Back to Journals » Journal of Blood Medicine » Volume 15
Management of Advanced Systemic Mastocytosis: Clinical Challenges
Authors Tremblay D ![]() , Wagner NE, Mascarenhas J
, Wagner NE, Mascarenhas J
Received 21 June 2024
Accepted for publication 2 September 2024
Published 11 September 2024 Volume 2024:15 Pages 421—433
DOI https://doi.org/10.2147/JBM.S366367
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Douglas Tremblay,1 Nicole E Wagner,2 John Mascarenhas1
1Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York, NY, USA; 2Department of Medicine, Icahn School of Medicine at Mount Sinai, New York, NY, USA
Correspondence: John Mascarenhas, Myeloproliferative Disorders Program, Tisch Cancer Institute, Division of Hematology/Oncology, Icahn School of Medicine at Mount Sinai, One Gustave L Levy Place, Box 1079, New York, NY, 10029, USA, Tel +1 212 241 3417, Fax +12128765276, Email [email protected]
Abstract: Advanced systemic mastocytosis (AdvSM) is a rare hematologic malignancy with organ damage and compromised life expectancy arising from organ accumulation of neoplastic mast cells. Identification of the gain-of-function KITD816V in the majority of cases has accelerated pharmaceutical development culminating with the development of selective KIT inhibitors such as avapritinib. While the advent of these therapies has improved the quality and quantity of life in patients with AdvSM, current challenges remain in the management of this disease. In this review, we summarize the present and future therapeutics landscape of AdvSM, highlighting the development of novel KIT inhibitors including elenestinib and bezuclastinib. We also explore the continued role of additional treatment modalities including allogeneic stem cell transplantation before discussing unresolved clinical challenges in the management of AdvSM.
Keywords: systemic mastocytosis, KITD816V, avapritinib, midostaurin
Introduction
Systemic mastocytosis (SM) encompasses a diverse group of diseases involving neoplastic mast cells (MCs) that span a disease spectrum from indolent SM (ISM), which also includes a smoldering form (SSM), to an advanced form (AdvSM) that compromises life span. AdvSM is comprised of aggressive SM (ASM), SM with associated hematologic neoplasm (SM-AHN) and mast cell leukemia (MCL). The incidence of approximately 1.5 cases per 100,000 and a prevalence of 25 cases per 100,000 population.1
SM originates from clonal MCs derived from hematopoietic stem cells2 that are inappropriately activated and accumulate in extramedullary tissues. These MCs can be associated with significant symptom burden as well as the potential to induce organomegaly with frank organ dysfunction. Both chronic and episodic activation of MCs results in varied symptomatology that is attributed to release of mast cell mediators such as histamine, heparin, leukotrienes, prostaglandins, platelet-activating factor, and proteases.3
The molecular pathogenesis of SM is characterized in the majority of patients by a gain of function oncogenic mutation in the stem cell factor (SCF) transmembrane class III receptor KIT (CD117).4 KIT signaling promotes the proliferation, differentiation and activation of MCs. Over 95% of patients with SM harbor mutations in exon 17 of the KIT gene involving an adenine to thymine base switch at nucleotide position 2468, which results in an aspartic acid-to-valine change at codon 816 (D816V).4,5 KIT mutations, as well as tryptase, can be effectively assayed in the peripheral blood. The functional consequence of this activation loop mutation is constitutive kinase activity leading to downstream signaling through MAPK, AKT, PI3K, and STAT signaling cascades.6,7 It is now recognized that alternative activating mutations of KIT outside of D816V can also lead to MC activation, differentiation and proliferation and may alter the activation of the complex downstream signaling pathways.
While clinical manifestations in patients with ISM or SMM are primarily related to mediator symptoms, patients with AdvSM largely suffer from symptoms that are a result of MC proliferation leading to organomegaly (B-findings) or organ failure (C-findings).8 ASM is defined by the presence of at least one C-findings, which are listed in Table 1, however patients with SM-AHN or MCL frequently also exhibit C-findings. Cytopenias are secondary to MC marrow infiltration in ASM and MCL, however in patients with SM-AHN low blood counts may also be related to associated neoplasm. Other features such as hepatomegaly and splenomegaly are present in approximately 40% of AdvSM patients.9 Measurement of MC burden outside of C-findings occurs through several mechanisms. The most direct is histopathologic evaluation of MC tissue infiltration in the bone marrow (or other organs).10 Tryptase is a serine protease that is concentrated in MCs and is a marker of MC activation.11 The KITD816V mutation is present in the vast majority of AdvSM patients and its allele burden is significantly higher in patients with AdvSM as compared to patients with ISM or SSM.12 The key diagnostic, clinical and prognostic distinctions between SM subtypes are detailed in Table 2.
These markers of MC burden and activation can also be used to assess response to treatment. In the International Working Group-Myeloproliferative Neoplasms Research and Treatment and European Competence Network on Mastocytosis (IWG-MRT-ECNM) response criteria, reduction in serum tryptase level to less than 20 ng/mL is required to fulfill a complete response (Table 3).13 In addition, reduction in KITD816V allele burden of at least 25% has been shown to be predictive of improved overall survival (OS).14 In recent years, there has been significant progress in attaining these responses, and ultimately improving patient outcomes because of the development of selective KITD816V inhibitors. Despite these improvements, several unresolved clinical challenges remain.
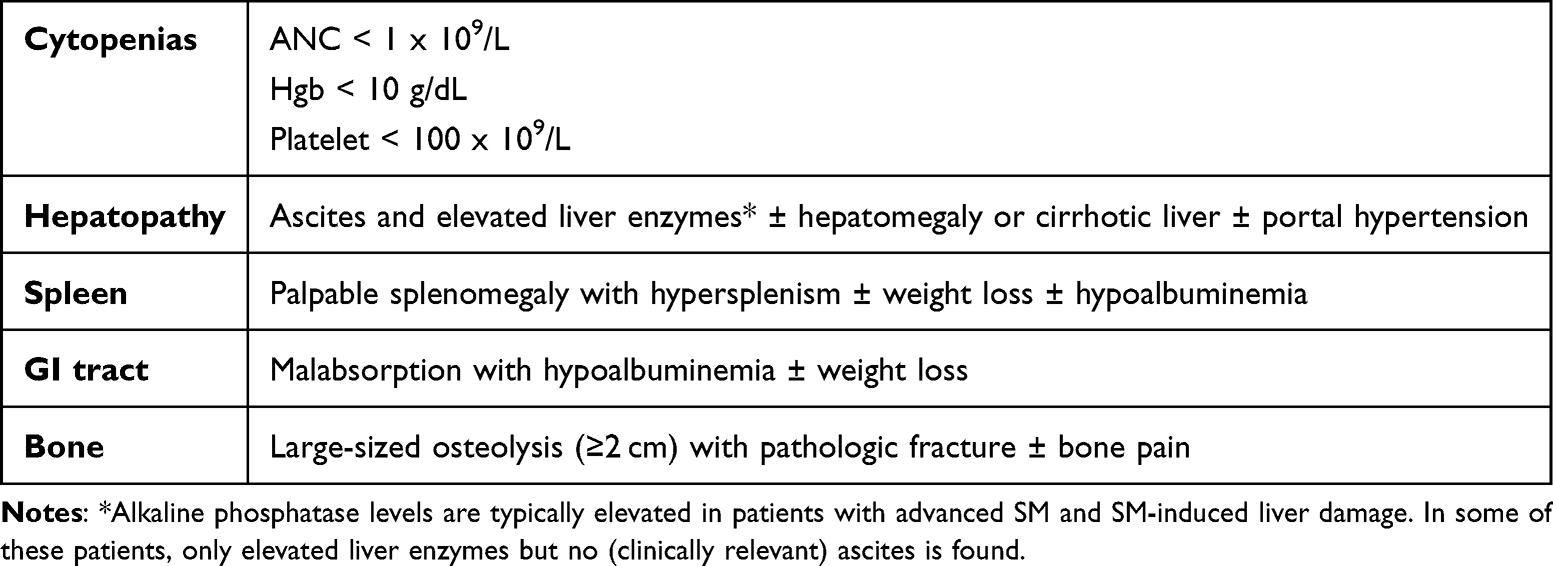 |
Table 1 C Findings for the Diagnosis of Aggressive Systemic Mastocytosis |
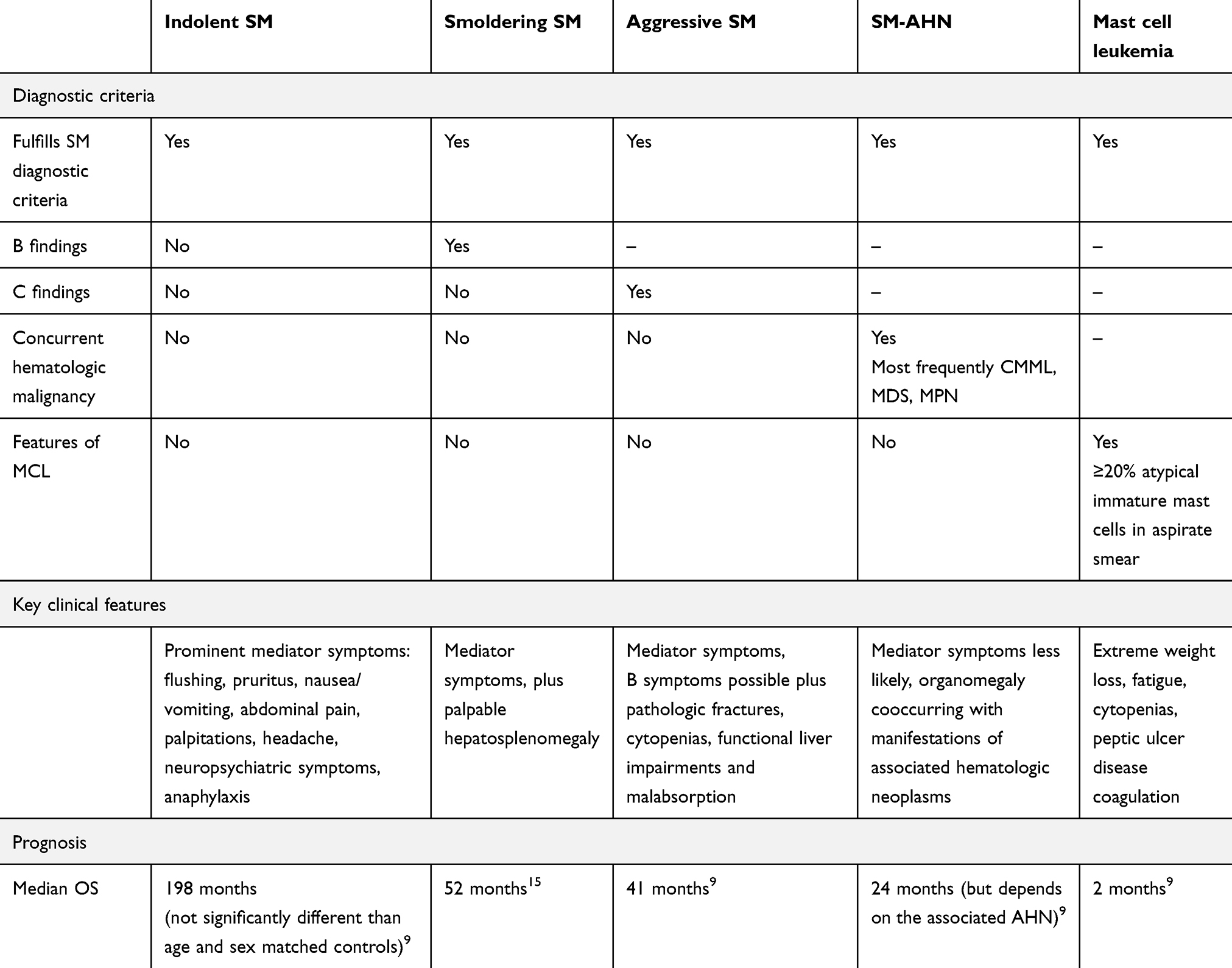 |
Table 2 Subtypes of Systemic Mastocytosis |
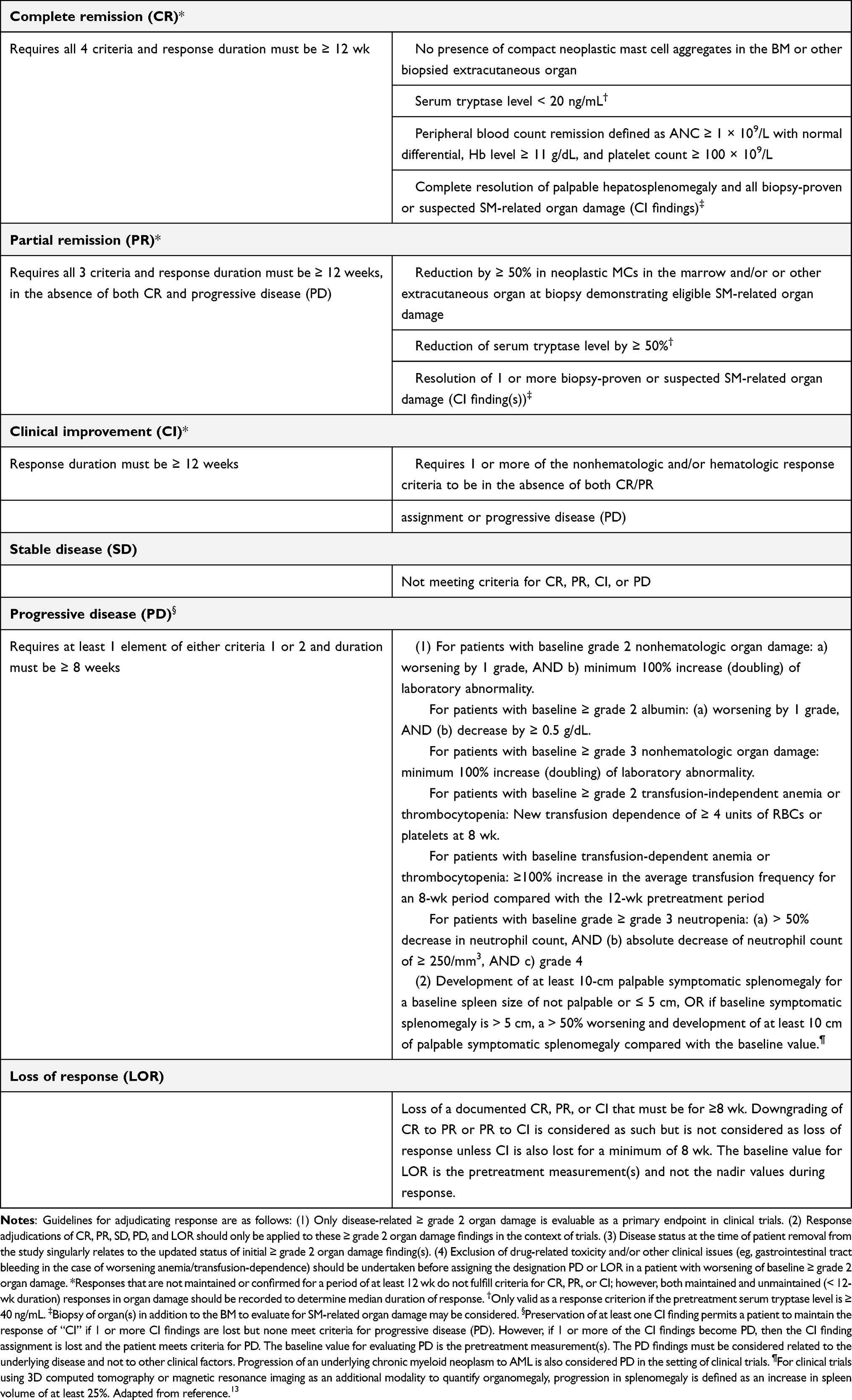 |
Table 3 IWG-MRT-ECNM Response Criteria for Advanced Systemic Mastocytosis |
In this review, we describe the evolving risk stratification of AdvSM before detailing the current treatment landscape including midostaurin and avapritinib. We then describe novel therapeutics in development and then described remaining clinical challenges for the optimal management of AdvSM.
Risk Stratification
In 2022, both the WHO and the International Consensus Classification (ICC) introduced updates for the classification and diagnostic criteria of SM.16,17 The ICC upheld the five subtypes of systemic mastocytosis from 2016, while the WHO 5th edition (2022) classification system categorizes SM into six different classes with one new variant, BMM. The first category is ISM which meets the criteria of SM, requiring at least 1 major and 1 minor or 3 major SM criteria, without additional B or C findings. This is the most common variant of SM and is associated with a favorable prognosis, both in terms of OS and leukemia-free survival. ISM progresses slowly and OS that is likely similar to that of the age- and sex-matched population based off a retrospective study with 342 patients.9 However, a subsequent analysis of OS in the ISM population demonstrated a modest but statistically significant decrease in survival for patients in the first 4 years of their disease course, regardless of whether their disease progressed to advanced SM.18 Patients with indolent or smoldering SM tend to be younger at presentation, present with a higher percentage of skin lesions and GI symptoms and are less likely to exhibit constitutional symptoms or hepatosplenomegaly.
The WHO 5th edition (2022) added an additional variant of SM not included in the 2016 classification system or by the ICC. This additional category, bone marrow mastocytosis (BMM) is defined as neoplastic MC proliferation solely involving the BM. BMM is characterized by limited BM infiltration, absence of cutaneous lesions, normal or minimally elevated serum tryptase levels (<125 ng/mL), older age and male predominance.19 Patients with isolated bone marrow neoplastic mast cell involvement but who also have B findings or a tryptase level ≥125 ng/mL have an inferior PFS and OS as compared to BMM or ISM patients without these two clinical features.20
SSM is also a recognized diagnostic category. This is considered an intermediate-stage variant and is characterized by 2 or more “B findings”. The prognosis is worse compared to ISM but not as aggressive as the AdvSM categories. Patients with SSM tend to present at an older age, have higher bone marrow MC burden, higher serum tryptase level, as well as increased prevalence of palpable hepatosplenomegaly. SSM is associated with inferior OS and an increased risk of progression to ASM compared to the other ISM subtypes.21
Aggressive Mastocytosis (ASM) is characterized by the presence of “C findings”. It requires fulfilling the SM criteria with the presence of ≥1 C finding, which include impairment or loss of organ function due to mast cell infiltrates (Table 1).22 Associated symptoms include constitutional symptoms, hepatosplenomegaly (with impairment of liver function, ascites or portal hypertension), lymphadenopathy, severe anemia (hemoglobin <10g/dL) and/or thrombocytopenia (platelets 100 × 109/L), leukocytosis (ANC < 1.0x109/L due to bone marrow dysfunction). Due to gastrointestinal mast cell infiltrates, patients may have abdominal pain, nausea, vomiting, diarrhea or GI bleeding and may have malabsorption with hypoalbuminemia and weight loss. They may have musculoskeletal pain or osteopenia, due to skeletal involvement, which may manifest with osteoporosis and pathologic fractures.23,24
The next category is SM with associated hematological neoplasm (SM-AHN), which requires meeting criteria for both SM and another hematologic malignancy. SM-AHN has a more aggressive clinical course. The AHN component most often includes chronic myelomonocytic leukemia (CMML), MDS, myeloproliferative neoplasms (MPN), AML, B-cell lymphoma and plasma cell neoplasms.25 SM-AHN is associated with an inferior OS, however the prognosis is generally determined by the aggressiveness of the AHN.26
Mast cell leukemia (MCL) is the rarest subtype, extremely aggressive and categorized by the highest mortality.27 This subtype accounts for less than 1% of all SM cases. MCL is considered a form of acute leukemia and is defined by the presence of at least 20% neoplastic immature MCs in the bone marrow and 10% in the PB. MCL can either be secondary MCL following progression from another SM or can present as primary MCL.28
Associated Mutations
More than 90% of typical ISM and 70% of AdvSM carry acquired point mutation in the KIT gene. Additional somatic mutations (ASXL1, RUNX1, SRSF2, NRAS) have been found in 90% of ASM patients.29 A recent next-generation sequencing study of one hundred and fifty patients revealed 75% of patients possessed KITD816V. Sixty-three (42%) patients were either unmutated or had no additional mutation other than KITD816V. For the remaining 87 patients, a total of 148 non-KIT mutations were identified: 46 (31%) patients harbored one mutation, 24 (16%) two mutations, 14 (9%) three mutations and three (2%) had four mutations. The most frequently mutated non-KIT genes were TET2 (29%), ASXL1 (17%), CBL (11%), SF3B1/DNMT3A/JAK2 (6% each), U2AF1 (4%), and RUNX1 (3%). ASXL1 and RUNX1 mutations are associated with inferior survival, independent of age and WHO subtype.30 The frequency of these mutations is significantly greater in AdvSM as compared to non-AdvSM, 19 of 27 non-KIT mutations were found in patients with advanced SM.23
Prognostic Scoring Systems
There are several prognostic scoring systems to help categorize AdvSM based on clinical and molecular factors. However, these are often challenging to incorporate into clinical practice.
The Mayo Alliance Prognostic System (MAPS) was developed in 2018 and incorporates two different models. The scoring system was developed based on 580 patients seen at Mayo Clinic between 1968 and 2015. The first system includes only 5 clinical variables, which were advanced SM vs ISM/SSM, age >60 years, platelets <150x109/L, anemia below sex-adjusted normal and serum ALP above normal range. Survival was directly correlated with the number of risk factors, with a great prognosis for patient with ≤1 risk factor (median survival not reached) and poor outcomes for patients 4 or 5 risk factors (median survival, 9–27 months). This study showed that the model was equally effective whether it was applied to patients with AdvSM or ISM/SSM. The second prognostic model incorporates adverse molecular data, such as the presence of ASXL1/RUNX1/NRAS and incorporated the previously defined clinical variables. The OS without adverse mutations was median 70 months compared to 10 months with the identification of an adverse mutation present (ASXL1, RUNX1, NRAS).31 These models included the WHO classification system for SM, which is subject to variable interpretation. A subsequent WHO-independent MAPS system was developed to eliminate this subjectivity, which focused solely on age, platelet count, sex-adjusted hemoglobin, increased alkaline phosphatase and serum albumin.31
The Mayo clinic group subsequently proposed a Mutation-Augmented Prognostic Scoring System (MAPSS) with next-generation sequencing of 27 relevant genes in 150 SM patients that could be integrated into a prognostic model. In multivariate analysis, age >60 years, hemoglobin <10 g/dL or transfusion-dependence, platelet count <150x109/L, serum albumin <3.5 g/dL, and ASXL1 mutation were associated with inferior survival. This study stratified ASM into three distinct risk groups: low-risk, intermediate-risk and high risk with associated median survivals of 86, 21, and 5 months, respectively.30
In 2019, the International Prognostic Scoring System of Mastocytosis (IPSM) was created based on a study by Sperr at all.32 This study utilized a database of 1639 patients with SM and divided patients into three groups based on age >60 years and elevated alkaline phosphatase value: low (no risk factors), intermediate 1 (one risk factor) and intermediate 2 (two risk factors). In patients with AdvSM (n=259), age 60 years or older concentration of tryptase 125 ng/mL or higher leukocyte count of 16 x 109/L or higher, hemoglobin of ≤11 g/dL, platelet count of ≤100 x 109 /L, and skin involvement were independent prognostic factors for OS in multivariate analyses. Each risk factor with an HR greater than 1.50 scored 1 point and risk factors with an HR of 0.50 or lower scored −1 point. By adding the risk factors, four different risk groups were established. Based on these variables, a separate score was established with four risk categories for AdvSM. OS and PFS differed significantly among these groups (p < 0.0001).33
The Global Prognostic Score for Mastocytosis (GPSM) further identified variables that impacted disease progression (GPSM-PFS) and survival (GPSM-OS) and were based on platelet count ≤100 × 109 cells per L, serum β2-microglobulin ≥2.5 μg/mL, and serum baseline tryptase ≥125 μg/L for PFS and hemoglobin ≤11 g/dL, serum alkaline phosphatase ≥140 IU/L, and at least one mutation in SRSF2, ASXL1, RUNX1, or DNMT3 for OS. The GPSM-PFS and GPSM-OS models were able to discriminate between low-risk and high-risk patients for worse PFS and OS in the discovery and validation cohorts, with a discovery cohort of 422 and an independent cohort of 853 patients, respectively. This prognostic tool was able to predict survival outcomes in patients with SM.34
The Mutation-Adjusted Risk Score (MARS) was developed from a study analyzing 383 patients with ASM from the German Registry on Disorders of Eosinophils and Mast cells. Multivariable analysis identified risk factors associated with OS: age >60 years, hemoglobin <10 g/dL, thrombocytopenia (<100 x 109/L) presence of one high molecular risk gene mutation (SRSF2, ASXL1 and/or RUNX1) and presence of two or more high molecular risk gene mutations. This MARS was independent of WHO classification type and was confirmed with an independent validation cohort.35
One registry-based study reviewed 2607 patients enrolled within the European Competence Network on Mastocytosis (ECNM) and 575 patients enrolled within the German Registry on Eosinophils and Mast cells (GRM). This study found that many patients with AdvSM are misdiagnosed or experience delayed diagnosis especially if patients lack skin involvement or MC mediator-related symptoms during presentation. This study identified the following serum parameters as the most relevant: tryptase, alkaline phosphatase, B2-microglobulin, lactate dehydrogenase, albumin, vitamin B12 and C-reactive protein and concluded that serum chemistry profiling is crucial for diagnosis and prognostication.36 A panel of experts from the ECNM together with an expert panel of the American Initiative in Mast Cell Diseases (AIM) reviewed these prognostic scoring systems and recommended utilizing the IPSM and GPSM-PFS for non-aggressive SM and the IPSM, GPSM and MARS for patients with ASM.37
Treatment
Supportive Care
Although more pronounced in patients with ISM, mediator symptoms can be present in AdvSM patients and frequently require therapies, which can ameliorate the effects of MC degranulation. These therapies including histamine blockers, leukotriene inhibitors, sodium cromolyn, proton pump inhibitors and corticosteroids should be tailored based on mediator symptoms. Avoidance of symptom triggers should be discussed with all patients and those at risk for anaphylaxis should carry a self-injected epinephrine kit (EpiPen) at all times.38 In patients with AdvSM, additional supportive measures that may be required including screening and management of osteoporosis as well as transfusion support in addition to AdvSM directed therapy described below.
Midostaurin
Midostaurin is a multi-kinase inhibitor with activity against both wildtype and D816V mutated KIT that was approved for the treatment of AdvSM by the FDA in 2017.39 This agent has been evaluated in an open-label Phase 2 study, which included 116 AdvSM patients, of which 89 were included in the primary efficacy analysis (16 ASM, 57 SM-AHN, and 16 MCL) who were treated with midostaurin at a dose of 100mg twice daily. The primary endpoint of overall response was 60% by modified Valent and Cheson criteria.24,40 However, a post-hoc analysis using the IWG-MRT-ECNM consensus criteria identified the overall response rate (ORR) to be 28% when including clinical improvement (CI) as a response.41 Breakdown of responses among subtype is shown in Table 4. Responses were durable with a median duration of 24.1 months and there were significant reductions in MC burden in the bone marrow as well as serum tryptase levels. The median OS was 28.7 months with median PFS of 14.1 months. Importantly, there was also reversal of organ damage as evidenced by normalization of hypoalbuminemia in 58% of patients, and achievement of red blood cell and platelet transfusion independence in 40% and 100% of dependent patients, respectively. However, gastrointestinal adverse events (AEs) were common, with all grade nausea being observed in 79% of patients, vomiting in 66% of patients, and in 54% of patients. Dose reductions because of AEs were required in 41% of patients and AEs led to discontinuation in 22% of patients.42
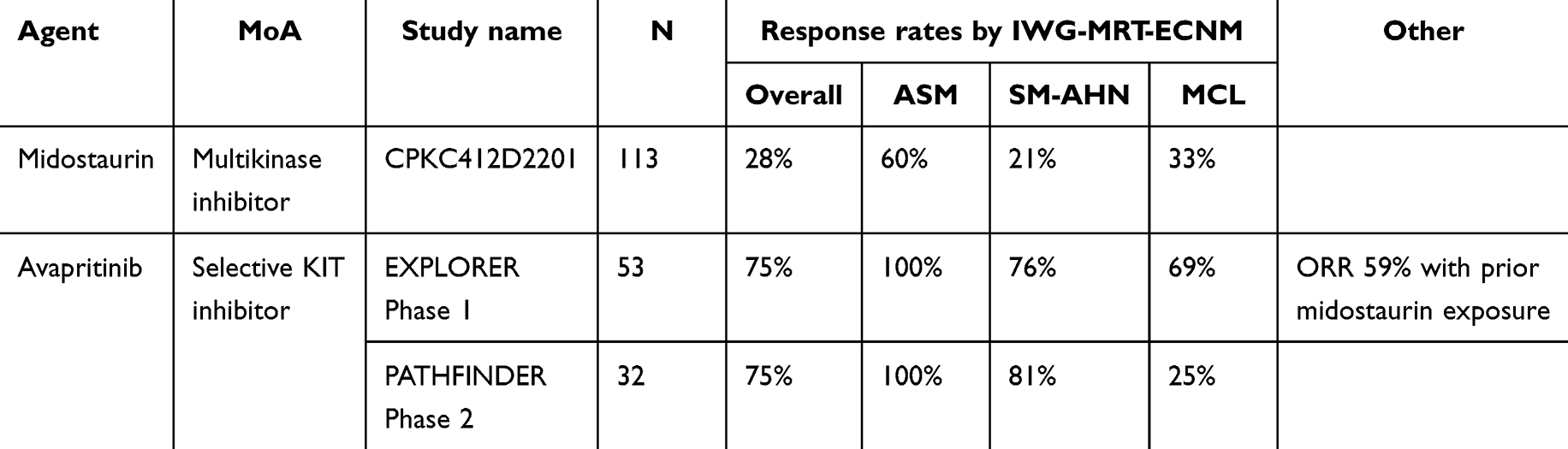 |
Table 4 Outcomes of Midostaurin and Avapritinib Clinical Trials in Advanced Systemic Mastocytosis |
Subsequent studies have aimed to compare midostaurin with cladribine using propensity-score matching and demonstrated superior OS (4.2 years versus 1.9 years) and leukemia-free survival (2.7 years versus 1.3 years).43 Predictors of superior OS in midostaurin-treated AdvSM patients include reduction of KITD816V allele burden by ≥25%. Of note, the same analysis also demonstrated that clonal evolution occurs while receiving midostaurin treatment, with acquisition of new mutations in KRAS, NRAS, RUNX1, IDH2, and NPM1.14 Midostaurin was the standard front-line therapy for AdvSM patients, however its use has largely been replaced by the introduction of avapritinib.
Avapritinib
Avapritinib is a highly selective type 1 inhibitor of KITD816V with higher potency as compared with midostaurin (IC50 0.27 versus 2.9) with negligible activity against wildtype KIT.44 Avapritinib was evaluated in AdvSM patients in the phase 1 EXPLORER study which enrolled 86 AdvSM patients. After dose escalation, the 200mg and 300mg dose cohorts were expanded. Among 69 evaluable patients, the ORR by IWG criteria was 75% (with breakdown by subtype shown in Table 3). ORR was higher in midostaurin naïve patients as compared to those previously treated (83% versus 59%). Importantly, 36% of patients experience a CR or CR with partial hematologic recovery (CRh) and 30% of patients experience of molecular CR.45 Bone marrow evaluation demonstrated reduction of MC aggregates, loss of CD25 expression, improvement in bone marrow fibrosis and reversal of spindled MC morphology.46 During a median follow-up of 23 months, 14 patients (20%) experienced disease progression, including 6 patients (9%) who developed acute myeloid leukemia (AML).45
Avapritinib has also been tested in the phase 2 PATHFINDER study at a dose of 200mg daily. The interim results have been published which includes 62 AdvSM patients with evaluable mIWG–MRT–ECNM C-finding or MCL. The ORR was also 75% including 19% with CR/CRh. Similar to EXPLORER, there was evidence of profound reduction in MC burden with 60% of patients attaining complete elimination of bone marrow MCs and 93% of patients attaining ≥50% reduction in tryptase levels. In addition, 60% of patients had ≥50% reduction in peripheral blood KITD816V allele burden.47 The results after three years of follow-up were recently presented and demonstrated that the median duration of response and OS was not reached.48
Despite these substantial benefits with avapritinib treatment in AdvSM, there are several safety considerations worth highlighting. In a pooled analysis of avapritinib 200mg daily from the EXPLORER and PATHFINDER trials, the most common non-hematologic AEs included peripheral/periorbital edema (all grades 81%), diarrhea (34%), nausea (31%), fatigue/asthenia (28%), and cognitive effects (25%). The cognitive effects included memory impairment and encephalopathy, which were reversible with dose reduction or interruption.49 In addition, intracranial hemorrhage occurred in 9 patients (13%) of patients in the EXPLORER study, although it was asymptomatic in 5 patients and occurred in the setting of antecedent thrombocytopenia in 7 patients.45 Based on these findings, a platelet count cut off of 50 × 109/L was added as an amendment in PATHFINDER. Only 1 patient (2%) experienced an intracranial hemorrhage before this exclusion criteria was implemented.47 Hematologic toxicities with avapritinib include neutropenia, anemia, and thrombocytopenia which were grade 3 in 16%, 27% and 30% of patients, respectively.45
As avapritinib has only been evaluated in single-arm studies, a recent retrospective analysis attempted to assess the difference between avapritinib and best available therapy (BAT) after adjusting for key covariates. Comparing 176 avapritinib treated patients in EXPLORER and PATHFINDER to 141 patients treated with 222 lines of therapy, which included tyrosine kinase inhibitors, mostly midostaurin (51%), cytoreductive agents including cladribine (25%) and hydroxyurea (9%), there was an improved OS with a hazard ratio (HR) of 0.48 (p=0.004) and significantly longer duration of treatment (HR 0.36, p<0.001). Tryptase reduction was also significantly deeper in the avapritinib group as compared to BAT.50 These results support the efficacy of avapritinib in patients with AdvSM in lieu of randomized controlled trial data.
Avapritinib is currently the standard therapy for newly diagnosed or previously treated AdvSM patients. Caution should be taken in patients with baseline thrombocytopenia, particularly those who have SM-AHN.
Other Therapies
Although largely supplanted by the availability of selective KIT inhibitors, therapies traditionally utilized for the treatment of AdvSM still may have a role. Cladribine, a nucleoside analogue, is an effective agent for rapid de-bulking of MCs or in AdvSM patients relapsed or refractory to other agents. Of note, while this agent is associated with clinical responses, treatment-related toxicity can also occur. This is highlighted in one of the largest experiences of cladribine in SM, a French nationwide retrospective experience which included 32 patients with AdvSM. The ORR was 50% in AdvSM patients with a duration of response of 2.5 years for ASM and 4.8 years in SM-AHN. Myelosuppression is relatively common with neutropenia in 47% of patients and 22% experiencing infectious complications in the total cohort (including ISM patients).51
Interferon alfa (IFN-a) treatment has also been historically used for the treatment of all subtypes of SM.52 In a report of 36 AdvSM patients treatment with IFN-a with or without prednisone resulted in an ORR of 60% and 45% for ASM and SM-AHN, respectively.53 Notable toxicities include depression, thrombocytopenia, and flu-like symptoms after administration.54 A pegylated version has less frequent dosing and improved tolerability. We reserve IFN-a for patients with slowly progressive AdvSM who are not candidates for other therapies. Hydroxyurea has also been explored, although there is minimal data to effectively characterize the clinical benefit.53
Finally, imatinib can be utilized in the rare patient who does not harbor KITD816V mutation or who has a mutation outside of exon 17.55 Imatinib has demonstrated efficacy against wild-type KIT and certain trans-membrane and juxta-membrane KIT mutants, however, the KITD816V mutation is resistant to imatinib.56
Allogeneic Stem Cell Transplantation
Allogeneic stem cell transplantation (ASCT) is a potentially curative option in patients with AdvSM, although experience to date has largely been reported in SM-AHN. The largest retrospective series of 57 patients (38 with SM-AHN, 7 with ASM, 12 with MCL) demonstrated significant decreases in bone marrow MC percentages and serum tryptase levels. All patients with SM-AHN achieved a CR from their associated hematologic disease but 10 went on to relapse and five of those ultimately died. MCL patients had the highest rate of treatment-related mortality and highest primary resistance to ASCT. OS at 3 years was 43%, 17%, and 74% for ASM, MCL, SM-AHN, respectively.57 Consensus opinion on the role of ASCT in AdvSM recommends for MC debulking with the use of a KIT inhibitor or chemotherapy before proceeding to ASCT, particularly in the setting of MCL. Outside of this subtype, appropriate AdvSM patients for ASCT include younger patients who have achieved a response and have a suitable donor.58 However, the calculation of when to proceed to ASCT has been complicated by the availability of selective KIT inhibitors. In follow-up from the phase 1 avapritinib study, the 2-year OS rates were 100%, 92%, 67%, for ASM, MCL, SM-AHN, respectively, which compares favorably to ASCT data with the exception of SM-AHN.45 Therefore, in the case of patients with SM-AHN, we preferentially triage patients to ASCT if eligible as a curative modality for both the SM and AHN components.
Novel Agents
The development of TKIs has revolutionized treatment for AdvSM. Previously, cytoreductive therapy was the mainstay of treatment and now selective KIT inhibitors such as avapritinib represent the standard of care he D816V KIT point mutation also confers resistance against several tyrosine kinase inhibitors including imatinib.59 There are several clinical trials underway evaluating novel TKIs in this patient population.
Elenestinib (BLU-263)
Elenestinib (BLU-263) is a potent and selective small-molecule inhibitor of KITD816V with limited central nervous system (CNS) penetration and daily dosing strategy. This agent showed favorable tolerability and safety profile in a phase 1 trial. The ongoing randomized double-blind phase 2/3 HARBOR trial (NCT04910685) includes patients with ISM. After 12 weeks of therapy, elenestinib demonstrated beneficial effects on total symptom score and biomarkers of MC burden. Patients receiving elenestinib at 25 mg, 50 mg, and 100 mg doses showed reduction from baseline for tryptase (−15.4%, −50.9%, and −68.4% vs 3.3 respectively) and KITD816V VAF (−37.5%, −70.3%, and −77.0% vs −2.5%, respectively) as compared to placebo.60 This agent is also being evaluated in the AZURE phase 1/2 trial (NCT05609942) for patients with advanced AdvSM as a monotherapy or in combination with azacytidine if indicated for an AHN.61
Bezuclastinib (CGT9486)
Bezuclastinib is a potent and selective inhibitor of KITD816V, with minimal effects on other kinases. This agent has low CNS penetration, high selectivity, and favorable pharmacokinetics, which ideally minimize systemic and CNS side effects. Bezuclastinib is currently being evaluated in a Phase 2 clinical trial, APEX (NCT04996875) with 140 adult patients with AdvSM per WHO criteria with SM-related organ damage, baseline serum tryptase of ≥20 ng/mL and could have received prior TKI therapy.62 As of April 2023, Part 1 was fully enrolled with 33 AdvSM patients. Data with 32 evaluable patients showed 56% ORR rate and 75% ORR as well as deep reductions across biomarkers of MC activity, with 94% of patients experiencing a ≥50% decrease in serum tryptase, 93% with ≥50% reduction in KITD816V VAF and 97% of patients with a ≥50% bone marrow MC burden. The majority of AEs were low grade and reversible. The most frequent AEs were hair color changes 34%, thrombocytopenia 22%, increases in transaminase 22%, neutropenia 19% and taste disorder 19% and no reported cognitive or bleeding events.63,64
Conclusions and Unresolved Clinical Challenges
There has been undeniable progress over the last decade in the treatment of AdvSM, culminating in the approval of the selective KITD816V inhibitor avapritinib. However, there remain several unresolved clinical challenges. For one, with the potential introduction of additional selective KIT inhibitors including BLU-263 and bezuclastinib, the ideal sequencing of available KIT inhibitors will need to be clarified. In particular, for patients who are relapsed, refractory or intolerant to avapritinib, the efficacy of additional KIT inhibitors in this setting will need to be established. Targets outside of KIT that can be targeted in combination with KIT inhibitors, including antibody directed therapy targeting MCs,65,66 intracellular signaling pathways such as JAK-STAT,67 and BCL-2 mediating induction of apoptosis,68 should be explored to improve upon the efficacy seen with avapritinib.
While KIT inhibition has been efficacious in controlling SM features, SM-AHN patients may continue to have complications related to the AHN. For instance, in patients with CMML (the most common AHN), reductions in bone marrow monocyte burden are minimal with midostaurin, but treatment did result in the complete normalization of eosinophilia.69 The dynamics between neoplastic MCs and the AHN during KIT inhibition will need to be dissected in further studies. The optimal incorporation of KIT directed therapy into treatment of the AHN is also not well explored and the limitation in terms of thrombocytopenia with avapritinib introduces concurrent treatment challenges. The incorporation of KIT inhibitors associated with less myelosuppression may allow exploration of the concurrent treatment for both the SM and the AHN component.
Given the impressive activity of selective KIT inhibition in reducing and in many cases eliminating KITD816V mutational burden, the concept of measurable residual disease (MRD) may now be relevant to AdvSM patients. Exploration of the predictive potential of KIT 816V responses for survival and incorporation of MRD into established response criteria will be important as therapeutic advances in AdvSM continue. Finally, treatment outcomes of high-risk patients, including patients with MCL, remain inadequate and further therapeutic advances are urgently needed to improve outcomes in these patients. Thanks largely to collaborations between academia and the pharmaceutical industry as well as patient advocacy groups, the increased attention directed towards this rare disease will continue to propel therapeutic advances that can improve the quantity and quality of life for patients with AdvSM.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
DT received research funding from Sobi, Sumitomo, Cogent Biosciences and Gilead and honoraria from Sobi, Novartis, AbbVie, PharmaEssentia, Sierra Oncology, GSK and Cogent Biosciences. JM received research funding from Incyte, BMS, Novartis, AbbVie, Geron, Kartos, Karyopharm, CTI/Sobi and PharmaEssentia and honoraria from Incyte, Blueprint Medicines, Keros, DISC Medicines, BMS, AbbVie, Kartos, Geron, GSK, Roche, Merck, Pfizer, PharmaEssentia, MorphoSys, Novartis, Galecto, Sobi, Sumitomo, and Karyopharm. The authors report no other conflicts of interest in this work.
References
1. Bergstrom A, Hagglund H, Berglund A, Nilsson G, Lambe M. Epidemiology of mastocytosis: a population-based study (Sweden). Acta Oncol. 2024;63:44–50. doi:10.2340/1651-226X.2024.31406
2. Rottem M, Kirshenbaum AS, Metcalfe DD. Early development of mast cells. Int Arch Allergy Appl Immunol. 1991;94(1–4):104–109. doi:10.1159/000235339
3. Martelli M, Monaldi C, De Santis S, et al. Recent advances in the molecular biology of systemic mastocytosis: implications for diagnosis, prognosis, and therapy. Int J Mol Sci. 2020;21(11):3987. doi:10.3390/ijms21113987
4. Nagata H, Worobec AS, Oh CK, et al. Identification of a point mutation in the catalytic domain of the protooncogene c-kit in peripheral blood mononuclear cells of patients who have mastocytosis with an associated hematologic disorder. Proc Natl Acad Sci USA. 1995;92(23):10560–10564. doi:10.1073/pnas.92.23.10560
5. Bibi S, Langenfeld F, Jeanningros S, et al. Molecular defects in mastocytosis: KIT and beyond KIT. Immunol Allergy Clin North Am. 2014;34(2):239–262. doi:10.1016/j.iac.2014.01.009
6. Cruse G, Metcalfe DD, Olivera A. Functional deregulation of KIT: link to mast cell proliferative diseases and other neoplasms. Immunol Allergy Clin North Am. 2014;34(2):219–237. doi:10.1016/j.iac.2014.01.002
7. Harir N, Boudot C, Friedbichler K, et al. Oncogenic Kit controls neoplastic mast cell growth through a Stat5/PI3-kinase signaling cascade. Blood. 2008;112(6):2463–2473. doi:10.1182/blood-2007-09-115477
8. Valent P, Horny HP, Escribano L, et al. Diagnostic criteria and classification of mastocytosis: a consensus proposal. Leukemia Res. 2001;25(7):603–625. doi:10.1016/s0145-2126(01)00038-8
9. Lim KH, Tefferi A, Lasho TL, et al. Systemic mastocytosis in 342 consecutive adults: survival studies and prognostic factors. Blood. 2009;113(23):5727–5736. doi:10.1182/blood-2009-02-205237
10. Stevens EC, Rosenthal NS. Bone marrow mast cell morphologic features and hematopoietic dyspoiesis in systemic mast cell disease. Am J Clin Pathol. 2001;116(2):177–182. doi:10.1309/Q2WJ-46CL-YRFT-M5JF
11. He S, Gaca MD, Walls AF. A role for tryptase in the activation of human mast cells: modulation of histamine release by tryptase and inhibitors of tryptase. J Pharmacol Exp Ther. 1998;286(1):289–297.
12. Hoermann G, Gleixner KV, Dinu GE, et al. The KIT D816V allele burden predicts survival in patients with mastocytosis and correlates with the WHO type of the disease. Allergy. 2014;69(6):810–813. doi:10.1111/all.12409
13. Gotlib J, Pardanani A, Akin C, et al. International working group-myeloproliferative neoplasms research and treatment (IWG-MRT) & European Competence Network on Mastocytosis (ECNM) consensus response criteria in advanced systemic mastocytosis. Blood. 2013;121(13):2393–2401. doi:10.1182/blood-2012-09-458521
14. Jawhar M, Schwaab J, Naumann N, et al. Response and progression on midostaurin in advanced systemic mastocytosis: KIT D816V and other molecular markers. Blood. 2017;130(2):137–145. doi:10.1182/blood-2017-01-764423
15. Tefferi A, Shah S, Reichard KK, Hanson CA, Pardanani A. Smoldering mastocytosis: survival comparisons with indolent and aggressive mastocytosis. Am J Hematol. 2019;94(1):E1–E2. doi:10.1002/ajh.25302
16. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391–2405. doi:10.1182/blood-2016-03-643544
17. Arber DA, Hasserjian RP, Borowitz MJ, et al. International consensus classification of myeloid neoplasms and acute leukemias: integrating morphologic, clinical, and genomic data. Blood. 2022;140(11):1200–1228. PMID: 35767897; PMCID: PMC9479031. doi:10.1182/blood.2022015850
18. Mukherjee S, Cattie DJ, Shaheen D, Powell D, Green T. Decreased survival among patients with indolent systemic mastocytosis: a population-level retrospective cohort analysis using healthcare claims dataset. Blood. 2023;142:75. doi:10.1182/blood-2023-188617
19. Cree IA. The WHO classification of haematolymphoid tumours. Leukemia. 2022;36(7):1701–1702. doi:10.1038/s41375-022-01625-x
20. Zanotti R, Bonifacio M, Lucchini G, et al. Refined diagnostic criteria for bone marrow mastocytosis: a proposal of the European competence network on mastocytosis. Leukemia. 2022;36(2):516–524. doi:10.1038/s41375-021-01406-y
21. Khoury JD, Solary E, Abla O, et al. The 5th edition of the World Health Organization classification of haematolymphoid tumours: myeloid and histiocytic/dendritic neoplasms. leukemia. 2022;36(7):1703–1719. doi:10.1038/s41375-022-01613-1
22. Valent P, Akin C, Metcalfe DD. Mastocytosis: 2016 updated WHO classification and novel emerging treatment concepts. Blood. 2017;129(11):1420–1427. doi:10.1182/blood-2016-09-731893
23. Pardanani A. Systemic mastocytosis in adults: 2021 update on diagnosis, risk stratification and management. Am J Hematol. 2021;96(4):508–525. doi:10.1002/ajh.26118
24. Valent P, Akin C, Sperr WR, et al. Aggressive systemic mastocytosis and related mast cell disorders: current treatment options and proposed response criteria. Leukemia Res. 2003;27(7):635–641. doi:10.1016/S0145-2126(02)00168-6
25. Pardanani A, Tefferi A. Systemic mastocytosis in adults: a review on prognosis and treatment based on 342 Mayo clinic patients and current literature. Curr Opin Hematol. 2010;17(2):125–132. doi:10.1097/MOH.0b013e3283366c59
26. Pardanani A, Lim KH, Lasho TL, et al. Prognostically relevant breakdown of 123 patients with systemic mastocytosis associated with other myeloid malignancies. Blood. 2009;114(18):3769–3772. doi:10.1182/blood-2009-05-220145
27. Jain P, Wang S, Patel KP, et al. Mast cell leukemia (MCL): clinico-pathologic and molecular features and survival outcome. Leuk Res. 2017;59:105–109. doi:10.1016/j.leukres.2017.05.018
28. Zini G, Bennett JM. ICC-2022 versus WHO-2022 classification systems for acute leukemias and myeloid neoplasms: the perspective from two classical morphologists. Am J Hematol. 2023;98(8):E209–E211. doi:10.1002/ajh.26963
29. Schwaab J, Schnittger S, Sotlar K, et al. Comprehensive mutational profiling in advanced systemic mastocytosis. Blood. 2013;122(14):2460–2466. doi:10.1182/blood-2013-04-496448
30. Pardanani A, Lasho T, Elala Y, et al. Next-generation sequencing in systemic mastocytosis: derivation of a mutation-augmented clinical prognostic model for survival. Am J Hematol. 2016;91(9):888–893. doi:10.1002/ajh.24426
31. Pardanani A, Lasho TL, Reichard KK, Hanson CA, Tefferi A. World Health Organization class-independent risk categorization in mastocytosis. Blood Cancer J. 2019;9(3):29. doi:10.1038/s41408-019-0189-5
32. Sperr WR, Kundi M, Alvarez-Twose I, et al. International prognostic scoring system for mastocytosis (IPSM): a retrospective cohort study. Lancet Haematol. 2019;6(12):e638–e649. doi:10.1016/S2352-3026(19)30166-8
33. Sperr WR, Kundi M, Alvarez-Twose I, et al. International prognostic scoring system for mastocytosis (IPSM): a retrospective cohort study. Lancet Haematol. 2019;6(12):e638–e649. doi:10.1016/S2352-3026(19)30166-8
34. Munoz-Gonzalez JI, Alvarez-Twose I, Jara-Acevedo M, et al. Proposed global prognostic score for systemic mastocytosis: a retrospective prognostic modelling study. Lancet Haematol. 2021;8(3):e194–e204. doi:10.1016/S2352-3026(20)30400-2
35. Jawhar M, Schwaab J, Alvarez-Twose I, et al. Mars: mutation-adjusted risk score for advanced systemic mastocytosis. J Clin Oncol. 2019;37(31):2846–2856. doi:10.1200/JCO.19.00640
36. Lübke J, Schmid A, Christen D, et al. Serum chemistry profiling and prognostication in systemic mastocytosis: a registry-based study of the ECNM and GREM. Blood Adv. 2024;8(11):2890–2900. doi:10.1182/bloodadvances.2024012756
37. Valent P, Hartmann K, Schwaab J, et al. Personalized management strategies in mast cell disorders: ECNM-AIM user’s guide for daily clinical practice. J Allergy Clin Immunol Pract. 2022;10(8):1999–2012e6. doi:10.1016/j.jaip.2022.03.007
38. Valent P, Sperr WR, Akin C. How I treat patients with advanced systemic mastocytosis. Blood. 2010;116(26):5812–5817. doi:10.1182/blood-2010-08-292144
39. Kim ES. Midostaurin: first global approval. Drugs. 2017;77:1251–1259. doi:10.1007/s40265-017-0779-0
40. Cheson BD, Greenberg PL, Bennett JM, et al. Clinical application and proposal for modification of the International Working Group (IWG) response criteria in myelodysplasia. Blood. 2006;108(2):419–425. doi:10.1182/blood-2005-10-4149
41. European Medicines Agency. Summary of product characteristics. Available from: https://www.ema.europa.eu/en/glossary-terms/summary-product-characteristics#:~:text=A%20document%20describing%20the%20properties,Abbreviated%20as%20SmPC.
42. Gotlib J, Kluin-Nelemans HC, George TI, et al. Efficacy and safety of midostaurin in advanced systemic mastocytosis. New Engl J Med. 2016;374(26):2530–2541. doi:10.1056/NEJMoa1513098
43. Lubke J, Schwaab J, Naumann N, et al. Superior efficacy of midostaurin over cladribine in advanced systemic mastocytosis: a registry-based analysis. J Clin Oncol. 2022;40(16):1783–1794. doi:10.1200/JCO.21.01849
44. Evans EK, Gardino AK, Kim JL, et al. A precision therapy against cancers driven by KIT/PDGFRA mutations. Sci Transl Med. 2017;9(414). doi:10.1126/scitranslmed.aao1690
45. DeAngelo DJ, Radia DH, George TI, et al. Safety and efficacy of avapritinib in advanced systemic mastocytosis: the phase 1 EXPLORER trial. Nature Med. 2021;27(12):2183–2191. doi:10.1038/s41591-021-01538-9
46. George TI, Karner KH, Moser KA, et al. Efficacy of avapritinib in patients with advanced systemic mastocytosis: hematologic and bone marrow responses from the phase 2 open-label, single-arm, pathfinder study. Blood. 2021;138:2565. doi:10.1182/blood-2021-146873
47. Gotlib J, Reiter A, Radia DH, et al. Efficacy and safety of avapritinib in advanced systemic mastocytosis: interim analysis of the phase 2 PATHFINDER trial. Nature Med. 2021;27(12):2192–2199. doi:10.1038/s41591-021-01539-8
48. Reiter A, Gotlib J, Radia D, et al. Avapritinib in patients with advanced systemic mastocytosis (Advsm): efficacy and safety analysis from the phase 2 Pathfinder study with 3-year follow-up.
49. Radia D, DeAngelo D, Deininger MW, et al. MPN-395: efficacy and safety of≤ 200 mg avapritinib in patients with advanced systemic mastocytosis: pooled results from the phase 1 EXPLORER and interim phase 2 PATHFINDER studies. Clin Lymphoma Myeloma Leukemia. 2021;21:S367–S368. doi:10.1016/S2152-2650(21)01843-7
50. Reiter A, Gotlib J, Alvarez-Twose I, et al. Efficacy of avapritinib versus best available therapy in the treatment of advanced systemic mastocytosis. Leukemia. 2022;36(8):2108–2120. doi:10.1038/s41375-022-01615-z
51. Barete S, Lortholary O, Damaj G, et al. Long-term efficacy and safety of cladribine (2-CdA) in adult patients with mastocytosis. Blood. 2015;126(8):1009–1016. doi:10.1182/blood-2014-12-614743
52. Kluin-Nelemans HC, Jansen JH, Breukelman H, et al. Response to interferon alfa-2b in a patient with systemic mastocytosis. New Engl J Med. 1992;326(9):619–623. doi:10.1056/NEJM199202273260907
53. Lim KH, Pardanani A, Butterfield JH, Li CY, Tefferi A. Cytoreductive therapy in 108 adults with systemic mastocytosis: outcome analysis and response prediction during treatment with interferon-alpha, hydroxyurea, imatinib mesylate or 2-chlorodeoxyadenosine. Am J Hematol. 2009;84(12):790–794. doi:10.1002/ajh.21561
54. Casassus P, Caillat-Vigneron N, Martin A, et al. Treatment of adult systemic mastocytosis with interferon-alpha: results of a multicentre Phase II trial on 20 patients. Br J Haematol. 2002;119(4):1090–1097. doi:10.1046/j.1365-2141.2002.03944.x
55. Vega-Ruiz A, Cortes JE, Sever M, et al. Phase II study of imatinib mesylate as therapy for patients with systemic mastocytosis. Leukemia Res. 2009;33(11):1481–1484. doi:10.1016/j.leukres.2008.12.020
56. Akin C, Fumo G, Yavuz AS, Lipsky PE, Neckers L, Metcalfe DD. A novel form of mastocytosis associated with a transmembrane c-kit mutation and response to imatinib. Blood. 2004;103(8):3222–3225. doi:10.1182/blood-2003-11-3816
57. Ustun C, Reiter A, Scott BL, et al. Hematopoietic stem-cell transplantation for advanced systemic mastocytosis. J Clin Oncol. 2014;32(29):3264–3274. doi:10.1200/JCO.2014.55.2018
58. Ustun C, Gotlib J, Popat U, et al. Consensus opinion on allogeneic hematopoietic cell transplantation in advanced systemic mastocytosis. Bio Blood Marrow Transplant. 2016;22(8):1348–1356. doi:10.1016/j.bbmt.2016.04.018
59. Shah NP, Lee FY, Luo R, Jiang Y, Donker M, Akin C. Dasatinib (BMS-354825) inhibits KITD816V, an imatinib-resistant activating mutation that triggers neoplastic growth in most patients with systemic mastocytosis. Blood. 2006;108(1):286–291. doi:10.1182/blood-2005-10-3969
60. Tashi T, Hermine O, Castells M, et al. Elenestinib, an investigational, next generation KIT D816V inhibitor, reduces mast cell burden, improves symptoms, and has a favorable safety profile in patients with indolent systemic mastocytosis: analysis of the harbor trial. Blood. 2023;142(Supplement 1):76. doi:10.1182/blood-2023-188904
61. DeAngelo DJ, George TI, Reiter A, et al. AZURE: a phase 1/2 study of Blu-263 as monotherapy and in combination with azacitidine in patients with advanced systemic mastocytosis. Blood. 2022;140:6877–6878. doi:10.1182/blood-2022-167410
62. DeAngelo DJ, Pullarkat V, Piris-Villaespesa M, et al. P1049: a phase 2 study of bezuclastinib (CGT9486), a novel, highly selective, potent kit D816v Inhibitor, in adults with advanced systemic mastocytosis (APEX): methods, baseline data, and early insights. Hemasphere. 2022;6:939–940. eCollection 2022 Jun. doi:10.1097/01.HS9.0000847064.38588.9b
63. DeAngelo DJ, Pullarkat V, Piris-Villaespesa M, et al. Preliminary safety and efficacy from Apex, a phase 2 study of bezuclastinib (CGT9486), a novel, highly selective, potent KIT D816V tyrosine kinase inhibitor, in adults with advanced systemic mastocytosis (AdvSM). Blood. 2022;140:1512–1513. doi:10.1182/blood-2022-156311
64. Vachhani P, Tashi T, Schiller GJ, et al. Safety and efficacy of bezuclastinib (CGT9486), a novel, highly selective, potent KIT D816V tyrosine kinase inhibitor, in patients with advanced systemic mastocytosis (AdvSM): results from part 1 of the phase 2 Apex trial. Blood. 2023;142(Supplement 1):4567. doi:10.1182/blood-2023-178885
65. Gotlib J, Baird JH, George TI, et al. A phase 2 study of brentuximab vedotin in patients with CD30-positive advanced systemic mastocytosis. Blood Adv. 2019;3(15):2264–2271. doi:10.1182/bloodadvances.2019000152
66. Alvarez-Twose I, Martinez-Barranco P, Gotlib J, et al. Complete response to gemtuzumab ozogamicin in a patient with refractory mast cell leukemia. Leukemia. 2016;30(8):1753–1756. doi:10.1038/leu.2016.30
67. Yacoub A, Prochaska L. Ruxolitinib improves symptoms and quality of life in a patient with systemic mastocytosis. Biomark Res. 2016;4:2. doi:10.1186/s40364-016-0056-5
68. Canioni D, Moraly J, Lhermitte L, et al. BCL-2 is expressed in advanced mastocytosis and midaustorin induces venetoclax sensitivity of mast leukemia cell lines. Blood. 2019;134:1683. doi:10.1182/blood-2019-131256
69. DeAngelo DJ, George TI, Linder A, et al. Efficacy and safety of midostaurin in patients with advanced systemic mastocytosis: 10-year median follow-up of a phase II trial. Leukemia. 2018;32(2):470–478. doi:10.1038/leu.2017.234
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.