Back to Journals » International Medical Case Reports Journal » Volume 18
Malignant Transformation Associated with Endometrioid Adenocarcinoma of Abdominal Wall Endometriosis: A Case Report and Literature Review
Authors Wei M, Liu W, Zheng Z, Liu Y, Zhang X
Received 6 October 2025
Accepted for publication 23 December 2025
Published 30 December 2025 Volume 2025:18 Pages 1699—1707
DOI https://doi.org/10.2147/IMCRJ.S572060
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Thomas E Hutson
Ming Wei,1 Weijun Liu,1– 3 Zhangqiang Zheng,1 Yun Liu,1 Xingzhou Zhang1
1Tianjin NanKai Hospital, Tianjin Medical University, Tianjin, People’s Republic of China; 2Department of Scientific Research, Tianjin Key Laboratory of Acute Abdomen Disease Associated Organ Injury and ITCWM Repair, Tianjin, People’s Republic of China; 3Department of Scientific Research, Institute of Integrative Medicine for Acute Abdominal Diseases, Tianjin, People’s Republic of China
Correspondence: Xingzhou Zhang, Email [email protected]
Introduction: Endometriosis is a prevalent chronic gynecological disease, characterized by the growth of endometrial glands and stroma outside the uterus and by the presence of chronic inflammatory lesions. This condition is one of the most common benign endometrioid proliferations, especially among premenopausal women. Although it is considered benign, endometriosis shares biological characteristics with malignant tumors, including invasion, implantation, metastasis, and recurrence. Abdominal wall endometriosis (AWE) refers to the presence of endometriosis lesions within the abdominal wall, with an extremely low incidence. Malignant transformation of AWE is exceptionally rare.
Case Presentation: A 39-year-old female was admitted to the hospital on May 11, 2023, due to progressive enlargement of an abdominal mass noticed over a period of 4 months. To our knowledge, malignant transformation of abdominal wall endometriosis (AWE) is extremely rare in clinical practice, and cases of endometrioid adenocarcinoma arising from cesarean section-related AWE are even more scarce. Her medical history included surgery for a left lung teratoma 20 years ago and a cesarean section 6 years ago, with no family history of malignant tumor. This report presents a case of AWE subsequent to cesarean section, demonstrating a rare occurrence of malignant transformation into endometrioid adenocarcinoma.
Conclusion: This article emphasizes the need for heightened vigilance regarding the possibility of malignant transformation in AWE patients and suggests a multidisciplinary team (MDT) approach and individualized treatment to improve clinical outcomes. A summary of the malignant transformation associated with endometrioid adenocarcinoma in cases of AWE has been provided to describe the Pathogenesis, Clinical Manifestation, Auxiliary Examination, Pathological Features, Treatment and Follow-up of this rare condition.
Keywords: abdominal wall endometriosis, malignant transformation, endometrioid adenocarcinoma
Introduction
Endometriosis is defined as the presence of endometrial glands and stroma outside the uterine cavity.1 It affects approximately 176 million women worldwide, with an incidence rate of 10–15% among women of childbearing age.1 As a benign disease, endometriosis exhibits characteristics reminiscent of malignant tumors,2 and a small percentage (0.7% to 1%) of endometriosis patients have a risk of malignancy. In 1925, Sampson first described of malignant transformation of ectopic endometrial tissue and proposed three diagnostic criteria for the disease: (1) close association of endometriosis with the tumor; (2) histological consistency with endometrial origin; (3) absence of other primary tumor sites. Subsequently, in 1953, Scott introduced an additional diagnostic criterion: (4) morphologic demonstration of benign endometriosis contiguous with malignant tissue.2,3 However, the clinical application of these criteria has limitations, especially when dealing with small adjacent benign endometriosis lesions or those affected by adjacent malignant tissue destruction. Therefore, in clinical practice, a comprehensive diagnosis should also consider the patient’s history and clinical manifestations. It is worth noting that 80% of endometriosis-associated malignancies (EAM) manifest within the ovaries, while extrinsic EAM primarily occurs in the rectosigmoid colon and rectovaginal septum.4
AWE refers to the presence of endometriosis lesions within the abdominal wall, with an exceedingly low incidence ranging from 0.03% to 1.34%.4,5 AWE includes both primary cases (predominantly located in the umbilicus or groin) and secondary cases (resulting from trauma or surgery, particularly after cesarean section).6 Notably, the malignant transformation of AWE is even rarer, with an incidence of 0.3% to 1.0%, and most cases are documented in case reports.7 Malignant transformation of AWE is rare, with challenging preoperative diagnosis, limited treatment experience, and potentially poor prognosis. In this report, we present a rare case of secondary AWE (subsequent to cesarean section) that underwent malignant transformation into endometrioid adenocarcinoma, aiming to provide valuable clinical reference for the diagnosis and management of this uncommon entity.
Case Presentation
A 39-year-old female was admitted to the hospital on May 11, 2023, due to progressive enlargement of an abdominal mass noticed over a period of 4 months. Her medical history included surgery for a left lung teratoma 20 years ago and a cesarean section 6 years ago, with no family history of malignant tumors. Upon physical examination, a transverse cesarean section scar approximately 10 cm long was observed in the lower abdomen, along with a palpable, immobile, and well-defined mass in the left lower abdominal wall at a distance from the scar. Abdominal ultrasound upon admission revealed a cystic-solid mixed mass measuring 126×112 × 108 mm in lower abdomen, without blood flow signals (Figure 1), however this finding may be influenced thick abdominal fat layer (BMI: 38.97kg/m2). Abdominal enhanced CT scan exhibited a mass measuring 117×112 mm in anterior abdominal wall, suspected to originate from mesenchymal tissue, not ruling out leiomyoma with degeneration or sarcoma, without pelvic abdominal lymph node metastasis (Figure 2). Tumor markers showed serums CA125: 20.0 U/mL, CEA: 1.07 ng/mL, CA199: 3.90 U/mL, CA153: 8.2 U/mL, SCC: 0.330 ng/mL and HE4: 361.92 pmol/L (elevated).
 |
Figure 1 Abdominal ultrasound showing a solid cystic mass in the pelvic cavity ((A) Hyperechoic solid component and adjacent anechoic cystic region; (B) No blood flow signal in mass; M. solid cystic mass; Red arrow indicate solid component of the mass). |
 |
Figure 2 Preoperative contrast-enhanced abdominal computed tomography (CT) scans revealing a soft tissue mass in the anterior pelvic abdominal wall. Radiological findings suggested a mesenchymal-origin lesion, with degenerative leiomyoma or sarcomatous change not ruled out. ((A) Unenhanced axial CT scan of the pelvis; (B) Contrast-enhanced axial CT scan of the pelvis (C) Contrast-enhanced sagittal CT scan of the pelvis; Red arrows indicate the location of the mass, in the abdominal wall layer). |
Subsequently, on May 11, 2023, the patient underwent a combination of laparoscopic exploration, abdominal wall mass resection, and abdominal wall plastic surgery: The tumor was initially identified extraperitoneally in the lower abdomen during laparoscopy. A longitudinal incision was then made in the midline of the lower abdomen, revealing a tumor within the rectus abdominis muscle with distinct borders, solid cystic texture, and dimensions of approximately 15 cm×16 cm (Figure 3). The tumor had invaded the posterior sheath and peritoneum, which were excised using an ultrasonic knife (Preoperative contrast-enhanced abdominal computed tomography (CT) scans revealing a soft tissue mass in the anterior pelvic abdominal wall. Radiological findings suggested a mesenchymal-origin lesion, with degenerative leiomyoma or sarcomatous change not ruled out. (A. Unenhanced axial CT scan of the pelvis; B. Contrast-enhanced axial CT scan of the pelvis C. Contrast-enhanced sagittal CT scan of the pelvis; Red arrows indicate the location of the mass). Following this excision, the peritoneal layer was closed, the anterior peritoneal space was freed, and a biological patch was inserted. The anterior sheath was closed, and the patch was sutured in place, with placement of a negative pressure drainage tube. Postoperative pathology revealed highly differentiated adenocarcinoma with squamous cell features, consistent with endometrioid carcinoma (Figure 4). Immunohistochemistry demonstrated positive staining for CKpan (mostly+), partially positive staining for CK7, PAX-8, Vimentin and CD10, weakly positive staining for CDX-2 in focal areas and approximately 40% positive staining for Ki67. Negative staining was observed for Villin.
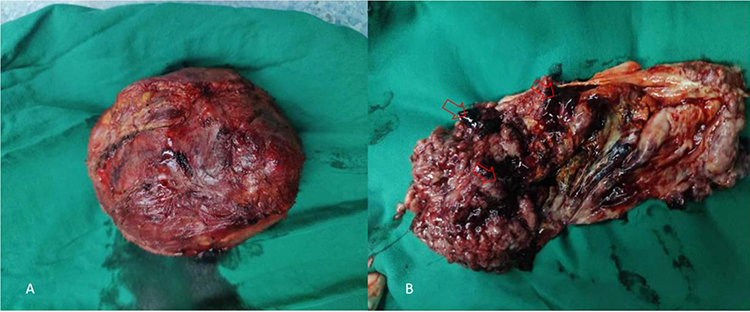 |
Figure 3 Intraoperative macroscopic view of the Anterior abdominal exenteration specimen ((A) gross specimen; (B) The interior of the specimen after incision; Arrows indicate old bleeding). |
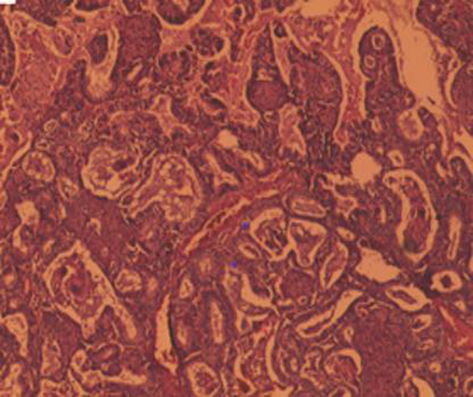 |
Figure 4 Histology of Anterior abdominal exenteration specimen (endometrial glands with surrounding stromal tissues). |
Two weeks post-operation, the patient exhibited poor abdominal wound healing accompanied by purulent secretions. A CT examination revealed a new low-density cystic lesion beneath the skin. Wound debridement and puncture drainage were performed, leading to gradual improvement in the abdominal wound. The patient underwent three courses of adjuvant chemotherapy following surgery. Diagnostic curettage pathology indicated atypical endometrial hyperplasia. Currently, the patient’s condition is stable, hysterectomy with bilateral salpingo-oophorectomy and pelvic and abdominal lymph node dissection are recommended.
Discussion
A study by Liu et al6 found that in 46 patients with malignant transformation of AWE, clear cell carcinoma accounted for 71.7% (33/46) of cases, followed by endometrioid carcinoma at 8.7% (4/46), serous adenocarcinoma at 6.5% (3/46), and other types at 13% (6/46). We conducted an investigation using PUBMED, combining keywords such as “carcinoma”, “adenocarcinoma”, “malignancy”, “endometriosis” and “abdominal wall scar”. The search covered literature from January 1980 to April 2024. We identified a total of seven AWE cases with pathologically confirmed endometrioid adenocarcinoma: five cases of malignant transformation confirmed as endometrioid carcinoma, one case with both endometrioid carcinoma and clear cell carcinoma, and another case combining endometrioid carcinoma and serous carcinoma (Table 1).8–14
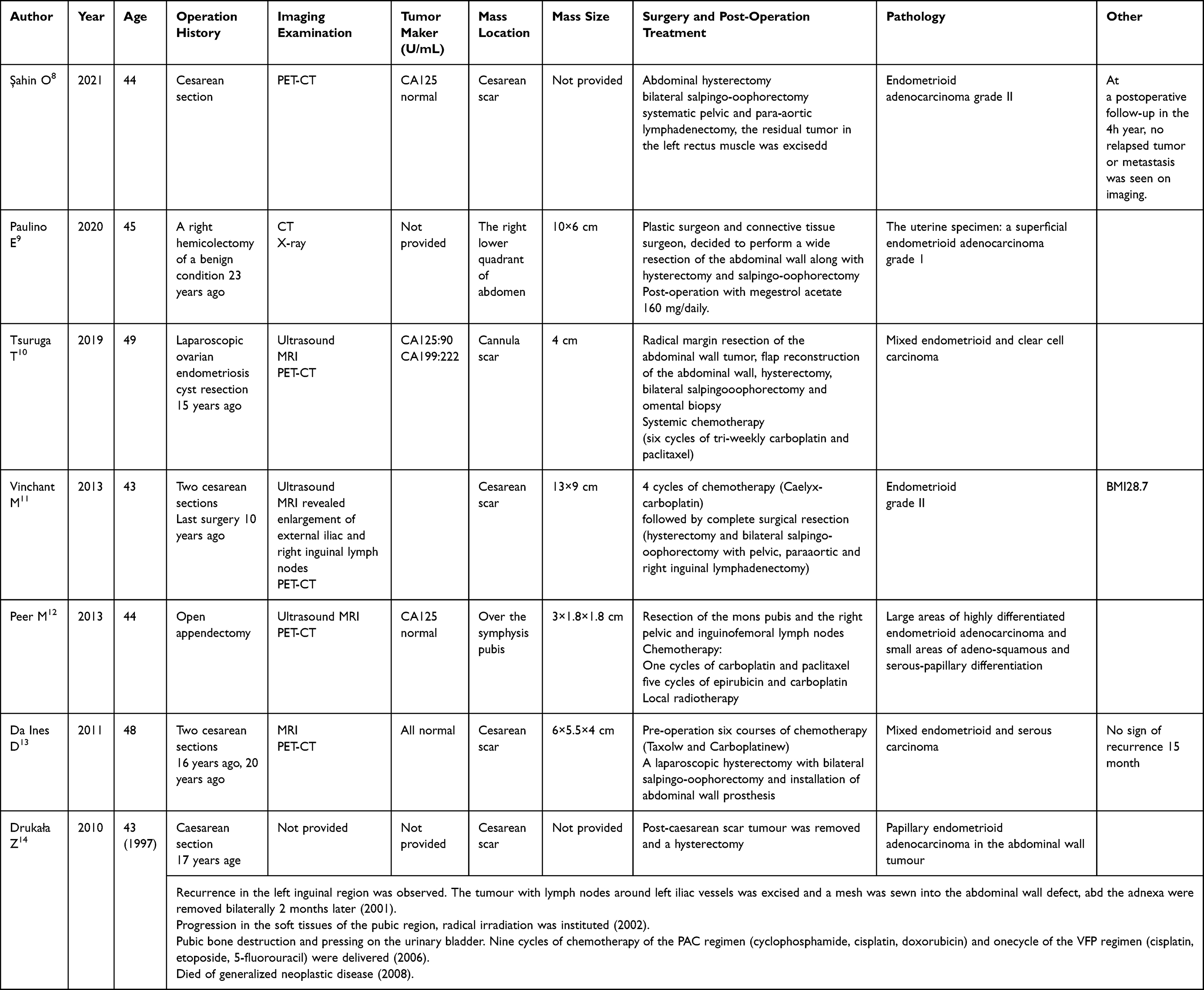 |
Table 1 Case of AWE with Pathologically Confirmed Endometrioid Adenocarcinoma in the Literature |
Pathogenesis
Endometriosis is a complex and multifactorial benign condition, yet its pathophysiological mechanisms remain poorly understood. The main theories on the origin of ectopic endometrium include retrograde menstruation, coelomic metaplasia, lymphatic and vascular metastasis, and stem cell theory. The formation of ectopic lesions is influenced by various factors such as hormone, heredity, immunity and environment. There are two prevailing hypotheses concerning malignant transformation of endometriosis: firstly, typical endometriosis serves as a precancerous state with Endometriosis-Associated Malignancy (EAM) evolving from atypical endometriosis; secondly, endometriosis and EAM share a comparable “tissue environment”. Indeed, the coexistence of benign lesions and malignant tumor tissues in certain instances supports the latter point.
Malignant transformation of AWE, particularly endometrioid adenocarcinoma, is rare, The molecular mechanism of malignant transformation of endometriosis is currently based on studies of endometriosis associated ovarian carcinoma (EAOC). Studies suggest a correlation between genetic mutations and the pathogenesis of endometriosis and EAM: (1) PTEN gene: Loss of heterozygosity (LOH) in the tumor suppressor gene PTEN, leading to the activation of the downstream PI3K/AKT/mTOR signaling pathway, is considered a significant mechanism contributing to the onset and progression of endometriosis. Sato et al15 additionally confirmed PTEN mutation in 42.15% of endometriosis-associated ovarian endometrioid adenocarcinomas and 27.3% of endometriosis-associated ovarian clear cell carcinomas; (2) ARID1A gene: Wiegand et al16 reported ARID1A gene mutations in 30% of endometriosis-associated ovarian endometrioid adenocarcinomas and 46% of endometriosis-associated ovarian clear cell carcinomas. Furthermore, mutations were observed in atypical endometriosis proximal to the tumor, yet absent in distant endometriosis. Therefore, ARID1A mutation is regarded as an early event in malignant transformation; (3) Changes in CTNNB1 and RAS genes also play a significant role in the malignancy of endometriosis.2
Clinical Manifestation and Auxiliary Examination
Patients with AWE typically present with complaints of discovering nodules or masses on the abdominal wall, often accompanied by periodic or irregular pain. Among imaging methods, ultrasound is the most commonly used in clinical settings due to its convenience and cost-effectiveness. Ultrasound can visualize masses within the soft tissue layer of the abdominal wall, displaying either isoechoic or hyperechoic characteristics, while blood flow signals can be detected by color doppler ultrasonography. MRI provides high-resolution soft tissue images, enabling observation of irregular masses in the abdominal wall that extend into layers such as adipose tissue, fascia, muscle, or peritoneum. CT imaging reveals irregular masses in the abdominal wall with uneven enhancement. Additionally, CT scans can detect metastases in various regions such as the groin, pelvis, abdominal paracolic gutter, cardiophrenic angle, mediastinum, and upper and lower clavicular lymph nodes, assisting in determination the presence of distant metastasis. Elevated CA125 levels exceeding 200 U/mL are typically observed in cases of EAM, while in malignant transformation of AWE, CA125 levels are usually normal or only slightly elevated. Thus, CA125 is of limited value in diagnosing malignant transformation of AWE. Therefore, CA125 levels are not as valuable in diagnosing malignant transformation of AWE.2,6 In this case, because CT scan exhibited a mass suspected to originate from mesenchymal tissue, and CA125 is normal, We did not diagnose malignant transformation of AWF preoperatively. We found that in the reported cases, puncture biopsy and histopathological examination is helpful to make a definite diagnosis.
Pathological Features
The predominant pathological pattern of EAOC is typically endometrioid adenocarcinoma. However, clear cell carcinoma is the most frequently reported type of malignant transformation of AWE. This is followed by endometrioid adenocarcinoma, serous carcinoma, and other relatively rare mixed cancers. The use of immunohistochemical staining combined with pathological features can improve the accuracy of diagnosing endometrioid adenocarcinoma. Notably, typical endometrioid morphology can be seen at low magnification, characterized by densely packed endometrioid glands with sparse interstitium. At medium magnification, columnar cells are arranged around the endometrioid glands, while at high magnification, pseudostratified nuclei exhibit no more than moderate atypia, the cytoplasm appears small, and the nuclei are oval-shaped.17 The immunohistochemical analysis, in line with the literature’s findings, provides additional support for the diagnosis of endometrioid adenocarcinoma in this case.18,19
Treatment and Post-Treatment Monitoring
There is no consensus on the optimal surgical and postoperative approach. However, the current common treatment for malignant transformation of AWE is wide resection. Most studiers suggest that abdominal wall tumor resection should be accompanied by hysterectomy and bilateral adnexectomy, as well as inguinal lymph node dissection. Adjuvant chemotherapy and radiotherapy are administered post-surgery in some cases, in this case three cycles of adjuvant chemotherapy were also administered. A study of 33 cases reported a high recurrence rate within 2 years and poor prognosis for malignant transformation of AWE. Specifically, 17 cases experienced recurrence or progression within 2 years, while 3 cases showed recurrence or progression after 2 years.6
Conclusion
We suggest the following: (1) It is crucial to implement preventive measures, such as reducing cesarean section rates and meticulous incision protection, to minimize iatrogenic endometrial implantation. (2) The assessment of abdominal wall masses requires integration of clinical and radiologic information. Biopsy and histopathology are required to confirm the diagnosis. (3) Although there is no consensus on the optimal surgical approach, for patients not desiring fertility preservation, upon confirmation of malignant transformation of AWE, abdominal wall mass resection, prophylactic hysterectomy, bilateral adnexectomy, and pelvic and abdominal lymph node dissection should be considered.
Ethic Approval and Consent to Participate
Before each operation, written informed consent was obtained from each patient that gave permission. Ethics committee approval has won. As this study was a case report, only with ultrasound images, CT images, macroscopic images and microscopic image of specimen, there is no concern about identifying information in the case.
Consent for Publication
All authors consent to participate and publication of this work.
Acknowledgments
We are very grateful to everyone who contributed to this report and related funds for their support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was sponsored by Tianjin Health Research Project (Grant No. TJWJ2024MS042), Scientific Research Program of Hebei Administration of Traditional Chinese Medicine (Grant No. T2025038) and the Scientific Research Program of Tianjin Municipal Education Commission (Grant No.2024KJ246) to Ming Wei and Xingzhou Zhang.
Disclosure
The authors declare no competing interests in this work.
References
1. Zondervan KT, Becker CM, Koga K, et al. Endometriosis. Nat Rev Dis Primers. 2018;4(1):9. doi:10.1038/s41572-018-0008-5
2. Alkatout İ, Meinhold-Heerlein I, Keckstein J, et al. Endometriosis: a concise practical guide to current diagnosis and treatment. Endo Press. 2017. doi:10.4274/jtgga.2018.0026
3. Scott RB. Malignant changes in endometriosis. Obstet Gynecol. 1953;2:283–289. doi:10.1079/PNS19530066
4. Allen SE, Rindos NB, Mansuria S. Abdominal wall endometriosis: an update in diagnosis, perioperative considerations and management. Curr Opin Obstet Gynecol. 2021;33(4):288–295. doi:10.1097/GCO.0000000000000714
5. Khan Z, Zanfagnin V, El-Nashar SA, et al. Risk factors, clinical presentation, and outcomes for abdominal wall endometriosis. J Minim Invasive Gynecol. 2017;24(3):478–484. doi:10.1016/j.jmig.2017.01.005
6. Liu G, Wang Y, Chen Y, et al. Malignant transformation of abdominal wall endometriosis: a systematic review of the epidemiology, diagnosis, treatment, and outcomes. Eur J Obstet Gynecol Reprod Biol. 2021;264:363–367. doi:10.1016/j.ejogrb.2021.08.006
7. Miller DM, Schouls JJ, Ehlen TG. Clear cell carcinoma arising in extragonadal endometriosis in a caesarean section scar during pregnancy. Gynecologic Oncol. 1998;70(1):127–130. doi:10.1006/gyno.1998.4989
8. Şahin O, Tokgözoğlu N, Taşcı T. Localized endometrioid cancer in the abdominal wall with synchronous early-stage endometrial cancer. Turk J Obstet Gynecol. 2021;18(3):264–266. doi:10.4274/tjod.galenos.2021.85530
9. Paulino E, de Melo AC, da Silva VF. Endometrioid carcinoma arising from an endometriosis-associated abdominal wall scar. Am J Case Rep. 2020;21:e922973. doi:10.12659/AJCR.922973
10. Tsuruga T, Hirata T, Akiyama I, et al. Mixed endometrioid and clear cell carcinoma arising from laparoscopic trocar site endometriosis. J Obstet Gynaecol Res. 2019;45(8):1613–1618. doi:10.1111/jog.14014
11. Vinchant M, Poncelet C, Ziol M, et al. Malignant transformation of abdominal wall endometriosis: case report and literature review. Tumori. 2013;99(2):e49–54. doi:10.1177/030089161309900228
12. Peer M, Fellner W, Seeber BE, et al. Endometroid carcinoma developing in endometriosis over the symphysis pubis. Gynecol Oncol Case Rep. 2013;10(6):45–46. doi:10.1016/j.gynor.2013.08.001
13. Da Ines D, Bourdel N, Charpy C, et al. Mixed endometrioid and serous carcinoma developing in abdominal wall endometriosis following Cesarean section. Acta Radiol. 2011;52(5):587–590. doi:10.1258/ar.2011.100483
14. Drukała Z, Ciborowska-Zielińska B, Kubrak J, et al. Outcome of a multimodal therapy of a recurrent adenocarcinoma arising from Caesarean section scar endometriosis-A case report. Rep Pract Oncol Radiother. 2010;15(3):75–77. doi:10.1016/j.rpor.2010.03.002
15. Sato N, Tsunoda H, Nishida M, et al. Loss of heterozygosity on 10q23.3 and mutation of the tumor suppressor gene PTEN in benign endometrial cyst of the ovary: possible sequence progression from benign endometrial cyst to endometrioid carcinoma and clear cell carcinoma of the ovary. Cancer Res. 2000;60(24):7052–7056.
16. Wiegand KC, Shah SP, Al-Agha OM, et al. ARID1A mutations in endometriosis-associated ovarian carcinomas. N Engl J Med. 2010;363(16):1532–1543. doi:10.1056/NEJMoa1008433
17. González-Martín A, Harter P, Leary A, et al. Newly diagnosed and relapsed epithelial ovarian cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2023;34(10):833–848. doi:10.1016/j.annonc.2023.07.011
18. Lucas E, Carrick KS. Low grade endometrial endometrioid adenocarcinoma: a review and update with emphasis on morphologic variants, mimics, immunohistochemical and molecular features. Semin Diagn Pathol. 2022;39(3):159–175. doi:10.1053/j.semdp.2022.02.002
19. Song H, Lee S, Kim MJ, et al. Abdominal wall mass suspected of endometriosis: clinical and pathologic features. Obstet Gynecol Sci. 2020;63(3):357–362. doi:10.5468/ogs.2020.63.3.357
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.