Back to Journals » International Medical Case Reports Journal » Volume 15
MALT Lymphoma Presenting with Peripheral Ulcerative Keratitis
Authors Patil S, Colby K, Lazzaro D
Received 23 February 2022
Accepted for publication 5 May 2022
Published 11 September 2022 Volume 2022:15 Pages 485—490
DOI https://doi.org/10.2147/IMCRJ.S361865
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sachi Patil, Kathryn Colby, Douglas Lazzaro
Department of Ophthalmology, New York University Langone Health, New York, NY, USA
Correspondence: Sachi Patil, New York University Grossman School of Medicine, 550 First Avenue, New York, NY, 10016, USA, Tel +1 (631)-793-2594, Email [email protected]
Objective: To report a case of ocular mucosa-associated lymphoid tissue (MALT) lymphoma presenting with peripheral ulcerative keratitis.
Methods: A 58-year-old man with a history of vitreous syneresis in both eyes and glaucoma presented with an abnormal, painful sensation of the left eye and mild hyperemia. Physical examination revealed peripheral ulcerative keratitis superiorly and a salmon-colored lesion in the superior conjunctiva.
Results: The differential diagnosis of superior corneal thinning includes collagen vascular disease, Terrien’s marginal degeneration, infectious keratitis, and other forms of peripheral keratitis. Our patient was diagnosed with conjunctival MALT lymphoma by surgical excision of the mass, and the peripheral ulcerative keratitis may be related to this diagnosis.
Conclusion: Although rare, this case demonstrates a peripheral keratitis possibly related to the underlying disease of MALT lymphoma. The patient is being treated with local radiation treatment.
Keywords: ocular lymphoma, peripheral ulcerative keratitis, MALT lymphoma
Mucosa-associated lymphoid tissue (MALT) lymphomas are neoplastic proliferations of B cells of the marginal zone of lymphoid tissue which can arise along any mucosal lining. They most commonly affect the gastric lining, but other extra nodal sites include the salivary gland, lacrimal glands, thyroid, breast, skin, and eyes. MALT lymphomas, particularly when extragastric, are often associated with underlying autoimmune disease.1 By incidence, ocular lymphomas are rare and have been estimated to represent 1.86% of the ocular malignant tumors.2 Diagnosis is challenging because patients present with common complaints of worsening vision, floaters, or a combination of both depending on which portion of the eye is affected. Ocular lymphomas can be divided into three groups: ocular adnexal, uveal, and vitreoretinal. Ocular adnexal lymphomas involve the eyelid, conjunctiva, lacrimal gland, and other orbital structures. The majority of these lymphomas are low grade, B-cell predominantly non-Hodgkin’s lymphomas, and 80% are extra-nodal marginal zone lymphoma subtypes.3 The goal of this case is to illustrate an atypical case of ocular MALT lymphoma presenting with peripheral ulcerative keratitis.
Case Presentation
The patient is a 58-year-old man with a history of well-managed glaucoma and psoriasis. The patient was notified of the writing of this deidentified case report and provided written consent. Institutional approval was not required to publish case details. His glaucoma was maintained with a single topical agent taken twice daily. The patient initially presented for examination with mild pain and conjunctival hyperemia, without visual changes. He also denied photophobia.
On exam, the patient’s visual acuity was 20/40 OD and 20/25 OS. In the left eye, the patient had a salmon-colored lesion on the superior conjunctiva depicted in Figure 1. The cornea below the lesion had an area of thinning consistent with peripheral ulcerative keratitis (Figure 2). The epithelium measured 40 microns superiorly (Figure 3). On fluorescein staining, there was a partial defect in the central part of the circumferential ulcer. There was mild conjunctival hyperemia without episcleritis, corneal infiltrate, scleritis, or anterior chamber inflammation. There were no ocular surface changes such as tear film abnormalities, blepharitis, or dry eye. Fundus examnation revealed superior arcade cream colored faint lesions (Figure 4). The rest of the physical exam including tonometry was within normal limits.
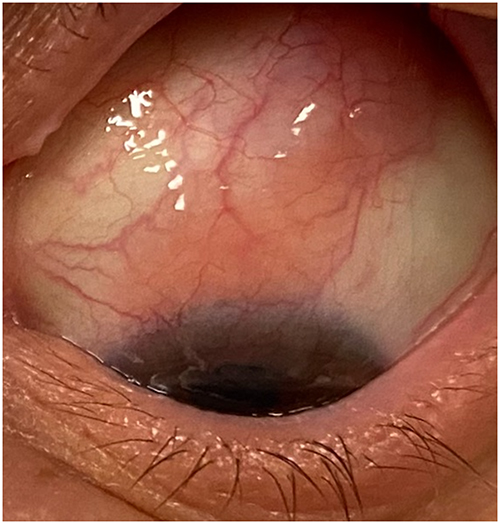 |
Figure 1 Color photograph visualizing salmon-colored lesion on the conjunctiva. |
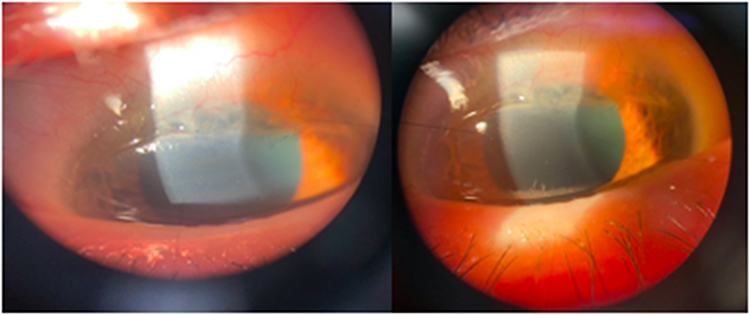 |
Figure 2 Color photographs visualizing corneal thinning and peripheral ulcerative keratitis lesion in the cornea. |
 |
Figure 3 Corneal topography of patient at initial visit indicating area of superior epithelial thinning OS. |
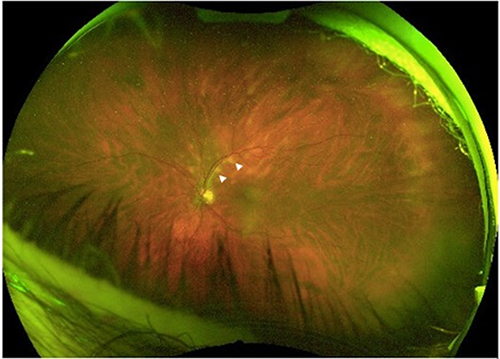 |
Figure 4 Fundus photograph OS. Lesions involving the choroid along the superior arcades are indicated with white arrowheads. |
The patient underwent excisional biopsy of the left conjunctival lesion with placement of an amniotic membrane graft and was prescribed tobramycin–dexamethasone QID for a week after surgery. Flow cytometry demonstrated an aberrant population of CD5 negative, CD10 negative small B lymphocytes compatible with a B-cell non-Hodgkin’s lymphoma. The pathologic surgical specimen confirmed the diagnosis of extranodal marginal zone lymphoma (EMZL). The patient was referred to oncology and underwent a systemic workup including PET/MRI imaging to search for orbital involvement and underlying primary disease elsewhere. All tests were negative for tumor elsewhere. The patient had undergone screening colonoscopy 1-month prior to presentation, which was normal. No other local therapies were administered for the PUK. The patient is following up closely with oncology and is being treated with local radiation therapy of the conjunctiva. He is receiving radiation of the conjunctival sac and lacrimal gland. On follow-up, 3 months after the initial work-up, excision of lesion, and radiation treatment, the area of superior thinning has improved (Figure 5). His visual acuity OS was 20/30, and he refracted to −5.00, −1.50 with an axis of 090, and is doing very well.
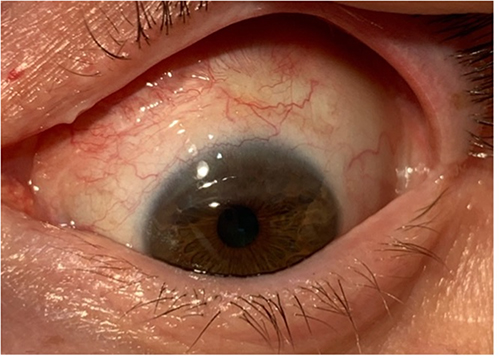 |
Figure 5 Images of left eye 3 months after excision and radiation. Inflammation is resolved and epithelium is healing. |
Discussion
The differential diagnosis for the corneal thinning was broad, with the first necessary distinction to discern if the lesion was secondary to local or systemic pathology. Within local defects, the epithelial defect may have been secondary to non-inflammatory peripheral thinning disorders such as Terrien’s marginal degeneration. However, in Terrien’s, patients are usually asymptomatic except for decreased vision and have an intact epithelium.4,5 Terrien’s marginal degeneration was further unlikely given the lack of a leading edge of lipid, as well the absence of against the rule or oblique astigmatism from flattening of the vertical meridian.5 Another item on the differential was a corneal dellen, which is a shallow excavation at the margin of the cornea. Other local causes of epithelial defects, including local marginal keratitis, blepharitis secondary to staphylococcal infection, contact lens use, chemical injury, or trauma to the eyes, were ruled out based on history.
A multitude of laboratory tests were ordered to rule out underlying etiologies including infection, connective tissue disease, sarcoidosis, inflammatory bowel disease, and alpha-1 antitrypsin deficiency.6,7 Laboratory panels included a complete blood count with differential, erythrocyte sedimentation rate, anti-neutrophil cytoplasmic antibody (ANCA), fluorescent treponemal antibody and venereal disease research lab tests (FTA/VDRL), rheumatoid factor (RF), anti-myeloperoxidase, anti Scl-70, anti-chromatin, anti-DNA, anti-ribonucleoprotein, and anti-Jo-1, which all were negative. The two positive results were the Sjogren’s anti-la antibody and anti-nuclear antibody which were mildly elevated. Many of these systemic illnesses present with characteristic findings throughout the body, such as a facial butterfly rash in the setting of SLE, facial telangiectasias in the setting of rosacea, or upper and lower respiratory symptoms in granulomatosis with polyangiitis, all of which were absent in this patient. Given the fact that the patient had no episcleritis, scleritis, uveitis, or other ocular surface symptoms, systemic inflammatory diseases further remained low on our differential.
Ultimately, the diagnosis of PUK was made given the constellation of clinical findings including mild pain, hyperemia of the conjunctiva, and the extensive work-up to rule out other causes of the corneal thinning. We did not believe this was a thinning due to a corneal wetting abnormality. Peripheral ulcerative keratitis is a term used to describe a group of destructive inflammatory diseases involving the peripheral cornea whose final common pathway is characterized by sloughing of the corneal epithelium and keratolysis. On examination, patients present with a crescent sharped, juxtalimbal corneal stromal process associated with an epithelial defect, stromal inflammatory cells, and stromal degradation. Conjunctival, episcleral and scleral inflammation are usually evident. PUK has been previously described as a presentation of hepatitis B and as a Mooren type ulcer in hepatitis C, which were also ruled out. PUK is seen in other autoimmune inflammatory conditions such as rheumatoid arthritis, polyarteritis nodosa, and collagen vascular diseases such as systemic lupus erythematosus. PUK has also been reported in a case secondary to gout.8
Extranodal marginal zone lymphoma is the most common subtype of conjunctival lymphoma, representing 80% of the cases.9 Approximately 5–15% of all extranodal lymphomas are found in the ocular adnexal region, and approximately 25% of those involve the conjunctiva.10 Treatment for ocular lymphoma, particularly MALT lymphoma, depends on the histology and clinical stage. Histologically, extranodal and follicular lymphomas are considered generally low grade, while diffuse large B cell and mantle cell are much rarer and considered high grade. Extent of disease is also critical to proper treatment. Most low-grade lymphomas present as isolated entities without systemic involvement, as seen in this patient. The preferred treatment modality for stage 1E, an early stage, localized lymphoma, is radiation therapy. Radiation is used as curative single-modality therapy in early stage localized MALT lymphoma. As the lymphoma was confined to the conjunctiva, the radiation would include the entire conjunctiva, but would not need to include the entire orbit. The oncologists took additional efforts to spare the lens of the eye to reduce the incidence of cataract formation by utilizing an eye shield on the opposite eye. The logistics and potential adverse acute and late effects from the recommended radiotherapy were discussed, including but not limited to conjunctivitis, cataract formation (up to 50% of the patients), mild xerophthalmia (20–40% of the patients), corneal ulceration (very low risk at this dose), vision loss (extremely low risk as this dose), dermatitis, infection, pain, fatigue, and radiation-induced malignancies.11,12
The purpose of this case is to demonstrate the rare finding and potential association of peripheral ulcerative keratitis to the underlying disease of MALT lymphoma. We hope that this case is illustrative and informative for ophthalmologists and other physicians, as early detection and treatment of MALT lymphoma is favorable for patient outcomes.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wöhrer S, Troch M, Streubel B, et al. MALT lymphoma in patients with autoimmune diseases: a comparative analysis of characteristics and clinical course. Leukemia. 2007;21(8):1812–1818. doi:10.1038/sj.leu.2404782
2. Tang LJ, Gu CL, Zhang P. Intraocular lymphoma. Int J Ophthalmol. 2017;10(8):1301–1307. doi:10.18240/ijo.2017.08.19
3. Eckardt AM, Lemound J, Rana M, Gellrich NC. Orbital lymphoma: diagnostic approach and treatment outcome. World J Surg Oncol. 2013;11:73. doi:10.1186/1477-7819-11-73
4. Jinabhai A, Radhakrishnan H, O’Donnell C. Pellucid corneal marginal degeneration: a review. Cont Lens Anterior Eye. 2011;34(2):56–63. doi:10.1016/j.clae.2010.11.007
5. Chan AT, Ulate R, Goldich Y, Rootman DS, Chan CC. Terrien marginal degeneration: clinical characteristics and outcomes. Am J Ophthalmol. 2015;160(5):867–872.e1. doi:10.1016/j.ajo.2015.07.031
6. Harthan JS, Reeder RE. Peripheral ulcerative keratitis in association with sarcoidosis. Cont Lens Anterior Eye. 2013;36(6):313–317. doi:10.1016/j.clae.2013.07.013
7. Cao Y, Zhang W, Wu J, Zhang H, Zhou H. Peripheral ulcerative keratitis associated with autoimmune disease: pathogenesis and treatment. J Ophthalmol. 2017;2017:7298026. doi:10.1155/2017/7298026
8. Yazdanyar A, Rizzuti AE, Mechel E, Denisova K, Lazzaro DR. Gout keratitis: a case of peripheral ulcerative keratitis secondary to gout with a review of the literature. Cornea. 2018;37(3):379–381. doi:10.1097/ICO.0000000000001415
9. Kalogeropoulos D, Papoudou-Bai A, Kanavaros P, Kalogeropoulos C. Ocular adnexal marginal zone lymphoma of mucosa-associated lymphoid tissue. Clin Exp Med. 2018;18(2):151–163. doi:10.1007/s10238-017-0474-1
10. Tanenbaum RE, Galor A, Dubovy SR, Karp CL. Classification, diagnosis, and management of conjunctival lymphoma. Eye Vis. 2019;6:22. doi:10.1186/s40662-019-0146-1
11. Janjan NA. Radiation effects on the eye. Clin Plast Surg. 1993;20(3):535–549. doi:10.1016/S0094-1298(20)31196-2
12. Kleiman NJ, Stewart FA, Hall EJ. Modifiers of radiation effects in the eye. Life Sci Space Res. 2017;15:43–54. doi:10.1016/j.lssr.2017.07.005
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.