Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 18
Management of Chronic Inflammatory Gingival Enlargement Using Conventional and Electrosurgical Techniques in an Orthodontic Patient: A Case Report
Authors Ramadhani S, Metta P, Reviansyah FH ![]() , Miranda A
, Miranda A ![]()
Received 6 April 2026
Accepted for publication 26 June 2026
Published 10 July 2026 Volume 2026:18 613808
DOI https://doi.org/10.2147/CCIDE.S613808
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Renan Dal Fabbro
Sischa Ramadhani, Prajna Metta, Faris Hernando Reviansyah, Aldilla Miranda
Department of Periodontology, Faculty of Dentistry, Universitas Padjadjaran, Bandung, Indonesia
*These authors contributed equally to this work
Correspondence: Aldilla Miranda, Email [email protected]
Background: Chronic inflammatory gingival enlargement associated with orthodontic appliances may interfere with oral hygiene maintenance and orthodontic treatment. When non-surgical therapy is unsuccessful, gingivectomy may be indicated. Conventional scalpel and electrosurgical techniques are both established treatment modalities for gingival tissue excision, each with distinct clinical characteristics. This case report aims to describe the management of chronic inflammatory gingival enlargement in an orthodontic patient treated with conventional scalpel and electrosurgical gingivectomy.
Case Presentation: A 14-year-old female undergoing orthodontic treatment presented with localized chronic inflammatory gingival enlargement affecting the maxillary teeth, which interfered with proper orthodontic bracket placement and oral hygiene maintenance. Following initial periodontal therapy, gingivectomy was performed using a conventional scalpel technique in the maxillary left region (teeth 23– 24). At a subsequent visit, electrosurgical gingivectomy was performed in the maxillary right region (teeth 14– 15) after discussion of alternative treatment options with the patient and her parent. Both procedures resulted in satisfactory healing and restoration of physiological gingival contours. The electrosurgical approach was associated with improved hemostasis and less patient-reported postoperative discomfort.
Conclusion: Both conventional scalpel and electrosurgical gingivectomy resulted in satisfactory clinical outcomes in the management of orthodontic-associated chronic inflammatory gingival enlargement. In this patient, the electrosurgical approach was associated with improved hemostasis and less postoperative discomfort. However, these findings are limited to a single case and should be interpreted with caution.
Keywords: gingival enlargement, gingivectomy, scalpel, electrosurgery, laser
Introduction
Chronic inflammatory gingival enlargement often results from the accumulation of dental plaque and persistent local irritation. Inadequate oral hygiene is considered the primary etiological factor, while additional local contributing factors, such as anatomical irregularities and irritation from defective restorations or orthodontic appliances, may exacerbate the condition.1–5 This condition may result in the thickening of gingival tissues, causing discomfort, bleeding, and obstructing normal oral hygiene practices.6,7
Initial management of chronic inflammatory gingival enlargement involves the elimination of local etiologic factors through oral hygiene reinforcement and non-surgical periodontal therapy. In cases where non-surgical therapy does not eliminate gingival enlargement, surgical removal of the gingival tissue is indicated. Gingivectomy is a surgical procedure designed to excise excess gingival tissue; it remains one of the most effective treatments for such conditions.6,7 In periodontal practice, gingivectomy is performed through multiple techniques, including the conventional scalpel method, laser surgery, and electrosurgery. Gingivectomy facilitates pocket depth reduction, thereby enhancing access for the thorough elimination of residual plaque and calculus deposits.1–3
Historically, gingivectomy has been performed using a scalpel, offering precise incisions with minimal collateral tissue damage. However, this method is often associated with significant postoperative discomfort and the risk of excessive bleeding.8,9 In response to these limitations, electrosurgery has emerged as an alternative, gaining popularity due to its ability to provide better hemostasis and reduce the risk of bleeding during surgery.8,10 Electrosurgery works by using high-frequency current to cut and coagulate tissue, resulting in a bloodless surgical field. While it offers reduced operative time and less pain during recovery, electrosurgery comes with challenges such as potential thermal damage to surrounding tissues, which can affect healing and lead to complications like delayed wound closure.9
Given the widespread occurrence of gingival enlargement in patients undergoing orthodontic treatment, particularly in those with inadequate plaque control, choosing the optimal gingivectomy technique is critical to ensuring minimal discomfort and maximal therapeutic efficacy. This case report describes the management of chronic inflammatory gingival enlargement in a patient undergoing orthodontic treatment using conventional scalpel and electrosurgical gingivectomy performed at different treatment sites, and discusses the clinical outcomes observed during follow-up.
Case Report
A 14-year-old female patient presented to the Department of Periodontology at Padjadjaran University Dental and Oral Hospital, Bandung, West Java, Indonesia, with the chief complaint of gingiva enlargement in her upper teeth, which interfered with the placement of orthodontic brackets. She had undergone fixed orthodontic treatment nineteen months back. The patient’s height and weight were within normal limits, and her medical, hematological, and family histories did not contribute to any relevant findings. The enlargement was asymptomatic. Upon intraoral examination, a localized gingival enlargement was observed, extending from the upper right first premolar to the second premolar and from the upper left canine to the first premolar. It involved the labial/buccal gingiva. The gingiva appeared pale pink and firm, though certain areas exhibited signs of persistent chronic inflammation (Figure 1). Plaque and calculus deposits were predominantly observed around the enlarged gingival tissues, particularly in areas adjacent to the orthodontic appliances, with bleeding observed upon probing. Pockets ranging from 4 to 5 mm were recorded on the labial/buccal and palatal surfaces of the affected teeth. The orthopantomogram (OPG) showed no evidence of bone loss in the affected teeth on radiographic examination (Figure 2). The diagnosis was established as dental plaque-induced gingivitis associated with a local risk factor (orthodontic appliances) accompanied by localized chronic inflammatory gingival enlargement involving teeth 14, 15, 23, and 24.
 |
Figure 1 Preoperative clinical presentation of chronic inflammatory gingival enlargement associated with orthodontic treatment: (A) Right lateral view, (B) Frontal view, (C) Left lateral view. |
 |
Figure 2 The Orthopantomogram (OPG) images showed an absence of bone loss. |
Case Management
Gingivectomy had been planned for the patient. Surgical intervention was considered following the persistence of gingival enlargement despite initial non-surgical periodontal therapy and reinforcement of oral hygiene measures. The enlargement interfered with orthodontic bracket placement and compromised effective plaque control. Although gingival changes may occur during active orthodontic treatment, the severity and persistence of the condition in this case warranted surgical management to restore the gingival contour, facilitate oral hygiene, and support ongoing orthodontic therapy. The timing of intervention was carefully considered to balance periodontal health and orthodontic treatment progression. Presurgical preparation consisted of scaling and oral hygiene instructions. The patient and her parent were thoroughly informed about the disease condition, available treatment options, the indications, contraindications, potential benefits, and limitations of the proposed surgical procedures. Because the enlarged tissues were located in two separate quadrants, surgical treatment was planned in two stages and performed at different appointments to improve patient comfort and facilitate postoperative monitoring. Written informed consent was obtained from the patient’s parent prior to the procedure.
At the first surgical visit, gingivectomy was performed in the maxillary left region (teeth 23–24) using the conventional scalpel technique. Local infiltration anesthesia was administered to the tissues, and a gingivectomy was performed on teeth 23–24 using a scalpel with a 15c blade. The soft tissue wall was excised down to the base of the pocket (Figure 3). Following the scalpel surgery, the area was thoroughly debrided, and gingivoplasty was performed to reshape the tissue contours. The procedure was completed successfully; however, during the postoperative period, the patient reported mild discomfort and expressed concern regarding residual bleeding associated with the conventional technique.
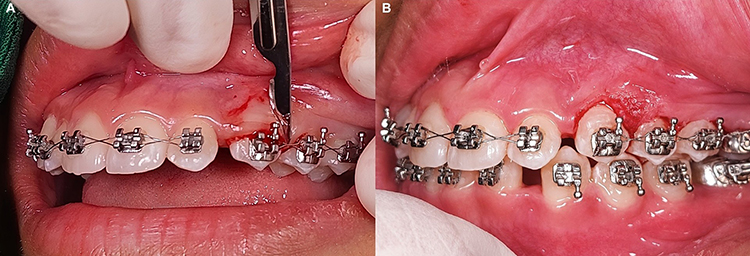 |
Figure 3 Conventional scalpel gingivectomy procedure: (A) Gingival tissue excision using a scalpel, (B) Immediate postoperative view following gingivectomy and gingivoplasty. |
At a subsequent appointment, treatment of the contralateral region (teeth 14–15) was performed using electrosurgery. Following the first surgical procedure, the patient reported mild postoperative discomfort and expressed concern regarding residual bleeding. Therefore, alternative treatment options were discussed with the patient and her parent. Both electrosurgery and laser-assisted gingivectomy were presented as potential alternatives for the second procedure, and the indications, contraindications, benefits, limitations, and costs associated with each approach were explained. Although laser-assisted treatment was considered, the patient and her parent declined this option because of the additional financial cost. Consequently, electrosurgery was selected as an alternative surgical approach for the second procedure. Prior to the procedure, the patient and her parent received an explanation regarding the indications, contraindications, benefits, and limitations of both approaches, and written informed consent was obtained from the patient’s parent for the electrosurgical procedure. An electrosurgery unit (PerFect® TCS II Tissue Contouring System) was used on teeth 14–15 to decrease the gingival bulk. A loop electrode was utilized to remove the excessive gingival tissue and a needle electrode was used for precise cutting (Figure 4). Post-operative instructions were explained to the patient. The interval between each surgical procedure was five weeks.
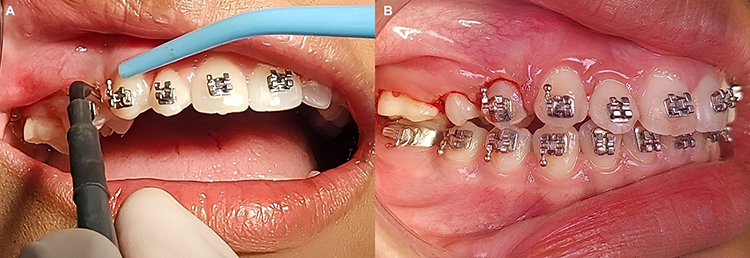 |
Figure 4 Electrosurgical gingivectomy procedure: (A) Gingival tissue excision using an electrosurgical unit, (B) Immediate postoperative view following electrosurgical gingivectomy. |
Clinical Outcomes
At the five-week follow-up, both surgical sites demonstrated satisfactory healing with no evidence of recurrent gingival enlargement. Upon examination, there was no evidence of probing or plaque accumulation. The patient demonstrated an understanding of proper oral hygiene and was practicing it following the surgical procedure (Figure 5).
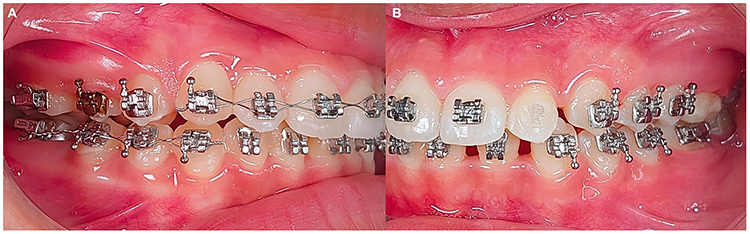 |
Figure 5 Clinical outcomes at the five-week follow-up: (A) Five weeks postoperative view after gingivectomy with electrosurgery; (B) Five weeks postoperative view after gingivectomy with scalpel. |
When asked about her postoperative experience, the patient expressed a preference for the electrosurgical procedure. According to the patient’s report, the electrosurgically treated area was associated with less postoperative discomfort and was perceived to heal more rapidly compared with the area treated using the conventional scalpel technique.
Discussion and Literature Review
Chronic inflammatory gingival enlargement is a common challenge encountered in patients undergoing orthodontic treatment, particularly in the presence of inadequate oral hygiene and persistent plaque accumulation. Orthodontic brackets, bands, and arch wires create plaque-retentive areas that favor biofilm accumulation and hinder effective plaque control. As gingival enlargement progresses, access for routine oral hygiene procedures becomes increasingly limited, resulting in further plaque retention and perpetuating a cycle of chronic inflammation and tissue enlargement. In addition to plaque-induced inflammation, mechanical irritation from orthodontic appliances and local tissue responses to orthodontic forces may further contribute to the development and persistence of gingival enlargement. Beyond its aesthetic implications, persistent gingival enlargement may adversely affect periodontal health by promoting gingival bleeding, pseudopocket formation, and the accumulation of additional plaque and calculus deposits. These conditions may increase the risk of periodontal tissue deterioration if left untreated. Furthermore, excessive gingival tissue can interfere with orthodontic treatment by obstructing proper bracket positioning, limiting access for wire adjustments, and compromising effective tooth movement. Consequently, early recognition and appropriate management of gingival enlargement are essential to restore periodontal health, facilitate adequate oral hygiene, and support the successful progression of orthodontic treatment.4,5
In this case, a 14-year-old female presented with localized gingival enlargement around the upper teeth, particularly affecting the area around the orthodontic brackets. The diagnosis of dental plaque-induced gingivitis associated with a local risk factor (orthodontic appliances) accompanied by localized chronic inflammatory gingival enlargement in the affected teeth (14, 15, 23, and 24) was confirmed after a thorough clinical examination. The plaque and calculus accumulation, along with signs of chronic inflammation, indicated that the gingival enlargement was more likely related to an inflammatory response rather than other systemic condition.7,8 The absence of bone loss on the OPG further supported the diagnosis, suggesting that the enlargement was limited to the soft tissues without involvement of the underlying bones.10
The management of chronic inflammatory gingival enlargement in orthodontic patients typically involves a combination of conservative and surgical approaches. In the present case, initial periodontal therapy, including scaling and oral hygiene instruction, was performed before surgical intervention. However, the gingival enlargement persisted and interfered with the proper placement and function of the orthodontic brackets. The excessive gingival tissue partially covered the clinical crowns and limited access for bracket positioning, potentially compromising the effectiveness of orthodontic tooth movement and hindering adequate plaque control. Because the enlargement remained after non-surgical therapy and affected the progression of orthodontic treatment, gingivectomy was indicated to remove the excess gingival tissue, re-establish physiological gingival contours, facilitate oral hygiene maintenance, and allow optimal function of the orthodontic appliance.4,5 Two different surgical techniques were used to treat the affected areas: conventional scalpel gingivectomy for teeth 23–24 and electrosurgery for teeth 14–15. Both methods are well-established for soft tissue management in periodontics, but each offers distinct advantages and limitations.
The decision to use two different gingivectomy techniques in this case was based on the patient’s clinical experience and preferences during treatment rather than for experimental comparison purposes. At the initial visit, conventional scalpel gingivectomy was performed in the maxillary left region (teeth 23–24) because it is a well-established technique that allows precise tissue excision and predictable healing outcomes. The procedure was completed successfully and resulted in satisfactory healing. However, the patient reported mild postoperative discomfort and expressed concern regarding residual bleeding during the immediate postoperative period. When treatment of the contralateral region (teeth 14–15) was scheduled at a subsequent visit, alternative treatment options were discussed with the patient and her parent. Both electrosurgery and laser-assisted gingivectomy were presented as potential alternatives to the conventional scalpel technique. However, laser-assisted treatment was not selected because of the additional financial cost associated with the procedure. Electrosurgery was subsequently chosen because of its ability to simultaneously incise and coagulate soft tissues, thereby improving hemostasis and reducing intraoperative bleeding. In addition, electrosurgery may shorten operative time and provide a clearer surgical field.8,9
At the five-week follow-up, both areas treated with scalpel and electrosurgery showed satisfactory healing with no recurrence of gingival enlargement. The patient demonstrated improved oral hygiene practices, which is crucial for the long-term success of the treatments. Interestingly, the patient expressed a preference for the electrosurgery procedure, citing less pain and quicker healing compared to the scalpel procedure.10 These observations are consistent with previous reports suggesting that electrosurgery may enhance patient comfort and intraoperative efficiency, although careful handling is required to avoid thermal damage to surrounding tissues.7,8 Nevertheless, because this report is limited by its nature as a single case, and therefore the findings cannot be generalized.
The selection of the gingivectomy technique should be guided by specific clinical indications, contraindications, advantages, and limitations. Conventional scalpel gingivectomy remains one of the most widely used surgical approaches for the management of gingival enlargement because it allows precise tissue excision, excellent tactile feedback, and predictable postoperative healing. The technique is particularly indicated for the management of inflammatory or fibrotic gingival enlargement, crown-lengthening procedures, gingival recontouring, and situations in which precise tissue removal with minimal collateral tissue injury is required. In addition, scalpel surgery may be preferred when treatment is performed in close proximity to bone because it does not produce thermal damage to adjacent tissues. Its advantages include ease of use, cost-effectiveness, well-defined incision margins, and relatively rapid healing. However, the procedure is commonly associated with increased intraoperative bleeding, which may reduce visibility of the surgical field and occasionally prolong treatment. Postoperative discomfort, the need for periodontal dressing, and the requirement for effective bleeding control may also be encountered. Although there are no absolute contraindications to conventional scalpel gingivectomy, the technique may be less suitable in situations where optimal hemostasis is critical, such as in patients with bleeding tendencies or in procedures where surgical visibility is significantly compromised by hemorrhage. Therefore, while conventional gingivectomy remains a reliable and economical treatment option, careful patient selection and appropriate intraoperative management are important considerations.3,5,8,11
Electrosurgical gingivectomy has been proposed as an alternative to conventional scalpel surgery because it enables simultaneous tissue incision and coagulation through the application of high-frequency electrical current. The technique is particularly indicated for the management of gingival enlargement and other soft-tissue procedures in which effective hemostasis, improved surgical visibility, and efficient tissue removal are desirable. Its advantages include superior bleeding control, a relatively bloodless surgical field, reduced operative time, and improved access in areas where visualization may otherwise be compromised. However, electrosurgery also has important limitations. Excessive heat generation may cause lateral thermal damage to adjacent tissues, potentially resulting in delayed healing, tissue necrosis, or impairment of the underlying structures. Therefore, electrosurgery is relatively contraindicated in areas where direct contact with bone is unavoidable and should be used cautiously around metallic restorations, orthodontic appliances, and implant components because heat conduction may increase the risk of tissue injury. In addition, careful control of power settings, electrode selection, and application time is required to minimize unwanted thermal effects. Consequently, appropriate case selection and operator experience are essential to maximize the benefits of electrosurgical treatment while reducing the risk of complications.9–11
According to the literature, electrosurgery has specific guidelines that ensure its effectiveness while minimizing complications. The following key points should be considered during electrosurgical procedures:9,12
1) Electrode Selection and Application:
- Active Electrode: The smallest electrode possible should be used to minimize lateral heat damage and ensure precision. Needle-like electrodes are preferred for cutting, while larger electrodes are used for coagulation. A minimum incision speed of 7 mm/s should be maintained during electrosurgery. An 8-second cooling period should be allowed between each incision with a needle electrode at the same surgical site. For excisional procedures using loop electrodes, the cooling period should be extended to 15 seconds.
- Movement: To minimize lateral heat damage, incisions should be made at a minimum speed of 7 mm/s.
2) Frequency and Waveform:
- Waveform Selection: To minimize thermal damage, intraoral incisions should be made using a fully rectified, filtered waveform at an elevated frequency.
- Power Output: Lower power settings are recommended to minimize tissue damage, with higher power settings reserved for coagulation.
3) Handling Thermal Effects:
- Lateral Heat: Prolonged contact with tissue should be avoided as it may cause necrosis of adjacent tissues. Cooling breaks of 8 seconds are essential between successive incisions with needle electrodes, and up to 15 seconds for loop electrodes. A cooling period helps to dissipate heat effectively.
- Bone Contact: Active electrodes should not contact bone, as this can cause necrosis and delay healing.
- Metallic Restorations: In metallic restorations, the active electrosurgery electrode should only make contact for less than 0.4 seconds, as extended contact may lead to pulpal necrosis.
4) Postoperative Care:
- Post-surgical Instructions: Following surgery, patients should avoid smoking, consuming spicy foods, and using tobacco products immediately after surgery. Analgesics should be prescribed to manage discomfort, and cold packs can help reduce swelling.
5) Other Considerations:
- Electrosurgery should be considered only after all other clinical options have been exhausted, as it generates fulgurating sparks to control hemorrhage. Following fulguration, a delayed healing response is typically observed.
- Electrosurgery can be used for the excision of inflammatory papillary hyperplasia in a safe and convenient manner.
In addition to conventional scalpel and electrosurgical techniques, other treatment modalities such as laser-assisted gingivectomy have also been widely reported.8,13 Laser systems, including diode and CO2 lasers, are indicated for soft-tissue excision, gingival recontouring, and the management of inflammatory gingival enlargement, particularly when enhanced hemostasis and patient comfort are desired.14 The advantages of laser surgery include excellent bleeding control, reduced postoperative pain and edema, minimal tissue trauma, improved patient comfort, and a reduced need for suturing. Furthermore, the bactericidal effects of laser energy may contribute to improved wound healing in selected cases. However, laser-assisted procedures also have limitations, including higher equipment and maintenance costs, the need for specialized training, and the potential risk of thermal injury when inappropriate settings or techniques are used. In addition, limited availability may restrict its routine use in some clinical settings. Although laser-assisted gingivectomy was discussed as a treatment option with the patient and her parent in the present case, it was not selected because of the additional financial cost associated with the procedure. Therefore, the choice of gingivectomy technique should be based on clinical indications, operator experience, patient preferences, and available resources.1,8,14
Conclusion
Within the limitations of a single case report, both conventional scalpel and electrosurgical gingivectomy resulted in satisfactory clinical outcomes in the management of chronic inflammatory gingival enlargement associated with orthodontic treatment. The use of either technique successfully restored physiological gingival contours, facilitated oral hygiene maintenance, and supported the continuation of orthodontic therapy. In this patient, the electrosurgical approach was perceived to provide improved hemostasis and greater postoperative comfort, while the conventional scalpel technique allowed precise tissue contouring. However, these observations are limited to a single clinical case and should not be generalized. Further prospective studies with larger sample sizes are required to evaluate the clinical outcomes, patient-reported experiences, and potential indications of each treatment modality.
Abbreviation
OPG, orthopantomogram.
Consent for Publication
The authors certify that they have obtained written informed consent from the patient’s parent before starting the treatment. In the consent form, the patient and her parent were informed about the disease condition, the proposed treatment procedures, and the available treatment options. The patient’s parent also provided written consent for the publication of the case report and accompanying clinical photographs included in this report. The patient and her parent understood that due efforts will be made to conceal her identity and that her name will not be published. Institutional approval was not required to publish the case details.
Acknowledgments
The authors appreciate the Department of Periodontology and the Department of Orthodontics, Faculty of Dentistry, Universitas Padjadjaran for their support in this case report.
Funding
This work was supported by the Indonesia Endowment Fund for Education (LPDP), Ministry of Finance of the Republic of Indonesia (Scholarship No. 202308110805552).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bhasker A, Goel V, Jain D, Mehta V. Comparison of scalpel and diode laser in management of gingival enlargement: a case report. Int Healthc Res J. 2021;4(12):CR1–8. doi:10.26440/ihrj/0412.03398
2. Bathla S. Textbook of Periodontics.
3. Newman MG, Takei HH, Klokkevold PR, Carranza FA. Newman and Carranza Clinical Periodontology.
4. Dhande S. Gingivectomy as a treatment option for gingival enlargement induced by orthodontic treatment: a case report. J Dental Reports. 2022;2(1):1–9. doi:10.37191/mapsci-jdr-3(1)-018
5. Dalal AM, Oza RR, Shirbhate U, Gurav T. Conventional gingivectomy procedure in the management of orthodontic-induced gingival overgrowth: a case report. Cureus. 2024;16(7). doi:10.7759/cureus.64556
6. Keerthana R, Varghese SS, Chaudhary M. Gingivectomy by different techniques - A comparative analysis. Int J Dent Oral Sci. 2019;6(Special Issue 8):11–16. doi:10.19070/2377-8075-SI02-08003
7. Sandhu A, Jyoti D, Malhotra R, Phull T, Sidhu HS, Nayak S. Management of chronic inflammatory gingival enlargement: a short review and case report. Cureus. 2023. doi:10.7759/cureus.46770
8. Funde S, Dixit Baburaj M, Pimpale SK. Comparison between laser, electrocautery and scalpel in the treatment of drug-induced gingival overgrowth: a case report. IJSS Case Reports Rev. 2015. doi:10.17354/cr/2015/43
9. Raaja Sreepathy CS, Rathinasamy K, Ulaganathan A. Electrosurgery in periodontics: an advent of invention - a literature review. Galore Int J Health Sci Res. 2023;8(2):9–15. doi:10.52403/gijhsr.20230203
10. Xu D, Wang P, Liu H, Gu M. Efficacy of three surgical methods for gingivectomy of permanent anterior teeth with delayed tooth eruption in children. Head Face Med. 2022;18(1):23. doi:10.1186/s13005-022-00328-z
11. Manivannan N, Ahathya RS, Rajaram PC. Scalpel versus electrosurgery: comparison of gingival perfusion status using ultrasound doppler flowmetry. J Pharm Bioallied Sci. 2013;5(SUPPL. 2):154. doi:10.4103/0975-7406.114317
12. Baigrie D, Qafiti FN, Buicko Lopez JL. Electrosurgery. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2026. Available from: http://www.ncbi.nlm.nih.gov/books/NBK482380/.
13. Hamadah O, Almahayni S, Ghazzawi R, Mounajjed R, Altayeb W, Khalil M. Effectiveness of laser-assisted gingivectomy compared to surgical methods: a systematic review. Explor Med. 2025;6:1001325. doi:10.37349/emed.2025.1001325
14. Sachelarie L, Cristea R, Burlui E, Hurjui LL. Laser technology in dentistry: from clinical applications to future innovations. Dent J. 2024;12(12):420. doi:10.3390/dj12120420
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.