Back to Journals » Journal of Inflammation Research » Volume 11
Magnesium deficiency and increased inflammation: current perspectives
Authors Nielsen FH
Received 11 October 2017
Accepted for publication 12 December 2017
Published 18 January 2018 Volume 2018:11 Pages 25—34
DOI https://doi.org/10.2147/JIR.S136742
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Forrest H Nielsen
Research Nutritionist Consultant, Grand Forks, ND, USA
Abstract: Animal studies have shown that magnesium deficiency induces an inflammatory response that results in leukocyte and macrophage activation, release of inflammatory cytokines and acute-phase proteins, and excessive production of free radicals. Animal and in vitro studies indicate that the primary mechanism through which magnesium deficiency has this effect is through increasing cellular Ca2+, which is the signal that results in the priming of cells to give the inflammatory response. Primary pro-inflammatory cytokines such as tumor necrosis factor-α and interleukin (IL)-1; the messenger cytokine IL-6; cytokine responders E-selectin, intracellular adhesion molecule-1 and vascular cell adhesion molecule-1; and acute-phase reactants C-reactive protein and fibrinogen have been determined to associate magnesium deficiency with chronic low-grade inflammation (inflammatory stress). When magnesium dietary intake, supplementation, and/or serum concentration suggest/s the presence of magnesium deficiency, it often is associated with low-grade inflammation and/or with pathological conditions for which inflammatory stress is considered a risk factor. When magnesium intake, supplementation, and/or serum concentration suggest/s an adequate status, magnesium generally has not been found to significantly affect markers of chronic low-grade inflammation or chronic disease. The consistency of these findings can be modified by other nutritional and metabolic factors that affect inflammatory and oxidative stress. In spite of this, findings to date provide convincing evidence that magnesium deficiency is a significant contributor to chronic low-grade inflammation that is a risk factor for a variety of pathological conditions such as cardiovascular disease, hypertension, and diabetes. Because magnesium deficiency commonly occurs in countries where foods rich in magnesium are not consumed in recommended amounts, magnesium should be considered an element of significant nutritional concern for health and well-being in these countries.
Keywords: magnesium deficiency, magnesium adequacy, inflammatory stress, oxidative stress, chronic disease
Introduction
Over 85 years ago, findings were obtained that indicated magnesium deprivation in rats resulted in an inflammatory response.1 However, it was in the 1990s when evidence showing that magnesium deficiency is associated with pathological conditions characterized as having a chronic inflammatory stress (heightened inflammatory response) component gained momentum. As reviewed in 2007, animal experiments found that limiting magnesium intake to less than 10% of the recognized requirement resulted in an inflammatory response characterized by leukocyte and macrophage activation, release of inflammatory cytokines and acute-phase proteins, and excessive production of free radicals.2 Another review emphasized the roles of pro-inflammatory neuropeptide substance P and calcitonin – gene-related peptide in inflammatory stress induced by severe magnesium deficiency in rats.3 At first glance, these findings could be considered irrelevant for humans because they were obtained by using deficient magnesium intakes that are unlikely for humans based on dietary surveys.4 Most people will have intakes that meet at least 50% of the current US Estimated Average Requirement (EAR).4 Animal experiments in which moderate-to-marginal or subclinical (~50% to less than 100% of recognized requirement) magnesium was fed relatively short-term (several weeks) have not been found to markedly affect variables associated with inflammatory stress.5,6 However, a small number of animal studies indicate that a subclinical or moderate magnesium deficiency can result in inflammatory stress if the deficiency is long-term. Reduction of dietary magnesium to 25% and 50% of the requirement for 3–6 months increased substance P and tumor necrosis factor-α (TNF-α) in tibia bone of rats.7,8 Long-term moderate magnesium deficiency (150 mg or 6.2 mmol magnesium/kg diet) during aging was found to increase inflammatory and oxidative stress and thus cardiovascular risks in rats.9,10 Animal studies also indicate that environmental or nutritional factors increasing the need for magnesium or causing inflammatory and oxidative stress can result in relatively short-term magnesium deficiency inducing or exacerbating increased inflammation. For example, the fatty acid composition of the diet, which can affect inflammatory and oxidative stress, was found to alter the response to marginal magnesium deficiency in rats.11 The epidermal growth factor receptor tyrosine kinase inhibitor, erlotinib (Tarceva), was found to induce mild magnesium deficiency that triggered substance P-mediated oxidative/inflammatory stress in rats.12 Although limited in number, these latter studies suggest that animal findings involving inflammatory stress can be reasonably extrapolated to humans.
Plausible mechanism through which magnesium deficiency is linked to increased inflammation and resulting oxidative pathology
Animal and in vitro studies indicate a plausible mechanism through which magnesium deficiency induces increased inflammation resulting in an increased risk for chronic disease. The increased inflammation can involve the priming of phagocytic cells to give an inflammatory response; increasing substance P, a tachykinin neuropeptide that induces the production of proinflammatory cytokines; and activating nuclear factor-kappa β (NFκβ), a transcription factor responsible for the expression of inflammation-related genes. As described in a review, animal studies show that magnesium deficiency enhances the recruitment of phagocytic cells to perform their effector functions, which ultimately leads to the generation of reactive oxygen species.13 Excessive or chronic production of reactive oxygen species (oxidative stress) pathologically affecting tissue is a reason that inflammatory stress is considered a risk factor for numerous chronic diseases. Priming agents are needed to stimulate phagocytic cells to produce reactive oxygen species. These priming agents do not elicit oxidative effects but stimulate the production of other factors that do. The priming agent can be cytokines such as TNF-α, whose release is induced by increased intracellular Ca2+, which is considered a signal to initiate the inflammatory process. The increase in cellular Ca2+ could occur through magnesium deficiency activating the L-type calcium channel.14 Increased intracellular Ca2+ also could occur through enhanced activation of the of N-methyl-D-aspartate (NMDA) receptor.3,15 It has been hypothesized that increased intracellular Ca2+ via the NMDA receptor is the stimulus for increased production of substance P in the primary sensory (C) fibers that increases pro-inflammatory cytokines and ultimately causes neuronal injury through oxidative activity in magnesium-deficient animals.3 Recent studies also have indicated that pro-inflammatory cytokine production induced by magnesium deficiency involves NFκβ, including TNF-α and IL-1β.16,17 L-type calcium channels were found to be involved in magnesium supplementation attenuating the production of pro-inflammatory cytokines whose production was increased by NFκβ.14,16
All the systems involved in magnesium deficiency affecting inflammatory stress already described involve magnesium’s role as a physiologic Ca2+ channel blocker, that is, in magnesium deficiency, cellular Ca2+ increases through an influx from extracellular sources via slow Ca2+ transport channels, and the release from intracellular stores such as the sarcoplasmic reticulum. This suggests that increasing cellular Ca2+ is the primary mechanism through which magnesium deficiency induces inflammatory stress.
Markers of chronic inflammatory stress used in magnesium deficiency studies
Numerous substances have been used to determine whether increased chronic low-grade inflammation has occurred that could lead to pathological effects. Many of these are used to associate magnesium deficiency with increased inflammation and are described in an American Heart Association/Center for Disease Control and Prevention Scientific Statement.18 The substances include primary pro-inflammatory cytokines TNF-α and interleukin-1 (IL-1); the messenger cytokine IL-6; cytokine responders E-selectin, P-selectin, intracellular adhesion molecule-1 (ICAM-1) and vascular cell adhesion molecule-1 (VCAM-1); and acute-phase reactants C-reactive protein (CRP), fibrinogen and serum amyloid A. In this statement, CRP was determined to be a useful marker of inflammatory stress that could lead to atherosclerosis, with a value of >3.0 mg/L indicating a high risk of inflammatory stress. Based on the statement, CRP is one of the more commonly used markers of inflammatory stress in pathological conditions, especially chronic diseases, associated with magnesium deficiency.
Determination of magnesium deficiency in humans
Because magnesium has so many critical functions, the body has mechanisms to assure that it is readily available to perform them. During low intakes of magnesium, the percent absorbed from the diet is increased, the amount in urine is decreased, and body reserves (bone is the major reserve) are used. When the dietary intake of magnesium is adequate, the opposite occurs. Thus, the response of the body to maintain magnesium homeostasis when changes in dietary intakes occur has made it difficult to establish indicators and dietary intakes disclosing the presence of magnesium deficiency. Dietary intake and serum concentration of magnesium usually are used as markers of magnesium status. In 1997, the USA and Canada set the EAR and Recommended Dietary Allowance (RDA) for adult women at 255–265 mg (10.49–10.90 mmol)/day and 310–320 mg (12.75–13.16 mmol)/day, respectively.19 The EAR and RDA, respectively, for adult men were set at 330–350 mg (13.57–14.40 mmol)/day and 410–420 mg (16.86–17.28 mmol)/day.19 These Dietary Reference Intakes (DRIs) were based on highly variable balance data from 16 men and 18 women on self-selected diets with reduced magnesium during the period when balance determinations were made. The current reference interval for serum magnesium of 0.75–0.95 mmol/L (1.82–2.30 mg/dL) is based on data reported in 1974.20 This reference value was based on the distribution of serum magnesium in a normal population, not on the basis of a relationship between serum magnesium and clinical outcomes.
Since the DRIs and serum reference values for magnesium were established, data have accumulated indicating that using these values might be of questionable validity for establishing the likelihood of a subclinical magnesium deficiency in an individual. The newer data indicate that the DRIs might be too high for some individuals and the “normal” serum reference range might include some magnesium-deficient individuals. Thus, using the current old reference values could result in the conclusion that some individuals are subclinical magnesium deficient when they have an adequate magnesium status, or vice versa. This could be partly the basis for magnesium deficiency not being consistently found in pathological conditions with which it is often associated, and for assumed magnesium-deficient individuals to not always exhibit some type of pathology.21
Balance data obtained since 1997 indicate that the EAR and RDA for magnesium should be 175 and 250 mg (7.20 and 10.28 mmol)/day, respectively, for 70 kg healthy individuals, and increase or decrease based on body weight.22,23 Data from balance studies indicate that 40–80 mg (1.65–3.29 mmol) magnesium/day is excreted when magnesium intakes are less <250 mg (10.28 mmol)/day and 80–160 mg (3.29–6.58 mmol)/day when intakes are >250 mg (10.28 mmol)/day.23 It should be noted that urinary magnesium excretion changes within a few days after any significant change in magnesium intake.23 Thus, a single 24-hour determination of urinary magnesium would not be useful as an indicator of current magnesium status because magnesium excretion may be low while the individual still has an adequate status, and vice versa. However, urinary magnesium would be useful in indicating magnesium intakes or status in population studies. Metabolic unit depletion/repletion experiments show that serum magnesium concentrations decrease only after a prolonged depletion if an individual starts with an adequate magnesium status. As a result, individuals with serum magnesium concentrations in excess of 0.75 mmol/L (1.82 mg/dL) might be magnesium deficient because such individuals respond to magnesium supplementation.23 This is consistent with a recent workshop conclusion that some individuals within the “normal” reference range for serum magnesium could be subclinical magnesium deficient.24 Recent evaluations of serum magnesium as an indicator of status have indicated individuals with serum magnesium values ≤0.75 mmol/L (1.82 mg/dL) most likely are magnesium deficient and those with values of >0.85 mmol/L (2.07 mg/dL) are most likely magnesium adequate.23–25 Individuals with serum magnesium concentrations between these values need the determination of additional measures to establish magnesium deficiency or adequacy. A urinary excretion of <80 mg (3.29 mmol)/day and/or a dietary intake history showing a magnesium intake of <250 mg (10.28 mmol)/day would support the presence of magnesium deficiency, especially if there is a concurrent chronic disease that is associated with chronic inflammatory stress.23
The occurrence of subclinical magnesium deficiency based on set or suggested DRIs commonly occurs in countries in which magnesium-rich foods such as whole grains, pulses, nuts, and green vegetables are not regularly consumed. In the USA, a 2005–2006 survey indicated that ~60% of all adults did not meet the set EARs for magnesium.4 If the suggested RDA of 250 mg (10.28 mmol)/day for a healthy 70 kg person22,23 is used, the survey indicates that almost 50% of adult females and 25% of adult males still would have intakes less than recommended. Many individuals weigh more than 70 kg and thus it is likely that more than 25% of adults have usual intakes less than the suggested EAR of 175 mg (7.20 mmol) for a healthy 70 kg person.22,23
Magnesium deficiency and increased inflammation
A meta-analysis and systematic review of seven cross-sectional studies with a total of 32,198 individuals were performed to evaluate the effect of magnesium status on serum CRP concentrations.26 Meta-regression analysis found that dietary magnesium was significantly and inversely associated with serum CRP concentrations in four cross-sectional studies. In three of the studies where the data were appropriate to use, dietary intake ranged from 205 to 398 mg (8.43–16.37 mmol)/day. The three studies gave a pooled odds ratio of 1.49 (95% CI: 1.18–1.89) for a CRP of at least 3.0 mg/L for the lowest in comparison to the highest magnesium intake. A prospective cohort study also showed a significant inverse association between dietary magnesium intake and serum CRP concentration.27 In addition, with a comparison between apparently deficient to sufficient concentrations, serum magnesium concentration was significantly inversely correlated to serum CRP concentrations in two cross-sectional studies.26
Although CRP is commonly used to show an association between inflammatory stress and magnesium deficiency, the association has been substantiated by other indicators of inflammatory stress. In a cross-sectional study involving 192 non-diabetic, non-hypertensive participants, obese individuals were found to exhibit higher serum concentrations of TNF-α and lower serum concentrations of magnesium than lean and overweight individuals.28 In each group of 54, obese individuals had a mean serum magnesium concentration of 0.67 mmol/L and a TNF-α mean concentration of 8.4 pg/mL, whereas the lean and overweight individuals had mean magnesium concentrations of 0.83 and 0.81 mmol/L and mean TNF-α concentrations of 4.1 and 6.2 pg/mL, respectively. Elevated concentrations of TNF-α (≥3.5 pg/mL) were found in 91 individuals – 7 (10.9% of group), 31 (48.4% of group), and 43 (67.2% of group) in lean, overweight, and obese groups, respectively.28 The odds ratio between serum magnesium and TNF-α in obese individuals was 1.8 (95% CI: 1.2–9.1), and in lean and overweight individuals was 1.1 (CI: 0.7–8.7) and 1.3 (95% CI: 0.9–10.8), respectively. In another cross-sectional study involving 98 individuals newly diagnosed with metabolic syndrome, severe hypomagnesemia (≤0.49 mmol/L) but not hypomagnesemia (≥0.49–≤0.74 mmol/L), when compared to individuals with serum magnesium concentrations of >0.74 mmol/L (considered normomagnesemia), was associated with elevated concentrations of TNF-α.29 The odds ratio, adjusted by the obesity measure waist circumference, between serum TNF-α and severe hypomagnesemia was 3.7 (95% CI: 1.1–12.1) and hypomagnesemia was 1.6 (95% CI: 0.7–3.6). However, the odds ratio of 0.28 (95% CI: 0.1–0.6) for normomagnesemia indicated that magnesium had a protective role against elevated TNF-α. A more recent cross-sectional study involving 300 individuals with known coronary heart disease found that serum TNF-α was significantly higher with serum magnesium concentrations ≤0.66 mmol/L than with higher concentrations, and with dietary intakes of ≤350 mg (14.40 mmol)/day compared to intakes >350 mg (14.40 mmol)/day.30 This study also found a similar result with IL-6, which confirmed earlier reports associating a lower magnesium status with higher serum IL-6. In the longitudinal Coronary Artery Risk Development in Young Adults (CARDIA) study involving 4,497 Americans, dietary magnesium intakes at baseline, 7 and 20 years and IL-6 at 20 years were determined.27 With quintiles in which the lowest intake was 99.9 mg/1,000 kcal (4.11 mmol)/4.2 MJ) and the highest was 201.5/1000 kcal (8.35 mmol/ 4.2 MJ), dietary magnesium intake was inversely associated with serum IL-6 concentration. In the Women’s Health Initiative Observational Study (WHI-OS), dietary magnesium and IL-6 were measured at baseline in 3,713 postmenopausal women free of cardiovascular disease, cancer, and diabetes.31 With quintiles of magnesium intakes ranging from 168.5 to 310.2 mg/day (6.93–12.76 mmol/day), an increase in 100 mg (4.12 mmol)/day in magnesium was inversely associated with serum IL-6 concentration. Interestingly, the inverse relationship was more obvious in overweight than in normal weight women. The WHI-OS study also found that an increase of 100 mg (4.12 mmol)/day in magnesium intake was inversely associated with the serum adhesion factor VCAM-1.31 The CARDIA study also found that magnesium intake was inversely associated with the acute-phase reactant fibrinogen in serum.27
Although cross-sectional studies suggest that dietary magnesium deficiency is a risk factor for chronic low-grade inflammation, it cannot be discounted that the deficiency association with inflammatory stress is confounded by another dietary factor concurrently occurring with the low intake. A recent report stated that 45 dietary factors are associated with the serum concentrations of six inflammatory markers according to peer-reviewed publications through 2010.32 Thus, intervention studies may give a better indication of whether magnesium deficiency is a significant contributor to inflammatory stress that can lead to pathological conditions. The review by Dibaba et al evaluated five intervention studies that used serum magnesium concentration as a marker of magnesium status.26 Three studies involved participants with elevated serum CRP concentrations (≥3.0 mg/L) and deficient serum magnesium concentrations (<0.75 mmol/L) that were increased by magnesium supplementation.33–35 The magnesium supplementation alleviated elevated serum CRP concentrations. A similar finding was obtained in a subsequent randomized double-blind placebo-controlled study of 62 men and women.36 Magnesium supplementation decreased highly elevated CRP more than did the placebo. Although the placebo group also exhibited decreased serum CRP at the end of the study, it was still elevated compared to the supplemented group (17.5 vs 4.8 nmol/L). The placebo attenuation finding was attributed to diet intervention and exercise during the study that had anti-inflammatory stress effects. In the review by Dibaba et al, two studies did not show a significant effect of magnesium supplementation on serum CRP.26 In both of these studies, the participants did not have elevated serum CRP concentrations (<3.0 mg/L) and had serum magnesium concentrations indicating an adequate magnesium status (~0.80 and 0.90 mmol/L, respectively).37,38 Further evidence that the participants in these studies were magnesium adequate was that the magnesium supplementation did not significantly increase serum magnesium concentrations. Without a magnesium deficiency to induce or exacerbate an elevated CRP and without an elevated CRP to be attenuated with magnesium supplementation, it might be predicted that these two studies would not show an effect of magnesium on a marker of chronic low-grade inflammation. A recent study that also found magnesium supplementation did not significantly affect markers of chronic low-grade inflammation can be critiqued in a similar manner.39 Magnesium was supplemented for 24 weeks in 52 overweight/obese individuals with mean serum magnesium concentrations ranging from 0.84 to 0.87 mmol/L. In these apparently magnesium-adequate individual, magnesium supplementation did not decrease adhesion factors serum VCAM-1, ICAM-1, and E-selectin.39 A recent systematic review and meta-analysis of randomized controlled trials support the suggestion that magnesium supplementation will affect markers of inflammatory stress only when they are elevated.40 In the overall meta-analysis, magnesium treatment did not significantly affect CRP. However, when the analysis was stratified to compare subgroups of studies in populations with baseline plasma/serum CRP concentrations of ≤3 mg/L and >3 mg/L, magnesium treatment significantly decreased CRP in the latter group.40
Magnesium deficiency in pathological conditions characterized with an inflammatory stress component
The concept that a moderate or subclinical magnesium deficiency can eventually induce chronic low-grade inflammation by itself or exacerbate inflammatory stress caused by other factors is supported by numerous studies showing an association between a low magnesium status and pathological conditions for which chronic low-grade inflammation is considered a risk factor (see Table 1). The pathological conditions receiving the most attention are hypertension, cardiovascular disorders, the metabolic syndrome, and diabetes.
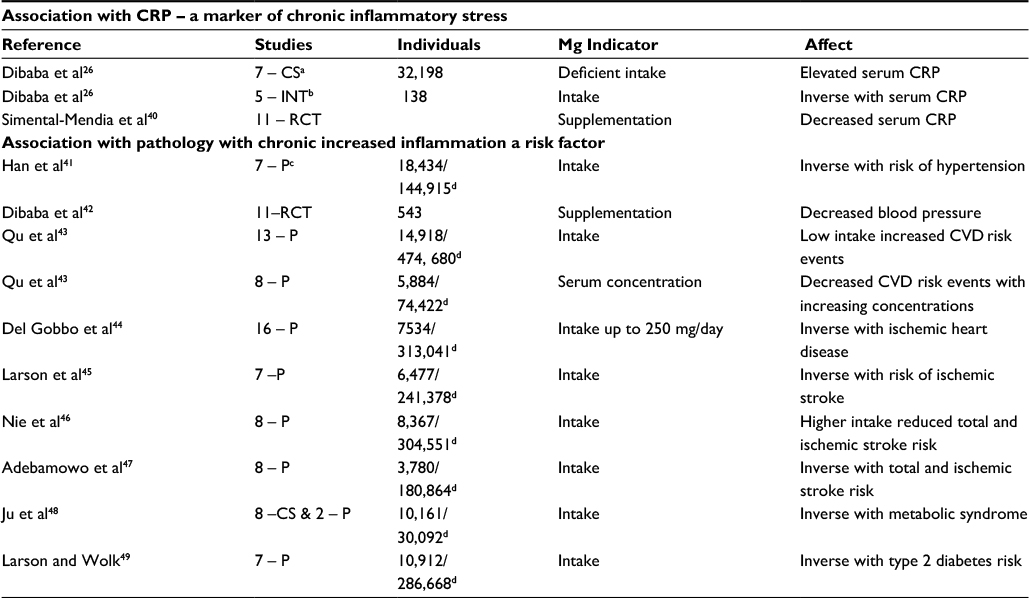 | Table 1 Summary of meta-analyses indicating that magnesium deficiency is associated with increased inflammation Notes: aCS, cross-sectional studies; bINT, intervention trials; cP, prospective studies; dcases or events/sample size. Abbreviations: CRP, C-reactive protein; CVD, cardiovascular disease; RCT, randomized controlled trial. |
In a meta-analysis of six studies involving 20,119 cases of hypertension, an inverse relationship was found between dietary magnesium and hypertension when the highest magnesium intake group (mostly >300 mg [12.34 mmol]/day) was compared to the lowest magnesium intake group (mostly <200 mg [8.23 mmol]/day) in each study.41 A 100 mg (4.11 mmol)/day increment in magnesium intake was associated with a 5% reduction in the risk of hypertension. Another meta-analysis that included 11 studies with 543 individuals with insulin resistance, prediabetes, or non-communicable disease found that magnesium supplementation (365–450 mg [15.0–18.5 mmol]/day) for a median of 3.6 months gave mean reductions of 4.18 mm mercury (Hg) in systolic blood pressure and 2.27 mm Hg in diastolic blood pressure.42
A meta-analysis of 19 studies with 532,979 participants found an inverse association between dietary magnesium and the risk for cardiovascular events such as coronary heart disease, stroke, and cardiac disease mortality.43 The greatest risk reduction occurred when magnesium intake increased from 150 to 400 mg (6.17–16.45 mmol)/day. A meta-analysis of 16 studies comprising 313,041 individuals, of which there were 7534 cases of ischemic heart disease and 2686 fatal ischemic heart disease events, found an inverse association between these events and magnesium intake.44 The inverse association was non-linear in which it occurred up to a threshold intake of ~250 mg (10.28 mmol)/day. Three meta-analyses have shown an inverse association between magnesium intake and stroke. In seven studies with 6477 cases of stroke among 241,378 participants, an intake increment of 100 mg (4.11 mmol)/day was associated with an 8% reduction for the risk of stroke.45 In a meta-analysis of eight studies that had 8367 stroke cases among 304,551 participants, an inverse association was found between magnesium intake and total stroke cases and the risk for ischemic stroke.46 The range of mean magnesium intakes for the quartiles or quintiles was 228–471 mg/day (9.38–19.37 mmol/day). In an analysis of 86,149 and 94,715 women in the Nurses’ Health Study I and II, respectively, 3780 stroke cases were documented.47 A comparison between the lowest quintiles of magnesium intake (226 and 240 mg/day or 9.30 and 9.87 mmol/day, respectively) and the highest quintiles of intake (387 and 434 mg/day or 15.92 and 17.84 mmol/day, respectively) in these two studies also found an inverse association with magnesium intake and total stroke cases and the risk for ischemic stroke.47
Meta-analyses also have been performed, which show an inverse association between magnesium intake and the metabolic syndrome and diabetes. Based on eight cross-sectional and two prospective cohort studies, a meta-regression determination found a generally linear inverse association between magnesium intake and the metabolic syndrome.48 The pooled relative risk for the metabolic syndrome per 150 mg (6.17 mmol)/day increment in magnesium intake was 0.88 (95% CI: 0.84–0.93). In all but one of seven cohort studies that included 286,668 participants and 10,192 cases of type II diabetes, an inverse relation between magnesium intake and the risk for diabetes was found.49 The overall relative risk for a 100 mg (4.11 mmol)/day increase in magnesium intake was 0.85 (95% CI: 0.79–0.92). Most recent support for the association between magnesium and diabetes is findings from the Canadian Health Measures Survey cycle 3 (2012 and 2013) involving 5561 individuals aged 3–79 years.50 Type 1 or 2 diabetes was associated with 0.04–0.07 mmol/L lower serum magnesium compared with not having diabetes. Serum magnesium concentration was not only negatively associated with diabetes, but also with serum glucose, serum insulin, hemoglobin A1c, and homeostatic model assessment of insulin resistance.50 A substantial percentage of adult sex-age groups and adolescents were found to have serum magnesium concentrations <0.75 mmol/L.50
Other pathological conditions for which low serum magnesium concentrations or dietary magnesium intake have been inversely associated include colon cancer and osteoporosis. In a meta-analysis that involved three case–control studies of colorectal adenomas and six prospective cohort studies of carcinomas, every 100 mg (4.11 mmol)/day increase in magnesium intake was associated with a 13% lower risk of colorectal adenomas and tumors.51 In the Kuopio Ischemic Heart Disease prospective cohort study involving 2245 men aged 42–61 years, low serum magnesium concentrations and magnesium intakes were associated with an increased risk for total and femoral fractures.52 The serum association was obtained by using quartiles in which the lowest concentration was 0.74 mmol/L and the highest was 0.89 mmol/L. A study involving 224 postmenopausal women found that those with magnesium intakes <237 mg (9.75 mmol)/day had poorer bone mineral contents, densities, and T scores than those with higher intakes.53 This study is consistent with a meta-analysis that found a marginally significant correlation between magnesium intake and bone mineral density of the femoral neck and total hip.54
Modifiers of the association between magnesium deficiency and pathology whose risk is increased by chronic low-grade inflammation
Not every study of a group of individuals has shown an association between magnesium intake or serum concentration and pathology whose risk is increased by inflammatory stress. With these studies, magnesium intakes and serum concentrations need to be closely examined. For example, in a prospective cohort of 39, 876 women aged 39–89 years with no history of cardiovascular disease or cancer, a median 10-year follow-up identified 1037 incident cases of cardiovascular disease.55 Comparing the highest quintile of magnesium intake (median 433 mg [17.81 mmol]/day) with the lowest quintile (median 255 [10.48 mmol]/day) found that magnesium intake was not significantly associated with incident cardiovascular disease. Based on the suggested DRIs for a 70 kg person,22,23 the dietary intakes could be considered adequate for most of the women whose mean body mass indexes (BMIs) ranged between 25.2 and 26.7 kg/m2. In another study of 23,366 Swedish men aged 45–79 years, dietary magnesium intake was not associated with all-cause cardiovascular disease or cancer mortality.56 In this study, mean tertile magnesium intakes ranged from 387 to 523 mg (15.92–21.51 mmol)/day; these intakes indicated that most of the individuals did not have a deficient magnesium intake based on the 1997 DRIs19 or the suggested DRIs for 70 kg individuals.22,23 The findings in these studies indicating an adequate intake of magnesium was not associated with the chronic disease studied, is consistent with the comparison of populations with baseline plasma/serum CRP concentrations of ≤3 mg/L and >3 mg/L; magnesium supplementation significantly decreased CRP concentrations in the population with >3 mg/L.40 The negative findings with apparent adequate magnesium intakes or serum concentrations conform to the concept that the response or beneficial effect of a nutrient as it approaches adequacy will decrease based on the typical, sigmoid-shaped dose response to a nutrient deficiency.57 In other words, no effect is likely to be seen with an increased intake of a nutrient in individuals with an adequate status, while an effect is likely if the starting status of the nutrient is deficient.
Another possible reason for not consistently finding an apparent magnesium deficiency significantly associated with chronic low-grade inflammation or pathological conditions whose risk is increased by inflammatory stress is that other dietary factors or metabolic changes have not been factored in the analysis. The relationship between calcium, vitamin D, and protein is an example of how the response to a nutrient may depend upon the status of another nutrient.57 As indicated by animal experiments described in the Introduction, the detrimental effect of magnesium deficiency may be magnified if other factors are present such as nutrient deficiencies or metabolic changes that have a similar detrimental effect. Conversely, the effect of magnesium deficiency may be attenuated if other factors with similar beneficial effects, such as on inflammatory or oxidative stress, are provided in sufficient amounts.
An example of how magnesium deficiency effects can be modified is its relationship with obesity and its associated risk for chronic disease. Numerous experimental, epidemiological, and clinical studies have shown that obesity is associated with chronic low-grade inflammation that increases inflammatory signaling pathway activation and cytokine and acute-phase reactants production.58 For example, in a cross-sectional study of 16,573 individuals in the third NHANES study (1988–1994), logistic regression analysis found odds ratios for an elevated serum CRP concentration among individuals with BMIs of 25<30, 30<35, 35<40, and ≥40 kg/m2 were 1.51. 3.9, 6.11, and 9.30, respectively.59 Another cross-sectional study found that CRP and IL-6 increased significantly with increasing adiposity in children.60
However, similar to magnesium-deficient individuals, not all overweight and obese individuals exhibit signs of chronic low-grade inflammation or associated pathological conditions.28,38,61 This lack of inflammatory stress may be caused by attenuation through increased intakes of long-chain ω-3 fatty acids, antioxidant vitamins, and plant flavonoids.62 For example, intakes of total fat, the antioxidant vitamins C and E, and carotene were determinants of subclinical inflammation in overweight Swiss children.60
Magnesium deficiency or sufficiency also may be factors of whether chronic low-grade inflammation occurs in obesity. Several studies have found that obese individuals are more likely to have serum magnesium concentrations indicative of magnesium deficiency.28,38,63 In these studies, the magnesium deficiency in obesity is associated with chronic low-grade inflammation. Other studies have found markers of inflammatory stress not elevated in obese or overweight individuals with serum magnesium concentrations indicating adequacy.38,39 Conversely, obesity or being overweight may be significant factors in finding an association between magnesium and chronic low-grade inflammation. Obese and overweight individuals might have a higher magnesium requirement to counteract chronic low-grade inflammation. In addition, these individuals often having fat- and sugar- rich diets deficient in magnesium, which would make them at risk for a more severe magnesium deficiency that induces chronic low-grade inflammation.
Because chronic low-grade inflammation and resulting oxidative stress can be attenuated by factors such as increased intakes of long-chain ω-3 fatty acids, antioxidant vitamins, and plant flavonoids, or enhanced by deficient nutrients that induce inflammatory and oxidative stress,62 it is likely that these factors would also magnify or attenuate the response to magnesium deficiency. In addition, the possible involvement of a low magnesium status in the induction of chronic low-grade inflammation by other factors may not be recognized.
Conclusion
Many factors affect the determination of the extent to which magnesium deficiency has a role in the occurrence of chronic low-grade inflammation that increase the risk for chronic disease. However, because of magnesium’s role as a physiologic Ca2+ channel blocker, the indication of widespread inadequate intakes of magnesium, and large number of reports associating magnesium deficiency with inflammatory and oxidative stress, the role of magnesium can be considered extensive.
Disclosure
The author reports no conflicts of interest in this work.
References
Kruse HD, Orent ER, McCollum EV. Studies on magnesium deficiency in animals. I. Symptomatology resulting from magnesium deprivation. J Biol Chem. 1932;96:519–539. | ||
Mazur A, Maier JA, Rock E, Gueux E, Nowacki W, Rayssiguier Y. Magnesium and the inflammatory response: potential physiopathological implications. Arch Bioch Biophys. 2007;458(1):48–56. | ||
Weglicki WB. Hypomagnesemia and inflammation: clinical and basic aspects. Ann Rev Nutr. 2012;32:55–71. | ||
Moshfegh A, Goldman J, Ahuja J, Rodes D, LaComb R. What We Eat in America, NHANES 2005-2006: Usual Nutrient Intakes from Food and Water Compared to 1997 Dietary Reference Intakes for Vitamin D, Calcium, Phosphorus, and Magnesium. US Department of Agriculture, Agricultural Research Service; 2009. Available from: http://www.ars.usda.gov/ba/bhnrc/fsrg. Accessed November, 2009. | ||
Vormann J, Günther T, Höllriegl V, Schümann K. Pathobiochemical effects of graded magnesium deficiency in rats. Z Ernährungswiss. 1998;37(Suppl 1):92–97. | ||
Kramer JH, Mak IT, Phillips TM, Weglicki WB. Dietary magnesium intake influences circulating pro-inflammatory neuropeptide levels and loss of myocardial tolerance to postischemic stress. Exp Bio Med (Maywood). 2003;228(6):665–673. | ||
Rude RK, Gruber HE, Norton HJ, Wei LY, Frausto A, Kilburn J. Dietary magnesium reduction to 25% of nutrient requirement disrupts bone and mineral metabolism in the rat. Bone. 2005;37(2):211–219. | ||
Rude RK, Gruber HE, Norton HJ, Wei LY, Frausto A, Kilburn J. Reduction of dietary magnesium by only 50% in the rat disrupts bone and mineral metabolism. Osteoporos Int. 2006;17(7):1022–1032. | ||
Blache D, Devaux S, Joubert O, et al. Long-term moderate magnesium-deficient diet shows relationships between blood pressure, inflammation and oxidant stress defense in aging rats. Free Radic Biol Med. 2006;41(2):277–284. | ||
Adrian M, Chanut E, Laurant P, Gaume V, Berthelot A. A long-term moderate magnesium-deficient diet aggravates cardiovascular risks associated with aging and increases mortality in rats. J Hypertens. 2008;26(1):44–52. | ||
Nielsen FH. Dietary fatty acid composition alters magnesium metabolism, distribution, and marginal deficiency response in rats. Magnes Res. 2009;22(4):280–288. | ||
Mak IT, Kramer JH, Chmielinska JJ, Spurney CF, Weglicki WB. EGFR-TKI, erlotinib, causes hypomagnesemia, oxidative stress and cardiac dysfunction: attenuation by NK-1 receptor blockade. J Cardiovasc Pharmacol. 2015;65(1):54–61. | ||
Libako P, Nowacki W, Rock E, Rayssiguier Y, Mazur A. Phagocyte priming by low magnesium status: input to the enhanced inflammatory and oxidative stress responses. Magnes Res. 2010;23(1):1–4. | ||
Lin CY, Tsai PS, Hung YC, Huang CJ. L-type calcium channels are involved in mediating the anti-inflammatory effects of magnesium sulphate. Br J Anaesth. 2010;104(1):44–51. | ||
Reynolds IJ. Intracellular calcium and magnesium: critical determinants of excitotoxicity? Prog Brain Res. 1998;116:225–243. | ||
Sugimoto J, Romani AM, Valentin-Torres AM, et al. Magnesium decreases inflammatory cytokine production: a novel innate immunomodulatory mechanism. J Immunol. 2012;188(12):L6338–L6346. | ||
Gao F, Ding B, Zhou L, Gao X, Guo H, Xu H. Magnesium sulfate provides neuroprotection in lipopolysaccharide-activated primary microglia by inhibiting NF-κ-β pathway. J Surg Res. 2013;184(2):944–950. | ||
Pearson TA, Mensah GA, Alexander RW, et al. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: a statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation. 2003;107(3):499–511. | ||
Food and Nutrition Board, Institute of Medicine. Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride. Washington, DC: National Academies Press; 1997. | ||
Lowenstein FW, Stanton MF. Serum magnesium levels in the United States, 1971–1974. J Amer Coll Nutr. 1986;5:399–414. | ||
Nielsen FH. Effects of magnesium depletion on inflammation in chronic disease. Curr Opin Clin Nutr Metab Care. 3014;17(6):525–530. | ||
Hunt CD, Johnson LK. Magnesium requirements, new estimates for men and women by cross-sectional statistical analysis of metabolic magnesium balance data. Am J Clin Nutr. 2006;84(4):843–852. | ||
Nielsen FH. Guidance for the determination of status indicators and dietary requirements for magnesium. Magnes Res. 2017;29(4):154–160. | ||
Costello RB, Elin RJ, Rosanoff A, et al. Perspective: the case for an evidence-based reference interval for serum magnesium: the time has come. Adv Nutr. 2016;7(6):977–993. | ||
Nielsen FH, Johnson LA. Data from controlled metabolic ward studies provide guidance for the determination of status indicators and dietary requirements for magnesium. Biol Trace Elem Res. 2017;177(1):43–52. | ||
Dibaba DT, Xun P, He K. Dietary magnesium intake is inversely associated with serum C-reactive protein levels: meta-analysis and systematic review. Eur J Clin Nut. 2014;68(4):510–516. | ||
Kim DJ, Xun P, Liu K, et al. Magnesium intake in relation to systemic inflammation, insulin resistance, and the incidence of diabetes. Diabetes Care. 2010;33(12):2604–2610. | ||
Rodriguez-Morán M, Guerrero-Romero F. Elevated concentrations of TNF-alpha are related to low serum magnesium levels in obese subjects. Magnes Res. 2004;17(3):189–196. | ||
Guerrero-Romero F, Bermudez-Peña C, Rodriguez-Morán M. Severe hypomagnesemia and low-grade inflammation in metabolic syndrome. Magnes Res. 2011;24(2):45–53. | ||
Mahalle N, Garg MK, Kulkarni MV, Naik SS. Relation of magnesium with insulin resistance and inflammatory markers in subjects with known coronary heart disease. J Cariovasc Dis Res. 2014;5:22–29. | ||
Chacko SA, Song Y, Nathan L, et al. Relations of dietary magnesium intake to biomarkers of inflammation and endothelial dysfunction in an ethnically diverse cohort of postmenopausal women. Diabetes Care. 2010;33(2):304–310. | ||
Shivappa N, Steck SE, Hurley TG, Hussey JR, Hebert JR. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014;17(8):1689–1696. | ||
Almoznino-Sarafian D, Berman S, Mor A, et al. Magnesium and C-reactive protein in heart failure: an anti-inflammatory effect of magnesium administration? Eur J Nutr. 2007;46(4):230–237. | ||
Nielsen FH, Johnson LK, Zeng H. Magnesium supplementation improves indicators of low magnesium status and inflammatory stress in adults older than 51 years with poor quality sleep. Magnes Res. 2010;23(4):158–168. | ||
Rodriguez-Hernandez H, Cervantes-Huerta M, Rodriguez-Moran M, Guerrero-Romero F. Oral magnesium supplementation decreases alanine aminotransferase levels in obese women. Magnes Res. 2010;23(2):90–96. | ||
Simental-Mendía LE, Rodríquez-Morán M, Guerrero-Romero F. Oral magnesium supplementation decreases C-reactive protein levels in subjects with prediabetes and hypomagnesemia: a clinical randomized double-blind placebo-controlled trial. Arch Med Res. 2014;45(4):325–330. | ||
Chacko SA, Sul J, Song Y, et al. Magnesium supplementation, metabolic and inflammatory markers, and global genomic and proteomic profiling: a randomized, double-blind, controlled, crossover trial in overweight individuals. Am J Clin Nutr. 2011;93(2):463–473. | ||
Moslehi N, Vafa M, Rahimi-Foroushani A, Golestan B. Effects of oral magnesium supplementation on inflammatory markers in middle-aged overweight women. J Res Med Sci. 2012;17(7):607–614. | ||
Joris PJ, Plat J, Bakker SJL, Mensink RP. Effects of long-term magnesium supplementation on endothelial function and cardiometabolic risk markers: A randomized controlled trial in overweight/obese subjects. Sci Rep. 2017;7(1):106. | ||
Simental-Mendia LE, Sahebkar A, Rodriguez-Morán M, Zambrano-Galvin G, Guerrero-Romero F. Effect of magnesium supplementation on plasma C-reactive protein concentrations: a systematic review and meta-analysis of randomized controlled trials. Curr Pharm Des. Epub 2017 May 25. | ||
Han H, Fang X, Wei X, et al. Dose-response relationship between dietary magnesium intake, serum magnesium concentration, and risk of hypertension: a systematic review and meta-analysis of prospective cohort studies. Nutr J. 2017;16(1):26. | ||
Dibaba DT, Xun P, Song Y, Rosanoff A, Shechter M, He K. The effect of magnesium supplementation on blood pressure in individuals with insulin resistance, prediabetes, or non-communicable chronic diseases: a meta-analysis of randomized controlled trials. Am J Clin Nutr. 2017;106(3):921–929. | ||
Qu X, Jin F, Hao Y, et al. Magnesium and the risk of cardiovascular events: a meta-analysis of prospective cohort studies. PLoS One. 2013;8(3):e57720. | ||
Del Gobbo LC, Imamura F, Wu JH, De Oliveira Otto MC, Chiuve SE, Mozaffarian D. Circulating and dietary magnesium and risk of cardiovascular disease: a systematic review and meta-analysis of prospective studies. Am J Clin Nutr. 2013;98(1):160–173. | ||
Larsson SC, Orsini N, Wolk A. Dietary magnesium intake and risk of stroke: a meta-analysis of prospective studies. Am J Clin Nutr. 2012;95(2):362–366. | ||
Nie ZL, Wang ZM, Zhou B, Tang ZP, Wand SK. Magnesium intake and incidence of stroke: meta-analysis of cohort studies. Nutr Metab Cardiovasc Dis. 2013;23(3):169–176. | ||
Adebamowo SN, Spiegelman D, Willett WC, Rexrode KM. Association between intakes of magnesium, potassium, and calcium and risk of stroke: 2 cohorts of US women and updated meta-analyses. Am J Clin Nutr. 2015;101(6):1269–1277. | ||
Ju SY, Choi WS, Ock SM, Kim CM, Kim DH. Dietary magnesium intake and metabolic syndrome in the adult population: dose response meta-analysis and meta-regression. Nutrients. 2014;6(12):6005–6019. | ||
Larsson SC, Wolk A. Magnesium intake and risk of type 2 diabetes: a meta-analysis. J Internal Med. 2007;262(2):208–214. | ||
Bertinato J, Wang KC, Hayward S. Serum magnesium concentrations in the Canadian population and associations with diabetes, glycemic regulation, and insulin resistance. Nutrients. 2017;9(3):E296. | ||
Wark PA, Lau R, Norat T, Kampman E. Magnesium intake and colorectal tumor risk: a case-control study and meta-analysis. Am J Clin Nutr. 2012;96(3):622–631. | ||
Kunutsor SK, Whitehouse MR, Blom AW, Laukkanen JA. Low serum magnesium levels are associated with increased risk of fractures: a long-term prospective cohort study. Eur J Epidemiol. 2017;32(7):593–603. | ||
Nielsen FH, Lukaski HC, Johnson LK, Roughead ZK. Reported zinc, but not copper, intakes influence whole-body bone density, mineral content, and T score responses to zinc and copper supplementation in healthy postmenopausal women. Brit J Nutr. 2011;106(12):1872–1879. | ||
Farsinejad-Marj M, Saneei P, Esmailzadeh A. Dietary magnesium intake, bone mineral density and risk of fracture: a systematic review and meta-analysis. Osteoporos Int. 2016;27(4):1389–1399. | ||
Song Y, Manson JE, Cook NR, Albert CM, Buring JE, Liu S. Dietary magnesium intake and risk of cardiovascular disease among women. Am J Cardiol. 2005;96(8):1135–1141. | ||
Kaluza J, Orsini N, Levitan EB, Brzozowska A, Roszkowski W, Wolk A. Dietary calcium and magnesium intake and mortality: a prospective study of men. Am J Epidemiol. 2010;171(7):801–807. | ||
Heaney RP. Guidelines for optimizing design and analysis of clinical studies of nutrient effects. Nutr Rev. 2014;72(1):48–54. | ||
Hevener AL, Febbraio MA; the Stock Conference Working Group. The 2009 Stock Conference report: inflammation, obesity and metabolic disease. Obesity Rev. 2010;11(9):635–644. | ||
Ford ES. Body mass index, diabetes, and C-reactive protein among U.S. adults. Diabetes Care. 1999;22(12):1971–1977. | ||
Aeberli I, Molinari L, Spinas G, Lehmann R, L’Allemand D, Zimmerman MB. Dietary intakes of fat and antioxidant vitamins are predictors of subclinical inflammation in overweight Swiss children. Am J Clin Nutr. 2006;84(4):746–755. | ||
Stępień M, Stępień A, Wlazel RN, Paradowski M, Banach M, Rysz J. Obesity indices and inflammatory markers in obese non-diabetic normo- and hypertensive patients: a comparative study. Lipids Health Dis. 2014;13:29. | ||
Calder PC, Albers R, Antoine JM, et al. Inflammatory disease processes and interactions with nutrition. Brit J Nutr. 2009;101(Suppl 1):S1–S45. | ||
Guerrero-Romero F, Rodríguez-Morán M. Relationship between serum magnesium levels, and C-reactive protein concentration, in non-diabetic, non-hypertensive obese subjects. Int J Obes Relat Metab Disord. 2002;26(4):469–474. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.