Back to Journals » Journal of Healthcare Leadership » Volume 17
Making Multidisciplinary Team-Based Care (MTBC) a Success in Primary Care: A Scoping Review Care: A Scoping Review
Authors Liang Z ![]() , Montgomery J, Dingelstad C
, Montgomery J, Dingelstad C ![]() , Koschel A, Redford M
, Koschel A, Redford M ![]()
Received 14 August 2025
Accepted for publication 24 October 2025
Published 11 November 2025 Volume 2025:17 Pages 681—695
DOI https://doi.org/10.2147/JHL.S560629
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Pavani Rangachari
Zhanming Liang,1 Jasmine Montgomery,1 Cate Dingelstad,2 Alison Koschel,2 Michelle Redford2
1College of Business, Law and Governance, James Cook University, Townsville, QLD, Australia; 2Hunter New England and Central Coast Primary Health Network, Newcastle, NSW, Australia
Correspondence: Zhanming Liang, College of Business, Law and Governance, Building 27 First Floor, JCU Townsville Campus Douglas, Townsville, QLD, 4870, Australia, Email [email protected]
Abstract: Patient-centred care is the foundation for safe and high-quality care that enhances patient health outcomes, with multidisciplinary team-based care (MTBC) being a key enabling factor. MTBC is an integrated approach in care provision involving health professionals with different skillsets working in collaboration. Shared goals, clarity of roles, mutual trust, effective communication, and the evaluation of team functions are important for MTBC success. No reviews were identified on the system or cross-organisational approaches that support MTBC in primary care settings. A scoping review was conducted between October and December 2024 to identify international innovations in operationalising MTBC in primary care and the factors that impact its success. The databases searched were CINAHL, ProQuest Central, PubMed, Scopus, and Web of Science, in October 2024. The search terms were informed by two central concepts: MTBC (concept 1) and primary care (concept 2). Concepts of design (concept 3) and factors (concept 4) were added to refine the scope of the search. Following the Arksey and O’Malley framework, the scoping review included 58 articles on data extraction, and confirmed 14 key success factors and 14 barriers that could affect the implementation and adoption of MTBC. The strengths of MTBC in the primary care setting are summarised by six themes: patient-centred benefits, teamwork and collaboration, decision-making and clinical care, communication and coordination, improved access and performance management, and supportive infrastructure. This review further confirms six core benefits and 11 core components of the MTBC model, providing important guidance for MTBC development. A multidisciplinary team-based care model was designed to deliver comprehensive patient-centred care by integrating expertise from various disciplines. By integrating the key elements identified in this review into a specific primary care context, successful implementation of an adaptable MTBC model may lead to improved service delivery and outcomes in primary care.
Keywords: interprofessional, integrated care, patient-centered, multidisciplinary team-based care, interdisciplinary care
Introduction
Primary care is key to a resilient healthcare system that provides continuation of non-hospital care, supports chronic disease management, and is responsive to crises. 1 It optimises health outcomes and directly affects the sustainability of the health system to meet the growing and more complex healthcare needs of the population. 2 The organization and funding of primary care are vastly different between countries. It can be funded as part of public hospital services such as in China, publicly funded but privately delivered in the United Kingdom, publicly funded but subsidised by out-of-pocket from care recipients as in Canada, mixed with public and private provision as in Australia, and primarily privately funded as in the US.3,4 The complexity of funding arrangements and difficulties in coordinating multilevel service providers have been attributed to a fragmented system that makes it difficult for consumers to navigate and access.3 Regardless of how primary care is organised, it is believed that inflexible fee-for-service models, limited scope of practice, and lack of team support make the implementation of a patient-centred approach in the primary care setting challenging.3,4 Furthermore, the changing healthcare needs of the population and common challenges facing primary care provision have necessitated the adoption of new primary care models that enable integration, collaboration, and patient-centredness.3,5,6
Patient-centred care (PCC) is the foundation of safe and high-quality care that enhances patient health outcomes.7 Guided by Picker’s principles of patient-centred care (PCC), the PCC approach demonstrates healthcare providers’ commitment to respecting and responding to the preferences, needs, and values of their patients and consumers,8,9 in the process of providing coordinated, continued, and integrated care.10 Multidisciplinary teams with the required skill mix and ability to collaborate across disciplines is an enabling factor. In primary care, the provision of chronic and preventive care can be negatively affected by rigid funding and time constraints.3,6 As part of a multidisciplinary care team, chronic and preventative care can be delegated across the team, improving patient access to holistic care.11 Evidence further suggests that well-organised multidisciplinary teams increase patient satisfaction and reduce staff burnout,12,13 and hospital readmissions.14,15
Multidisciplinary team-based care (MTBC) is an integrated approach to providing care. A variety of health professionals may be included as part of a multidisciplinary team, and the discipline varies depending on the patient’s health needs. In primary care, multidisciplinary teams may include general practitioners, nurses, allied and community health disciplines, and indigenous health workers and work closely with stakeholders such as hospital management staff who work together in the decision-making process.16 In general practice, practitioners are often at the core of a multidisciplinary team working in collaboration with a variety of healthcare professionals. By utilising the skills and experience of health professionals from different disciplines, multidisciplinary teams apply more knowledge and experience than disciplines operating in isolation to determine the most appropriate care for their patients.16–18 This is particularly beneficial for addressing the needs of patients with complex or chronic diseases.19 In non-hospital settings, MTBC can improve transitional care for patients transitioning from hospitals to the community,20 integrate primary and secondary tertiary care for people with complex chronic diseases,21 and be used as part of a holistic approach to meet the health promotion and prevention needs of community members.19
A systematic review of the literature on integrated primary care conducted by Mitchell et al21 and Mulvale et al22 synthesised the key success elements of multidisciplinary team approaches in primary care. 1) Interdisciplinary teamwork with the right skill mix; 2) commutation and information exchange; 3) use of shared care guidelines or pathways; 4) training and education, access, and acceptability; 5) team vision and shared goals; 6) formal quality processes; 7) information systems; and 8) professional feelings as part of the team.21,22 Mulvale et al further categorised the key elements into the macro (governance), meso (information systems and organizational culture), micro, and individual levels. The micro level includes team structures, social processes, formal processes, and team attitudes, whereas factors at the individual level refer to beliefs in interprofessional care and flexibility.22
Many factors may diminish the success of implementation and adoption of a multidisciplinary team approach. Commonly mentioned factors23–28 include:
- Inadequate communication within the team;
- Inadequate patient data, missing medical records owing to delays in diagnostic tests, and insufficient coordination across different disciplines.
- Lack of technical and administrative support;
- Lack of long term funding;
- Lack of motivation and involvement of team members;
- Staff shortages and staff absences from multidisciplinary team meetings when many patient cases are scheduled for discussion, and
- Team members’ lack of understanding of how an integrated team works differently, roles, and responsibilities.
Therefore, adequate resources and dedicated time, adoption of technology to facilitate timely communication and sharing of patient data and documents, effective team leadership, and patient involvement are enabling factors.29
International experience in the formulation and implementation of MTBC can provide useful guidance in different healthcare contexts. A quick desktop search only identified published systematic or scoping reviews focusing on specific care such as cancer care,29 care pathways,26 geriatric medicine,30 and integration of primary and secondary care.21 No reviews were identified on system or cross organization approaches that support multidisciplinary team-based care in primary care settings and factors influencing its adoption and implementation success. Hence, a scoping review was conducted between October and December 2024 to identify international innovations in operationalising MTBC in primary care and the factors that impact its success. This study focused on the following research questions:
- What are the approaches, key strategies, and innovations that support MTBC implementation and adoption in primary care, with specific attention given to general practice (including funding models)?
- What are the key enabling factors for MTBC success?
- What are the common barriers to MTBC and associating strategies in addressing such barriers?
Materials and Methods
This scoping review followed the five-step framework of Arksey and O’Malley (2005)31 and was conducted in accordance with PRISMA guidelines32 to ensure transparency and consistency in reporting.
Search Strategy
A comprehensive search was conducted using the following databases: CINAHL, ProQuest Central, PubMed, Scopus, and Web of Science. The search terms were based on two central concepts: (1) multidisciplinary team-based care (MTBC) and (2) primary care. Before conducting the search, keywords under four different concepts were determined. The initial design of the search strategies was to use keywords under concepts 1 (multidisciplinary or interdisciplinary), 2 (primary care), 3 (model, design, or framework), or 4 (success factor, enablers, or obstacles). However, this search generated a large number of studies (>24,000). Quick scanning of some titles confirmed that most papers were irrelevant to answering the research questions. Therefore, we implemented a revised search strategy. First, keywords under concept 1 (Interdisciplinary OR Multidisciplinary) were used to conduct a broad search of the following five databases: Scopus, PubMed, CINAHL, ProQuest Central, and Web of Science. Keywords under concepts 2 (General Practice OR General Practitioner, OR Primary Health OR Primary Care OR Physician), 3 (Model OR Framework OR Design), and 4 (success factor OR enablers OR obstacles) were used to search the identified papers using the following strategies: 1) concept 2 + concept 3 and 2) concept 2 + concept 4. Additional citations were identified in the review papers found in the database search.
The search was conducted in October 2024 to identify the most recent and relevant studies published between 2010 and 2024. After full-text review of the articles (study selection) has been completed, a complimentary search of grey literature was conducted via ChatGPT and Google Search Engine using search words of “government policy on multidisciplinary team”, “commissioned reports on multidisciplinary team”, “expand search on google scale” to identify relevant commissioned reports or position papers.
No ethical approval was required to complete the scoping review.
Inclusion and Exclusion Criteria
Studies were included in the review if they were peer-reviewed, written in English, and focused on primary care or general practice using a multidisciplinary team-based model. Articles that did not meet the inclusion criteria or were not published in English were excluded from data extraction.
Study Selection and Screening Process
The Concept 1 keyword search generated 24155 potentially relevant papers from five databases. After the removal of 9638 duplicates, 14517 papers went through further keyword searches under concepts 2 and 3 or concepts 2 and 4. This resulted in 3666 non-review papers and 17 review papers for the title screening. The title, abstract, and full-text screening of the 17 review papers confirmed that six papers may be relevant to the topic. Screening of the references was performed on six review papers, identifying 27 potentially relevant papers. In total 3687 (3666+17) papers went to the title screening stage performed by ZL, resulting in 188 papers which were uploaded to Covidence.com - systematic review software (32) for abstract screening performed by JM and EG (colleagues of ZL) individually and independently. ZL reviewed 17 papers that received differing decisions made by JM and EG, and made a final decision regarding inclusion or exclusion from the full-text review. The full-text review of 188 articles performed by ZL resulted in the inclusion of 55 articles for JM to perform data extraction. A review of the documents did not reveal any supplementary information to be added to the existing review. A PRISMA flow diagram summarising the screening process and its outcomes is shown in Figure 1. A gray literature search using ChatGPT and Google identified six relevant documents.
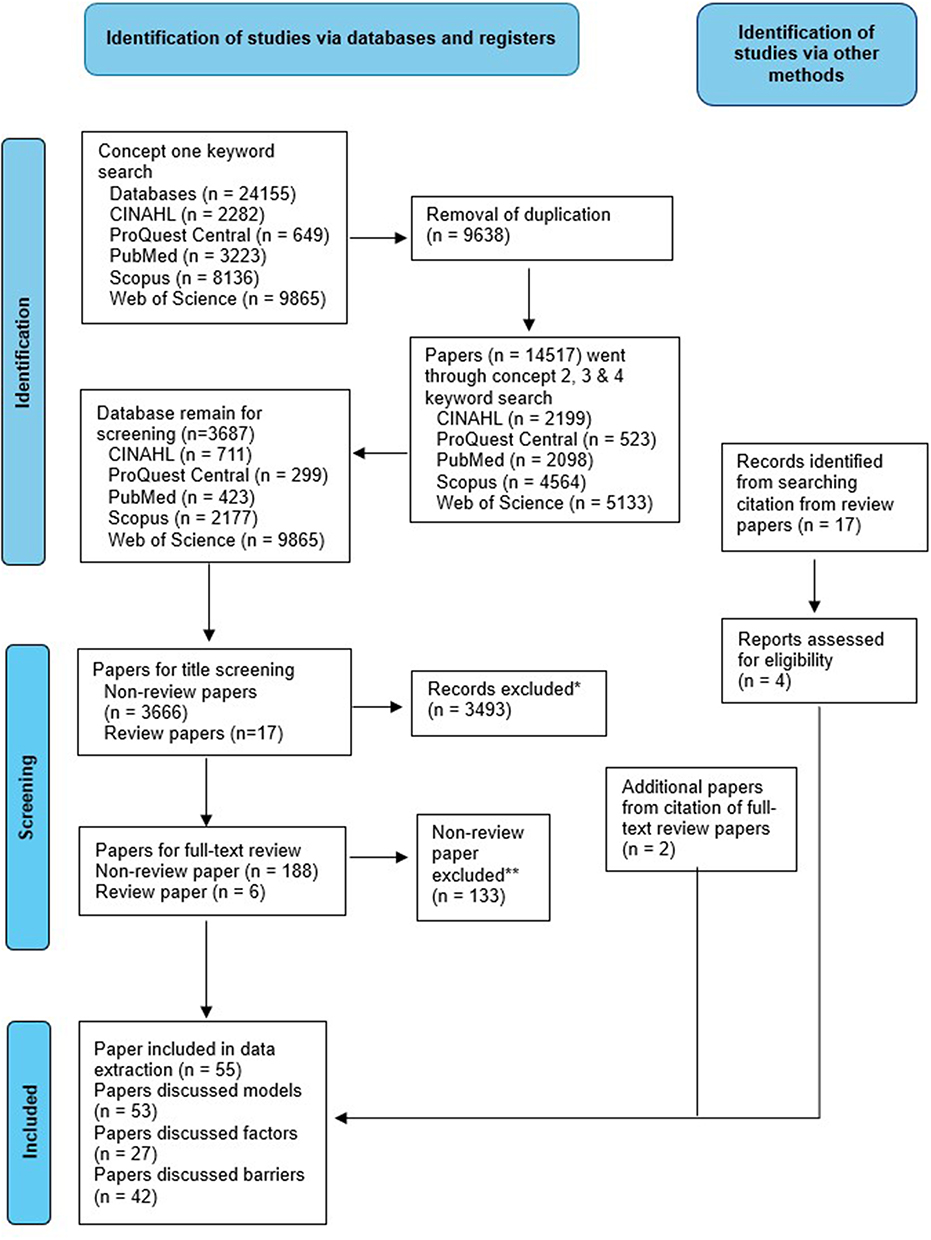 |
Figure 1 PRISMA Flow Diagram. *Main reasons for exclusion: Focus on hospital settings. **Main reasons for exclusion: Focus on benefits (not models). |
Data Extraction
Qualtrics software was used to extract data from the studies33 included the following characteristics: author(s), year of publication, country of study, geographical location, focus of the study, research methods, study population, sample size, and response rates. The following information relevant to the research questions was extracted:
1) Types and core components of multidisciplinary models;
2) Funding models supporting a multidisciplinary approach;
3) Success factors and barriers for MTBC.
The data were exported from Qualtrics to a Microsoft Excel spreadsheet and imported into NVivo 20 for further analysis and synthesis.
Data Synthesis
The data analysis involved a descriptive summary of the included studies, focusing on key variables, such as core components, success factors, barriers, and strengths of the interdisciplinary models. A deductive approach using Braun and Clarke’s (2006)34 thematic analysis was applied to identify key themes by grouping similar concepts and examining the patterns in the data. A comparative analysis was also conducted to explore differences in findings across various study designs, contexts, and populations. The results were synthesised to identify commonalities and discrepancies in the literature, addressing gaps and barriers which guided the development of a flexible MTBC model applicable to primary care settings. To ensure the accuracy and reliability of the analysis process, a codebook with descriptive meanings was generated and discussed between authors, allowing for the clarification and refinement of codes and enhancing the depth of analysis to ensure that the identified themes accurately represented the data.
Results
Data were extracted from the 55 identified papers, as detailed in Appendix 1. Additional information such as the focus of the paper, country of publication, study design, and core content coverage are included in Appendix 1. These studies were published in 21 countries. Countries in which these papers were published were the US (n = 11), Canada (n = 8), and Australia (n = 7). The publication years span from 2010 to 2024, with the following distribution: 2020–2024 (n = 19), 2015–2019 (n = 23), and 2010–2014 (n = 13). The majority of the papers focused on the primary care sector and general practice (n = 44).
Success Factors and Barriers
Collectively, eighty-nine factors that contributed to the success and/or implementation of MTBC were extracted from the 27 identified papers (see Figure 1, PRISMA diagram).11,21,35–59 Based on the themes created in some of the papers and the similarity of the factors, 14 key success factors are listed in Figure 2.
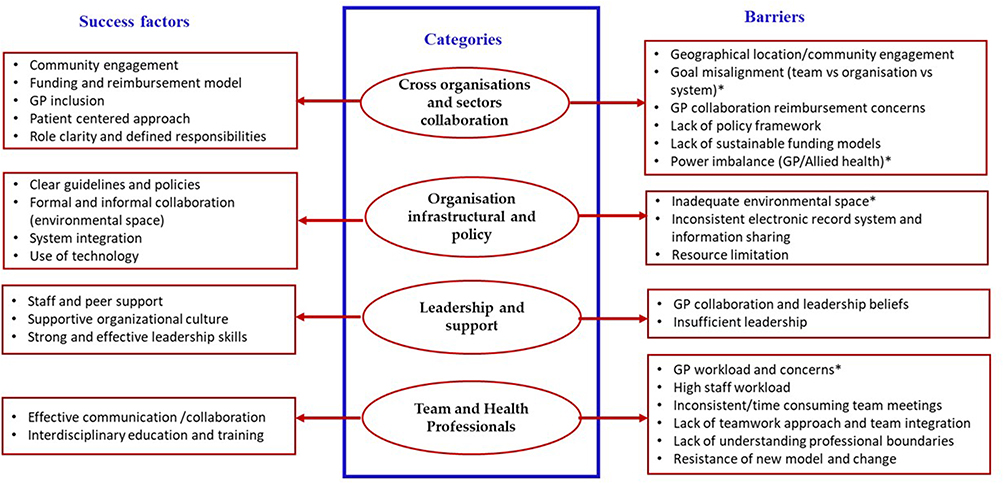 |
Figure 2 Influencing factors for MTBC. *Goal misalignment presents significant barriers to effective collaboration in healthcare, as conflicting individual and team goals, legislative requirements, and patient care objectives often arise. *Power imbalances rooted in traditional hierarchical models between GPs and allied health professionals complicate collaboration, creating obstacles to achieving shared goals and delivering optimal care. |
In contrast, 17 barriers to the introduction and/or implementation of MTBC were extracted from the 42 identified papers (see Figure 1, PRISMA diagram). Some of the barriers are similar to success factors but from a negative perspective. After comparing the similarity between barriers and removing barriers that were similar to success factors, 17 barriers were finalised, as shown in Figure 2. 4,21,36,37,41–43,45,47,49,50,55,60–72
Goal misalignment presents significant barriers to effective collaboration in healthcare, as conflicting individual and team goals, legislative requirements, and patient care objectives often arise.36,41,60–62,68,70 However, interprofessional education plays a crucial role in overcoming these challenges by training healthcare professionals together, which enhances teamwork and improves healthcare delivery.4,42,43,55,63,65–67
The environmental context, including working conditions and available resources, also plays a pivotal role in supporting collaboration.42,43,63 Adequate resources and regular team meetings are essential for fostering effective communication and coordinated care.4,42,43,55,63,65–67
General Practitioners (GPs) face numerous challenges, including heavy workloads, leadership responsibilities, burnout, time constraints, and limited community networks, which can undermine their ability to collaborate effectively.21,59–62,71 Trust in staff and shared perspectives on collaboration can strengthen GP leadership and their effectiveness in team-based settings.21,37,45,47,49,50,55,62,64,68,72,73 Addressing GP recruitment and retention can empower GPs and ensure sustainability in the primary care sector.40,47,50,55,62,64,71,72,74
Power imbalances rooted in traditional hierarchical models between GPs and allied health professionals complicate collaboration, creating obstacles to achieving shared goals and delivering optimal care.21,42,47,62,64,67,68,72
By further comparing the factors and barriers, four categories emerged to collectively accommodate the factors that influenced the success of MTBC, as illustrated in Figure 2.
Core Components of a MTBC Model
A multidisciplinary team-based care model was designed to deliver comprehensive patient-centred care by integrating expertise from various disciplines. Typically, teams regularly plan for patient care. Based on the 24 identified papers that discussed elements of various MTBC models (see Figure 1 PRISMA diagram)4,11,21,36,39,41,43,45,47,50,54,55,58,59,64,72–80 eleven key components are illustrated in Figure 3 with brief explanations provided below.
- Collaborative communication strategies – Implementation of collaborative communication strategies such as regular interdisciplinary team meetings that enable integration, transparent, and timely communication among team members.
- Collaborative team development and cohesion - Investment in collaborative team building initiatives to foster trust, mutual respect, and a cohesive, high-functioning team culture.
- Co-location and Physical Proximity of Practitioners – Facilitation of more effective and immediate collaboration and coordination of care by considering the physical or environmental location of healthcare professionals.
- Flexible and integrated model of care – Adoption of adaptable care models that are responsive to different social, policy, and community contexts, taking local needs into consideration and allowing for the engagement of practitioners and other healthcare providers and professionals.
- Governance, leadership and shared vision – Establishment of a clear governance structure, shared goals, vision and decision-making, effective leadership, and developing a sense of belonging among staff.
- Integrated communication and information technology – Utilisation of integrated information technologies and digital referral systems to ensure seamless access to patient records and data by team members.
- Multidisciplinary learning and workforce support - Provision of interdisciplinary training opportunities, staff development, and support resources to foster effective collaborative practice across professional boundaries.
- Patient-Centred Care and Engagement – Active involvement of patients in care planning and delivery, ensuring that care is tailored and responsive to individual circumstances.
- Quality assurance and outcome measurement – developing quality indicators, metrics, and measures for outcomes, processes, and disease registries for follow-up and monitoring.
- Sustainable Funding and Reimbursement Models – Developing sustainable financial structures that support team operations and patient care.
- Stakeholder engagement and service collaboration – Strengthening stakeholder partnerships and collaborative working relationships across services.
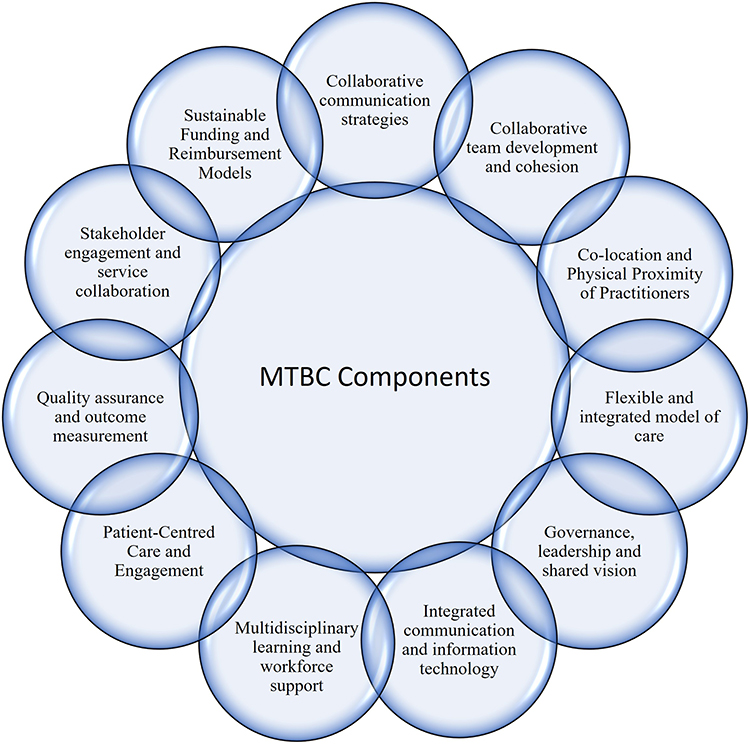 |
Figure 3 MTBC core components. |
To build collaborative teams, the following details should be considered:4,21,37,42,43,45,47,49,55,62–67,72,73
- A culture of mutual respect and trust.
- Clear team structure and composition.
- Collaboration and working relationships between services.
- Fostering a sense of belonging within the team.
- Setting and respecting professional boundaries.
- Relaxation of traditional medical hierarchy models.
- Well defined roles and responsibilities for team members.
For a patient-centred approach and engagement, the following actions are also required:11,21,35–37,41,43,46–48,50,53,54,61,63,73,75,77,79
- Active patient involvement.
- Coordination of care.
- Empowerment of patients in treatment.
- Cross-cultural sensitivity and tailored care approaches.
- Professional support in patient self-management.
- Case management to enhance patient support.
- Protect patient confidentiality.
- Enable information sharing.
Benefits of MTBC
A total of 37 papers discussed the strengths of MTBC papers discussed the strengths of multidisciplinary care.4,11,21,29,35–38,40–51,53–55,58–64,69,73,75–77,81,82 These benefits can be categorized in six domains as outlined in Figure 4.
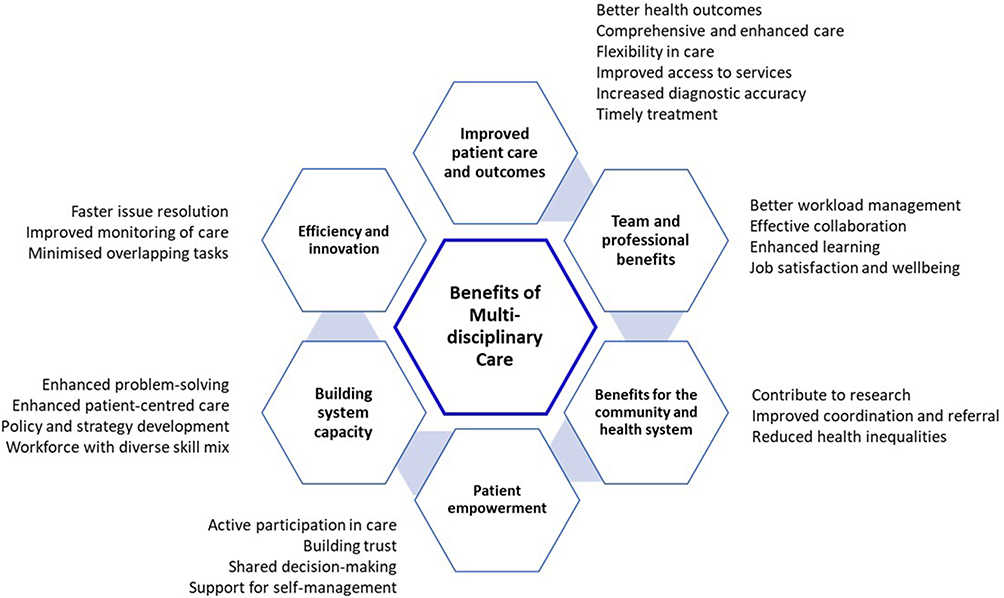 |
Figure 4 Benefits of multidisciplinary care. |
Discussion
Through a systematic process, this study synthesised research evidence from the past 15 years, the current review highlighting the growing importance of applying multidisciplinary team concepts in the delivery of care and services in primary care settings. Previous systematic reviews confirmed that MTBC could improve patient health outcomes17,74 and service efficiency,15 better chronic disease management,13 and enhance continuity of care during the transition between primary and secondary tertiary settings.21,35,83 The current review identified additional benefits beyond patient and service provision. Specifically, MTBC can strengthen health service capacity to better meet the needs of patients and customers by enabling improved resource sharing and exchange of expertise.36–38,60,61,75,84 Moreover, an MTBC approach fosters innovation by reducing task duplication, facilitating faster problem solving, and improving monitoring of care.36,39,81
Improving Skills and Capability in Better Patient Care
By encouraging collaboration among professionals with diverse skills from different primary and social care organisations, patient care can be designed and delivered in a more holistic manner which is facilitated by the timely and effective sharing of patient data.40,76,81,85 This improved timely access to patient data throughout the care process by different professional teams is said to indirectly advance research focusing on patient cohorts or population groups.11,41,42,60,81 However, the seamless sharing of data across disciplines can only be achieved with consistent electronic patient / health records and a functional and adaptable data management system supported by robust information technology.29,38,43,44 Furthermore, team members must have the skills to interpret unfamiliar forms of data or use the data to guide decision making and design patient care plans. Therefore, investing in developing these skills at the organisational and system levels is essential for health professionals to thrive in this new collaborative model.29,43,44 This commitment, in turn, helps reduce resistance to change while fostering greater acceptance and compliance among the staff.37,39,44,45,62,75,77
Funding and Reimbursement
Healthcare organisations operate in a financially constrained environment, which limits their capacity to innovate and support new models of care, owing to rigid funding mechanisms that lack long-term sustainability.44 The current review consistently highlights the need for dedicated funding and new funding models that support infrastructure development, team operations, patient care, and compensation for the time required by health professionals working within multidisciplinary teams.11,39,46,63,76,78 A comprehensive reimbursement model should compensate allied health professionals, general practitioners and other key primary health care professionals for a range of services, ensuring accessibility to care and covering administrative costs, such as digital technology and team collaboration.36,42,47 To maximise the efficiency of a new care model, additional funding is needed for new positions that lead or support smooth coordination and functioning of multidisciplinary teams, with a focus on addressing complex needs of patients rather than simply managing individual care episodes.47,64 Research has shown that flexible models are more responsive than rigid, fee-for-service structures.44,65 More research into what constitutes a sustainable funding and reimbursement model that supports MTBC across different healthcare systems, along with an understanding of commonalities and differences, would be valuable in guiding the development of MTBC.
Developing Mutual Understanding, Trust and Respect
Multidisciplinary teams foster “on the job” learning for their members, maximising support and skill development. This approach not only improves staff job satisfaction and well-being, but also enables better workload management by increasing efficiency.60,62,64 In a rapidly changing healthcare environment where the complexity of patient care and rising expectations are common challenges, upskilling and developing a diverse skill mix among health professionals is crucial for the sustainability of healthcare organisations and systems to meet the needs of the population.75 A well-organised and collaborative multidisciplinary team provides a valuable platform for learning across different disciplines and skill sets.29,48–52,66,76,79,81,86 However, concerns about power imbalance, such as doctors assuming a more dominant role in decision-making compared to allied health professionals and others29,36,51,52,61,82,85 and the lack of trust between health professionals from different disciplines and service providers were also noted.38,64,67,68,76 Therefore, fostering cross-cultural learning and cultivating a collaborative and accepting culture across primary care, community and social care is essential.
The development of mutual understanding, respect, and trust among healthcare professionals is essential for effective collaboration and the quality of care provided.53–55,75 These qualities are cultivated through strong leadership, a supportive environment that encourages both ad hoc and routine communication, and a culture that promotes participatory action, shared decision-making, and collective goal-setting with a focus on patient-centred care.36,41,47,56,64 Trust within a team enhances willingness to share relevant information and engage in collaborative decision-making. It also fosters psychological safety by allowing individuals to express their opinions, offer suggestions, and challenge ideas without fear of judgment. This created an environment in which all the team members felt empowered and valued.43,77 Such openness and support are critical for effective problem solving and decision-making, ultimately leading to improved patient outcomes.57,58
Governance, Leadership, Team Structure and Role Clarity
The structural components of interdisciplinary collaboration are crucial to the overall effectiveness of the MTBC approach. Key factors such as governance, leadership, team structure, and role clarity are instrumental in shaping the functionality of the team and the efficiency with which patient care is provided.43,59,62 A well-defined governance framework offers essential guidance for decision-making, accountability, and the distribution of responsibilities within the team.36 This structure ensures that each team member is aware of who is responsible for specific decisions, the processes through which decisions are made, and a clear care plan,36,79 thereby reducing the likelihood of confusion and conflict. Investing in leadership capacity that enables MTBC is crucial for enhancing team cohesion, improving patient outcomes, and supporting the integration of care across settings.11,38,46,51 “Equally significant is the precise definition of roles within the team, as healthcare professionals often come from diverse educational backgrounds, each bringing distinct professional language, expertise, and approaches to care. These differences can create uncertainty regarding roles and boundaries, which may lead to role overlap, miscommunication, and diminished team effectiveness, ultimately compromising the collaborative process.43,63,69–71,73,79 This clarity enhances both individual and collective performance, ensuring that the team functions cohesively and optimally in delivering patient-centred care.80
Proposing a MTBC Enabling Model
Based on an understanding of the key factors that influence the success of multidisciplinary team-based care, a model for enabling MTBC is proposed, as shown in Figure 5. This model uses a patient-centred approach as the guiding principle in the design and funding of multidisciplinary primary care teams at the system level, with stakeholder engagement as the key strategy to enable effective MTBC across organisations within primary care, community, and social care settings. The proposed model emphasises the integration of key factors such as communication, collaboration, leadership and governance, patient-centred care, flexibility, and the development of a sustainable funding model with flexible reimbursement options. These components are critical for maintaining the longevity of the model and supporting the key success factors and elements of the MTBC.
 |
Figure 5 A proposed MTBC enabling model. |
Effective communication plays a central role, emphasising the importance of clear and thorough information exchange between team members within a patient-centred approach. A consistent information technology system is essential for effective communication in a multidisciplinary model. Shared patient records and a digital referral system allow timely, coordinated care, while integrated information systems support regular interdisciplinary meetings and transparent decision making.1,21 Leadership and governance are fundamental to the model’s success, with a clear governance framework that aligns shared goals and fosters a supportive participatory environment. Successful leadership encourages mutual respect and trust, breaks down traditional hierarchical structures, and promotes collaboration and team cohesion.12,58,72
The model must also be flexible and adaptable to respond to local needs and policy changes, while ensuring care coordination across providers. Continuous professional development and multidisciplinary learning equipment teams to deliver high-quality services.75 Effective stakeholder engagement strengthens service integration, reduces isolation, and fosters mutual reliance between team members and services.15,37 To ensure the effectiveness of the model, it should be guided by clear metrics and quality control measures, including disease registries for follow-up and patient monitoring, to ensure ongoing adaptability, efficiency, and sustainability. By integrating all key elements into a specific primary care context, the successful implementation of an adaptable MTBC model may lead to improved service delivery and outcomes in primary care.
Implications
The scoping review identified successful approaches and barriers to MTBC implementation in primary care contexts. The key factors that affect the MTBC model are applicable across sectors and organisations. MTBC can improve patient care and outcomes by fostering collaboration between general practitioners and diverse professionals, thus benefiting both patients and healthcare providers. The proposed MTBC-enabling model empowers patients, enhances the system capacity and efficiency, and drives innovation, ultimately contributing to stronger health systems and better community health. This study will inform further work on identifying the factors limiting the adoption of MTBC in general practice and the development of a sustainable and scalable model or models of MTBC aligned with relevant strategies and funding imperatives.
Limitations
Although the scoping review used a rigorous and transparent approach, systematically reviewing relevant studies and offering a critical evaluation and analysis of the results, it did not assess the quality of the articles. In addition, the scoping review potentially excluded relevant articles that were not published in English and those potentially missing valuable cultural perspectives. Overall, this review was useful in identifying the existing knowledge of multidisciplinary based team models in the primary care context which may not be applicable in hospital and acute settings.
Conclusion
This scoping review identified approaches and innovations in operationalising multidisciplinary team-based care (MTBC) in primary care settings, and the factors impacting MTBC success. An MTBC approach to the provision of primary care services is likely to affect access and equity for communities across all regions (remote, rural, regional, and metropolitan). The community’s need for primary care services is growing, the number of general practitioners is decreasing, particularly in rural and regional areas, and the hospital capacity is under pressure. By changing the skills mix in the primary care setting, the MTBC approach has proven effective in improving care processes, patient experience, service outcomes, team collaboration, and staff job satisfaction, thus enabling better preventive care and chronic disease management.
Data Sharing Statement
Data are available upon reasonable request to the corresponding author.
Ethical Approval
Ethical approval was not required for this study.
Patient and Public Involvement
Patients and the public were not involved in this research in any way.
Acknowledgments
We acknowledge the funding provided by Hunter New England and the Central Coast Primary Health Network for conducting the scoping review and the current manuscript. We also thank Emily Grahn for conducting abstract review during the scoping process.
Funding
Hunter New England and Central Coast Primary Health Network.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Australian Institute of Health and Welfare. Health system overview. Australian Institute of Health and Welfare; 2024 [updated June 17, 2024]. Available from: https://www.aihw.gov.au/reports/australias-health/health-system-overview.
2. World Health Organization. Primary health care. World Health Organization; 2024 [reviewed August 28, 2024]. Available from: https://www.who.int/news-room/fact-sheets/detail/primary-health-care.
3. Duckett S, Hunt J. Contemporary challenges for primary care. Aust Health Rev. 2023;47(2):135–136. doi:10.1071/AH23042
4. Wranik WD, Haydt SM. Funding models and medical dominance in interdisciplinary primary care teams: qualitative evidence from three Canadian provinces. Hum Resour Health. 2018;16(38):1–9. doi:10.1186/s12960-018-0299-3
5. Dale H, Lee A. Behavioural health consultants in integrated primary care teams: a model for future care. BMC Fam Pract. 2016;17:1–9. doi:10.1186/s12875-016-0485-0
6. Endalamaw A, Khatri RB, Erku D, et al. Barriers and strategies for primary health care workforce development: synthesis of evidence. BMC Prim Care. 2024;25(1):99. doi:10.1186/s12875-024-02336-1
7. Institute of Medicine, editor. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington (DC): National Academies Press; 2001.
8. Picker Institute, Europe. Picker principles of patient-centred care [Internet]. UK; [reviewed January 25, 2025]. Available from: https://picker.org/who-we-are/the-picker-principles-of-person-centred-care/.
9. Gerteis M, Edgman-Levitan S, Daley J, Delbanco TL. Through the Patient’s Eyes: Understanding and Promoting Patient-Centered Care. 1993.
10. World Health Organization. Integrated people-centred care [Internet]. World Health Organization; 2025 [reviewed January 25, 2025]. Available from: https://www.who.int/health-topics/integrated-people-centered-care#tab=tab_1.
11. Leach B, Morgan P, Strand de Oliveira J, Hull S, Østbye T, Everett C. Primary care multidisciplinary teams in practice: a qualitative study. BMC Fam Pract. 2017;18:1–10. doi:10.1186/s12875-017-0701-6
12. Green LV, Savin S, Lu Y. Primary care physician shortages could be eliminated through use of teams, nonphysicians, and electronic communication. Health Aff. 2013;32(1):11–19. doi:10.1377/hlthaff.2012.1086
13. Shipman SA, Sinsky CA. Expanding primary care capacity by reducing waste and improving the efficiency of care. Health Aff. 2013;32(11):1990–1997. doi:10.1377/hlthaff.2013.0539
14. Coskun S, Duygulu S. The effects of nurse-led transitional care model on elderly patients undergoing open heart surgery: a randomized controlled trial. Eur J Cardiovasc Nurs. 2022;21(1):46–55. doi:10.1093/eurjcn/zvab005
15. Markle-Reid M, Fisher K, Ganann R, Pollard C, Whitmore C. An integrated transitional care intervention improves patient-reported outcomes in older adults with stroke. Innov Aging. 2023;7(Supplement_1):642. doi:10.1093/geroni/igad104.2091
16. Department of Health and Aged Care. What primary health networks are in Australia? [Internet]. Commonwealth of Australia; 2021 [reviewed March 17, 2025]. Available from: https://www.health.gov.au/our-work/phn/what-PHNs-are.
17. Jessup RL. Interdisciplinary versus multidisciplinary care teams: do we understand the difference? Aust Health Rev. 2007;31(3):330–331. doi:10.3316/ielapa.391839420392843
18. Royal Australian College of General Practitioners. Collaboration and multidisciplinary team-based care.
19. Dobbins MI, Thomas SA, Melton S, Lee S. Integrated care and the evolution of the multidisciplinary team. Prim Care. 2016;43(2):177–190. doi:10.1016/j.pop.2016.01.003
20. Collet R, van Grootel J, van der Leeden M, et al. Facilitators, barriers, and guidance to successful implementation of multidisciplinary transitional care interventions: a qualitative systematic review using the consolidated framework for implementation research. Int J Nurs Stud Adv. 2025;8:100269. doi:10.1016/j.ijnsa.2024.100269
21. Mitchell GK, Burridge L, Zhang J, et al. Systematic review of integrated models of health care delivered at the primary–secondary interface: how effective is it and what determines effectiveness? Aust J Prim Health. 2015;21(4):391–408. doi:10.1071/PY14172
22. Mulvale G, Embrett M, Razavi SD. ‘Gearing up’ to improve interprofessional collaboration in primary care: a systematic review and conceptual framework. BMC Fam Pract. 2016;17(83):1–13. doi:10.1186/s12875-016-0492-1
23. Lamprell K, Arnolda G, Delaney GP, Liauw W, Braithwaite J. The challenge of putting principles into practice: resource tensions and real‐world constraints in multidisciplinary oncology team meetings. Asia Pac J Clin Oncol. 2019;15(4):199–207. doi:10.1111/ajco.13166
24. Lumenta DB, Sendlhofer G, Pregartner G, et al. Quality of teamwork in multidisciplinary cancer team meetings: a feasibility study. PLoS One. 2019;14(2):e0212556. doi:10.1371/journal.pone.0212556
25. Page AJ, Cosgrove D, Elnahal SM, Herman JM, Pawlik TM. Organizing a multidisciplinary clinic. Chin Clin Oncol. 2014;3(4):43. doi:10.3978/j.issn.2304-3865.2014.06.02
26. Seckler E, Regauer V, Rotter T, Bauer P, Müller M. Barriers to and facilitators of the implementation of multi-disciplinary care pathways in primary care: a systematic review. BMC Fam Pract. 2020;21(113):1–19. doi:10.1186/s12875-020-01179-w
27. Soukup T, Lamb BW, Morbi A, et al. Cancer multidisciplinary team meetings: impact of logistical challenges on communication and decision-making. BJS Open. 2022;6(4). doi:10.1093/bjsopen/zrac093
28. Supper O, Catala O, Lustman M, Chemla C, Bourgueil Y, Letrilliart L. Interprofessional collaboration in primary health care: a review of facilitators and barriers perceived by involved actors. J Public Health. 2015;37(4):716–727. doi:10.1093/pubmed/fdu102
29. Morabito A, Mercadante E, Muto P, et al. Improving the quality of patient care in lung cancer: key factors for successful multidisciplinary team working. Explor Target Antitumor Ther. 2024;5(2):260. doi:10.37349/etat.2024.00217
30. Ellis G, Sevdalis N. Understanding and improving multidisciplinary team working in geriatric medicine. Age Ageing. 2019;48(4):498–505. doi:10.1093/ageing/afz021
31. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
32. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;10(1). doi:10.1186/s13643-021-01626-4
33. Qualtrics. Customer satisfaction survey [Internet]. Queensland (AU); 2024 [cited February 6, 2025]. Available from: https://jcu.syd1.qualtrics.com/jfe/form/SV_9uzdnBHcFi9psWO.
34. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
35. Hawes EM, Smith JN, Pinelli NR, et al. Accountable care organizations and team-based care in primary care. Am J Manag Care. 2019;25(6):e175–e182.
36. Abdulrhim S, Sankaralingam S, Mohamed Ibrahim MI, et al. Collaborative care model for diabetes in primary care settings in Qatar: a qualitative exploration among healthcare professionals and patients who experienced the service. BMC Health Serv Res. 2021;21:1–12. doi:10.1186/s12913-021-06183-z
37. Ciccone MM, Aquilino A, Cortese F, et al. Feasibility and effectiveness of a disease and care management model in the primary health care system for patients with heart failure and diabetes (Project Leonardo). Vasc Health Risk Manag. 2010;6(1):297–305. doi:10.2147/vhrm.s9252
38. Smith-Carrier T, Neysmith S. Analyzing the interprofessional working of a home-based primary care team. Can J Aging. 2014;33(3):271–284. doi:10.1017/S071498081400021X
39. Suter E, Mallinson S, Misfeldt R, Boakye O, Nasmith L, Wong ST. Advancing team-based primary health care: a comparative analysis of policies in western Canada. BMC Health Serv Res. 2017;17:1–11. doi:10.1186/s12913-017-2439-1
40. Kirby A, Murphy A, Bradley C. Multi-disciplinary decision making in general practice. J Health Organ Manag. 2018;32(2):146–156. doi:10.1108/jhom-08-2017-0197
41. Bidwell S, Copeland A. A model of multidisciplinary professional development for health professionals in rural Canterbury, New Zealand. J Prim Health Care. 2017;9(4):292–296. doi:10.1071/HC17049
42. Grol SM, Molleman GRM, Kuijpers A, et al. The role of the general practitioner in multidisciplinary teams: a qualitative study in elderly care. BMC Fam Pract. 2018;19:1–7. doi:10.1186/s12875-018-0726-5
43. Drummond N, Abbott K, Williamson T, Somji B. Interprofessional primary care in academic family medicine clinics: implications for education and training. Can Fam Physician. 2012;58(8):e450–e8.
44. Mathews M, Hedden L, Lukewich J, et al. Adapting care provision in family practice during the COVID-19 pandemic: a qualitative study exploring the impact of primary care reforms in four Canadian regions. BMC Prim Care. 2024;25(1):1–9. doi:10.1186/s12875-024-02356-x
45. Lawn S, Lloyd A, King A, Sweet L, Gum L. Integration of primary health services: being put together does not mean they will work together. BMC Res Notes. 2014;7(1):66. doi:10.1186/1756-0500-7-66
46. Johnson P, Linzer M, Shippee ND, Heegaard W, Webb F, Vickery KD. Development and implementation of an interdisciplinary intensive primary care clinic for high-need high-cost patients in a safety net hospital. Popul Health Manag. 2020;23(2):124–131. doi:10.1089/pop.2019.0068
47. Fjaagesund SD, Graham W, Jones E, et al. Chiropractors in multidisciplinary teams: enablers of colocation integration in GP-led primary health care. Healthcare. 2024;12(9):926. doi:10.3390/healthcare12090926
48. Bunnell CA, Weingart SN, Swanson S, Mamon HJ, Shulman LN. Models of multidisciplinary cancer care: physician and patient perceptions in a comprehensive cancer center. J Oncol Pract. 2010;6(6):283–288. doi:10.1200/JOP.2010.000138
49. Christensen LD, Huibers L, Bro F, Christensen MB, Mygind A. Interprofessional team-based collaboration between designated GPs and care home staff: a qualitative study in an urban Danish setting. BMC Prim Care. 2023;24(1):3. doi:10.1186/s12875-023-01966-1
50. Gibbs C, Murphy B, Ratnaike D, Hoppe K, Lovelock H. Implementing a collaborative mental health care model: the MHPN. J Integr Care. 2017;25(4):237–246. doi:10.1108/JICA-06-2017-0014
51. Pullon S, Morgan S, Macdonal L, McKinlay E, Gray B. Observation of interprofessional collaboration in primary care practice: a multiple case study. J Interprof Care. 2016;30(6):784–794. doi:10.1080/13561820.2016.1220929
52. Purcell N, Zamora K, Tighe J, Li Y, Douraghi M, Seal K. The integrated pain team: a mixed-methods evaluation of the impact of an embedded interdisciplinary pain care intervention on primary care team satisfaction, confidence, and perceptions of care effectiveness. Pain Med. 2018;19(9):1748–1763. doi:10.1093/pm/pnx254
53. DeMiglio L, Williams A. Factors enabling shared care with primary health care providers in community settings: the experiences of interdisciplinary palliative care teams. J Palliat Care. 2012;28(4):282–289. doi:10.1177/082585971202800407
54. Lyson CH, Ackerman S, Lyles C, et al. Redesigning primary care in the safety net: a qualitative analysis of team-based care implementation. Healthcare. 2019;7:22–29. doi:10.1016/j.hjdsi.2018.09.004
55. Nieuwboer MS, Perry M, van der Sande R, Maasse ITHM, Olde Rikkert MGM, van der Marck MA. Identification of influencing factors and strategies to improve communication between general practitioners and community nurses: a qualitative focus group study. Fam Pract. 2018;35(5):619–625. doi:10.1093/fampra/cmy009
56. Reckrey JM, Soriano TA, Hernandez CR, et al. The team approach to home-based primary care: restructuring care to meet individual, program, and system needs. J Am Geriatr Soc. 2015;63(2):358–364. doi:10.1111/jgs.13196
57. Gardenier D, Woody A, Amory C, Weiss JJ. Interprofessional team-based approach to patients with chronic hepatitis C and personality disorder: three case studies. Arch Psychiatr Nurs. 2019;33(4):352–357. doi:10.1016/j.apnu.2019.02.001
58. Slåtsveen RE, Wibe T, Halvorsrud L, Lund A. Balancing between dual belongings when organised into interdisciplinary teams, with the trust model as the context: a qualitative study. BMC Prim Care. 2024;25(1):314. doi:10.1186/s12875-024-02554-7
59. Metzelthin SF, Daniels R, Rossum EV, et al. A nurse-led interdisciplinary primary care approach to prevent disability among community-dwelling frail older people: a large-scale process evaluation. Int J Nurs Stud. 2013;50(9):1184–1196. doi:10.1016/j.ijnurstu.2012.12.016
60. Caeiro C, Canhão H, Paiva S, et al. Interdisciplinary stratified care for low back pain: a qualitative study on the acceptability, potential facilitators, and barriers to implementation. PLoS One. 2019;14(11):e0225336. doi:10.1371/journal.pone.0225336
61. Cheong LH, Armour CL, Bosnic-Anticevich SZ. Multidisciplinary collaboration in primary care: through the eyes of patients. Aust J Prim Health. 2013;19(3):190–197. doi:10.1071/PY12019
62. Donaghy E, Huang H, Henderson D, Wang HH, Guthrie B, Mercer SW. Primary care transformation in Scotland: a qualitative study of GPs’ and multidisciplinary team members’ views. Br J Gen Pract. 2024;74(738):e1–e8. doi:10.3399/bjgp.2023.0086
63. Elissen AMJ, Van Raak AJA, Paulus ATG. Can we make sense of multidisciplinary co-operation in primary care by considering routines and rules? Health Soc Care Community. 2011;19(1):33–42. doi:10.1111/j.1365-2524.2010.00946.x
64. Weber CE, Kortkamp C, Maurer I, Hummers E. Boundary work in response to professionals’ contextual constraints: micro-strategies in interprofessional collaboration. Organ Stud. 2022;43(9):1453–1477. doi:10.1177/01708406221074135
65. Somé NH, Devlin RA, Mehta N, Zaric GS, Sarma S. Team-based primary care practice and physician’s services: evidence from family health teams in Ontario, Canada. Soc Sci Med. 2020;264:N.PAG–1. doi:10.1016/j.socscimed.2020.113310
66. Rosell L, Alexandersson N, Hagberg O, Nilbert M. Benefits, barriers and opinions on multidisciplinary team meetings: a survey in Swedish cancer care. BMC Health Serv Res. 2018;18(1):1. doi:10.1186/s12913-018-2990-4
67. Bissett SM, Preshaw PM, Presseau J, Rapley T. A qualitative study exploring strategies to improve the inter-professional management of diabetes and periodontitis. Prim Care Diabetes. 2020;14(2):126–132. doi:10.1016/j.pcd.2019.11.010
68. Chong JBK, Yap CYH, Tan SLL, Thong XR, Fang Y, Smith HE. General practitioners’ perceptions of the roles of community pharmacists and their willingness to collaborate with pharmacists in primary care. J Pharm Policy Pract. 2023;16(1):114. doi:10.1186/s40545-023-00613-5
69. Kooffreh-Ada M, Iheanacho OE, Nwagbara VI, et al. Case studies of multi-disciplinary team management of atypical gastric cancer: challenges and lessons learned (about two cases). Pan Afr Med J. 2023;45:113. doi:10.11604/pamj.2023.45.113.38579
70. Berkowitz SA, Eisenstat SA, Barnard LS, Wexler DJ. Multidisciplinary coordinated care for Type 2 diabetes: a qualitative analysis of patient perspectives. Prim Care Diabetes. 2018;12(3):218–223. doi:10.1016/j.pcd.2018.01.005
71. Naqvi D, Malik A, Al-Zubaidy M, et al. The general practice perspective on barriers to integration between primary and social care: a London, United Kingdom-based qualitative interview study. BMJ Open. 2019;9(8):e029702. doi:10.1136/bmjopen-2019-029702
72. Vegesna A, Coschignano C, Hegarty SE, et al. Attitudes towards physician-nurse collaboration in a primary care team-based setting: survey-based research conducted in the chronic care units of the Tuscany region of Italy. J Interprof Care. 2016;30(1):65–70. doi:10.3109/13561820.2015.1081878
73. Felder MM, Van De Bovenkamp HHM, Maaijen MMH, De Bont AAA. Together alone: organizing integrated, patient-centered primary care in the layered institutional context of Dutch healthcare governance. J Prof Organ. 2018;5(3):88–105. doi:10.1093/jpo/joy006
74. Kósa K, Katona C, Papp M, et al. Health mediators as members of multidisciplinary group practice: lessons learned from a primary health care model programme in Hungary. BMC Fam Pract. 2020;21(1):1–9. doi:10.1186/s12875-020-1092-7
75. Albarqi MN. Assessing the impact of multidisciplinary collaboration on quality of life in older patients receiving primary care: cross-sectional study. Healthcare. 2024;12(13). doi:10.3390/healthcare12131258
76. Gaboury I, Boon H, Verhoef M, Bujold M, Lapierre LM, Moher D. Practitioners’ validation of framework of team-oriented practice models in integrative health care: a mixed methods study. BMC Health Serv Res. 2010;10:289. doi:10.1186/1472-6963-10-289
77. Boorsma M, Frijters DH, Knol DL, et al. Effects of multidisciplinary integrated care on quality of care in residential care facilities for elderly people: a cluster randomized trial. CMAJ. 2011;183(11):E724–32. doi:10.1503/cmaj.101498
78. Wranik WD, Haydt SM, Katz A, et al. Funding and remuneration of interdisciplinary primary care teams in Canada: a conceptual framework and application. BMC Health Serv Res. 2017;17:1–12. doi:10.1186/s12913-017-2290-4
79. Giannitrapani KF, Soban L, Hamilton AB, et al. Role expansion on interprofessional primary care teams: barriers of role self-efficacy among clinical associates. Healthcare. 2016;4(4):321–326. doi:10.1016/j.hjdsi.2016.03.004
80. Liberati EG, Gorli M, Scaratti G. Invisible walls within multidisciplinary teams: disciplinary boundaries and their effects on integrated care. Soc Sci Med. 2016;150:31–39. doi:10.1016/j.socscimed.2015.12.002
81. Powell HA, Baldwin DR. Multidisciplinary team management in thoracic oncology: more than just a concept? Eur Respir J. 2014;43(6):1776–1786. doi:10.1183/09031936.00150813
82. Wang C, Li M, Huang Y, Xi X. Factors influencing clinical pharmacists’ integration into the clinical multidisciplinary care team. Front Pharmacol. 2023;14. doi:10.3389/fphar.2023.1202433
83. Mitchell GK, Young CE, Janamian T, et al. Factors affecting the embedding of integrated primary-secondary care into a health district. Aust J Prim Health. 2020;26(3):216–221. doi:10.1071/py18177
84. Debar LL, Kindler L, Keefe FJ, et al. A primary care-based interdisciplinary team approach to the treatment of chronic pain utilizing a pragmatic clinical trials framework. Transl Behav Med. 2012;2(4):523–530. doi:10.1007/s13142-012-0163-2
85. Alty J, Lawler K, Salmon K, et al. A new one-stop interdisciplinary cognitive clinic model tackles rural health inequality and halves the time to diagnosis: benchmarked against a national dementia registry. Int J Geriatr Psychiatry. 2023;38(8):1118–1126. doi:10.1002/gps.5988
86. Seaton J, Jones A, Johnston C, Francis K, D’Alesio AM, Rosen D. Facilitators of effective interprofessional collaborative practice for physiotherapy private practitioners: an interpretive descriptive study. J Interprof Educ Pract. 2023;33. doi:10.1016/j.xjep.2023.100671
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.