Back to Journals » International Journal of Women's Health » Volume 17
Managing Rare Postoperative Complications in Cornual Heterotopic Pregnancy: Two Case Reports
Authors Hao Y, Xin L, Chen J, Huang D
Received 8 July 2025
Accepted for publication 23 October 2025
Published 14 November 2025 Volume 2025:17 Pages 4461—4469
DOI https://doi.org/10.2147/IJWH.S551024
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Video abstract presented by Hao.
Views: 29
Yanqing Hao,1– 3 Liaobing Xin,1– 3 Jianmin Chen,1– 3 Dong Huang1– 3
1Assisted Reproduction Unit, Department of Obstetrics and Gynecology, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 2Zhejiang Provincial Clinical Research Center for Reproductive Health and Disease, Hangzhou, Zhejiang, 310016, People’s Republic of China; 3Zhejiang Key Laboratory of Precise Protection and Promotion of Fertility, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Dong Huang, Department of Obstetrics, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, No. 3 East Qing Chun Road, Hangzhou, 310016, People’s Republic of China, Tel +86 15924176867, Email [email protected]
Objective: To evaluate complications following laparoscopic cornuostomy or cornual repair in the management of cornual heterotopic pregnancy (CHP), and to assess the feasibility of repeat surgical interventions without compromising intrauterine pregnancy outcomes.
Methods: We conducted a case-based review involving two patients diagnosed with CHP following assisted reproductive technology (frozen embryo transfer and IVF). Both underwent initial laparoscopic cornuostomy or cornual repair, with postoperative complications managed through further interventions. Diagnostic tools, surgical approaches, and pregnancy outcomes were analyzed.
Results: In the first case, a 28-year-old woman developed a uterine arteriovenous fistula (AVF) after laparoscopic cornuostomy, detected by transvaginal ultrasound. Open AVF repair at 13 weeks under lumbar anesthesia resulted in a live birth at 32+ weeks. In the second case, a 30-year-old woman required laparotomy at 15+ weeks for removal of residual ectopic tissue after laparoscopic cornual repair; she subsequently delivered at term. Both cases demonstrated that repeat surgeries, including open procedures, can be safely performed without compromising ongoing intrauterine pregnancies.
Conclusion: Minimally invasive surgery is effective for CHP, but complications such as AVF and persistent ectopic tissue can arise and require timely reintervention. Transvaginal ultrasonography is essential for early detection. With multidisciplinary care and careful surgical planning, even repeat open surgeries can result in favorable maternal and fetal outcomes.
Keywords: cornual heterotopic pregnancy, uterine arteriovenous fistula, persistent ectopic pregnancy, laparoscopic cornuostomy
Introduction
Heterotopic pregnancies (HP) are complex clinical entities characterized by the simultaneous occurrence of twin gestations at separate implantation sites.1,2 The overall incidence of HP in pregnancies hovers around 1 in 3900 cases.3 However, this rate has been escalating in recent years, largely attributable to the rising application of exogenous gonadotropins and assisted reproductive technologies (ART), which could position the incidence at an estimated 1 in 3600. Notably, a history of salpingectomy markedly elevates the risk of cornual pregnancies, particularly following an ectopic pregnancy.4
Cornual Heterotopic Pregnancy (CHP), a distinctive form of heterotopic pregnancy, emerges in the segment of the fallopian tube that traverses the myometrium, and is at times interchangeably referred to as an interstitial pregnancy.5 Primary concerns for the pregnant individual include the threat of severe bleeding or hemorrhagic shock stemming from a ruptured cornual pregnancy, in addition to potential treatment-related complications such as treatment failure, persistent ectopic pregnancy, uterine rupture, infection, and complications from anesthesia.6 The associated risks for the intrauterine pregnancy encompass miscarriage, preterm delivery, infection, and other adverse outcomes. Given the concurrent presence of an intrauterine pregnancy, safeguarding the integrity of the uterus is of paramount importance. In recent times, there has been a gradual shift toward surgical interventions that prioritize cornuostomy or cornual repair, owing to their superior preservation of uterine myometrium integrity and diminished impact on uterine vasculature.7 Such tension-free repair techniques foster effective healing at the site of the uterine horn, significantly diminishing the risk of uterine rupture in subsequent pregnancies.8 Nonetheless, the management and prognostication of treatment-related complications are scarcely reported.
In this article, we delineate the postoperative complications and prognoses of two cases managed with laparoscopic cornuostomy while concurrently appraising the complications associated with alternative treatment modalities.
General Information
We extracted data from the medical record system. This study received approval from the Ethics Committee of the Sir Run Run Shaw Hospital, Affiliated to Zhejiang University School of Medicine. This clinical study adheres to the provisions of the Declaration of Helsinki, the Ethical Review Measures for Research Involving Human Life Sciences and Medical Research, the Administrative Measures for Investigator-Initiated Clinical Research in Medical and Health Institutions (Trial), and the Regulations on the Management of Human Genetic Resources of the People’s Republic of China, as well as other relevant laws and regulations.
Written informed consent was obtained from all patients, and the study was reviewed and approved by the Ethics Committee.
The project researchers will collectively bear the responsibility for maintaining the confidentiality of the participants’ relevant information and commit to not disclosing any content related to the participants. Any public report of the results of this study will not reveal the personal identities of the participants. We will make every effort, within the bounds of the law, to protect the privacy of the participants’ personal medical data and personal information.
Case Introduction
Case 1
A 28-year-old healthy pregnant woman, at 13 weeks’ gestation, presented to our hospital with persistent abdominal distension and a dull ache for 5 weeks. She had previously lost both fallopian tubes due to ectopic pregnancies. Recently, she had two frozen embryos successfully implanted in her uterus at our hospital’s reproductive center. Twenty-five days following the embryo transfer, she experienced light vaginal bleeding, and a subsequent transvaginal ultrasound revealed an intrauterine gestational sac measuring 19.4 × 26.0 × 15.5 mm with a detectable fetal heartbeat. Another gestational sac, comparable in size to the intrauterine one and with a visible heartbeat, was identified in the right uterine horn (illustrated in Figure 1A). Given the circumstances, an emergency laparoscopic cornuostomy and cornual repair were performed to effectively reconstruct the corneal area and minimize the risk of uterine rupture. Post-surgery, the patient was administered progesterone to prevent miscarriage. However, for 5 weeks post-operation, the patient complained of lingering lower abdominal pain, though no vaginal bleeding was noted. Sequential color Doppler ultrasounds presented a cystic mass within the right horn of the uterus that progressively enlarged with the pregnancy (as seen in Figure 1B). This cystic mass, measuring 3.47 × 3.72 cm at the uterine horn, was demarcated with a clear boundary and a regular shape, exhibiting internal cloud-like shadows. Color Doppler Flow Imaging (CDFI) highlighted an abundance of blood flow around the uterine horn, with multiple slender blood vessels penetrating the cyst. The blood flow was characterized by high velocity (Vmax = 83.9 cm/s) and low resistance (RI = 0.21) (as seen in Figure 1C and Video S1). The mass was situated close to the medial placenta and uterine cavity, with the lateral muscular layer approximately 0.41 cm thick. At this time, the color Doppler ultrasound suggested a single viable intrauterine pregnancy with a crown-rump length (CRL) of 62.8 mm (depicted in Figure 1D). The cystic mass in the right fundus muscle layer was diagnosed as a uterine arteriovenous fistula (AVF).
 |
Figure 1 Transvaginal ultrasound findings of Case 1. (A) Gestational sac (white arrow) in the right cornual region (2.08 × 1.85 × 1.92 cm), adjacent to the intrauterine sac (black asterisk). (B) A cystic lesion located at the right cornual region (white arrow), demonstrating internal cloud-like echoes, with its medial aspect closely approximating the maternal placental surface and the uterine cavity (white asterisk). (C) The lesion demonstrates rich peripheral vascularity with fine intralesional vessels. Pulsed-wave Doppler interrogation reveals high-velocity flow (peak systolic velocity: 83.9 cm/s) and markedly low resistance (resistance index: 0.21). (D) Intrauterine singleton pregnancy with viable fetus (crown-rump length: 62.8 mm). |
With the progressive enlargement of arteriovenous fistula lesions, the risk of rupture and hemorrhage also increases. A laparotomy cornuostomy and suture arteriovenous fistula were performed in order to reconstruct the corneal area efficiently, thus minimising the risk of uterine rupture in the pregnancy at 13 weeks of gestation. Under general anesthesia, and via a longitudinal incision, a mass barely beneath the serosal surface of the uterus’s right horn was exposed, revealing a network of rich and tortuous vessels on its surface. To control the uterine blood flow, the assistant applied gentle pressure with the index fingers along the parauterine space, lifting the uterine horn mass to the level of the abdominal incision. Without the need for uterotonic agents, the thinnest part of the AVF was incised, revealing a cavity filled with bright red blood but absent of any suspicious trophoblastic tissue. The fibrotic tissue within the cavity was excised, and active bleeding vessels were meticulously sutured. After complete removal of fibrotic tissues, the cornual incision was sutured in a single continuous layer.
To further prevent miscarriage, the patient was administered progesterone and magnesium sulfate. She successfully carried the pregnancy to 32+ weeks and delivered a healthy infant weighing 1800 grams by cesarean section, achieving Apgar scores of 10 at both 1 and 5 minutes post-delivery. The newborn was discharged in good health after treatment in the neonatal intensive care unit. The follow-up period is longer than 5 years. At present, the patient has successfully given birth to her second child.
Case 2
We report a case involving a 30-year-old woman, gravida 3, para 0, who underwent transfer of two frozen embryos as a result of a previous right salpingectomy for an ectopic pregnancy and confirmed obstruction of the left fallopian tube. At 38 days post-in vitro fertilization (IVF), a color ultrasound examination revealed an intrauterine complex left cornual pregnancy. She underwent an emergency laparoscopic left cornual resection for ectopic pregnancy removal and uterine horn repair. Postoperatively, the patient experienced recurrent, minimal vaginal bleeding for over a month. The color Doppler ultrasonography showed a single viable intrauterine fetus at approximately 13 weeks’ gestation (illustrated in Figure 2A), accompanied by a hypoechoic mass between the wall of the left uterine cornu close to the amniotic sac that protruded toward the serous membrane. The lesion, measuring 4.36 × 4.14 × 4.84 cm, had a clear boundary and an uneven internal echo with sparse dotted blood flow signals and no discernible normal myometrial echoes at the outer edge of the mass. This suggested the presence of residual left cornual pregnancy tissue (shown in Figure 2B).
 |
Figure 2 Transvaginal ultrasound findings of Case 2. (A) A single viable intrauterine fetus is present (biparietal diameter: 7.28 cm). (B) A hypoechoic mass is observed in the left uterine cornua (white arrow), adjacent to the intrauterine gestational sac (white asterisk). The lesion protrudes toward the serosal surface and demonstrates internal blood flow signals. |
During the follow-up, color Doppler ultrasound indicated that the mass in the uterine horn gradually protruded beyond the uterine serosa, and its internal blood supply increased. At 15+ weeks’ gestation, a laparotomy was performed to excise the residual pregnancy tissue and repair the cornual region. Intraoperatively, a mass in the left uterine horn, approximately 5 × 4 cm in size with a purplish-red surface (shown in Figure 3A), was elevated into the abdominal cavity. The surgical team minimized uterine blood flow by applying pressure along the parauterine space (shown in Figure 3B). Using an electrosurgical knife, they incised the base of the cornual mass. They clamped the edges of the incision with ALLIS dental forceps and extracted the decidual tissue and villi with oval forceps before suturing the area in layers to reconstruct the uterine cornual (shown in Figure 3C and D). Progesterone and magnesium sulfate were administered postoperatively to prevent miscarriage. Pathological examination revealed a few villi and desquamated tissue (depicted in Figure 4).
 |
Figure 3 Laparotomy for residual cornual ectopic pregnancy: Surgical steps (Case 2). (A) A subserosal mass (4 × 5 cm) at the left uterine cornua, displaying a purplish-red surface indicative of vascular engorgement (white arrow). (B) Intraoperative vascular control via manual para-uterine compression (white arrow) and Allis forceps application to retract the incision edge, exposing residual ectopic tissue (white asterisk). (C) Viable myometrial margins with fresh pink tissue are observed, without evidence of active bleeding. (D) Layered closure of the cornual defect using absorbable sutures, achieving tension-free repair. |
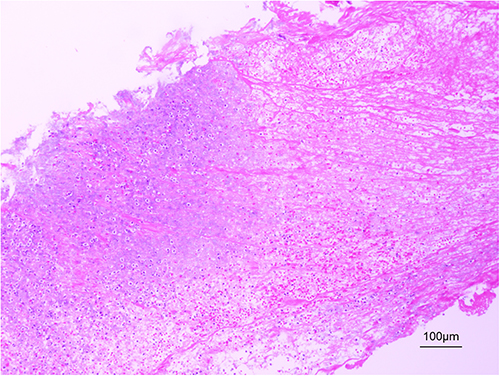 |
Figure 4 Residual gestational trophoblast (100 µm; x100; hematoxylin and eosin staining). |
Regular antenatal check-ups confirmed no further complications during the rest of the gestation, and the patient successfully delivered a healthy infant via cesarean section at 37+ weeks’ gestation. The picture of the uterine horn at the patient’s full-term cesarean delivery shows no significant abnormal vascular proliferation and good myometrial integrity (Figure 5). The follow-up period is longer than 5 years. In the following three years, this patient also successfully gave birth to her second child.
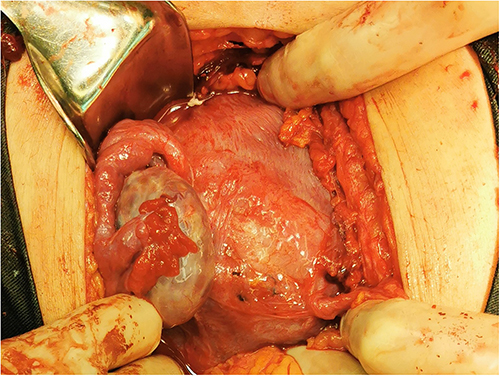 |
Figure 5 The picture of the uterine horn at the patient’s full-term cesarean delivery of case 2. |
Discussion
Assisted reproduction and salpingectomy significantly elevate the incidence of cornual pregnancy, particularly in those with a prior history of ectopic pregnancy.9,10 Cornual pregnancy constitutes 2–4% of ectopic pregnancies and carries a mortality rate roughly six to seven times higher than other forms of ectopic pregnancy.11 The cornual region’s vascularization from ovarian and uterine arterial branches can lead to significant bleeding either from a ruptured cornu or from a surgical incision.8
Management of Cornual Heterotopic Pregnancy can be challenging as the therapy necessitates preserving the intrauterine pregnancy as much as possible. The choice of management strategies hinges on the patient’s unique characteristics, including gestational age, viability of the ectopic pregnancy, symptoms, and the rupture status of the ectopic pregnancy.10 However, intervention-related complications, such as serious uterine rupture during gestation, infection, persistent ectopic pregnancy, or even therapeutic failure, should not be overlooked. Multiple treatment options are available for cornual pregnancy, individually tailored according to the patient’s condition and the surgical scenario. Medical management primarily involves the administration of Methotrexate or potassium chloride, while surgical procedures predominantly comprise laparoscopic or even laparotomic cornuostomy or cornuotomy. Expectant management is seldom employed in this context due to the high risk of uterine rupture.12
Medical treatment is a safe and effective approach for early detected, small-sized, asymptomatic, unruptured cornual ectopic pregnancies. Nevertheless, intrauterine fetal toxicity effects may occur following drug administration, including periventricular leukomalacia and limb anomalies.13 In addition to the risks associated with pharmaceutic application, infection, bleeding, and therapeutic failure must be considered.9 Failed treatment commonly presents as continuous enlargement of the gestational sac and abrupt rupture, with emergency laparotomy corner resection often chosen based on literature review.14,15
Certain surgeons favor performing a cornual resection, particularly if the embedding of the extrauterine pregnancy deeply invades the myometrium or the mass is relatively large. Tulandi et al reported that this approach is more suitable for lesions with a diameter exceeding 4 cm.16 Additionally, the incorporation of surgical methods such as cornuostomy and the placement of a purse-string suture around the cornual regions of the uterus followed by removal of the interstitial pregnancy via a flushing technique can also effectively address bleeding issues.6–8 Cornuostomy preserves the continuity of the muscular layer and the integrity of crucial blood vessels, enabling the uterine incision to heal more efficiently, obviating the need for tension repair, and diminishing the risk of miscarriage, preterm labor, uterine rupture, and so on.7 It’s been reported that within 75 patients having interstitial pregnancy without intrauterine pregnancy who underwent primary laparoscopic cornual resection or cornuostomy, five patients required secondary treatment.17 Laparoscopic cornual resection did not diminish the incidence of persistent pregnancy. Two cases of uterine rupture with fetal demise in the second trimester post cornual wedge resection have been documented in the literature.18,19 However, the management and prognosis of complications linked to laparoscopic cornuostomy are infrequently reported.
Our cases highlight clinically significant complications that are rarely reported in the literature (Table 1).
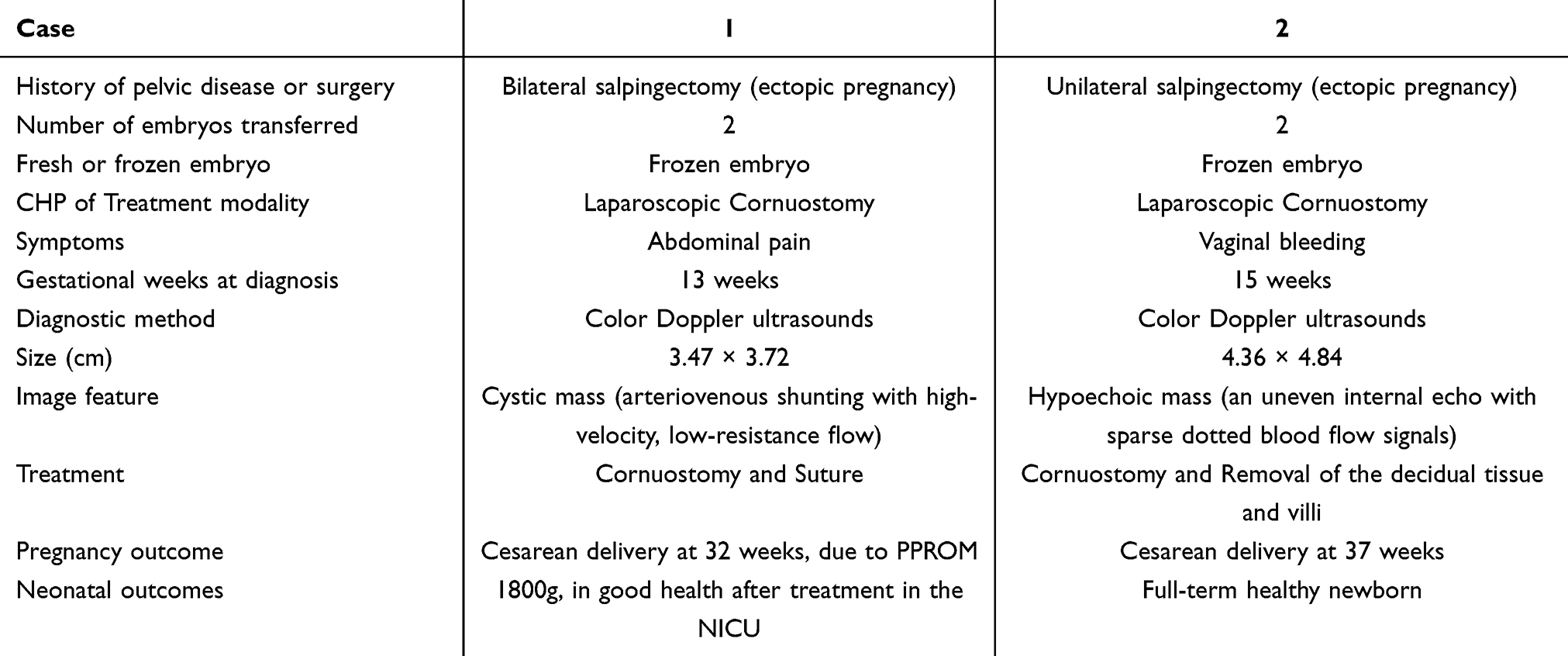 |
Table 1 Summary of Patient’s Diagnostic and Therapeutic Data |
In Case 1, the patient experienced persistent abdominal pain and discomfort following laparoscopic cornuostomy. Transvaginal sonography (TVS) revealed a cystic mass at the uterine horn with a well-defined margin and regular contour. Color Doppler Flow Imaging (CDFI) demonstrated abundant vascularity surrounding the horn, along with a tangle of multidirectional high-velocity blood flow, producing a characteristic “color mosai” pattern. Spectral Doppler analysis confirmed arteriovenous shunting, with high-velocity and low-resistance flow (Vmax = 83.9 cm/s, RI = 0.21). The sonographic findings, which can also be seen in patients with a history of uterine surgery or gestational trophoblastic disease, typically originate from the lateral uterine wall and may extend to the endometrial cavity.
Uterine arteriovenous fistula (AVF) is typically classified as either congenital or acquired. Acquired AVF results from abnormal direct communication between one or more uterine arteries and the myometrial and/or endometrial venous plexus, without an intervening vascular nidus. In some cases, other arterial sources such as ovarian arteries or branches from the round ligament may also contribute to the fistula formation.20,21 The development of acquired AVF is commonly associated with major pelvic trauma, including uterine surgeries, childbirth, abortion (spontaneous or induced), dilation and curettage, infections, or gestational trophoblastic tumors.22 The overall incidence of uterine AVF is considered extremely low, and precise epidemiological data remain unavailable. Clinically, uterine AVF most often presents with abnormal uterine bleeding, commonly described as menorrhagia or intermenstrual hemorrhage, and may be accompanied by dyspareunia or pelvic pain. In early pregnancy, its presentation may mimic conditions such as threatened abortion or hydatidiform mole, complicating the diagnosis.23 On color Doppler ultrasound, AVF typically appears as an intensely vascular tangle, demonstrating high-velocity, low-resistance flow. This hallmark “color mosaic” pattern, often accompanied by spectral Doppler findings of arteriovenous shunting, is crucial for diagnosis.24 Vascular intervention plays a critical role in both the diagnosis and management of such lesions. In patients with an ongoing intrauterine pregnancy, serial ultrasound monitoring is essential to evaluate the risk of lesion enlargement or rupture and to help determine optimal surgical timing. While uterine artery embolization (UAE) or vascular ligation is commonly reported as first-line management, the blood supply to lesions at the uterine horn often derives from both uterine and ovarian arteries, which may contribute to the failure of interventional treatments and necessitate multiple procedures.
In Case 2, serum HCG levels lost their diagnostic utility in identifying persistent ectopic pregnancy, as is observed in approximately 6.67% of such cases.17 Regular postoperative transvaginal ultrasound, alongside clinical signs—such as abnormal vaginal bleeding, lower abdominal discomfort, or sudden pelvic pain—became crucial diagnostic clues. Regardless of whether the initial management is surgical or medical, clinicians must remain highly vigilant when patients present with persistent vaginal bleeding and vague abdominal pain. When imaging reveals a mass-like lesion at the uterine horn with heterogeneous echotexture, varying degrees of vascularity, and progressive enlargement, persistent interstitial pregnancy should be strongly suspected. In this case, the patient experienced ongoing light vaginal bleeding following laparoscopic cornual repair. Serial ultrasound scans identified a progressively enlarging vascular mass at the uterine horn, with absence of normal surrounding myometrium, indicating a high risk of rupture. Drawing on the surgical insights from Case 1, the uterine horn was incised to fully expose and excise the residual gestational trophoblastic tissue. Layered, tension-free sutures were placed to reconstruct the horn, ensuring preservation of sufficient healthy myometrial tissue. At the time of full-term cesarean section, the uterine horn appeared intact, with no abnormal vascular proliferation and well-preserved myometrial architecture, confirming the long-term success of the repair.
In recent years, the popularity of laparoscopic surgical treatment has grown due to advances in timeliness of diagnosis and improvement of laparoscopic techniques. Open surgery has its advantages in cases of large pregnancy masses or ruptured bleeding, such as swift hemostasis and stratified repair. The choice between these modalities should always prioritize the patient’s safety.25,26 The occurrence of surgical complications is closely related to the surgeon’s proficiency and the patient’s condition. However, given the limited number of cases, all of which were delivered by cesarean section, it remains uncertain whether these findings can be broadly generalized.
Conclusion
The incidence of cornual heterotopic pregnancy (CHP) has risen in recent years, partly due to multiple gestations and prior salpingectomy in patients undergoing assisted reproductive technology. Both laparoscopic and open cornuostomy or repair remain feasible options, even in challenging cases, provided that meticulous hemostasis and maximal preservation of the myometrium are ensured. Our clinical experience suggests that careful attention to subtle maternal symptoms, timely and skilled assessment by experienced ultrasonographers, and close multidisciplinary collaboration are crucial for optimizing outcomes. Although the coexistence of an intrauterine pregnancy increases the complexity of management, cornuostomy appears to be relatively safe with regard to maintaining intrauterine gestation and preventing uterine rupture, when performed under such careful monitoring and support.
Institutional Review Board Statement
This case report was conducted in accordance with the ethical standards of Sir Run Run Shaw Hospital, affiliated with Zhejiang University School of Medicine. Formal approval for publication was granted by the Hospital’s Ethical and Research Committee (Approval No. 1140, 2024 Research Project; approval date: 6 November 2023). Written informed consent was obtained from the patient.
Data Sharing Statement
All data are available in the manuscript.
Consent for Publication
Informed consent was obtained from both patients for the publication of this case report and any clinical images.
Acknowledgments
Yanqing Hao is first authors for this work. We would like to thank all patients who have made genuine contributions to the article and who endorse the data and conclusions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the “Pioneer” and “Leading Goose” R&D Program of Zhejiang (2024C03200).
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Shaw JL, Diamandis EP, Horne AW, Barnhart K, Bourne T, Messinis IE. Ectopic pregnancy. Clin Chem. 2012;58(9):1278–1285. doi:10.1373/clinchem.2012.184168
2. Farquhar CM. Ectopic pregnancy. Lancet. 2005;366(9485):583–591. doi:10.1016/S0140-6736(05)67103-6
3. Molinaro TA, Barnhart KT, Levine D, et al. Abdominal pregnancy, cesarean scar pregnancy, and heterotopic pregnancy. 2015.
4. Habana A, Dokras A, Giraldo JL, et al. Cornual heterotopic pregnancy: contemporary management options. Am J Obstet Gynecol. 2000;182:1264–1270. doi:10.1067/mob.2000.103620
5. Moawad NS, Mahajan ST, Moniz MH, Taylor SE, Hurd WW. Current diagnosis and treatment of interstitial pregnancy. Am J Obstet Gynecol. 2010;202(1):15–29. doi:10.1016/j.ajog.2009.07.054
6. Gao B, Cheng C, Pan Q, Johnson G, Qin X, Xu D. Laparoscopic strategy for heterotopic interstitial pregnancy following assisted reproductive techniques. JSLS. 2019;23(2):e2018–00109. doi:10.4293/JSLS.2018.00109
7. Xu W, Lin X, Huang D, et al. Laparoscopic treatment of cornual heterotopic pregnancy: a retrospective cohort study. Int J Surg. 2018;53:98–102. doi:10.1016/j.ijsu.2018.03.025
8. Lei R, Liang J, Ling X, et al. Use of laparoscopic slip knot with purse-string suture in surgical management of unruptured heterotopic interstitial pregnancies. Med Sci Monit. 2020;26:e921185. doi:10.12659/MSM.921185
9. Xu Y, Zheng L, Chen H, Lu Y, Li D, Zhang J. Heterotopic pregnancy after in-vitro fertilization and embryo transfer following bilateral total salpingectomy/tubal ligation: case report and literature review. J Minim Invasive Gynecol. 2016;23(3):338–345. doi:10.1016/j.jmig.2015.11.013
10. Dendas W, Schobbens JC, Mestdagh G, Meylaerts L, Verswijvel G, Van Holsbeke C. Management and outcome of heterotopic interstitial pregnancy: case report and review of literature. Ultrasound. 2017;25(3):134–142. doi:10.1177/1742271X17710965
11. Oral S, Akpak YK, Karaca N, Babacan A, Savan K. Cornual heterotopic pregnancy after bilateral salpingectomy and uterine septum resection resulting in term delivery of a healthy infant. Case Rep Obstet Gynecol. 2014;2014:157030. doi:10.1155/2014/157030
12. Gaetani M, Di Gennaro D, Vimercati A, et al. Cornual Pregnancy. Gynecol Minim Invasive Ther. 2023;12(3):130–134. doi:10.4103/gmit.gmit_10_23
13. Qiong Z, Yanping L, Prasad DJ, Lin Z. Treatment of cornual heterotopic pregnancy via selective reduction without feticide drug. J Minim Invasive Gynecol. 2011;18(6):766–768. doi:10.1016/j.jmig.2011.08.007
14. Wu Z, Zhang X, Xu P, Huang X. Clinical analysis of 50 patients with heterotopic pregnancy after ovulation induction or embryo transfer. Eur J Med Res. 2018;23:17. doi:10.1186/s40001-018-0316-y
15. Yang X, Zhu L, Le F, et al. The effect of local aspiration and methotrexate injection on live interstitial pregnancy coexisting with live intrauterine pregnancy after assisted reproductive technology. J Obstet Gynaecol Res. 2019;45(7):1296–1302. doi:10.1111/jog.13975
16. Tulandi T, Vilos G, Gomel V. Laparoscopic treatment of interstitial pregnancy. Obstet Gynecol. 1995;85:465–467. doi:10.1016/0029-7844(94)00423-B
17. Lee MH, Im SY, Kim MK, Shin SY, Park WI. Comparison of laparoscopic cornual resection and cornuotomy for interstitial pregnancy. J Minim Invasive Gynecol. 2017;24(3):397–401. doi:10.1016/j.jmig.2016.11.016
18. Shang J, Peng R, Zheng J, Lin M. The indicator of clinical outcomes for patients with heterotopic pregnancy following in-vitro fertilization with embryo transfer. Taiwan J Obstet Gynecol. 2019;58(6):827–832. doi:10.1016/j.tjog.2019.09.018
19. Li JB, Kong LZ, Yang JB, et al. Management of heterotopic pregnancy: experience from 1 tertiary medical center. Medicine. 2016;95(5):e2570. doi:10.1097/MD.0000000000002570
20. Timmerman D, Wauters J, Van Calenbergh S, et al. Color Doppler imaging is a valuable tool for the diagnosis and management of uterine vascular malformation. Ultrasound Obstet Gynecol. 2003;21:
21. Levy-Zaubermann Y, Capmas P, Legendre G, Fernandez H. Laparoscopic management of uterine arteriovenous malformation via occlusion of internal iliac arteries. J Minim Invasive Gynecol. 2012;19(6):785–788. doi:10.1016/j.jmig.2012.07.009
22. Raherinantenaina F, Rajaonanahary TM, Randriamandrato TA, Rakoto Ratsimba HN. Successful management of an acquired uterine arteriovenous malformation by selective ligation of the internal iliac artery. J Mal Vasc. 2015;40(3):182–186. doi:10.1016/j.jmv.2015.02.001
23. Yahi-Mountasser H, Collinet P, Nayama M, Boukerrou M, Robert Y, Deruelle P. Intrauterine arteriovenous malformations. J Gynecol Obstet Biol Reprod. 2006;35:614–620. doi:10.1016/j.gyobfe.2011.05.008
24. O’Brien P, Neyastani A, Buckley AR, Chang SD, Legiehn GM. Uterine arteriovenous malformations: from diagnosis to treatment. J Ultrasound Med. 2006;25(11):1387–92; quiz1394–5. doi:10.7863/jum.2006.25.11.1387
25. Siristatidis C, Bellos I, Karageorgiou V, Kapnias D. A three-layer reconstruction of the uterus in a heterotopic interstitial pregnancy. J Obstet Gynaecol. 2019;39(4):564–565. doi:10.1080/01443615.2018.1525694
26. Anderson J, Patterson C, Riley A. Heterotopic interstitial pregnancy: a case report. Case Rep Womens Health. 2018;17:8–10. doi:10.1016/j.crwh.2018.02.003
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.