Back to Journals » Research and Reports in Tropical Medicine » Volume 12
Magnitude, Diversity, and Antibiograms of Bacteria Isolated from Patient-Care Equipment and Inanimate Objects of Selected Wards in Arba Minch General Hospital, Southern Ethiopia
Authors Birru M, Mengistu M, Siraj M, Aklilu A ![]() , Boru K
, Boru K ![]() , Woldemariam M
, Woldemariam M ![]() , Biresaw G
, Biresaw G ![]() , Seid M
, Seid M ![]() , Manilal A
, Manilal A ![]()
Received 9 January 2021
Accepted for publication 7 April 2021
Published 4 May 2021 Volume 2021:12 Pages 39—49
DOI https://doi.org/10.2147/RRTM.S301215
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mario Rodríguez-Pérez
Melkam Birru, Matusal Mengistu, Munira Siraj, Addis Aklilu, Kalicha Boru, Melat Woldemariam, Gelila Biresaw, Mohammed Seid, Aseer Manilal
Department of Medical Laboratory Science, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia
Correspondence: Aseer Manilal
Department of Medical Laboratory Science, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia
Tel +251-91-990-4201
Email [email protected]
Intoduction: Patient-care equipment and inanimate objects contaminated with bacteria are a persistent problem in countries like Ethiopia, and remain overlooked. This study aimed to elucidate the magnitude of contaminations, diversity, and antimicrobial-susceptibility patterns of bacterial isolates from selected wards of Arba Minch General Hospital, Ethiopia.
Methods: Samples were inoculated into bacteriological media and identified by biochemical characterization, followed by antimicrobial-susceptibility tests.
Results: Of the 99 inanimate objects and items of patient-care equipment examined, 71 (71.7%) showed contamination: 26 (76.4%) from the surgical ward and 22 (66.6%) and 23 (71.8%), respectively, from the pediatric ward and neonatal intensive care unit. In the case of Gram-positive bacteria, coagulase-negative staphylococci (CoNS; 52.2%) were predominant, followed by Staphylococcus aureus (47.7%), whereas common Gram-negative counterparts were Acinetobacter spp. (28.5%) and Klebsiella spp. (23.8%). Antibiograms of S. aureus and CoNS showed 100% and 78% resistance, respectively, against penicillin. Isolates of Acinetobacter spp. showed 100% resistance to ceftriaxone and ampicillin, whereas those of Klebsiella spp. displayed complete resistance against ampicillin and trimethoprim–sulfamethoxazole. All isolates of Citrobacter spp., Enterobacter spp., Salmonella spp., Escherichia coli, and Serratia spp. exhibited 100% resistance to amoxicillin, ampicillin, and trimethoprim–sulfamethoxazole. Overall prevalence of multidrug-resistant bacteria was 57.7%.
Conclusion: A stringent infection-vigilance program comprising routine sampling from equipment and inanimate objects combined with antimicrobial-resistance surveillance and decontamination efforts must be instituted promptly.
Keywords: bacterial contamination, patient-care equipment, inanimate objects, Arba Minch General Hospital, multidrug resistance
Introduction
Worldwide, hospital-acquired infections (HAIs) are considered a major public health challenge. They cause severe financial burden, potential disability, and sometimes even deaths in hospital settings.1 The magnitude of this problem remains underestimated in many developing countries, and recently the prevalence of HAIs has gone beyond 20%.2 A perusal of the literature reveals that in Ethiopia, there is a lack of documentation pertaining to all HAIs and HAI-associated mortality. However, the prevalence of HAIs in two teaching hospitals in Ethiopia remained at a lower level, ie, only 14.9%.3
Any microorganism of endogenous or exogenous origin can cause an HAI. The most problematic in terms of prevalence and treatment are bacteria,4 which often act as primary or secondary invaders and can inflict a wide array of potentially fatal diseases. Reservoirs and sources of bacteria associated with HAIs exist in both inanimate and animate environments. It has been stated that both Gram-positive and Gram-negative bacteria can persist for months on dry inanimate surfaces under humid and adverse conditions, and can serve as transmission points among health-care workers themselves and also in patients.5 It is envisaged that up to 60% of surfaces in the patients' environment are contaminated with HAI-causing organisms. Indeed, those bacteria can easily enter susceptible patients through contacts with fomites in the surroundings (eg, bed rails, emergency carts, and trolleys) or by the use of contaminated patient-care equipment (eg, stethoscopes and sphygmomanometers). In recent decades, due to irrational and inappropriate usage of antibiotics, multidrug-resistant (MDR) bacteria are gradually emerging in hospital setups.6 Colonization by MDR bacteria is considered one of the predisposing factors for HAIs and is a daily challenge for the clinicians, particularly dealing with critically ill patients.6,7 Bacteria that are frequently implicated as MDR are ESKAPE pathogens (encompassing six pathogens with growing multidrug resistance and virulence: Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter spp.), and are responsible for a substantial percentage of HAIs in the current scenario.8 The diversity of species and strains is dramatically widening.
Bacterial contamination from exogenous inanimate origins, such as patient-care equipment and fomites, is considered one of the probable causes of HAIs.7,9 Proper use of disinfectants is essential for limiting the transmission of infectious pathogens. However, in developing countries like Ethiopia, the use of expensive techniques for cleaning, disinfection, and sterilization is not always possible, so poorly decontaminated patient-care equipment and inanimate objects can serve as potential sources of infection. Diversity, prevalence, and antibiotic-susceptibility patterns of bacterial isolates may vary geographically, particularly among various health-care units of the same hospital at different times. Therefore, periodic monitoring by bacteriological analyses of inanimate surfaces and patient-care equipment is needed to detect changing trends in types and counts of bacterial flora.10 As bacterial pathogens still play a critical role in HAIs in Ethiopia, it is imperative to know location/institution-based etiological and susceptibility profiles. A survey of the literature demonstrated that only a few studies have been done in the country to indicate the magnitude of bacterial contaminations in patient-care equipment and inanimate objects.11–14 Hitherto, no such studies have been conducted at Arba Minch General Hospital (AMGH). This work was initiated to elucidate the magnitude of contamination, etiological profile, and antimicrobial-susceptibility patterns of bacteria isolated from patient-care equipment and inanimate objects of selected wards in AMGH, Arba Minch, Ethiopia.
Methods
Study Area, Design, and Period
This study was carried out at AMGH, Arba Minch, Ethiopia. The study protocol was approved by the Institutional Review Board of the College of Medicine and Health Sciences, Arba Minch University (CMHS/4920/54/2018). The hospital contains 300 beds over eleven service areas. Many individuals from the surrounding area and nearby zones visit as inpatients and outpatients. A cross-sectional study was conducted to identify the magnitude of contamination, etiological profile, and drug-susceptibility patterns of bacteria isolated between May 1 and June 30, 2018.
Sampling Technique
The hospital wards were selected purposively (convenience sampling). Patient-care equipment and inanimate objects were selected randomly by lottery method from the lists obtained from the head office of selected wards in AMGH. Samples were collected 4 hours after the last cleaning of the selected wards: the neonatal intensive care unit (NICU) and surgical and pediatric wards. Objects chosen for sampling are shown in Figure 1.
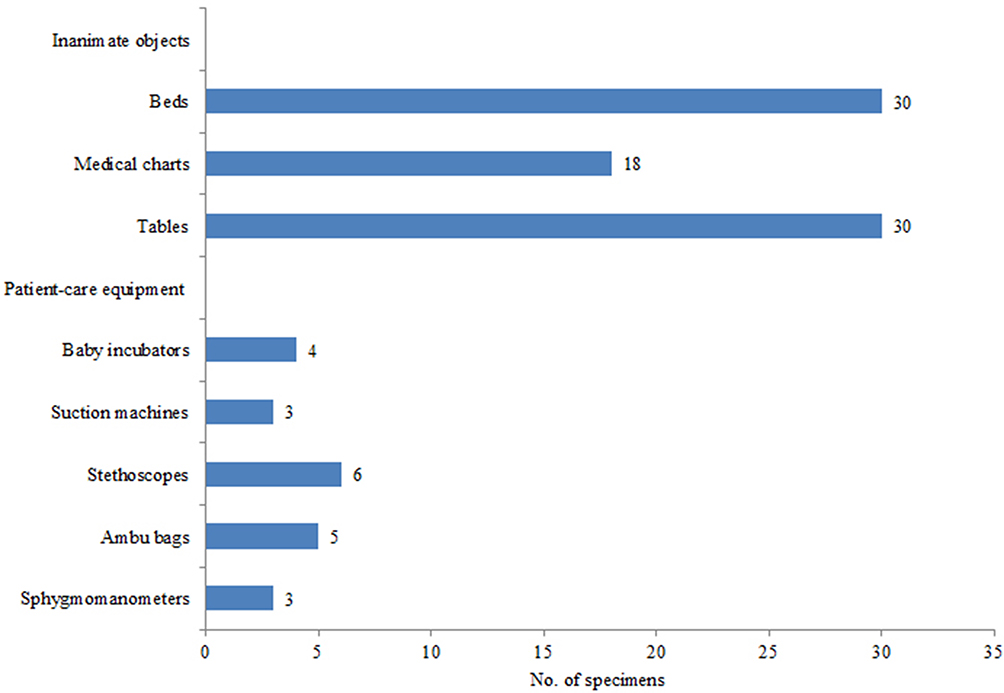 |
Figure 1 Number of specimens collected from inanimate objects and patient-care equipment at AMGH. |
Specimen Collection and Processing
Specimen were taken from selected patient-care equipment and inanimate objects. A swab soaked in normal sterile saline was used to procure samples from the representative area (high-frequency patient-touch sites) of the equipment and inanimate objects. Afterward, swabs were placed in sterile labelled sleeves and transported to the Microbiology and Parasitology Laboratory, Department of Medical Laboratory Science, College of Medicine and Health Sciences, Arba Minch University at room temperature and stored at 5°C until processing on the same day.
Isolation and Identification of Bacterial Isolates
Isolation and identification of bacterial isolates were done at the Microbiology and Parasitology Laboratory. All samples were plated out on various isolation media, including MacConkey agar, blood agar, and mannitol salt agar. The inoculated plates were incubated face-up for 24 hours at 37°C. Following incubation, plates were inspected for bacterial growth. Pure cultures of respective bacterial isolates were subsequently subjected to species identification and confirmation. Macroscopic and microscopic analyses and biochemical and physiological characteristics of isolated bacteria were evaluated via standard laboratory methods.15 Briefly mentioning, Gram-positive isolates were identified using catalase and coagulase tests. Isolates of members of Enterobacteriaceae family were identified biochemically by means of a series of tests: catalase, indole, citrate, urease, H2S production, methyl red, Voges–Proskauer, and triple-sugar iron. Non–lactose fermenting Gram-negative bacteria were identified by indole, triple-sugar iron, urease oxidase, and catalase tests. Corresponding American Type Culture Collection (ATCC) strains were used as reference standards: E. coli (ATCC 25922), K. pneumoniae (ATCC 13883), E. cloacae (ATCC 23355), S. aureus (ATCC 25923), E. faecalis (ATCC 29212), and S. typhimurium (ATCC 14028).
Antimicrobial-Susceptibility Testing
Kirby–Bauer disk diffusion was used for determining the antibiotic-sensitivity profile of each isolate.16 Fourteen commercially available antibiotic disks (HiMedia, Mumbai) were used for determination of antibiograms. Inocula were prepared by aseptically collecting the test organisms with a sterile wire loop and then suspending them in normal saline. The density of suspensions was determined by comparison with the opacity standard on McFarland 0.5 barium sulfate solution. Bacterial suspensions were then inoculated onto Mueller–Hinton agar plates to attain an approximate lawn concentration of 1.5×106 CFU/cm2. Five antibiotic disks were dispensed, equidistant pentagonally, in each petri dish. After 24 hours of incubation at 37°C, the diameter of the zones of inhibition around the disks were measured and categorized as sensitive, intermediate, and resistant according to the standardized table of the Clinical and Laboratory Standards Institute.17 Antibiotic disks containing penicillin (10 IU), tetracycline (30 μg), cefoxitin (30 μg), gentamicin (10 μg), erythromycin (15 µg), ciprofloxacin (5 μg), norfloxacin (10 μg), clindamycin (30 μg), chloramphenicol (30 μg), amikacin (30 µg), trimethoprim–sulfamethoxazole (1.25/23.75 µg), ceftriaxone (30 μg), ampicillin (10 μg), and amoxicillin (20 μg) were used to determine antibiograms. Bacteria showing resistance to three classes (and above) of antibiotics were considered MDR.
Results
Magnitude of Overall Bacterial Contamination
In total, 99 swab specimens were collected from the surgical ward (n=34), pediatric ward (n=32), and NICU (n=33). Results of microbial inspection revealed that of the 99 swab specimens collected, 71 (71.7%) showed bacterial contamination. Of these, 26 (76.4%) were from surgical ward and 22 (66.6%) and 23 (71.8%), respectively, from the pediatric ward and NICU.
Prevalence and Types of Bacteria
In total, 109 bacterial isolates were retrieved and tentatively identified in different culture media. Among the diverse bacterial isolates, 80.7% (n=88) comprised Gram-positive cocci and the remaining 19.2% (n=21) Gram-negative bacilli (Table 1). Based on colony morphology, biochemical characteristics, and subsequent comparison with previous reports, isolates were identified and sorted into nine species: Gram-negative bacilli, ie, Acinetobacter spp., E. coli, Klebsiella spp., Enterobacter spp., Citrobacter spp., Serratia spp., and Salmonella spp., and Gram-positive cocci, ie, S. aureus and CoNS. Among the Gram-positive cocci identified, CoNS 46 (52.2%) was the predominant bacterium, followed by S. aureus (42, 47.7%). In the case of Gram-negative bacilli, the most common isolate was Acinetobacter spp. (28.5%), followed by Klebsiella spp. (23.8%).
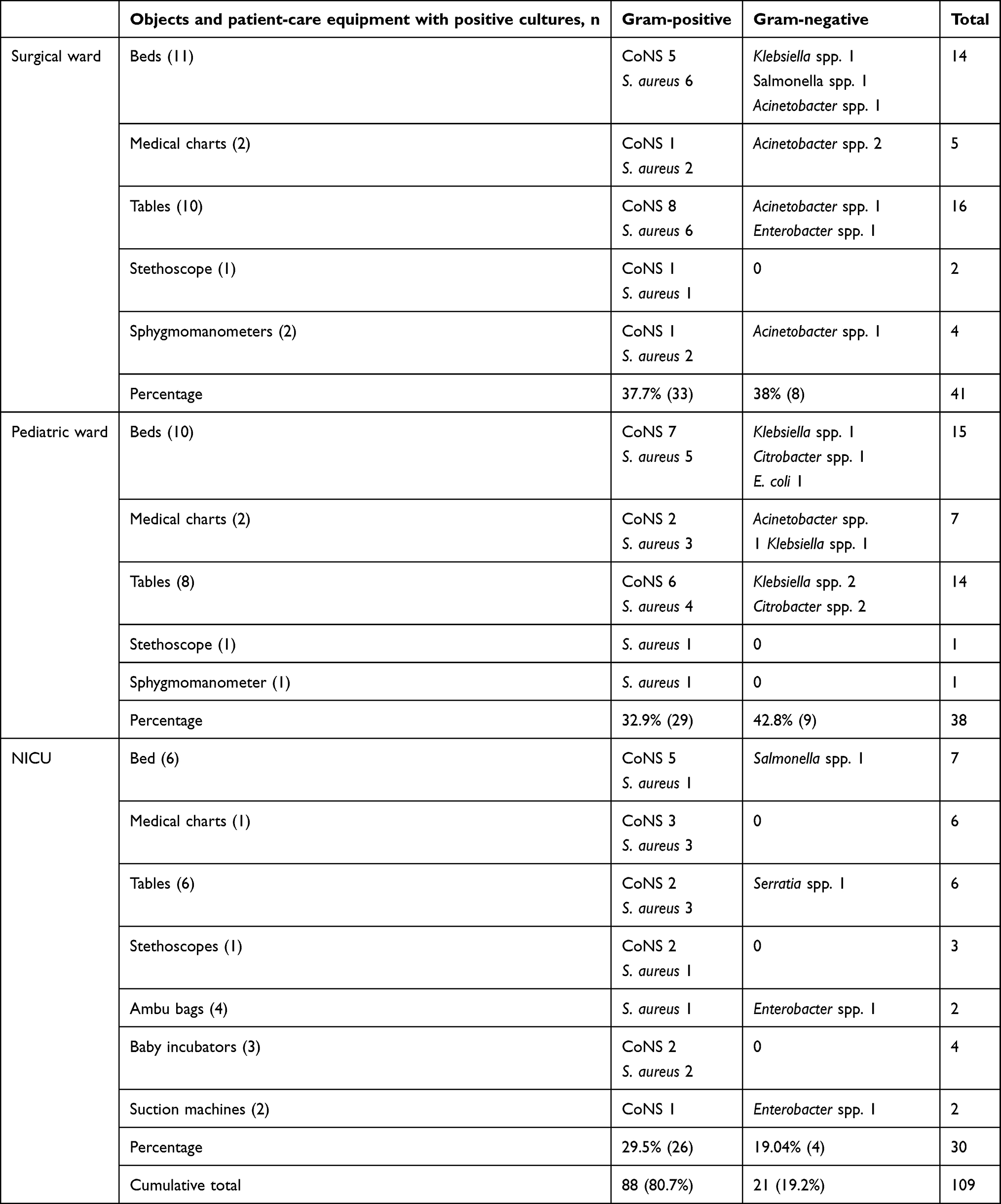 |
Table 1 Bacteria isolated from inanimate objects and patient-care equipment in three wards at AMGH |
Contamination of Inanimate Objects and Patient-Care Equipment
Results of the microbiological analysis (Table 1) revealed that among the three wards, the most contaminated was the surgical ward. It demonstrated the highest number of isolates, both from inanimate objects and patient-care equipment (n=41), corresponding to 33 (37.7%) Gram-positive and 8 (38.0%) Gram-negative bacteria. Notably, isolates of S. aureus (n=17) and Acinetobacter spp. (n=5) were found to be the predominant Gram-positive and Gram-negative bacteria, respectively. Heavily contaminated inanimate objects in the surgical ward were tables and beds, with 25 Gram-positive and 5 Gram-negative bacteria isolated. The second most contaminated was the pediatric ward, from where 38 isolates comprising 29 (32.9%) Gram-positive and 9 (42.8%) Gram-negative bacteria were isolated. Major Gram-positive and Gram-negative bacteria retrieved were isolates of CoNS (n=15) and Klebsiella spp. (n=4), respectively. In the pediatric ward, the highest level of contamination was associated with inanimate objects, with 27 Gram-positive and 9 Gram-negative bacteria isolated. Gram-negative isolates obtained comprised Klebsiella spp., Citrobacter spp., Enterobacter spp., E. coli, and Acinetobacter spp. Among the inanimate objects, beds were found to be the most contaminated, with 13 Gram-positive and 3 Gram-negative bacteria isolated. The NICU showed the lowest prevalence and fewest types of bacterial isolates. Of the total 30 isolates from the NICU, 26 (29.5%) were Gram-positive and the other 4(19.04%) were Gram-negative. Notably, isolates of CoNS (n=15) and Enterobacter spp. (n=2) were the predominant Gram-positive and Gram-negative bacteria, respectively. Similar to other wards, inanimate objects from the NICU were found to be heavily contaminated compared to patient-care equipment. In sum, 19 bacteria were isolated from inanimate objects. Beddings in the NICU was heavily contaminated. Among the patient-care equipment, baby incubators were observed to be heavily contaminated. In all three wards, tables, bed frames, medical charts, and patient-care equipment like stethoscopes, Ambu bags, suction machines, sphygmomanometers, and baby incubators were contaminated with Gram-positive bacteria, particularly Staphylococcus spp. (Table 1).
Antibiogram Profiles
Antibiotic-sensitivity profiles of all isolates were inspected using 14 antibiotics. Antibiograms of Gram-positive and Gram-negative bacteria are given in Tables 2 and 3, respectively. It was observed that Gram-positive cocci were highly sensitive to most of the antibiotics tested. Drug sensitivity manifested by S. aureus against clindamycin was 95.2%, followed by chloramphenicol (92.9%), ciprofloxacin (90.5%), erythromycin (80.9%), amikacin (76.1%), ceftriaxone (69%), gentamicin (64.3%), and tetracycline (61.9%). It was noted that 100% of S. aureus was resistant to penicillin, but for trimethoprim–sulfamethoxazole resistance was just 30.9%. The proportion of methicillin-resistant S. aureus was only 19.1%. In the case of CoNS, corresponding values were clindamycin 82.6%, amikacin 78.2%, ciprofloxacin 73.9%, and chloramphenicol 63.4%. Isolates of CoNS showed a high degree of resistance (78.3%) to penicillin and a moderate degree (43.4%) to trimethoprim–sulfamethoxazole, and resistance of 32.6% to tetracycline and 28.1% to both chloramphenicol and erythromycin.
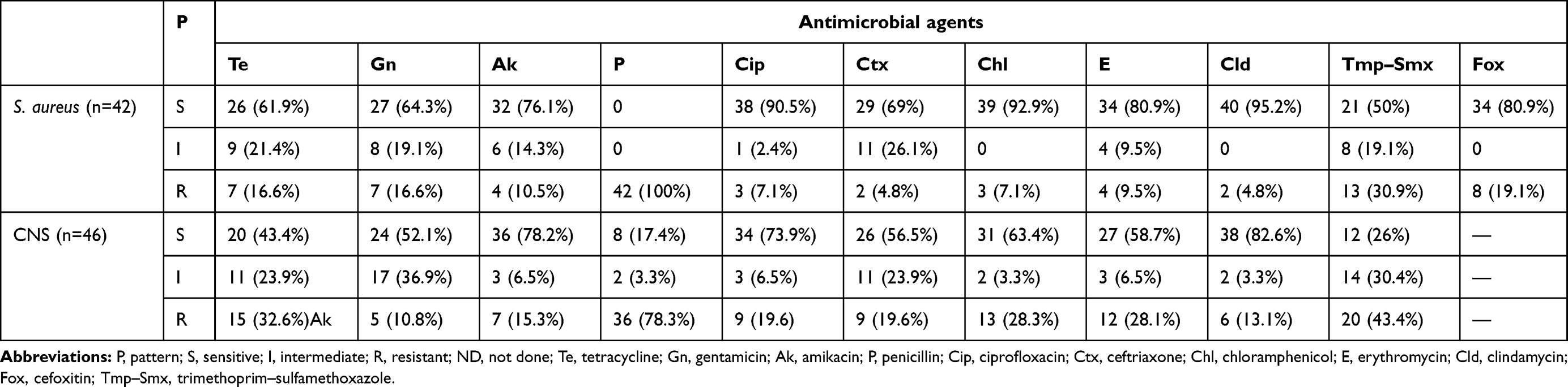 |
Table 2 Antimicrobial-susceptibility patterns of Gram-positive cocci isolated from patient-care equipment and inanimate objects at AMGH |
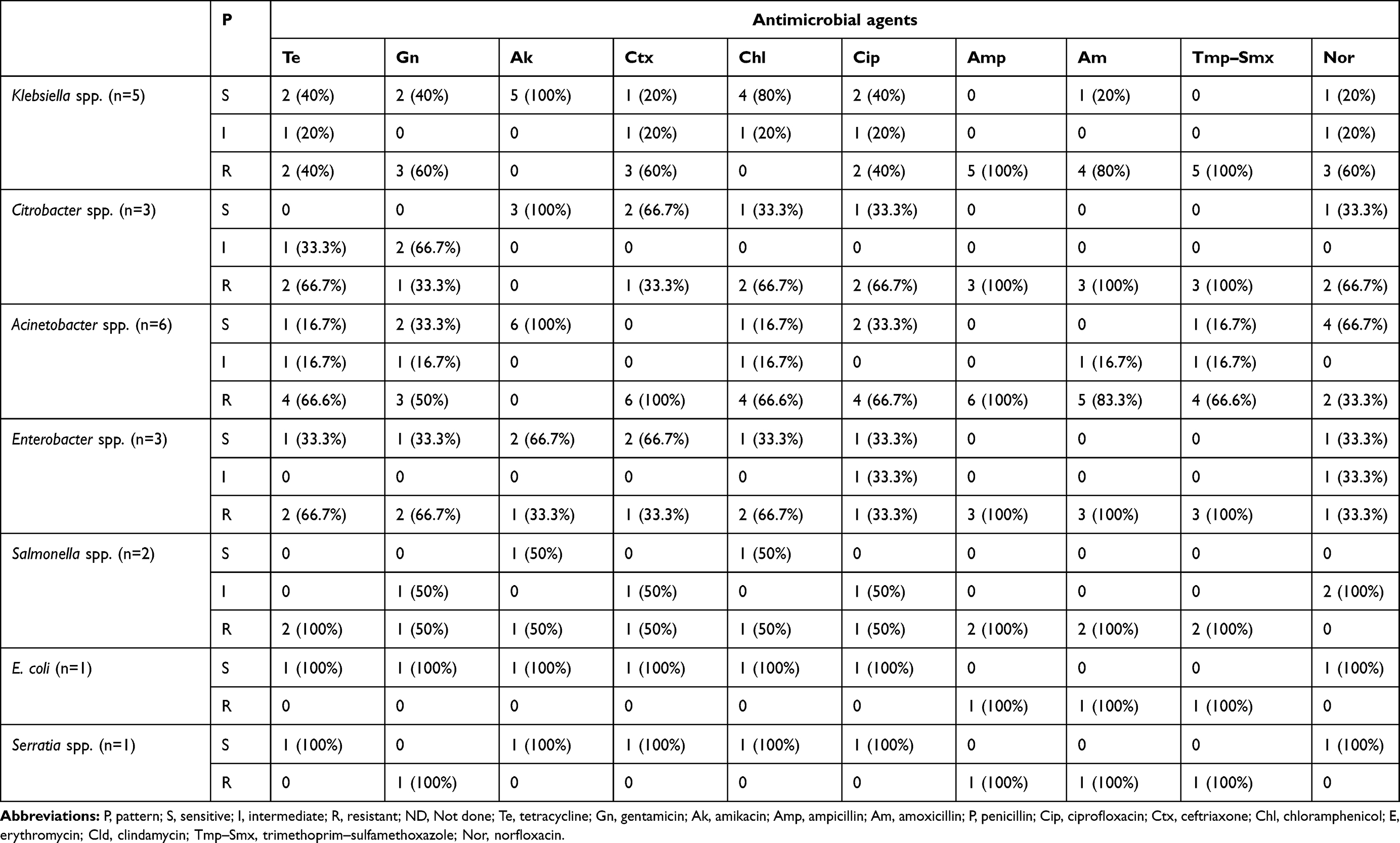 |
Table 3 Antimicrobial-susceptibility patterns of Gram-negative bacilli isolated from patient-care equipment and inanimate objects at AMGH |
The susceptibility patterns of Gram-negative bacilli revealed that the predominant isolate, Acinetobacter spp. showed a low range of sensitivity to five of the antibiotics tested (tetracycline, norfloxacin, trimethoprim–sulfamethoxazole, gentamicin, and ciprofloxacin) of 16.7%–33.3%. Invariably, all isolates were extremely susceptible (100%) to amikacin. However, isolates showed 100% resistance to both ceftriaxone and ampicillin. Antibiograms of Klebsiella spp. and Citrobacter spp., revealed that 100% of the isolates were susceptible to amikacin. Isolates of Klebsiella spp. showed considerable resistance (100%) to ampicillin and trimethoprim–sulfamethoxazole, whereas isolates of Enterobacter spp. exhibited less susceptibility (33.3%–66.7%) against the five antibiotics tested. It was observed that 66.7% of the isolates belonging to the latter were sensitive to both amikacin and ceftriaxone. In the case of Salmonella spp., 50% of the isolates were susceptible to both amikacin and ceftriaxone. Antibiotic-sensitivity patterns of E. coli and Serratia spp. indicated that both isolates were extremely susceptible (100%) to tetracycline, amikacin, ceftriaxone, chloramphenicol, ciprofloxacin, and norfloxacin. Invariably, all isolates of Citrobacter spp., Enterobacter spp., Salmonella spp., E. coli, and Serratia spp. exhibited 100% resistance to amoxicillin, ampicillin, and trimethoprim–sulfamethoxazole.
Isolates of Klebsiella spp. showed notable resistance (80%–100%) to amoxicillin, ampicillin, and trimethoprim–sulfamethoxazole. Invariably, all isolates of Citrobacter spp. showed maximum resistance (100%) to amoxicillin, ampicillin, and trimethoprim–sulfamethoxazole. This phenomenon also occurred in the case of Enterobacter spp. Salmonella spp., and E. coli. Resistance of Salmonella spp. to gentamicin, amikacin, ceftriaxone, chloramphenicol, and ciprofloxacin was 50%. The least diverse bacterial isolate, Serratia spp., were resistant to gentamicin, amoxicillin, ampicillin, and trimethoprim–sulfamethoxazole (100%). In this study, multidrug resistance was taken as resistance to three or more groups of antibiotics tested. Altogether, 47.7% of Gram-positive cocci were found to be MDR, of which 42.8% and 52.17% of S. aureus and CoNS, respectively, were resistant to three or more antibiotics. All Gram-negative bacteria were found to be MDR. The overall prevalence of MDR isolates in this study was found to be 57.7% (Table 4).
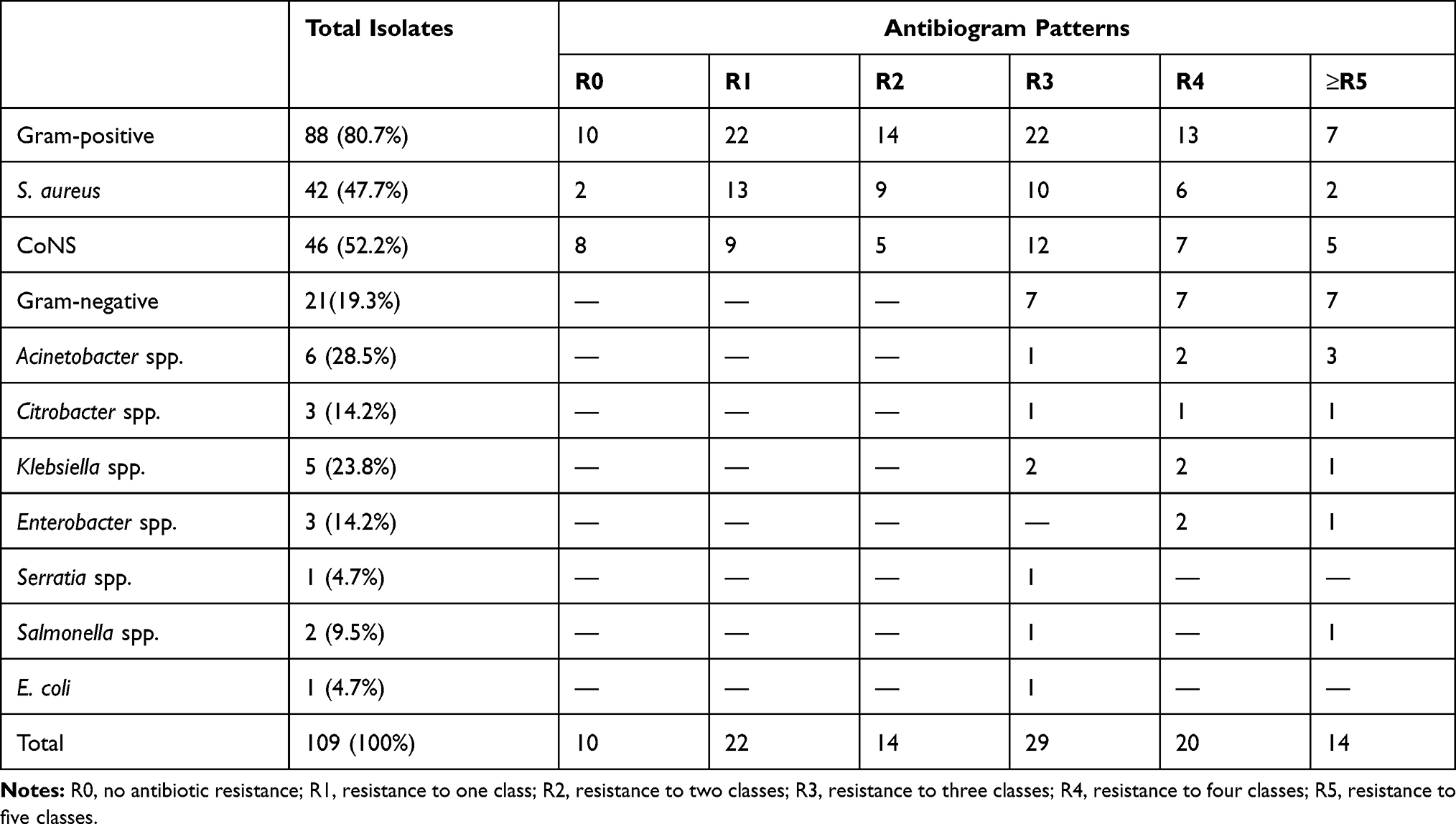 |
Table 4 Multidrug-resistance patterns of bacteria isolated from of patient-care equipment and inanimate objects at AMGH |
Discussion
Magnitude of Bacterial Contamination
Contaminated inanimate objects and patient-care equipment are proven sources of infections, and the bacteria can spread throughout hospital wards in an epidemic fashion. Among the three wards studied, the surgical ward showed the highest degree of bacterial contamination, followed by the pediatric ward. Total bacteria isolated from the surgical ward were more than obtained from other wards. These results are in line with two earlier reports from Ethiopia itself.11,18 In contrast, a study from Kenya noted that operation/surgical rooms had the lowest degree of bacterial contamination.19 Among inanimate objects, tables were the most contaminated, followed by beds. This was in agreement with studies conducted in Ethiopia and Kenya.11,19 The presence of bacterial isolates on inanimate objects can cause cross infections during postoperative care in patients who have undergone surgery. Among patient-care equipment, sphygmomanometers were the most contaminated, followed by stethoscopes. In other studies, almost the same patterns of bacterial contamination were observed.9,11,12,21 Contaminated patient-care equipment, such as stethoscopes, sphygmomanometers, Ambu bags, suction machines, and baby incubators, can come into direct contact with patients, thereby putting them at greater risk of developing infections.22 It is likely that patients in surgical wards are at higher risk of cross infection. The second–most contaminated spot in this study was the pediatric ward. Our results are in concordance with a report from Nigeria.20 However, in comparison to our results, research from northwestern Ethiopia reported a much lower level of bacterial contamination in NICU.18 The magnitude of contamination dealt with in this study could be attributed to cleaning personnel, products, or even procedures. Housekeeping is of prime importance in reducing the risk of transmission of nosocomial bacterial pathogens to susceptible patients. Therefore, periodic sterilization of patient-care equipment to a sufficient extent before usage and frequent disinfection of inanimate objects are extremely important.
Prevalence and Types of Bacterial Isolates
In all three wards, patient-care equipment and inanimate objects directly or indirectly associated with patients were heavily contaminated with diverse species of bacterial pathogens. Of the isolates, Gram-positive cocci were the most dominant, and the extent of contamination was comparable to a number of studies reported from Ethiopia and Nigeria.11,13,14,18,23 Contrary to our results, other studies have reported that Gram-negative bacilli are the predominant isolates in hospital settings.7,24 Among the Gram-positive cocci, CoNS (46, 52.2%) were the most frequently isolated from all the samples, followed by S. aureus (42, 38.5%). These findings are in line with results of other studies that reported CoNS as the major bacteria that colonized the surface of inanimate and therapeutic equipment in hospital setups.11,13,25–27 However, our results are not in agreement with the conclusions of other researchers from Ethiopia and Nigeria, who reported S. aureus was the most encountered isolate in inanimate and therapeutic equipment.12,14,23 Isolation of Staphylococcus spp. from patient-care equipment and inanimate objects of all three wards indicated their ubiquitous nature. This can be related to the fact that Staphylococcus spp. are members of the microbiome of both healthy as well as sick individuals. They can be dispersed widely through direct contact with contaminated inanimate objects or medical equipment and even by transient carriage on the hands of health-care workers. The results of this study also proved that Gram-negative bacilli colonized the surface of many inanimate objects and patient-care equipment in all three wards. Acinetobacter spp. were the predominant isolates followed by Klebsiella spp., Citrobacter spp., Enterobacter spp., Salmonella spp., Serratia spp., and E. coli. The prevalence and types of bacterial isolates observed in this work are in concordance with findings of other studies conducted in different parts of the world.12,14,18,23,28
It has been reported that Acinetobacter spp. were the main Gram-negative bacilli isolated from therapeutic equipment of hospital settings.30 In contrast, other studies have found that E. coli was the most common Gram-negative bacteria isolated from medical equipment and the hospital environment.14,20,23 The second–most predominant Gram-negative bacilli obtained were Klebsiella spp., as in the case of another study done in Ethiopia.14 In contrast, several studies from Ethiopia and Mexico reported that Klebsiella spp. were the major bacteria isolated from medical equipment and the hospital environment,12,21,24 whereas a recent study from the former country showed that Citrobacter spp. were the most commonly isolated bacteria, followed by Klebsiella spp.13 The prevalence of Citrobacter spp. and Enterobacter spp. observed in this study is comparable to a certain extent to an earlier report from Ethiopia.11 However, we were able to isolate Salmonella spp., Serratia spp., and E. coli only rarely. Previous studies from this nation have reported similar trends in the case of Salmonella, E. coli, and Serratia while examining therapeutic equipment and inanimate objects.12,14,21 These discrepancies in prevalence and types of bacterial isolates in various studies could be due to fluctuations in the standards of hygiene practices and environmental sanitation methods applied in hospitals.
Antibiograms
We found that the most predominant Gram-positive isolate, CoNS, showed resistance to both penicillin and trimethoprim–sulfamethoxazole to a greater extent than the others. Similar phenomena have been observed in a number of studies reported from various regions of Ethiopia.12–14 Isolates of CoNS were highly susceptible to clindamycin and amikacin. In contrast, a previous study from Ethiopia, CoNS was least susceptible to clindamycin.18 Isolates of S. aureus showed higher resistance to penicillin, followed by trimethoprim–sulfamethoxazole, which has been documented in previous studies.12–14,18,21 On the other hand, most of the isolates were sensitive to clindamycin, chloramphenicol, and ciprofloxacin.19 The percentage of methicillin-resistant S. aureus observed in this study is almost comparable to the results of an earlier work done in northwestern Ethiopia.18 The predominant Gram-negative bacilli, Acinetobacter spp., displayed higher resistance to two commonly used antibiotics, ceftriaxone and ampicillin, and this situation is well-nigh similar to the results of a prior study.29 Isolates of Acinetobacter spp. were found to be especially susceptible to amikacin. The second predominant Gram-negative bacilli, Klebsiella spp., showed resistance to trimethoprim–sulfamethoxazole, ampicillin, and amoxicillin. A similar trend of resistance patterns has been observed in studies conducted in other regions of Ethiopia.12,14
Susceptibility patterns exhibited by isolates of Klebsiella spp. to amikacin and chloramphenicol were by and large similar to those revealed by earlier works.13,18 Apart from Klebsiella spp., other Gram-negative bacilli, such as Citrobacter spp., Salmonella spp., Enterobacter spp., E. coli, and Serratia spp., exhibited appreciable resistance to the same antibiotics. A similar trend of resistance has been documented in various studies done in different locales of Ethiopia.12–14,18 In addition, we found that isolates of Salmonella spp. exhibited resistance to four antibiotics: trimethoprim–sulfamethoxazole, ampicillin, amoxicillin, and tetracycline. In similar fashion, a study done in eastern Ethiopia12 reported that Salmonella spp. isolated from patient-care equipment was resistant to tetracycline, whereas resistance patterns exhibited against trimethoprim–sulfamethoxazole and amoxicillin in our observations were not in concurrence.12 E. coli and Serratia spp. exhibited a similar trend of susceptibility toward six antibiotics: tetracycline, amikacin, ceftriaxone, chloramphenicol, ciprofloxacin, and norfloxacin. The susceptibility pattern of E. coli was consistent with results of recent studies done in Ethiopia.12,13 Also, our results are in accordance with the outcome of a study reporting that Serratia spp. were highly susceptible to ceftriaxone and ciprofloxacin.14 Multiple-antibiotic resistance was detected in 57.7% of isolates, comparable to the results of a previous study,14 but lower than that found in another study in Ethiopia.18 The high prevalence of MDR bacteria observed in this study might have emerged as a result of indiscriminatory and frequent usage of antibiotics per patient per ward. Therefore, it is high time to develop and implement policies for periodic surveillance of pathogens and provide proper guidance, on the judicious selection of antibiotics. In addition, rapid implementation of remedial measures upon the detection of antibiotic-resistant bacteria is essential.
Limitations
Limitations of this study include the small sample size, the restricted period of collection, and the lack of advanced techniques for the identification of fastidious bacterial pathogens.
Conclusion
Medical equipment and inanimate objects in the surgical ward were heavily contaminated with different species of bacterial pathogens, followed by the pediatric and the NICU. The predominant bacteria responsible for the contamination of patient-care equipment and inanimate objects were S. aureus, CoNS, Klebsiella spp., and Acinetobacter spp. Antimicrobial-susceptibility tests revealed that bacterial isolates were resistant to multiple antibiotics, indicating a high risk of nosocomial outbreaks due to drug-resistant bacteria. Therefore, stringent infection-prevention and control programs comprising routine sampling from patient-care equipment and inanimate objects among wards must be implemented, along with antimicrobial-resistance surveillance and decontamination efforts.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Haque M, Sartelli M, McKimm J, Bakar MA. Health care-associated infections – an overview. Infect Drug Resist. 2018;11:2321–2333. doi:10.2147/IDR.S177247
2. Health care-associated infections fact sheet [Internet]. Available from: https://www.who.int/gpsc/country_work/gpsc_ccisc_fact_sheet_en.pdf.
3. Yallew WW, Takele AK, Yehuala FM. Point prevalence of hospital-acquired infections in two teaching hospitals of Amhara region in Ethiopia. Drug Healthc Patient Saf. 2016;8:71–76. doi:10.2147/DHPS.S107344
4. Khan HA, Baig FK, Mehboob R. Nosocomial infections: epidemiology, prevention, control and surveillance. Asian Pac J Trop Biomed. 2017;7(5):478–482. doi:10.1016/j.apjtb.2017.01.019
5. Kramer A, Assadian O. Survival of microorganisms on inanimate surfaces. In: Use of Biocidal Surfaces for Reduction of Healthcare Acquired Infections. Borkow G (editor), Springer International Publishers, 2014:7–26.
6. Wang M, Wei H, Zhao Y, et al. Analysis of multidrug-resistant bacteria in 3223 patients with hospital-acquired infections (HAI) from a tertiary general hospital in China. Bosn J Basic Med Sci. 2019;19(1):86–93. doi:10.17305/bjbms.2018.3826
7. Mbim EN, Mboto CI, Edet UO. Plasmid profile analysis and curing of multidrug resistant bacteria isolated from two hospital environments in Calabar Metropolis, Nigeria. Asian J Med Health. 2016;1:1–11. doi:10.9734/AJMAH/2016/28587
8. Sastry AS, Sandhya BK. Essentials of Medical Microbiology.
9. Yusha’u M, Bukar A, Aliyu BS, Abdulkareem A. Bacterial contamination of some hospital equipment in Kano, Nigeria. Hamdard Med. 2012;55:3.
10. Ahmed EH, Hassan HM, El-Sherbiny NM, Soliman AMA. Bacteriological monitoring of inanimate surfaces and equipment in some referral hospitals in Assiut City, Egypt. Int J Microbiol. 2019;2019:5907507. doi:10.1155/2019/5907507
11. Gelaw A, Gebre-Selassie S, Tiruneh M, Mathios E, Yifru S. Isolation of bacterial pathogens from patients with postoperative surgical site infection and possible sources of infection at university of Gondar hospital, northwest Ethiopia. J Environ Occup Sci. 2014;3:103–108. doi:10.5455/jeos.20140512124135
12. Weldegebreal F, Admassu D, Meaza D, Asfaw M. Non-critical healthcare tools as a potential source of healthcare-acquired bacterial infections in eastern Ethiopia: a hospital-based cross-sectional study. SAGE Open Med. 2019;7:205031211882262. doi:10.1177/2050312118822627
13. Darge A, Kahsay AG, Hailekiros H, Niguse S, Abdulkader M. Bacterial contamination and antimicrobial susceptibility patterns of intensive care units medical equipment and inanimate surfaces at ayder comprehensive specialized hospital, Mekelle, Northern Ethiopia. BMC Res Notes. 2019;12(1):621. doi:10.1186/s13104-019-4658-5
14. Worku T, Derseh D, Kumalo A. Bacterial profile and antimicrobial susceptibility pattern of the isolates from stethoscope, thermometer, and inanimate surfaces of Mizan-Tepi University Teaching Hospital, Southwest Ethiopia. Int J Microbiol. 2018;2018:1–7. doi:10.1155/2018/9824251
15. Holt JG, Krieg NR, Sneath PHA, Staley JT, Williams ST. Bergey’s Manual of Determinative Bacteriology.
16. Bauer AW, Kirby WM, Sherris JC, Turck M. Antibiotic susceptibility testing by a standardized single disk method. Am J Clin Pathol. 1966;45(4_ts):493–496. doi:10.1093/ajcp/45.4_ts.493
17. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing. Wayne: CLSI; 2016.
18. Getachew H, Derbie A, Mekonnen S. Surfaces and air bacteriology of selected wards at a referral hospital, Northwest Ethiopia: a Cross-Sectional Study. Int J Microbiol. 2018;2018.
19. Maina SM, Nyerere AK, Ngugi CW. Isolation of bacterial diversity present in medical waste and health care settings in hospitals in Kenya. Afr J Microbiol Res. 2018;12:606–615. doi:10.5897/AJMR2018.8876
20. Chikere C, Omoni V, Chikere B. Distribution of potential nosocomial pathogens in a hospital environment. Afr J Biotechnol. 2008;7:3535–3539.
21. Shiferaw T, Beyene G, Kassa T, Sewunet T. Bacterial contamination, bacterial profile and antimicrobial susceptibility pattern of isolates from stethoscopes at Jimma University Specialized Hospital. Ann Clin Microbiol Antimicrob. 2013;12(1):39. doi:10.1186/1476-0711-12-39
22. Willey JM, Sherwood LM, Woolverton CJ. Prescott, Harley and Klein’s Microbiology.
23. Maryam A, Usman-Sani H, Usman MA. Characterization and determination of antibiotic susceptibility pattern of bacteria isolated from some fomites in a teaching hospital in northern Nigeria. Afr J Microbiol Res. 2014;8:814–818. doi:10.5897/AJMR2013.6512
24. Garcia-Cruz CP, Aguilar MJN, Arroyo-Helguera OE. Fungal and bacterial contamination on indoor surfaces of a hospital in Mexico. Jundishapur J Microbiol. 2012;5:460–464. doi:10.5812/jjm.2625
25. Teng S-O, Lee W-S, Ou T-Y, Hsieh Y-C, Lee W-C, Lin Y-C. Bacterial contamination of patients‘ medical charts in a surgical ward and the intensive care unit: impact on nosocomial infections. J Microbiol Immunol Infect. 2009;42(1):86–91.
26. Abubakar AS, Barma MM, Balla HJ, et al. Spectrum of bacterial isolates among intensive care unit patients in a tertiary hospital in Northwestern Nigeria. Indian J Sci Res Technol. 2014;2:42–47.
27. Ekrami AR, Kayedani A, Jahangir M, Kalantar E, Jalali M. Isolation of common aerobic bacterial pathogens from the environment of seven hospitals, Ahvaz, Iran. Jundishapur J Microbiol. 2011;4:75–82.
28. Bakkali MEL, Hmid K, Kari KE, Zouhdi M, Mzibri MEL, Laglaoui A. Characterization of bacterial strains and their resistance status in hospital environment. J Trop Dis. 2015;4:180. doi:10.4172/2329-891X.1000180
29. Kim LJ, Lee H, Kim H, Chang K. Isolation frequency and antimicrobial susceptibility of bacterial pathogens isolated from physical therapeutic instruments in general hospitals. J Phys Ther Sci. 2010;22:61–67. doi:10.1589/jpts.22.61
30. Ayatollahi AA, Amini A, Rahimi S, Takrami SR, Darsanaki RK, Nezhad MS. Prevalence of gram-negative bacilli isolated from the equipment and surfaces in hospital wards of Golestan Province, North of Iran. Eur J Microbiol Immunol. 2017;7(4):261–266. doi:10.1556/1886.2017.00015
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.