Back to Journals » International Journal of Women's Health » Volume 17
Malignant Peritoneal Cytology Predicts Poor Prognosis and Differential Adjuvant Therapy Benefit in Endometrioid Endometrial Carcinoma: A SEER-Based Propensity Score-Matched Analysis
Authors Yang H ![]()
Received 16 April 2025
Accepted for publication 7 August 2025
Published 21 August 2025 Volume 2025:17 Pages 2637—2650
DOI https://doi.org/10.2147/IJWH.S534822
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Hua Yang
Department of Gynecology, The Fifth Affiliated Hospital of Sun Yat-sen University, Zhuhai, 519000, People’s Republic of China
Correspondence: Hua Yang, Department of Gynecology, The Fifth Affiliated Hospital of Sun Yat-sen University, Zhuhai, 519000, People’s Republic of China, Email [email protected]
Background: The prognostic significance of malignant peritoneal cytology (PC) in endometrioid endometrial carcinoma (EC) and its clinical implications for adjuvant therapy selection remain controversial.
Methods: This retrospective cohort study analyzed 9631 endometrioid EC patients from Surveillance, Epidemiology, and End Results (SEER) Program data (2010– 2017). Prognostic determinants of overall survival (OS) were identified through Cox regression. Propensity score matching (PSM) generated balanced cohorts: 826 malignant PC, 148 atypical/suspicious PC, and 974 negative PC cases. Survival distributions were compared using Kaplan-Meier analysis.
Results: Univariable analysis identified significant OS associations with age, histopathological grade, tumor stage, and PC status (all p < 0.05). Multivariable analysis confirmed malignant PC as an independent prognostic factor. Post-PSM: Malignant PC subgroup showed significantly reduced OS vs others (p < 0.001). Stage-specific effects in malignant PC subgroup: Radiation improved OS only in regional disease (p = 0.016). Systemic therapy reduced OS in all-stage malignant PC (p = 0.022). Atypical/suspicious PC subgroup: No survival benefit from radiation (p = 0.71) or systemic therapy (p = 0.38).
Conclusion: Malignant PC independently predicts poor prognosis in endometrioid EC but requires cautious interpretation in therapeutic decision-making due to its differential adjuvant therapy effects. PC status alone cannot guide risk stratification; treatment decisions should integrate stage-specific efficacy data. Prospective validation is imperative.
Keywords: endometrioid endometrial carcinoma, malignant peritoneal cytology, propensity score matching, prognostic factor, overall survival
Introduction
Endometrial carcinoma (EC) has emerged as the most prevalent gynecologic malignancy in developed countries, demonstrating a paradoxical epidemiological trend of increasing incidence alongside improving overall survival (OS) rates - a phenomenon largely attributable to enhanced early detection protocols and evolution in therapeutic approaches.1 Endometrioid EC constitutes the predominant histological subtype, accounting for approximately 75–80% of all EC cases according to population-based registry data.2,3 Global epidemiological patterns reveal marked geographical heterogeneity in EC incidence and mortality rates, mediated through complex interactions between genetic susceptibility profiles (eg, Lynch syndrome), metabolic determinants (particularly obesity-driven estrogen exposure), and disparities in healthcare resource allocation.4 Within the United States healthcare landscape, the American Cancer Society’s 2023 surveillance report projects 66,200 new EC diagnoses alongside 13,030 disease-related deaths, highlighting persistent oncologic challenges despite diagnostic advancements.5 The clinical trajectory of EC is notably characterized by frequent diagnosis at localized stages (Stage I–II disease in >70% of cases), a testament to the success of current screening paradigms employing vaginal bleeding symptom awareness and ultrasonographic endometrial surveillance.6,7 For patients presenting with clinically apparent early-stage disease, contemporary management guidelines mandate comprehensive surgical staging through total hysterectomy with bilateral salpingo-oophorectomy, supplemented by strategic lymphadenectomy in select high-risk populations.8 Critical to postoperative risk stratification, histomorphological assessment of surgical specimens enables identification of recurrence-predictive parameters including: depth of myometrial invasion, cervical stromal compromise, adnexal/uterine serosal involvement, lymphovascular space invasion, emerging molecular classifiers (eg, TCGA molecular subgroups).9,10 These clinicopathological variables are systematically incorporated into the revised 2023 FIGO staging system, forming the foundation for evidence-based adjuvant therapy algorithms tailored to individualized recurrence risk profiles.11 This multidimensional risk assessment paradigm underscores the indispensable role of precision pathology in optimizing therapeutic decision-making and improving oncologic outcomes for EC patients.
Malignant peritoneal cytology (PC), defined as the presence of exfoliated neoplastic cells in peritoneal washings, persists as a clinically contentious element in endometrioid EC management. Its historical designation as a stage IIIA criterion in FIGO staging (1988–2009) contrasts with exclusion from contemporary systems, reflecting persistent uncertainty regarding independent prognostic value—a controversy perpetuated by decades of conflicting evidence hindering clinical consensus. This uncertainty directly translates to dilemmas when malignant PC is detected: clinicians must weigh escalating adjuvant therapy against overtreatment toxicity or maintaining standard regimens risking under-treatment of aggressive disease.
Three unresolved questions sustain this equipoise: whether malignant PC retains prognostic independence after comprehensive confounder adjustment; how it modulates adjuvant therapy efficacy; and which PC subgroups benefit from tailored strategies. Contradictory reports exacerbate the ambiguity, with some studies12–14 documenting significant survival reduction while others15,16 demonstrate null effects after multivariate analysis. Notably, major societies (ACOG/ESGO)17 continue mandating routine cytologic evaluation despite evolving staging paradigms, highlighting the urgent need for definitive evidence.
To resolve these evidence gaps, this investigation harnesses the epidemiological breadth of the Surveillance, Epidemiology, and End Results (SEER) Program (2010–2017 cohort) to conduct a rigorous reappraisal. Through propensity score-matched (PSM) survival analysis and treatment interaction modeling, we quantify malignant PC-associated survival decrements, delineate stage-specific therapeutic responses to adjuvant modalities, and establish evidence thresholds for cytology-integrated risk stratification. This approach directly addresses methodological limitations in prior studies—including heterogeneous designs, inadequate adjustment for treatment-era effects, and insufficient power to detect critical interactions—by leveraging population-level analytics for robust conclusions.
Materials and Methods
Data Source and Study Design
This registry-based retrospective cohort study leveraged data from the SEER Program (2010–2017 release), a nationally representative cancer surveillance system covering ~35% of the US population with 97% case ascertainment completeness.18 The SEER database employs standardized protocols for case identification, centralized quality assurance, and NCI-certified abstraction procedures to ensure data integrity and longitudinal validity.
Ethical approval exemption was granted by the Institutional Review Board of The Fifth Affiliated Hospital of Sun Yat-sen University under China’s Measures for Ethical Review.
Cohort Selection
The study population was derived through rigorous application of the following selection criteria:
Inclusion Criteria
- Histologically confirmed endometrioid endometrial carcinoma (EC; WHO 2020 Classification).
- Primary tumor site confined to uterine corpus (ICD-O-3 topography code C54.1).
- Morphologically verified endometrioid adenocarcinoma (ICD-O-3 histology code 8380/3).
- Complete surgical staging documentation (2010–2017).
- Available peritoneal cytopathology reports.
- Comprehensive demographic, therapeutic, and survival data.
Exclusion Criteria
- Non-endometrioid histologic subtypes (serous, clear cell, carcinosarcoma, etc).
- Non-corporeal uterine malignancies (cervical [C53.x] or unspecified uterine [C55.x] origin).
- Secondary metastatic involvement of endometrium.
- Synchronous primary malignancies.
- Missing essential prognostic variables (clinical stage, histologic grade, treatment modality).
Exposure Allocation
Peritoneal cytology/washing results were stratified into three clinically relevant categories based on standardized cytopathology reporting criteria:
Malignant (positive for malignancy): defined as cytologically confirmed adenocarcinoma cells with: cellular features of malignancy (high nuclear-cytoplasmic ratio, nuclear pleomorphism), and architectural patterns incompatible with mesothelial origin.
Atypical and/or suspicious: atypical cells (mild nuclear atypia without definitive malignant criteria), or suspicious for malignancy (incomplete diagnostic features warranting pathologist annotation).
Negative for malignancy: benign findings (normal mesothelial cells, inflammatory cells), or technical inadequacy (insufficient cellularity, obscuring blood).
Clinical Variables
Demographic and Disease Characteristics
Age: categorized into three groups: <50 years, 50–75 years, and ≥75 years.
Year of diagnosis: grouped into two periods: 2010–2013 and 2014–2017.
Race/ethnicity: classified into four categories: American Indian/Alaska Native, Asian or Pacific Islander, Black, and White.
Histopathological grade: divided into four grades: well differentiated (Grade I), moderately differentiated (Grade II), poorly differentiated (Grade III), and undifferentiated/anaplastic (Grade IV).
Clinical stage (spread extent): grouped into three stages: local, regional, and distant.
Localized stage: tumor confined to the primary organ (endometrium), no extension beyond the uterine corpus, and excludes microscopic/minimal myometrial invasion (classified under pathologic staging).
Regional stage: direct extension to adjacent structures (cervix, parametria, adnexae, or pelvic peritoneum); or metastasis to regional lymph nodes (pelvic/para-aortic), includes contiguous spread but excludes distant organ involvement.
Distant stage: discontinuous metastasis beyond the pelvis, involvement of non-regional lymph nodes (eg, supraclavicular), distant organ metastases (eg, lung, liver, bone); malignant pleural/peritoneal effusions unrelated to direct extension.
Treatment Details
Types of lymph node assessment: categorized into two levels: 1 to 3 regional lymph nodes removed/biopsy or aspiration of regional lymph node/sentinel lymph node biopsy, and 4 or more regional lymph nodes removed/sentinel node biopsy and lymph nodes removed at different times/sentinel node biopsy and lymph nodes removed at the same/unstated time.
Radiation: divided into two groups: without radiation, and with radiation (before and/or after Surgery and/or intraoperative radiation).
Systemic therapy: grouped into two categories: without systemic therapy, and with systemic therapy (before and/or after surgery).
Para-aortic lymph nodes examined: classified into two groups: with 1–70 para-aortic lymph nodes removed or para-aortic nodes examined, number unknown, and no para-aortic nodes examined or no para-aortic lymph nodes removed, but aspiration or core biopsy only.
Pelvic lymph nodes examined: classified into two groups: with 1–90 pelvic lymph nodes removed or pelvic nodes examined, number unknown, and no pelvic nodes examined or no pelvic lymph nodes removed, but aspiration or core biopsy only.
Follow-Up
Survival Time: the length of time from the diagnosis until death or the end of the study period.
Survival status: includes four states: alive, dead of other cause, dead (attributable to endometroid EC), and dead of missing/unknown cause.
Outcome Measures
OS was the primary outcome measure in this study, defined as the time interval between the diagnosis of endometroid EC and death from any cause. Patients who were still alive at their last follow-up visit were censored for survival analysis. The SEER program ensures near-universal updates for survival status and externally links to the National Death Index for validation, enhancing the accuracy and reliability of the data.
Statistical Approach
The statistical analysis was conducted in three main steps to assess the impact of various factors on OS and the benefits of adjuvant therapy for endometroid EC patients with malignant PC.
Step 1: identifying independent risk factors for OS
The first step involved identifying independent risk factors associated with OS through sequential analytical approaches. Initially, univariate Cox proportional hazards models screened clinical variables for preliminary associations with OS. Subsequently, multivariate Cox regression adjusted for potential confounders to verify independent predictors. To address selection bias and residual confounding, PSM was implemented, incorporating the following covariates: age at diagnosis, diagnosis year, race/ethnicity, histopathological grade, clinical stage, lymph node evaluation strategy, para-aortic/pelvic lymph node dissection extent, and systemic therapy/radiation administration. Matching employed a 1:1 nearest-neighbor algorithm with a caliper width of 0.05, performed strictly after excluding cases with missing variables. Finally, additional univariate and multivariate Cox analyses were conducted on the matched cohort to confirm the robustness of identified risk factors.
Step 2: Assessing OS related to malignant / atypical / suspicious PC
The second step focused on evaluating the relationship between malignant / atypical / suspicious PC and OS. K-M plots were utilized to visually illustrate the correlation between peritoneal cytology/washing status and OS.
Step 3: Evaluating the benefit of adjuvant therapy
The final step assessed the benefit of adjuvant therapy for endometroid EC patients with malignant PC. K-M plots were again used to visually demonstrate the correlation between adjuvant chemotherapy or radiation (with versus without) and OS. A sensitivity analysis based on clinical stage was performed to evaluate the robustness of the study findings.
Missing Data Handling
Missing data handling followed a complete-case analysis approach for variables exceeding 5% missingness. Sensitivity analysis comparing complete-case analysis with multiple imputation (chained equations, 20 imputations) demonstrated clinically negligible variation in OS estimates (HR < 5% for all covariates).
Atypical/Suspicious PC Subgroup Retention
The atypical/suspicious PC category was retained as a distinct analytical subgroup for two clinical reasons:
It represents a clinically relevant entity frequently encountered in practice, where pathologists document uncertainty (eg “atypical cells of undetermined significance”).
Current guidelines (ESGO/ACOG) recommend differential management for this subgroup versus definitively malignant/negative casesNo sensitivity analyses combining or excluding this subgroup were performed, as doing so would obscure its unique clinical implications.
SEER Data Limitations
Acknowledged limitations include:
- Absence of recurrence-specific endpoints;
- Lack of chemotherapy details (agents, cycles, dose intensity);
- Radiotherapy techniques unspecified;
- Molecular biomarkers unavailable.
Statistical analyses were conducted using two-sided hypotheses, with a p-value of less than 0.05 considered statistically significant. All analyses were performed using R version 3.5.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
From a database encompassing 153,302 women, we identified 9632 cases of endometroid EC with comprehensive records on demographics, disease characteristics, treatment details, follow-up, and outcomes. The age distribution among these patients was as follows: 1129 (11.72%) were under 50 years old, 7359 (76.41%) ranged from 50 to 75 years, and 1143 (11.87%) were aged 75 years or older. Regarding the histopathological grade, 4423 (45.92%) were classified as well-differentiated (Grade I), 3475 (36.08%) as moderately differentiated (Grade II), 1470 (15.26%) as poorly differentiated (Grade III), and 263 (2.73%) as undifferentiated/anaplastic (Grade IV). In terms of tumor stage, 7110 (73.82%) patients had localized disease, 2306 (23.92%) presented with regional spread, and 215 (2.23%) had distant metastasis. Malignant PC was documented in 826 (8.58%) endometroid EC, and 148 (1.54%) with atypical and/or suspicious PC. A detailed summary of the baseline characteristics for this endometroid EC cohort is provided in Table 1.
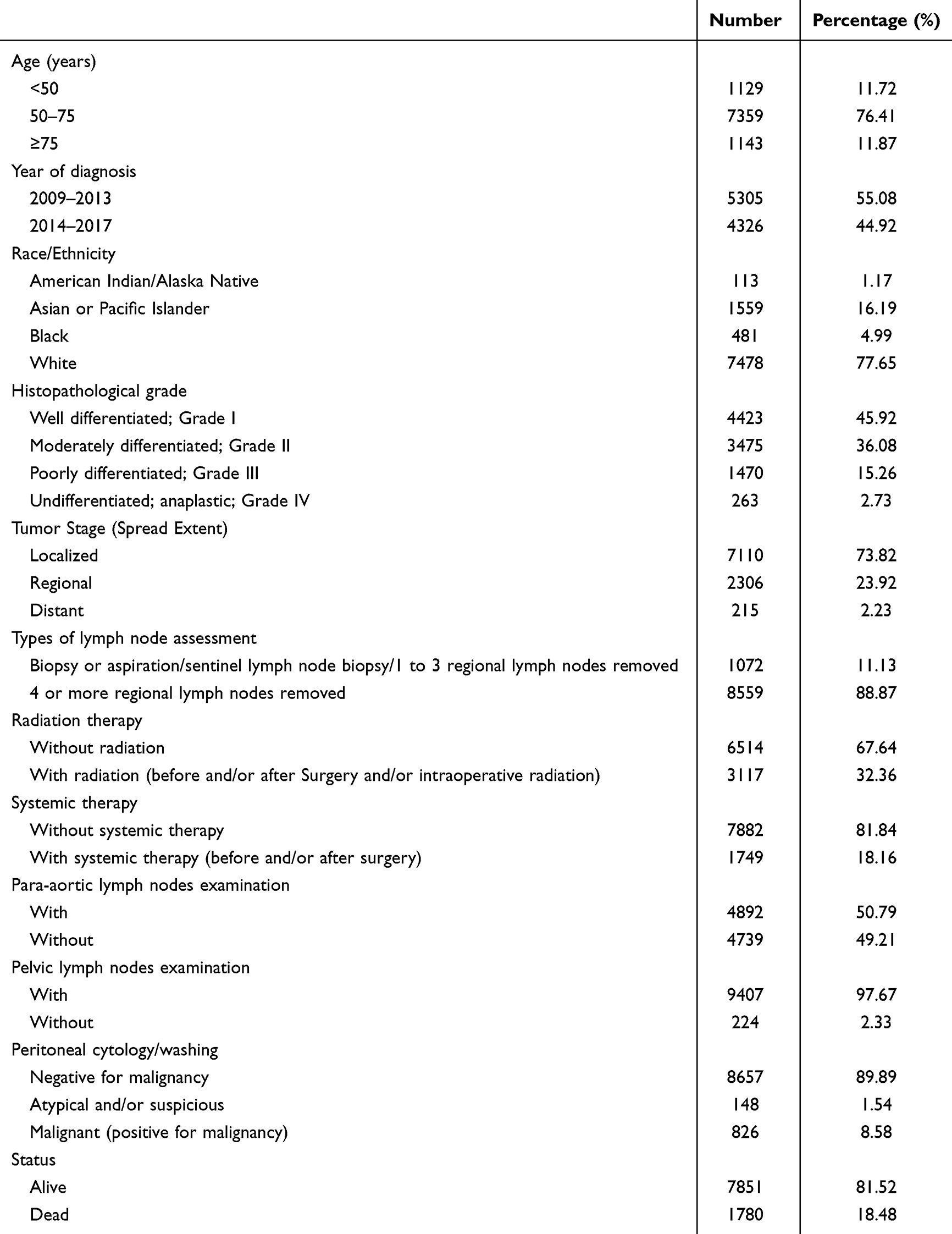 |
Table 1 Baseline Characteristics of the Included Endometrioid Endometrial Cancer |
The univariate Cox proportional hazards model revealed that age, year of diagnosis, race/ethnicity, histopathological grade, tumor stage, types of lymph node assessment, systemic therapy administration, para-aortic/pelvic lymph node examination, and PC status were significantly correlated with OS of endometroid EC (Table 2). The K-M plots displayed age < 50 group, year of diagnosis at 2014–2017, Asian or Pacific islander or White, well differentiated group, local stage, systemic lymph node removed group, systemic therapy administration, with para-aortic lymph nodes examination, with pelvic lymph nodes examination and negative PC had better prognosis (Figure 1A–K). Upon multivariate adjustment, these variables, except with pelvic lymph nodes examination, maintained their independence as prognostic indicators for OS (Table 2). Notably, the 5-year OS for endometroid EC with negative PC was 46.8% (43.0–50.9%), exhibited a markedly superior 5-year OS compared to those with atypical and/or suspicious PC (44.6% (29.9–66.5%), p =0.0054) and malignant PC (30.8% (29.9–41.4%), p <2e-16) (Figure 1A).
 |
Table 2 Univariate and Multivariate Cox Analysis of Overall Survival in the Included Endometrioid Endometrial Cancer |
 |
Figure 1 Kaplan-Meier (K-M) plots of overall survival (OS) in the included endometrioid endometrial cancer. (A) K-M plot grouped by age. (B) K-M plot grouped by year of diagnosis. (C) K-M plot grouped by race/ethnicity. (D) K-M plot grouped by histopathological grade. (E) K-M plot grouped by tumor stage. (F) K-M plot grouped by types of lymph node assessment. (G) K-M plot grouped by radiation. (H) K-M plot grouped by systemic therapy. (I) K-M plot grouped by para-aortic lymph nodes examination. (J) K-M plot grouped by pelvic lymph nodes examination. (K) K-M plot grouped by Peritoneal cytology/washing. |
To further scrutinize the prognostic impact of malignant PC, PSM was employed to balance clinical characteristics, 974 endometroid EC with negative PC, 148 with atypical and/or suspicious PC and 826 malignant PC were enrolled. Reanalysis through univariate Cox proportional hazards model revealed that age, histopathological grade, tumor stage, types of lymph node assessment, systemic therapy administration, para-aortic/pelvic lymph node examination, and PC status were significantly correlated with OS of endometroid EC (Table 3). The K-M plots displayed age < 50 group, well differentiated group, local stage, systemic lymph node removed group, systemic therapy administration, with para-aortic lymph nodes examination, with pelvic lymph nodes examination and negative PC had better prognosis (Figure 2A–K). Upon multivariate adjustment, these variables, except with pelvic lymph nodes examination and PC status, maintained their independence as prognostic indicators for OS (Table 3). Consistent with prior findings, the 5-year OS for endometroid EC with negative PC was 60.5% (50.8–70.1%), exhibited a markedly superior 5-year OS compared to those with atypical and/or suspicious PC (p =0.0086) and malignant PC (p=3 8.8e-07) (Figure 2A), underscoring its significance as a negative prognostic factor in endometroid EC.
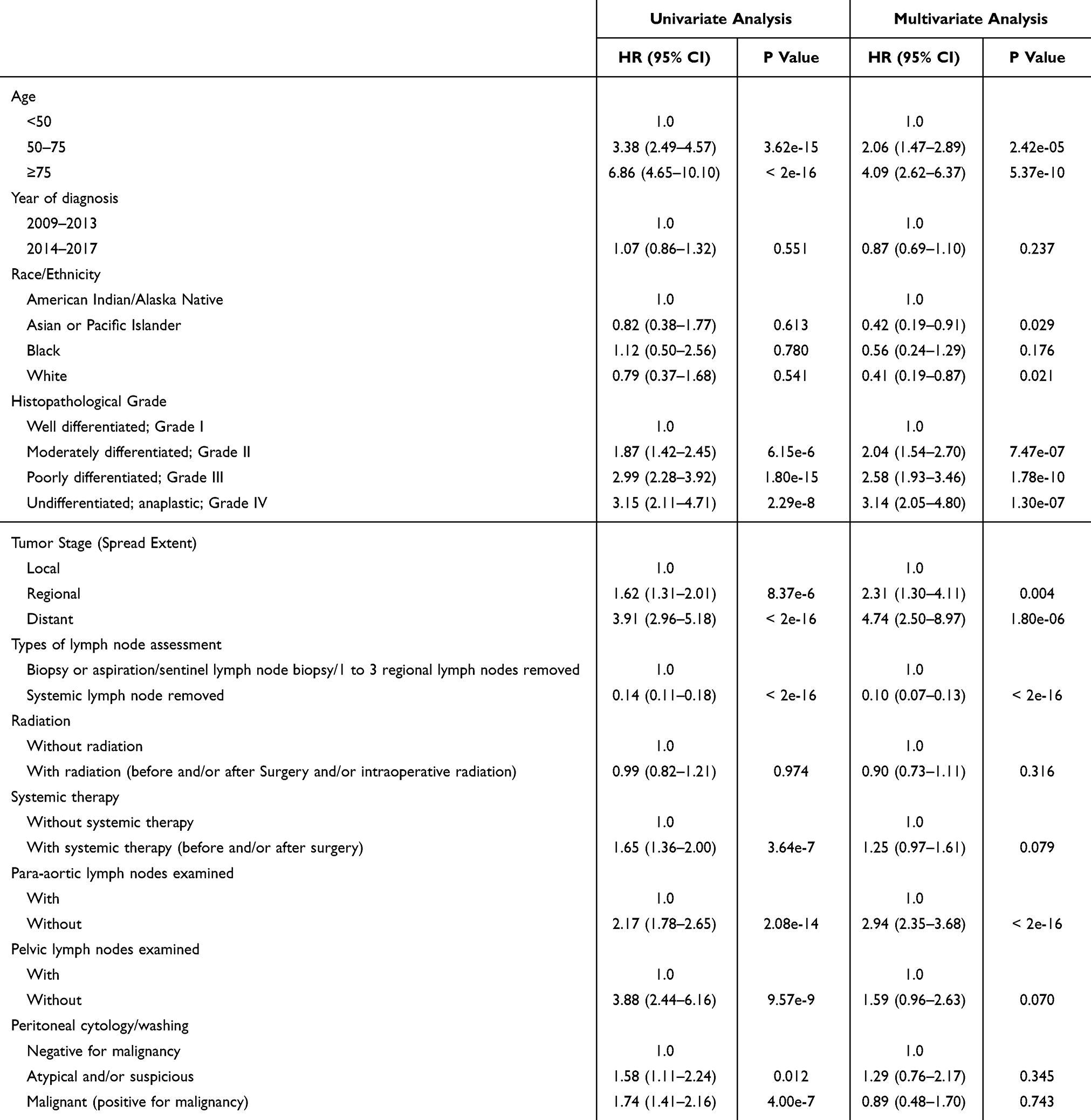 |
Table 3 Univariate and Multivariate Cox Analysis of Overall Survival in the Endometrioid EC Population Selected Through Propensity Score Matching |
 |
Figure 2 Kaplan-Meier (K-M) plots of overall survival (OS) in the endometrioid endometrial cancer selected through propensity score matching. (A) K-M plot grouped by age. (B) K-M plot grouped by year of diagnosis. (C) K-M plot grouped by race/ethnicity. (D) K-M plot grouped by histopathological grade. (E) K-M plot grouped by tumor stage. (F) K-M plot grouped by types of lymph node assessment. (G) K-M plot grouped by radiation. (H) K-M plot grouped by systemic therapy. (I) K-M plot grouped by para-aortic lymph nodes examination. (J) K-M plot grouped by pelvic lymph nodes examination. (K) K-M plot grouped by Peritoneal cytology/washing. |
In assessing the influence of adjuvant therapies on endometrioid EC patients with differing PC statuses, subgroup analyses revealed distinct survival patterns. Kaplan-Meier analysis demonstrated that adjuvant radiation conferred significant OS benefits in the malignant PC group (p = 0.002; Figure 3A). Paradoxically, adjuvant systemic therapy was associated with significantly reduced OS in the same group (p = 0.022; Figure 3B). Conversely, neither adjuvant radiation (p = 0.71; Figure 3C) nor systemic therapy (p = 0.38; Figure 3D) provided OS benefits in the atypical/suspicious PC group. These findings suggest that while adjuvant radiation may improve OS in malignant PC endometrioid EC, systemic therapy appears detrimental.
 |
Figure 3 Subgroup analysis of Kaplan-Meier (K-M) plots of overall survival (OS) during endometrioid endometrial cancer with malignant or atypical peritoneal cytology. (A) K-M plot grouped by radiation during malignant PC cohort; (B) K-M plot grouped by systemic therapy during malignant PC cohort; (C) K-M plot grouped by radiation during atypical and/or suspicious PC cohort; (D) K-M plot grouped by systemic therapy during atypical and/or suspicious PC cohort; (E) K-M plot grouped by radiation during localized stage of malignant PC cohort; (F) K-M plot grouped by systemic therapy during localized stage of malignant PC cohort; (G) K-M plot grouped by radiation during regional stage of malignant PC cohort; (H) K-M plot grouped by systemic therapy during regional stage of malignant PC cohort; (I) K-M plot grouped by radiation during distant stage of malignant PC cohort; (J) K-M plot grouped by systemic therapy during distant stage of malignant PC cohort. |
Further stage-stratified analysis of malignant PC patients revealed differential effects:
Localized Stage: No significant OS difference with adjuvant radiation (p = 0.48; Figure 3E) or systemic therapy (p = 0.58; Figure 3F)
Regional Stage: Adjuvant radiation conferred significant OS advantage (p = 0.016; Figure 3G), whereas systemic therapy showed no benefit (p = 0.41; Figure 3H)
Distant Stage: Neither radiation (p = 0.73; Figure 3I) nor systemic therapy (p = 0.81; Figure 3J) improved OS
These results indicate that adjuvant radiation’s OS benefit is confined to regional-stage disease, with no efficacy in localized or distant stages. Systemic therapy demonstrated no survival advantage at any stage. Consequently, PC status alone cannot reliably guide adjuvant therapy decisions or risk stratification.
Discussion
Endometroid EC is frequently diagnosed at an early, localized stage due to symptomatic presentations like abnormal uterine bleeding, coupled with its typically slower biological progression. The cornerstone of endometroid EC management across all histological variants involves comprehensive surgical staging. This encompasses meticulous exploration of both the pelvic and abdominal regions, biopsy of any suspect lesions, acquisition of peritoneal fluid or washings for cytology, and a total hysterectomy accompanied by bilateral salpingo-oophorectomy. Additionally, pelvic and para-aortic lymph node dissection is performed to assess metastatic spread. Post-surgical risk stratification, which informs subsequent adjuvant therapy decisions, is predicated on a constellation of prognostic factors integrated into the cancer staging system. Key among these factors are: depth of myometrial invasion, cervical stromal involvement, adnexal/uterine serosal metastases, lymph node metastasis, histopathological grade, and molecular markers. This multidimensional assessment allows for tailored adjuvant therapies, including radiation and/or systemic therapy, aimed at reducing the risk of recurrence and improving OS outcomes.
The role of malignant PC in endometroid EC as a prognostic indicator has indeed been a subject of debate for many years. Malignant PC was traditionally considered a potential marker for microscopic peritoneal spread and, consequently, associated with a poorer prognosis, particularly in early-stage disease. This perspective led to its inclusion as a predictive factor in the staging systems by the International Federation of Gynecology and Obstetrics (FIGO). However, in 2009, malignant PC was removed from the FIGO staging system, a decision that sparked further investigation and controversy regarding its true significance. The rationale behind this removal was not explicitly detailed but likely stemmed from conflicting evidence in the literature questioning the robustness of malignant PC as an independent prognostic factor. Several studies highlighted this ambiguity: Tebeu et al19 reported that patients with local-stage endometroid EC and malignant PC had a similar prognosis compared to those without malignant PC and better outcomes than those with serosal or adnexal involvement, suggesting that malignant PC alone might not portend worse survival when other risk factors are absent. Kasamatsu et al20 found that malignant PC was not an independent prognostic factor for patients whose disease was confined to the uterus, implying that adjuvant therapy based solely on the presence of malignant PC may not be beneficial. Fadare et al21 also concluded that malignant PC, in the absence of other extrauterine disease, did not seem to impact overall patient outcomes significantly. A retrospective population-based cohort study utilizing data from the British Columbia Cancer Registry between 2003 and 2009 found no association between malignant PC and disease-free or overall survival in women diagnosed with low and intermediate-risk endometroid EC.22
Recent advancements in large-scale, population-based research have solidified the prognostic significance of malignant PC in endometroid EC patients. A comprehensive multicenter retrospective analysis conducted by Zhang et al23 examined 6313 EC cases from 27 medical centers across China, spanning the years 2000 to 2019. Of these cases, 384 patients exhibited malignant PC. Multivariate Cox regression analysis revealed a significant association between malignant PC and reduced progression-free survival (PFS) (hazard ratio [HR]: 2.20 [1.55–3.13], p < 0.001) and OS (HR: 2.25 [1.49–3.40], p < 0.001) specifically within the intermediate and high-intermediate risk groups of endometroid EC. In contrast, the low-risk group demonstrated no notable differences in PFS or OS based on peritoneal cytology status. Further corroboration comes from a substantial cohort study by Seagle et al,24 utilizing data from the National Cancer Database. This study underscored the prognostic impact of malignant PC, revealing a significant decrease in OS for early-stage endometroid EC patients with malignant PC (64.9 months vs 60.6 months, p < 0.001). Notably, this negative prognostic correlation remained robust across various sensitivity analyses, model specifications, variable adjustments, and potential unmeasured confounders. Garg et al25 conducted a retrospective analysis using the SEER database from 1988 to 2005, finding that patients with malignant PC had significantly worse survival outcomes compared to those with negative peritoneal cytology (p < 0.0001). Specifically, the 5-year disease-specific survival (DFS) rates were 95.1% versus 80.8% for endometrioid EC, 78.0% versus 50.4% for clear cell/serous carcinoma, and 64.7% versus 32.3% for carcinosarcoma. After accounting for other contributing factors in a multivariable model, malignant PC emerged as an independent predictor of poor survival across all histologic types examined (p < 0.0001). A meta-analysis by Lee et al14 suggested that malignant PC could serve as a potential prognostic factor in endometrioid EC due to its strong connection with other prognostic indicators and its considerable influence on survival outcomes. Similarly, the latest meta-analysis by Pergialiotis et al15 found that women with early-stage endometrioid EC and malignant PC had significantly lower 5-year recurrence-free survival (RFS) (HR: 0.26 [0.09–0.71]) and 5-year OS (HR: 0.50 [0.27–0.92]). The included patients without malignant PC exhibited considerably higher overall survival (HR: 12.76 [2.78–58.51]), suggesting malignant PC as a negative prognostic indicator for survival outcomes in endometrioid EC patients.
The present study builds upon these findings by leveraging the most recent data (2010–2017) from the SEER database, encompassing a larger, more comprehensive sample across all tumor stages. This approach provides more reliable evidence confirming that malignant PC is associated with poor prognosis in endometrioid EC and serves as an independent risk factor.
The role of malignant PC in risk stratification and adjuvant therapy for endometrioid EC remains underexplored. Matsuo et al26 investigated treatment alternatives based on peritoneal cytology status and their impact on survival, finding that neither hormone therapy nor systemic chemotherapy significantly altered 5-year survival outcomes compared to no adjuvant therapy. This suggests that the predictive value of peritoneal cytology may not directly influence the effectiveness of these treatments in improving survival rates. Tang et al27 conducted a retrospective observational cohort study using the SEER database from 2010 to 2019, involving 3616 patients with early-stage endometrial clear cell carcinoma (CCC) and serous carcinoma (SC). Of these, 368 patients (10.2%) had malignant PC. Women with malignant PC were more likely to receive postoperative chemotherapy (odds ratio [OR]: 2.033 [1.589–2.602]). Multivariate analysis revealed that chemotherapy improved prognosis in patients with malignant PC (OS: p = 0.005; clinically significant survival [CSS]: p = 0.010). Kanno et al28 enrolled 989 stage Ia (confined to the endometrium) endometrioid EC patients between 2005 and 2015, finding that adjuvant chemotherapy did not significantly affect the 5-year recurrence-free survival (RFS) rate in patients with malignant PC (p = 0.78). In contrast, Matsuo et al29 analyzed data from the SEER database from 2010 to 2016, involving 7467 women with stage II–III (FIGO 2009) endometrioid EC, of whom 1662 had malignant PC (22.3%). They found that the combination of chemotherapy and whole pelvic radiotherapy (WPRT) was associated with improved overall survival (OS) compared to chemotherapy or WPRT alone (p < 0.05). Seagle et al24 observed in their retrospective cohort study using the 2010–2013 National Cancer Database that adjuvant chemotherapy during early-stage endometrioid EC with malignant PC was associated with increased survival (hazard ratio [HR]: 0.62 [0.40–0.95], p = 0.03).
During our study, through adjusting confounding factors by PSM, multivariable Cox proportional hazards regression found neither adjuvant radiation nor systemic therapy could improve the OS of endometrioid EC. Further analysis revealed that in the malignant PC cohort, adjuvant radiation improved OS in regional stage, whereas it did not confer a OS advantage in local and distant stages. During atypical and/or suspicious PC cohort, adjuvant radiation did not confer a OS advantage. Conversely, adjuvant systemic therapy paradoxically did not confer a OS advantage during both malignant PC cohort and atypical and/or suspicious PC cohort. These results suggested that malignant PC may not be suitable for guiding risk stratification and adjuvant therapy in endometrioid EC.
The present study has several notable strengths. Foremost is its population-based design, which—to our knowledge—provides the largest endometrioid EC cohort reported in the literature. The inclusion of a wide spectrum of tumor varieties enhances the robustness and generalizability of our findings. Furthermore, our analytical approach incorporated PSM with rigorous subgroup analyses, thereby strengthening statistical validity and deepening the interpretability of our conclusions.
Nevertheless, we acknowledge several potential limitations inherent to our study. Primarily, its retrospective nature introduces an element of unmeasured bias, given that certain surgical-pathological variables such as lymphovascular space invasion, personal histories of tubal surgery, preoperative diagnostic hysteroscopy usage, omentometry biopsy outcomes, and molecular markers—all of which could influence both the prevalence of malignant PC and patient outcomes—were not retrievable from the SEER database. Notably, prior research has implicated diagnostic hysteroscopy in heightened malignant PC risk; thus, the absence of data on this procedure may have introduced some bias into our observations. Future research is warranted to elucidate the precise prognostic implications of malignant PC in the context of diagnostic hysterectomy.
Secondly, the accuracy and consistency of malignant PC diagnoses across diverse pathology practices remain uncertain due to the lack of centralized pathology review in our study. This variability could potentially confound our results.
Thirdly, while our findings are based on a US cohort, caution should be exercised when extrapolating these outcomes to populations of different ethnicities or healthcare systems, necessitating further validation studies.
Fourth, the SEER dataset’s limitation in capturing detailed recurrence data precluded a thorough analysis of oncologic outcomes, including the specific sites of recurrence and the potential impact of systemic chemotherapy on reducing distant metastases, as suggested by earlier hypotheses.
Fifth, there exists a possibility of misclassification regarding adjuvant therapy regimens, as cases with unreported or unknown treatment statuses were aggregated within the SEER Program’s chemotherapy and radiotherapy categories.
Lastly, the unavailability of specific chemotherapy protocols and cycle counts in the SEER dataset impedes definitive conclusions about the comparative efficacy of chemotherapy versus radiotherapy in the malignant PC subset, particularly concerning whether inadequate dosing might have contributed to observed survival disparities.
Conclusion and Future Perspectives
The findings of our study underscore the significance of malignant PC as an independent prognostic indicator in patients diagnosed with endometrioid EC. This discovery adds a nuanced layer to the understanding of disease progression and patient outcomes, emphasizing the need for tailored therapeutic strategies that account for the presence of malignant PC.
However, the precise role of malignant PC in refining risk categories and guiding adjuvant treatment decisions remains ambiguous. To bridge this knowledge gap, rigorous validation through well-designed randomized controlled trials (RCTs) is imperative. Such studies would not only corroborate the observed association but also elucidate whether incorporating malignant PC into risk assessment algorithms can enhance the precision of prognostication and personalize therapeutic interventions more effectively. To implement RCTs effectively, several key considerations must be addressed: 1). Patients should be stratified based on the presence or absence of malignant PC at the time of initial diagnosis. This stratification will allow for a direct comparison of outcomes between these two groups. 2). Consistent treatment regimens should be administered within each group to ensure that any observed differences in outcomes can be attributed to the presence of malignant PC rather than variations in treatment. 3). Critical endpoints such as OS, DFS, and recurrence rates should be meticulously documented to provide a comprehensive assessment of the impact of malignant PC on patient outcomes. 4). Incorporating molecular profiling of tumors may reveal underlying biological mechanisms that contribute to the development of malignant PC, thereby enhancing our understanding of its prognostic significance.30 5). Long-term follow-up is essential to capture the full spectrum of oncological outcomes and to assess the durability of any observed effects related to malignant PC. By addressing these considerations, RCTs can robustly validate the prognostic significance of malignant PC and inform clinical decision-making processes. The results from such trials could potentially lead to the integration of malignant PC status into clinical practice guidelines, optimizing patient care and improving survival rates.
Furthermore, exploring the underlying biological mechanisms driving malignant PC and its interaction with other clinicopathological variables could pave the way for novel therapeutic targets and refined management protocols. As we advance in our comprehension of endometrioid EC’s heterogeneity, integrating malignant PC status into clinical practice holds promise for optimizing patient care and improving survival rates.
In conclusion, while our research solidifies malignant PC as an independent prognostic factor for reduced OS in endometrioid EC, it further uncovers critical treatment-specific interactions: Radiation therapy improved OS only in malignant PC patients with regional disease; Systemic therapy significantly reduced OS in malignant PC patients across all stages; No survival benefit was observed from radiation or systemic therapy in the atypical/suspicious PC subgroup). These findings highlight an urgent need to refine risk stratification and re-evaluate adjuvant therapy selection based on PC status. Future endeavors must prioritize RCTs validating PC-directed treatment algorithms and mechanistic studies elucidating underlying resistance pathways, ultimately enabling individualized clinical management.
Data Sharing Statement
All analyzed data in this study are fully presented in the main text, figures and tables. No additional datasets are available.
Ethical Approval
Ethical approval exemption was granted by the Institutional Review Board of The Fifth Affiliated Hospital of Sun Yat-sen University under Article 32 of China’s Measures for Ethical Review.
Funding
This work was supported by the Guangdong Foundation for Basic and Applied Fundamental Research (23202104030001207).
Disclosure
The author declares no conflicts of interest in this work.
References
1. Harkenrider MM, Abu-Rustum N, Albuquerque K, et al. Radiation therapy for endometrial cancer: an American society for radiation oncology clinical practice guideline. Pract Radiat Oncol. 2023;13(1):41–65. doi:10.1016/j.prro.2022.09.002
2. Rosario-Santos A, Torres-Cintrón CR, López-Rexach AG, Gonzalez-Carcache P, Tortolero-Luna G, Umpierre S. A comparative analysis of endometrial cancer disparities in incidence, mortality, and survival between women living in Puerto Rico, Non-Hispanic Blacks, Non-Hispanic Whites, and US Hispanics between 2000–2018. Gynecol Oncol Rep. 2023;49:101275. doi:10.1016/j.gore.2023.101275
3. Sun KX, Zheng RS, Zuo J, et al. The incidence and mortality of endometrial cancer in China, 2015. Zhonghua Yi Xue Za Zhi. 2022;102(26):1987–1992. Chinese. doi:10.3760/cma.j.cn112137-20211029-02403
4. Asami Y, Hiranuma K, Takayanagi D, et al. Predictive model for the preoperative assessment and prognostic modeling of lymph node metastasis in endometrial cancer. Sci Rep. 2022;12(1):19004. doi:10.1038/s41598-022-23252-3
5. Kasius JC, Pijnenborg JMA, Lindemann K, et al. Risk stratification of endometrial cancer patients: FIGO stage, biomarkers and molecular classification. Cancers. 2021;13(22):5848. doi:10.3390/cancers13225848
6. Hamilton CA, Pothuri B, Arend RC, et al. Endometrial cancer: a society of gynecologic oncology evidence-based review and recommendations. Gynecol Oncol. 2021;160(3):817–826. doi:10.1016/j.ygyno.2020.12.021
7. Jamieson A, McAlpine JN. Molecular profiling of endometrial cancer from TCGA to clinical practice. J Natl Compr Canc Netw. 2023;21(2):210–216. doi:10.6004/jnccn.2022.7096
8. Angelico G, Santoro A, Rossi ED, Zannoni GF. The role of cytology in endometrial cancer: diagnostic and clinical considerations from peritoneal/pelvic washings. Is it still a heated debate? Cancer Cytopathol. 2021;129(7):497–498. doi:10.1002/cncy.22407
9. Guo XM, Roman LD, Klar M, Wright JD, Matsuo K. Malignant peritoneal cytology in endometrial cancer: a contemporary review. Expert Rev Anticancer Ther. 2022;22(9):947–955. doi:10.1080/14737140.2022.2105208
10. Shigeta S, Konno Y, Terai Y, et al. A qualitative systematic review of the significance of adjuvant therapy in patients with low-risk endometrial cancer presenting positive peritoneal cytology: a relevant study to the guideline update for endometrial cancer by the Japan society of gynecologic oncology guideline committee. Jpn J Clin Oncol. 2024;54(2):217–220. doi:10.1093/jjco/hyad140
11. Berek JS, Matias-Guiu X, Creutzberg C, et al; Endometrial Cancer Staging Subcommittee, FIGO Women’s Cancer Committee. FIGO staging of endometrial cancer: 2023. J Gynecol Oncol. 2023;34(5):e85. doi:10.3802/jgo.2023.34.e85
12. Ueno Y, Toyoshima M, Shigemi D, et al. Significance of positive peritoneal cytology for recurrence and survival in patients with endometrial cancer. J Obstet Gynaecol Res. 2023;49(1):304–313. doi:10.1111/jog.15457
13. Shiozaki T, Tabata T, Yamada T, Yamamoto Y, Yamawaki T, Ikeda T. Does positive peritoneal cytology not affect the prognosis for stage I uterine endometrial cancer?: the remaining controversy and review of the literature. Int J Gynecol Cancer. 2014;24(3):549–555. doi:10.1097/IGC.0000000000000072
14. Lee B, Suh DH, Kim K, No JH, Kim YB. Influence of positive peritoneal cytology on prognostic factors and survival in early-stage endometrial cancer: a systematic review and meta-analysis. Jpn J Clin Oncol. 2016;46(8):711–717. doi:10.1093/jjco/hyw063
15. Pergialiotis V, Panagiotopoulos M, Koutras A, et al. The impact of positive peritoneal cytology on the survival rates of early-stage-disease endometrial cancer patients: systematic review and meta-analysis. Medicina. 2024;60(5):733. doi:10.3390/medicina60050733
16. Behtash N, Sheikhhasani S, Nezamabadi V. Prognostic significance of positive peritoneal cytology in endometrial cancer patients. J Obstet Gynaecol. 2022;42(6):2336–2340. doi:10.1080/01443615.2022.2049725
17. Concin N, Matias-Guiu X, Vergote I, et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int J Gynecol Cancer. 2021;31(1):12–39. doi:10.1136/ijgc-2020-002230
18. Penberthy L, Friedman S. The SEER Program’s evolution: supporting clinically meaningful population-level research. J Natl Cancer Inst Monogr. 2024;2024(65):110–117. doi:10.1093/jncimonographs/lgae022
19. Tebeu PM, Popowski Y, Verkooijen HM, et al. Positive peritoneal cytology in early-stage endometrial cancer does not influence prognosis. Br J Cancer. 2004;91(4):720–724. doi:10.1038/sj.bjc.6602035
20. Kasamatsu T, Onda T, Katsumata N, et al. Prognostic significance of positive peritoneal cytology in endometrial carcinoma confined to the uterus. Br J Cancer. 2003;88(2):245–250. doi:10.1038/sj.bjc.6600698
21. Fadare O, Mariappan MR, Hileeto D, Wang S, McAlpine JN, Rimm DL. Upstaging based solely on positive peritoneal washing does not affect outcome in endometrial cancer. Mod Pathol. 2005;18(5):673–680. doi:10.1038/modpathol.3800342
22. Scott SA, van der Zanden C, Cai E, McGahan CE, Kwon JS. Prognostic significance of peritoneal cytology in low-intermediate risk endometrial cancer. Gynecol Oncol. 2017;145(2):262–268. doi:10.1016/j.ygyno.2017.03.011
23. Zhang Y, Chu R, Zhang Z, et al; Chinese Endometrial Carcinoma Consortium (CECC). Prognostic significance of positive peritoneal cytology in endometrial carcinoma based on ESGO/ESTRO/ESP risk classification: a multicenter retrospective study. Gynecol Oncol. 2023;176:43–52. doi:10.1016/j.ygyno.2023.06.578
24. Seagle BL, Alexander AL, Lantsman T, Shahabi S. Prognosis and treatment of positive peritoneal cytology in early endometrial cancer: matched cohort analyses from the National Cancer Database. Am J Obstet Gynecol. 2018;218(3):
25. Garg G, Gao F, Wright JD, Hagemann AR, Mutch DG, Powell MA. Positive peritoneal cytology is an independent risk-factor in early stage endometrial cancer. Gynecol Oncol. 2013;128(1):77–82. doi:10.1016/j.ygyno.2012.09.026
26. Matsuo K, Nusbaum DJ, Matsuzaki S, et al. Malignant peritoneal cytology and increased mortality risk in stage I non-endometrioid endometrial cancer. Gynecol Oncol. 2020;159(1):43–51. doi:10.1016/j.ygyno.2020.07.010
27. Tang X, Li N, Hu Y. Prognosis and adjuvant chemotherapy for patients with malignant peritoneal cytology in early-stage non-endometrioid endometrial cancer. Eur J Surg Oncol. 2023;49(11):107071. doi:10.1016/j.ejso.2023.107071
28. Kanno M, Yunokawa M, Nakabayashi M, et al. Prognosis and adjuvant chemotherapy for patients with positive peritoneal cytology in stage IA endometrial cancer. Sci Rep. 2022;12(1):166. doi:10.1038/s41598-021-03975-5
29. Matsuo K, Matsuzaki S, Nusbaum DJ, et al. Association between adjuvant therapy and survival in stage II-III endometrial cancer: influence of malignant peritoneal cytology. Ann Surg Oncol. 2021;28(12):7591–7603. doi:10.1245/s10434-021-09900-4
30. Besharat AR, Giannini A, Caserta D. Pathogenesis and treatments of endometrial carcinoma. Clin Exp Obstet Gynecol. 2023;50(11):229. doi:10.31083/j.ceog5011229
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.