Back to Archived Journals » Chronic Wound Care Management and Research » Volume 6
Management of patients with calciphylaxis: current perspectives
Authors Erfurt-Berge C, Renner R ![]()
Received 15 April 2019
Accepted for publication 19 July 2019
Published 17 October 2019 Volume 2019:6 Pages 109—115
DOI https://doi.org/10.2147/CWCMR.S182417
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Marco Romanelli
Video abstract presented by Cornelia Erfurt-Berge.
Views: 5535
Cornelia Erfurt-Berge, Regina Renner
Department of Dermatology, University Hospital Erlangen, Erlangen 91054, Germany
Correspondence: Cornelia Erfurt-Berge
Department of Dermatology, University Hospital Erlangen, Ulmenweg 18, Erlangen 91054, Germany
Tel + 49 9 131 853 5000
Email [email protected]
Abstract: Calciphylaxis (CP) is a rare disorder presenting with painful ischemic skin ulcerations. Its association with end-stage renal disease, but also non-uremic cases have been described. Several risk factors, like metabolic syndrome, calcium-phosphate imbalance, anticoagulative medication and female gender have been discussed. Multidisciplinary therapeutic approaches are necessary since evidence-based guidelines are missing due to lack of pathophysiological understanding of the disease and the absence of studies with large patient cohorts. However, strategies for local wound therapy, reduction of risk factors and systemic therapies are being developed. Changes in duration, frequency and method of hemodialysis and specific medication to lower the calcium upload can be effective in uremic CP cases. Systemic treatments with cinacalcet, sodium thiosulfate or bisphosphonates have been applied successfully in CP patients, but large placebo-controlled randomized trials are still needed to gather better insight into this fatal disease.
Keywords: calciphylaxis, calcific uremic arteriolopathy, non-uremic calciphylaxis, calcification, treatment, sodium thiosulfate
Calciphylaxis (CP) is a rare vasculopathic disorder associated with necrotic skin ulcers and high mortality due to calcification of small cutaneous vessels. It has to be discussed as differential diagnosis when unusual and recalcitrant chronic wounds appear. Since the exact pathogenesis remains unclear, different entities might be subsumed under the term CP. Well known is the synonym calcific uremic arteriolopathy (CUA) when the typical necrotic ulcers appear together with end-stage renal disease, a frequent observed co-morbidity. Around 1% of patients depending on hemodialysis suffer from CUA.1 Most of the studies dealing with CP were performed in patients with CUA. Typically, in the histological analysis of a deep scalpel biopsy with skin and subcutaneous tissue one can find the trias of calcification of the media layer of small cutaneous vessels, intimal hyperplasia/fibrosis and thrombotic occlusion. The stenosis and occlusion of small dermal and pannicular arterioles leads to the typical clinical presentation of a skin infarction.2 Additional stainings like van Kossa might help to confirm the calcium deposits.3 But on the other hand, one can also find lesions with the typical histological pattern without the abovementioned associated renal disease. These cases are described as non-uremic CP and are even harder to verify and to treat.4 However, the serum calcium and phosphate levels can be affected by a large number of possible underlying disorders beyond chronic kidney disease and these have to be clarified. Among these disorders are hyperparathyroidism, tumors, medication or vitamin imbalances.2
For lack of alternative options, treatment options known from CUA are also transferred to non-uremic cases despite their off-label use and missing recommendations for a particular therapeutic approach. The systemic therapies and the local wound management for CP will be discussed below. The high mortality described for CUA patients is the impetus for an early diagnosis and treatment. In a case-control study, a 1-year survival rate of 45% was found for CP patients.5 A monocentric retrospective study in Spain showed a mortality rate higher in CUA than in non-uremic cases of CP.6 It has been observed that the risk for death is eightfold higher in patients with CP and associated end-stage renal disease compared to other hemodialysis patients.7
Diagnosis
CP is considered when necrotic ulcers with surrounding livedo racemosa or indurated plaques occur – particularly in the lower extremities – and additionally when the patient´s history is positive for chronic renal disease or even hemodialysis. However, the presentation of the cutaneous lesions can highly vary concerning their clinical appearance with subcutaneous induration, hemorrhagic patches or stellate-shaped ulcers with thick necrosis as well as the associated comorbidities with likewise described cases of non-uremic CP. An unusual localization can even hinder finding a clear diagnosis.8
A review about CP would not be complete without discussion of differential diagnoses, specifically when the association with renal disease as a diagnostic clue is missing. When the ulcers appear on the lower leg, frequent causes of leg ulcer like vascular ulcers have to be clarified. Another important and highly discussed diagnosis with some overlapping patterns to CP is the hypertensive ischemic leg ulcer Martorell.9 Here, we also find rapidly progressive, painful necrotic ulcers, preferentially on the dorsal calf in association with a history of long-lasting arterial hypertension. Histological findings show also calcification in small cutaneous arterioles. A clear differentiation from CP is often hard to find and some authors postulate a common origin for these ulcers.
Thrombophilic disorders also have to be differentiated when thrombosis of small vessels can be seen in the histological investigation. Livedoid vasculopathy also with painful, necrotic ulcers of the lower leg, livedo racemosa of the surrounding skin and occlusion of small cutaneous vessels can be mentioned as a thrombotic disease which can appear clinically like ulcers from CP.10 Some authors advocate strict anticoagulative therapy for patients with CP, but the choice of anticoagulative agent is highly restricted since warfarin has been implicated in the pathogenesis of CP as described below.11 Other causes of cutaneous vessel occlusion like cholesterin embolization, cryoglobulinemia or medication-induced ulcerations have to be differentiated, too.12 In a case-control study of CP patients with concomitant renal disease, the authors found higher rates of hypercoagulability in the CP patients than in controls with same stages of renal diseases.13
To differentiate other underlying diseases with the presentation of skin ulcers parameter for collagenoses or vasculitis, as well as cryoglobulines and antiphospholipid antibodies should be controlled.12 Taken together, there is some hint of a correlation between CP and hypercoagulability.14
Calcium-phosphate levels, stage of renal disease, hypercoagulability and exclusion of differential diagnoses can mainly be performed via an orientating blood analysis. More specific markers of calcification can be added when necessary. Table 1 gives an overview of possible blood markers. To confirm the diagnosis of CP, a single elevated parameter (eg, an increased value of calcium-phosphate product) alone is not evidentiary enough.
 |
Table 1 Recommendations for possible blood analysis in patients with suspicion of CP. The values marked with * might be restricted to cases with further research interest |
Risk factors and co-morbidities
A number of risk factors for the development of CP have been described in case-control studies, mainly for patients with end-stage renal disease. But most studies are still limited by small number of patients or selection bias and true causality has not been determined. In most cases, no data about direct affectation of CP by the described co-morbidity are available.15 Table 2 shows an overview of highly acknowledged risk factors. Next to end-stage renal disease and its co-morbidities like anemia and cardiovascular diseases, associations of CP with diabetes mellitus have been described.16 Moreover, smaller numbers of reports have been published about possible associations between CP and autoimmune disorders, infectious or alcoholic hepatitis, antiphospholipid syndrome or duration of dialysis.15 Chronic inflammatory states are discussed as possible risk factors for vascular calcification as TNF-a induces an osteogenic phenotype of human smooth-muscle cells in vitro.17 Other cytokines are also linked to calcification. Aluminum excess has also been discussed to be at least a co-factor in the pathogenesis of some CP cases by involvement in the NFkB pathway which itself might influence vascular calcification.2
 |
Table 2 Overview of risk factors observed for development of CP (data from5,7) |
Special emphasis has been placed on the discussion about induction of CP by drugs.18 Patients with end-stage renal disease are often under multiple medications and should be subject to an explicit review of drugs possibly contributing to CP. Warfarin is one of the best known factors associated with CP and the course of disease. It has been shown that warfarin can negatively influence vitamin K-dependent proteins which prevent vascular calcification. Although this could be shown in animal models, the role of warfarin in human vascular calcification remains unclear.19 Some authors even postulated distinguishing between warfarin-associated and -unassociated CP.20 To explore the effect of vitamin K supplementation in patients with uremic CP, a randomized controlled study trial is currently recruiting (ClinicalTrials.gov Identifier: NCT02278692). However, the identification and treatment of underlying coagulative disorders in any case of CP is essential.21 Stopping warfarin, vitamin D, calcium supplements and iron intake is recommended by the majority when treating CP patients.18,22,23 Direct thrombin inhibitors have been shown to be safe and well tolerated in smaller case series and lead to improvement of CP.24 Another case series with 15 patients observed a positive effect for tissue plasminogen activator as an adjunctive treatment option in CP.25,26 However, these therapeutic decisions require an interdisciplinary approach regarding the individual patient and his underlying morbidities.
Treatment
Clear therapeutic guidelines for the treatment of CP are still missing which is caused by the missing insights into CP pathophysiology so far. Efficient therapeutic procedures and evidence-based recommendations are needed especially for non-uremic CP, since therapeutic strategies can so far only be transferred from CUA treatment without a pathophysiological correlation.27
Concepts of a modern wound management should be followed with special emphasis on debridement and prevention or early treatment of wound infections which are involved in the high mortality of CP patients due to sepsis. Non-adhesive modern wound dressings or products with silicone layer can be applied to the wound to enable an atraumatic dressing change and reduce pain. Antiseptics like octenidin, polihexanide or hypochloric acids as well as antimicrobial effective substances are part of the local treatment regimens. Removal of necrosis and wound debris is essential but often hard to implement due to pain or the patient´s multimorbidity. While some authors advocate an early, consequent surgical debridement,9 others prefer less invasive treatment like maggot therapy.28 Debridement can also be combined with negative pressure wound therapy and – after achieving a satisfying granulation tissue – split skin grafting.29 In a retrospective study of 64 patients, an estimated 1-year survival rate of 61.6% was observed for 17 patients receiving surgical debridement compared with 27.4% for the 46 who did not (p=0.008).5 However, there is even discussion whether performing deep skin biopsy may worsen the clinical course30,31 and too intensive manipulation is not advised.1
Hyperbaric oxygen therapy (HBOT) might be an adjunctive topical treatment option, but is only available in a small number of specialised centres. In a retrospective analysis of 34 patients with uremic CP, HBOT was very effective with 50% complete wound healing and 58% improvement.32 Patients have to be selected according to availability and their overall health condition for such specific and extensive local wound treatments.
In addition to modern wound management, a supportive analgesic medication is essential for CP patients. The course of disease is often prolonged or chronic and pain is a frequent symptom which has to be addressed according to its characteristics and specificity with adequate medication according to the analgesic ladder and the patient´s needs.
In summary, local wound therapy in CP patients has to be performed in a professional manner and where available in specialized wound care centers.33 A clear therapeutic recommendation beyond intensive and antimicrobial local wound care cannot be given according to the currently available literature. Individual therapeutic decisions have to be made and an evaluation by experienced wound carers has to be ensured.
Systemic treatment
While the cessation of warfarin medication and vitamin D or calcium intake has already been discussed above, therapeutic approaches with systemic medication shall be addressed in the following section. As the presented therapeutic strategies mainly derive from those for uremic CP, more efficient therapeutic measures and evidence-based recommendations are needed for non-uremic cases.27 A clear diagnostic classification as CP is mandatory.
Searching for clinical trials in CP patients does not reveal many hits in research databases. Due to the multimorbidity and limited mobility of CP patients, randomized controlled trials in specialized centers are highly restricted in terms of patient acquisition.1
Systematic data collection might be supported by clinical registers like the German Calciphylaxis Network (www.calciphylaxis.net) (NCT02635373).34
In CP patients with hemodialysis, the calcium-phosphate product might be positively influenced by changes in frequency, duration or method of blood filtration. Additionally, vitamin D intake or calcium supplements have to be restricted. In a small pilot study, four dialysis patients with CP were successfully treated with lanthanum carbonate, a calcium-free phosphate binder inhibiting the intestinal absorption of phosphate.35 Results from the EVOLVE trial showed that patients with end-stage renal disease and uncontrolled hyperparathyroidism, a risk factor for CP, showed a lowered incidence of CP over an observation period of 5 years when treated with cinacalcet, a calcimimetic substance activating the calcium-sensing receptor and thereby reducing parathyroid hormone production.36 Parathyroidectomy is also discussed as a treatment option for patients with CP and secondary hyperparathyroidism.37 Early treatment is recommended for these cases.38 However in a comprehensive review, the use of cinacalcet showed a reduction of parathyroid hormone within a period of 1–2 years,39 so some authors only recommend parathyroidectomy in cases with no response to medication with cinacalcet.12 A new substance (SNF472) to inhibit progressive calcification in patients with hemodialysis may be promising and future study results have to be awaited to assess its efficacy in CP patients (NCT02790073). The substance inhibits the development of ectopic calcification by blocking the formation and growth of hydroxyapatite crystal.40 When it comes to treatments focusing on inhibition of calcification, bisphosphonates were also successfully applied in CP patients with and without renal diseases. While the use of bisphosphonates in patients with severe renal disease is usually avoided due to long-term adverse events concerning bone-turnover effects, their effect in a potentially life-threatening disease like CP is promising. Newly proposed pathways discuss the influence of bisphosphonates on different calcification pathways like enhancing osteoprotegerin, inhibiting calcification of vascular smooth-muscle cells or the formation of calcium-phosphate crystals.41 Even anti-inflammatory effects are discussed.41 Several case series showed successful use of bisphosphonates also in non-uremic CP patients.42,43
Another approach with a growing number of reported cases of successful treatment is the intravenous use of sodium thiosulfate (STS) in CP patients. The proposed mechanism behind this therapy is its ability to enhance the solubility of calcium in deposits and therefore its availability for dialysis.41 Other effects may be antioxidative or vasodilatory.31 Currently, two clinical studies dealing with STS are recruiting in France and the United States. One multicentre, Phase III, randomized placebo-controlled study is focusing on the potential of STS to reduce pain in CP patients (NCT03150420) next to the clinical improvement of skin lesions while another retrospective follow-up study comprises one of the largest global cohorts of CP patients treated with STS and investigates the influence of STS on patients´ mortality. More than 350 cases with the use of STS in CP patients have been reported so far,44 either with STS alone or as part of a combination therapy. Positive effects were seen in CP patients with renal disease/dialysis45 as well as in non-uremic CP cases46 where the therapeutic effect cannot be explained so far. Even intralesional injections have been described occasionally47 and showed a good clinical improvement but pain during injections. Due to the renal clearance of STS, dosages and application frequency for intravenous application have to be adapted to renal function and the presence of dialysis. Specific side effects are rare and can be handled by supportive therapy.41 Table 3 summarizes therapeutic attempts made in CP patients while Table 4 gives an overview of currently recruiting clinical studies.
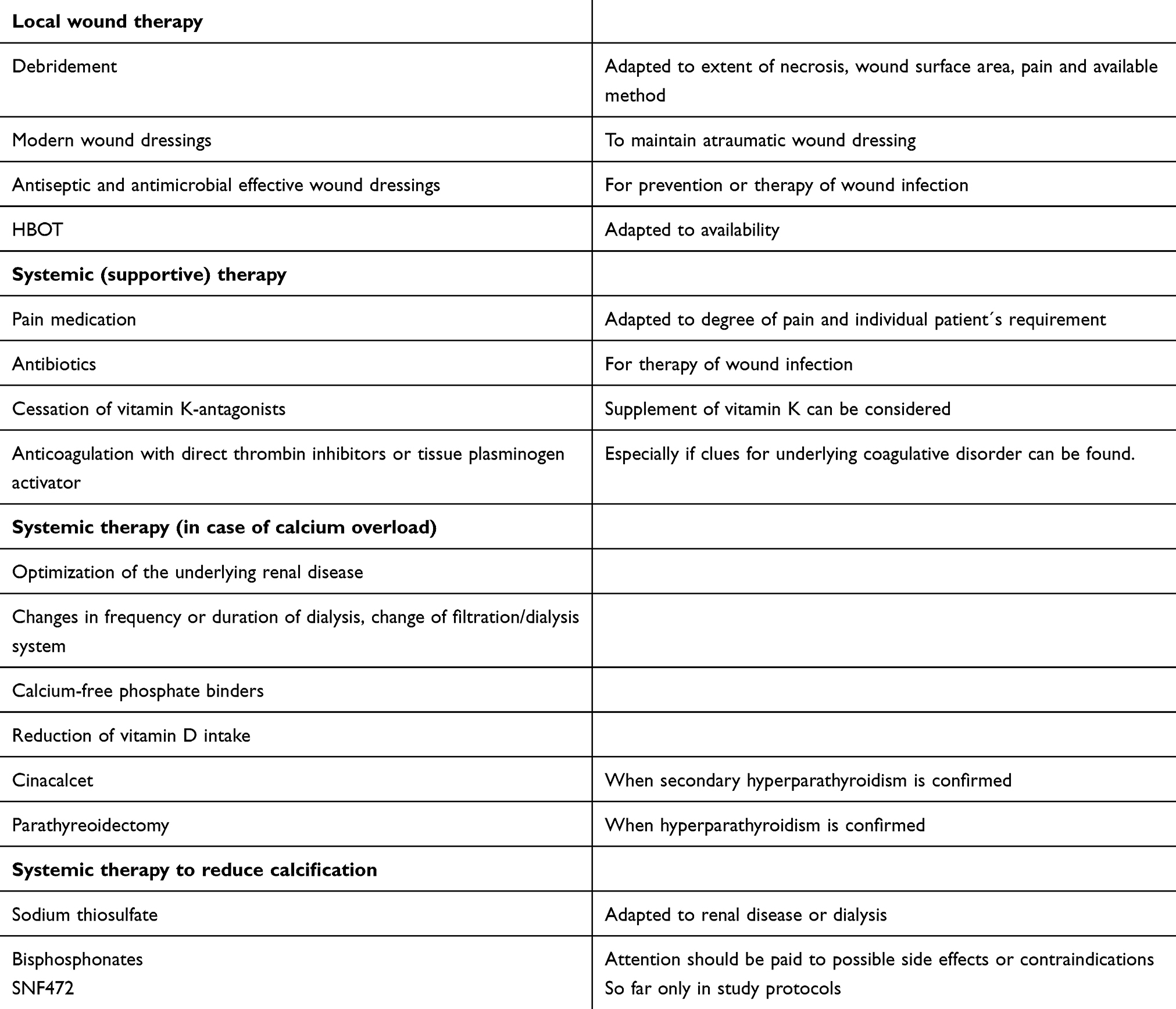 |
Table 3 Therapeutic options for the treatment of CP |
 |
Table 4 Overview of recruiting studies worldwide (data survey on clinicaltrials.gov on 05/06/2019) |
Conclusion
The diagnosis of CP is often obvious with the typical necrotic ulcers and a history of chronic renal disease or dialysis. Several risk factors have been identified and should be addressed early in affected patients. Different treatment approaches for local and systemic therapy have been acknowledged although randomized controlled studies are still missing. Next to an atraumatic and antiseptic wound management, systemic approaches like improvement of calcium and phosphate levels as well as treatment of secondary hyperparathyroidisms are among the therapeutic considerations. The systemic application of STS or bisphosphonates is confirmed as successful in several case studies. Randomized controlled studies on larger cohorts are needed to clear upcoming issues about dosage, treatment duration and long-term outcomes. Diagnosis and treatment are hindered for the non-uremic forms of CP where so far the concepts of CUA can only be transferred in lack of distinct recommendations.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brandenburg VM, Martin H, Sohn CM, et al. [Calciphylaxis]. Dtsch Med Wochenschr. 2015;140:347–351. doi:10.1055/s-0041-100834
2. Weenig RH. Pathogenesis of calciphylaxis: hans Selye to nuclear factor kappa-B. J Am Acad Dermatol. 2008;58:458–471. doi:10.1016/j.jaad.2007.12.006
3. Mochel MC, Arakaki RY, Wang G, et al. Cutaneous calciphylaxis: a retrospective histopathologic evaluation. Am J Dermatopathol. 2013;35:582–586. doi:10.1097/DAD.0b013e31827c7f5d
4. Nigwekar SU, Wolf M, Sterns RH, Hix JK. Calciphylaxis from nonuremic causes: a systematic review. Clin J Am Soc Nephrol. 2008;3:1139–1143. doi:10.2215/CJN.00530108
5. Weenig RH, Sewell LD, Davis MD, et al. Calciphylaxis: natural history, risk factor analysis, and outcome. J Am Acad Dermatol. 2007;56:569–579. doi:10.1016/j.jaad.2006.08.065
6. Fernandez M, Morales E, Gutierrez E, et al. Calciphylaxis: beyond CKD-MBD. Nefrologia. 2017;37:501–507. doi:10.1016/j.nefro.2017.02.006
7. Mazhar AR, Johnson RJ, Gillen D, et al. Risk factors and mortality associated with calciphylaxis in end-stage renal disease. Kidney Int. 2001;60:324–332. doi:10.1046/j.1523-1755.2001.00803.x
8. Garcia-Lozano JA, Ocampo-Candiani J, Martinez-Cabriales SA, et al. An update on calciphylaxis. Am J Clin Dermatol. 2018;19:599–608. doi:10.1007/s40257-018-0361-x
9. Hafner J. Calciphylaxis and martorell hypertensive ischemic leg ulcer: same pattern - one pathophysiology. Dermatology. 2016;232:523–533. doi:10.1159/000448245
10. Kerk N, Goerge T. Livedoid vasculopathy - current aspects of diagnosis and treatment of cutaneous infarction. J Dtsch Dermatol Ges. 2013;11:407–410. doi:10.1111/ddg.12064
11. El-Azhary RA, Hickson L, McBane RD. Calciphylaxis. N Engl J Med. 2018;379:397–398. doi:10.1056/NEJMc1807324
12. Hoff NP, Homey B. [Calciphylaxis. Pathogenesis and therapy]. Hautarzt. 2011;62:509–515. doi:10.1007/s00105-010-2111-8
13. Dobry AS, Ko LN, St JJ, et al. Association between hypercoagulable conditions and calciphylaxis in patients with renal disease: a case-control study. JAMA Dermatol. 2018;154:182–187. doi:10.1001/jamadermatol.2017.4920
14. Harris RJ, Cropley TG. Possible role of hypercoagulability in calciphylaxis: review of the literature. J Am Acad Dermatol. 2011;64:405–412. doi:10.1016/j.jaad.2009.12.007
15. Nigwekar SU, Kroshinsky D, Nazarian RM, et al. Calciphylaxis: risk factors, diagnosis, and treatment. Am J Kidney Dis. 2015;66:133–146. doi:10.1053/j.ajkd.2015.01.034
16. Renner R, Dissemond J, Goerge T, et al. Analysis of the German DRG data for livedoid vasculopathy and calciphylaxis. J Eur Acad Dermatol Venereol. 2017;31:1884–1889. doi:10.1111/jdv.14190
17. Tintut Y, Patel J, Parhami F, Demer LL. Tumor necrosis factor-alpha promotes in vitro calcification of vascular cells via the cAMP pathway. Circulation. 2000;102:2636–2642. doi:10.1161/01.cir.102.21.2636
18. Portales-Castillo I, Kroshinsky D, Malhotra CK, et al. Calciphylaxis-as a drug induced adverse event. Expert Opin Drug Saf. 2019;18:29–35. doi:10.1080/14740338.2019.1559813
19. Danziger J. Vitamin K-dependent proteins, warfarin, and vascular calcification. Clin J Am Soc Nephrol. 2008;3:1504–1510. doi:10.2215/CJN.00770208
20. Yu WY, Bhutani T, Kornik R, et al. Warfarin-associated nonuremic calciphylaxis. JAMA Dermatol. 2017;153:309–314. doi:10.1001/jamadermatol.2016.4821
21. Lehman JS, Chen TY, Lohse CM, et al. Evaluating the validity of subclassifying warfarin-associated nonuremic calciphylaxis: a retrospective cohort study. Int J Dermatol. 2018;57:572–574. doi:10.1111/ijd.13884
22. Seethapathy H, Brandenburg VM, Sinha S, et al. Review: update on the management of calciphylaxis. QJM. 2019;112:29–34. doi:10.1093/qjmed/hcy234
23. Zacharias JM, Fontaine B, Fine A. Calcium use increases risk of calciphylaxis: a case-control study. Perit Dial Int. 1999;19:248–252.
24. King BJ, El-Azhary RA, McEvoy MT, et al. Direct oral anticoagulant medications in calciphylaxis. Int J Dermatol. 2017;56:1065–1070. doi:10.1111/ijd.13685
25. El-Azhary RA, Arthur AK, Davis MD, et al. Retrospective analysis of tissue plasminogen activator as an adjuvant treatment for calciphylaxis. JAMA Dermatol. 2013;149:63–67. doi:10.1001/2013.jamadermatol.5
26. Sewell LD, Weenig RH, Davis MD, et al. Low-dose tissue plasminogen activator for calciphylaxis. Arch Dermatol. 2004;140:1045–1048. doi:10.1001/archderm.140.9.1045
27. Gomes F, La FP, Costa C, et al. Non-uremic calciphylaxis: a rare diagnosis with limited therapeutic strategies. Eur J Case Rep Intern Med. 2018;5:000986.
28. Tittelbach J, Graefe T, Wollina U. Painful ulcers in calciphylaxis - combined treatment with maggot therapy and oral pentoxyfillin. J Dermatolog Treat. 2001;12:211–214. doi:10.1080/09546630152696035
29. Sattler DR, Preiss S, Altmann S, et al. [The plastic surgical treatment of progressive skin lesions caused by calciphylaxis]. Zentralbl Chir. 2011;136:621–624. doi:10.1055/s-0031-1271458
30. Latus J, Kimmel M, Ott G, et al. Early stages of calciphylaxis: are skin biopsies the answer? Case Rep Dermatol. 2011;3:201–205. doi:10.1159/000333007
31. Ross EA. Evolution of treatment strategies for calciphylaxis. Am J Nephrol. 2011;34:460–467. doi:10.1159/000332221
32. An J, Devaney B, Ooi KY, et al. Hyperbaric oxygen in the treatment of calciphylaxis: a case series and literature review. Nephrology (Carlton). 2015;20:444–450. doi:10.1111/nep.12433
33. Dado DN, Huang B, Foster DV, et al. Management of calciphylaxis in a burn center: a case series and review of the literature. Burns. 2019;45:241–246. doi:10.1016/j.burns.2018.09.008
34. Brandenburg VM, Kramann R, Rothe H. et al. Calcific uraemic arteriolopathy (calciphylaxis): data from a large nationwide registry. Nephrol Dial Transplant. 2016. gfv438. doi:10.1093/ndt/gfv438
35. Chan MR, Ghandour F, Murali NS, et al. Pilot study of the effect of lanthanum carbonate (Fosrenol(R)) in patients with calciphylaxis: a Wisconsin Network for Health Research (WiNHR) study. J Nephrol Ther. 2014;4:1000162. doi:10.4172/2161-0959.1000162
36. Floege J, Kubo Y, Floege A, Chertow GM, Parfrey PS. The effect of cinacalcet on calcific uremic arteriolopathy events in patients receiving hemodialysis: the EVOLVE trial. Clin J Am Soc Nephrol. 2015;10:800–807. doi:10.2215/CJN.10221014
37. Girotto JA, Harmon JW, Ratner LE, Nicol TL, Wong L, Chen H. Parathyroidectomy promotes wound healing and prolongs survival in patients with calciphylaxis from secondary hyperparathyroidism. Surgery. 2001;130:645–650. doi:10.1067/msy.2001.117101
38. Duffy A, Schurr M, Warner T, Chen H. Long-term outcomes in patients with calciphylaxis from hyperparathyroidism. Ann Surg Oncol. 2006;13:96–102. doi:10.1245/ASO.2006.03.042
39. Deen J, Schaider H. The use of cinacalcet for the treatment of calciphylaxis in patients with chronic kidney disease: a comprehensive review. Australas J Dermatol. 2019. doi:10.1111/ajd.12992
40. Ferrer MD, Perez MM, Canaves MM, et al. A novel pharmacodynamic assay to evaluate the effects of crystallization inhibitors on calcium phosphate crystallization in human plasma. Sci Rep. 2017;7:6858. doi:10.1038/s41598-017-07203-x
41. Ross EA. What is the role of using sodium thiosulfate or bisphosphonates in the treatment for calciphylaxis? Semin Dial. 2011;24:434–436. doi:10.1111/j.1525-139X.2011.00954.x
42. Schliep S, Schuler G, Kiesewetter F. Successful treatment of calciphylaxis with pamidronate. Eur J Dermatol. 2008;18:554–556. doi:10.1684/ejd.2008.0499
43. Torregrosa JV, Duran CE, Barros X, et al. Successful treatment of calcific uraemic arteriolopathy with bisphosphonates. Nefrologia. 2012;32:329–334. doi:10.3265/Nefrologia.pre2012.Jan.11137
44. Peng T, Zhuo L, Wang Y, et al. Systematic review of sodium thiosulfate in treating calciphylaxis in chronic kidney disease patients. Nephrology (Carlton). 2018;23:669–675. doi:10.1111/nep.13081
45. Devey S, Valois A, Cazajous G, et al. [Calciphylaxis in hemodialysis patients: 8 cases treated with sodium thiosulfate]. Ann Dermatol Venereol. 2018;145:288–292. doi:10.1016/j.annder.2018.02.002
46. Bourgeois P, De HP. Sodium thiosulfate as a treatment for calciphylaxis: a case series. J Dermatolog Treat. 2016;27:520–524. doi:10.3109/09546634.2016.1163316
47. Isoherranen K, Bouchard L, Kluger N. Benefits of intralesional injections of sodium thiosulfate in the treatment of calciphylaxis. Int Wound J. 2017;14:955–959. doi:10.1111/iwj.12738
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.