Back to Journals » Open Access Emergency Medicine » Volume 12
Management of Alcohol Withdrawal in the Emergency Department: Current Perspectives
Authors Wolf C, Curry A, Nacht J, Simpson SA ![]()
Received 19 October 2019
Accepted for publication 18 February 2020
Published 19 March 2020 Volume 2020:12 Pages 53—65
DOI https://doi.org/10.2147/OAEM.S235288
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Chelsea Wolf,1,2 Ashley Curry,1,2 Jacob Nacht,1,3 Scott A Simpson1,2
1Denver Health Medical Center, Denver, CO, USA; 2Department of Psychiatry, University of Colorado Anschutz Medical Campus, Aurora, CO, USA; 3Department of Emergency Medicine, University of Colorado Anschutz Medical Campus, Aurora, CO, USA
Correspondence: Chelsea Wolf
Department of Psychiatry, 777 Bannock Street MC 0490, Denver, CO 80204, USA
Tel +1 303 602 6890
Fax +1 303 602 6930
Email [email protected]
Abstract: Alcohol withdrawal syndrome (AWS) is a common, heterogenous, and life-threatening complication of alcohol use disorder (AUD). AUD is a leading cause of worldwide mortality, and many patients with AUD will develop AWS during their ED course. This review summarizes the epidemiology, pathology, and management of AWS and AUD in the emergency setting. The time course of AWS and its impact on ED treatment is emphasized. Once AWS is diagnosed, symptom-triggered benzodiazepine administration remains the most commonly provided treatment but may not be appropriate for patients with significant medical or psychiatric comorbidity or pending discharge. In these cases, ED clinicians may consider short courses of barbiturates or alternative regimens based on novel anticonvulsants. Specific treatment protocols are enumerated for clinical practice. Finally, emergency providers must not only manage acute patients’ AWS but also lay the foundation for successful treatment of AUD. An approach to the disposition of the patient with AUD is presented. The authors examine shortcomings in the extant literature and suggest opportunities for further study.
Keywords: alcohol withdrawal syndrome, benzodiazepine, phenobarbital, delirium tremens, gabapentin, alcohol use disorder
Introduction
Alcohol withdrawal syndrome (AWS) is an acute and life-threatening complication of alcohol use disorder (AUD) that is common among emergency department (ED) patients.1 Nearly one-third of patients presenting primarily for alcohol use disorder will experience moderate to severe withdrawal during the course of their ED stay.2 Alcohol withdrawal in the ED is associated with increased use of critical care resources and inpatient hospitalization.3 In cases of withdrawal that progress to delirium tremens (DTs), mortality is 1–4%.4
Alcohol is the most heavily used substance in the United States (USA) and widely consumed worldwide. Only a minority of users experience complicated use of alcohol. In the USA, an estimated 179 million people over the age of 12 report consuming alcohol in the past year.5 Of these persons, 67 million binge-drink (≥5 drinks at one time for males or 4 for females), and almost 17 million exhibit a pattern of heavy drinking (≥5 binge episodes in a 30-day period).5 Alcohol use disorder (AUD) is a pattern of use that has led to functional impairment or distress and manifests as decreased control over use, social impairment, risky use patterns and physiologic tolerance and withdrawal.6 Lifetime prevalence for AUD in the USA is approximately 29%, with 5.4% of individuals over the age of 12 meeting criteria for AUD in a given year.7,8 Rates are highest among men, white and native American individuals, single, and low-income adults. Only 20% of those with an alcohol use disorder engage in some sort of treatment in their lifetime.7 Per capita alcohol consumption is higher among European countries, Australia, and New Zealand, and the lowest among countries with large Islamic populations whose faith encourages abstention.9 Every year, excessive alcohol use is responsible for 88,000 deaths in the USA and more than 2.5 million deaths globally, due to both acute and chronic complications.10
The emergency department (ED) is a common first point of contact for individuals with complications of alcohol use. Alcohol-related visits to EDs in the USA increased 61% from 2006 to 2014, and increases were seen for both acute and chronic alcohol-related problems, despite relatively stable alcohol consumption over the same time period.1 This increase in alcohol-related visits has outpaced the rate of increase in overall ED visits.11
Emergency providers should be familiar with emergent as well as pharmacologic and behavioral interventions to address withdrawal and facilitate alcohol cessation upon discharge. This review summarizes literature regarding the identification and management of alcohol withdrawal in the ED as well as techniques for facilitating transitions of care for individuals experiencing alcohol withdrawal.
Methods
The literature on alcohol use disorder is broad and voluminous. Thus, a narrative review approach was applied to critically synthesize the literature for active clinical practice in emergency settings.12,13 An interdisciplinary authorship group of hospital-based emergency and psychiatric physicians with experience treating substance use disorders agreed on core clinical topics important to the emergent treatment of alcohol withdrawal. Topics included initial identification, stabilization, and determination of level of care. Based on these topics, English-language literature was searched using PubMed and Google Scholar with pertinent keywords including combinations and variations of “alcohol withdrawal,” “alcohol use disorder,” and “emergency department.” There were no date limits on searches. Reference lists of included articles were an additional resource for identifying literature. Papers were prioritized if they were peer-reviewed, published more recently, specific to emergency practice, and/or demonstrated a higher level of evidence.14
Alcohol Withdrawal Syndrome
Diagnostic Criteria
The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) defines alcohol withdrawal as 2 or more distinguishing symptoms which develop within several hours to days following a significant decrease in alcohol consumption after a prolonged period of heavy drinking.6 These symptoms include nausea or vomiting, autonomic hyperactivity, insomnia, increased anxiety and agitation, tremor, perceptual disturbances and seizures. Importantly, alcohol withdrawal is due to a relative decrease in serum alcohol level as opposed to a complete absence of alcohol. As such, an individual may experience significant symptoms of withdrawal while serum blood alcohol levels remain elevated.15,16
Pathophysiology
Alterations in neurotransmission lead to many of the symptoms associated with alcohol withdrawal. Acute alcohol ingestion causes increased gamma-Aminobutyric (GABA)-ergic transmission and decreased glutamatergic activity, including the inhibition of N-methyl-D-aspartate (NMDA) receptors. Chronic alcohol use leads to the down-regulation of GABAA receptors and the upregulation of NMDA receptors.17 During alcohol withdrawal, an acute reduction in alcohol use leads to decreased neurotransmission in GABAA pathways and increased neurotransmission in NMDA pathways. The resulting neuronal hyperexcitability lowers the threshold for seizures.17–19 Similarly, upregulation of noradrenergic and dopaminergic pathways induces the autonomic hyperactivity and hallucinations associated with alcohol withdrawal.17,19
Stages of AWS
The majority of individuals with alcohol use disorder who are at risk for AWS—those with prolonged and heavy drinking—experience only minor, uncomplicated withdrawal symptoms.20–22 These symptoms include increased anxiety, headache, nausea, vomiting, insomnia, and mild tremors. Uncomplicated alcohol withdrawal can also include mild to moderate autonomic hyperactivity of tachycardia, hypertension, and hyperthermia. These uncomplicated symptoms begin as early as 6 hrs after an acute reduction in alcohol use, typically last 24–48 hrs, and disappear entirely within a week of abstinence. A small subgroup of these individuals experiences a more complicated syndrome that includes hallucinations, seizures, delirium and/or more severe autonomic hyperactivity.4,16,17 The signs, symptoms, and timing of AWS are summarized in Figure 1.
 |
Figure 1 Stages of alcohol withdrawal syndrome. |
Alcohol withdrawal hallucinations affect 2–8% of individuals with chronic, heavy alcohol use, particularly those who began drinking at age 17 or earlier.23 Hallucinations begin 8–12 hrs after the last drink and include auditory, visual, tactile, gustatory and olfactory hallucinations.20,23 In this stage of AWS, individuals may experience paranoia and other delusions as well, though importantly they maintain a clear sensorium, thus differentiating it from DTs. Alcohol withdrawal hallucinations should be only judiciously treated with antipsychotics as these medications can mask the symptoms of progressing withdrawal and delay definitive treatment.15
Alcohol withdrawal seizures most commonly occur 12–24 hrs after the individual’s last drink, though the risk for seizures can last for up to 48 hrs following abstinence.24 Seizures occur in 5–10% of individuals with active AWS and are typically generalized tonic-clonic.21,25 Approximately two-thirds of individuals who have an initial, untreated, alcohol withdrawal seizure, will go on to have multiple seizures typically occurring in close succession to one another.24 Three percent will develop status epilepticus.22
Alcohol withdrawal delirium, commonly called delirium tremens (DTs), occurs in approximately 3–5% of patients hospitalized with AWS.26,27 DTs are characterized by confusion and an alteration in consciousness, often accompanied by severe autonomic changes and hallucinations. DTs typically begin after 1–3 days of abstinence, though can begin abruptly as early as 8 hrs after an acute reduction in alcohol use, particularly in those who have experienced complicated withdrawal previously.16,21 Mortality rates in cases of DTs without intervention the rate can be as high as 20%–with death most commonly resultant from infection, cardiac arrhythmias, or respiratory collapse.16,19
Once the presence of alcohol withdrawal has been established, symptom scales allow regular and objective documentation of the progression of withdrawal. The Revised Clinical Institute Withdrawal Assessment for Alcohol scale (CIWA-Ar) is one of the most commonly used tools. It is a 10-item scale that tracks the degree of nausea and vomiting, headache, tremor, diaphoresis, anxiety, agitation, disorientation, and auditory, visual and tactile disturbances.28
However, the CIWA-Ar has limitations: it can be cumbersome to administer in a busy emergency department (5 mins every 1–2 hrs for 5–7 measurements), patients’ cognitive and communicative abilities must be intact for questions to be answered appropriately, and co-morbid psychiatric symptoms may confound and inappropriately increase scores. Further, the CIWA-Ar was initially validated in a population of voluntary patients at detoxification centers, and has not been validated for use in the ED or with acutely ill or injured hospitalized patients.29–32 The Richmond Agitation-Sedation Scale and the Riker Agitation-Sedation Scale are alternatives to the CIWA-Ar that can be helpful to ensure an appropriate level of sedation during the management of acute alcohol withdrawal.26 Yet another alternative to the CIWA-Ar includes the use of fixed-dosing protocols, discussed in detail below.
Given the morbidity and mortality associated with AWS, anticipating the risk of withdrawal may aid in speeding treatment or even preventing incipient withdrawal. The Prediction of Alcohol Withdrawal Severity Scale (PAWSS) identifies medically ill individuals who are at risk of developing severe alcohol withdrawal symptoms.21 PAWSS has been found to be the most accurate of predictive tools in inpatient medical settings.20 The PAWSS factors in the Blood Alcohol Level (BAL) and the presence of autonomic hyperactivity, as well as the presence or absence of several other factors detailed in Figure 2;21 anecdotally, some services have found a higher, more specific cutoff necessary for guiding treatment.
 |
Figure 2 Prediction of Alcohol Withdrawal Severity Scale Notes: Reproduced with permissin from Oxford University Press. Maldonado Jet al. Prospective Validation of the Prediction of Alcohol Withdrawal Severity Scale (PAWSS) in medically ill inpatients: a new scale for the prediction of complicated alcohol withdrawal syndrome. Alcohol Alcoholism. 2015;50(5):509–518.21Abbreviations: BAL, blood alcohol level; PAWSS, Prediction of Alcohol Withdrawal Severity Scale; AA, Alcoholics Anonymous; AWS, alcohol withdrawal syndrome. |
Management of Acute Alcohol Withdrawal
Stabilization
The immediate management of any patient presenting with altered mental status begins with a rapid primary assessment of airway, breathing, circulation, and disability. Recognition of concomitant trauma at this point significantly changes the approach to management. Instability at any element of this evaluation requires prompt intervention including airway adjuncts such as oral and nasopharyngeal airways, intubation, oxygen, and fluid resuscitation. Measurement of blood glucose and appropriate administration of dextrose as well as the use of naloxone can be life-saving and produce immediate changes in mentation thus revealing the etiology of the presentation.15 Fluid resuscitation in patients with alcohol use disorder requires close monitoring of serum sodium to avoid beer potomania, a syndrome whereby the rapid provision of intravenous solute prompts sudden diuresis and hyponatremia.33 Thiamine (vitamin B1) should be administered empirically for prevention of Wernicke’s encephalopathy (WE) and Korsakoff’s psychosis. Protocols to guide thiamine dosing and route of administration differ among institutions and medical society guidelines, with doses varying from 100 mg of thiamine in a typical intravenous fluid infusion up to 200–500 mg every 8 hrs for a minimum of 72 hrs if WE is suspected.34–36
Patients who are actively seizing should be immediately treated with benzodiazepines until cessation of seizure activity is achieved. Typical starting doses are 5–10 mg intravenous (IV) of diazepam and of 2–4 mg of lorazepam, which can be repeated in 5–10 mins. Midazolam can be given intramuscularly (IM) at a dose of 2–4 mg if IV access has not been secured.4,37 The specific agent often varies by institution. Most importantly, the selected agent should be the most readily available. Patients who are found to be in status epilepticus require escalating pharmaceutical intervention that may include concomitant airway management. Most treatment algorithms progress from benzodiazepines to phenytoin or fosphenytoin and then on to phenobarbital, valproic acid, propofol and pentobarbital. Once the patient is stabilized and immediate life threats are identified, the provider can move to further characterize the nature of the presentation.
Some patients present with a chief complaint and symptoms that direct providers immediately to the etiology of alcohol withdrawal. In other cases, the symptoms of withdrawal can be attributed to a number of other conditions.4 Providers must maintain a high index of suspicion for withdrawal while in parallel, evaluating for, and treating other causes of symptoms such as trauma, intoxication, toxicological ingestion, infection, and primary cardiac or pulmonary pathologies. Furthermore, a number of patients present to the emergency department for complaints not at all related to alcohol withdrawal and yet proceed to develop symptoms of acute alcohol withdrawal during their stay.
As with all visits, effective patient-centered communication during the history and physical exam is crucial to identifying and allowing the patient to discuss alcohol-related problems. Once identified, early and aggressive pharmacologic treatment of withdrawal is paramount and life-saving.37
Benzodiazepines
Benzodiazepines have long been the mainstay of treatment for alcohol withdrawal. Benzodiazepines are agonists at the GABAA receptors and, as such, are cross-tolerant with alcohol. They act to increase the frequency of the GABA-receptor opening and enhance the inhibitory action of GABA.4,24,38 Benzodiazepines decrease symptom severity, the risk of delirium, and the length and frequency of seizures associated with AWS.39 A 2010 Cochrane review found benzodiazepines to be superior to placebo for the treatment of alcohol withdrawal seizures and trend towards superior when compared to other agents used to treat AWS.40
Several benzodiazepines are available to treat AWS, each with variable administration formulations, onset of action, and half-lives. Table 1 summarizes the key characteristics of common benzodiazepines used in the management of AWS. A systematic review of 64 studies found no statistical difference among various benzodiazepines notwithstanding some trend favoring chlordiazepoxide for symptom control.40
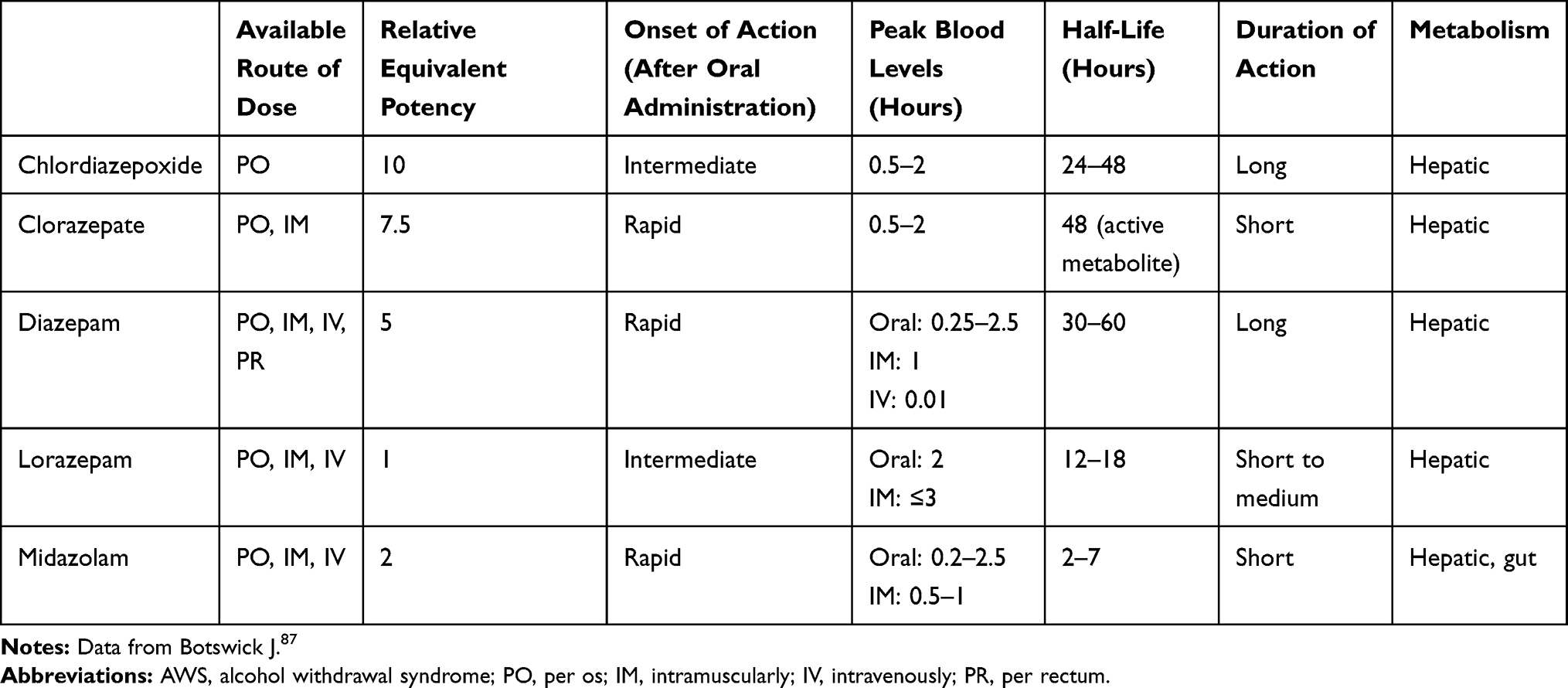 |
Table 1 Characteristics of Benzodiazepines Used for AWS |
The goals of initial treatment with benzodiazepines are the control of alcohol withdrawal symptoms, improvement in autonomic hyperactivity (temperature, heart rate, and blood pressure within near-normal limits), and seizure prevention. The appropriate level of sedation is for the patient to be drowsy yet arousable. Frequently, a protocol begins with either oral (PO) or intravenous (IV) loading of the benzodiazepine, depending on the severity of symptoms and the patient’s ability to tolerate oral intake. Following the initial loading dose, subsequent doses of the benzodiazepines can be based on either a symptom-triggered or a fixed-schedule protocol. Symptom-triggered protocols are typically based on the patients’ vital signs, level of agitation, or on CIWA-Ar scores reassessed every 1–2 hrs. In fixed-schedule protocols, a gradually tapered dose of a benzodiazepine is administered over a period of several days. Table 2 demonstrates several sample benzodiazepine protocols.
 |
Table 2 Sample Alcohol Withdrawal Protocols |
While both types of protocols are widely used, several studies have demonstrated the superiority of a symptom-triggered strategy for management of AWS. However, only a few studies have been performed in an ED environment.29,41,42 A randomized controlled trial of 117 patients beginning an alcohol treatment program found that the mean amount of benzodiazepine administered to patients in the symptom-triggered group was significantly less than the mean amount administered to the fixed-schedule group (37mg of oxazepam versus 231mg, respectively).41 Similarly, the total duration of treatment was significantly less for the symptom-triggered group compared to the fixed-schedule group (20 hrs versus 63 hrs, respectively).41 In a retrospective study of 100 patients with AWS who were treated in an ED clinical decision unit, the total dose of benzodiazepines administered was nearly 50% lower with a symptom-triggered protocol compared to a fixed-schedule protocol (median 80mg diazepam equivalent versus 170mg, respectively). Again, the length of stay for the symptom-triggered group was 50% lower when compared to the fixed-schedule group (2 days versus 3 days, respectively).29
A recent systematic review and meta-analysis involving 6 studies and more than 650 patients also found moderate-strength evidence supporting symptom-triggered dosing in regard to total dose of benzodiazepines used and total length of treatment. The authors, however, cautioned that these findings may not be applicable in a hospital setting as several of the studies were conducted in outpatient alcohol treatment facilities. They additionally established that there is inadequate evidence to determine the superiority of symptom-triggered dosing over a fixed-schedule protocol in regards to alcohol withdrawal seizures, delirium and death.43
Symptom-triggered protocols can be complicated by co-morbid psychiatric or medical illness given that there may be significant overlap between symptoms of alcohol withdrawal and a primary psychotic or mood disorder (anxiety, agitation, hallucinations). Similarly, several of the symptoms of AWS may be seen independently in medically ill patients (nausea, vomiting, headache, diaphoresis) and in those with delirium due to a separate etiology (clouded sensorium, perceptual disturbances). Furthermore, some patients may exaggerate the subjective symptoms of alcohol withdrawal in order to receive more benzodiazepines. Clinicians should use caution when using symptom-triggered protocols among patients with these co-morbidities. Fixed dosing regimens or even benzodiazepine-sparing protocols should be considered instead.
Despite remaining the gold standard for the treatment of AWS, benzodiazepine use is not without risk. Adverse effects of benzodiazepines have been well documented and include risk of mortality in overdose particularly when combined with alcohol or opioids, abuse and addiction potential, psychomotor slowing and increased risk of falls, as well as cognitive impairment.44,45 Additionally, when administered by continuous infusion, benzodiazepines can accumulate in the central nervous system and adipose tissue, prolonging the length of drug action and adverse effects. Hepatic disease, highly prevalent in individuals with AUD, further impacts the elimination half-life of benzodiazepines, compounding the duration of effects.46,47
Barbiturates
Because chronic, heavy alcohol use can cause some patients to develop a cross-tolerance to benzodiazepines, treatment of AWS with only benzodiazepines may prove inadequate for some individuals. Barbiturates, either alone or in combination with benzodiazepines, offer an alternative for treatment of AWS. Like benzodiazepines, barbiturates also work at the GABAA receptor. However, barbiturates have a unique binding site by which they increase the duration of the chloride channel openings, and, at higher doses, can open the chloride channels even in the absence of GABA.37,48 Additionally, barbiturates inhibit the release of glutamate through action on voltage-activated calcium channels.49
One of the most commonly used barbiturates for the treatment of AWS is phenobarbital, which has a rapid onset of action 5–30 mins and a long half-life of 50–140 hrs.37 Because phenobarbital remains pharmacodynamically active for several days after administration, this medication may be an ideal candidate for the treatment of AWS in the ED setting. The medication’s self-tapering properties may obviate the need to discharge the patient with additional oral medication that may be misused or diverted.48,50
Many studies suggest phenobarbital to be an effective and safe agent for AWS.48,50–53 A prospective, randomized, double-blind study compared the use of IV phenobarbital to IV lorazepam plus oral chlordiazepoxide in 44 patients who presented to the ED with mild-moderate AWS. The study found no difference in effectiveness, length of ED stays, hospital admissions, or symptoms at 48 hrs after discharge from ED.50 A retrospective review of 562 admitted inpatients found no statistical significance in regards to effectiveness or complications between benzodiazepine-only and phenobarbital-only protocols for management of AWS.48 Another retrospective study examined three alcohol withdrawal protocols used in an ED: diazepam only, lorazepam plus phenobarbital, or phenobarbital only.51 This investigation found no difference in ICU admission rates across the three protocols, though the study did find an increase in overall hospital admission rates in the phenobarbital-only group compared to the diazepam-only group.
Other studies have assessed the concomitant administration of phenobarbital plus a benzodiazepine. A prospective, randomized, placebo-controlled study compared outcomes of 102 patients treated in the ED with a symptom-triggered protocol of lorazepam-only and patients who were treated with the symptom-triggered, lorazepam-based protocol and additionally were front-loaded with a single dose of intravenous phenobarbital (10mg/kg).52 The study found that those patients who received the single dose of phenobarbital had a decreased admission rate to the ICU and no increased rate of adverse events.52 A replication retrospective cohort study examined benzodiazepine-only versus phenobarbital-adjunct protocols for treatment of AWS.53 The replication study found no statistical between-group differences in ICU admissions, admissions to the hospital, discharges from the ED, and complications, though the phenobarbital-adjunct group did have a statistically shorter hospital stay. However, it should be noted that the mean dose of phenobarbital used in this latter study was 260mg versus the 10mg/kg dose of phenobarbital used in the original study.
Similarly, a retrospective chart review comparing lorazepam-only treatment to lorazepam plus a single, unstandardized dose of phenobarbital on hospital day one, found a statistical difference in the length of hospital stay.54 The lorazepam plus phenobarbital group had significantly more patients discharged from the hospital within three days. There was no statistical difference between groups on other parameters, including daily benzodiazepine requirements, total length of stay, number of patients discharged from the emergency department or admitted to the hospital, and number of adverse events.
Finally, a systematic review of clinical trials examining the use of phenobarbital in the treatment of AWS concluded that the combination of phenobarbital with benzodiazepines seemed to have additive effects in the management of AWS symptoms and tended to be more effective for patients with severe AWS compared to mild or moderate AWS. The authors also summarized that barbiturates seemed to be well tolerated and did not lead to an increase in adverse events.55
Other Pharmacological Approaches
Gabapentin
Gabapentin has anxiolytic, sedative and anticonvulsive properties, all of which are useful in the management of AWS.56 It boasts a good safety profile and a lower abuse potential compared to benzodiazepines. The medication was developed to mimic the neurotransmitter GABA but does not in fact directly interact with GABA neuroreceptors. Instead, gabapentin inhibits voltage-dependent calcium channels and indirectly modulate the neurotransmission of GABA.22,56,57
Although studies supporting gabapentin’s use were all outside the ED setting, extant evidence suggests that gabapentin may be useful to ED clinicians given the risk inherent when sending a patient home with an unmonitored prescription for a benzodiazepine taper. Multiple studies and reviews have examined the efficacy and safety of gabapentin for alcohol withdrawal.22,56–58 A retrospective cohort study of 100 patients who presented to an ED found that those who received high-dose gabapentin (1800 mg/day) during the first two days of hospital admission required a significantly lower total dose of benzodiazepines.56 The gabapentin cohort also had both a significantly lower mean and maximum CIWA-Ar score on the third day of hospitalization. In general, gabapentin appears particularly beneficial for mild AWS rather than more severe presentations.58 Sample protocols utilizing gabapentin are presented in Table 3.
In addition to being relatively safe and well tolerated, another distinct benefit of gabapentin is its utility in the longer-term treatment of alcohol use disorder (AUD). Gabapentin can be beneficial in treating the cravings associated with AUD and can promote sobriety from alcohol. In a randomized controlled study of 150 patients, high-dose gabapentin (1800 mg/day) was found to be significantly more effective than low-dose gabapentin (900mg/day) or placebo.59 The rate of abstinence in the high-dose group compared to the low-dose and the placebo groups was 17%, 11% and 4%, respectively. Similarly, the rate of no-heavy drinking was significantly higher in the high-dose gabapentin group compared to the low-dose group or to placebo (45%, 30%, and 22%, respectively). This same study also showed significant improvements in sleep, mood, and alcohol cravings for those receiving high-dose gabapentin.59
Further research will be important to clarify conflicting results regarding the effectiveness of gabapentin in the treatment of both AWS and AUD. A meta-analysis of 7 randomized-control studies assessing the use of gabapentin for treating alcohol use disorder found that while gabapentin appeared to more efficacious than placebo in the treatment of alcohol use disorder, the only specific outcome in which gabapentin was clearly favored over placebo was a decrease of percentage of heavy drinking days.60
Other Anti-Epileptic Drugs
Multiple studies have investigated the use of other anti-epileptic drugs (AEDs), including divalproex,61 carbamazepine,62 and phenytoin63 in the treatment of AWS. A Cochrane review examining 56 studies found no statistically significant differences between AEDs and placebo in regards to effectiveness in the treatment of alcohol withdrawal seizures, DTs, alcohol cravings and other symptoms of AWS measured by the CIWA-Ar scale.64 When comparing AEDs to other drugs, the results of the meta-analysis favored carbamazepine over benzodiazepines in the management of AWS symptoms measured by CIWA-Ar. The incidence of alcohol withdrawal seizures also tended to be lower in patients treated with an AED compared to other drugs.
Adjunctive Medications
There is a subset of patients who experience benzodiazepine-resistant alcohol withdrawal (RAW). Although the precise pathophysiology of RAW remains unclear, proposed mechanisms include a significant down-regulation of GABAA receptors and a decrease in the sensitivity of these receptors to benzodiazepines.65,66 Furthermore, in addition to having no effect on the NMDA pathway, the clinical effects of benzodiazepines are dependent on circulating GABA. Given that reduced plasma concentrations of GABA have been noted in individuals with AUD, this may provide an additional explanation for RAW in some patients.67
While the incidence of RAW is unknown, it has been suggested that the defining criteria for RAW are the requirement of >40 mg of diazepam (or benzodiazepine equivalent) within one hour.66,68 Given the need for high benzodiazepine doses, various adjunctive medications with alternative mechanisms of action, including NMDA-antagonism, GABAB agonism, ß-blockade and ⍺-agonism, have been investigated to aid in the management of severe AWS symptoms. These are discussed briefly below, though studies regarding their use in the ED are limited.
Propofol, which inhibits the effects of glutamate at NMDA receptors as well as acts as a GABAA agonist, has been shown in several small studies and case reports to be efficacious as an adjuvant in some patients experiencing RAW.69–72 Other studies, however, have demonstrated that propofol is associated with longer hospital stays, and the significant risks of hypotension and respiratory depression associated with this medication necessitate mechanical ventilation and close monitoring in the ICU.71,73,74
Ketamine is another NMDA-antagonist with less potential for respiratory depression. Two small retrospective studies found that the use of ketamine as an adjunct reduced benzodiazepine requirements in patients with RAW.75,76 Another retrospective study found that the adjunctive use of ketamine resulted in a decreased length of ICU stay and a decreased need for mechanical ventilation.77 Further prospective studies will be important to further evaluate the efficacy and safety of this medication, particularly in an ED setting.
ß-blockers and ⍺-agonists, such as clonidine, may be helpful in some patients as adjuvants for the control of autonomic symptoms of AWS. Importantly, they do not treat or prevent DTs or alcohol withdrawal seizures and can mask the severity of AWS. As such, these should be used with caution and only as an adjunctive agent to a benzodiazepine or other GABA-agonist.66,78
Similarly, dexmedetomidine, an ⍺-2-agonist that is more highly selective for the ⍺-2 receptor than clonidine, has been studied for use in the treatment of AWS. Several studies have shown it to be beneficial as an adjuvant medication, specifically reducing the short-term benzodiazepine requirement and providing sedation without causing respiratory depression.78–80 Dexmedetomidine can, however, lead to bradycardia and hypotension. Additionally, given its lack of action at GABA receptors, it does not target the underlying mechanism of alcohol withdrawal and as such, does not treat DTs, alcohol withdrawal seizures, or prevent the progression of AWS.79
Finally, several small studies have examined the use of baclofen, a pure GABAB agonist.81,82 However, a recent Cochrane review found that there is insufficient evidence to make a judgement regarding the efficacy and safety of baclofen for AWS; further research will be important to support its use.83
Behavioral Interventions
Behavioral interventions focused on increasing motivation to seek treatment among individuals with alcohol-related visits to the ED have yielded mixed results. Screening Brief Intervention, Referral and Treatment (SBIRT) encompasses a variety of screening tools and motivational techniques to engage individuals with alcohol use disorders to explore treatment and cessation options.30 Motivational interviewing and cognitive behavioral strategies form the basis of the patient interaction. SBIRT is used most frequently in emergency settings with patients who present with acute intoxication and alcohol-related injuries and has not been studied specifically in individuals with alcohol withdrawal. Meta-analyses of these interventions in the ED show a small reduction in drinking in low to moderate alcohol users with many individual studies failing to show significant reduction in alcohol consumption. Interventions with follow-up contact were not superior to single interactions. There is limited evidence to support a small reduction in subsequent instances of alcohol-related injuries.84,85 More research is needed to establish effective interventions for individuals presenting to the ED with complications of alcohol use.
Disposition
Once the patient is stabilized and management of the alcohol withdrawal symptoms is underway in the ED, the clinician must establish the next appropriate level of care for further alcohol detoxification for the patient. The American Society of Addiction Medicine (ASAM) provides criteria for disposition based on medical needs, psychiatric needs, readiness for change, and risk of relapse.86 The clinician should assess these biopsychosocial domains in determining the level of care that the patient requires for safe detoxification and effective treatment initiation. Options for detoxification include an extended stay in the ED, discharge home, discharge to an outpatient treatment facility, or admission to a medical floor, inpatient psychiatric unit or ICU. Table 3 describes these criteria and suggests appropriate levels of care.
 |
Table 3 Level of Care for Alcohol Detoxification After Emergent Treatment |
Conclusion and Future Directions
Nearly half of adults with AUD will experience AWS, and many of these individuals will be seen in an ED. AWS carries significant morbidity and mortality on its own, and the syndrome may complicate co-morbid treatment of medical illness or trauma. While benzodiazepines have long been the mainstay of AWS treatment, novel approaches have garnered increasing evidence and acceptance. In their role as gatekeepers to systems of care, ED clinicians should also be familiar with levels of care and behavioral interventions available to patients with AUD.
There remain many opportunities for further research and clinical development. Tools for assessing the risk for severe alcohol withdrawal and for monitoring the severity of symptoms need to be validated for use in the ED and consider the high prevalence of co-morbid medical and psychiatric illness; symptom scales should also be less time-consuming to administer, perhaps by considering the availability of electronic medical record data. The limits of symptom scales complicate the use of symptom-triggers and benzodiazepine-sparing protocols in the ED. Moreover, additional data are required around outcomes of acute treatment in the ED—for example, treatment retention outcomes at 7 or 30 days as are commonly cited among studies of ED-based buprenorphine induction. Use of these outcomes could allow greater insight into the utility of the increasing range of medications available not only for acute withdrawal but also for helping patients achieve sobriety.
For patients with problematic alcohol use, an emergency department visit can be a life-saving encounter. Emergency medicine clinicians must recognize their vital role not only in treating life-threatening withdrawal but also setting the patient on a path towards recovery.
Disclosure
SA Simpson sits on the advisory board for Impel Neuropharma and has received royalties from Taylor and Francis. The authors report no other conflicts of interest in this work.
References
1. White AM, Slater ME, Ng G, Hingson R, Breslow R. Trends in alcohol-related emergency Department visits in the United States: results from the Nationwide Emergency Department Sample, 2006 to 2014. Alcohol Clin Exp Res. 2018;42(2):352–359. doi:10.1111/acer.2018.42.issue-2
2. Qian S, Irani M, Brighton R, et al. Investigating the management of alcohol‐related presentations in an Australian teaching hospital. Drug Alcohol Rev. 2019. doi:10.1111/dar.12906
3. Klein LR, Cole JB, Driver BE, Battista C, Jelinek R, Martel ML. Unsuspected critical illness among emergency Department patients presenting for acute alcohol intoxication. Ann Emerg Med. 2018;71(3):279–288. doi:10.1016/j.annemergmed.2017.07.021
4. Long D, Long B, Koyfman A. The emergency medicine management of severe alcohol withdrawal. Am J Emerg Med. 2017;35:1005–1011. doi:10.1016/j.ajem.2017.02.002
5. Substance Abuse and Mental Health Services Administration. 2018 National Survey on Drug Use and Health (NSDUH). Tables 2.28A, 2.30A, 2.31A. Available from: https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/NSDUHDetailedTabs2018R2/NSDUHDetTabs2-28to2-31pe2018.pdf. Accessed September 16, 2019.
6. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
7. Grant BF, Goldstein RB, Saha TD, et al. Epidemiology of DSM-5 alcohol use disorder. JAMA Psychiatry. 2015;72(8):757. doi:10.1001/jamapsychiatry.2015.0584
8. Substance Abuse and Mental Health Services Administration. 2018 National Survey on Drug Use and Health (NSDUH). Table 5.2B - Substance use disorder in past year among persons aged 12 or older, by detailed age category: percentages, 2017 and 2018; 2019. Available from: https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/NSDUHDetailedTabs2018R2/NSDUHDetTabs5-2pe2018.pdf.
9. World Health Organization. Global status report on alcohol and health. World Health Organization; 2011.
10. Centers for Disease Control and Prevention. Alcohol Related Disease Impact (ARDI) application; 2013. Available from: www.cdc.gov/ARDI.
11. Mullins PM, Mazer-Amirshahi M, Pines JM. Alcohol-Related Visits to US Emergency Departments, 2001–2011. 2016.
12. Snyder H. Literature review as a research methodology: an overview and guidelines. J Bus Res. 2019;104:333–339. doi:10.1016/j.jbusres.2019.07.039
13. Wong G, Greenhalgh T, Westhorp G, Buckingham J, Pawson R. RAMESES publication standards: meta-narrative reviews. BMC Med. 2013;11. doi:10.1186/1741-7015-1111-1120
14. Burns P, Rohrich R, Chung K. The levels of evidence and their role in evidence-based medicine. Plast Reconstr Surg. 2011;128(1):305–310. doi:10.1097/PRS.0b013e318219c171
15. Simpson S, Wilson M, Nordstrom K. Psychiatric emergencies for clinicians: emergency department management of alcohol withdrawal. J Emerg Med. 2016;51(3):269–273. doi:10.1016/j.jemermed.2016.03.027
16. Cohen B. Theory and Practice of Psychiatry. New York, NY: Oxford University Press; 2003.
17. Mirijello A, D’Angelo C, Ferrulli A, et al. Identification and management of alcohol withdrawal syndrome. Drugs. 2015;75(4):353–365. doi:10.1007/s40265-015-0358-1
18. Kosten T, O’Connor P. Management of drug and alcohol withdrawal. N Engl J Med. 2003;348:1786–1795. doi:10.1056/NEJMra020617
19. Hall W, Zador D. The alcohol withdrawal syndrome. Lancet. 1997;349:1897–1900. doi:10.1016/S0140-6736(97)04572-8
20. Wood E, Albarouni L, Tkachuk S, et al. Will this hospitalized patient develop severe alcohol withdrawal syndrome? JAMA. 2018;320(8):825–833. doi:10.1001/jama.2018.10574
21. Maldonado J, Sher Y, Das S, et al. Prospective Validation of the Prediction of Alcohol Withdrawal Severity Scale (PAWSS) in medically ill inpatients: a new scale for the prediction of complicated alcohol withdrawal syndrome. Alcohol Alcoholism. 2015;50(5):509–518. doi:10.1093/alcalc/agv043
22. Maldonado J. Novel algorithms for the prophylaxis and management of alcohol withdrawal syndromes – beyond benzodiazepines. Crit Care Clin. 2017;33(3):559–599. doi:10.1016/j.ccc.2017.03.012
23. Stephane M, Arnaout B, Yoon G. Alcohol withdrawal hallucinations in the general population, an epidemiological study. Psychiatry Res. 2018;262:129–134. doi:10.1016/j.psychres.2018.02.021
24. Rathlev N, Ulrich A, Delanty N, D’Onofrio G. Alcohol-related seizures. J Emerg Med. 2006;31(2):157–165. doi:10.1016/j.jemermed.2005.09.012
25. Eyer F, Schuster T, Felgenhauer N, et al. Risk assessment of moderate to severe alcohol withdrawal—predictors for seizures and delirium tremens in the course of withdrawal. Alcohol Alcoholism. 2011;46(4):427–433. doi:10.1093/alcalc/agr053
26. Schmidt K, Doshi M, Holzhausen J, Natavio A, Cadiz M, Winegardner J. Treatment of severe alcohol withdrawal. Ann Pharmacother. 2016;50(5):389–401. doi:10.1177/1060028016629161
27. Schuckit M. Recognition and management of withdrawal delirium (delirium tremens). N Engl J Med. 2014;371(22):2109–2113. doi:10.1056/NEJMra1407298
28. Sullivan J, Sykora K, Schneiderman J, Naranjo C, Sellers E. Assessment of alcohol withdrawal: the revised clinical institute withdrawal assessment for alcohol scale (CIWA-Ar). Br J Addict. 1989;84(11):1353–1357. doi:10.1111/add.1989.84.issue-11
29. Cassidy E, O’Sullivan I, Bradshaw P, Islam T, Onovo C. Symptom-triggered benzodiazepine therapy for alcohol withdrawal syndrome in the emergency department: a comparison with the standard fixed dose benzodiazepine regimen. Emerg Med J. 2012;29:802–804. doi:10.1136/emermed-2011-200509
30. Gray S, Borgundvaag B, Sirvastava A, Randall I, Kahan M. Feasibility and reliability of the SHOT: A short scale for measuring pretreatment severity of alcohol withdrawal in the emergency department. Acad Emerg Med. 2010;17(10):1048–1054. doi:10.1111/acem.2010.17.issue-10
31. Higgins J, Bugajski A, Church D, et al. A psychometric analysis of CIWA-Ar in acutely ill and injured hospitalized patients. J Trauma Nurs. 2019;26(1):41–49. doi:10.1097/JTN.0000000000000414
32. Eloma A, Tucciarone J, Hayes E, Bronson B. Evaluation of the appropriate use of a CIWA-Ar alcohol withdrawal protocol in the general hospital setting. Am J Drug Alcohol Abuse. 2018;44(4):418–425. doi:10.1080/00952990.2017.1362418
33. Allison MG, McCurdy MT. Alcoholic metabolic emergencies. Emerg Med Clin North Am. 2014;32(2):293–301. doi:10.1016/j.emc.2013.12.002
34. Flannery A, Adkins D, Cook A. Unpeeling the evidence for the banana bag: evidence-based recommendations for the management of alcohol-associated vitamin and electrolyte deficiencies in the ICU. Crit Care Med. 2016;44(8):1545–1552. doi:10.1097/CCM.0000000000001659
35. Sharp C, Wilson M, Nordstrom K. Psychiatric emergencies for clinicians: emergency department management of Wernicke-Korsakoff syndrome. J Emerg Med. 2016;51(4):401–404. doi:10.1016/j.jemermed.2016.05.044
36. Day E, Bentham P, Callaghan R, Kuruvilla T, George S. Thiamine for prevention and treatment of Wernicke‐Korsakoff Syndrome in people who abuse alcohol. Cochrane Database Syst Rev. 2013;7.
37. Stehman C, Mycyk M. A rational approach to the treatment of alcohol withdrawal in the ED. Am J Emerg Med. 2013;31:734–742. doi:10.1016/j.ajem.2012.12.029
38. Stahl S. Stahl’s Essential Psychopharmacology. Vol. 4th. New York: Cambridge University Press; 2013.
39. Mayo-Smith M. Pharmacological management of alcohol withdrawal: a meta-analysis and evidence-based practice guideline. JAMA. 1997;278(2):144–151. doi:10.1001/jama.1997.03550020076042
40. Amato L, Minozzi S, Vecchi S, Davoli M. Benzodiazepines for alcohol withdrawal. Cochrane Database Syst Rev. 2010;3.
41. Daeppen J, Gache P, Landry U, et al. Symptom-triggered vs fixed-schedule doses of benzodiazepine for alcohol withdrawal: a randomized treatment trial. Arch Intern Med. 2002;162(10):1117–1121. doi:10.1001/archinte.162.10.1117
42. Weaver M, Hoffman H, Johnson R, Mauck K. Alcohol withdrawal pharmacotherapy for inpatients with medical comorbidity. J Addict Dis. 2006;25(2):17–24. doi:10.1300/J069v25n02_03
43. Holleck J, Merchant N, Gunderson C. Symptom-triggered therapy for alcohol withdrawal syndrome: a systematic review and meta-analysis of randomized controlled trials. J Gen Intern Med. 2019;34(6):1018–1024. doi:10.1007/s11606-019-04899-7
44. Bachhuber M, Hennessy S, Cunningham C, Starrels J. Increasing benzodiazepine prescriptions and overdose mortality in the United States, 1996–2013. Am J Public Health. 2016;106(4):686–688. doi:10.2105/AJPH.2016.303061
45. Longo L, Johnson B. Addiction: part 1. Benzodiazepines - side effects, abuse risk and alternatives. Am Fam Physician. 2000;61(7):2121–2128.
46. Grover S, Ghosh A. Delirium tremens: assessment and management. J Clin Exp Hepatol. 2018;8(4):460–470. doi:10.1016/j.jceh.2018.04.012
47. Griffin C, Kaye A, Bueno F, Kaye A. Benzodiazepine pharmacology and central nervous system-mediated effects. Ochsner J. 2013;13(2):214–223.
48. Nisavic M, Nejad S, Isenberg B, et al. Use of phenobarbital in alcohol withdrawal management – a retrospective comparison study of phenobarbital and benzodiazepines for acute alcohol withdrawal management in general medical patients. Psychosomatics. 2019;60(5):458–467. doi:10.1016/j.psym.2019.02.002
49. Löscher W. How theories evolved concerning the mechanism of action of barbiturates. MRES. 2012;53(Suppl 8):12–25.
50. Hendey G, Dery R, Barnes R, Snowden B, Mentler P. A prospective, randomized, trial of phenobarbital versus benzodiazepines for acute alcohol withdrawal. Am J Emerg Med. 2011;29(4):382–385. doi:10.1016/j.ajem.2009.10.010
51. Nelson A, Kehoe J, Sankoff J, Mintzer D, Taub J, Kaucher K. Benzodiazepines vs barbiturates for alcohol withdrawal: analysis of 3 different treatment protocols. Am J Emerg Med. 2019;37(4):733–736. doi:10.1016/j.ajem.2019.01.002
52. Rosenson J, Clements C, Simon B, et al. Phenobarbital for acute alcohol withdrawal: a prospective randomized double-blind placebo-controlled study. J Emerg Med. 2013;44(3):592–598. doi:10.1016/j.jemermed.2012.07.056
53. Sullivan S, Dewey B, Jarrell D, Vadiei N, Patanwala A. Comparison of phenobarbital-adjunct versus benzodiazepine-only approach for alcohol withdrawal syndrome in the ED. Am J Emerg Med. 2019;37:1313–1316. doi:10.1016/j.ajem.2018.10.007
54. Ibarra F. Single dose phenobarbital in addition to symptom-triggered lorazepam in alcohol withdrawal. Am J Emerg Med. 2019. doi:10.1016/j.ajem.2019.01.053
55. Mo Y, Thomas M, Karras G. Barbiturates for the treatment of alcohol withdrawal syndrome: a systematic review of clinical trials. J Crit Care. 2016;32:101–107. doi:10.1016/j.jcrc.2015.11.022
56. Levine A, Carrasquillo L, Mueller J, Nounou M, Naut E, Ibrahim D. High-dose gabapentin for the treatment of severe alcohol withdrawal syndrome: a retrospective cohort analysis. Pharmacotherapy. 2019;39(9):881–888. doi:10.1002/phar.v39.9
57. Leung J, Hall-Flavin D, Nelson S, Schmidt K, Schak K. Role of gabapentin in the management of alcohol withdrawal and dependence. Ann Pharmacother. 2015;49(8):897–906. doi:10.1177/1060028015585849
58. Leung J, Rakocevic D, Allen N, et al. Use of a gabapentin protocol for the management of alcohol withdrawal: a preliminary experience expanding form the consult-liaison psychiatry service. Psychosomatics. 2018;59(5):496–505. doi:10.1016/j.psym.2018.03.002
59. Mason B, Quello S, Goodell V, Shadan F, Kyle M, Begovic A. Gabapentin treatment for alcohol dependence: a randomized clinical trial. JAMA Intern Med. 2014;174(1):70–77. doi:10.1001/jamainternmed.2013.11950
60. Kranzler H, Feinn R, Morris P, Hartwell E. A meta-analysis of the efficacy of gabapentin for treating alcohol use disorder. Addiction. 2019;114(9):1547–1555. doi:10.1111/add.v114.9
61. Reoux J, Saxon A, Malte C, Baer J, Sloan K. Divalproex sodium in alcohol withdrawal: a randomized double-blind placebo-controlled clinical trial. Alcohol Clin Exp Res. 2001;25(9):1324–1329.
62. Barrons R, Roberts N. The role of carbamazepine and oxcarbazepine in alcohol withdrawal syndrome. J Clin Pharm Ther. 2010;35(2):153–167. doi:10.1111/j.1365-2710.2009.01098.x
63. Chance J. Emergency department treatment of alcohol withdrawal seizures with phenytoin. Ann Emerg Med. 1991;20(5):520–522. doi:10.1016/S0196-0644(05)81606-3
64. Minozzi S, Amato L, Vecchi S, Davoli M. Anticonvulsants for alcohol withdrawal. Cochrane Database Syst Rev. 2010;3.
65. Benedict N, Wong A, Cassidy E, et al. Predictors of resistant alcohol withdrawal (RAW): a retrospective case-control study. Drug Alcohol Depend. 2018;192:303–308. doi:10.1016/j.drugalcdep.2018.08.017
66. Sarff M, Gold J. Alcohol withdrawal syndromes in the intensive care unit. Crit Care Med. 2010;38(9 Suppl):S494–S501. doi:10.1097/CCM.0b013e3181ec5412
67. Ratsma JE, Stelt OVD, Gunning W. Neurochemical markers of alcoholism vulnerability in humans. Alcohol Alcoholism. 2002;37(6):522–533. doi:10.1093/alcalc/37.6.522
68. Hack J, Hoffmann R, Nelson L. Resistant alcohol withdrawal: does unexpectedly large sedative requirement identify these patients early? J Med Toxicol. 2006;2(2):55–60. doi:10.1007/BF03161171
69. Sohraby R, Attridge R, Hughes D. Use of propofol-containing versus benzodiazepine regimens for alcohol withdrawal requiring mechanical ventilation. Ann Pharmacother. 2014;48(4):456–461. doi:10.1177/1060028013515846
70. Lorentzen K, Lauritsen A, Bendtsen A. Use of propofol infusion in alcohol withdrawal-induced refractory delirium tremens. Dan Med J. 2014;61(5):1–5.
71. Brotherton A, Hamilton E, Kloss H, Hammond D. Propofol for treatment of refractory alcohol withdrawal syndrome: a review of the literature. Pharmacotherapy. 2016;36(4):433–442. doi:10.1002/phar.2016.36.issue-4
72. Coomes T, Smith S. Successful use of propofol in refractory delirium tremens. Ann Emerg Med. 1997;30(6):825–828. doi:10.1016/S0196-0644(97)70059-3
73. Wong A, Benedict N, Lohr B, Pizon A, Kane-Gill S. Management of benzodiazepine-resistant alcohol withdrawal across a healthcare system: benzodiazepine dose-escalation with or without propofol. Drug Alcohol Depend. 2015;154:296–299. doi:10.1016/j.drugalcdep.2015.07.005
74. Dixit D, Endicott J, Burry L, et al. Management of acute alcohol withdrawal syndrome in critically ill patients. Pharmacotherapy. 2016;36(7):797–822. doi:10.1002/phar.1770
75. Shah P, McDowell M, Ebisu R, Hanif T, Toerne T. Adjunctive use of ketamine for benzodiazepine-resistant severe alcohol withdrawal: a retrospective evaluation. J Med Toxicol. 2018;14(3):229–236. doi:10.1007/s13181-018-0662-8
76. Wong A, Benedict N, Armahizer M, Kane-Gill S. Evaluation of adjunctive ketamine to benzodiazepines for management of alcohol withdrawal syndrome. Ann Pharmacother. 2015;49(1):14–19. doi:10.1177/1060028014555859
77. Pizon A, Lynch M, Benedict N, et al. Adjunct ketamine use in the management of severe ethanol withdrawal. Crit Care Med. 2018;46(8):E768–E771. doi:10.1097/CCM.0000000000003204
78. Muzyk A, Fowler J, Norwood D, Chilipko A. Role of α2-agonists in the treatment of acute alcohol withdrawal. Ann Pharmacother. 2011;45(5):649–657. doi:10.1345/aph.1P575
79. Wong A, Smithburger P, Kane-Gill S. Review of adjunctive dexmedetomidine in the management of severe acute alcohol withdrawal syndrome. Am J Drug Alcohol Abuse. 2015;41(5):382–391. doi:10.3109/00952990.2015.1058390
80. Mueller S, Preslaski C, Kiser T, et al. A randomized, double-blind, placebo-controlled dose range study of dexmedetomidine as adjunctive therapy for alcohol withdrawal. Crit Care Med. 2014;42(5):1131–1139. doi:10.1097/CCM.0000000000000141
81. Lyon J, Khan R, Gessert C, Larson P, Renier C. Treating alcohol withdrawal with oral baclofen: a randomized, double-blind, placebo-controlled trial. J Hosp Med. 2011;6(8):469–474. doi:10.1002/jhm.928
82. Cooney G, Heydtmann M, Smith I. Baclofen and the alcohol withdrawal syndrome - a short review. Front Psychiatry. 2019;9:1–5. doi:10.3389/fpsyt.2018.00773
83. Liu J, Wang L. Baclofen for alcohol withdrawal. Cochrane Database Syst Rev. 2017;8.
84. Barata I, Shandro J, Montgomery M, et al. Effectiveness of SBIRT for alcohol use disorders in the emergency department: a systematic review. West J Emerg Med. 2017;18(6):1143–1152. doi:10.5811/westjem.2017.7.34373
85. Schmidt CS, Schulte B, Seo HN, et al. Meta-Analysis on the Effectiveness of Alcohol Screening with Brief Interventions for Patients in Emergency Care Settings. 2015:
86. Mee-Lee D, Shulman G. The ASAM criteria and matching patients to treatment. In: Ries R, Fiellin D, Miller S, Saitz R, editors. The ASAM Principles of addiction Medicine.
87. Botswick J. Medication Table 6: benzodiazepines. In: Chavez B, editor. CPNP Psychiatric Pharmacotherapy Review Course. 2018–2019 ed. Lincoln, NE: College of Psychiatric and Neurologic Pharmacists; 2018.
88. Daeppen JB, Gache P, Landry U, et al. Symptom-triggered vs fixed-schedule doses of benzodiazepine for alcohol withdrawal: a randomized treatment trial. Arch Intern Med. 2002;162(10):1117–1121. doi:10.1001/archinte.162.10.1117
89. Sachdeva A, Chandra M, Deshpande SN. A comparative study of fixed tapering dose regimen versus symptom-triggered regimen of lorazepam for alcohol detoxification. Alcohol Alcohol. 2014;49(3):287–291. doi:10.1093/alcalc/agt181
90. Krishnamjurthy A; American Society of Addiction Medicine. Management of alcohol intoxication and withdrawal. In: Cavacuiti C editor, Principles of Addiction Medicine: The Essentials. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2011:204–211.
91. Malcolm R, Ballenger JC, Sturgis ET, Anton R. Double-blind controlled trial comparing carbamazepine to oxazepam treatment of alcohol withdrawal. Am J Psychiatry. 1989;146(5):617–621.
92. Myrick H, Malcolm R, Randall PK, et al. A double-blind trial of gabapentin versus lorazepam in the treatment of alcohol withdrawal. Alcohol Clin Exp Res. 2009;33(9):1582–1588. doi:10.1111/acer.2009.33.issue-9
93. Lyon JE, Khan RA, Gessert CE, Larson PM, Renier CM. Treating alcohol withdrawal with oral baclofen: a randomized, double-blind, placebo-controlled trial. J Hosp Med. 2011;6(8):469–474. doi:10.1002/jhm.928
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.