Back to Journals » Hepatic Medicine: Evidence and Research » Volume 17
MAFLD: A Comprehensive Review of the Link Between Metabolic Dysfunction and Cardiovascular Risk
Authors Mostafa AM, Pan Z, Yu ML ![]() , Örmeci N, Fouad Y, Eslam M
, Örmeci N, Fouad Y, Eslam M ![]()
Received 3 June 2025
Accepted for publication 12 August 2025
Published 19 August 2025 Volume 2025:17 Pages 75—90
DOI https://doi.org/10.2147/HMER.S506402
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gerry Lake-Bakaar
Alaa M Mostafa,1 Ziyan Pan,2 Ming-Lung Yu,3,4 Necati Örmeci,5 Yasser Fouad,1 Mohammed Eslam2
1Department of Gastroenterology, Hepatology and Endemic Medicine, Faculty of Medicine, Minia University, Minia, Egypt; 2Storr Liver Centre, Westmead Institute for Medical Research, Westmead Hospital and University of Sydney, Sydney, NSW, Australia; 3School of Medicine, College of Medicine and Center of Excellence for Metabolic Associated Fatty Liver Disease, National Sun Yat-sen University, Kaohsiung, Taiwan; 4Hepatobiliary Division, Department of Internal Medicine, Kaohsiung Medical University Hospital; College of Medicine and Center of Metabolic Disorders and Obesity, Kaohsiung Medical University, Kaohsiung, Taiwan; 5Department of Internal Medicine, Istanbul Health and Technology University, İstanbul, Türkiye
Correspondence: Mohammed Eslam, Storr Liver Centre, Westmead Institute for Medical Research, Westmead Hospital and University of Sydney, Westmead, Sydney, NSW, 2145, Australia, Tel +61 2 88907705, Email [email protected]
Abstract: Metabolic dysfunction-associated fatty liver disease (MAFLD) affects over 30% of the global population. It is a multisystem condition with a strong association with cardiovascular disease (CVD), the leading cause of mortality worldwide. Key shared mechanisms, including insulin resistance, systemic inflammation, oxidative stress, and genetic predisposition, couple MAFLD with increased risks of coronary artery disease, ischemic heart disease, and heart failure. Early detection via non-invasive imaging and biomarkers is crucial for effective risk stratification. Management strategies emphasize lifestyle modifications and the development of targeted pharmacotherapies addressing metabolic and inflammatory pathways. Understanding the interconnected pathogenic mechanisms facilitates personalized interventions to reduce morbidity and improve long-term outcomes. A multidisciplinary approach remains essential to prevent and manage the cardiovascular implications of MAFLD.
Keywords: fatty liver, cardiometabolic risk, metabolic dysfunction, pharmacotherapy
Introduction
Metabolic dysfunction-associated fatty liver disease (MAFLD), formerly known as non-alcoholic fatty liver disease (NAFLD), affects over 30% of the global adult population, posing a significant health, economic, and societal challenge worldwide.1,2 Over the last decade, there has been an 11.2% increase in age-standardized rates of MAFLD, which parallels the rising rates of obesity and type 2 diabetes mellitus (T2DM), reflecting a decline in overall global metabolic health.3,4 Alarmingly, the prevalence of MAFLD is also rising among adolescents and children.
The core pathogenesis basis of MAFLD is linked to metabolic dysfunction. The disease spectrum ranges from simple hepatic steatosis to more advanced stages, including steatohepatitis, fibrosis, and cirrhosis.5,6 MAFLD has emerged as a primary contributor to end-stage liver disease, hepatocellular carcinoma, and liver transplantation.7 Moreover, it is a multisystem disease that elevates the risk of T2DM, chronic kidney disease (CKD), cardiovascular disease (CVD), and various extra-hepatic cancers.8,9
Cardiovascular disease remains the primary cause of death worldwide and is the leading cause of mortality in patients with MAFLD. The prevalence of CVD is anticipated to increase, especially in low- and middle-income nations, driven by urbanization, an aging population, and shifts in lifestyle habits.10,11 A robust reciprocal correlation between MAFLD and CVD has been established through observational, cohort, and genetic studies, revealing various shared underlying pathogenic mechanisms.12
This review aims to provide an updated narrative on the relationship between MAFLD and CVD, emphasizing the key role of metabolic dysfunction in mediating this interaction. The implications for understanding pathogenesis, diagnosis, and management, particularly in relation to mitigating cardiovascular risk in MAFLD patients, will also be discussed.
Metabolic Health and Dysfunction
There is currently no clear consensus on the variables or cut-off values used to define metabolic health. However, it is typically regarded as the lack of cardiometabolic disease or risk factors that may contribute to the potential development of such diseases. Metabolic health is characterized by normal insulin sensitivity, balanced lipid profiles, stable blood pressure, and low levels of systemic inflammation.13
Metabolic dysfunction is a complex process that reflects a failure of metabolic homeostasis, which subsequently raises the risk of cardiometabolic diseases through several interconnected mechanisms.14 Key metabolic abnormalities, such as insulin resistance, elevated triglycerides, decreased HDL cholesterol, increased waist circumference, elevated fasting glucose, and a chronic low-grade inflammatory state, are frequently used to indicate metabolic dysfunction. This dysfunction is a pivotal determinant in the pathogenesis of MAFLD, with the risk of both hepatic and extra-hepatic outcomes increasing with the increase in the number of metabolic abnormalities present in a patient.15
Though MAFLD is typically associated with obesity, it is increasingly recognized in lean individuals, who constitute up to 40% of the total MAFLD population and often exhibit distinct clinical and pathological characteristics shaped by metabolic adaptation at early stages of the disease.16 This adaptation is lost with the advancement of the disease, and those with lean MAFLD tend to have a worse outcome compared to their obese counterpart.17 This further emphasises the fundamental role of metabolic health and dysfunction in the disease’s pathogenesis, which extends beyond the definitions of overweight or obesity based on body mass index (BMI).18,19
Stemming from this, a significant paradigm shift has occurred with the redefinition of fatty liver disease as MAFLD, aligning the disease nomenclature and diagnostic criteria with the core underlying pathophysiological mechanisms of metabolic dysfunction that cause the condition.20,21 MAFLD is diagnosed based on hepatic steatosis identified by histology or imaging, accompanied by evidence of metabolic dysfunction indicated by the presence of one or more of the following factors: obesity/overweight, T2DM, or two of the metabolic risk dysregulations.2,22 MAFLD has been shown to more accurately identify patients with significant hepatic fibrosis and extra-hepatic manifestations, including cardiovascular disease risk, compared to other definitions of the disease.23–27
MAFLD and Cardiovascular Disease
A robust reciprocal correlation between MAFLD and CVD has been established through observational, cohort, and genetic studies. Individuals with MAFLD face a markedly increased risk of cardiovascular events, regardless of conventional risk factors.
Epidemiological Evidence
Studies consistently show elevated prevalence of cardiovascular morbidity and mortality in these patients, especially those with advanced fibrosis (F3–F4).28,29 They are more likely to develop conditions such as coronary artery disease, stroke, atrial fibrillation, heart failure, and unfavorable ventricular remodeling, underscoring the strong link between MAFLD severity and cardiovascular outcomes.30,31
A study consisting of 9,775,066 adults revealed that MAFLD, measured by a fatty liver index (FLI) of ≥ 30, was independently linked to a higher risk of new CVD events. These events were defined as a combination of myocardial infarction, ischemic stroke, heart failure, or cardiovascular death, with an adjusted hazard ratio (HR) of 1.39.32 A meta-analysis involving 10 cohort studies showed that the rates of CVD and CVD-related mortality were 2.26 times and 1.57 times greater in the MAFLD group compared to the control group, respectively.33 Similar results were also reported in other meta-analysis, strengthening the relationship between MAFLD and CV events.34–36 Additionally, a longitudinal study of 34,865 participants found that FLI, especially moderate/severe FLI, significantly increased the risk of new-onset hypertension, which is also linked to greater cardiovascular risk.37
Research increasingly focuses on MAFLD impact in older adults, where the relationship to cardiovascular outcomes might differ from younger cohorts. Some studies indicate an increased risk of atrial fibrillation (AF),38–40 but the association with major adverse cardiovascular events or mortality may be less significant after adjusting for age and comorbidities.41 Notably, liver stiffness, independent of steatosis, might be relevant for cardiovascular risk.42 Thus, while MAFLD is common in older adults, its impact requires careful consideration of age-related factors and liver fibrosis.43 Further research is needed to clarify these nuances for targeted management.44
Coronary Artery Disease (CAD)
Patients with MAFLD have approximately double the risk of developing coronary artery disease (CAD) compared to those without MAFLD.45 Previous research has highlighted a strong association between MAFLD and increased CAD risk.46 A 20-year follow-up study (1991–2009) showed that high liver fat content predicted CAD, even when adjusting for factors like age and gender, with an HR of 1.92.47 Furthermore, a cross-sectional study in Iran involving 296 participants found a significantly higher prevalence of CAD in MAFLD patients, with an odds ratio (OR) of 2.01.48 Meta-analysis comprising 32 studies with over 5.6 million participants also confirmed this relationship, noting a relative risk (RR) of 1.21.49
Moreover, recent studies emphasize the link between ischemic heart disease (IHD), a form of CAD, and MAFLD. Data from the NHANES survey (1999–2016) revealed that an increased FLI, indicating hepatic steatosis, correlated with higher IHD prevalence. Specifically, for every standard deviation increase in FLI, the risk of IHD rose by 27%.50 Another study of 2,088 individuals demonstrated that those with mild, moderate, and severe fatty liver had increased risks of developing IHD by 1.88, 2.37, and 2.76 times, respectively.51 A Danish cohort study of 94,708 individuals, including 10,897 with IHD, found that the risk of IHD increased progressively with higher liver fat content across quartiles, reaching an OR of 2.41. Additionally, the OR for IHD in individuals with versus without MAFLD was 1.65.52 However, some studies may have limitations due to inadequate adjustment for potential confounders and cardiovascular risk factors and challenge to establish causal relationships.
Heart Failure
An elevated risk of heart failure and cardiac fibrosis has been associated with MAFLD, particularly in advanced MAFLD, where essential monitoring of similar cardiac fibrosis and failure is required.53 A study included about 175,000 outpatients, both with and without MAFLD, matched for sex, age, index year, and known heart failure risk factors, revealed that MAFLD was significantly linked to a 10-year increased cumulative incidence of heart failure (HR 1.34) in men and women from various age groups.54 A recent meta-analysis of 11 longitudinal cohort studies, which included more than 11 million middle-aged individuals, revealed that MAFLD is linked to a 1.5-fold greater long-term risk of new-onset heart failure, a relationship that remained significant regardless of hypertension, T2DM, and other prevalent cardiometabolic risk factors.55
Evidence from Mendelian Randomization Studies
Mendelian Randomization has emerged as a powerful tool, providing strong evidence for the causal links between metabolic traits, inflammation, MAFLD, and CVD.56 Besides these epidemiological evidence, Mendelian Randomization also established a strong link between MAFLD and CVD. For instance, recent studies demonstrated that genetically predicted MAFLD increased the risk of CVD even after adjusting for established metabolic variables, supporting the notion that MAFLD actively promotes atherogenesis and vascular dysfunction rather than merely being a bystander.57,58
Another comprehensive Mendelian randomization study examining circulating blood metabolites found that specific metabolites, such as branched-chain amino acids, ketone bodies, and lipids, directly influence liver fat accumulation and may also contribute to cardiovascular risk.59
Genetic Factors
Genetic predisposition significantly influences MAFLD and CVD, with key risk variants mainly studied in Europeans.60 The most robust association was demonstrated for the single-nucleotide polymorphism (SNP) rs738409 in Patatin-like phospholipase domain-containing protein (PNPLA3) that is linked to the entire spectrum of the disease including increased liver fat, cirrhosis, and cancer, independent of other factors.61,62 Recent evidence suggests that PNPLA3 variants may be protective against CVD, contrasting with the pathogenic role they play in liver disease, and is characterized by lipid accumulation with specific lipidomic features.63,64
Some other variants in Transmembrane 6 superfamily member 2 (TM6SF2), membrane-bound O-acyltransferases (MBOAT7) and 17β-hydroxysteroid dehydrogenase type 13 (HSD17B13) also has been shown consistently to impact disease progression. For example, TM6SF2 E167K increases MASH and fibrosis risk but may protect against cardiovascular events, highlighting the complex relationship between liver and heart health.65–68 The MBOAT7 rs641738C>T variant is associated with liver fat, inflammation, and fibrosis; it alters phospholipid remodeling and immune responses, worsening liver damage.69–71 HSD17B13 is involved in lipid and retinol metabolism, mainly expressed in periportal hepatocytes, has a truncating variant (rs72613567) that offers protection against liver inflammation, fibrosis, and cirrhosis even in high-risk individuals.72–77 Other loss-of-function variants, like rs62305723, also reduce liver disease risk.75
Others identified polymorphisms include in glucokinase regulatory protein (GCKR) and Sterol Regulatory Element-binding Protein 1 (SREBP-1), both of which are involved in lipid regulation, may also influence CVD risk.78 Recent studies suggest that genetic changes of fibroblast growth factor 21 (FGF21) is a broad metabolic regulator, could be impacting both MAFLD and heart disease risks.79,80 Additionally, signaling of myeloid-epithelial-reproductive tyrosine kinase (MERTK) are regulating core pathway of fibrosis across various organs.81,82 Additionally, genetic evidence linking SNPs associated with BMI, T2D, and inflammation marked by CRP showed an association with MAFLD and cardiovascular risk.56,83
Pathophysiology of Cardiovascular Events in MAFLD
MAFLD and CVD share numerous common risk factors, and the pathophysiological mechanisms connecting the two conditions are intricate and multifaceted, involving various pathways (Figure 1).
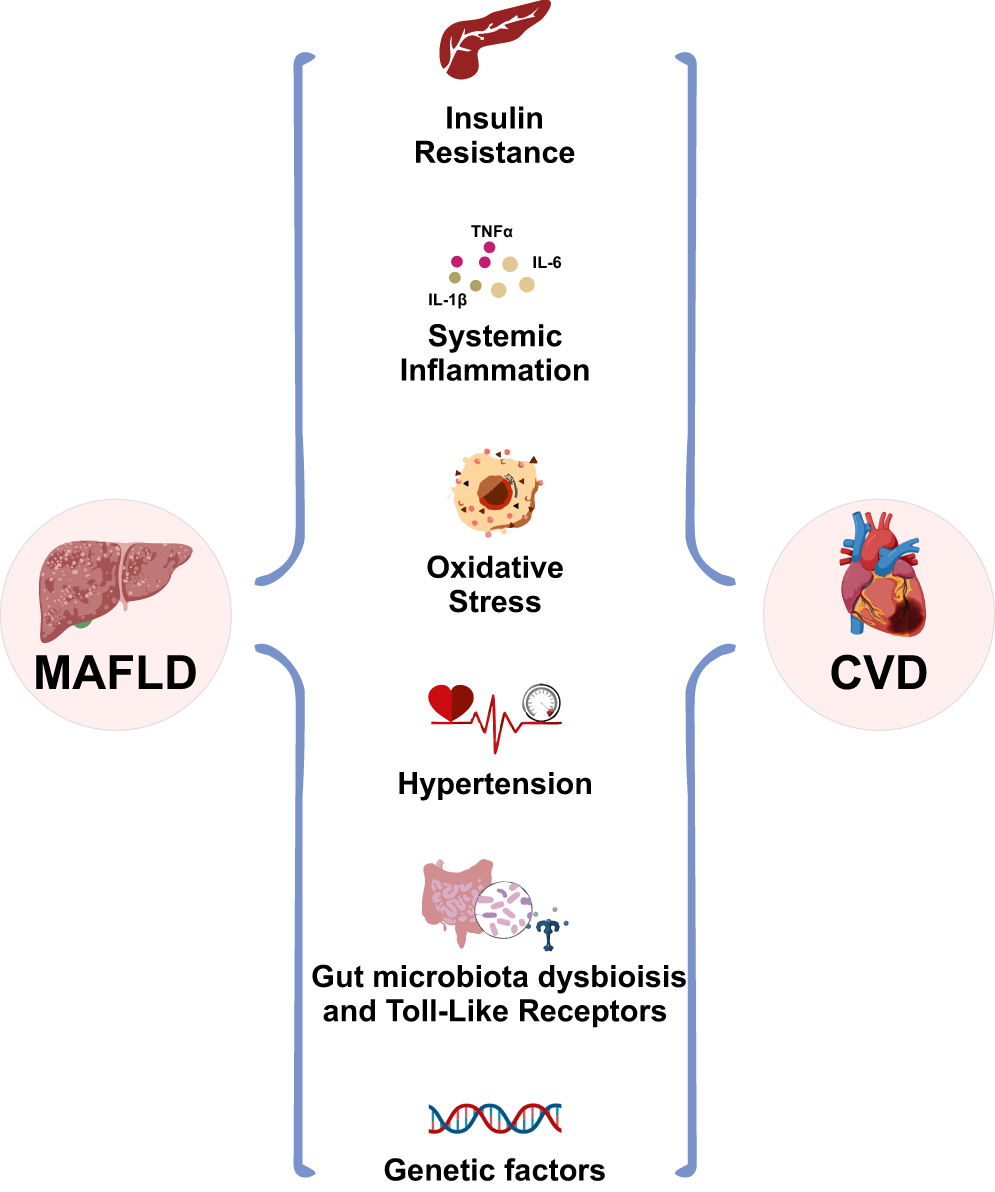 |
Figure 1 Overview of the shared pathophysiological mechanisms between MAFLD and CVD. |
Insulin Resistance
The occurrence of metabolic dysfunction that underpins the risk of MAFLD and cardiovascular events and mediates the link between the two conditions could be broadly attributed to an intertwined interaction between insulin resistance and chronic low-grade inflammation.14
Insulin resistance is a key mechanism connecting MAFLD with cardiovascular risk.84 It disrupts lipid metabolism, leading to increased levels of circulating free fatty acids and the formation of atherogenic lipoprotein profiles. This is characterized by lower levels of high-density lipoprotein cholesterol (HDL-C) and higher triglyceride levels, which can lead to atherosclerosis and increase the risk of cardiovascular complications.85
As a compensatory response to insulin resistance, insulin secretion rises, resulting in hyperinsulinemia. This condition can harm the vascular endothelium by promoting hepatic gluconeogenesis and heightening systemic inflammation.84 Pro-inflammatory cytokines produced due to insulin resistance exacerbate oxidative stress, further contributing to arterial stiffness and hypertension.86 Furthermore, insulin resistance and the lipotoxic milieu produced by MAFLD stimulate the release of pro-coagulant factors, increasing the likelihood of thrombotic events. This significantly elevates the risk of adverse cardiovascular outcomes in patients with MAFLD.13,87
Systemic Inflammation
Systemic inflammation is another crucial pathophysiological pathway linking CVD and MAFLD. Obesity, which occurs in about 80–90% of MAFLD patients, is linked to low-grade systemic inflammation, ER stress dysregulation, or lipotoxicity.88 Excess lipids and the hypertrophy of adipocytes in adipose tissue cause local macrophages to adopt a more inflammatory phenotype, releasing cytokines such as tumor necrosis factor alpha (TNF-α), interleukin-1 beta (IL-1β), and Interleukin-6 (IL-6).89,90 These cytokines disrupt insulin receptor signaling by promoting serine phosphorylation of insulin receptor substrates, which reduces insulin sensitivity and leads to hyperinsulinemia.91 Concurrently, resident Kupffer cells and recently recruited monocyte-derived macrophages in the liver produce pro-inflammatory mediators in response to metabolic stress, which worsens insulin resistance, encourages steatosis, and ultimately leads to fibrosis.91,92 This vicious cycle, where insulin resistance fuels further inflammation and vice versa, also results in endothelial dysfunction and atherosclerotic changes, creating a pathway for cardiovascular events.91
Additionally, MAFLD can frequently exist with viral hepatitis, which may also impact the risk of CVD in these patients.93–96 For instance, Chronic Hepatitis C Virus (HCV) infection can influence lipid profiles and cardiovascular risk, with studies showing increased cholesterol and triglycerides after successful HCV eradication, particularly in genotype 3 patients.97 Furthermore, recognizing that MAFLD can co-exist with other liver conditions, such as alcohol-related liver disease, highlights the potential for synergistic effects that exacerbate inflammation and disease progression, which will increase risk of CVD further.98
Oxidative Stress
Dyslipidemia, characterized by elevated triglycerides, reduced HDL cholesterol, and increased LDL cholesterol (especially small, dense LDL particles), is a hallmark of MAFLD, which increases oxidative stress.99 Oxidative stress is one of the major contributing factors to the emergence of cardiovascular events in patients with MAFLD, which occurs as a result of increased reactive oxygen species (ROS) generation, mitochondrial dysfunction, and impaired antioxidant defence.92,100
The metabolic imbalance in MAFLD causes lipid peroxidation, which damages endothelial cells and increases foam cell production, a critical step in atherosclerosis.101 Furthermore, oxidative stress reduces nitric oxide (NO) bioavailability, which contributes to endothelial dysfunction and arterial stiffness, increasing cardiovascular risk.102,103 Moreover, oxidative stress-induced damage to vascular cells exacerbates the progression of atherosclerotic lesions, thereby increasing the risk of cardiovascular events in this patient population.103
Hypertension
As is well established, insulin resistance and hypertension are intricately linked to various metabolic dysfunctions, playing central roles in the pathogenesis of cardiovascular disease.104,105 Hyperinsulinemia, a hallmark of insulin resistance, promotes renal salt reabsorption, which can lead to volume expansion, vasoconstriction, and consequently, elevated blood pressure.106 In addition, longitudinal cohort studies have demonstrated that obesity elevates cardiovascular risk indirectly through mediating factors such as hypertension, dyslipidemia, specifically hyper-LDL cholesterol and T2D.107,108
These interrelated risk variables not only contribute significantly to the heightened incidence of cardiovascular events in obese populations but also exemplify the complex interplay between metabolic disturbances and cardiovascular health. Recognizing these interconnected pathways underscores the importance of holistic management strategies targeting both metabolic and cardiovascular risk factors to effectively mitigate disease progression and improve long-term outcomes.109
Gut Microbiota Dysbiosis and Toll-Like Receptors
The gut-liver axis is vital in MAFLD development, with gut dysbiosis, barrier dysfunction, and endotoxemia promoting liver inflammation and fat accumulation.110 Imbalances in gut microbiota can increase harmful compounds like trimethylamine N-oxide (TMAO), which is linked to atherosclerosis and cardiovascular risk, while a healthy microbiome produces beneficial metabolites such as short-chain fatty acids that support inflammation regulation and vascular health.111–113
In patients with MAFLD and CVD, notable shifts in microbiota composition—such as increased Copococcus and Veillonella and decreased Parabacteroides, Ruminococcus, Bacteroides, and Bifidobacterium—appear to influence disease severity.114,115 Furthermore, metabolomic studies suggest that MAFLD in CVD patients may worsen clinical outcomes by altering circulating metabolites and microbiota characteristics,116 while changes in fungal microbiota may also impact metabolic regulation.117 Collectively, these findings highlight a potential significant role for the gut–liver–heart axis in the interconnected pathophysiology of MAFLD and its related metabolic disorders and CVD risk.
Toll-Like Receptors (TLRs), a type of membrane-bound pattern recognition receptor, plays a critical role in the pathophysiology of MAFLD. TLR4 is the most widely implicated member of the TLR family, with activation by gut-derived microbial products such as lipopolysaccharides (LPS) triggering hepatic inflammatory cascades and promoting insulin resistance.118 This inflammatory environment increases intestinal permeability, allowing microbial ligands to move further into the portal circulation, prolonging systemic metabolic abnormalities and aggravating liver injury.118,119
Likewise, hepatocyte damage in MAFLD and MASH triggers the release of endogenous TLR9 ligands, which maintains a pro-inflammatory environment.120 Moreover, TLR1, an under-researched member of the TLR family, is involved in MAFLD and suggested as a possible treatment target for early-stage MAFLD.120 TLR1 expression is associated with the degree of hepatic steatosis and inflammation, and its pharmacologic suppression reduced pro-inflammatory cytokine expression.121
Assessment of Cardiovascular Risk in Patients with MAFLD
Given that the primary cause of death for patients with MAFLD is CVD, therefore, accurate risk assessment is crucial for timely interventions.33,122 A multidisciplinary approach that includes non-invasive hepatic and cardiovascular evaluations is essential, as liver and heart dysfunction are closely intertwined.123
Non-invasive screening methods, including Coronary Artery Calcium (CAC) scoring and the Atherosclerotic Cardiovascular Disease (ASCVD) risk calculator, have gained prominence for routine cardiovascular health assessments.33,124 Advanced imaging techniques, such as Two-Dimensional Speckle Tracking Echocardiography (2D-STE) and Three-Dimensional Speckle Tracking Echocardiography (3D-STE), provide valuable insights into cardiac function.124,125
Similar to liver biopsy, which is the gold standard for diagnosing MAFLD, Coronary Computed Tomography Angiography (CCTA) is the preferred method for diagnosing coronary artery disease (CAD). CCTA allows the measurement of epicardial fat volume (EFV) and the assessment of coronary stenosis. Studies have linked increased EFV to a higher risk of major adverse cardiac events (MACE) among MAFLD patients.126–128 Assessing cardiovascular risk in MAFLD requires a comprehensive approach integrating advanced imaging and risk prediction tools to facilitate early intervention and improve patient outcomes.
Clinical Management and Pharmacotherapy
The management of MAFLD patients relies on a multidisciplinary prevention and management approach that aims not only to resolve hepatic inflammation and fibrosis but also to attenuate the cardiovascular risk (Figure 2). The holy grail of management of both conditions remains the lifestyle changes.
 |
Figure 2 Proposed algorithm for the assessment and management of cardiovascular disease risk in patients with MAFLD. |
Lifestyle Modifications
Losing weight by 7–10% has been linked with regression of liver fibrosis and reducing cardiovascular risk in these patients. This can be achieved via calorie restriction, improving the quality of diet and regular exercise, with a role for pharomcotherapy and bariatric surgery in selected indications.129
A Mediterranean diet prioritising fruits, vegetables, whole grains, lean meats, and healthy fats, while minimising processed foods and carbohydrates, has shown strong associations with decreased hepatic steatosis and cardiovascular risk.130
Aerobic exercises with moderate to strenuous activity for 2.5–5 h/ week can reduce liver fat, enhance insulin action, and lower hepatic inflammation. While Resistance Training for a minimum of 2 sessions/ week is reported to augment muscle mass, glucose uptake, and enhance metabolic health. Exercise recommendations should be tailored according to individual fitness levels, comorbidities, and patient preferences.2 Moreover, a combination of aerobic and weight exercise provides a synergistic effect with more recorded exercise maintenance over time.
Mechanistically, frequent exercise enhances free fatty acid flow and substrate metabolism in the liver, muscle, and adipose tissues.129,131,132 This helps to minimize steatosis and improve metabolic balance. It had been shown that exercise could be beneficial, even in the absence of weight loss.2
Pharmacotherapy
Although the Food and Drug Administration (FDA) does not explicitly require all MAFLD drugs to have a positive impact on cardiovascular disease, they do consider cardiovascular risk in the approval process and encourage the development of drugs with potential benefits for both MAFLD and cardiovascular health or at least have no negative effect. Pharmacological interventions can target different pathways related to the pathophysiology of MAFLD and its metabolic comorbidities to enhance liver health and lower the risk of cardiovascular complications.133
Medications
Resmetirom (THR-β Agonist)
Resmetirom (MGL-3196), a selective THR-β agonist, is currently the only approved treatment for MAFLD that was approved in 2024. Its efficacy and safety were confirmed in a Phase 3 trial involving patients with biopsy-confirmed steatohepatitis and fibrosis stages F1-F3, showing significant reductions in liver fat, improvements in non-invasive fibrosis markers, and NASH resolution without increasing fibrosis, more effectively than placebo. Additionally, it lowered LDL-C and triglyceride levels, which are linked to cardiovascular risk.134 Resmetirom was well tolerated, with mild to moderate gastrointestinal symptoms and transient liver enzyme increases being the most common adverse effects.135
It improves hepatic lipid oxidation, promotes mitochondrial biogenesis, and reduces de novo lipogenesis by targeting THR-β in hepatocytes. It also offers broader cardiometabolic benefits by addressing key metabolic issues at the liver level.134
Pioglitazone (PPAR-γ Agonist)
Pioglitazone, a thiazolidinedione, activates PPAR-γ mainly in fat, liver, and muscle, improving insulin sensitivity and promoting fat cell development. PPAR-α, found in liver and muscle, enhances fatty acid breakdown, lowers triglycerides, and has anti-inflammatory effects.136,137 PPAR-δ, expressed throughout the body, regulates fatty acid use and energy expenditure, aiding in glucose absorption and reducing inflammation.136,137 Beyond glucose control, pioglitazone exhibits anti-inflammatory, antifibrotic, and lipid-modulating properties, which help treat liver fat buildup and prevent disease progression, and it has been linked to fewer cardiovascular events.138–140
Studies show pioglitazone improves liver enzymes and metabolic health, especially in prediabetic patients, with histological benefits like reduced liver fat and inflammation.141 However, pioglitazone use is limited by potential side effects such as weight gain and fluid retention, as well as concerns regarding heart failure exacerbation.
New PPAR drugs, such as Lanifibranor and Saroglitazar, show promise in fibrosis reduction and MASH resolution.142,143 Dual PPAR-α/γ agonists promote liver fat breakdown and enhance blood sugar metabolism, addressing key factors in MAFLD development.137,144
Glucagon-Like Peptide-1 Receptor Agonists
GLP-1 RAs have shown promise in treating hepatic necroinflammation, diabetes, and CVD.145 By mimicking GLP-1, these agents increase insulin secretion, reduce glucagon, slow gastric emptying, and promote satiety. They are effective in reducing hepatic steatosis, inflammation, and improving glycaemic control and weight loss in MAFLD.145,146
Studies showed that GLP-1 RAs induce histological improvements in inflammation and fibrosis, along with decreased liver fat and normalized enzymes.145 Semaglutide, used for T2DM and obesity, boosts insulin secretion and reduces appetite, with promising hepatic and cardiovascular benefits.147,148 Liraglutide, initially used for T2DM, reduces hepatic steatosis, inflammation, hepatocyte ballooning, and liver stiffness, showing potential in MAFLD management.149,150
Metformin
Metformin reduces hepatic steatosis and liver enzymes in MAFLD with T2DM by inhibiting hepatic gluconeogenesis through activation of AMP-activated protein kinase (AMPK), a key energy regulator. AMPK activation improves insulin sensitivity, promotes fatty acid oxidation, and decreases liver fat synthesis, while also enhancing mitochondrial function, reducing oxidative stress, and modulating inflammation—key factors in MAFLD progression.151,152 Recent research suggests it may also protect liver cells by decreasing ferroptosis and apoptosis via oxidative stress pathways, potentially halting disease progression at the cellular level.153,154 Additionally, metformin improves endothelial function, reducing cardiovascular risks associated with diabetes.155
Empagliflozin
Empagliflozin, a sodium-glucose cotransporter 2 (SGLT2) inhibitor originally used for managing hyperglycemia in T2DM, has gained attention for its significant cardiometabolic benefits beyond glycemic control.156
Empagliflozin has been used as a targeted therapy for MAFLD for its role in the reduction of hepatic steatosis, fibrosis, and aminotransferase levels via de novo lipogenesis, enhancing fatty acid oxidation, decreasing hepatic inflammation, and oxidative stress.153 Moreover, Empagliflozin has been favored in patients with cardiovascular events for its role in reducing visceral adiposity, improving endothelial function, and its anti-inflammatory effect.157
Statins and Other Lipid-Lowering Drugs
Lipid-lowering medications, especially statins, are well-established treatments due to their cardiovascular benefits and emerging liver-protective effects.158 They effectively treat dyslipidemia in MAFLD patients, with meta-analyses showing improvements in lipid profiles and liver enzymes, particularly in patients without advanced liver disease.159
Besides statins, drugs like ezetimibe, fibrates, and omega-3 fatty acids have also been studied, especially for mixed dyslipidemia.160 Fibrates, such as fenofibrate and pemafibrate, activate PPAR-α, reducing triglycerides, improving hepatic steatosis, and decreasing endoplasmic reticulum stress, which also enhances insulin sensitivity, lowers liver fat, and may reduce fibrosis by altering gene expression, including downregulating Transforming growth factor beta (TGF-β).161,162
Omega-3 fatty acids EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid) are crucial for various health benefits and have been shown to lower liver fat and improve liver enzyme levels in MAFLD patients.163,164
Obeticholic Acid
Obeticholic acid (OCA) is a semi-synthetic derivative of chenodeoxycholic acid that acts as a selective farnesoid X receptor (FXR) agonist, a nuclear receptor highly expressed in the liver and intestines, playing key roles in bile acid, glucose, and fat metabolism. Activation of FXR by OCA reduces hepatic lipogenesis and enhances insulin sensitivity.165 It has shown promise in improving the histological features of MASH and fibrosis, with studies reporting significant improvements in liver fibrosis scores compared to placebo.166 However, potential off-target effects, particularly dyslipidemia, necessitate cardiovascular risk monitoring, especially during long-term therapy.167,168
Additionally, the pipeline for MAFLD treatment comprises various other promising drugs offer additional strategies for fatty liver disease and related metabolic disorders. For instance, Efruxifermin, a long-acting fibroblast growth factor 21 (FGF21) analog showed limited fibrosis reduction in MASH cirrhosis patients in a Phase 2b trial, although some benefits were observed at 96 weeks.169 Dapagliflozin, a SGLT2 inhibitor improved MASH and fibrosis.170
Some drugs combinations or multi-targets ones have also demonstrated promising results. Tirzepatide, a dual glucose-dependent insulinotropic polypeptide (GIP) and GLP-1 receptor agonist significantly reduced weight in obese, type 2 diabetic adults.171 Cotadutide, a dual GLP-1 and glucagon receptor agonist, reduced UACR, suggesting kidney benefits in type 2 diabetes and CKD in a phase 2 study.172 Pemvidutide, a GLP-1/glucagon dual receptor agonist, may address obesity comorbidities.173 These emerging therapies highlight the evolving landscape and potential for more targeted approaches in managing MAFLD and associated cardiovascular risks.
Conclusion
MAFLD is a multisystem disease closely linked to increased cardiovascular risk, driven by metabolic abnormalities such as insulin resistance, inflammation, and dyslipidemia. With it rising prevalence worldwide, early assessment and a multidisciplinary approach that combines risk stratification, non-invasive screening, individualized treatment strategies, comprehensive management, including lifestyle modifications and targeted therapies, is vital to improve patient outcomes and address the interconnected pathways of liver and cardiovascular health.
Funding
ME is supported by a National Health and Medical Research Council of Australia (NHMRC) investigator and ideas grants (AAP2008983 and APP2001692). MLY is supported by the “Center of Excellence for Metabolic Associated Fatty Liver Disease, National Sun Yat-sen University, Kaohsiung” from The Featured Areas Research Centre Program within the framework of the Higher Education Sprout Project by the Ministry of Education (MOE) in Taiwan, and Center for Liquid Biopsy and Cohort Research KMU-TC109B05, Kaohsiung Medical University.
Disclosure
Professor Ming-Lung Yu reports grants from Abbvie, Abbott Diagnostic, BMS, Gilead, Merck, Novo Nordisc and Roche diagnostics, other from Abbvie, Abbott Diagnostic, BMS, Gilead, Novo Nordisc, Roche and Roche diagnostics, other from Abbvie, BMS, Eisai, Gilead, Roche and Roche diagnostics, outside the submitted work. The authors report no other conflicts of interest.
References
1. Habibullah M, Jemmieh K, Ouda A, Haider MZ, Malki MI, Elzouki AN. Metabolic-associated fatty liver disease: a selective review of pathogenesis, diagnostic approaches, and therapeutic strategies. Front Med. 2024;11:1291501. doi:10.3389/fmed.2024.1291501
2. Eslam M, Fan JG, Yu ML, et al. The Asian Pacific association for the study of the liver clinical practice guidelines for the diagnosis and management of metabolic dysfunction-associated fatty liver disease. Hepatol Int. 2025;19:261–301.
3. Guo Z, Wu D, Mao R, Yao Z, Wu Q, Lv W. Global burden of MAFLD, MAFLD related cirrhosis and MASH related liver cancer from 1990 to 2021. Sci Rep. 2025;15:7083. doi:10.1038/s41598-025-91312-5
4. Witkowski M, Moreno SI, Fernandes J, Johansen P, Augusto M, Nair S. The economic burden of non-alcoholic steatohepatitis: a systematic review. Pharmacoeconomics. 2022;40:751–776. doi:10.1007/s40273-022-01140-y
5. Wondmkun YT. Obesity, insulin resistance, and type 2 diabetes: associations and therapeutic implications. Diabetes Metab Syndr Obes. 2020;13:3611–3616. doi:10.2147/DMSO.S275898
6. Boccatonda A, Andreetto L, D’Ardes D, et al. From NAFLD to MAFLD: definition, pathophysiological basis and cardiovascular implications. Biomedicines. 2023;12:11. doi:10.3390/biomedicines12010011
7. Sarin SK, Kumar M, Eslam M, et al. Liver diseases in the Asia-Pacific region: a Lancet Gastroenterology & Hepatology Commission. Lancet Gastroenterol Hepatol. 2020;5:167–228. doi:10.1016/S2468-1253(19)30342-5
8. Pipitone RM, Ciccioli C, Infantino G, et al. MAFLD: a multisystem disease. Ther Adv Endocrinol Metab. 2023;14:20420188221145549. doi:10.1177/20420188221145549
9. Pan Z, Derbala M, AlNaamani K, Ghazinian H, Fan JG, Eslam M. MAFLD criteria are better than MASLD criteria at predicting the risk of chronic kidney disease. Ann Hepatol. 2024;29:101512. doi:10.1016/j.aohep.2024.101512
10. Gaziano TA, Bitton A, Anand S, Abrahams-Gessel S, Murphy A. Growing epidemic of coronary heart disease in low- and middle-income countries. Curr Probl Cardiol. 2010;35:72–115. doi:10.1016/j.cpcardiol.2009.10.002
11. Joseph P, Lanas F, Roth G, et al. Cardiovascular disease in the Americas: the epidemiology of cardiovascular disease and its risk factors. Lancet Reg Health Am. 2025;42:100960. doi:10.1016/j.lana.2024.100960
12. Hassen G, Singh A, Belete G, et al. Nonalcoholic fatty liver disease: an emerging modern-day risk factor for cardiovascular disease. Cureus. 2022;14:e25495.
13. Roberts CK, Hevener AL, Barnard RJ. Metabolic syndrome and insulin resistance: underlying causes and modification by exercise training. Compr Physiol. 2013;3:1–58. doi:10.1002/j.2040-4603.2013.tb00484.x
14. Puschel GP, Klauder J, Henkel J. Macrophages, low-grade inflammation, insulin resistance and hyperinsulinemia: a mutual ambiguous relationship in the development of metabolic diseases. J Clin Med. 2022;12:11. doi:10.3390/jcm12010011
15. Ramirez-Mejia MM, Qi X, Abenavoli L, Romero-Gomez M, Eslam M, Mendez-Sanchez N. Metabolic dysfunction: the silenced connection with fatty liver disease. Ann Hepatol. 2023;28:101138. doi:10.1016/j.aohep.2023.101138
16. Alharthi J, Pan Z, Gloss BS, et al. Loss of metabolic adaptation in lean MAFLD is driven by endotoxemia leading to epigenetic reprogramming. Metabolism. 2023;144:155583. doi:10.1016/j.metabol.2023.155583
17. Alarabi M, Pan Z, Romero-Gómez M, George J, Eslam M. Telomere length and mortality in lean MAFLD: the other face of metabolic adaptation. Hepatol Int. 2024;18:1448–1458. doi:10.1007/s12072-024-10701-6
18. Pan Z, Khatry MA, Yu ML, et al. MAFLD: an ideal framework for understanding disease phenotype in individuals of normal weight. Ther Adv Endocrinol Metab. 2024;15:20420188241252543. doi:10.1177/20420188241252543
19. Eslam M, El-Serag HB, Francque S, et al. Metabolic (dysfunction)-associated fatty liver disease in individuals of normal weight. Nat Rev Gastroenterol Hepatol. 2022;19:638–651. doi:10.1038/s41575-022-00635-5
20. Tang SY, Tan JS, Pang XZ, Lee GH. Metabolic dysfunction associated fatty liver disease: the new nomenclature and its impact. World J Gastroenterol. 2023;29:549–560. doi:10.3748/wjg.v29.i3.549
21. Eslam M, Ahmed A, Despres JP, et al. Incorporating fatty liver disease in multidisciplinary care and novel clinical trial designs for patients with metabolic diseases. Lancet Gastroenterol Hepatol. 2021;6:743–753. doi:10.1016/S2468-1253(21)00132-1
22. Eslam M, Newsome PN, Sarin SK, et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol. 2020;73:202–209. doi:10.1016/j.jhep.2020.03.039
23. Yamamura S, Eslam M, Kawaguchi T, et al. MAFLD identifies patients with significant hepatic fibrosis better than NAFLD. Liver Int. 2020;40:3018–3030. doi:10.1111/liv.14675
24. Pan Z, Al-Busafi SA, Abdulla M, Fouad Y, Sebastiani G, Eslam M. MAFLD identifies patients with significant hepatic fibrosis better than MASLD. Hepatol Int. 2024;18:964–972. doi:10.1007/s12072-024-10673-7
25. Pan Z, Shiha G, Esmat G, Méndez-Sánchez N, Eslam M. MAFLD predicts cardiovascular disease risk better than MASLD. Liver Int. 2024;44:1567–1574. doi:10.1111/liv.15931
26. Kim H, Lee CJ, Ahn SH, et al. MAFLD predicts the risk of cardiovascular disease better than NAFLD in asymptomatic subjects with health check-ups. Dig Dis Sci. 2022;67:4919–4928. doi:10.1007/s10620-022-07508-6
27. Jiang M, Butt AS, Cua IH, et al. MAFLD vs. MASLD: a year in review. Expert Rev Endocrinol Metab. 2025;1–12.
28. Gheorghe L, Nemteanu R, Clim A, Botnariu GE, Costache II, Plesa A. Risk scores for prediction of major cardiovascular events in non-alcoholic fatty liver disease: a no man’s land? Life. 2023;14:13. doi:10.3390/life14010013
29. Ismaiel A, Dumitrascu DL. Cardiovascular risk in fatty liver disease: the liver-heart axis-literature review. Front Med Lausanne. 2019;6:202. doi:10.3389/fmed.2019.00202
30. Lonardo A, Nascimbeni F, Mantovani A, Targher G. Hypertension, diabetes, atherosclerosis and NASH: cause or consequence? J Hepatol. 2018;68:335–352. doi:10.1016/j.jhep.2017.09.021
31. Soderberg C, Stal P, Askling J, et al. Decreased survival of subjects with elevated liver function tests during a 28-year follow-up. Hepatology. 2010;51:595–602. doi:10.1002/hep.23314
32. Lee HH, Lee HA, Kim EJ, et al. Metabolic dysfunction-associated steatotic liver disease and risk of cardiovascular disease. Gut. 2024;73:533–540. doi:10.1136/gutjnl-2023-331003
33. Wen W, Li H, Wang C, et al. Metabolic dysfunction-associated fatty liver disease and cardiovascular disease: a meta-analysis. Front Endocrinol. 2022;13:934225. doi:10.3389/fendo.2022.934225
34. Mahfood Haddad T, Hamdeh S, Kanmanthareddy A, Alla VM. Nonalcoholic fatty liver disease and the risk of clinical cardiovascular events: a systematic review and meta-analysis. Diabetes Metab Syndr. 2017;11(Suppl 1):S209–S216. doi:10.1016/j.dsx.2016.12.033
35. Targher G, Byrne CD, Lonardo A, Zoppini G, Barbui C. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: a meta-analysis. J Hepatol. 2016;65:589–600. doi:10.1016/j.jhep.2016.05.013
36. Toh JZK, Pan XH, Tay PWL, et al. A meta-analysis on the global prevalence, risk factors and screening of coronary heart disease in nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol. 2022;20:2462–2473e2410. doi:10.1016/j.cgh.2021.09.021
37. Shih CI, Wu KT, Hsieh MH, et al. Severity of fatty liver is highly correlated with the risk of hypertension and diabetes: a cross-sectional and longitudinal cohort study. Hepatol Internat. 2023;18:138–154. doi:10.1007/s12072-023-10576-z
38. Clayton-Chubb D, Roberts SK, Majeed A, et al. Associations between MASLD, atrial fibrillation, cardiovascular events, mortality and aspirin use in older adults. Geroscience. 2025;47:1303–1318. doi:10.1007/s11357-024-01435-2
39. Karajamaki AJ, Hukkanen J, Ukkola O. The association of non-alcoholic fatty liver disease and atrial fibrillation: a review. Ann Med. 2018;50:371–380. doi:10.1080/07853890.2018.1492147
40. Chen Z, Liu J, Zhou F, et al. Nonalcoholic fatty liver disease: an emerging driver of cardiac arrhythmia. Circ Res. 2021;128:1747–1765. doi:10.1161/CIRCRESAHA.121.319059
41. Clayton-Chubb D, Majeed A, Commins I, et al. Prevalence and outcomes of steatotic liver disease subtypes in older adults. Hepatol Commun. 2025;9.
42. van Kleef LA, Lu Z, Ikram MA, de Groot NMS, Kavousi M, de Knegt RJ. Liver stiffness not fatty liver disease is associated with atrial fibrillation: the Rotterdam study. J Hepatol. 2022;77:931–938. doi:10.1016/j.jhep.2022.05.030
43. Clayton-Chubb D, Kemp WW, Majeed A, et al. Steatotic liver disease in older adults: clinical implications and unmet needs. Nutrients. 2025;17.
44. van Kleef LA, Sonneveld MJ, Kavousi M, Ikram MA, de Man RA, de Knegt RJ. Fatty liver disease is not associated with increased mortality in the elderly: a prospective cohort study. Hepatology. 2023;77:585–593. doi:10.1002/hep.32635
45. Huang XJ, Yin M, Zhou BQ, Tan XY, Xia YQ, Qin CX. Impact renaming non-alcoholic fatty liver disease to metabolic associated fatty liver disease in prevalence, characteristics and risk factors. World J Hepatol. 2023;15:985–1000. doi:10.4254/wjh.v15.i8.985
46. Arslan U, Yenercag M. Relationship between non-alcoholic fatty liver disease and coronary heart disease. World J Clin Cases. 2020;8:4688–4699. doi:10.12998/wjcc.v8.i20.4688
47. Pisto P, Santaniemi M, Bloigu R, Ukkola O, Kesaniemi YA. Fatty liver predicts the risk for cardiovascular events in middle-aged population: a population-based cohort study. BMJ Open. 2014;4:e004973. doi:10.1136/bmjopen-2014-004973
48. Gholoobi A, Gifani M, Gholoobi A, Akhlaghi S, Rad MP, Rahimi VB. Relationship between the prevalence and severity of non-alcoholic fatty liver disease and coronary artery disease: findings from a cross-sectional study of a referral center in northeast Iran. Jgh Open. 2022;6:330–337. doi:10.1002/jgh3.12746
49. Abosheaishaa H, Hussein M, Ghallab M, et al. Association between non-alcoholic fatty liver disease and coronary artery disease outcomes: a systematic review and meta-analysis. Diab Met Synd Clin R. 2024;18.
50. Niu Y, Wang G, Feng X, Niu H, Shi W. Significance of fatty liver index to detect prevalent ischemic heart disease: evidence from national health and nutrition examination survey 1999–2016. Front Cardiovasc Med. 2023;10:1171754. doi:10.3389/fcvm.2023.1171754
51. Lin YC, Lo HM, Chen JD. Sonographic fatty liver, overweight and ischemic heart disease. World J Gastroenterol. 2005;11:4838–4842. doi:10.3748/wjg.v11.i31.4838
52. Lauridsen BK, Stender S, Kristensen TS, et al. Liver fat content, non-alcoholic fatty liver disease, and ischaemic heart disease: mendelian randomization and meta-analysis of 279 013 individuals. Eur Heart J. 2018;39:385–393. doi:10.1093/eurheartj/ehx662
53. Inciardi RM, Mantovani A, Targher G. Non-alcoholic fatty liver disease as an emerging risk factor for heart failure. Curr Heart Fail Rep. 2023;20:308–319. doi:10.1007/s11897-023-00613-1
54. Roderburg C, Krieg S, Krieg A, et al. Non-Alcoholic Fatty Liver Disease (NAFLD) and risk of new-onset heart failure: a retrospective analysis of 173,966 patients. Clin Res Cardiol. 2023;112:1446–1453. doi:10.1007/s00392-023-02250-z
55. Mantovani A, Petracca G, Csermely A, et al. Non-alcoholic fatty liver disease and risk of new-onset heart failure: an updated meta-analysis of about 11 million individuals. Gut. 2023;72:372–380. doi:10.1136/gutjnl-2022-327672
56. Wang X, Zhao D, Cheng L, Gao J, Li J, Geng C. Mendelian randomization explores the causal relationships between obesity, diabetes, inflammation and nonalcoholic fatty liver disease. Medicine. 2023;102:e34638. doi:10.1097/MD.0000000000034638
57. Moon JH, Kim W, Koo BK, Cho NH. Innovative target exploration of Nc. Metabolic dysfunction-associated fatty liver disease predicts long-term mortality and cardiovascular disease. Gut Liver. 2022;16:433–442. doi:10.5009/gnl210167
58. Peng H, Wang S, Wang M, et al. Nonalcoholic fatty liver disease and cardiovascular diseases: a Mendelian randomization study. Metabolism. 2022;133:155220. doi:10.1016/j.metabol.2022.155220
59. Guo Z, Zhang T, Yun Z, et al. Assessing the causal relationships between human blood metabolites and the risk of NAFLD: a comprehensive mendelian randomization study. Front Genet. 2023;14:1108086. doi:10.3389/fgene.2023.1108086
60. Pan Z, Alqahtani SA, Al-Busafi SA, et al. Underrepresentation of Arabs in functional genetics studies: opportunities and obstacles for advancing biology and human health. Liver Int. 2025;45:e70088. doi:10.1111/liv.70088
61. Cherubini A, Casirati E, Tomasi M, Valenti L. PNPLA3 as a therapeutic target for fatty liver disease: the evidence to date. Expert Opin Ther Targets. 2021;25:1033–1043. doi:10.1080/14728222.2021.2018418
62. Shen JH, Li YL, Li D, Wang NN, Jing L, Huang YH. The rs738409 (I148M) variant of the PNPLA3 gene and cirrhosis: a meta-analysis. J Lipid Res. 2015;56:167–175. doi:10.1194/jlr.M048777
63. Yki-Jarvinen H, Luukkonen PK. Function of PNPLA3 I148M-lessons from in vivo studies in humans. Liver Int. 2025;45:e70047. doi:10.1111/liv.70047
64. Toffoli B, Comar C, Grillo A, et al. PNPLA3 polymorphism is inversely correlated with aortic stiffness in patients with metabolic dysfunction-associated steatotic liver disease without fibrosis. Int J Mol Sci. 2025;26.
65. Alharthi J, Bayoumi A, Thabet K, et al. A metabolic associated fatty liver disease risk variant in MBOAT7 regulates toll like receptor induced outcomes. Nat Commun. 2022;13:7430. doi:10.1038/s41467-022-35158-9
66. Huang G, Wallace DF, Powell EE, Rahman T, Clark PJ, Subramaniam VN. Gene variants implicated in steatotic liver disease: opportunities for diagnostics and therapeutics. Biomedicines. 2023;12:11.
67. Eslam M, Mangia A, Berg T, et al. Diverse impacts of the rs58542926 E167K variant in TM6SF2 on viral and metabolic liver disease phenotypes. Hepatology. 2016;64:34–46. doi:10.1002/hep.28475
68. Dongiovanni P, Petta S, Maglio C, et al. Transmembrane 6 superfamily member 2 gene variant disentangles nonalcoholic steatohepatitis from cardiovascular disease. Hepatology. 2015;61:506–514. doi:10.1002/hep.27490
69. Meroni M, Longo M, Fracanzani AL, Dongiovanni P. MBOAT7 down-regulation by genetic and environmental factors predisposes to MAFLD. EBioMedicine. 2020;57:102866. doi:10.1016/j.ebiom.2020.102866
70. Teo K, Abeysekera KWM, Adams L, et al. rs641738C>T near MBOAT7 is associated with liver fat, ALT and fibrosis in NAFLD: a meta-analysis. J Hepatol. 2021;74:20–30. doi:10.1016/j.jhep.2020.08.027
71. Pan Z, Alharthi J, Bayoumi A, George J, Eslam M. A cell specific effect of MBOAT7 MAFLD-risk variant on immune cells. Front Biosci. 2024;29:148. doi:10.31083/j.fbl2904148
72. Iakovleva V, de Jong YP. Gene-based therapies for steatotic liver disease. Mol Ther. 2025;33:2527–2547. doi:10.1016/j.ymthe.2025.04.024
73. Wang P, Wu CX, Li Y, Shen N. HSD17B13 rs72613567 protects against liver diseases and histological progression of nonalcoholic fatty liver disease: a systematic review and meta-analysis. Eur Rev Med Pharmacol Sci. 2020;24:8997–9007. doi:10.26355/eurrev_202009_22842
74. Abul-Husn NS, Cheng X, Li AH, et al. A protein-truncating variant and protection from chronic liver disease. New Engl J Med. 2018;378:1096–1106. doi:10.1056/NEJMoa1712191
75. Ma YL, Belyaeva OV, Brown PM, et al. 17-beta hydroxysteroid dehydrogenase 13 is a hepatic retinol dehydrogenase associated with histological features of nonalcoholic fatty liver disease. Hepatology. 2019;69:1504–1519. doi:10.1002/hep.30350
76. Su W, Wang Y, Jia X, et al. Comparative proteomic study reveals 17β-HSD13 as a pathogenic protein in nonalcoholic fatty liver disease. Proc Natl Acad Sci U S A. 2014;111:11437–11442. doi:10.1073/pnas.1410741111
77. Tang S, Zhang J, Mei TT, Zhang WY, Zheng SJ, Yu HB. Association of HSD17B13 rs72613567: TA allelic variant with liver disease: review and meta-analysis. BMC Gastroenterol. 2021;21:490. doi:10.1186/s12876-021-02067-y
78. Jonas W, Schurmann A. Genetic and epigenetic factors determining NAFLD risk. Mol Metab. 2021;50:101111. doi:10.1016/j.molmet.2020.101111
79. Tan H, Yue T, Chen Z, Wu W, Xu S, Weng J. Targeting FGF21 in cardiovascular and metabolic diseases: from mechanism to medicine. Int J Biol Sci. 2023;19:66–88. doi:10.7150/ijbs.73936
80. Bayoumi A, Elsayed A, Han S, et al. Mistranslation drives alterations in protein levels and the effects of a synonymous variant at the fibroblast growth factor 21 locus. Adv Sci. 2021;8:2004168. doi:10.1002/advs.202004168
81. DeBerge M, Yeap XY, Dehn S, et al. MerTK cleavage on resident cardiac macrophages compromises repair after myocardial ischemia reperfusion injury. Circ Res. 2017;121:930–940. doi:10.1161/CIRCRESAHA.117.311327
82. Pan Z, El Sharkway R, Bayoumi A, et al. Inhibition of MERTK reduces organ fibrosis in mouse models of fibrotic disease. Sci Transl Med. 2024;16:eadj0133. doi:10.1126/scitranslmed.adj0133
83. Chew NWS, Chong B, Ng CH, et al. The genetic interactions between non-alcoholic fatty liver disease and cardiovascular diseases. Front Genet. 2022;13:971484. doi:10.3389/fgene.2022.971484
84. Nogueira JP, Cusi K. Role of insulin resistance in the development of nonalcoholic fatty liver disease in people with type 2 diabetes: from bench to patient care. Diabetes Spectr. 2024;37:20–28. doi:10.2337/dsi23-0013
85. Guria S, Hoory A, Das S, Chattopadhyay D, Mukherjee S. Adipose tissue macrophages and their role in obesity-associated insulin resistance: an overview of the complex dynamics at play. Biosci Rep. 2023;43.
86. Oguntibeju OO. Type 2 diabetes mellitus, oxidative stress and inflammation: examining the links. Int J Physiol Pathophysiol Pharmacol. 2019;11:45–63.
87. Zatterale F, Longo M, Naderi J, et al. Chronic adipose tissue inflammation linking obesity to insulin resistance and type 2 diabetes. Front Physiol. 2019;10:1607. doi:10.3389/fphys.2019.01607
88. Hotamisligil GS. Inflammation, metaflammation and immunometabolic disorders. Nature. 2017;542:177–185. doi:10.1038/nature21363
89. Kawai T, Autieri MV, Scalia R. Adipose tissue inflammation and metabolic dysfunction in obesity. Am J Physiol Cell Physiol. 2021;320:C375–C391. doi:10.1152/ajpcell.00379.2020
90. Alharthi J, Latchoumanin O, George J, Eslam M. Macrophages in metabolic associated fatty liver disease. World J Gastroenterol. 2020;26:1861–1878. doi:10.3748/wjg.v26.i16.1861
91. Sood S, Mittal N, Singh TG, Devi S. Pathogenesis of obesity-associated cardiovascular diseases: key role of biomolecules. Health Sci Rev. 2023;7:100098. doi:10.1016/j.hsr.2023.100098
92. Arroyave-Ospina JC, Wu Z, Geng Y, Moshage H. Role of oxidative stress in the pathogenesis of non-alcoholic fatty liver disease: implications for prevention and therapy. Antioxidants. 2021;11:10. doi:10.3390/antiox11010010
93. HCVC PO. Global prevalence and genotype distribution of hepatitis C virus infection in 2015: a modelling study. Lancet Gastroenterol Hepatol. 2017;2:161–176. doi:10.1016/S2468-1253(16)30181-9
94. Attia D, Abdel Alem S, El-Akel W, et al. Prevalence and clinical characteristics of patients with metabolic dysfunction-associated fatty liver disease with hepatitis C virus infection-a population-based study. Aliment Pharmacol Ther. 2022;56:1581–1590. doi:10.1111/apt.17233
95. Eslam M, Kawaguchi T, Del Campo JA, Sata M, Khattab MA, Romero-Gomez M. Use of HOMA-IR in hepatitis C. J Viral Hepat. 2011;18:675–684. doi:10.1111/j.1365-2893.2011.01474.x
96. Khattab MA, Eslam M, Alavian SM. Hepatitis C virus as a multifaceted disease: a simple and updated approach for extrahepatic manifestations of Hepatitis C virus infection. Hepat Mon. 2010;10:258–269.
97. Liu CJ, Seto WK, Yu ML. Dual-etiology MAFLD: the interactions between viral hepatitis B, viral hepatitis C, alcohol, and MAFLD. Hepatol Internat. 2024;18:897–908. doi:10.1007/s12072-024-10699-x
98. Shadi Z, Amedeo L, Jian-Gao F, et al. Dual etiology vs. MetALD: how MAFLD and MASLD address liver diseases coexistence. Metabo Target Organ Damage. 2025;5:15.
99. Deprince A, Haas JT, Staels B. Dysregulated lipid metabolism links NAFLD to cardiovascular disease. Mol Metab. 2020;42:101092. doi:10.1016/j.molmet.2020.101092
100. Irshad I, Alqahtani SA, Ikejima K, Yu ML, Romero-Gomez M, Eslam M. Energy metabolism: an emerging therapeutic frontier in liver fibrosis. Ann Hepatol. 2025;30:101896. doi:10.1016/j.aohep.2025.101896
101. Monserrat-Mesquida M, Quetglas-Llabres M, Abbate M, et al. Oxidative stress and pro-inflammatory status in patients with non-alcoholic fatty liver disease. Antioxidants. 2020;10:9. doi:10.3390/antiox10010009
102. Ionescu VA, Gheorghe G, Bacalbasa N, Diaconu CC. Metabolic dysfunction-associated steatotic liver disease: pathogenetic links to cardiovascular risk. Biomolecules. 2025;15.
103. Minetti ET, Hamburg NM, Matsui R. Drivers of cardiovascular disease in metabolic dysfunction-associated steatotic liver disease: the threats of oxidative stress. Front Cardiovasc Med. 2024;11:1469492. doi:10.3389/fcvm.2024.1469492
104. Zhao X, An X, Yang C, Sun W, Ji H, Lian F. The crucial role and mechanism of insulin resistance in metabolic disease. Front Endocrinol. 2023;14:1149239. doi:10.3389/fendo.2023.1149239
105. Jia G, Sowers JR. Hypertension in diabetes: an update of basic mechanisms and clinical disease. Hypertension. 2021;78:1197–1205. doi:10.1161/HYPERTENSIONAHA.121.17981
106. Soleimani M. Insulin resistance and hypertension: new insights. Kidney Int. 2015;87:497–499. doi:10.1038/ki.2014.392
107. Shih CI, Wu KT, Hsieh MH, et al. Severity of fatty liver is highly correlated with the risk of hypertension and diabetes: a cross-sectional and longitudinal cohort study. Hepatol Int. 2024;18:138–154.
108. Welsh A, Hammad M, Pina IL, Kulinski J. Obesity and cardiovascular health. Eur J Prev Cardiol. 2024;31:1026–1035. doi:10.1093/eurjpc/zwae025
109. Al-Shoaibi AAA, Li Y, Song Z, et al. Associations of overweight and obesity with the risk of cardiovascular disease according to metabolic risk factors among middle-aged Japanese workers: the Aichi Workers’ cohort study. Obes Res Clin Pract. 2024;18:101–108. doi:10.1016/j.orcp.2024.02.006
110. Ni Y, Ni L, Zhuge F, Fu Z. The gut microbiota and its metabolites, novel targets for treating and preventing non-alcoholic fatty liver disease. Mol Nutr Food Res. 2020;64:e2000375. doi:10.1002/mnfr.202000375
111. Heianza Y, Ma W, Manson JE, Rexrode KM, Qi L. Gut microbiota metabolites and risk of major adverse cardiovascular disease events and death: a systematic review and meta-analysis of prospective studies. J Am Heart Assoc. 2017;6.
112. Nesci A, Carnuccio C, Ruggieri V, et al. Gut microbiota and cardiovascular disease: evidence on the metabolic and inflammatory background of a complex relationship. Int J Mol Sci. 2023;25:24. doi:10.3390/ijms25010024
113. Mostafavi Abdolmaleky H, Zhou JR. Gut microbiota dysbiosis, oxidative stress, inflammation, and epigenetic alterations in metabolic diseases. Antioxidants. 2024;14:13. doi:10.3390/antiox14010013
114. Fadieienko G, Gridnyev O, Kurinna O, Chereliuk N. Gut microbiota changes in nonalcoholic fatty liver disease and concomitant coronary artery disease. Cor Vasa. 2023;65:489–495. doi:10.33678/cor.2022.126
115. Zhang Y, Xu J, Wang X, Ren X, Liu Y. Changes of intestinal bacterial microbiota in coronary heart disease complicated with nonalcoholic fatty liver disease. BMC Genomics. 2019;20:862. doi:10.1186/s12864-019-6251-7
116. Hu X, Zhou R, Li H, et al. Alterations of gut microbiome and serum metabolome in coronary artery disease patients complicated with non-alcoholic fatty liver disease are associated with adverse cardiovascular outcomes. Front Cardiovasc Med. 2021;8:805812. doi:10.3389/fcvm.2021.805812
117. Xu J, Zhang Y, Wang X, Ren X, Liu Y. Changes and roles of intestinal fungal microbiota in coronary heart disease complicated with nonalcoholic fatty liver disease. Am J Transl Res. 2020;12:3445–3460.
118. Fan Y, Li Y, Chu Y, Liu J, Cui L, Zhang D. Toll-like receptors recognize intestinal microbes in liver cirrhosis. Front Immunol. 2021;12:608498. doi:10.3389/fimmu.2021.608498
119. Khanmohammadi S, Kuchay MS. Toll-like receptors and metabolic (dysfunction)-associated fatty liver disease. Pharmacol Res. 2022;185:106507. doi:10.1016/j.phrs.2022.106507
120. Baumann A, Nier A, Hernandez-Arriaga A, et al. Toll-like receptor 1 as a possible target in non-alcoholic fatty liver disease. Sci Rep. 2021;11:17815. doi:10.1038/s41598-021-97346-9
121. Shepard CR. TLR9 in MAFLD and NASH: at the intersection of inflammation and metabolism. Front Endocrinol. 2020;11:613639. doi:10.3389/fendo.2020.613639
122. Choudhary NS, Duseja A. Screening of cardiovascular disease in nonalcoholic fatty liver disease: whom and how? J Clin Exp Hepatol. 2019;9:506–514. doi:10.1016/j.jceh.2019.02.005
123. Beer S, Babel J, Martin N, Blank V, Wiegand J, Karlas T. Non-invasive assessment of steatohepatitis indicates increased risk of coronary artery disease. PLoS One. 2023;18:e0286882.
124. Castera L, Friedrich-Rust M, Loomba R. Noninvasive assessment of liver disease in patients with nonalcoholic fatty liver disease. Gastroenterology. 2019;156:1264–1281e1264.
125. Moharram MA, Lamberts RR, Whalley G, Williams MJA, Coffey S. Myocardial tissue characterisation using echocardiographic deformation imaging. Cardiovasc Ultrasound. 2019;17:27. doi:10.1186/s12947-019-0176-9
126. Nishihara T, Miyoshi T, Nakashima M, et al. Prognostic value of metabolic dysfunction-associated steatotic liver disease over coronary computed tomography angiography findings: comparison with no-alcoholic fatty liver disease. Cardiovasc Diabetol. 2024;23:167.
127. Orzan RI, Gligor RI, Agoston R, et al. Metabolic dysfunction associated liver disease in patients undergoing coronary computed tomography angiography. J Cardiovasc Dev Dis. 2024;12:11. doi:10.3390/jcdd12010011
128. Munnur RK, Cameron JD, Ko BS, Meredith IT, Wong DT. Cardiac CT: atherosclerosis to acute coronary syndrome. Cardiovasc Diagn Ther. 2014;4:430–448. doi:10.3978/j.issn.2223-3652.2014.11.03
129. Mellemkjaer A, Kjaer MB, Haldrup D, Gronbaek H, Thomsen KL. Management of cardiovascular risk in patients with metabolic dysfunction-associated steatotic liver disease. Eur J Intern Med. 2024;122:28–34.
130. Widmer RJ, Flammer AJ, Lerman LO, Lerman A. The Mediterranean diet, its components, and cardiovascular disease. Am J Med. 2015;128:229–238. doi:10.1016/j.amjmed.2014.10.014
131. Muscogiuri G, Verde L, Sulu C, et al. Mediterranean diet and obesity-related disorders: what is the evidence? Curr Obes Rep. 2022;11:287–304. doi:10.1007/s13679-022-00481-1
132. Keating SE, Chawla Y, De A, George ES. Lifestyle intervention for metabolic dysfunction-associated fatty liver disease: a 24-h integrated behavior perspective. Hepatol Int. 2024;18:959–976. doi:10.1007/s12072-024-10663-9
133. Stefan N, Haring HU, Cusi K. Non-alcoholic fatty liver disease: causes, diagnosis, cardiometabolic consequences, and treatment strategies. Lancet Diabetes Endocrinol. 2019;7:313–324.
134. Harrison SA, Taub R, Neff GW, et al. Resmetirom for nonalcoholic fatty liver disease: a randomized, double-blind, placebo-controlled phase 3 trial. Nat Med. 2023;29:2919–2928. doi:10.1038/s41591-023-02603-1
135. Chen VL, Morgan TR, Rotman Y, et al. Resmetirom therapy for metabolic dysfunction-associated steatotic liver disease: October 2024 updates to AASLD Practice Guidance. Hepatology. 2025;81:312–320. doi:10.1097/HEP.0000000000001112
136. Mabrouk Gabr N, Fouda A. Role of Thiazolidinediones (TZDs) and Glucagon-Like Peptide-1 (GLP-1) agonists and antagonosts in type-II diabetes mellitus on adult male albino rats. Al-Azhar Med J. 2018;47:475–492. doi:10.12816/0052811
137. Guru B, Tamrakar AK, Manjula SN, Prashantha Kumar BR. Novel dual PPARalpha/gamma agonists protect against liver steatosis and improve insulin sensitivity while avoiding side effects. Eur J Pharmacol. 2022;935:175322. doi:10.1016/j.ejphar.2022.175322
138. Basak S, Murmu A, Matore BW, Roy PP, Singh J. Thiazolidinedione an auspicious Scaffold as PPAR-γ agonist: its possible mechanism to Manoeuvre against insulin resistant diabetes mellitus. Eur J Med Chem Rep. 2024;100160. doi:10.1016/j.ejmcr.2024.100160
139. Czaja MJ. Pioglitazone: more than just an insulin sensitizer. Hepatology. 2009;49:1427–1430. doi:10.1002/hep.22983
140. Attaran F, Emami S, Sohrabi M, et al. Effect of Empagliflozin and Pioglitazone on left ventricular function in patients with type two diabetes and nonalcoholic fatty liver disease without established cardiovascular disease: a randomized single-blind clinical trial. BMC Gastroenterol. 2023;23:327. doi:10.1186/s12876-023-02948-4
141. Kamolvisit S, Chirnaksorn S, Nimitphong H, Sungkanuparph S. Pioglitazone for the treatment of metabolic-associated fatty liver disease in people living with HIV and prediabetes. Cureus. 2021;13:e19046. doi:10.7759/cureus.19046
142. Barb D, Kalavalapalli S, Godinez Leiva E, et al. Pan-PPAR agonist lanifibranor improves insulin resistance and hepatic steatosis in patients with T2D and MASLD. J Hepatol. 2025;82:979–991. doi:10.1016/j.jhep.2024.12.045
143. Joshi SR. Saroglitazar for the treatment of dyslipidemia in diabetic patients. Expert Opin Pharmacother. 2015;16:597–606. doi:10.1517/14656566.2015.1009894
144. Miao L, Xu J, Targher G, Byrne CD, Zheng MH. Old and new classes of glucose-lowering agents as treatments for non-alcoholic fatty liver disease: a narrative review. Clin Mol Hepatol. 2022;28:725–738. doi:10.3350/cmh.2022.0015
145. Westermeier F, Fisman EZ. Glucagon like peptide-1 (GLP-1) agonists and cardiometabolic protection: historical development and future challenges. Cardiovasc Diabetol. 2025;24:44. doi:10.1186/s12933-025-02608-9
146. Nevola R, Epifani R, Imbriani S, et al. GLP-1 receptor agonists in non-alcoholic fatty liver disease: current evidence and future perspectives. Int J Mol Sci. 2023;25:24.
147. Bea S, Jeong HE, Filion KB, et al. Outcomes of SGLT-2i and GLP-1RA therapy among patients with type 2 diabetes and varying NAFLD status. JAMA Network Open. 2023;6:e2349856. doi:10.1001/jamanetworkopen.2023.49856
148. Cersosimo A, Salerno N, Sabatino J, et al. Underlying mechanisms and cardioprotective effects of SGLT2i and GLP-1Ra: insights from cardiovascular magnetic resonance. Cardiovasc Diabetol. 2024;23:94. doi:10.1186/s12933-024-02181-7
149. Guss DA, Mohanty SR. Liraglutide’s use in treatment of non-alcoholic fatty liver: an evaluation of the non-alcoholic steatohepatitis study. Hepatobiliary Surg Nutr. 2016;5:515–518. doi:10.21037/hbsn.2016.11.09
150. Song T, Jia Y, Li Z, Wang F, Ren L, Chen S. Effects of liraglutide on nonalcoholic fatty liver disease in patients with type 2 diabetes mellitus: a systematic review and meta-analysis. Diabetes Ther. 2021;12:1735–1749. doi:10.1007/s13300-021-01072-4
151. Zachou M, Flevari P, Nasiri-Ansari N, et al. The role of anti-diabetic drugs in NAFLD. Have we found the Holy Grail? A narrative review. Eur J Clin Pharmacol. 2024;80:127–150. doi:10.1007/s00228-023-03586-1
152. Pinyopornpanish K, Leerapun A, Pinyopornpanish K, Chattipakorn N. Effects of metformin on hepatic steatosis in adults with nonalcoholic fatty liver disease and diabetes: insights from the cellular to patient levels. Gut Liver. 2021;15:827–840. doi:10.5009/gnl20367
153. Scheen AJ. Comparative effects between old and new antidiabetic agents on metabolic-associated fatty liver disease (MAFLD). Diab Epidemiol Manag. 2023;11:100145. doi:10.1016/j.deman.2023.100145
154. Li Z, Cui C, Xu L, Ding M, Wang Y. Metformin suppresses metabolic dysfunction-associated fatty liver disease by ferroptosis and apoptosis via activation of oxidative stress. Free Radic Res. 2024;58:686–701. doi:10.1080/10715762.2024.2417279
155. Quinn CE, Hamilton PK, Lockhart CJ, McVeigh GE. Thiazolidinediones: effects on insulin resistance and the cardiovascular system. Br J Pharmacol. 2008;153:636–645. doi:10.1038/sj.bjp.0707452
156. Cheung KS, Ng HY, Hui RWH, et al. Effects of empagliflozin on liver fat in patients with metabolic dysfunction-associated steatotic liver disease without diabetes mellitus: a randomized, double-blind, placebo-controlled trial. Hepatology. 2024;80:916–927. doi:10.1097/HEP.0000000000000855
157. Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, Cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373:2117–2128. doi:10.1056/NEJMoa1504720
158. da Silva Pereira ENG, Franco RLC, Santos R, Daliry A. Statins and non-alcoholic fatty liver disease: a concise review. Biomed Pharmacother. 2025;183:117805. doi:10.1016/j.biopha.2024.117805
159. Abdallah M, Brown L, Provenza J, Tariq R, Gowda S, Singal AK. Safety and efficacy of dyslipidemia treatment in NAFLD patients: a meta-analysis of randomized controlled trials. Ann Hepatol. 2022;27:100738. doi:10.1016/j.aohep.2022.100738
160. Tziomalos K. Lipid-lowering agents in the management of nonalcoholic fatty liver disease. World J Hepatol. 2014;6:738–744. doi:10.4254/wjh.v6.i10.738
161. Katsuyama H, Yanai H, Adachi H, Hakoshima M. A significant effect of pemafibrate on hepatic steatosis and fibrosis indexes in patients with hypertriglyceridemia. Gastroenterol Res. 2023;16:240–243. doi:10.14740/gr1656
162. Zhang D, Niu S, Ma Y, et al. Fenofibrate improves insulin resistance and hepatic steatosis and regulates the Let-7/SERCA2b axis in high-fat diet-induced non-alcoholic fatty liver disease mice. Front Pharmacol. 2021;12:770652. doi:10.3389/fphar.2021.770652
163. Parker HM, Johnson NA, Burdon CA, et al. Omega-3 supplementation and non-alcoholic fatty liver disease: a systematic review and meta-analysis. J Hepatol. 2012;56:944–951. doi:10.1016/j.jhep.2011.08.018
164. Lee CH, Fu Y, Yang SJ, Chi CC. Effects of Omega-3 polyunsaturated fatty acid supplementation on non-alcoholic fatty liver: a systematic review and meta-analysis. Nutrients. 2020;13:12. doi:10.3390/nu13010012
165. Makri E, Cholongitas E, Tziomalos K. Emerging role of obeticholic acid in the management of nonalcoholic fatty liver disease. World J Gastroenterol. 2016;22:9039–9043. doi:10.3748/wjg.v22.i41.9039
166. Zhao J, Li B, Zhang K, Zhu Z. The effect and safety of obeticholic acid for patients with nonalcoholic steatohepatitis: a systematic review and meta-analysis of randomized controlled trials. Medicine (Baltimore). 2024;103:e37271. doi:10.1097/MD.0000000000037271
167. Abenavoli L, Falalyeyeva T, Boccuto L, Tsyryuk O, Kobyliak N. Obeticholic acid: a new era in the treatment of nonalcoholic fatty liver disease. Pharmaceuticals. 2018;11:11. doi:10.3390/ph11010011
168. Eslam M, Alvani R, Shiha G. Obeticholic acid: towards first approval for NASH. Lancet. 2019;394:2131–2133. doi:10.1016/S0140-6736(19)32963-0
169. Noureddin M, Rinella ME, Chalasani NP, et al. Efruxifermin in compensated liver cirrhosis caused by MASH. N Engl J Med. 2025;392:2413–2424. doi:10.1056/NEJMoa2502242
170. Lin J, Huang Y, Xu B, et al. Effect of dapagliflozin on metabolic dysfunction-associated steatohepatitis: multicentre, double blind, randomised, placebo controlled trial. BMJ. 2025;389:e083735. doi:10.1136/bmj-2024-083735
171. Garvey WT, Frias JP, Jastreboff AM, et al. Tirzepatide once weekly for the treatment of obesity in people with type 2 diabetes (SURMOUNT-2): a double-blind, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet. 2023;402:613–626. doi:10.1016/S0140-6736(23)01200-X
172. Selvarajah V, Robertson D, Hansen L, et al. A randomized phase 2b trial examined the effects of the glucagon-like peptide-1 and glucagon receptor agonist cotadutide on kidney outcomes in patients with diabetic kidney disease. Kidney Int. 2024;106:1170–1180. doi:10.1016/j.kint.2024.08.023
173. Anderson SL. Review: special Issue: real-world evidence on the use of GLP1 receptor agonists: emerging concepts in obesity management: focus on glucagon receptor agonist combinations. Drugs Context. 2025;14.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.