Back to Journals » Journal of Asthma and Allergy » Volume 13
Major Pollen Allergen Components and CCD Detection in Bermuda Grass Sensitized Patients in Guangzhou, China
Authors Liao C ![]() , Liang C, Hu H, Luo W, Wu G, Huang Z
, Liang C, Hu H, Luo W, Wu G, Huang Z ![]() , Wu L, Sun B
, Wu L, Sun B ![]()
Received 19 August 2020
Accepted for publication 20 October 2020
Published 16 November 2020 Volume 2020:13 Pages 615—623
DOI https://doi.org/10.2147/JAA.S277704
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Chenxi Liao,* Cuiying Liang,* Haisheng Hu,* Wenting Luo, Ge Wu, Zhifeng Huang, Liting Wu, Baoqing Sun
Department of Allergy and Clinical Immunology, State Key Laboratory of Respiratory Disease, National Clinical Research Center of Respiratory Disease, Guangzhou Institute of Respiratory Health, First Affiliated Hospital of Guangzhou Medical University, Guangzhou Medical University, Guangzhou, Guangdong 510120, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Baoqing Sun
State Key Laboratory of Respiratory Disease, National Clinical Research Center of Respiratory Disease, Guangzhou Institute of Respiratory Health, First Affiliated Hospital of Guangzhou Medical University, Guangzhou Medical University, 151 Yanjiangxi Road, Guangzhou, Guangdong 510120, People’s Republic of China
Tel +86 20 8306 2865
Fax +86 20 8306 2729
Email [email protected]
Objective: Bermuda grass pollen is a common inhaled allergen. The aim of this study was to investigate the molecular sensitization patterns to major pollen allergens (Bermuda grass, Mugwort and Timothy grass) and cross-reactive carbohydrate determinants (CCD) in Bermuda grass sensitized patients in southern China.
Methods: Serum specific IgE (sIgE) levels of Bermuda grass allergen components (Cyn d 1 and Cyn d 12), Timothy grass allergen components (Phl p 1, Phl p 4, Phl p 5, Phl p 7 and Phl p 12), Mugwort allergen components (Art v 1, Art v 3 and Art v 4) and CCD were detected in 78 patients sensitized to Bermuda grass via EUROBlotMaster system.
Results: Compared with CCD-positive patients, those with negative CCD results had significant higher positive rates of Cyn d 1 (47.8% vs 14.5%), Phl p 1 (26.1% vs 7.3%), Phl p 12 (21.7% vs 3.6%) and Art v 4 (26.1% vs 3.6%) (all p < 0.05). Patients < 18 years old had the highest positive rate of Cyn d 1 (40.7%). Additionally, rhinitis patients had the highest positive rate of Cyn d 1 (60.0%), and all patients with Cyn d 12 sensitization (17.2%) were asthmatic patients. Optimal scale analysis showed that Phl p 1 and Cyn d 1 were closely related (Cronbach’s alpha = 85.1%).
Conclusion: The highest positive rate of pollen allergen components was Cyn d 1 in Bermuda grass sensitized patients in southern China. Most patients were sensitized to CCD alone, and CCD may have less interference in the detection of Cyn d 1, Art v 4, Phl p 1 and Phl p 12. The sensitization patterns of pollen allergen components varied in different ages and diseases, and the diagnostic strategy of pollen allergen needs to be considered in the future.
Keywords: Bermuda grass, component-resolved diagnosis, CRD, cross-reactive carbohydrate determinants, CCD, pollen allergen component, special IgE, EUROBlotMaster
Introduction
Bermuda grass, a major inhaled allergen in Asia and Europe, release abundant pollen from late spring to early summer, causing cough, wheezing or rhinorrhea and reducing the quality of life in asthma/rhinitis patients.1,2 Recent research from Argentina found that 48.1% of patients with seasonal allergic rhinitis were sensitized to Bermuda grass pollen, while in Thailand, the positive rate of Bermuda grass was 21.1% in patients with allergic diseases by skin prick test.3,4
Our previous research found that more than 60% of Bermuda grass sensitized rhinitis/asthma patients were sensitized to Timothy grass, while another study showed that some Bermuda grass sensitized patients were also co-sensitized to Mugwort.5 It is likely that these allergens might contain the same protein components inducing cross-reactive. Alternatively, it could be due to the cross-reactive carbohydrate determinants (CCD), a substance that led to positive detection results without causing any allergic symptoms, which was found in a large number of plant allergens.6 Ebo et al found that 23.5% of Timothy grass sensitized patients were positive for CCD, and research from China showed that the positive rates of CCD in patients who were Mugwort sensitized was 9.0%.7 However, research is lacking to analyse the relationship between Bermuda grass, Mugwort, Timothy grass allergen components and CCD in southern China, which contains a large population and a variety of vegetation.
Component-resolved diagnosis (CRD) can distinguish true sensitized components and cross-reactive protein from the molecular allergens, which provides the possibility for accurate diagnosis and treatment.8 Thus, this study used CRD technology to detect the serum sIgE of Bermuda grass, Mugwort, Timothy grass allergen components and CCD at the same time, aiming to investigate the relationship of Bermuda grass, Mugwort, Timothy grass allergen components and CCD, providing guidance for clinical diagnosis and treatment.
Materials and Methods
Ethics
This study was reviewed and approved by the ethics committee of First affiliated hospital of Guangzhou Medical University (GYFYY-2016-73). The use of human serum samples was in accordance of legislation in China and the wishes of donors, their legal guardians or next of kin, where applicable, who had offered written informed consent to using the serum samples for future unspecified research purposes.
Study Design
This was a cross-sectional study. Patients with Bermuda grass sensitization from Allergy Information Repository of State Key Laboratory of Respiratory Disease (AIR-SKLRD) during June 2017 to June 2019 in southern China were included by the following inclusion criteria: 1) the history of pollen exposure and lead to respiratory allergic symptoms, such as wheezing, dyspnea, sneezing, runny nose, nasal obstruction or nasal itching; and 2) the specific IgE (sIgE) level of Bermuda grass (Cynodon dactylon) was ≥ 0.35 kU/L. Patients with specific immunotherapy, cancer, autoimmune diseases and parasitic diseases were excluded. A total of 78 patients sensitized to Bermuda grass underwent detection of sIgE of Bermuda grass, Mugwort (Artemisia vulgaris), Timothy grass (Phleum pratense) allergen components and CCD. The diagnosis of asthma, rhinitis, chronic obstructive pulmonary diseases (COPD) and chronic cough were based on guidelines of GINA,9 ARIA,10 GOLD-COPD11 and The Chinese national guidelines on diagnosis and management of cough,12 respectively. All patients included in this study were not combined with multiple respiratory diseases. Details of study subjects are shown in Table 1, and the average age was 34.60±23.30 years old.
 |
Table 1 The characteristics of patients with Bermuda grass sensitization |
Measurement
Serum samples of patients were obtained by 10-minute-centrifugation at 3000g of venous blood collecting with separation gel containing vacutainer tubes. Aliquots of serum were stored at −80°C in AIR-SKLRD.
The serum sIgE levels of Bermuda grass allergen components [Cyn d 1 (g216), Cyn d 12 (unencoded)], Timothy grass allergen components [Phl p 1 (g205), Phl p 4 (g208), Phl p 5 (g215), Phl p 7 (g210), Phl p 12 (g212)], Mugwort allergen components [Art v 1 (w231), Art v 3 (w233), Art v 4 (w234)] and CCD were detected by EUROBlotMaster system (EUROIMMUN Medizinische Labordiagnostika AG, Lübeck, SH, Germany) according to the instructions provided by the manufacturer. Art v 1 was natural component and the other components used in this study were recombinant. Levels of sIgE were expressed in kU/L, and results of sIgE class based on RAST classification were defined as follows: class 0: <0.35 kU/L; class 1: ≥0.35 to <0.70 kU/L; class 2: ≥0.70 to <3.50 kU/L; class 3: ≥3.50 to <17.50 kU/L; class 4: ≥17.50 to <50.00 kU/L; class 5: ≥50.00 to <100.00 kU/L; and class 6: ≥100.00 kU/L.
Statistical Analysis
Statistical studies were conducted with SPSS 25.0 (Chicago, IL, USA). Parametric quantitative data was presented as mean ± standard deviation. Non-parametric quantitative data was presented as median (interquartile range). Categorical data was reported as a percentage showing the proportion of positive results, and chi-square test (χ2) was used to compare the variance of data among the groups. Correlation analysis were performed using Spearman’s tests, with the correlation coefficients presented as “rs”. The correlation between allergen components was calculated with optimal scale analysis. P <0.05 was considered statistically significant.
Results
Overview
Overall, Cyn d 1 had the highest positive rate (24.4%), followed by Phl p 1 (12.8%), Art v 3 (10.3%), Art v 4 (10.3%), Phl p 12 (9.0%) and Phl p 4 (7.7%). Besides, the majority of CCD-positive patients had Class 2 (23.1%) and Class 3 (19.2%) of CCD sIgE results, while most patients sensitized to Bermuda grass showed Class 3 (30.8%) of Bermuda grass sIgE results (Table 1). There were 14.1% of patients who were positive for one allergen component alone, while 24.3% were positive for multiple (at least two) allergen components. In polysensitized patients, 57.9% of them had allergic asthma. In addition, there were 59.0% (Figure 1A), 59.0% (Figure 1B) and 57.7% (Figure 1C) patients sensitized to CCD alone. Moreover, only 5.1% of patients were co-sensitized to CCD, Cyn d 1 and Phl p 1.
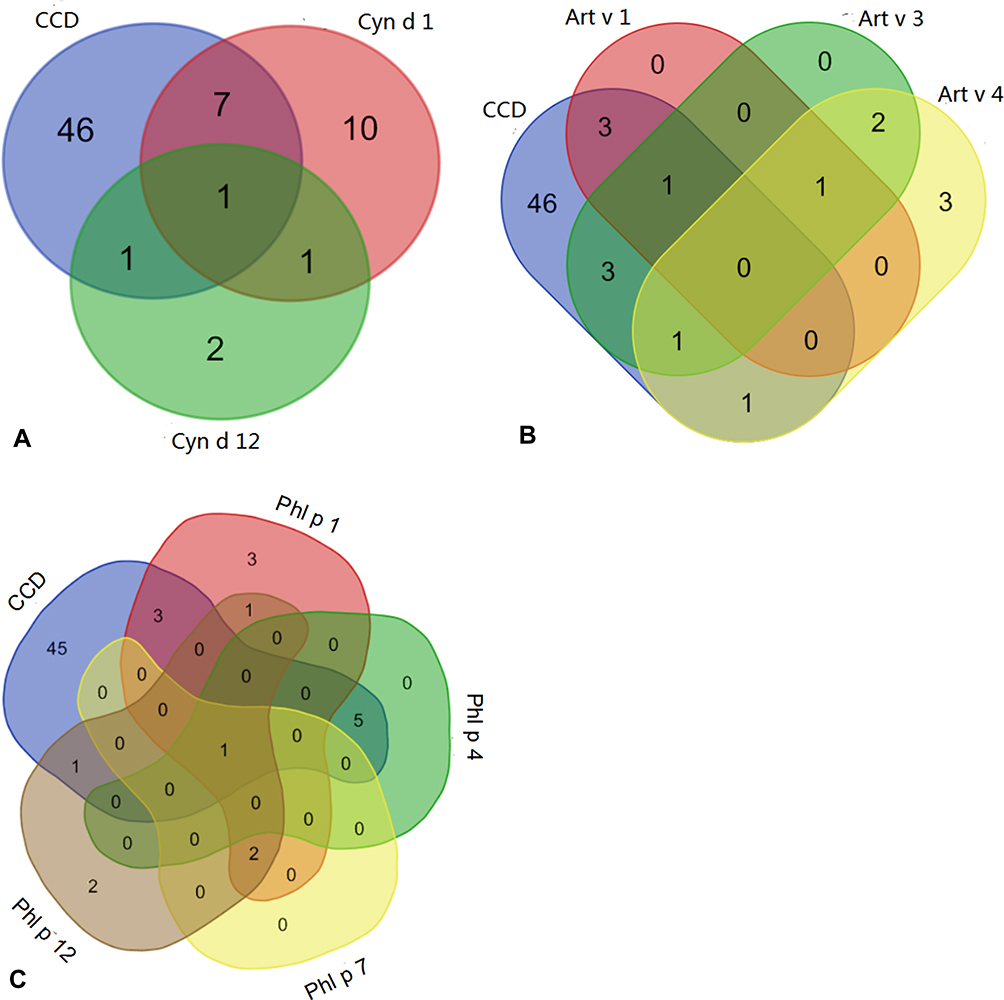 |
Figure 1 The co-sensitization between Bermuda grass, Mugwort, Timothy grass allergen components and CCD. The Venn Diagram shows the number of patients what were co-sensitized. (A) The co-sensitization between Bermuda grass allergen components and CCD. (B) The co-sensitization between Mugwort allergen components and CCD. (C) The co-sensitization between Timothy grass allergen components and CCD. |
The Positive Rate of Bermuda Grass, Mugwort and Timothy Grass Allergen Components Between CCD-Positive and -Negative Patients
Compared with CCD-positive patients, those with negative CCD results had significant higher positive rates of Cyn d 1 (47.8% vs 14.5%), Phl p 1 (26.1% vs 7.3%), Phl p 12 (21.7% vs 3.6%) and Art v 4 (26.1% vs 3.6%) (all p < 0.05). However, the positive rate of Phl p 4 (10.9% vs 0.0%) was significantly higher in patients with CCD positive than in patients with CCD negative (p < 0.05) (Table 2). There were no significant differences in Cyn d 12, Art v 3, Art v 1, Phl p 5 and Phl p 7 between the two populations.
 |
Table 2 The positive rate of pollen allergen components between CCD-positive and CCD-negative patients |
The Positive Rates of Bermuda Grass, Mugwort, Timothy Grass Allergen Components and CCD in Different Age Ranges
In patients <18 years old, Cyn d 1 (40.7%) had the highest positive rate, followed by Art v 3 (18.5%) and Art v 4 (18.5%), and 54.0% patients with Cyn d 1 positive had the sIgE levels class > 4. Similarly, in 18–60 year old patients, Cyn d 1 (20.0%) had the highest positive rate, followed by Phl p 1 (14.3%) and Phl p 4 (11.4%). In patients ≥60 years old, both Art v 1 and Phl p 4 (12.5%) had the highest positive rate, followed by Cyn d 1 (6.3%) (Figure 2). The positive rate of CCD in patients ≥60 years old (87.5%) was significantly higher than that in 18–60 year olds (77.1%) and <18 year olds (51.9%, p < 0.05). Notably, the positive class of CCD was low (range: class 1–class 3) in different ages. Besides, the positive rate of Cyn d 1 in patients <18 years old (40.7%) was significantly higher than that in 18–60 years old (20.0%) and ≥60 years old (6.3%, p < 0.05).
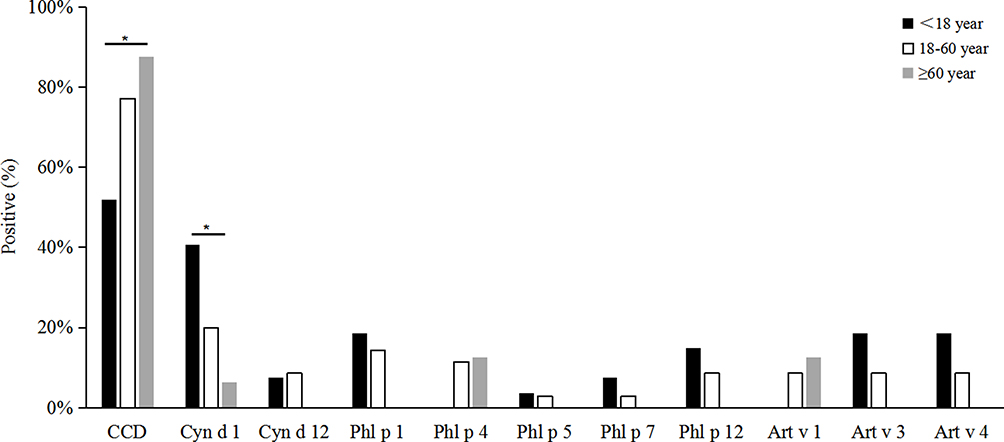 |
Figure 2 The positive rate of Bermuda grass, Mugwort, Timothy grass allergen components and CCD in different age groups. *p < 0.05, Chi-Square test. |
The Positive Rates of Bermuda Grass, Mugwort, Timothy Grass Allergen Components and CCD in Different Diseases
In the results of all detected pollen allergen components, the positive rates of Cyn d 1 were highest in both patients with rhinitis (60.0%) and asthma (31.0%), whereas the highest positive rate was Art v 1 in patients with COPD (33.3%), and in patients with chronic cough, no positive results to any detected allergen components were observed (Figure 3A-C). Interestingly, patients positive to Cyn d 12 were all asthma patients, with the positive rate of 17.2% (Figure 3A). In the results of Mugwort allergen components, asthma patients had the highest rate of Art v 3 (17.2%) and Art v 4 (24.1%) (Figure 3B). Besides, in the results of Timothy grass allergen components, patients with rhinitis had the highest positive rate of Phl p 1 (30.0%), while patients with asthma had the highest positive rate of Phl p 12 (20.7%) (Figure 3C). Regardless of the disease, CCD-positive rate was high (58.6–83.3%) (Figure 3D). However, no significant difference of the positive rate of CCD was found between the diseases (χ2 = 5.122, p > 0.05).
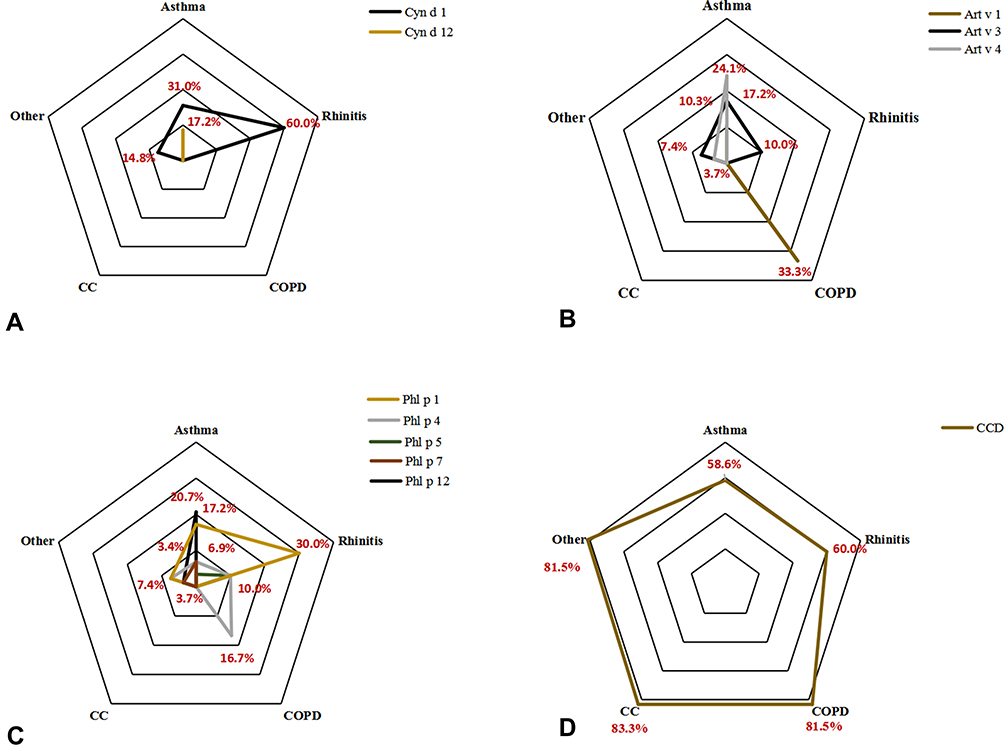 |
Figure 3 The positive rate of Bermuda grass, Mugwort, Timothy grass allergen components and CCD in different diseases. The positive rate of (A) Bermuda grass allergen components, (B) Mugwort allergen components, (C) Timothy grass allergen components and (D) CCD in different diseases. |
The Correlation Between CCD and Allergen Components of Bermuda Grass, Mugwort and Timothy Grass
Correlation analysis showed a positive correlation between Phl p 1 and Cyn d 1 (rs =0.715, p < 0.01), and Phl p 12 were positively correlated with Cyn d 12 (rs =0.791, p < 0.01), Art v 4 (rs =0.895, p < 0.01) and Phl p 7 (rs =0.659, p < 0.01). Optimal scale analysis also showed that Phl p 1 and Cyn d 1 were closely related, and the correlation among Phl p 4, Phl p 7 and Phl p 12 were close (Cronbach’s alpha = 85.1%) (Figure 4).
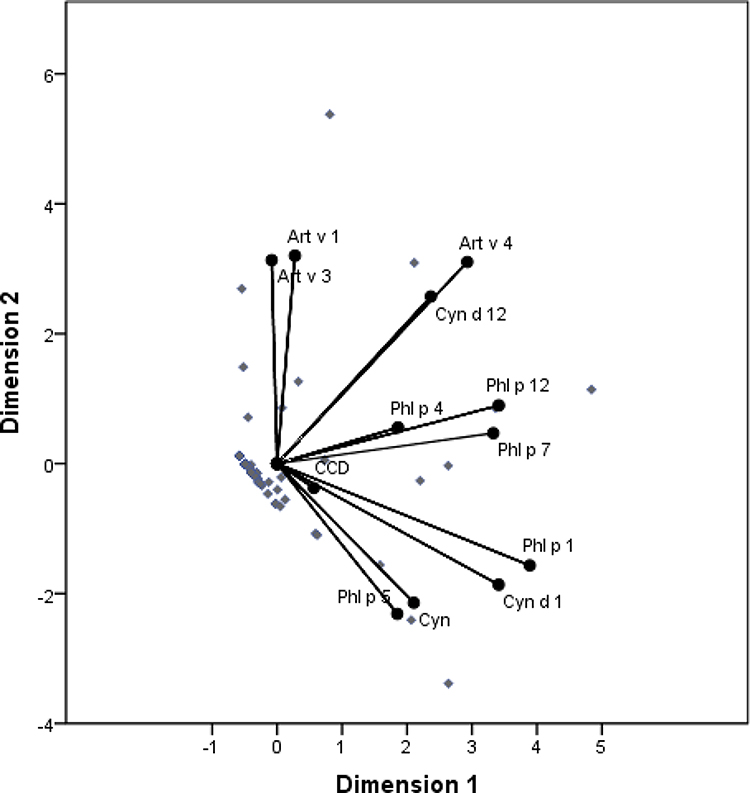 |
Figure 4 Optimal scale analysis between Bermuda grass, Mugwort and Timothy grass allergen components and CCD. The distance between the points represents the relative strength of correlation between them. The optimal scale analysis shows that there is a close relationship between Cyn d 1 and Phl p 1 (Cronbach’s alpha = 85.1%). |
Discussion
Bermuda grass pollen is one of a common inhaled allergens that can cause rhinoconjunctivitis in a certain amount of people. Component-resolved diagnosis, an advanced method of allergen diagnosis, helps personalized management and treatment of allergic diseases. In this study, we detected the serum sIgE levels of CCD and allergen components of Bermuda grass, Mugwort and Timothy grass in Bermuda grass sensitized patients by CRD. Our results showed that Cyn d 1 had the highest positive rate in pollen allergen components in the study population, followed by Phl p 1, Art v 3, Art v 4, Phl p 12 and Phl p 4. Cyn d 1, Phl p 1 and Art v 3 may be the major sensitization components in Bermuda grass sensitized patients. However, this may also be due to the geographical environment. Guangzhou is a central city of southern China with warm temperature and high humidity, and the climate here may affect the local composition of vegetation pollen and the content of CCD.
It is worth noting that CCD was considered as a potential source of positive IgE detecting results without clinical significance, which could happen in the detection of specific IgE of plant allergens.13 Regarding CCD and plant allergens, Sinson et al has reported that the CCD-positive rate in patients sensitized to Timothy grass was 16.7%14 and our previous study found that 41.4% of patients with positive sIgE results of Bermuda grass also showed CCD-sIgE positive.5 In this study, most of the components used in the EuroBlot tests were recombinant molecules, which provided good markers for the diagnosis of sensitization to components. Because certain purified allergen components were glycosylated and it may cause false positive result due to CCD reactivity. Nonetheless, there might be similar antigen epitope between CCD and the allergen components that could also cause IgE reactivity.
Further, our results show that the positive rates of CCD ranged from 52% to 88% in various age groups, whereas a large cohort study reported that the overall positive rate of CCD was 22%, where teenage group reached 35%.15 The inconsistence of CCD reactivity was possibly because our study population was positive for Bermuda grass. Furthermore, the high CCD positivity in our study may also suggest that serologic screening results of Bermuda grass without CCD blocker might not be reliable in grass pollen allergic subjects. Our result also showed that the positive rate of Cyn d 1, Art v 4, Phl p 1 and Phl p 12 in patients with CCD-negative result were significantly higher than in patients with CCD-positive result. This indicated that the positivity of CCD might have less impact in the detection of these allergen components. However, since inhibition assays were not performed in this study, the cross-reaction of CCD and pollen allergen components remain to be investigated. Despite this, our study demonstrated a high positivity of CCD in Bermuda grass sensitized population and provided the profile of CCD positivity in various pollen allergen components, which may aid in improving the diagnosis of Bermuda grass sensitization and give understanding of the cross-reaction patterns of CCD in these allergen components.
In addition, we reported a considerably high proportion of polysensitization in patients sensitized to pollen components, which should be noticed in clinical practice. In the United States and Europe, polysensitization is more prevalent in patients with moderate to severe respiratory diseases than monosensitization (range, 50%–80%).16 Another study showed that the polysensitization can even reach 97.4%.17 Additionally, polysensitization may also relate to multimorbidity, especially in children.18 Due to some of the clinical data of the studied population not being available, the multimorbidity as well as disease severity were not analyzed in polysensitization patients.
Besides, we have noticed that in patients <18 years old, Cyn d 1 had the highest positive rate, while in patients ≥60 years old, Art v 1 and Phl p 4 had the highest positive rate. This might not only be due to the discrepancy of the status of the immune system in different ages, but also relate to the living environment and lifestyles. A study in adolescents showed that the positive rate of Cyn d 1 was the second highest (36.0%), after the positive rate of Phl p 1 (39.0%).19 Although the allergen component with the highest positivity was different from our results, which might potentially be owning to the discrepancy of populations and/or geographical regions, both of the results showed high positive rate of Cyn d 1 in adolescents. Therefore, the sensitization patterns may differ in different ages, and it seems that adolescents allergic to Bermuda grass were more likely to be sensitized to Cyn d 1.
Meanwhile, we compared the sensitization pattern in different diseases. Patients with allergy rhinitis had the highest positive rate of Cyn d 1. Interestingly, we found that patients positive for Cyn d 12 were all asthma patients. Although our sample size was limited, this could also reveal the characteristics of sensitization pattern in the disease. A study in Argentina has shown that 43.5% of asthma patients were positive to Cyn d 12.3 With the advantage of CRD, which provides a more accurate sensitization profile, we were able to identify the correlation between disease and particular allergen components. Based on our results, there was an association between asthma and Cyn d 12, and thus, it should be considered to prevent asthma if patients were sensitized to Cyn d 12. Further studies with larger sample size were required to reveal the correlation of asthma and Cyn d 12 sensitization.
There were several limitations in this study. Firstly, our sample size was small. This was mainly due to the major sensitization allergen in Guangzhou being house dust mites (HDM), where the number of patients with weed pollen sensitization was relatively small.20,21 Secondly, because of the availability of patients’ clinical information, the associations between sensitization components and disease severity was not investigated. Thirdly, due to the limitation of conditions, none of our patients did the skin prick test and we did not include other allergic subjects in this study. Last but not least, inhibition assays were not performed and therefore the false positive rates of the detected allergen components were not clear as a result of the presence of CCD. Despite this, we compared the positive rates of pollen allergen components between CCD-positive and -negative patients, which provides the profile of allergen components that were likely to be interfered by CCD.
Conclusion
In conclusion, the highest positive rate of pollen allergen components was Cyn d 1 in Bermuda grass sensitized patients in southern China. Most patients were sensitized to CCD alone. The positive rate of Cyn d 1, Art v 4, Phl p 1, and Phl p 12 in patients with CCD negative were higher than in patients with CCD positive, while the positive rate of Phl p 4 was the contrary. Moreover, the sensitization patterns differed in various ages, where patients <18 years old exhibited the highest positive rate of Cyn d 1, and patients >60 years old showed the highest positive rate of Art v 1 and Phl p 4. In addition, Cyn d 12 sensitization might be closely associated with asthma.
Abbreviations
CCD, cross-reactive carbohydrate determinants; CRD, component-resolved diagnosis; sIgE, specific IgE; AIR-SKLRD, Allergy Information Repository of State Key Laboratory of Respiratory Disease; Cyn d, Cynodon dactylon; Art v, Artemisia vulgaris; Phl p, Phleum pratense; COPD, chronic obstructive pulmonary diseases; CC, chronic cough.
Data Sharing Statement
The data that support these findings are available on reasonable request from the corresponding author BQS. Data are not publicly available due to concerns regarding research participant privacy.
Acknowledgments
We would like to thank everyone involved in the collection, detection and date management of the serum samples.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This study was funded by the National Natural Science Foundation of China (Project No. 81871736, 81802076), Guangzhou Municipal Health Foundation (20191A011073), the Medicine and Health Care Technology Projects of Guangzhou (Project No. 2017A013010017), Guangzhou Science and Technology Foundation (Project No. 201804020043), National Key Technology R&D Program (2018YFC1311900), Guangdong Science and Technology Foundation (2019B030316028) and the SKLRD Foundation (Project No. SKLRD-MS-201906). The funders had no role in study design, data analysis, preparation of the manuscript or decision to publish.
Disclosure
The authors have no conflicts of interest to disclose in relation to this work.
References
1. Davies JM. Grass pollen allergens globally: the contribution of subtropical grasses to burden of allergic respiratory diseases. Clin Exp Allergy. 2014;44(6):790–801. doi:10.1111/cea.12317
2. Hu H, Luo W, Wu Z, Cai C, Huang H, Sun B. A pilot study on the allergen-specific IgE to molecular components on polysensitized mite allergic asthmatic patients in Guangzhou, China. Mol Immunol. 2019;105:38–45. doi:10.1016/j.molimm.2018.11.004
3. Ramon GD, Barrionuevo LB, Viego V, Vanegas E, Felix M, Cherrez-Ojeda I. Sensitization to subtropical grass pollens in patients with seasonal allergic rhinitis from Bahia Blanca, Argentina. World Allergy Organ J. 2019;12(9):100062. doi:10.1016/j.waojou.2019.100062
4. Oncham S, Udomsubpayakul U, Laisuan W. Skin prick test reactivity to aeroallergens in adult allergy clinic in Thailand: a 12-year retrospective study. Asia Pac Allergy. 2018;8(2):e17. doi:10.5415/apallergy.2018.8.e17
5. Luo W, Huang H, Zheng P, et al. Major grass pollen allergens and components detected in a southern Chinese cohort of patients with allergic rhinitis and/or asthma. Mol Immunol. 2016;78:105–112. doi:10.1016/j.molimm.2016.08.013
6. Melioli G, Passalacqua G, Canonica GW, Baena-Cagnani CE, Matricardi P. Component-resolved diagnosis in pediatric allergic rhinoconjunctivitis and asthma. Curr Opin Allergy Clin Immunol. 2013;13(4):446–451. doi:10.1097/ACI.0b013e32836274d8
7. Ebo DG, Hagendorens MM, Bridts CH, De Clerck LS, Stevens WJ. Sensitization to cross-reactive carbohydrate determinants and the ubiquitous protein profilin: mimickers of allergy. Clin Exp Allergy. 2004;34(1):137–144. doi:10.1111/j.1365-2222.2004.01837.x
8. Dodig S, Cepelak I. The potential of component-resolved diagnosis in laboratory diagnostics of allergy. Biochem Med (Zagreb). 2018;28(2):20501. doi:10.11613/BM.2018.020501
9. Global Initiative for Asthma. Global strategy for asthma management and prevention; 2018. Available from: www.ginasthma.org.
10. Bousquet J, Schunemann HJ, Togias A, et al. Next-generation Allergic Rhinitis and Its Impact on Asthma (ARIA) guidelines for allergic rhinitis based on Grading of Recommendations Assessment, Development and Evaluation (GRADE) and real-world evidence. J Allergy Clin Immunol. 2020;145(1):70–80. doi:10.1016/j.jaci.2019.06.049
11. Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J. 2019;53:5. doi:10.1183/13993003.00164-2019
12. Lai K. Chinese national guidelines on diagnosis and management of cough: consensus and controversy. J Thorac Dis. 2014;6(Suppl 7):S683–S688.
13. Malandain H. IgE-reactive carbohydrate epitopes–classification, cross-reactivity, and clinical impact. Eur Ann Allergy Clin Immunol. 2005;37(4):122–128.
14. Sinson E, Ocampo C, Liao C, et al. Cross-reactive carbohydrate determinant interference in cellulose-based IgE allergy tests utilizing recombinant allergen components. PLoS One. 2020;15(4):e231344. doi:10.1371/journal.pone.0231344
15. Holzweber F, Svehla E, Fellner W, et al. Inhibition of IgE binding to cross-reactive carbohydrate determinants enhances diagnostic selectivity. Allergy. 2013;68(10):1269–1277. doi:10.1111/all.12229
16. Calderon MA, Cox L, Casale TB, Moingeon P, Demoly P. Multiple-allergen and single-allergen immunotherapy strategies in polysensitized patients: looking at the published evidence. J Allergy Clin Immunol. 2012;129(4):929–934. doi:10.1016/j.jaci.2011.11.019
17. Navarro-Locsin CG, Lim-Jurado M. Aeroallergen sensitization and associated comorbid diseases of an adult Filipino population with allergic rhinitis. Asia Pac Allergy. 2018;8(3):e25. doi:10.5415/apallergy.2018.8.e25
18. Raciborski F, Bousquet J, Bousqet J, et al. Dissociating polysensitization and multimorbidity in children and adults from a Polish general population cohort. Clin Transl Allergy. 2019;9:4. doi:10.1186/s13601-019-0246-y
19. Sterner T, Uldahl A, Svensson A, et al. IgE sensitization in a cohort of adolescents in southern Sweden and its relation to allergic symptoms. Clin Mol Allergy. 2019;17:6. doi:10.1186/s12948-019-0110-6
20. Wang W, Huang X, Chen Z, et al. Prevalence and trends of sensitisation to aeroallergens in patients with allergic rhinitis in Guangzhou, China: a 10-year retrospective study. BMJ Open. 2016;6(5):e11085. doi:10.1136/bmjopen-2016-011085
21. Hu H, Xue M, Wei N, et al. Sensitisation of severe asthma in different occupations: A multicentre study in China. Clin Respir J. 2020. doi:10.1111/crj.13282
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.