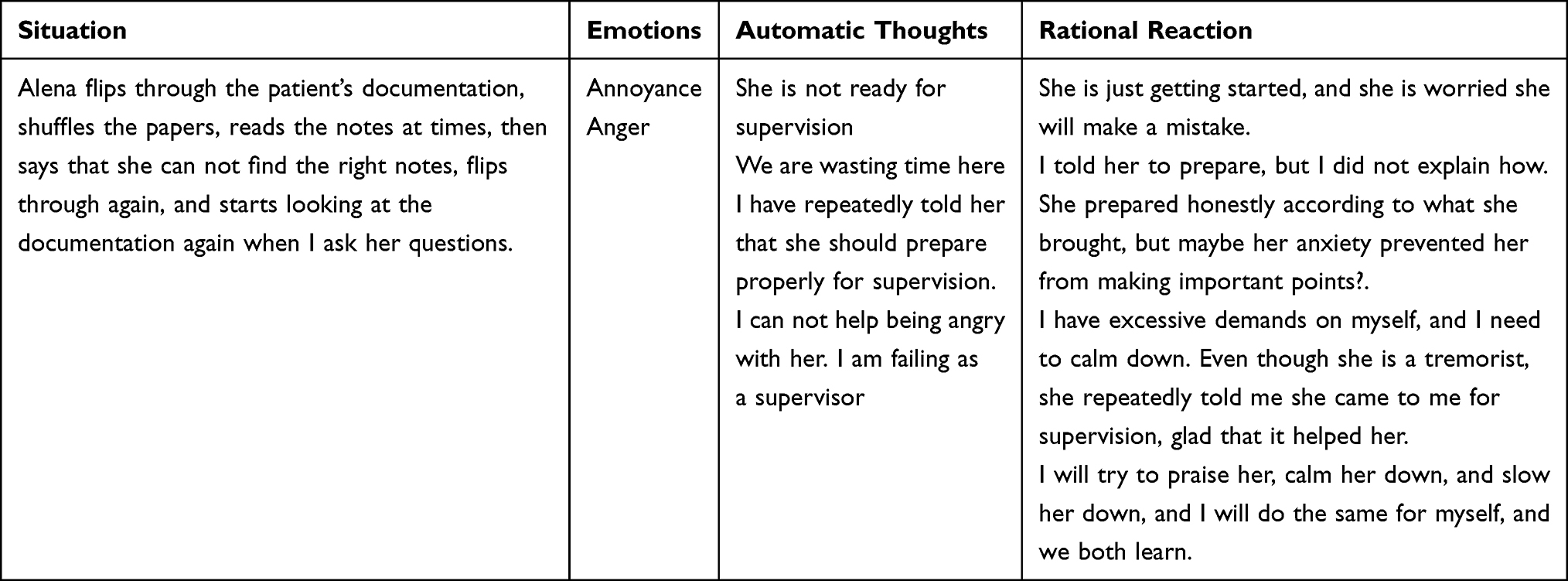 |
Table 4 Four-Column Record of Supervisor’s Dysfunctional Thoughts |
Another way how to make a cognitive reconstruction is also by asking to identify triggers and then:69
- What type of client has regularly “gotten to you” in your career?
- How do these people put your abilities to the test?
- Have you ever cooperated with a client due to a countertransference attraction or an overidentification of their problems?
- What do you anticipate from all of your clients, even if they appear unwilling or unable to perform at times?
- What exactly is the source of your and your client’s disagreement?
- How does this conflict ring true in your life? What does it make you think of?
- How do you want things to go?
- What can you do to bolster your resolve?
- Are you willing to make any specific changes?
- What have you done time after time that has not worked?
- What are three alternatives you may use?
Supervisor’s Supervision
Like a therapist, a supervisor may encounter problems supervising the supervisee that they do not fully understand or cannot solve.4 It is time to find their supervisor and discuss the supervision they do. Supervision of beginning supervisors is one of the obligatory components of supervisor training.
Conclusions
Transference and countertransference are important to monitor in therapy and supervision, and if they block therapy or lead to other problems, they need to be understood and processed. Transference mapping aims to improve the patient’s interpersonal functioning and remove blocks in therapy. Transference work in CBT seems to be especially important for patients with long-term problematic interpersonal relationships. Countertransference can block or push therapy beyond the benefit of a therapeutic relationship, but mapping it can be a valuable tool for understanding how people around the patient can respond to them.
The only method of identifying countertransference throughout supervision is constant alertness of the supervisor’s opinions and attitudes that impact their response to the supervisee’s behaviour. Rather than control their own emotions, the CBT supervisor is guided to notice them and consider their procedure in their supervision and which thoughts and attitudes they are related to.
Acknowledgments
This paper was supported by the research grant VEGA no. APVV-15-0502 Psychological, psychophysiological and anthropometric correlates of cardiovascular diseases.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Goin MK. A current perspective on the psychotherapies. Psychiatric Services. 2005;56(3):255–257.
2. Gilbert P, Leahy RL. The Therapeutic Relationship in Cognitive-Behavioral Therapy. London, England: Routledge-Brunner; 2007.
3. Kimmerling R, Zeiss A, Zeiss R. Therapist emotional responses to patients: building a learning-based language. Cogn Behav Pract. 2000;7(3):312–321.
4. Prasko J, Dicevicius D, Ociskova M, et al. Therapeutic and supervision relationship in cognitive behavioral supervision. Act Nerv Super Rediviva. 2021a;63(1):22–35.
5. Kernberg OF. Psychoanalytic supervision: the supervisor’s tasks. Psychoanal Q. 2010;79(3):603–627.
6. Stefana A. The origins of the notion of countertransference. Psychoanal Rev. 2015;102(4):437–460.
7. Raue PJ, Goldfried MR, Barkham M. The therapeutic alliance in psychodynamic-interpersonal and cognitive-behavioral therapy. J Consult Clin Psychol. 1997;65(4):582–587.
8. Swales MA, Heard HL. Dialectical Behaviour Therapy. London and New York: Routledge; 2009.
9. Zepf S, Hartmann S. Some thoughts on empathy and countertransference. J Am Psychoanal Assoc. 2008;56(3):741–768.
10. Høglend P. Analysis of transference in psychodynamic psychotherapy: a review of empirical research. Can J Psychoanal. 2004;12(2):279–300.
11. Kernberg OF. Reflections on Supervision. Am J Psychoanal. 2019;79(3):265–283.
12. Gabbard GO, Wilkinson SM. Management of Countertransference with Borderline Patients. Washington, DC: American Psychiatric Press; 1994.
13. Gelso C. A tripartite model of the therapeutic relationship: theory, research, and practice. Psychotherapy Res. 2014;24(2):117–131.
14. Watkins CE. Toward a tripartite vision of supervision for psychoanalysis and psychoanalytic psychotherapies: alliance, transference-countertransference configuration, and real relationship. Psychoanal Rev. 2011;98(4):557–590.
15. Gluhoski V. Misconceptions of cognitive therapy. Psychotherapy. 1994;31(4):594–600.
16. Beck AT, Rush AJ, Shaw BF, Emery G. Cognitive Therapy of Depression. Guilford: New York; 1979.
17. Beck JS. Cognitive Therapy: Basics and Beyond. Guilford: New York; 1995.
18. Persons J. Cognitive Therapy in Practice: A Case Formulation. New York: WW Norton; 1989.
19. Aubuchon PG, Malatesta VJ. Managing the therapeutic relationship in behavior therapy: the need for a case formulation. In: Bruch M, Bond FW, editors. Beyond Diagnosis. Case Formulation Approaches in CBT. Wiley, Chichester; 2003:141–166.
20. Wills F, Sanders D. Cognitive Behaviour Therapy: Foundation for Practice. Sage: London; 2013.
21. Beck AT. Cognitive Therapy and the Emotional Disorders. Madison, CT: International Universities Press, Inc; 1975.
22. Beck AT, Freeman A. Davis DD and Associates: Cognitive Therapy of Personality Disorder.
23. Newman CF. Core Competencies in Cognitive-Behavioral Therapy: Becoming a Highly Effective and Competent Cognitive-Behavioral Therapist. Routledge/Taylor & Francis Group; 2013.
24. Ryle A. Transferences and countertransference: cognitive analytic therapy perspective. Br J Psychotherapy. 1998;14(3):303–309.
25. Leahy RL. The therapeutic relationship in cognitive-behavioral therapy. Behav Cogn Psychother. 2008;36(6):769–777.
26. Safran JD, Moran JC. Negotiating the Therapeutic Alliance: A Relational Treatment Guide. New York: Guilford; 2000.
27. Miranda R, Andersen SM. The therapeutic relationship: implication from social cognition and transference. In: Gilbert P, Leahy RL, editors. The Therapeutic Relationship in the Cognitive Behavioral Psychotherapies. NY: Routledge; 2007:63–89.
28. Leahy RL. Schematic mismatch in the Therapeutic relationship: a social-cognitive approach. In: Gilbert P, Leahy RL, editors. The Therapeutic Relationship in the Cognitive Behavioral Psychotherapies. Routledge, NY; 2007:229–254.
29. Bennett-Levy J, Thwaites R. Self and self-reflection in the therapeutic relationship: a conceptual map and practical strategies for the training, supervision and self-supervision of interpersonal skills. In: Gilbert P, Leahy RL, editors. The Therapeutic Relationship in Cognitive-Behavioural Psychotherapies. New York: Routledge; 2007:255–282.
30. Cartwright C. Transference, countertransference, and reflective practice in cognitive therapy. Clinical Psychologist. 2011;15:112–120.
31. Hayes JA, Gelso CJ, Goldberg S, Kivlighan DM. Countertransference management and effective psychotherapy: meta-analytic findings. Psychotherapy. 2018;55(4):496–507.
32. Stefana A, Bulgari V, Youngstrom EA, Dakanalis A, Bordin C, Hopwood CJ. Patient personality and psychotherapist reactions in individual psychotherapy setting: a systematic review. Clin Psychol Psychother. 2020;27(5):697–713.
33. Rogers CR. Client-Centred Therapy – Its Current Practise, Implications, and Theory. Boston: Houghton Mifflin Company; 1965.
34. Schneider KJ, May R. The Psychology of Existence. An Integrative, Clinical Perspective. New York: McGraw-Hill; 1995.
35. Andersen SM, Przybylinski E. Experiments on transference in interpersonal relations: implications for treatment. Psychotherapy. 2012;49(3):370–383.
36. Prasko J, Diveky T, Grambal A, et al. Transference and countertransference in cognitive behavioral therapy. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2010;154(3):189–198.
37. Knapp H. Therapeutic Communication. Developing Professional Skills. Los Angeles: Sage Publications; 2007.
38. Linehan MM. Dialectical behavioral therapy in groups: treating borderline personality disorders and suicidal behavior. In: Brody CM, editor. Women in Groups. New York: Springer; 1987.
39. Leahy RL. Overcoming Resistance in Cognitive Therapy. New York: The Guilford Press; 2003.
40. Liotti G. Internal working models of attachment in the therapeutic relationship. In: Gilbert P, Leahy RL, editors. The Therapeutic Relationship in the Cognitive Behavioral Psychotherapies. New York: Routledge/Taylor & Francis Group; 2007:143–161.
41. Prasko J, Vyskocilova J. Countertransference during supervision in cognitive behavioral therapy. Act Nerv Super Rediviva. 2010;52(4):251–260.
42. Gelso CJ, Bhatia A. Crossing theoretical lines: the role and effect of transference in nonanalytic psychotherapies. Psychotherapy. 2012;49(3):384–390.
43. Prasko J, Mozny P, Novotny M, Slepecky M, Vyskocilova J. Self-reflection in cognitive behavioural therapy and supervision. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2012;156(4):377–384.
44. Breuer J, Freud S. Studies on Hysteria. London: Hogarth Press; 1955.
45. Young JE, Weishaar ME, Klosko JS. Schema Therapy: A Practitioner’s Guide. Guilford: New York; 2003.
46. Robbins B. Under attack: devaluation and the challenge of tolerating the transference. J Psychother Pract Res. 2000;9(3):136–141.
47. Prasko J, Vyskocilova J, Mozny P, Novotny M, Slepecky M. Therapist and supervisor competencies in cognitive behavioural therapy. Neuroendocrinol Lett. 2011;32(6):101–109.
48. Vyskocilova J, Prasko J. Countertransference, schema modes and ethical considerations in cognitive behavioral therapy. Activitas Nervosa Superior Rediviva. 2013;55(1–2):33–39.
49. Beck JS, Sarnat JE, Borenstein V. Psychotherapy-based approaches to supervision. In: Falender CA, Shafranske EP, editors. Casebook for Clinical Supervision. Washington: American Psychiatric Association; 2008:57–96.
50. Greben SE, Ruskin R. Significant aspects of the supervisor-supervisee relationship and interaction. In: Greben SE, Ruskin R, editors. Clinical Perspectives of Psychotherapy Supervision. American Psychiatric Press, Washington; 1994:1–10.
51. Wongpakaran T, Wongpakaran N. How the interpersonal and attachment styles of therapists impact upon the therapeutic alliance and therapeutic outcomes. J Med Assoc Thai. 2012;95(12):1583–1592.
52. Shafranske EP, Falender CA. Supervision addressing personal factors and countertransference. In: Falender CA, Shafranske EP, editors. Casebook for Clinical Supervision. Washington: American Psychiatric Association; 2008:97–120.
53. Betan E, Heim AK, Zittel Conklin C, Westen D. Countertransference phenomena and personality pathology in clinical practice: an empirical investigation. Am J Psychiatry. 2005;162(5):890–898.
54. Skovholt TM, Ronnestad MH. The long, textured path from novice to senior practitioner. In: Skovholt TM, editor. The Resilient Practitioner: Burnout Prevention and Self-Care Strategies for Counsellors, Therapists, Teachers, and Health Professionals. Boston: Allyn and Bacon; 2001:25–54.
55. Watkins CE. Handbook of Psychotherapy Supervision. New York: Wiley; 1997.
56. Prasko J, Abeltina M, Vanek J, et al. How to use self-reflection in cognitive behavioral supervision. Act Nerv Super Rediviva. 2021b;63(2):68–83.
57. Thwaites R, Bennett-Levy J. Conceptualizing empathy in cognitive behaviour therapy: making the implicit explicit. Behav Cogn Psychother. 2007;35(5):591–612.
58. Vyskocilova J, Prasko J. Socratic dialogue and guided discovery in cognitive behavioral supervision. Act Nerv Super Rediviva. 2012a;54(1):35–45.
59. Vyskocilova J, Prasko J, Slepecky M. Empathy in cognitive behavioral therapy and supervision. Activitas Nervosa Superior Rediviva. 2012;53(2):72–83.
60. Bennett-Levy J, McManus F, Westling BE, Fennell M. Acquiring and refining CBT skills and competencies: which training methods are perceived to be most effective? Behav Cogn Psychother. 2009;37(5):571–583.
61. Watkins CE. Psychotherapy supervisor and supervisee: developmental models and research nine years later. Clin Psychol Rev. 1995;15(7):647–680.
62. Overholser JC. The Socratic method as a technique in psychotherapy supervision. Prof Psychol Res Pr. 1991;22(1):68–74.
63. Linehan MM, McGhee DE. A cognitive-behavioral model of supervision with individual and group component. In: Greben SE, Ruskin R, editors. Clinical Perspectives on Psychotherapy Supervision. Washington DC: American Psychiatric Press, Inc; 1994:165–188.
64. Bennett-Levy J. Therapist skills: a cognitive model of their acquisition and refinement. Behav Cogn Psychother. 2006;34(1):57–78.
65. Greenberg LS. Emotion in the relationship in emotion-focused therapy. In: Gilbert P, Leahy RL, editors. The Therapeutic Relationship in the Cognitive-Behavioural Psychotherapies. London: Routledge; 2007:43–62.
66. Hoffart A, Hedley LM, Thornes K, Larsen SM, Friis S. Therapists’ emotional reactions to patients as a mediator in cognitive behavioural treatment of panic disorder with agoraphobia. Cogn Behav Ther. 2006;35(3):174–182.
67. Katz AW, Safran JD. Recognizing and resolving ruptures in the therapeutic alliance. In: Gilbert P, Leahy RL, editors. The Therapeutic Relationship in the Cognitive Behavioral Psychotherapies. New York: Routledge/Taylor & Francis Group; 2007:90–105.
68. Knox S, Burkard AW, Edwards LM, Smith JJ, Schlosser LZ. Supervisors’ reports of the effects of supervisor self-disclosure on supervisees. Psychother Res. 2008;18(5):543–559.
69. Kottler JA. The Therapist’s Workbook: Self-Assessment, Self-Care, and Self-Improvement Exercises for Mental Health Professionals. John Wiley & Sons; 2011.
70. Levy K and Scala J. Transference, Transference Interpretations, and Transference-Focused Psychotherapies. Psychotherapy (Chicago, Ill.). 2012; 49: 391–403.
71. Gutheil TG, Gabbard GO. Misuses and misunderstandings of boundary theory in clinical and regulatory settings. Am J Psychiatry. 1998;155(3): 409–414.
72. Zanarini MC. Psychotherapy of borderline personality disorder. Acta Psychiatr Scand. 2009; 120(5):373–377.
73. McCracken LM, Gutiérrez-Martínez O. Processes of change in psychological flexibility in an interdisciplinary group-based treatment for chronic pain based on Acceptance and Commitment Therapy. Behav Res Ther. 2011 Apr;49(4):267–74.
74. Spinhoven P, Giesen-Bloo J, van Dyck R, Kooiman K, Arntz A. The therapeutic alliance in schema-focused therapy and transference-focused psychotherapy for borderline personality disorder. J Consult Clin Psychol. 2007;75(1):104–15.
75. Rivera M, Darke JL. Integrating empirically supported therapies for treating personality disorders: a synthesis of psychodynamic and cognitive-behavioral group treatments. Int J Group Psychother. 2012; 62(4):500–529.
76. Linehan MM, Kehrer CA. Borderline personality disorder. In: Barlow, DH,editor. Clinical handbook of psychological disorders. A step-by-step treatment manual. The Guilford Press, New York; 1993; 396–441.
77. Williams G. Reflections on some dynamics of eating disorders: 'no entry' defences and foreign bodies. Int J Psychoanal. 1997;78 (Pt 5):927–941.
78. Spinhoven P, Bockting CL, Kremers IP, Schene AH, Mark J, Williams G. The endorsement of dysfunctional attitudes is associated with an impaired retrieval of specific autobiographical memories in response to matching cues. Memory. 2007;15(3):324–338.
79. Singer JA, Conway MA. Reconsidering therapeutic action: Loewald, cognitive neuroscience and the integration of memory's duality. Int J Psychoanal. 2011;92(5): 1183–207.
80. Nordgren LF, Chou EY. A Devil On Each Shoulder When (and Why) Greater Cognitive Capacity Impairs Self-Control? Social Psychological and Personality Science. 2013; 4(2):233–237.
81. Breuer J & Freud S. Studies on Hysteria. London: Hogarth Press 1955 (Original work published in 1895).
82. Adshead G. ‘Three Degrees of Security’, in F. Pffafflin and G. Adshead (eds)A Matter of Security: Attachment Theory and Forensic Psychiatry and Psychotherapy,pp. 47–66. London: Jessica Kingsley 2003.
83. Hayes AF, Preacher KJ. Conditional process modeling: Using structural equation modeling to examine contingent causal processes. In G. R. Hancock & R. O. Mueller (Eds.), Structural equation modeling: A second course (pp. 219–266). IAP Information Age Publishing 2013.
84. Høglend P, Hersoug AG, Bøgwald K-P, Amlo S, Marble A, Sørbye Ø, Røssberg JI, Ulberg R, Gabbard GO, Crits-Christoph P. Effects of transference work in the context of therapeutic alliance and quality of object relations. Journal of Consulting and Clinical Psychology. 2011; 79(5): 697–706.
85. Henry WP, Schacht TE, Strupp HH, Butler SF, Binder JL (1993). Effects of training in time-limited dynamic psychotherapy: Mediators of therapists' responses to training. Journal of Consulting and Clinical Psychology. 1993; 61(3): 441–447.
86. Hadley SW, Strupp HH. Contemporary views of negative effects in psychotherapy. An integrated account. Arch Gen Psychiatry 1976; 33(11): 1291–1302.
87. Prasko J, Krone I, Burkauskas J, Ociskova M, Vanek J, Abeltina M, Dicevicius D, Juskiene A, Slepecky M, Bagdonaviciene L. Guided discovery in cognitive behavioral supervision. Act Nerv Super Rediviva 2020; 62(1): 17–28.
88. Sareen J, Skakum K. Defining the core processes of psychotherapy. Am J Psychiatry. 2005; 162(8):1549;
89. Rabinovich M, Kacen L. Let's look at the elephant: metasynthesis of transference case studies for psychodynamic and cognitive psychotherapy integration. Psychol Psychother. 2009; 82(Pt 4):427–47.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.