Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 17
Management of hyperkalemia: Expert consensus from Kuwait – a Modified Delphi Approach
Authors AlSahow A ![]() , Bulbanat B, Alhelal B, Alhumoud K, Alkharaza A, Alotaibi T, Alrajab H, Alyousef A, Hadi F
, Bulbanat B, Alhelal B, Alhumoud K, Alkharaza A, Alotaibi T, Alrajab H, Alyousef A, Hadi F
Received 13 July 2024
Accepted for publication 26 August 2024
Published 5 October 2024 Volume 2024:17 Pages 227—240
DOI https://doi.org/10.2147/IJNRD.S476344
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pravin Singhal
Ali AlSahow,1 Bassam Bulbanat,2 Bassam Alhelal,3 Khaldoun Alhumoud,4 Ahmad Alkharaza,5 Torki Alotaibi,6 Heba Alrajab,7 Anas Alyousef,8 Fatimah Hadi9
1Nephrology division, Jahra Hospital, Al Jahra, Kuwait; 2Cardiac Center, Amiri Hospital, Kuwait City, Kuwait; 3Nephrology Division, Adan Hospital, Hadiya, Kuwait; 4Al salam International Hospital, Kuwait City, Kuwait; 5Cardiology Division, Adan Hospital, Hadiya, Kuwait; 6Hamad AlEssa Transplant Center, Ibn Sina Hospital, Kuwait City, Kuwait; 7Nephrology Division, Farwaniya Hospital, Sabah Al Nasser, Kuwait; 8Nephrology Division, Amiri Hospital, Kuwait City, Kuwait; 9Cardiology Division, Chest Diseases Hospital, Kuwait City, Kuwait
Correspondence: Ali AlSahow, Nephrology Division, Department of Medicine, Jahra Hospital, Bishr Bin Awana, Jahra, 00004, Kuwait, Email [email protected]
Introduction: Hyperkalemia is common in heart failure (HF) patients on renin angiotensin aldosterone inhibitors (RAASi), in chronic kidney disease (CKD), and in hemodialysis, and it negatively impacts their management. New potassium binders, such as sodium zirconium cyclosilicate (SZC), are effective in management of acute and chronic hyperkalemia. However, guidelines inconsistencies and lack of standardized treatment protocols are hindering proper and wider use of such agents. Therefore, an expert panel from Kuwait developed a consensus statement to address hyperkalemia management in acute settings, in HF, in CKD, and in hemodialysis.
Methods: A three-step modified Delphi method was adopted to develop the present consensus, which consisted of two rounds of voting and in-between a virtual meeting. Twelve experts from Kuwait participated in this consensus. Statements were developed and shared with experts for voting. A meeting was held to discuss statements that did not reach consensus at the first round and then the remaining statements were shared for final voting.
Results: The consensus consists of 44 statements involving an introduction to and the management of hyperkalemia in acute settings, HF, CKD, and hemodialysis. Thirty-six statements approved unanimously in the first vote. In the second vote, four statements were removed and four were approved after editing.
Conclusion: Hyperkalemia management lacks standardized definitions, treatment thresholds and consistent guidelines and laboratory practices. This consensus is in response to lack of standardized treatment in the Arabian Gulf, and it aims to establish guidance on hyperkalemia management for healthcare practitioners in Kuwait and highlight future needs.
Keywords: chronic kidney disease, heart failure, hemodialysis, hyperkalemia, potassium binders
Introduction
Hyperkalemia is a common electrolyte disorder in chronic kidney disease (CKD),1 which can have negative consequences for cardio-renal management in the medium and long term.1,2 The European Resuscitation Council defines hyperkalemia as a plasma K+ level greater than 5.5 mmol/L and severe hyperkalemia as a level greater than 6.5 mmol/L.3
Factors that can predispose to hyperkalemia include kidney-related factors such as low glomerular filtration rate (GFR), reduced tubular flow, reduced distal sodium delivery, and/or reduced aldosterone activity/production1,2,4–6, Also, one of the contributing factors to hyperkalemia in patients with CKD is metabolic acidosis, especially diabetics, which causes a shift of K+ from the intracellular to the extracellular space1,4, further exacerbating hyperkalemia and limiting the use of renin-angiotensin-aldosterone inhibitors (RAASi) for the treatment and prevention of cardiovascular diseases (CVD),1,7 and the management of CKD. Other major risk factors for hyperkalemia include diabetes mellitus, adrenal disease, and heart failure (HF).
Management of hyperkalemia is challenging at the level of thresholds and type of intervention.8 Another challenge is the inconsistencies reported between diagnostic laboratories as of when and how specialists are notified of hyperkalemia results and the suggested thresholds for urgent intervention.8
In acute cases of hyperkalemia, immediate interventions may be necessary to lower K+ levels and stabilize the patient.9 These interventions may include the administration of medications such as calcium gluconate to protect the heart from the effects of high K+ levels, insulin, and glucose to promote cellular uptake of K+ and medications that enhance K+ excretion, such as loop diuretics or sodium polystyrene sulfonate.3 Additionally, long-term management strategies to return to normokalemia in chronic hyperkalemia should involve the use of medications such as potassium-binders, which help remove excess K+ from the body, or the initiation of kidney replacement therapy (KRT) in severe cases.1
In recent years, there have been developments in the use of novel potassium-binders, such as sodium zirconium cyclosilicate (SZC) and patiromer, which have been found to effectively lower K+ levels and have been well tolerated by patients, and hence, are used to treat chronic hyperkalemia in patients with CKD.10–12 These binders aim to reduce dietary K+ absorption and may have implications for long-term cardiovascular and renal outcomes.11
With the lack of standardized treatments and evidence-based guidelines for outpatient hyperkalemia management,8,9 this consensus aims to gather experts’ insights and consensus regarding guidance for hyperkalemia management for healthcare practitioners in Kuwait. This consensus is based on identifying and critically appraising research evidence and generating recommendations based on the available evidence and expert opinion.
Materials and Methods
Study Design and Panel Recruitment
This consensus is based on a three-step modified Delphi method, which has proven its reliability for building consensus in a variety of clinical settings through repeated voting rounds on a specific set of statements; these statements were developed via a series of systematic literature searches and experts’ feedback. A modified version of the Delphi method, known as the modified Delphi process or Estimate-Talk-Estimate process, was then introduced to incorporate a face-to-face meeting in the Delphi process, and aims to gain more insights from the experts on statements with no consensus agreement in the first round of voting. The modified Delphi method provides more effective interaction and agreement than the original version of the Delphi process. This study utilized two rounds of voting and in-between virtual meetings to develop consensus statements.
A total of 12 experts from Kuwait were invited to participate in the Delphi study and were asked to participate in the process’s three steps. All experts were required to have an active research profile in the field of nephrology and cardiology.
Literature Review and Statements Development
A systematic literature search was conducted on Medline via PubMed from its inception to April 2023 to collect relevant information. The following search terms were used in combination with the term “hyperkalemia”: “management”, “treatment”, “diagnosis”, “acute hyperkalemia”, “heart failure”, “hemodialysis”, “Kuwait”, “guidelines”, “KDIGO”, “monitoring”, “chronic kidney disease”, “CKD”, “K+ binders”, and “potassium”. Initially, the titles and abstracts of the retrieved records were screened. Then, full texts of the publications that address the consensus objectives were reviewed. A manual search of the references of retrieved publications was also conducted.
Statements were developed and questionnaire was sent via Email to experts for revision and voting. The questionnaire consisted of binary statements, in which the experts were asked to choose between “agree”, “disagree”, and “abstain” options. Each expert was able to comment on each statement and provide suggestions. A descriptive statistic quantified experts’ responses to each statement. Each statement was considered to achieve consensus if it achieved an agreement level of ≥75%. The statements that did not achieve the agreement level were persevered for step 2 to be modified or omitted by the experts.
A virtual advisory board meeting was conducted in the second step and engaged all experts. Whether they reached the agreement level or not, all statements were presented during this meeting to gain the experts’ feedback and recommendations. The meeting was divided into two parts. In the first part, the statements that achieved ≥75% agreement were presented for full consensus by the panel, while the remaining statements were presented for modification or omission. The second part of the meeting aimed to develop the final guideline form for hyperkalemia management.
In the final step, the list of modified statements and the final form of the guidelines were emailed to experts for voting and followed the same voting process as step 1. The final consensus statements and manuscript were reviewed and approved by all experts.
Results and Discussion
A total of 44 statements were developed. At first voting round 36 received consensus and did not require a second voting round; eight statements were edited and proceeded to a second vote where four were removed and four achieved consensuses after editing. Finally, 40 statements are included in this consensus.
Hyperkalemia introduction and Management
Introductory statements to hyperkalemia and its management are outlined in Table 1. The panel agrees that hyperkalemia is defined by blood K+ level >5 mmol/L, as suggested by guidelines and medical societies.2,13–15 However, others define hyperkalemia as blood K+ level >5.5 mmol/L.16,17 The panel also agrees that blood K+ level >6.5 mEq/L is life-threatening increasing the risk of arrhythmia and cardiac arrest, in agreement with published literature.18,19 However, some suggests that a blood K+ level >6.0 mEq/L is where hyperkalemia starts to be life-threatening and increases the risk of arrhythmia and cardiac arrest.14,15,20
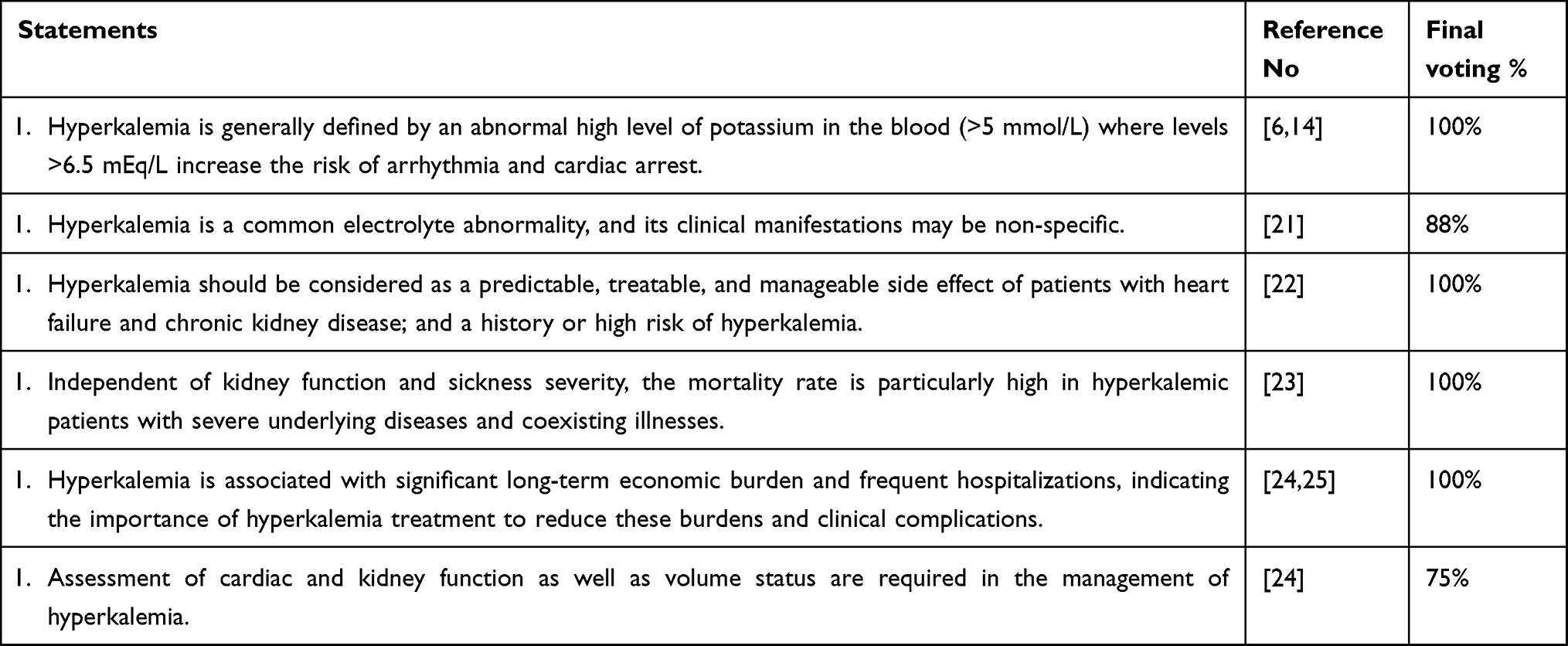 |
Table 1 Introductory Statements |
The panel also acknowledges the fact that hyperkalemia is a common electrolyte disorder and that its clinical manifestations may be non-specific, in agreement with published literature.9,26 Similarly, the panel agrees that hyperkalemia is a predictable, and manageable condition in high-risk patients such as HF and CKD.27–30 Also, studies declare that kidney function plays a significant role in K+ regulation, and impaired kidney function can increase the risk of hyperkalemia.31
The panel agrees that the mortality rate is particularly high in hyperkalemic patients with severe underlying diseases and coexisting illnesses independent of kidney function and sickness severity. As studies also show the mortality rate was higher in hyperkalemic patients with CKD than the non-hyperkalemic patients with CKD.32,33
The panel agrees with published literature that hyperkalemia is associated with significant long-term economic burdens due to an increase in emergency department (ED) visits, and associated with frequent hospitalizations and mortality, since studies show that hyperkalemia can have toxic effects on the cardiac conduction system, potentially leading to lethal outcomes.34 Thus, indicating the importance of hyperkalemia prevention and management to reduce these burdens and clinical complications.24,35,36
Regarding the management of hyperkalemia, the panel agrees that it requires assessment of cardiac and kidney function as well as volume status. The panel also agrees that assessment of cardiac function, kidney function, and volume status are crucial for hyperkalemia management, as recommended by published literature.3,37 Monitoring serum K+ levels and assessing kidney function help identify patients at risk of hyperkalemia especially in patients with CKD or patients taking RAASi, and help managing hyperkalemia by guiding medication adjustments.31,38
Managing Hyperkalemia in the Acute Setting
This section discussed all aspects of acute hyperkalemia and its management and statements discussed are in Table 2. The majority of the panel’s members (88%) agree that acute hyperkalemia, defined as 5.5 mmol/L or more, may be under-recognized in ED due to normal electrocardiogram (ECG) and absence of clear clinical signs and symptoms that lead to treatment. There are only a few recent studies on acute hyperkalemia and the most recent studies confirm that elevated serum K+ levels of 5.5 mmol/L or more is frequently asymptomatic with a normal ECG which mislead healthcare professionals causing hyperkalemia under-recognition.3,15,34,39–41
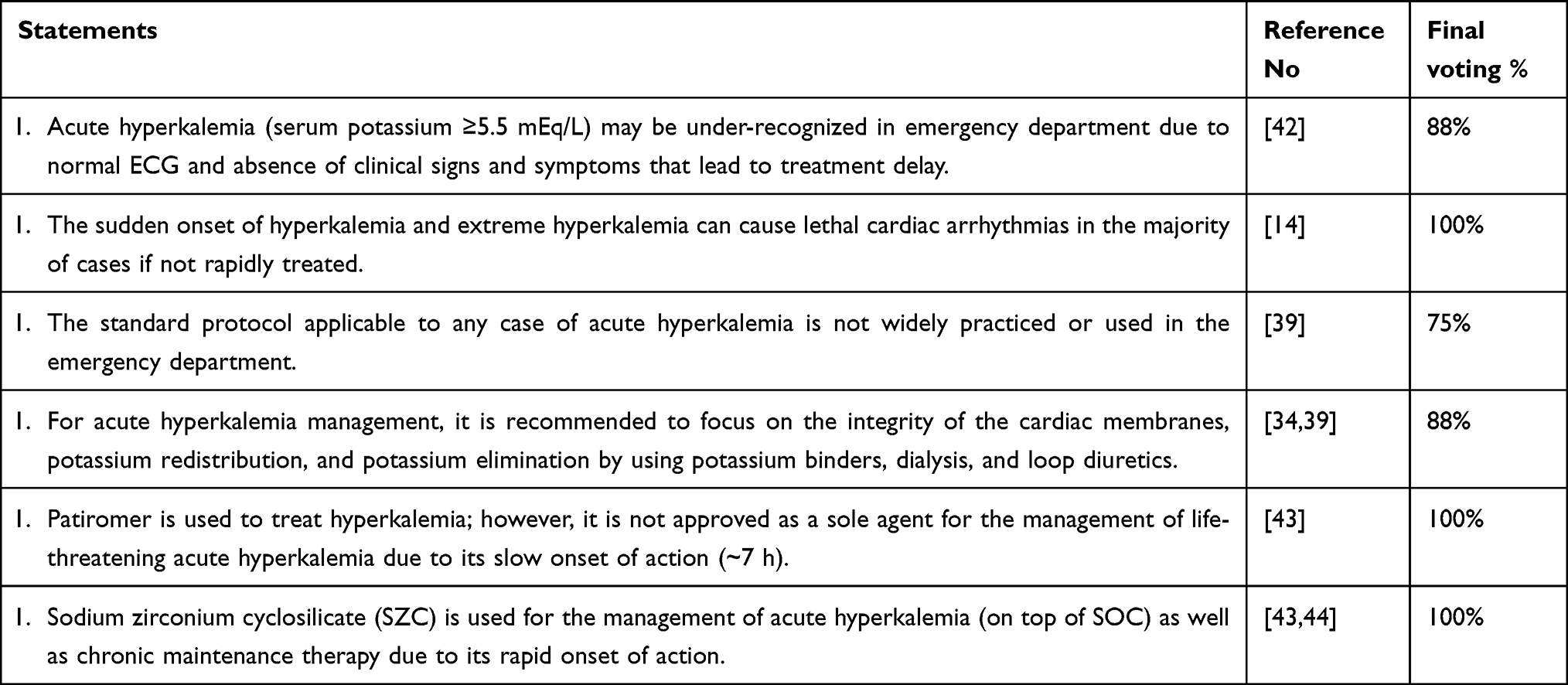 |
Table 2 Managing Hyperkalemia in Acute Setting |
On the other hand, the panel agrees with the fact that hyperkalemia of sudden onset and severe hyperkalemia can cause lethal cardiac arrhythmias in most cases if not rapidly treated. This is supported by several studies displaying that severe hyperkalemia is life-threatening and can lead to sudden death from cardiac arrhythmias and asystole if not corrected promptly with a rapid point-of-care.14,45–47
The majority of the panel’s members (75%) agree that there is no standard management protocol applicable to any case of acute hyperkalemia widely practiced or used in the ED. On the contrary, studies claim that no universally accepted standard of care protocol has been established for the treatment of patients presenting with acute hyperkalemia, whether in the ambulatory or ED setting.48–50
Regarding acute hyperkalemia management, the majority of the panel’s members (88%) agree that it is recommended to focus on stabilizing the myocardium, redistributing K+, and eliminating K+ with potassium-binders, dialysis, and loop diuretics. This is consistent with published literature that list these three methods for treating acute hyperkalemia.15,34,51 The panel also agrees that the potassium-binder patiromer can be used to treat hyperkalemia; however, it may not be effective as an add-on therapy to standard of care for management of life-threatening acute hyperkalemia when prompt reduction in blood K+ is required, due to its slow onset of action (∼7 h).30,52 On the other hand, the panel agrees that the potassium binder SZC can be used for the management of acute hyperkalemia as an add-on therapy to standard of care in the emergency setting for K+ removal from the body due to its more rapid onset of action, as studies showed that patients who received SZC had a decrease in serum K+ levels within one hour of therapy,53,54 and due to its effectiveness throughout the whole digestive system.10,55 Patients managed for life-threatening hyperkalemia require frequent monitoring of serum K+ to ensure reduction to a safe level in response to medical therapy. Otherwise, urgent hemodialysis is indicated.
Management of Hyperkalemia in Patients with Heart Failure
This section includes statements on the recommendations and guidelines for managing hyperkalemia in patients with HF, outlined in Table 3. The panel agrees that both hypo- and hyperkalemia are associated with increased mortality in patients with HF, as reported in recent studies.56–60 Cooper et al conducted a cohort study using data from the Swedish Heart Failure Registry and found an association between K+ levels and mortality, with the lowest risk of mortality observed at a K+ level of 4.2 mmol/L.58 Additionally, Linde et al reported that serum K+ >4.6 mmol/L is associated with an increased risk of 90-day mortality, while serum K+ >4.8 mmol/L in chronic HF patients increases all‐cause mortality risk.60 K+ is vital in maintaining the electrical activity of the heart, and imbalances in K+ levels can disrupt normal cardiac rhythm and function.59,60 Therefore, hypokalemia can lead to arrhythmias and impaired contractility, while hyperkalemia can cause cardiac conduction abnormalities and potentially fatal arrhythmias.
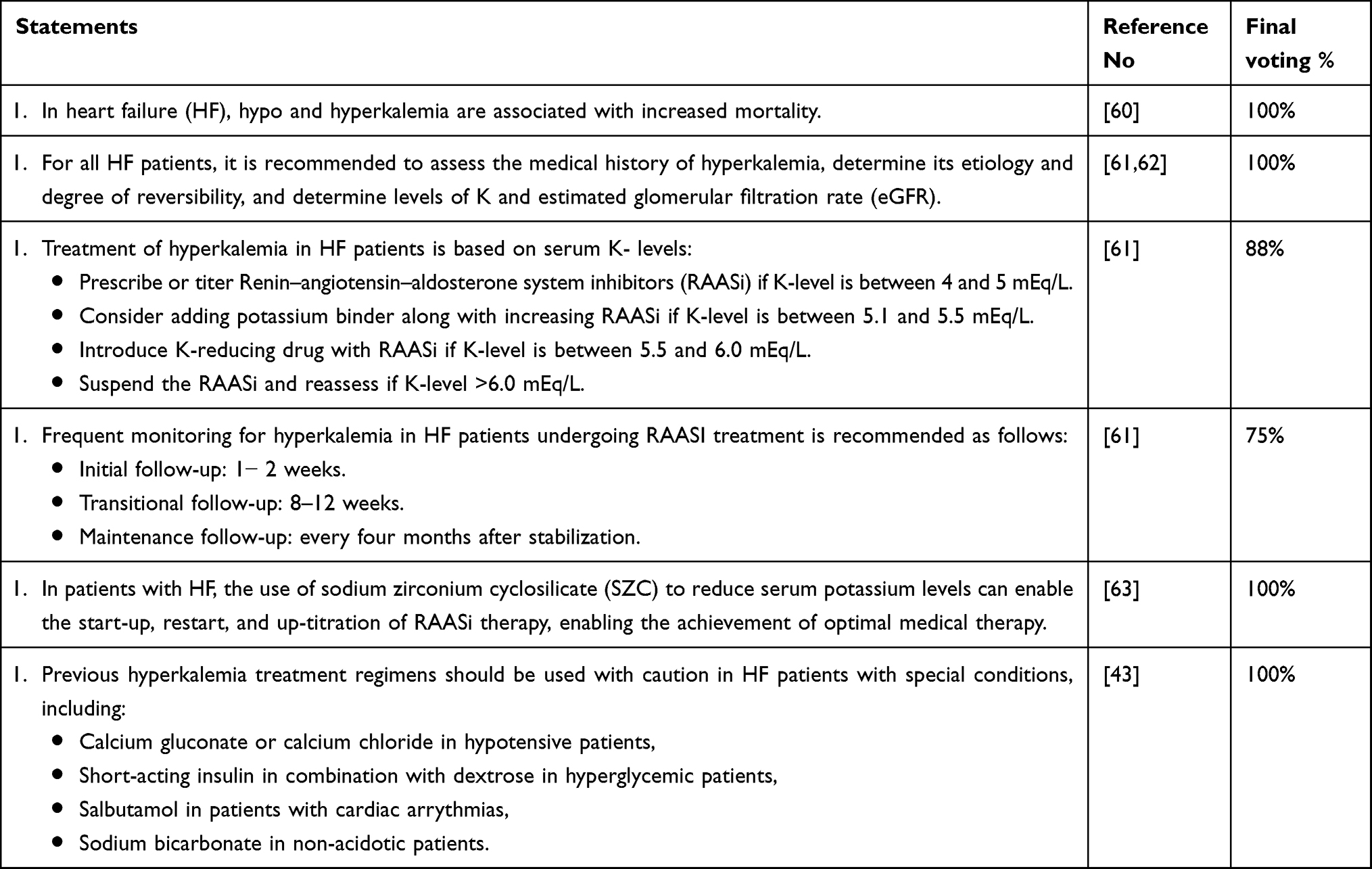 |
Table 3 Managing Hyperkalemia in Patients with Heart Failure |
The panel agrees that in HF patients, it is recommended to assess the medical history of hyperkalemia, determine its etiology and degree of reversibility, and determine levels of K+ and estimated glomerular filtration rate (eGFR), as advised by published literature.61,64,65
Also, the majority of the panel’s members (88%) agree that the management of hyperkalemia in patients with HF is based on serum K+ levels. This statement advises different treatment strategies for four K+ thresholds suggested by studies on hyperkalemic individuals with HF.61,66,67 The panel recommends prescribing or up tittering RAASi if K+-level is between 4 and 5.5mEq/L, adding potassium-binder when considering up titrating RAASi if K-level is between 5.1 and 5.5mEq/L, adding K-reducing drug to RAASi if K-level is between 5.5 and 6.0mEq/L, and finally withholding RAASi and reassess if K-level >6.0mEq/L. However, this approach differs from what is recommended in a multidisciplinary study that suggests the up titration of RAASi should not be restricted if serum K+ levels between 5.1 and 5.5 mEq/L, introducing novel potassium-binders with RAASi up titration when serum K+ levels >5.5 mEq/L, and discontinuing or reducing RAASi and introducing potassium-binders when serum K+ >6.0mEq/L.66
The majority of the panel’s members (75%) agree that HF patients receiving RAASi should be monitored for hyperkalemia frequently. The phrase implies that the first follow-up should occur 1–4 weeks after the initiation of RAASi; however, experts recommend reducing the time range to 1–2 weeks. Therefore, the panel agrees that the initial assessment after RAASi initiation should be at 1–2 weeks, followed by further evaluations at 8–12 weeks, and thereafter every four months once stability is achieved.66 Furthermore, the panel recommends to closely observe the serum potassium levels during a period of 7 to 10 days after initiating RAASi treatment and while adjusting the dosage.68 Although published literature agrees with the importance of frequent monitoring for hyperkalemia in HF patients receiving RAASi, some suggest that serum K+ levels should be checked first 48–72 hours after RAASi introduction and again a week later, then a month later, then every 3–6 months after.66,68–70
The panel agrees that SZC by lowering serum K+ levels facilitates the initiation, the reintroduction, and the up-titration of RAASi, allowing the optimization of medical therapy in HF patients, as shown in published studies.71–75
Finally, the panel agrees that current treatment regimens for acute hyperkalemia should be used with caution in certain groups of HF patients. This statement is divided into four sections. The first one discusses the cautious use of calcium gluconate or calcium chloride in hypotensive patients for the treatment of hyperkalemia. This is supported by a few studies showing that the administration of calcium gluconate or calcium chloride is not without risks. Since, extravasation of intravenous calcium preparations, such as calcium gluconate, can lead to complications such as calcinosis cutis, skin necrosis, and bullous reactions.76 Therefore, studies recommend that caution should be exercised when using these treatments, and healthcare professionals should be aware of the potential risks and monitor patients closely. However, other studies oppose this statement demonstrating that the administration of calcium gluconate or calcium chloride for hyperkalemia in hypotensive patients counteract the effects of elevated K+ levels on the heart.39,77,78
The second section deals with the use of short-acting intravenous insulin in combination with dextrose to shift K+ intracellularly, that must be used with caution in hyperglycemic patients for the treatment of hyperkalemia, and consider the risk of hypoglycemia.79–81 Hence, it is advised to supply enough glucose to prevent hypoglycemia, and careful glucose monitoring is essential while treating hyperkalemia with insulin and dextrose.81,82 The third part discusses the use of salbutamol for the treatment of hyperkalemia in patients with cardiac arrhythmias. Several studies highlighted the possible risks of cardiac arrhythmias like atrial fibrillation, supraventricular tachycardia, complete heart block, and ventricular tachycardia associated with salbutamol use.83 Another study linked salbutamol use to side effects including lactic acidosis, hyperglycemia, ketosis, diastolic hypotension, myocardial damage, and cardiac arrhythmias.84 Furthermore, in a study conducted on healthy individuals participating in intense rowing exercise, salbutamol administration attenuated exercise-induced hyperkalemia but exacerbated post-exercise hypokalemia. Additionally, impaired cardiac repolarization (QT hysteresis) associated with hypokalemia was observed suggesting that salbutamol may have an impact on cardiac electrical activity.85 Overall, these studies indicate that salbutamol use should be approached with caution in hyperkalemic patients with cardiac arrhythmias.
The fourth section advises on the cautious use of sodium bicarbonate in non-acidotic patients to treat hyperkalemia. Sodium bicarbonate is commonly used in the management of hyperkalemia, particularly in patients with metabolic acidosis; however, the use of sodium bicarbonate in non-acidotic hyperkalemic patients can lead to metabolic alkalosis, and/or hypernatremia.3,86 Hypocalcemia can also occur as a side effect of sodium bicarbonate administration due to the pH-dependent binding of calcium by bicarbonate. In addition, fluid overload, bloating, nausea, vomiting, and abdominal pain are common side effects reported after the use of sodium bicarbonate.3,87 Hence, sodium bicarbonate should be used with caution in non-acidotic hyperkalemic patients, and alternative treatments such as sodium polystyrene sulfonate may be considered.88
Management of Hyperkalemia in Patients with CKD
Statements related to the causes and the management of hyperkalemia in patients with CKD are outlined in Table 4. The majority of the panel (88%) agree that diabetic patients with CKD are more prone to hyperkalemia due to several factors. Firstly, CKD progression in itself can lead to hyperkalemia, especially in diabetics, since it leads to reduction in the urinary excretion of K+, causing K+ accumulation in the body.89 Furthermore, diabetic patients with CKD may develop renal tubular acidosis type 4 or hyporeninemic hypoaldosteronism, which is characterized by decreased ammonium excretion and impaired urinary acidification and impaired renal K+ excretion due to decreased mineralocorticoid activity.90 Other factors include the use of K+-sparing diuretics, such as spironolactone, which can increase serum K+ levels by inhibiting aldosterone activity.91
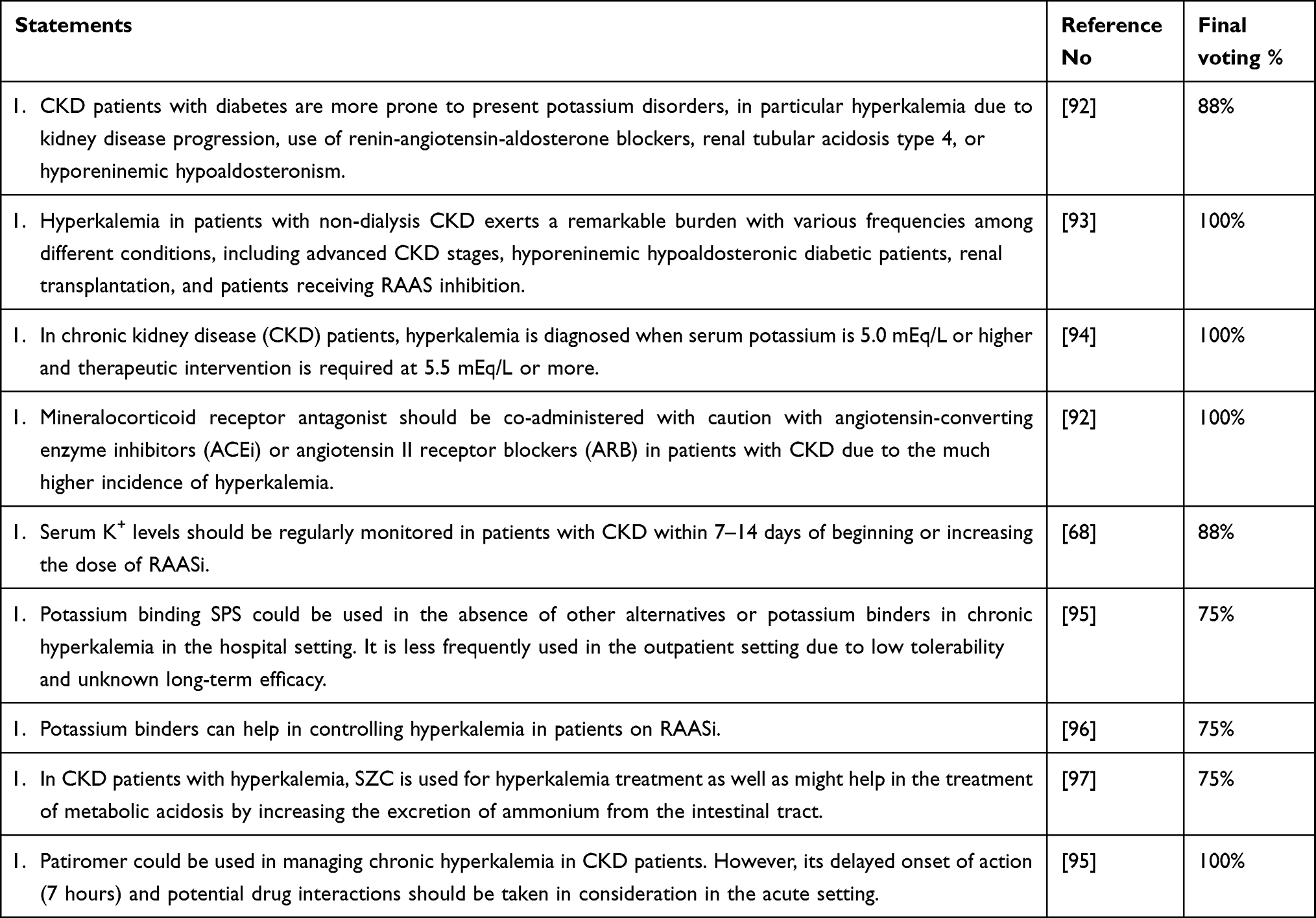 |
Table 4 Managing Hyperkalemia in Patients with CKD |
The panel also states that patients with CKD not treated by kidney replacement therapy with hyperkalemia experience a significant health and economic burden, that varies based on patient’s condition, such as CKD stage, hyporeninemic hypoaldosteronism in diabetic patients, renal transplantation, and RAASi use, in agreement with published literature.1,2,98
The panel also agrees that hyperkalemia in patients with CKD is present when serum K+ is 5.0 mEq/L or higher, with therapeutic intervention required at a level of 5.5 mEq/L or higher due to its association with increased risk of death, cardiovascular disease, hospitalization, and CKD progression, as supported by published literature.94,99,100 They also advised on the co-administration of mineralocorticoid receptor antagonists with RAASi in patients with CKD cautiously due to the increased incidence of hyperkalemia, in line with published literature.57,99,101,102
Furthermore, the majority of the panel (88%) agree that serum K+ levels should be regularly monitored in patients with CKD within 7–14 days of initiating or increasing the dose of RAASi. Published literature provides varying monitoring window duration.66,69,100 Chapman et al reported that repeated laboratory testing between 10 and 14 days after delaying, initiating, or adjusting RAASi dose is crucial, and close monitoring is essential once a stable RAASi dose is achieved.69 Blood K+ levels should be also checked at 48–72 hours and again after one week after initiating or increasing the dosage of a new potassium-binder.66
The majority of the panel (75%) agree that the potassium-binder sodium polystyrene sulfonate could be used in the absence of other potassium-binders for hyperkalemia in the hospital setting but not in the outpatient setting due to poor tolerability, uncertain onset of action, and unexpected K-lowering magnitude.103 Proper history and physical examination should be conducted before the initiation of SPS in any patient, and all interprofessional healthcare team members must be cautious when considering using SPS for the treatment of hyperkalemia if there is no available alternative medication. According to the recent international cardiorenal guidelines, the two-novel potassium-binders are safe and well tolerated for the management of chronic hyperkalemia, enabling RAASi utilization.104,105 Therefore, clinicians should now attempt to use the new potassium-binders to treat hyperkalemia.
The majority of the panel members (75%) agree that potassium-binders can help control hyperkalemia in patients on RAASi, as shown by several studies,68,106 and that the new potassium-binders can facilitate the continuation and optimization of RAASi, allowing the maintenance or up-titration of RAASi to maximum target doses.1,66 Additionally, potassium-binders utilization can increase primary care physicians and internists confidence in managing hyperkalemia.68
Studies have shown that SZC effectively reduces serum K+ levels in patients with hyperkalemia, leading to normokalemia within a few hours of the first dose.107 SZC exhibits non-pH-dependent binding of K+ throughout the gastrointestinal tract, including the small intestine,108 In addition, the majority of the panel members agree that SZC used for hyperkalemia may also have potential benefits of correcting CKD-associated metabolic acidosis by increasing ammonium excretion from the intestinal tract.109
The panel agree that patiromer could be used in managing chronic hyperkalemia in patients with CKD, while considering patient comorbidities, practical limitations due to drug-to-drug interactions and delayed onset of action particularly when rapid potassium control is needed.110–113
Table 5 addresses hyperkalemia management in hemodialysis patients. The majority of the panel members agree on the definition of hyperkalemia in hemodialysis patients as a serum K+ level of ≥5.5 mmol/L and that it is a common electrolyte disorder in this population. This statement is consistent with published literature.114,115 However, other groups characterize hyperkalemia in hemodialysis as serum K+ concentrations greater than 5.0 mmol/l.108,116
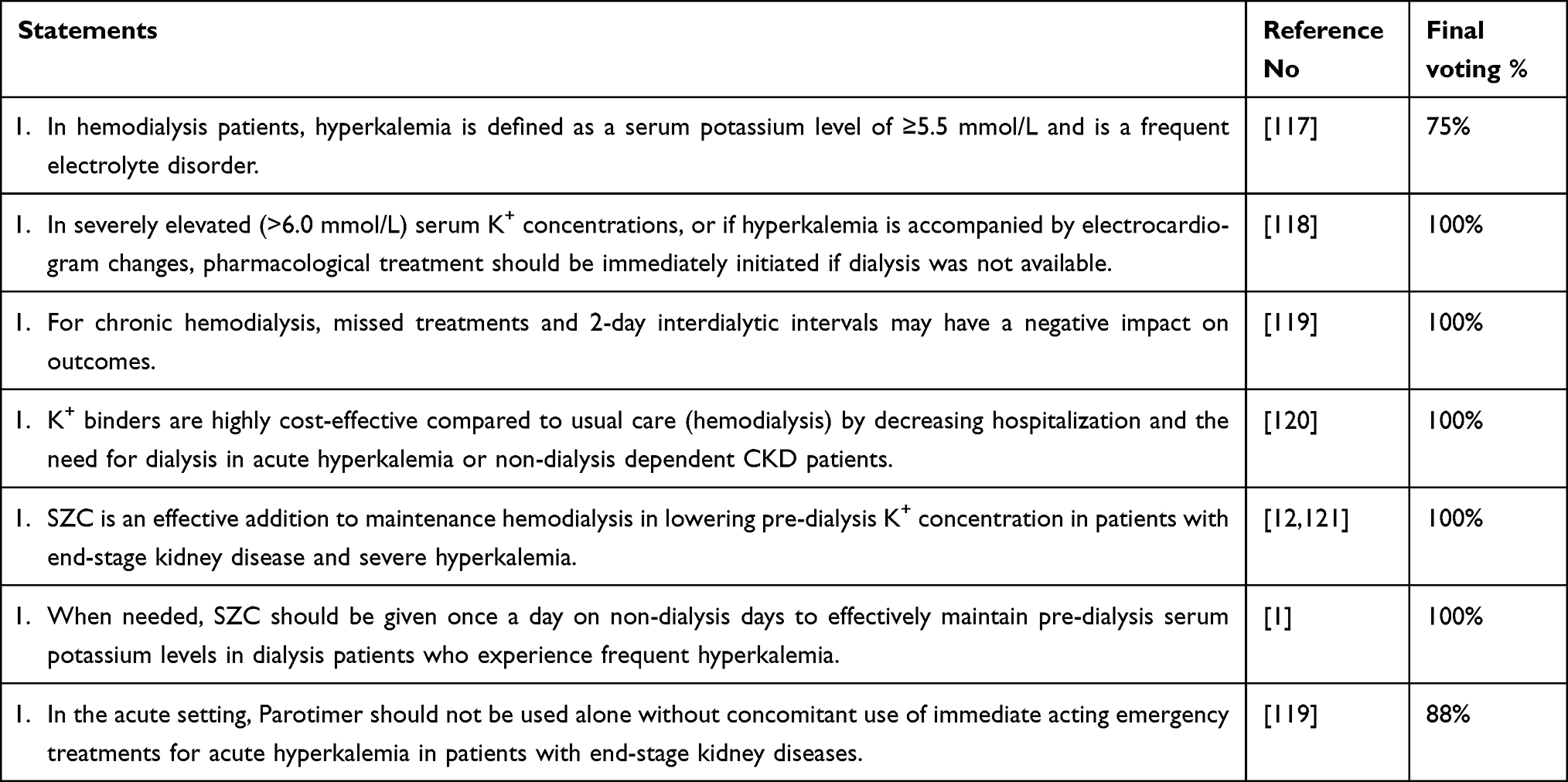 |
Table 5 Managing Hyperkalemia in Patients on Hemodialysis |
The panel agrees that in severely elevated serum K+ concentrations (>6.0 mmol/L), or if hyperkalemia is accompanied by ECG changes, pharmacological treatment should be initiated immediately if dialysis is not available.3,14
Chronic hemodialysis is a crucial treatment for patients with kidney failure, and the panel agreed that missed dialysis sessions and prolonged (>2-day) interdialytic intervals may have a negative impact on chronic hemodialysis outcomes,122 and treatment can be challenging.113
The panel also agrees that K+ binders are highly cost-effective compared to usual care (hemodialysis), since the use of this medication is reported to decrease hospitalization and the need for dialysis in acute hyperkalemia or patients with CKD not treated by kidney replacement therapy, and hyperkalemic events.120,123
The panel advises that SZC should be given once a day on non-dialysis days to effectively maintain pre-dialysis serum K+ levels in hemodialysis patients who experience frequent hyperkalemia. As per the DIALIZE trial, the only double-blind randomized control trial on hemodialysis patients, SZC can be administered on non-dialysis days at 5 g once daily, with the option of gradually up-titrating the dose if needed depending on patients’ response and on pre-dialysis serum K+ value after the long interdialytic interval.52,121,124
Closure Statements with Future Steps
Finally, the experts discussed future steps and recommendations for hyperkalemia treatment and improved outcomes, as outlined in Table 6.
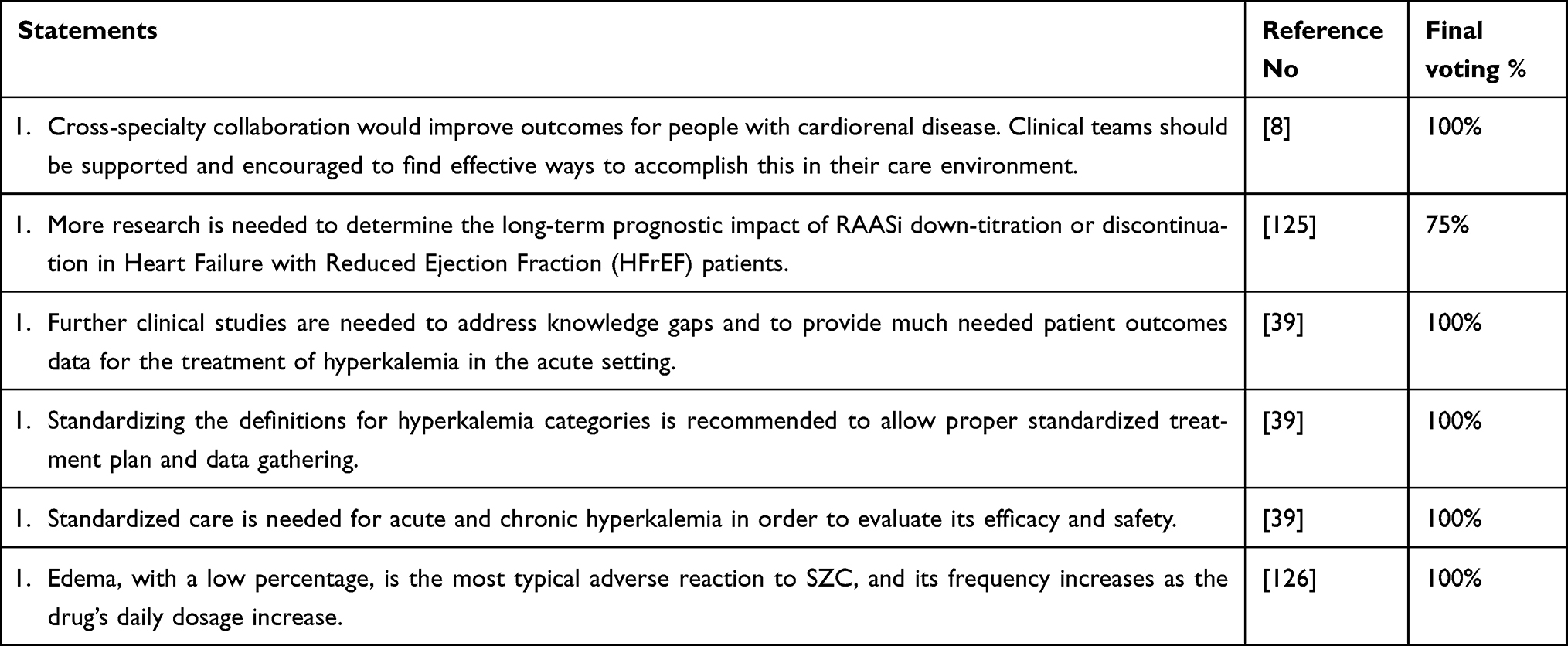 |
Table 6 Closure Statements with Future Steps |
The panel agrees that the management of hyperkalemic patients with cardiorenal disease requires a multidisciplinary approach involving healthcare professionals from various specialties, including primary care physicians, cardiologists, nephrologists, and endocrinologists, and that collaborative care teams can provide holistic, coordinated, and specialized care, leading to improved patient outcomes and optimized healthcare resources.127
The majority of the panel members (75%) suggest that more research is needed to determine the long-term prognostic impact of RAASi down-titration or discontinuation in patients with HFrEF. This statement is supported by calls for more research in published literature since guidelines recommend maximal RAASi dosing to improve clinical outcomes; however, this is often limited by the development of hyperkalemia.66 In addition, some evidence suggests that RAASi submaximal dosing and discontinuation may increase risks of adverse outcomes in patients with cardiorenal disorders such as faster progression to kidney failure, hospitalizations due to cardiovascular causes, and cardiovascular mortality at mid-to-long-term, and RAASi discontinuation may increase healthcare costs associated with such poor outcomes.123
The panel agrees that further clinical studies are also needed to address knowledge gaps and provide much-needed patient outcomes data for the treatment of hyperkalemia, as studies have indicated that there are significant unmet needs for managing hyperkalemia effectively, particularly in acute setting.39,68 The panel also suggests to develop a comprehensive review paper that outlines the knowledge gaps in management of acute and severe hyperkalemia in outpatients, guides best practices in the development of care and reporting recommendations and issues a call to action on the research needs.8
The panel also highlights the need for standardized definitions for hyperkalemia categories to allow proper standardized treatment plans and data gathering, since published literature lacks a clear definition for grading hyperkalemia severity as mild, moderate, or severe, to allow proper treatment and data gathering standardization.34,68,128
The panel reiterates the importance of establishing a standardized approach in acute and chronic hyperkalemia and evaluate its effectiveness among patients in Kuwait based on clinical presentation, K+ levels and comorbidities. The efficacy and safety of the different treatments for acute and chronic hyperkalemia in published literature are poorly explored.3,39,100,129
The panel also agrees that peripheral edema was the most common adverse event of 15 g SZC. It is observed at a low rate of 5.7% in clinical trials, with 53% of the edema resolving on its own without any intervention and 47% resolved after adjustment of diuretic dose.130 However, it is important to note that the 15 g dose is not approved nor available in GCC countries and hence, the risk is minimal. In addition, no gastrointestinal side effects were observed even when given on empty stomach and there are no significant drug–drug interactions reported with oral medications except for a limited list of PH-dependent drugs, including azole antifungals, anti-HIV drugs, tyrosine kinase inhibitors and tacrolimus. However, they should be administered at least ±2 hours before or after SZC intake to avoid any interaction.55,107,131
Conclusion
The management of hyperkalemia lacks standardized definitions and treatment threshold and lacks consistent guidelines and laboratory practices. This local consensus provides guidance and recommendations for healthcare practitioners in Kuwait for hyperkalemia management in acute settings, in HF, in CKD not treated by kidney replacement therapy, and in hemodialysis. It encourages the utilization of the new odorless and tasteless potassium-binder, SZC, due to its rapid onset of action (which is particularly helpful in acute settings) as well as its efficacy, tolerability and safety for patients with multiple comorbidities and on multiple oral medications. Moreover, this consensus highlights the need for future cross-specialty collaboration, standardized definitions and treatment protocols, and more research to address knowledge gaps related to hyperkalemia management.
Sponsorship
This research is sponsored by AstraZeneca Kuwait.
Ethical Approval
Not Applicable.
Acknowledgments
Authors thank CTI Clinical Trial and Consulting Services FZLCC-Middle East for the support in the consensus development, manuscript writeup, and submission.
Author Contributions
All authors made a significant contribution to the work reported including conception, design, execution, acquisition of data, analysis and interpretation; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Morales E, Cravedi P, Manrique J. Management of Chronic Hyperkalemia in Patients With Chronic Kidney Disease: an Old Problem With News Options. Front Med Lausanne. 2021;8. doi:10.3389/fmed.2021.653634
2. Hunter RW, Bailey MA. Hyperkalemia: pathophysiology, risk factors and consequences. Nephrol Dial Transplant. 2019;34. doi:10.1093/ndt/gfz206
3. Dépret F, Peacock WF, Liu KD, Rafique Z, Rossignol P, Legrand M. Management of hyperkalemia in the acutely ill patient. Ann Intensive Care. 2019;9. doi:10.1186/s13613-019-0509-8
4. Costa D, Patella G, Provenzano M, et al. Hyperkalemia in CKD: an overview of available therapeutic strategies 2023.
5. Nakano T, Tanaka S, Tsuruya K, Kitazono T. Low intake of β carotene and dietary fiber from vegetables and fruits in patients with chronic kidney disease. Sci Rep. 2022;12. doi:10.1038/s41598-022-24471-4
6. Palmer BF, Clegg DJ. SGLT2 Inhibition and Kidney Potassium Homeostasis 2023.
7. Sarnowski A, Gama RM, Dawson A, Mason H, Banerjee D. Hyperkalemia in Chronic Kidney Disease: links, Risks and Management. Int J Nephrol Renovasc Dis. 2022;15. doi:10.2147/IJNRD.S326464
8. Chiu M, Garg AX, Moist L, Jain AK. A New Perspective to Longstanding Challenges with Outpatient Hyperkalemia: a Narrative Review. Can J Kidney Health Dis. 2023;10. doi:10.1177/20543581221149710
9. Mushiyakh Y, Dangaria H, Qavi S, Ali N, Pannone J, Tompkins D. Treatment and pathogenesis of acute hyperkalemia. J Community Hosp Intern Med Perspect. 2011;1. doi:10.3402/jchimp.v1i4.7372
10. Fishbane S, Ford M, Fukagawa M, et al. A Phase 3B, randomized, double-blind, placebo-controlled study of sodium zirconium cyclosilicate for reducing the incidence of predialysis hyperkalemia. J Am Soc Nephrol. 2019:30. doi:10.1681/ASN.2019050450
11. Hoorn EJ, Gritter M, Cuevas CA, Fenton RA. Regulation of the renal NaCl cotransporter and its role in potassium homeostasis. Physiol Rev. 2020;100. doi:10.1152/physrev.00044.2018
12. Peacock WF, Rafique Z, Vishnevskiy K, et al. Emergency Potassium Normalization Treatment Including Sodium Zirconium Cyclosilicate: a Phase II, Randomized, Double-blind, Placebo-controlled Study (ENERGIZE). Acad Emergency Med. 2020:27. doi:10.1111/acem.13954
13. Lin Z, Zheng J, Liu X, Hu X, Fuxian R, Gao D. Assessing potassium levels in critically ill patients with heart failure: application of a group-based trajectory model. ESC Heart Fail. 2023;10. doi:10.1002/ehf2.14161
14. Simon LV, Hashmi MF, Farrell MW. Hyperkalemia. StatPearls Publishing LLC; 2023.
15. Davis J, Israni R, Betts KA, et al. Real-World Management of Hyperkalemia in the Emergency Department: an Electronic Medical Record Analysis. Adv Ther. 2022:39. doi:10.1007/s12325-021-02017-w
16. Schütt B, Kunz M, Blode H. Coadministration of estradiol/drospirenone and indomethacin does not cause hyperkalemia in healthy postmenopausal women: a randomized open-label crossover study. J Clin Pharmacol. 2007;47. doi:10.1177/0091270007300952
17. Shrimanker I, Bhattarai S. Electrolytes. StatPearls Publishing; 2023.
18. Hedbäck T, Chantzi Christos D. ABC om Hyperkalemi. Lakartidningen. 2023;120.
19. Ni Z, Jin H, Lu R, et al. Hyperkalaemia prevalence, recurrence and treatment in patients on haemodialysis in China: protocol for a prospective multicentre cohort study (PRECEDE-K). BMJ Open. 2021:11. doi:10.1136/bmjopen-2021-055770
20. Gorriz JL, D’Marco L, Pastor-González A, et al. Long-term mortality and trajectory of potassium measurements following an episode of acute severe hyperkalaemia. Nephrol Dial Transplant. 2022:37. doi:10.1093/ndt/gfab003
21. Lehnhardt A, Kemper MJ. Pathogenesis, diagnosis and management of hyperkalemia. Pediatr Nephrol. 2011;26. doi:10.1007/s00467-010-1699-3
22. Burton JO, Coats AJS, Kovesdy CP, et al. An international Delphi consensus regarding best practice recommendations for hyperkalaemia across the cardiorenal spectrum. Eur J Heart Fail. 2022:24. doi:10.1002/ejhf.2612
23. Brueske B, Sidhu MS, Schulman-Marcus J, Kashani KB, Barsness GW, Jentzer JC. Hyperkalemia is associated with increased mortality among unselected cardiac intensive care unit patients. J Am Heart Assoc. 2019;8. doi:10.1161/JAHA.118.011814
24. Kanda E, Kashihara N, Kohsaka S, Okami S, Yajima T. Clinical and Economic Burden of Hyperkalemia: a Nationwide Hospital-Based Cohort Study in Japan. Kidney Med. 2020;2. doi:10.1016/j.xkme.2020.09.003
25. Betts KA, Woolley JM, Mu F, et al. Postdischarge Health Care Costs and Readmission in Patients With Hyperkalemia-Related Hospitalizations. Kidney Int Rep. 2020;5. doi:10.1016/j.ekir.2020.06.004
26. Damianaki A, Wuerzner G. Hyperkaliemia in hypertensive patients: more than a coincidence? Rev Med Suisse. 2023.
27. Vodošek Hojs N, Bevc S, Ekart R, Piko N, Petreski T, Hojs R. Mineralocorticoid receptor antagonists in diabetic kidney disease. Pharmaceuticals. 2021;14. doi:10.3390/ph14060561
28. Watanabe R. Hyperkalemia in chronic kidney disease. Rev Assoc Med Bras. 2020;66. doi:10.1590/1806-9282.66.S1.31
29. AlSahow A, AbdulShafy M, Al‐Ghamdi S, et al. Prevalence and management of hyperkalemia in chronic kidney disease and heart failure patients in the Gulf Cooperation Council (GCC). J Clin Hypertens.
30. Ismail U, Sidhu K, Zieroth S. Hyperkalaemia in Heart Failure. Card Fail Rev. 2021;7. doi:10.15420/cfr.2020.29
31. Jun M, Jardine MJ, Perkovic V, et al. Hyperkalemia and renin-angiotensin aldosterone system inhibitor therapy in chronic kidney disease: a general practice-based, observational study. PLoS One. 2019:14. doi:10.1371/journal.pone.0213192
32. Zhang J, He X, Wu J. The Impact of Hyperkalemia on Mortality and Healthcare Resource Utilization Among Patients With Chronic Kidney Disease: a Matched Cohort Study in China. Front Public Health. 2022;10. doi:10.3389/fpubh.2022.855395
33. Hougen I, Leon SJ, Whitlock R, et al. Hyperkalemia and its Association With Mortality, Cardiovascular Events, Hospitalizations, and Intensive Care Unit Admissions in a Population-Based Retrospective Cohort. Kidney Int Rep. 2021:6. doi:10.1016/j.ekir.2021.02.038
34. Lindner G, Burdmann EA, Clase CM, et al. Acute hyperkalemia in the emergency department: a summary from a Kidney Disease: improving Global Outcomes conference.
35. Sharma A, Alvarez PJ, Woods SD, Fogli J, Dai D. Healthcare resource utilization and costs associated with hyperkalemia in a large managed care population. J Pharm Health Serv Res. 2021;12. doi:10.1093/jphsr/rmaa004
36. Kathryn Fitch J, Michael W, Tyler E, et al. The Clinical and Economic Burden of Hyperkalemia on Medicare and Commercial Payers. Am Health Drug Benefits. 2017;10(4):202–210.
37. Agarwal R, Joseph A, Anker SD, et al. Hyperkalemia Risk with Finerenone: results from the FIDELIO-DKD Trial. J Am Soc Nephrol. 2022:33. doi:10.1681/ASN.2021070942
38. Clegg DJ, Headley SA, Germain MJ. Impact of Dietary Potassium Restrictions in CKD on Clinical Outcomes: benefits of a Plant-Based Diet. Kidney Med. 2020;2. doi:10.1016/j.xkme.2020.04.007
39. Rafique Z, Peacock F, Armstead T, et al. Hyperkalemia management in the emergency department: an expert panel consensus. J Am Coll Emerg Physicians Open. 2021:2. doi:10.1002/emp2.12572
40. Emektar E. Acute hyperkalemia in adults. Turk J Emerg Med. 2023;23. doi:10.4103/tjem.tjem_288_22
41. Varga C, Kálmán Z, Szakáll A, et al. ECG alterations suggestive of hyperkalemia in normokalemic versus hyperkalemic patients. BMC Emerg Med. 2019:19. doi:10.1186/s12873-019-0247-0
42. Rossignol P, Legrand M, Kosiborod M, et al. Emergency management of severe hyperkalemia: guideline for best practice and opportunities for the future. Pharmacol Res. 2016:113. doi:10.1016/j.phrs.2016.09.039
43. Sidhu K, Sanjanwala R, Zieroth S. Hyperkalemia in heart failure. Curr Opin Cardiol. 2020;35. doi:10.1097/HCO.0000000000000709
44. Kosiborod M, Rasmussen HS, Lavin P, et al. Effect of sodium zirconium cyclosilicate on potassium lowering for 28 days among outpatients with hyperkalemia: the HARMONIZE randomized clinical trial. JAMA. 2014:312. doi:10.1001/jama.2014.15688
45. Abuelo JG. Treatment of Severe Hyperkalemia: confronting 4 Fallacies. Kidney Int Rep. 2018;3. doi:10.1016/j.ekir.2017.10.001
46. Dockery S, Dupré A, Deflorio P, Murray BP. Emergency Department Presentation of Life-threatening Symptomatic Hyperkalemia From an Angiotensin Receptor Blocker in a Low-risk Individual. Mil Med. 2022. doi:10.1093/milmed/usac376
47. Saad SM, Yasin S, Jain N, LeLorier P. Cardiac Manifestations in a Case of Severe Hyperkalemia. Cureus. 2021. doi:10.7759/cureus.13641
48. Hundemer GL, Talarico R, Tangri N, et al. Ambulatory treatments for raas inhibitor–related hyperkalemia and the 1-year risk of recurrence. Clin J Am Soc Nephrol. 2021;16. doi:10.2215/CJN.12990820
49. Georgianos PI, Agarwal R. Revisiting RAAS blockade in CKD with newer potassium-binding drugs. Kidney Int. 2018;93. doi:10.1016/j.kint.2017.08.038
50. Cañas AE, Troutt HR, Jiang L, et al. A randomized study to compare oral potassium binders in the treatment of acute hyperkalemia. BMC Nephrol. 2023;24. doi:10.1186/s12882-023-03145-x
51. Liu M, Rafique Z. Acute Management of Hyperkalemia. Curr Heart Fail Rep. 2019;16. doi:10.1007/s11897-019-00425-2
52. Esposito P, Conti NE, Falqui V, et al. New treatment options for hyperkalemia in patients with chronic kidney disease. J Clin Med. 2020;9. doi:10.3390/jcm9082337
53. Amin AN, Menoyo J, Singh B, Kim CS. Efficacy and safety of sodium zirconium cyclosilicate in patients with baseline serum potassium level ≥ 5.5 mmol/L: pooled analysis from two phase 3 trials. BMC Nephrol. 2019;20. doi:10.1186/s12882-019-1611-8
54. Shrestha DB, Budhathoki P, Sedhai YR, et al. Patiromer and Sodium Zirconium Cyclosilicate in Treatment of Hyperkalemia: a Systematic Review and Meta-Analysis. Curr Ther Res Clin Exp. 2021;95. doi:10.1016/j.curtheres.2021.100635
55. Zhang Y, Xu R, Wang F, et al. Effects and Safety of a Novel Oral Potassium-Lowering Drug-Sodium Zirconium Cyclosilicate for the Treatment of Hyperkalemia: a Systematic Review and Meta-Analysis. Cardiovasc Drugs Ther. 2021;35. doi:10.1007/s10557-020-07134-2
56. Matsushita K, Sang Y, Yang C, et al. Dyskalemia, its patterns, and prognosis among patients with incident heart failure: a nationwide study of US veterans. PLoS One. 2019:14. doi:10.1371/journal.pone.0219899
57. Lisi F, Parisi G, Gioia MI, et al. Mineralcorticoid Receptor Antagonist Withdrawal for Hyperkalemia and Mortality in Patients with Heart Failure. Cardiorenal Med. 2020:10. doi:10.1159/000505286
58. Basnet S, Dhital R, Tharu B, Ghimire S, Poudel DR, Donato A. Influence of abnormal potassium levels on mortality among hospitalized heart failure patients in the US: data from National Inpatient Sample. J Community Hosp Intern Med Perspect. 2019;9. doi:10.1080/20009666.2019.1593778
59. Beusekamp JC, Tromp J, Cleland JGF, et al. Hyperkalemia and Treatment With RAAS Inhibitors During Acute Heart Failure Hospitalizations and Their Association With Mortality. JACC Heart Fail. 2019;7. doi:10.1016/j.jchf.2019.07.010
60. Linde C, Qin L, Bakhai A, et al. Serum potassium and clinical outcomes in heart failure patients: results of risk calculations in 21 334 patients in the UK. ESC Heart Fail. 2019:6. doi:10.1002/ehf2.12402
61. Almenar Bonet L, Franco G. Consensus on the management of hyperkalemia in patients with heart failure: recommendations from the SEC-SEMI. Rev Clin Esp. 2022;222. doi:10.1016/j.rce.2020.11.009
62. Mullens W, Damman K, Testani JM, et al. Evaluation of kidney function throughout the heart failure trajectory – a position statement from the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2020:22. doi:10.1002/ejhf.1697
63. Williams R, James A, Ashton M, Vaughan S, Wong A. Use of sodium zirconium cyclosilicate for up-Titration of renin-Angiotensin-Aldosterone system inhibitor therapy in patients with heart failure: a case series. Eur Heart J Case Rep. 2021;5. doi:10.1093/ehjcr/ytab281
64. Crespo-Leiro MG, Barge-Caballero E, Segovia-Cubero J, et al. Hyperkalemia in heart failure patients in Spain and its impact on guidelines and recommendations: ESC-EORP-HFA Heart Failure Long-Term Registry. Revista Española de Cardiología. 2020;73. doi:10.1016/j.rec.2019.05.015
65. Thomsen RW, Nicolaisen SK, Hasvold P, et al. Elevated potassium levels in patients with congestive heart failure: occurrence, risk factors, and clinical outcomes a Danish population-based cohort study. J Am Heart Assoc. 2018;7. doi:10.1161/JAHA.118.008912
66. Silva-Cardoso J, Brito D, Frazão JM, et al. Management of RAASi-associated hyperkalemia in patients with cardiovascular disease. Heart Fail Rev. 2021;26. doi:10.1007/s10741-020-10069-3
67. Rakisheva A, Marketou M, Klimenko A, Troyanova-Shchutskaia T, Vardas P. Hyperkalemia in heart failure: foe or friend? Clin Cardiol. 2020;43:666–675. doi:10.1002/clc.23392
68. Palmer BF, Jesus Carrero J, Clegg DJ, Colbert GB, Emmett M. Clinical Management of Hyperkalemia
69. Chapman A, Gunning S. Real-World Associations Between Renin-Angiotensin-Aldosterone System Inhibition Therapy, Hyperkalemia, and Outcomes: a Clinical and Scientific Call to Action. J Am Heart Assoc. 2019;8. doi:10.1161/JAHA.119.014845
70. Kanda E, Rastogi A, Murohara T, et al. Clinical impact of suboptimal RAASi therapy following an episode of hyperkalemia. BMC Nephrol. 2023;24. doi:10.1186/s12882-022-03054-5
71. Oshima A, Imamura T, Narang N, Kinugawa K. Management of hyperkalemia in chronic heart failure using sodium zirconium cyclosilicate. Clin Cardiol. 2021;44. doi:10.1002/clc.23683
72. Nassif ME, Kosiborod M. New frontiers for management of hyperkalaemia: the emergence of novel agents. Eur Heart J. 2019;21. doi:10.1093/eurheartj/suy036
73. Murphy D, Ster IC, Kaski JC, Anderson L, Banerjee D. The LIFT trial: study protocol for a double-blind, randomised, placebo-controlled trial of K+-binder Lokelma for maximisation of RAAS inhibition in CKD patients with heart failure. BMC Nephrol. 2021;22. doi:10.1186/s12882-021-02439-2
74. Imamura T, Oshima A, Narang N, Kinugawa K. Clinical implications of sodium zirconium cyclosilicate therapy in patients with systolic heart failure and hyperkalemia. J Clin Med. 2021;10. doi:10.3390/jcm10235523
75. Butler J, Khan MS, Anker SD. Novel potassium binders as enabling therapy in heart failure. Eur J Heart Fail. 2019;21. doi:10.1002/ejhf.1474
76. Gresham LN, Alallaf J, Shah J. Calcinosis Cutis as an Unsuspecting Complication of Hyperkalemia Treatment. Cureus. 2021. doi:10.7759/cureus.17018
77. Yoo N, Song YB, Dubinsky I, Altshuler J. Single Dose of Sodium Zirconium Cyclosilicate Versus Sodium Polystyrene Sulfonate in Hospitalized Patients With Hyperkalemia. Ann. Pharmacother. 2022. doi:10.1177/10600280221141918
78. Kaisbain N, Lim WJ, Kaisbain V. Verapamil-Induced Hypotension in End-Stage Renal Disease: the Role of Calcium Gluconate. Cureus. 2023. doi:10.7759/cureus.33341
79. Boughton CK, Dixon D, Goble E, et al. Preventing hypoglycemia following treatment of hyperkalemia in hospitalized patients. J Hosp Med. 2019:14. doi:10.12788/jhm.3145
80. Crnobrnja L, Metlapalli M, Jiang C, Govinna M, Lim AKH. The Association of Insulin-dextrose Treatment with Hypoglycemia in Patients with Hyperkalemia. Sci Rep. 2020;10. doi:10.1038/s41598-020-79180-7
81. Farkas JD, Long B, Koyfman A, Menson K. BRASH Syndrome: bradycardia, Renal Failure, AV Blockade, Shock, and Hyperkalemia. J Emergency Med. 2020;59. doi:10.1016/j.jemermed.2020.05.001
82. Harel Z, Kamel KS. Optimal dose and method of administration of intravenous insulin in the management of emergency hyperkalemia: a systematic review. PLoS One. 2016;11. doi:10.1371/journal.pone.0154963
83. Desai AD, Boursiquot BC, Melki L, Wan EY. Management of Arrhythmias Associated with COVID-19. Curr Cardiol Rep. 2021;23. doi:10.1007/s11886-020-01434-7
84. Walsh S, Pan S, Sheng Y, et al. Optimising intravenous salbutamol in children: a Phase 2 study. Arch Dis Child. 2023:108. doi:10.1136/archdischild-2022-324008
85. Atanasovska T, Smith R, Graff C, et al. Protection against severe hypokalemia but impaired cardiac repolarization after intense rowing exercise in healthy humans receiving salbutamol. J Appl Physiol. 2018:125. doi:10.1152/japplphysiol.00680.2017
86. Weinstein J, Girard L-P, Lepage S, McKelvie RS, Tennankore K. Prevention and management of hyperkalemia in patients treated with renin-angiotensin-aldosterone system inhibitors. CMAJ. 2021;193:E836–41. doi:10.1503/cmaj.210831
87. Goraya N, Wesson DE. Clinical evidence that treatment of metabolic acidosis slows the progression of chronic kidney disease. Curr Opin Nephrol Hypertens. 2019;28. doi:10.1097/MNH.0000000000000491
88. Bouchard J, Mehta RL. Timing of Kidney Support Therapy in Acute Kidney Injury: what Are We Waiting For? Am J Kidney Dis. 2022;79. doi:10.1053/j.ajkd.2021.07.014
89. Tian R, Li R, Zhou X. Recent Progresses in Non-Dialysis Chronic Kidney Disease Patients with Hyperkalemia: outcomes and Therapeutic Strategies. Medicina. 2023;59. doi:10.3390/medicina59020353
90. Akchurin OM. Chronic Kidney Disease and Dietary Measures to Improve Outcomes. Pediatr Clin North Am. 2019;66. doi:10.1016/j.pcl.2018.09.007
91. Adelborg K, Nicolaisen SK, Hasvold P, Palaka E, Pedersen L, Thomsen RW. Predictors for repeated hyperkalemia and potassium trajectories in high-risk patients — a population-based cohort study. PLoS One. 2019;14. doi:10.1371/journal.pone.0218739
92. Goia-Nishide K, Coregliano-Ring L. Érika Bevilaqua Rangel. Hyperka Diabe Mellitus Setting.
93. Borrelli S, Matarazzo I, Lembo E, et al. Chronic Hyperkaliemia in Chronic Kidney Disease: an Old Concern with New Answers. Int J Mol Sci. 2022;23. doi:10.3390/ijms23126378
94. Yamada S, Inaba M. Potassium metabolism and management in patients with ckd. Nutrients. 2021;13. doi:10.3390/nu13061751
95. De Nicola L, Di Lullo L, Paoletti E, Cupisti A, Bianchi S. Chronic hyperkalemia in non-dialysis CKD: controversial issues in nephrology practice. J Nephrol. 2018;31. doi:10.1007/s40620-018-0502-6
96. Natale P, Palmer SC, Ruospo M, Saglimbene VM, Strippoli GFM. Potassium binders for chronic hyperkalaemia in people with chronic kidney disease. Cochrane Database Syst Rev. 2020;2020. doi:10.1002/14651858.CD013165.pub2
97. Mori D, Namiki Y, Sugimachi A, et al. The effect of sodium zirconium cyclosilicate on acid-base balance in chronic kidney disease. Clin Nephrol. 2022;97. doi:10.5414/CN110688
98. Mu F, Betts KA, Woolley JM, et al. Prevalence and economic burden of hyperkalemia in the United States Medicare population. Curr Med Res Opin. 2020;36. doi:10.1080/03007995.2020.1775072
99. Di Lullo L, Ronco C, Granata A, et al. Chronic Hyperkalemia in Cardiorenal Patients: risk Factors, Diagnosis, and New Treatment Options. Cardiorenal Med. 2019;9. doi:10.1159/000493395
100. Palmer BF, Clegg DJ. Diagnosis and treatment of hyperkalemia. Cleve Clin J Med. 2017;84. doi:10.3949/ccjm.84a.17056
101. Watson K, Kukin A, Wasik AK, Shulenberger CE. Nonsteroidal Mineralocorticoid Receptor Antagonists: exploring Role in Cardiovascular Disease. J Cardiovasc Pharmacol. 2021;77. doi:10.1097/FJC.0000000000000990
102. Goenka L, Padmanaban R, George M. The Ascent of Mineralocorticoid Receptor Antagonists in Diabetic Nephropathy. Curr Clin Pharmacol. 2018;14. doi:10.2174/1574884713666181116100946
103. Sajedur R, Rachana M. Sodium Polystyrene Sulfonate. Treasure Island (FL): StatPearls Publishing; 2023.
104. Batterink J, Lin J, Au-Yeung SHM, Cessford T. Effectiveness of sodium polystyrene sulfonate for short-term treatment of hyperkalemia. Canadian J Hospital Pharm. 2015;68. doi:10.4212/cjhp.v68i4.1469
105. Rossignol P, Pitt B. Sodium polystyrene is unsafe and should not be prescribed for the treatment of hyperkalaemia: primum non nocere ! Clin Kidney J. 2023. doi:10.1093/ckj/sfad090
106. Rosano GMC, Spoletini I, Vitale C, Agewall S. Hyperkalemia and Renin–Angiotensin–Aldosterone System Inhibitors Dose Therapy in Heart Failure With Reduced Ejection Fraction. Card Fail Rev. 2019;5. doi:10.15420/cfr.2019.8.2
107. Spinowitz BS, Fishbane S, Pergola PE, et al. Sodium zirconium cyclosilicate among individuals with hyperkalemia: a 12-month phase 3 study. Clin J Am Soc Nephrol. 2019:14. doi:10.2215/CJN.12651018
108. Bansal S, Pergola PE. Current Management of Hyperkalemia in Patients on Dialysis. Kidney Int Rep. 2020;5. doi:10.1016/j.ekir.2020.02.1028
109. Marmol F, Badaruddin M, Baig A, et al. Fecal ammonium in mice with CKD: gastrointestinal sequestration by sodium zirconium cyclosilicate. Am J Physiol Renal Physiol. 2023:324. doi:10.1152/ajprenal.00312.2022
110. Haller H, Bianchi S, McCafferty K, et al. Safety and Efficacy of Patiromer in Hyperkalemic Patients with CKD: a Pooled Analysis of Three Randomized Trials. Kidney360. 2022:3. doi:10.34067/kid.0001562022
111. Pitt B, Bakris GL, Weir MR, et al. Long-term effects of patiromer for hyperkalaemia treatment in patients with mild heart failure and diabetic nephropathy on angiotensin-converting enzymes/angiotensin receptor blockers: results from AMETHYST-DN. ESC Heart Fail. 2018;5. doi:10.1002/ehf2.12292
112. Kovesdy CP, Rowan CG, Conrad A, et al. Real-World Evaluation of Patiromer for the Treatment of Hyperkalemia in Hemodialysis Patients. Kidney Int Rep. 2019:4. doi:10.1016/j.ekir.2018.10.020
113. Palmer BF. Potassium Binders for Hyperkalemia in Chronic Kidney Disease—Diet, Renin-Angiotensin-Aldosterone System Inhibitor Therapy, and Hemodialysis. Mayo Clin Proc. 2020;95. doi:10.1016/j.mayocp.2019.05.019
114. Fishbane S, Charytan DM, Chertow GM, et al. Consensus-Based Recommendations for the Management of Hyperkalemia in the Hemodialysis Setting. J Ren Nutr. 2022:32. doi:10.1053/j.jrn.2021.06.003
115. Belmar Vega L, Galabia ER, da da Silva J B, et al. Epidemiology of hyperkalemia in chronic kidney disease. Nefrologia. 2019:39. doi:10.1016/j.nefroe.2018.11.014
116. Shibata S, Uchida S. Hyperkalemia in patients undergoing hemodialysis: its pathophysiology and management. Therapeutic Apheresis Dialysis. 2022;26. doi:10.1111/1744-9987.13721
117. de Rooij ENM, Dekker FW, Le Cessie S, et al. Serum Potassium and Mortality Risk in Hemodialysis Patients: a Cohort Study. Kidney Med. 2022:4. doi:10.1016/j.xkme.2021.08.013
118. Pirklbauer M. Hemodialysis treatment in patients with severe electrolyte disorders: management of hyperkalemia and hyponatremia. Hemodialysis Int. 2020;24. doi:10.1111/hdi.12845
119. Best Practices in Managing in Chronic Kidney Disease. National Kidney Foundation.
120. Kim K, Fagerström J, Chen G, Lagunova Z, Furuland H, McEwan P. Cost effectiveness of sodium zirconium cyclosilicate for the treatment of hyperkalaemia in patients with CKD in Norway and Sweden. BMC Nephrol. 2022;23. doi:10.1186/s12882-022-02903-7
121. Ford M, Fishbane S, Spinowitz B, Rastogi A, Guzman N, McCafferty K. Effectiveness of Sodium Zirconium Cyclosilicate in Hemodialysis Patients With Severe Hyperkalemia. Kidney Int Rep. 2021;6. doi:10.1016/j.ekir.2021.09.004
122. Loutradis C, Sarafidis PA, Papadopoulos CE, Papagianni A, Zoccali C. The Ebb and flow of echocardiographic cardiac function parameters in relationship to hemodialysis treatment in patients with ESRD. J Am Soc Nephrol. 2018;29. doi:10.1681/ASN.2017101102
123. Evans M, Palaka E, Furuland H, et al. The value of maintaining normokalaemia and enabling RAASi therapy in chronic kidney disease. BMC Nephrol. 2019;20. doi:10.1186/s12882-019-1228-y
124. Spinowitz B, McCafferty K, Fishbane S, et al. Dose effect analysis of sodium zirconium cyclosilicate in hemodialysis patients. Hemodialysis Int. 2022;26. doi:10.1111/hdi.12983
125. Fonseca C, Brito D, Branco P, Frazão JM, Silva-Cardoso J, Bettencourt P. Hyperkalemia and management of renin-angiotensin-aldosterone system inhibitors in chronic heart failure with reduced ejection fraction: a systematic review. Revista Portuguesa de Cardiologia. 2020;39. doi:10.1016/j.repc.2020.03.015
126. Levien TL. Sodium Zirconium Cyclosilicate.
127. de la Espriella R, Marcos MC, Ronco C, et al. Practical approaches to building up a cardiorenal clinic. Clin Kidney J. 2023;16. doi:10.1093/ckj/sfac258
128. Rafique Z, Liu M, Staggers KA, Minard CG, Peacock WF. Patiromer for Treatment of Hyperkalemia in the Emergency Department: a Pilot Study. Acad Emergency Med. 2020;27. doi:10.1111/acem.13868
129. Naderi ASA, Palmer BF. An unusual case of acute hyperkalemia during pregnancy. Am J Obstet Gynecol. 2007;197. doi:10.1016/j.ajog.2007.06.083
130. Lokelma CHMP, INN-sodium zirconium cyclosilicate.
131. Bridgeman MB, Shah M, Foote E. Potassium-lowering agents for the treatment of nonemergent hyperkalemia: pharmacology, dosing and comparative efficacy. Nephrol Dial Transplant. 2019;34. doi:10.1093/ndt/gfz223
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.