Back to Journals » Journal of Healthcare Leadership » Volume 17
Making Hospitals More Dementia Friendly: An Inclusive, User-Centered Approach
Authors Farsetta DL ![]() , Endicott SE, Woywod P, Bratzke LC
, Endicott SE, Woywod P, Bratzke LC
Received 25 October 2024
Accepted for publication 10 February 2025
Published 1 March 2025 Volume 2025:17 Pages 85—96
DOI https://doi.org/10.2147/JHL.S496288
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Russell Taichman
Diane L Farsetta,1,* Sarah E Endicott,1,* Paula Woywod,1,2 Lisa C Bratzke1
1School of Nursing, University of Wisconsin–Madison, Madison, WI, USA; 2UW Hospital and Clinics, Madison, WI, USA
*These authors contributed equally to this work
Correspondence: Diane L Farsetta, University of Wisconsin–Madison, 4149 Signe Skott Cooper Hall, University of Wisconsin–Madison, 701 Highland Ave, Madison, WI, 53705, USA, Email [email protected]
Purpose: People living with dementia and their care partners identify interactions with the healthcare system as among their greatest challenges. Many hospital staff do not feel prepared to care for people living with dementia. This contributes to poor outcomes for patients living with dementia, frustration and confusion for care partners, and distress for hospital staff.
Patients and Methods: An academic project team with expertise in education, geriatrics, simulation, and community engagement, who had previously developed dementia-friendly training materials for classroom and community use, designed a dementia-friendly hospital toolkit. Applying principles of user-centered design, the project team consulted with care partners of people living with dementia, hospital staff, hospital leadership, and advocates from communities disproportionately impacted by dementia to identify and address the needs of patients, care partners, hospital staff, and hospital leadership.
Results: The project team developed a dementia-friendly hospital toolkit, which includes training materials for hospital staff across roles and an organizational guide to facilitate uptake by a wide range of hospitals. In multiple rounds of pilot testing, hospital staff rated toolkit training activities highly, reporting new insights and applying the knowledge or skills gained in their professional roles. Five hospitals, ranging from large academic centers to rural critical access hospitals, used the toolkit to assess needs, develop plans, and organize training sessions for staff. All hospitals reported receiving positive feedback from staff, meeting staff learning objectives, and intending to continue using the toolkit to meet their dementia-friendly goals.
Conclusion: Following an inclusive, user-centered approach to developing dementia-friendly training materials allowed the project team to address the needs of key partners: people living with dementia, their care partners, hospital staff, and hospital leadership. Based on the positive responses from hospital pilot partners, the project team is supporting wider dissemination of the dementia-friendly hospital toolkit.
Keywords: dementia care, professional development, hospital, user-centered design
Introduction
The older adult population is projected to grow significantly, with the number of people over the age of 85 expected to double to 14.4 million by 2040.1 Age is the most important risk factor for dementia.2 Older adults represent 16% of the population, yet account for nearly 40% of hospitalizations.3,4 Many older adults (two out of five) admitted to hospitals have cognitive impairment, but only one-third of them have a dementia-related diagnosis in the medical record.4 Healthcare systems often struggle to provide acute care to people living with dementia and the need for such care is growing.
The unfamiliar and disorienting environments, loud noises, irregular schedules, and staff changes in hospitals can be challenging for anyone, but especially for people living with dementia.5 The added cognitive load of hospital environments can result in people living with dementia exhibiting challenging behaviors, or behaviors that staff may struggle to understand and respond to.6 Hospital care is focused on presenting diagnoses. When symptoms associated with dementia emerge, many hospital systems react by focusing on risk and disruptions to normal operations, rather than the underlying needs of the person living with dementia and their care partners.7 Hospital staff who do not have adequate dementia-specific training or support may respond to challenging behaviors with inappropriate medications or use of physical restraints.8
The repercussions for a growing number of hospital patients can be serious. Hospitalized older people with a diagnosis of dementia face a disproportionate risk of death and are more likely to experience complications such as dehydration, falls, poor nutrition, physical deconditioning, new infections, and delirium.9 Dementia-friendly initiatives are a potential strategy to mitigate these risks and improve hospital care. Such initiatives include training and other activities that aim to make the environment more supportive for those living with dementia.10 Dementia-friendly initiatives that focus on the autonomy, well-being, quality of life, social inclusion, and specific needs of people living with dementia offer an alternative to a deficit-oriented biomedical model of dementia care.11 Community members, non-profit organizations, and governmental bodies use dementia-friendly initiatives to support the social engagement and quality of life of people living with dementia.12
Following the project team’s development of a dementia-friendly toolkit for use in classrooms and the community,13 a large, academic medical center clinical partner voiced the need for dementia training materials specific to the hospital environment. A subsequent review of the literature documented that, while there was growing interest in dementia-friendly hospitals, there were no readily available resources for planning and implementing dementia-friendly strategies in hospitals in the United States.
Healthcare personnel report numerous challenges to working with people living with dementia.14 The most common challenges are communication with the person living with dementia and their care partner, and behavior and mood changes.15 In a noisy and fast-paced hospital environment, those living with dementia experience increased agitation and disorientation, disruption of their normal routines, and face stigma from staff.8 Lack of knowledge about dementia, basic understanding of person-centered care (PCC), and limited opportunities for in-service training are among the biggest barriers to providing high-quality care for people living with dementia in a hospital setting.14,16 Training programs have been piloted in acute care settings to address these challenges, but the literature is limited to interventions that focus only on nursing staff and have limited outcomes data.17,18 Poor uptake by hospital staff in some studies may be related to not engaging users and other key partners in the development of training materials.19
Dementia-friendly hospitals share many goals with other dementia-friendly initiatives. For example, dementia-friendly hospitals emphasize PCC, ie, seeing the person living with dementia as an individual, valuing them and their care partner, attempting to see the world from their point of view, and creating a positive physical and social environment that enhances their well-being.20 Therefore, the purpose of the current project was to develop and test a dementia-friendly toolkit for use in hospitals to provide more support for people living with dementia and their care partners.
Materials and Methods
Framework
Following institutional review board (IRB) protocol approval by the University of Wisconsin–Madison Minimal Risk IRB (2021–0755), the project team followed an inclusive, user-centered design approach to develop a dementia-friendly hospital toolkit (Figure 1). User-centered or human-centered design anchors the development of a product or program within an understanding of who will use it, why and how they will use it, and in what conditions they will use it.21 User feedback is incorporated throughout an iterative design and development process, including early stages when user needs and tasks are identified. Initially applied to software development, user-centered design has been adopted widely to increase product usefulness, effectiveness, usability, and acceptability.21 In healthcare, user-centered design approaches have been shown to reduce treatment errors and operational expenses, and to improve efficiency.22
 |
Figure 1 A user-centered design process. |
Project Input
Project Advisory Committee
In alignment with user-centered design principles, the project team convened a project advisory committee that met quarterly over two years. The purpose of this committee was not to participate in the project, but to provide critical insights to the project team throughout the design and development of dementia-friendly training materials.
The project advisory committee of 14 members included hospital staff who lead education services, oversee dementia education and outreach, coordinate care, connect patients with social services, and direct services for older patients. Also participating were a state-level health services department leader who helped develop the state’s dementia capable plan, an Alzheimer’s Association Latino-focused community outreach specialist, a member of the local Black Leaders for Brain Health Committee, a training specialist from a state-specific dementia community organization, and a dementia advocate and West African immigrant who owns and manages a culturally responsive home care agency. Committee members provided feedback on draft materials, assisted in evaluation of efforts, identified opportunities to further project goals, and advised on disseminating the dementia-friendly hospital toolkit. The project advisory committee members were offered reimbursement for their time.
Care Partners
Care partners of people living with dementia who had been hospitalized within the last two years were recruited to provide perspectives on how hospital staff interacted with their family members. They were recruited to participate in virtual focus group sessions via newsletters, social media posts, and invitations from community organization partners. Recruitment materials were translated into Spanish to allow for a more inclusive recruitment effort. Interested care partners were provided with a project information sheet per IRB protocol and filled out a screener survey. They documented consent via the survey and through participation in the focus group session (ie, participants stayed for the focus group when given the option not to participate). During the focus groups, we asked care partners about their family members entering the emergency department (ED) or being admitted to the hospital, their time in the ED or hospital, and their leaving the ED or being discharged from the hospital.
Hospital Staff
To ensure input from staff working in varied hospital settings, the project team recruited five hospitals as pilot partners, from urban academic centers to rural critical access hospitals. The hospital pilot partners circulated the hospital staff survey to clinical and non-clinical staff members, made staff available to participate in draft role-play scenario training sessions, provided feedback on draft scripts for training videos, and provided feedback on a draft toolkit table of contents.
Hospital staff across roles were recruited to provide feedback related to their experiences of caring for or interacting with patients living with dementia and their care partners. Hospital staff members were provided with a project information sheet at the beginning of the survey per IRB protocol and documented consent through continued participation in the survey (ie, clicking “next” to move to the survey questions). Each staff member completed an eight-item survey distributed by contacts at hospitals of various sizes, as well as statewide hospital and healthcare organizations. The survey asked for the staff member’s title and position at the hospital followed by questions regarding duration of time working with people living with dementia; staff perceptions of challenges that people living with dementia and their care partners face in a hospital setting; tools or resources needed by hospital staff to improve care for this population; and preferred delivery methods for training. One open-ended question sought additional input.
Hospital Education Leads
The project team also held a focus group with staff education leaders at three hospitals, including a Veteran’s Administration hospital, a large urban level I trauma center, and a rural independent not-for-profit hospital. Focus group questions explored how participants evaluate potential new training programs, what characteristics contribute to the effectiveness and sustainability of training programs at their hospital, and their feedback on the planned components of the dementia-friendly hospital toolkit.
Data Analysis
In designing the toolkit, the project team drew on their expertise in clinical care, simulation, teaching, and co-creation of training materials. To identify necessary and useful toolkit content, the project team analyzed and synthesized information from the hospital education leads focus group, hospital staff survey, interviews with contacts at two hospitals that had developed their own dementia-friendly programs, and published studies of dementia training programs for acute care settings.14,23–25 During care partner focus group sessions, a designated project team member took extensive notes. Session notes were distributed among project team members, who identified challenges faced by care partners during their interactions with hospital settings/staff. Hospital survey data were analyzed using descriptive statistics and counts for open-ended questions. The project team reviewed notes from the care partner focus groups and challenges documented in the hospital survey to develop a comprehensive list of challenges.
Development of Materials
Development of materials followed the user-centered design framework. For the five training videos, learning objectives and scripts were drafted based on the comprehensive list of challenges described above. Contacts at the five hospital pilot partners and advisory committee members reviewed and provided feedback on draft scripts prior to filming the videos. Based on partners’ input, the videos combined informative narration with hospital scenes illustrating best practices.
The training handouts, additional resources, and other toolkit content were drafted based on input gathered throughout the user-centered design process, along with relevant literature. Each section of the toolkit was reviewed by at least one expert, including hospital pilot partner contacts, project advisory committee members, and professionals in healthcare and allied fields who have experience of dementia-friendly initiatives.
Pilot Testing
The project team conducted five initial pilot tests with the eight role-play scenarios: three sessions with Doctor of Nursing Practice graduate students, one with interdisciplinary health sciences students, and one with speech therapy graduate students. The experiences leading people through the scenarios and students’ feedback identified ways in which to improve the presentation and scripting of the scenarios, as well as the structure of the debrief discussions.
After these improvements were made, the project team traveled to the five pilot partner hospitals to lead their staff through the role-play scenarios. Each hospital made available two groups of six people, including clinical and non-clinical staff members. Across these ten pilot sessions, each of the eight role-play scenarios was piloted at least once.
During each pilot session, the project team introduced themselves and the project; described the role-play scenario, learning objectives, and simulation equipment; gave hospital staff time to read a description of their role and act out the scenario in small groups; led a debriefing discussion; and administered an anonymous survey to collect immediate feedback. One of the project team members captured additional feedback by taking notes while staff participated in and discussed each role-play scenario. One month after each pilot session, the project team emailed hospital staff participants an online survey asking about the relevance of the training and their use of the knowledge or skills gained.
Hospital staff provided positive feedback on the role-play scenarios. They identified potential improvements, including giving all participants time to try on the simulation equipment at the beginning of a session, acknowledging at the start of debrief discussions when scenarios portray poor outcomes, and providing handouts specific to each scenario that summarize best care practices.
Following initial pilot testing and development of the full dementia-friendly hospital toolkit, the project team recruited five hospitals for a second round of pilot testing. Four of these hospitals had participated in initial pilot testing. Each hospital used the toolkit to develop its own dementia-friendly plan and carry out at least two training activities with hospital staff. Hospital pilot partners met with the project team at two time points, as detailed below.
For this second round of pilot testing, hospital partners agreed to:
- Use section two of the dementia-friendly hospital toolkit to create a plan for their hospital.
- Meet with the project team to review their dementia-friendly plan and answer questions about the planning process.
- Carry out at least two training activities with hospital staff, based on their plan and using any toolkit materials (role-play scenarios, training videos, and/or worksheets).
- Collect participant feedback after each training activity.
- Meet with the project team to share participant feedback and answer questions about the training activities.
The five hospitals assembled committees of between 2 and 16 people to develop a customized dementia-friendly plan using the toolkit. Additional information collected to guide their planning included staff surveys, statewide data on dementia care needs, and information from previous dementia-related training.
Results
Care Partner Focus Groups
Thirty-nine care partners completed a short screener survey. Based on their survey responses, 15 care partners from rural and urban communities across the state who had extensive hospital experience with family members living with dementia were invited to take part in focus group interviews. Reasons survey respondents were not invited to participate in a focus group included them not having been able to visit their family member in the hospital (three people); the care setting described not being a hospital (two people); the hospitalized relative not living with dementia (one person); the hospital being out of state (one person); and not completing the survey (four people). Ten care partners participated in two virtual focus group interviews. The ten care partners represented a range of geographic communities and different familial relationships with the person living with dementia. Nearly all identified as white, and one identified as Hispanic.
The project team analyzed care partners’ comments and identified six common challenges: inadequate hospital support for care partners; barriers to care partners’ access to the hospital; transitions of care; need for positive communication with people living with dementia; lack of dementia-specific education for healthcare workers; and the hospital environment, including sights, sounds, and physical spaces.
Hospital Staff Survey
The survey was completed by 315 hospital staff. Of the 315 surveys collected, 142 (45%) respondents did not indicate their role in the hospital and 28 (9%) selected “other”. The remaining respondents represented a variety of staff roles (see Table 1).
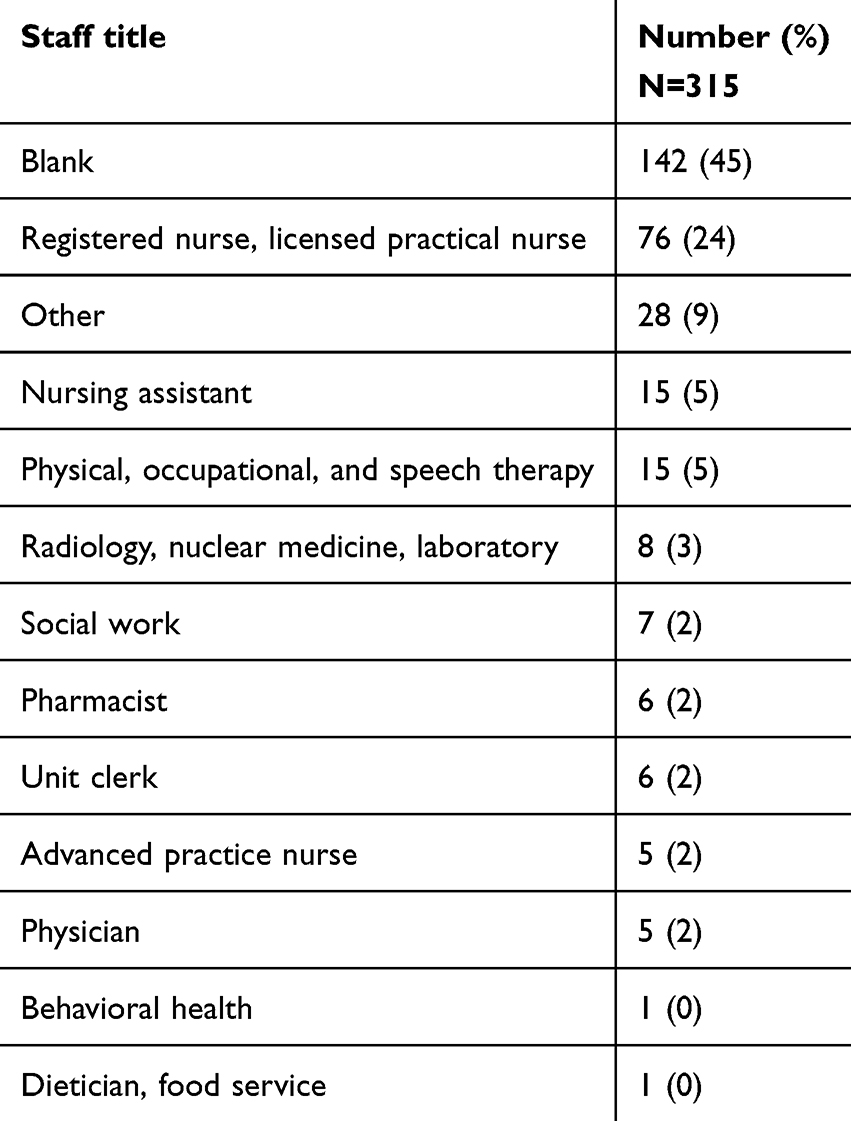 |
Table 1 Hospital Staff Survey Respondents |
The following challenges facing hospital patients living with dementia were identified by 171 staff respondents: stress from an unfamiliar environment (44%); physical symptoms such as confusion, untreated pain, or delirium (37%); and hospital staff having limited dementia-specific training or skills (30%). Asked about the challenges facing care partners, 160 staff respondents (42%) identified the overwhelming nature of an acute crisis and resulting emotional distress and 21% identified knowledge deficits.
Asked what tools or resources hospital staff need to care for people living with dementia and support their care partners, 136 staff respondents cited a need for training, specifically on communication strategies, types of dementia, de-escalation techniques, and managing behaviors (41%). Other needs included additional care staff, greater access to social workers and specialty-trained consultants, and more volunteers (20%). Other needed resources identified by hospital staff included adaptive equipment; activities suitable for people living with dementia; and environmental changes such as more home-like rooms, weighted blankets, spaces for wandering, and door signs or symbols to help with wayfinding (26%).
Hospital Education Leads Focus Group
Asked about materials necessary for a successful dementia-friendly training program, the three hospital education leads emphasized the need for tangible, accessible, and easily shared resources, such as handouts, worksheets, checklists, and training videos. They suggested that the toolkit outline options for training sessions of different lengths of time; for example, what could be covered in a 10-minute versus 30-minute training session. The education leads suggested including guidance on evaluating the impacts of a dementia-friendly hospital training program and on relating the initiative to broader hospital goals, such as staff knowledge and attitudes, patient and caregiver satisfaction, and readmission prevention.
Dementia-Friendly Hospital Toolkit Design
The dementia-friendly hospital toolkit table of contents included the following sections:
- Introductory material, including a definition of “dementia-friendly” and its importance in hospital settings;
- Planning for your hospital, including guidance on building leadership support, setting goals, and establishing dementia-friendly champions programs;
- Role-play scenarios, including options for structuring sessions and facilitator tips;
- Training videos, including learning objectives;
- Training handouts, including tip sheets, worksheets, and checklists; and
- Additional resources, including a planning flowchart, guidance on engaging care partners, sample surveys to evaluate training sessions, and how dementia-friendly hospital training aligns with the Age-Friendly Health Systems Initiative.
The project advisory committee reviewed and provided feedback on the draft toolkit table of contents. Changes made to incorporate their suggestions included emphasizing the importance of getting input from different hospital departments and staff roles when planning; organizing handouts in a separate section; and listing options for ongoing learning opportunities, such as staff meetings and newsletters.
People consulted throughout the user-centered design process, including the five hospital pilot partners, stressed that the toolkit should help users develop training plans customized for their hospital. Therefore, the project team included a robust planning section that walks users through creating a year-long plan that is responsive to their hospital’s challenges, dementia care goals, and training opportunities.
The toolkit’s planning section included information on the following, together with case studies from three hospitals:
- Building leadership support
- Getting input from staff with different roles and in different departments
- Identifying needs and setting training goals
- Finding opportunities in your hospital
- Building a dementia-friendly champions program
- Designing your training program
- Measuring progress
- Communicating with internal and external audiences
- Sustaining efforts over time
- Connecting with community organizations
The toolkit’s five training videos are described in Table 2, including titles and learning objectives.
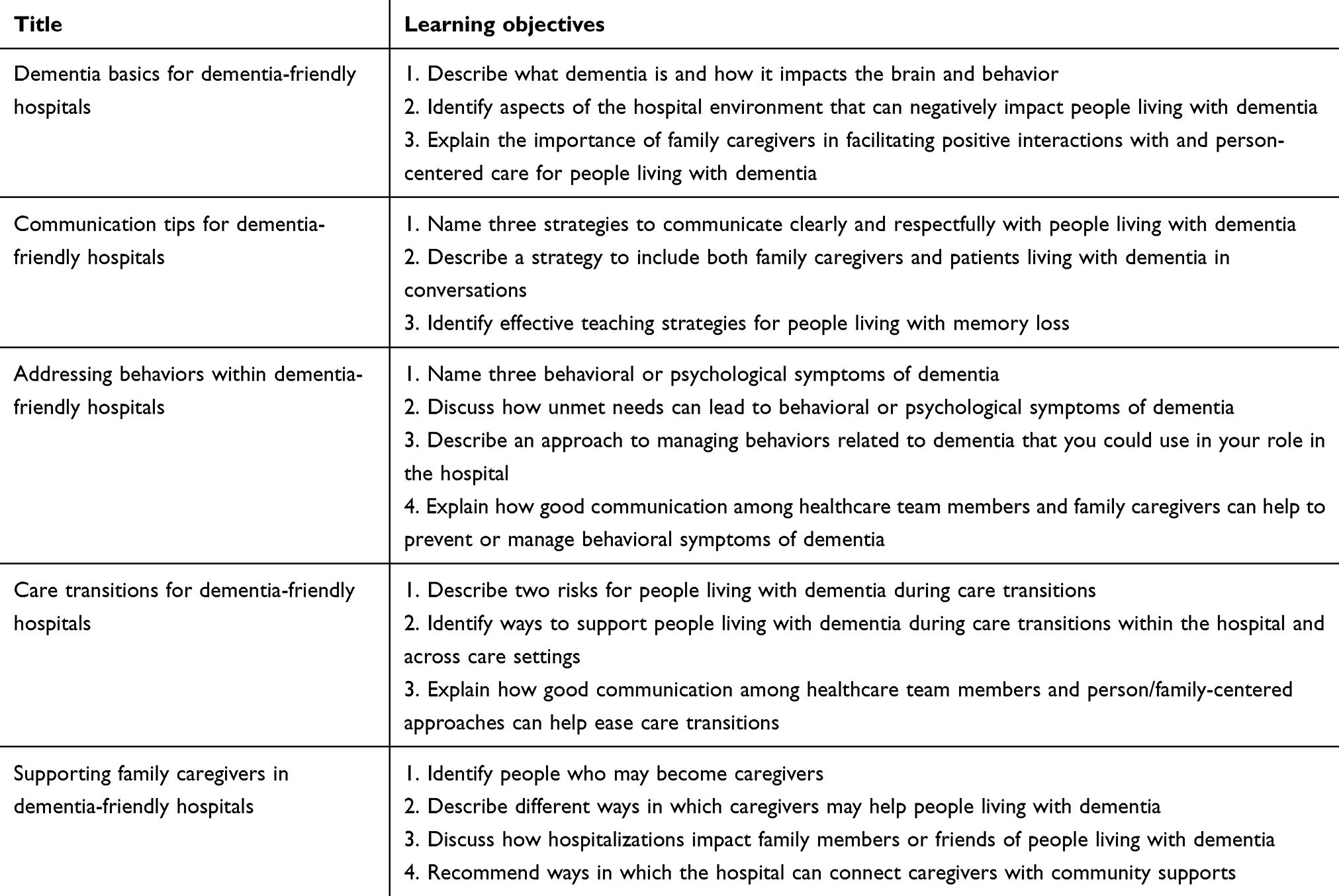 |
Table 2 Training Video Titles and Learning Objectives |
Pilot Testing
In response to the surveys administered at the end of the sessions piloting the role-play scenarios with hospital staff:
- 58 of 59 (98%) hospital staff participants agreed or strongly agreed that the learning objectives for the role-play scenario had been met;
- 50 of 59 (85%) hospital staff reported that their general expectations for the training session had been met; and
- 44 of 59 (75%) hospital staff rated the training session as excellent or very good.
In response to the surveys emailed one month after the pilot sessions, 13 of 24 (54%) hospital staff reported that they had since used knowledge or skills gained during the session in their professional roles. An additional five of 24 (21%) were unsure whether they had done so.
Asked how the training was informing their work, several hospital staff wrote about increased awareness of the experiences and needs of patients living with dementia and their care partners. One person reported being “more mindful of a patient’s surroundings and how the environment may impact” treatment. Another said that they “understand better what is happening to these patients and how hard it is for them to focus”. A third wrote that they had “a better understanding [of] healthcare experiences and environments from the patient perspective”.
Examples of how hospital staff feedback was incorporated into the role-play scenarios included:
- Encouraging all participants to try on the vision-limiting goggles and MP3 player headphones used to simulate dementia by limiting sensory input and adding distractions;
- Including lines for all roles on scenario scripts with one role highlighted, rather than just lines for one role and names indicating when other roles speak; and
- Developing handouts matched to each role-play scenario and training video that reinforce key points and best practices.
During the second pilot utilizing the complete dementia-friendly hospital toolkit, hospitals used various approaches to identify which topics to cover and staff to involve in their training sessions (see Table 3).
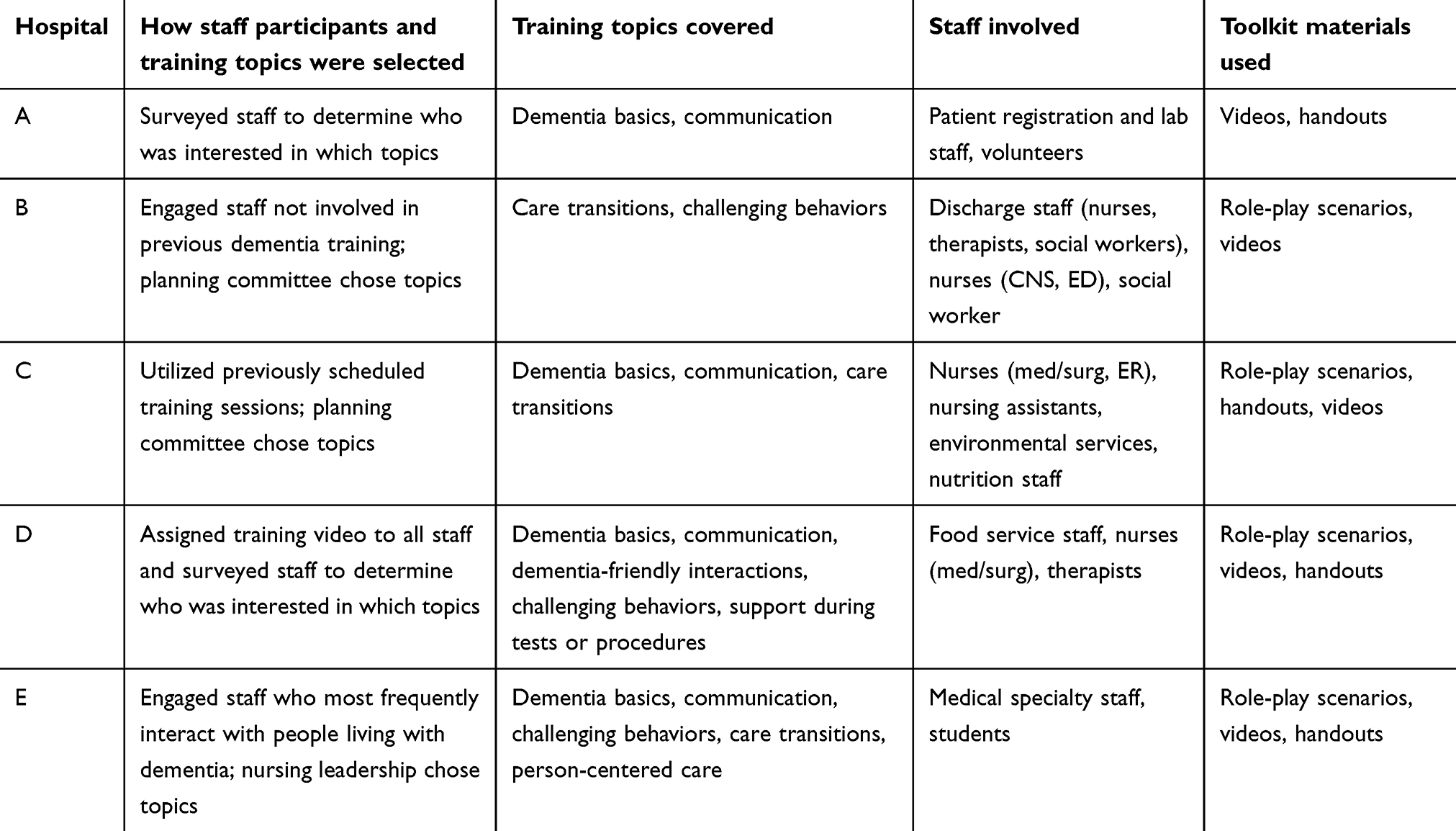 |
Table 3 Hospital Use of the Toolkit for Dementia-Friendly Planning and Training |
All five hospitals reported high staff satisfaction and met learning objectives for the dementia-friendly training sessions. See Table 3 for a list of staff, topics, and toolkit materials utilized in the sessions. Hospitals reported staff experiencing “lots of lightbulb moments”, applying dementia-friendly principles to their specific roles and reflecting on varied challenges that hospital environments present for people living with dementia. One contact at a pilot partner hospital said of the toolkit, “It takes you out of the medical model ‘I’m here to fix everything’ mindset to a person-centered perspective.” Four of the five hospitals used the toolkit surveys to evaluate their training sessions. All five hospitals valued the flexibility of approaches and intend to continue using the dementia-friendly hospital toolkit.
Hospitals participating in the second round of pilot testing described receiving support from their leadership and reported not needing additional resources for the training sessions. Still, they experienced challenges, including scheduling training sessions given the many demands on staff time, facilitating debriefing discussions if only a few people were participating in the session, and matching training materials to staff skill level and experience with people living with dementia.
Discussion
The number of people living with dementia is increasing. Further, age and several common chronic conditions are risk factors for dementia, increasing the likelihood of hospitalization for this vulnerable group. This project employed a user-centered approach to developing dementia friendly-training materials for hospital staff across roles, engaging potential users and other key partners throughout an iterative design process. Care partners, hospital staff, and others involved described challenges during hospitalization, as well as opportunities to improve care, communication, and support for people living with dementia and their care partners.
Initial feedback on the dementia-friendly hospital toolkit has been positive. Data from the second round of pilot testing suggests that the toolkit facilitates the planning and implementation of customized training sessions that are well received by staff and relevant to the challenges that they face when providing care or otherwise interacting with patients living with dementia. Hospital partners have commented on the toolkit’s usability, flexibility, and comprehensive materials. Potential future assessments of toolkit effectiveness include staff knowledge and attitudes towards people living with dementia, and the impact of training sessions on patient and family satisfaction and hospital readmission rates.
Hospitals considering dementia-friendly training may ask, as have some of this project’s hospital pilot partners: What are the criteria for designating a hospital as dementia-friendly? Who decides? This designation could provide an important indicator of quality, enhancing patient and family trust and demonstrating responsiveness to community needs.
Unlike Age Friendly Health Systems,26 which is a national initiative with a defined recognition process, dementia-friendly initiatives are often led by grassroots coalitions, with varying priorities shaped by local needs. The project team relies on the experience and perspectives of dementia-friendly communities and other dementia-friendly initiatives for guidance. Aspects common across dementia-friendly initiatives include the following:27
- Including people living with dementia and their care partners and centering their experiences;
- Making a commitment across sectors of a community or parts of an organization to support the participation and well-being of people living with dementia; and
- Promoting understanding, combating stigma, and building skills to respectfully engage people living with dementia.
In the project team’s region, dementia-friendly community groups offer training to local businesses, government agencies, and other public-facing entities, such as the city bus system. These local dementia-friendly initiatives require businesses to train at least half of their frontline staff and offer refresher training each year.28
Dementia-friendly signs, such as the purple angel symbol used internationally29 or other forms of public recognition, can encourage organizations to participate in dementia-friendly initiatives, while broadly communicating the importance of valuing and engaging people living with dementia. However, there are criticisms of this approach. These include the difficulty of setting appropriate criteria for “dementia friendliness” and concerns that doing so encourages a focus on “ticking boxes” rather than changing attitudes and behaviors.30
There is wide agreement on the need for dementia-specific training opportunities for healthcare staff. The strengths of this project’s work in terms of developing a dementia-friendly hospital toolkit include the emphasis on user-centered design, involving hospital leaders, hospital staff, care partners, and advocates of people living with dementia. The project team grounded the training materials on person-centered care and dementia-friendly principles, drawing on experiences collaborating with local dementia-friendly community groups over a decade. All training materials were drafted to reflect common challenges described to the project team by care partners and hospital staff, and further refined after piloting and/or review by people with relevant expertise, including lived experience. The project advisory committee was comprised of a diverse sample of dementia-friendly community leaders, providing multifaceted feedback on the materials developed.
Limitations
While the toolkit represents an innovative approach to developing training materials for hospital staff across roles, the project team acknowledges limitations in the approach. The hospital staff and leadership, service providers, family care partners, and advocates who provided input are all English speakers who reside in the same US state. The project team relied on care partners to share accounts of recent hospitalization experiences of people living with dementia. Despite developing recruitment materials in English and Spanish and sharing them with a variety of community organizations, almost all of the care partners who participated in the focus groups identified as white. To ensure participation by more diverse and representative samples of people living with dementia and their care partners, future work should allocate more time and resources to community partnerships and recruitment.
Conclusion
An inclusive, user-centered design approach to developing dementia-friendly training materials for hospital staff across roles was used for this project. The results demonstrate how input from people with different roles, perspectives, and areas of expertise can be synthesized to develop a robust educational program. Experiences shared by care partners of people living with dementia informed toolkit training materials on how hospital staff can engage and support care partners. Care partners’ input also shaped role-play scenarios and hospital scenes in the training videos, which hospital staff often called relatable and realistic. Surveys of hospital staff identified common challenges, as well as resources that they either currently use or felt would improve their ability to care for people living with dementia. Hospital education leads and project advisory committee members provided concrete suggestions to make dementia-friendly training programs more accessible to a wide range of hospitals. The hospitals participating in the project’s second round of pilot testing proved that the toolkit can be used to develop dementia-friendly plans that reflect the needs and priorities of each hospital. The project team will use information gathered from partners to guide toolkit dissemination and help hospitals pursue dementia-friendly goals.
Acknowledgments
Development of the dementia-friendly hospital toolkit was funded by the Oscar Rennebohm Foundation in Madison, WI. The project was reviewed and approved by the University of Wisconsin–Madison Institutional Review Board as minimal risk research (#2021-0755). The authors would like to thank the hospitals that participated in pilot testing: University of Wisconsin Health (UW-Health), Bellin Health, Cumberland Healthcare, Essentia Health St. Mary’s Hospital, Fort Memorial Health, and Gundersen Health.
Disclosure
The authors report no conflicts of interest in this work.
References
1. 2020 profile of older Americans. Washington DC: The Administration for Community Living; 2021. Available from: https://acl.gov/sites/default/files/aging%20and%20Disability%20In%20America/2020Profileolderamericans.final_.pdf.
2. Daviglus ML, Bell CC, Berrettini W, et al. NIH state-of-the-science conference statement: preventing Alzheimer’s disease and cognitive decline. NIH Consens State Sci Statements. 2010;27(4):1–30.
3. Number, percent distribution, rate, days of care with average length of stay, and standard error of discharges from short-stay hospitals, by sex and age: United States, 2010. Washington DC: Centers for Disease Control and Prevention; 2009. Available from: https://www.cdc.gov/nchs/data/nhds/2average/2009ave2_ratesexage.pdf.
4. Jackson TA, MacLullich AM, Gladman JR, Lord JM, Sheehan B. Undiagnosed long-term cognitive impairment in acutely hospitalised older medical patients with delirium: a prospective cohort study. Age Ageing. 2016;45(4):493–499. doi:10.1093/ageing/afw064
5. Naef R, Ernst J, Bürgi C, Petry H. Quality of acute care for persons with cognitive impairment and their families: a scoping review. Int. J Nurs Stud. 2018;85:80–89. doi:10.1016/j.ijnurstu.2018.05.006
6. Duah-Owusu White M, Kelly F. A narrative review of staff views about dementia care in hospital through the lens of a systems framework. J Res Nurs. 2023;28(2):120–140. doi:10.1177/17449871221142104
7. Nakahira M, Moyle W, Creedy D, Hitomi H. Attitudes toward dementia-related aggression among staff in Japanese aged care settings. J. Clin Nurs. 2009;18(6):807–816. doi:10.1111/j.1365-2702.2008.02479.x
8. Digby R, Lee S, Williams A. The experience of people with dementia and nurses in hospital: an integrative review. J Clin Nurs. 2017;26(9–10):1152–1171. doi:10.1111/jocn.13429
9. Fogg C, Griffiths P, Meredith P, Bridges J. Hospital outcomes of older people with cognitive impairment: an integrative review. Int J Geriatr Psychiatry. 2018;33(9):1177–1197. doi:10.1002/gps.4919
10. Dementia-friendly initiatives [webpage]. Geneva, Switzerland: World Health Organization; n.d.. Available from: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/5206#:~:text=Dementia%2Dfriendly%20initiatives%20and%20activities,age%2D%20and%20dementia%2Dfriendly.
11. Hebert CA, Scales K. Dementia friendly initiatives: a state of the science review. Dementia. 2019;18(5):1858–1895. doi:10.1177/1471301217731433
12. Lin SY. ‘Dementia-friendly communities’ and being dementia friendly in healthcare settings. Curr Opin Psychiatry. 2017;30(2):145–150. doi:10.1097/YCO.0000000000000304
13. Bratzke L, Endicott SE, Farsetta D, Woywood P, Zellman A. Dementia Friendly Toolkit: Role Play Simulations for Care and Community Settings. Center for Aging Research and Education, University of Wisconsin-Madison School of Nursing; 2018. https://care.nursing.wisc.edu/dementia-friendly-toolkit/.
14. Galvin JE, Kuntemeier B, Al-Hammadi N, Germino J, Murphy-White M, McGillick J. ”Dementia-friendly hospitals: care not crisis”: an educational program designed to improve the care of the hospitalized patient with dementia. Alzheimer Dis Assoc Disord. 2010;24(4):372–379. doi:10.1097/WAD.0b013e3181e9f829
15. Hetland B, McAndrew N, Perazzo J, Hickman R. A qualitative study of factors that influence active family involvement with patient care in the ICU: survey of critical care nurses. Intensive Crit Care Nurs. 2018;44:67–75. doi:10.1016/j.iccn.2017.08.008
16. Surr CA, Smith SJ, Crossland J, Robins J. Impact of a person-centred dementia care training programme on hospital staff attitudes, role efficacy and perceptions of caring for people with dementia: a repeated measures study. Int J Nurs Stud. 2016;53:144–151. doi:10.1016/j.ijnurstu.2015.09.009
17. Scerri A, Innes A, Scerri C. Dementia training programmes for staff working in general hospital settings - a systematic review of the literature. Aging Mental Health. 2017;21(8):783–796. doi:10.1080/13607863.2016.1231170
18. Surr CA, Gates C. What works in delivering dementia education or training to hospital staff? A critical synthesis of the evidence. Int J Nurs Stud. 2017;75:172–188. doi:10.1016/j.ijnurstu.2017.08.002
19. Toye C, Slatyer S, Quested E, et al. Obtaining information from family caregivers to inform hospital care for people with dementia: a pilot study. Int J Older People Nurs. 2019;14(1):e12219. doi:10.1111/opn.12219
20. Røsvik J, Rokstad AMM. What are the needs of people with dementia in acute hospital settings, and what interventions are made to meet these needs? A systematic integrative review of the literature. BMC Health Serv Res. 2020;20(1):723. doi:10.1186/s12913-020-05618-3
21. Notes on user centered design process [webpage]; 2004. Available from: https://www.w3.org/WAI/redesign/ucd.
22. Chandran S, Al-Sa’di A, Ahmad E. Exploring user centered design in healthcare: a literature review.
23. Chater K, Hughes N. Strategies to deliver dementia training and education in the acute hospital setting. J Res Nurs. 2013;18(6):578–593. doi:10.1177/1744987112446242
24. Karrer M, Schnelli A, Zeller A, Mayer H. A systematic review of interventions to improve acute hospital care for people with dementia. Geriatr Nurs. 2021;42(3):657–673. doi:10.1016/j.gerinurse.2021.03.006
25. Manietta C, Purwins D, Reinhard A, Knecht C, Roes M. Characteristics of dementia-friendly hospitals: an integrative review. BMC Geriatr. 2022;22(1):468. doi:10.1186/s12877-022-03103-6
26. Age-friendly health systems [webpage]. Boston: Institute for Healthcare Improvement; n.d.. Available from: https://www.ihi.org/initiatives/age-friendly-health-systems.
27. Shannon K, Bail K, Neville S. Dementia-friendly community initiatives: an integrative review. J Clin Nurs. 2019;28(11–12):2035–2045. doi:10.1111/jocn.14746
28. Dane county dementia friendly community impact report [report]. Madison, WI: Aging and Disability Resource Center of Dane County; 2019. Available from: https://www.daneadrc.org/documents/pdf/2019-DFC-Impact-Report.pdf.
29. The purple angel dementia awareness campaign [webpage]. Devon, UK: Norman McNamara, Design, Colours & Content; n.d.. Available from: https://purpleangel-global.com/.
30. Prior P; North East Dementia Alliance (UK). Knowing the foundations of dementia friendly communities for the North East. 2012. Available from: https://old.the-debenham-project.org.uk/downloads/articles/2012/dementiacommunities.pdf.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.