Back to Journals » Clinical Optometry » Volume 18
Macular, Foveal and RNFL Thickness Patterns in Amblyopia: A Comparative Study
Authors Majumder C, Mohd Khialdin S, Mukhopadhyay S, Omar R ![]()
Received 5 August 2025
Accepted for publication 9 January 2026
Published 20 February 2026 Volume 2026:18 558412
DOI https://doi.org/10.2147/OPTO.S558412
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Chris Lievens
Chiranjib Majumder,1 Safinaz Mohd Khialdin,2 Subrata Mukhopadhyay,3 Rokiah Omar1
1Optometry & Vision Science Programme, Fakulti Sains Keshihatan, Universiti Kebangsaan Malaysia, Kuala Lumpur, 50300, Malaysia; 2Department of Ophthalmology, Faculty of Medicine, Universiti Kebangsaan Malaysia, Cheras, 56000, Malaysia; 3Shankar Bhaban Netralaya, Rupnarayanpur, Asansol, WB, 713386, India
Correspondence: Rokiah Omar, Email [email protected]
Purpose: The purpose of this study is to compare the macular thickness, foveal thickness, and retinal nerve fiber layer (RNFL) thickness in amblyopic eyes with those of fellow non-amblyopic eyes using spectral-domain optical coherence tomography (OCT).
Methods: A cross-sectional, observational study was conducted with amblyopic subjects from August 2022 to December 2024. A pilot study was carried out using simple random sampling technique. The study involved OCT-based measurement of macular, foveal, and RNFL thickness in amblyopic and non-amblyopic eyes using standardized imaging protocols. Data were analysed using appropriate statistical tests (paired and independent t-tests) based on normality results to compare values across eye types and gender.
Results: The results showed significantly higher macular, foveal, and RNFL thickness in amblyopic eyes compared to non-amblyopic eyes (p < 0.05), with no significant differences between anisometropic and mixed amblyopia subtypes. Gender had no significant effect on retinal thickness, except for superior RNFL thickness, which was higher in the anisometropic group of non-amblyopic eyes.
Conclusion: This study confirms that amblyopia involves both functional and structural retinal changes, notably in the macula and RNFL, regardless of type or gender. OCT proves valuable in detecting these changes, and future studies should focus on axial length correction and post-treatment outcomes.
Keywords: refractive amblyopia, mixed amblyopia, optical coherence tomography, macular thickness, foveal thickness and RNFL thickness
Introduction
Amblyopia, or “lazy eye,” is one of the most common causes of preventable visual impairment in children, with significant long-term effects on quality of life, school performance, and vision. If diagnosed in a timely manner, amblyopia is in large part preventable and frequently treatable with proper therapy.1,2 Amblyopia is clinically characterized by a reduction in best-corrected visual acuity (BCVA) in one eye or both eyes as a consequence of pathological visual development in the absence of underlying organic ocular disease detected by physical examination. It is most often caused by abnormal binocular interaction or form-deprivation within the critical period of visual development.1,2 The American Academy of Ophthalmology says that amblyopia is diagnosed when there is an interocular difference in two or more lines of visual acuity on a logMAR chart, or when visual acuity in one eye is worse than or equal to 20/30 with or without optimal refractive correction.3
Amblyopia can be categorized as mild, moderate, or severe, depending on the degree of BCVA loss.4 Of all the diagnostic criteria, a BCVA of ≤20/40 or an interocular difference of ≥2 lines has the highest detection rate of amblyopia, with an estimated prevalence of approximately 2.5%.5 The global prevalence of amblyopia varies between 1.44% and 1.75%, with a big meta-analysis that included more than 4.6 million children estimating a global prevalence of 1.36%. Of particular note is the fact that the condition is very slightly more common in males (1.40%) than in females (1.24%), the highest geographical rate being seen in Europe (2.66%) and the lowest in Africa (0.38%).6 The prevalence in Asia is 1.16%. Alarmingly, the estimated number of affected people worldwide is set to rise from 99.2 million in 2019 to 221.9 million in 2040.5 Indian reports have indicated wide-ranging prevalence rates, such as a very high rate of 9.1% in rural Telangana and 2.5% in Bhopal.7,8
Amblyopia develops as a result of interference with normal visual stimulation of the cortical visual pathways during the critical period of neurodevelopment, extending from birth to about 7–8 years of age.9 Cortical visual areas are very plastic and sensitive to input from both eyes during this time. Any disruption, like strabismus (misalignment of eyes), uncorrected high refractive errors, cataracts, or ptosis, can interfere with cortical development, creating amblyopia.9 Visual information coming from the retina and processed along the visual pathway can become deformed through such interruption, producing maladaptive cortical modifications. These are corroborated by neurophysiological findings, revealing smaller cortical oscillatory responses and less activity within both the extrastriate and striate cortices among amblyopic individuals, with a different level of connectivity between dorsal and ventral visual pathway streams.10,11
Amblyopia is etiologically divided into a number of different types, such as refractive amblyopia (anisometropia or isometropia), strabismic amblyopia, mixed mechanism amblyopia, stimulus deprivation amblyopia (congenital cataract or ptosis), and occlusion amblyopia (over patching the dominant eye).12 Several risk factors for the development of amblyopia have been identified, such as premature birth, low birth weight, neurodevelopmental delay, family history of amblyopia, bronchopulmonary dysplasia, and delayed referrals for ocular assessment.13–15 Children with conditions like infantile esotropia are especially susceptible to developing amblyopia, though cross-fixation may provide some protection.16
Stereopsis impairment in amblyopia primarily results from suppression of the amblyopic eye rather than reduced visual acuity alone. Hence, treatments targeting both suppression reduction and acuity improvement are vital.17–19 While traditional management follows sequential optical correction and occlusion therapy, combined and alternative approaches—such as pharmacological penalization, Bangerter filters, perceptual learning, dichoptic and active vision therapy—have shown comparable or superior outcomes.20 Notably, optical correction alone can resolve up to one-third of cases, and engaging activities during patching enhance results.21 Integrated therapy combining occlusion, correction, and vision training yields improvements in acuity, contrast sensitivity, and binocularity.22–24
The structural retinal alterations of amblyopia are still a matter of debate. Although some research has indicated that there are no relevant differences in macular thickness, foveal thickness, or retinal nerve fiber layer thickness between amblyopic and non-amblyopic eyes, increased values in these parameters in amblyopic eyes have been detected by other studies.25–31 Differences in types of amblyopia, patient ages, degrees of severity, and duration, or else in imaging devices and analysis methods may be the reason for these divergent findings. In addition, there is evidence that amblyopia can affect postnatal retinal development, which can result in retinal ganglion cell loss and secondary macular thickening.32 Axial length has a negative correlation with the RNFL thickness. Studies showed the importance of considering Axial length compensation for retinal various parameter thickness measurements.33–35
Although some studies have reported structural retinal alterations following amblyopia treatment, including decreased macular and foveal thickness, results are inconsistent, particularly for RNFL thickness.31 In addition, most data available are related to anisometropic amblyopia, with few comparative data on strabismic amblyopia. To our knowledge, no such extensive study has assessed macular, foveal, and RNFL thickness changes in refractive and strabismic amblyopia prior to treatment, especially in relation to various retinal parameters. This study thus seeks to fill this gap by investigating structural retinal alterations in strabismic and refractive amblyopia through the application of optical coherence tomography (OCT) as a quantitative measure. Knowledge of these changes could enhance therapeutic decision-making and provide new insight into the reversibility and neural plasticity of amblyopia.
Methodology
A cross-sectional observational study was conducted with amblyopic subjects from August 2022 to December 2024. A complete list of all eligible subjects diagnosed with amblyopia (as per inclusion criteria) was prepared and assigned unique identification numbers. Random numbers corresponding to the number of required participants were generated using the Research Randomizer software. This software uses a computerized algorithm to produce random sequences, ensuring true randomness without human interference. The random numbers generated were matched with the assigned identification numbers on the list. Subjects whose numbers corresponded to the generated random numbers were selected for inclusion in the study. No healthy control subjects are included for the comparison of the retinal parameters with amblyopic eyes. The comparison was done with the fellow non-amblyopic eyes. Sample size determined by using G*Power 3.1.9.4 software version. The Alpha error in the present study was 0.05 and the effect size was medium. The Power of the study was taken as 80%. The Total required Sample size was 34. Inclusion criteria were Refractive amblyopia (Refractive anisometropia: amblyopia with presence of anisometropia of ≥0.50D spherical equivalent or ≥1.50Dof difference in astigmatism in any meridian, without any measurable heterotropia at distance or near fixation, which remained after at least 4 weeks of spectacle correction), Mixed amblyopia: Refractive amblyopia in the presence of either a heterotropia at distance and or near fixation or a history of strabismus surgery (or botulinum), A corrected visual acuity difference of ≥ 2 lines between the eyes, Visual acuity of the sound eye 20/40 or better, age group of 6–18 years and those are willing to follow-up, and Any type of refractive error less than +10 D or −15D. But exclusion criteria were any eye pathology (Corneal pathology, lenticular pathology, retinal pathology etc), Nystagmus, development retardation, Systemic and Neurological pathology, Mild amblyopia, History of previous other ocular surgery, spectacle wear, occlusion therapy or vision therapy, Subjects not cooperative enough for OCT, and Pupillary diameter ≤ 2.5mm.
Data Collection
In the beginning, approval from the ethical committee and permission from the hospital were obtained before conducting the study. The declaration of the Helsinki had been followed as human subjects are involved in the study. Screening test will involve thorough Optometric standard examination in the history of the persons and then visual acuity assessment, stereopsis assessment, extraocular motility test, pupillary assessment, objective and subjective refraction test, slit-lamp test, and fundus examination. Following detailed evaluation only those who met the inclusion criteria were enrolled into the study. Baseline readings for macular, foveal, and RNFL thickness were taken through Spectral domain Optical Coherence Tomography (SD-OCT) during the first visit. OCT scans were conducted with a spectral domain optical coherence tomography (SD OCT) scanner (Topcon 3D OCT-1 Maestro 2, Tokyo, Japan) by the same person through dilated pupils of minimum 5 mm diameter. Fast RNFL Thickness Map protocol within the Topcon Maestro2 OCT system is a fast, non-contact scan technique aimed to measure the Retinal Nerve Fiber Layer (RNFL) surrounding the optic nerve head. Originally developed for early detection and monitoring of glaucoma and other optic neuropathies, this protocol utilizes a high-speed, high-resolution spectral-domain OCT (SD-OCT) scan. It takes a 3.4 mm diameter circle scan centered exactly on the optic disc with infrared (IR) fundus image guidance. The scan measures RNFL thickness by determining the distance between the internal limiting membrane (ILM) and the outer edge of the RNFL. The resulting information are divided into various sectors such as temporal, superior, nasal, and inferior quadrants, 12 clock-hour segments, and a global average. The protocol provides a TSNIT (Temporal-Superior-Nasal-Inferior-Temporal) curve, a color-coded RNFL thickness map, and a deviation map comparing patient data to a pre-installed age-matched normative database. Color codes represent the RNFL thickness status: normal as green, borderline as yellow, and outside normal limits as red. The superior and inferior and average RNFL thickness were recorded for the research study. To reduce bias in RNFL measurements in OCT scans for research, there is a need to standardize imaging protocols, whereby scan settings, alignment, and timing are maintained consistently across all subjects. Media opacities like cataract has been omitted, since these can impair signal strength and lead to measurement inaccuracy. Only scans with good signal strength (>6/10) were included in the study and repeat scans done wherever necessary. Axial length, particularly in high myopia, can have a substantial effect on RNFL thickness through image magnification; hence ocular biometry done and adjusted for using algorithms or controlled for statistically. Adequate scan alignment centered on the optic disc is essential to prevent artifacts, and all segmentation borders checked and adjusted whenever needed. Macular Thickness Map protocol with six radial scan lines centered on the fovea, each with a 6 mm transverse length. For optimal image quality, adjusting an optimization setting were controlled, and scans only accepted if signal strength (SS) is >6 (ideally 9–10). Foveal decentrations [ie, with standard deviation of center point thickness >10%] scans will be remeasured. With the use of auto-alignment and auto-shot capabilities, Maestro2 guarantees precise centration and image quality. The output also consists of a thickness map according to the ETDRS grid (Early Treatment Diabetic Retinopathy Study), which splits the macular region into nine zones: a central 1 mm circle, an inner ring (3 mm) divided into four quadrants (superior, nasal, inferior, temporal), and an outer ring (6 mm) with the same subdivision. The protocol tests the important parameters of central macular thickness (CMT), total macular volume, and average retinal thickness. The average macular thickness and foveal thickness are major results of the macular thickness map protocol in OCT. Foveal thickness, also described as central macular thickness (CMT), is the retinal thickness in the central 1 mm region of the ETDRS grid and anatomically equates to the fovea. This measurement is taken from the internal limiting membrane (ILM) to the retinal pigment epithelium (RPE). The mean macular thickness is determined by averaging all nine ETDRS sectors, both the central and peripheral macular areas within the scan. The Operator related bias had been minimized, and all images are subject to strict quality control by the single researcher. All data necessary was uploaded to the excel spreadsheet for further processing. The data collection flow chart is shown in Figure 1.
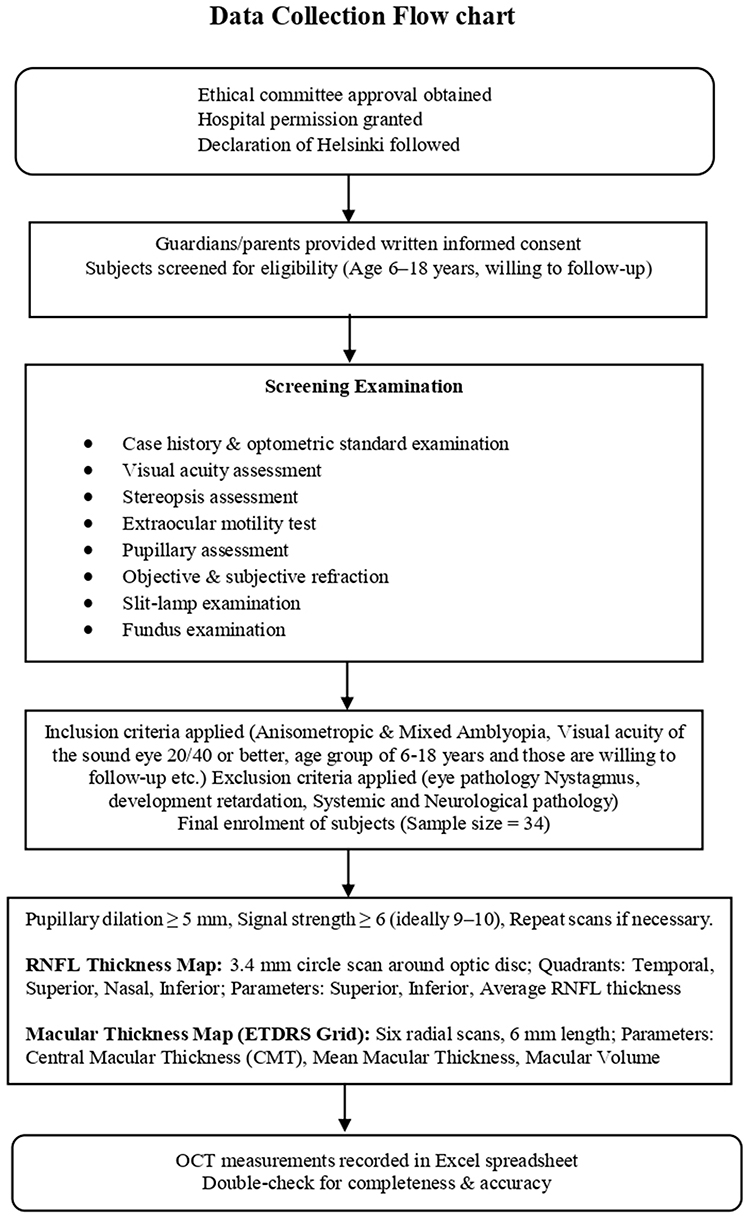 |
Figure 1 Data collection procedure. |
Statistical analysis was carried out by utilizing IBM SPSS Statistics 25.0. Normality test was performed using Shapiro–wilk Test. According to the result of normality test, parametric tests were applied. Foveal, Macular, and RNFL thickness in amblyopic eye and non-amblyopic fellow eye of the same subject was compared using paired T-test. Comparison of foveal, Macular, and RNFL thickness between gender for amblyopic eye and non- amblyopic fellow eye was carried out using Independent T-test. Similarly, Comparison of foveal, Macular, and RNFL thickness between anisometropic and mixed amblyopia in amblyopic and non-amblyopic fellow eyes were evaluated by using Independent T-test. Correlation of visual acuity with average macular thickness, foveal thickness and average RNFL thickness was done by using Pearson’s correlation.
Results
Normality of the data was assessed with Shapiro–Wilk tests and all data showed normal distribution. The demographic details are shown in Table 1.
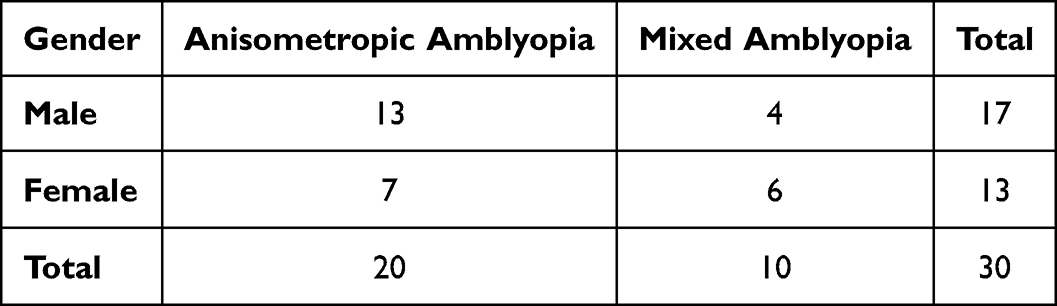 |
Table 1 Demographic Distribution of the Study Subjects |
In 30 subjects, amblyopic eyes demonstrated significantly higher mean macular thickness (M = 270.93 ± 13.35 µm) compared with non-amblyopic fellow eyes (M = 262.60 ± 15.80 µm), t(29) = 7.86, p < 0.05. Foveal thickness was also larger in amblyopic eyes (M = 242.83 ± 26.53 µm vs 230.83 ± 17.27 µm), t(29) = 2.89, p = 0.007. Correspondingly, mean RNFL thickness (M = 102.07 ± 12.33 µm) and superior RNFL thickness (M = 124.13 ± 25.20 µm) were found to be significantly higher in amblyopic eyes than non-amblyopic fellow eyes (M = 94.73 ± 14.63 µm and 115.83 ± 22.48 µm, respectively), p <0.05. A non-significant difference was seen for inferior RNFL thickness (p =0.07) as shown in Table 2.
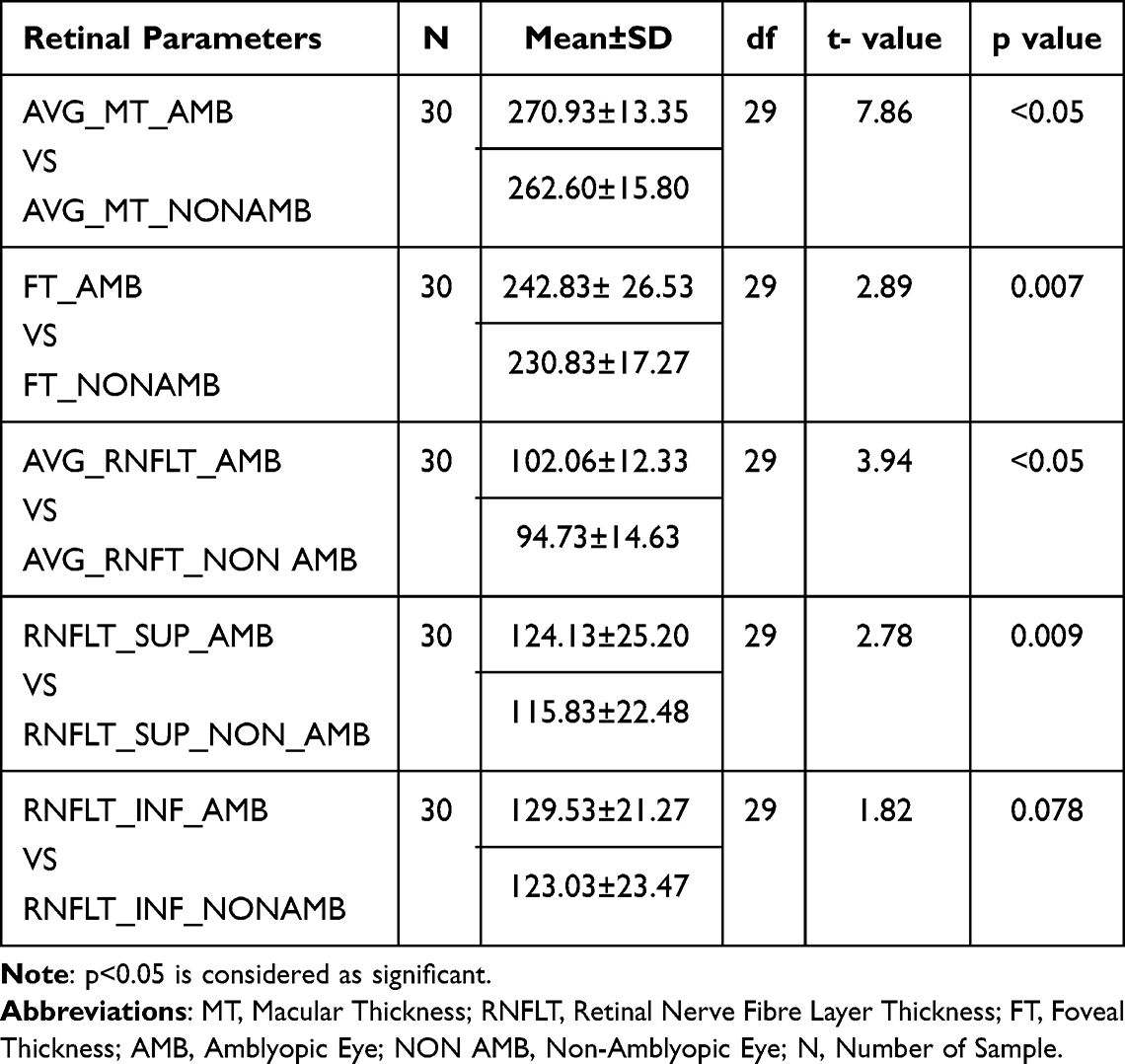 |
Table 2 Comparative Analysis of Foveal, Macular, and RNFL Thickness Between Amblyopic and Fellow Non-Amblyopic Eyes |
A comparison of retinal parameters was made between anisometropic and mixed amblyopia for amblyopic and fellow non-amblyopic eyes. The mean macular thickness in anisometropic amblyopic eyes was 271.42 ± 13.27 µm, whereas in fellow non-amblyopic eyes it was 263.66 ± 15.60 µm. This was not statistically significant (z = −0.13, p =0.89). Likewise, in the mixed amblyopia group, the mean macular thickness was 269.95 ± 14.19 µm in amblyopic eyes and 260.50 ± 16.83 µm in fellow non-amblyopic eyes. Foveal thickness was higher in the anisometropic amblyopic eyes (M = 237.20, SD = 29.12 µm) than in their fellow non-amblyopic eyes (M = 228.35, SD = 18.08 µm), though the difference was near but not quite at statistical significance (z = −1.76, p =0.07). In the mixed group, Foveal thickness measurements were 254.10 ± 16.34 µm in amblyopic eyes and 235.80 ± 15.17 µm in fellow non-amblyopic eyes. The mean retinal nerve fiber layer thickness was also greater in anisometropic amblyopic eyes (M = 104.15, SD = 13.48 µm) compared with fellow non-amblyopic eyes (M = 97.75, SD = 14.94 µm), but the difference was not significant (z = −1.29, p =0.19). For the mixed amblyopia group, the mean RNFL thickness was 97.90 ± 8.81 µm in amblyopic eyes and 88.70 ± 12.56 µm in fellow non-amblyopic eyes. The mean superior RNFL thickness was greater 129.70 ± 20.99 µm in anisometropic amblyopic eyes compare to 121.55 ± 19.55 µm in fellow non-amblyopic eyes (z = −1.38, p =0.16). For the mixed group, RNFL thickness superiorly was 113.00 ± 30.17 µm in amblyopic eyes and 104.40 ± 24.56 µm in fellow non-amblyopic eyes eyes. Thinner inferior RNFL thickness was 133.15 ± 23.59 µm in anisometropic amblyopic eyes and 127.65 ± 23.80 µm in fellow non-amblyopic eyes (z = −1.52, p =0.12). In the mixed group, RNFL thickness inferiorly was 122.30 ± 13.99 µm in amblyopic eyes. Overall, while amblyopic eyes showed consistently thicker retinal parameters than fellow non-amblyopic eyes in both types of amblyopia, none of these differences were statistically significant as shown in Table 3.
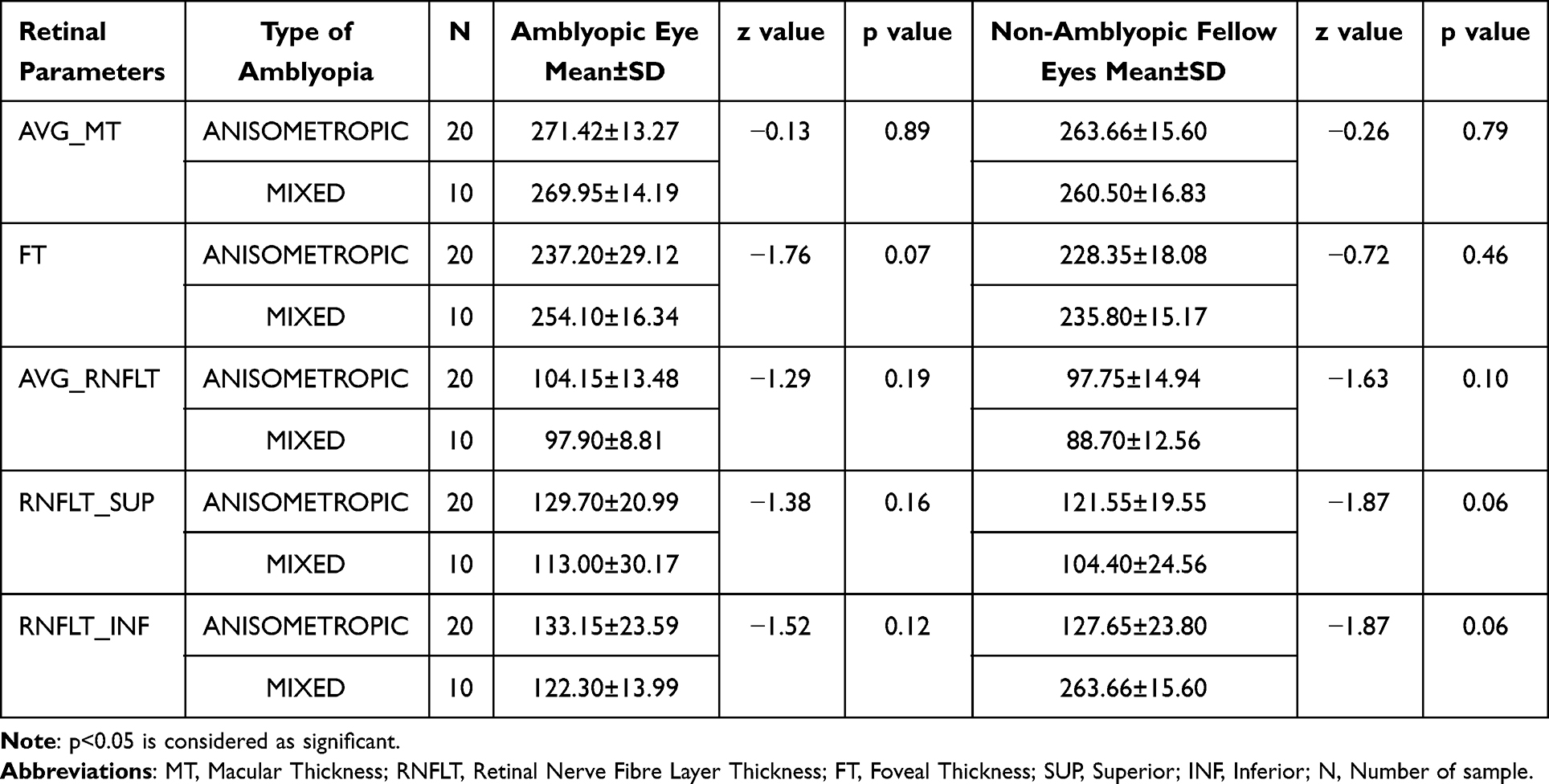 |
Table 3 Comparative Analysis of Foveal, Macular, and RNFL Thickness Between Anisometropic and Mixed Amblyopia in Amblyopic and Fellow Non-Amblyopic Eyes |
A gender-based comparison of retinal parameters between amblyopic eyes and fellow non-amblyopic eyes with and without amblyopia found no statistically significant differences within either group. In males (n = 18), amblyopic eyes had ever so slightly higher mean values on all parameters—mean macular thickness, foveal thickness, mean RNFL thickness, RNFL thickness superiorly, and RNFL thickness inferiorly—than fellow non-amblyopic eyes, but none of those differences were significant (p >0.05 for all). In like manner, in females (n = 12), amblyopic eyes repeatedly had higher mean values than fellow non-amblyopic eyes, but statistical analysis in this subgroup was not available. Overall, the data imply no significant gender-based difference in retinal structural parameters related to amblyopia as shown in Table 4.
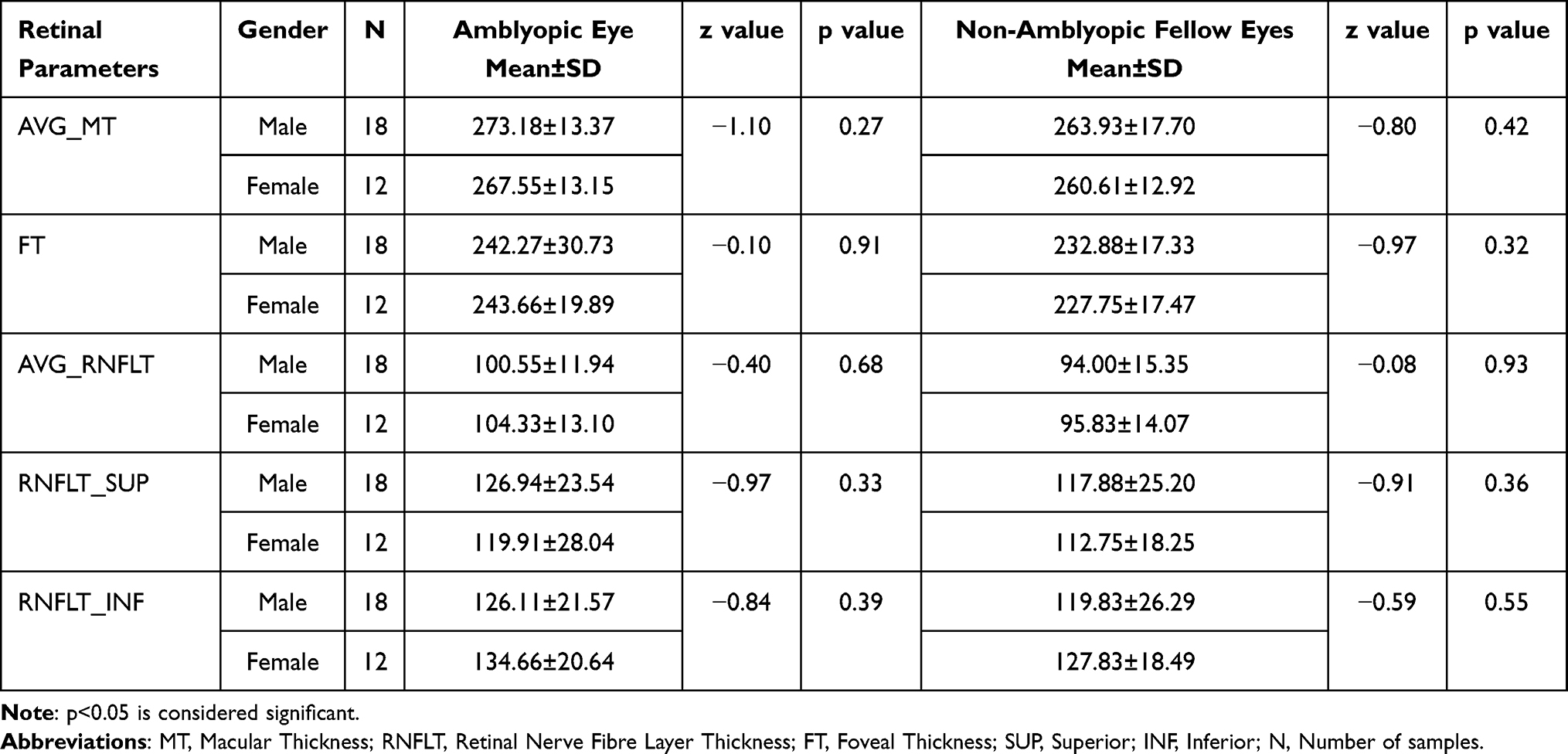 |
Table 4 Comparative Analysis of Foveal, Macular, and RNFL Thickness Between Genders in Amblyopic and Fellow Non-Amblyopic Eyes |
The study evaluated 30 amblyopic eyes and found that visual acuity showed weak correlations with various retinal structural parameters. Average macular thickness and RNFL thickness both showed weak negative correlations with visual acuity, while foveal thickness showed a weak positive correlation. None of these relationships were statistically significant (p>0.05), suggesting that, structural changes in macular or RNFL thickness were not meaningfully associated with the level of visual acuity in amblyopic eyes as shown in Table 5.
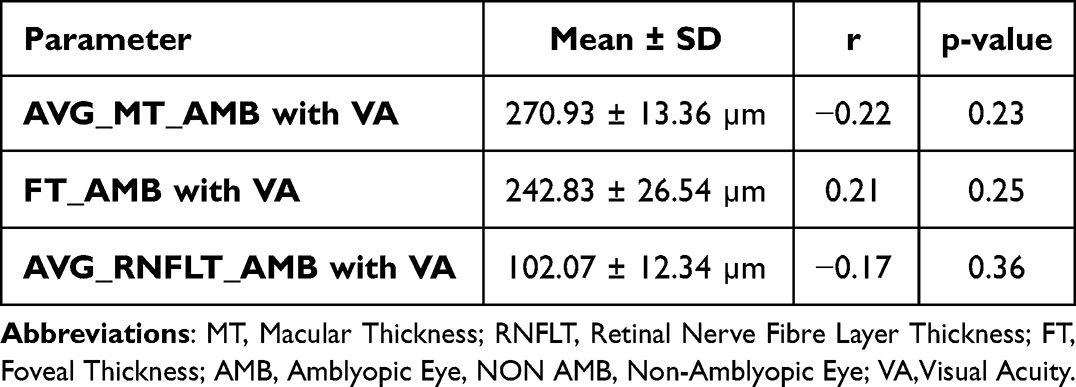 |
Table 5 Correlation of Visual Acuity with Average Macular Thickness, Foveal Thickness and Average RNFL Thickness of Amblyopic Eyes |
Discussion
The current study examined retinal structural differences between amblyopic and non-amblyopic eyes in children with spectral-domain optical coherence tomography (SD-OCT), noting parameters like macular thickness, foveal thickness, and retinal nerve fiber layer thickness. The results found that amblyopic eyes had significantly higher average macular thickness, foveal thickness, and RNFL thickness—namely average and superior quadrants—than non-amblyopic eyes. These findings firmly reinforce the hypothesis that amblyopia is more than a cortical process but also entails measurable morphologic changes in the retina.
The noted thickening of the average macular thickness (M = 270.93 ± 13.35 µm) in amblyopic eyes is consistent with previous findings by, Liu LL et al (2022),36 Zhu D et al (2022),37 Liao N et al (2019)38 and Nishikawa et al (2021),39 that inadequate visual input during critical developmental stages can impair retinal remodeling, especially in the macula. Likewise, far greater foveal thickness of amblyopic eyes (M = 242.83 ± 26.53 µm compared with 230.83 ± 17.27 µm for non-amblyopic eyes) supports reports of Pang et al (2011)29 and Yen et al (2004),32 that abnormal visual development can interfere with postnatal thining of inner retinal layers, such that the fovea remains hyperthick throughout. However, Studies showed bilateral alterations in inner retinal thickness among children with anisometropic amblyopia. Specifically, the ganglion cell layer (GCL) and inner plexiform layer (IPL) were significantly thinner in the peripheral macular regions of amblyopic eyes compared to control eyes, suggesting underlying structural differences. However, no significant thickness differences were found in the central macula, indicating that retinal changes may vary by macular location. The peripheral thinning of GCL + IPL in amblyopic eyes observed. The suggested possible causes are retinal ganglion cell degeneration, reduced bipolar synapses, and decreased Müller cell density.40,41
The greater mean and better RNFL thickness (M = 102.07 ± 12.33 µm and M = 124.13 ± 25.20 µm, respectively) in amblyopic eyes also indicate a possible deviation in axonal growth or glial distribution. Araki et al (2014),42 Alotaibi & Al Enazi (2011),25 and Kavitha et al (2019)31 reported similar trends, hypothesizing that decreased synaptic pruning or delayed maturation of ganglion cells may be the cause. But the absence of a statistically significant difference in inferior RNFL thickness (p = 0.078) reflects regional heterogeneity described in literature by Dickmann et al (2011)43 and Yalcin & Balci (2014),44 potentially reflecting variations in regional ganglion cell density or susceptibility.
Notably, no compelling structural variations were seen between amblyopia subtypes (anisometropic vs mixed) in amblyopic eyes, supporting findings by Kavitha et al (2019) that indicate the duration and severity of visual deprivation rather than etiology could be more important in shaping retinal anatomy.31 Moreover, except for a variation in superior RNFL thickness in the non-amblyopic eye between subtypes, no noteworthy changes were reported, which suggests possible subclinical changes or adaptation processes in the fellow eye.
Gender-based comparisons did not reveal any significant variation in retinal parameters in either group, consistent with previous studies (Zhu et al, 2022; Shen et al, 2021) that concluded paediatric ocular anatomy is relatively unaffected by gender-related hormonal differences.37,45
While our findings are consistent with many previous reports, conflicting evidence exists. Research like Repka et al (2009) and Altintas et al could not identify structural differences in amblyopic eyes, possibly due to methodological differences such as variations in OCT machines, sample size, age, ethnicity, and the omission of axial length adjustments. Omission of axial length measurements in this study is a significant shortcoming since axial length can dramatically affect retinal thickness measurements.26,46 An inverse correlation between axial length (AL) and intraretinal layer thickness in the macula, with greater thinning toward the outer retinal layers, suggesting retinal stretching with eye elongation.47
Clinically, these structural changes emphasize that amblyopia should be recognized as both a functional and an anatomical deviation. Consistent thickening of macular and RNFL areas in amblyopic eyes warrants inclusion of OCT imaging in the workup for amblyopia. Quantitative OCT measures can be useful as ancillary biomarkers for diagnosis, tracking, and measuring response to treatment.
Moreover, for both anisometropic and mixed amblyopia groups, amblyopic eyes had uniformly greater macular, foveal, and retinal nerve fiber layer (RNFL) thickness than their non-amblyopic fellow eyes. These trends are indicative of the possibility of subtle structural differences in amblyopic eyes, perhaps reflecting changed visual development or retarded retinal maturation. The increased foveal and RNFL thickness observed may suggest that amblyopia, particularly amblyopia with anisometropia or mixed etiology, could have a measurable but mild effect on the architecture of the retina. These anatomical patterns must be taken into account by clinicians interpreting OCT findings in amblyopic children, as increased foveal or RNFL measurements are not necessarily abnormal but may constitute the amblyopic pattern. Although these structural alterations do not yet influence treatment choices, they highlight the importance of close follow-up and may help to improve diagnostic standards for children with amblyopia.
This study found weak, non-significant correlations between visual acuity and retinal structural parameters in amblyopic eyes. The results align with prior conflicting evidence, highlighting ongoing debate over the structural changes associated with amblyopia.
Studies indicated that amblyopic eyes tend to show increased macular or foveal thickness compared to fellow or normal eyes, hypothesizing that abnormal postnatal visual stimulation may hinder normal foveal maturation.32,47 Yen et al suggested that amblyopia might impair the pruning of retinal ganglion cells, potentially leading to increased foveal and RNFL thickness.32 However, the current findings—showing no statistically significant association between these retinal structures and visual acuity—align with studies that have reported no substantial retinal structural differences in amblyopic eyes.46,48,49
The weak positive correlation between foveal thickness and visual acuity could hint at a subtle compensatory or developmental variation, although its clinical relevance remains unclear. In contrast, the weak negative correlations observed for both average macular thickness and RNFL thickness may suggest that greater thickness in these layers does not necessarily support better visual function in amblyopic eyes. Similar non-significant or inconsistent associations have been documented in studies by Pang et al and Dickmann et al, indicating that structural measurements alone may not be sufficient to explain the functional deficits seen in amblyopia.29,50
These findings underscore the multifactorial nature of amblyopia, where cortical and functional visual pathway alterations may play a more dominant role than retinal structural anomalies. Abnormal early visual experience (anisometropia, strabismus, deprivation) leads to altered binocular competition and suppression; neurons in primary visual cortex (V1) and higher visual cortex lose responsiveness/preference for the affected eye (reduced acuity, contrast sensitivity, positional coding).30 LGN (the thalamic relay) shows structural and functional changes in animal models and humans with amblyopia — reduced synaptic drive, altered cell size or responses — which can contribute to cortical abnormalities because LGN is the main input to V1.51,52 Amblyopic eyes sometimes show small but measurable differences in retinal structure (central macular thickness, RNFL) and microvasculature (OCTA measures of vessel density). Proposals include altered postnatal retinal development or neurovascular-unit changes in some amblyopia subtypes.52 Some studies report subtle functional changes (eg, fixation instability, small ERG/VEP differences) in amblyopic eyes — these functional abnormalities might reflect altered afferent signalling or downstream cortical suppression rather than primary retinal disease. Overall, functional retinal evidence is mixed and smaller in magnitude than cortical deficits.52 Moreover, this study suggests that reliance on macular or RNFL thickness as biomarkers for assessing amblyopic severity may be limited. Table 6 presents a comparative analysis of the findings from the present study with those of previous studies.
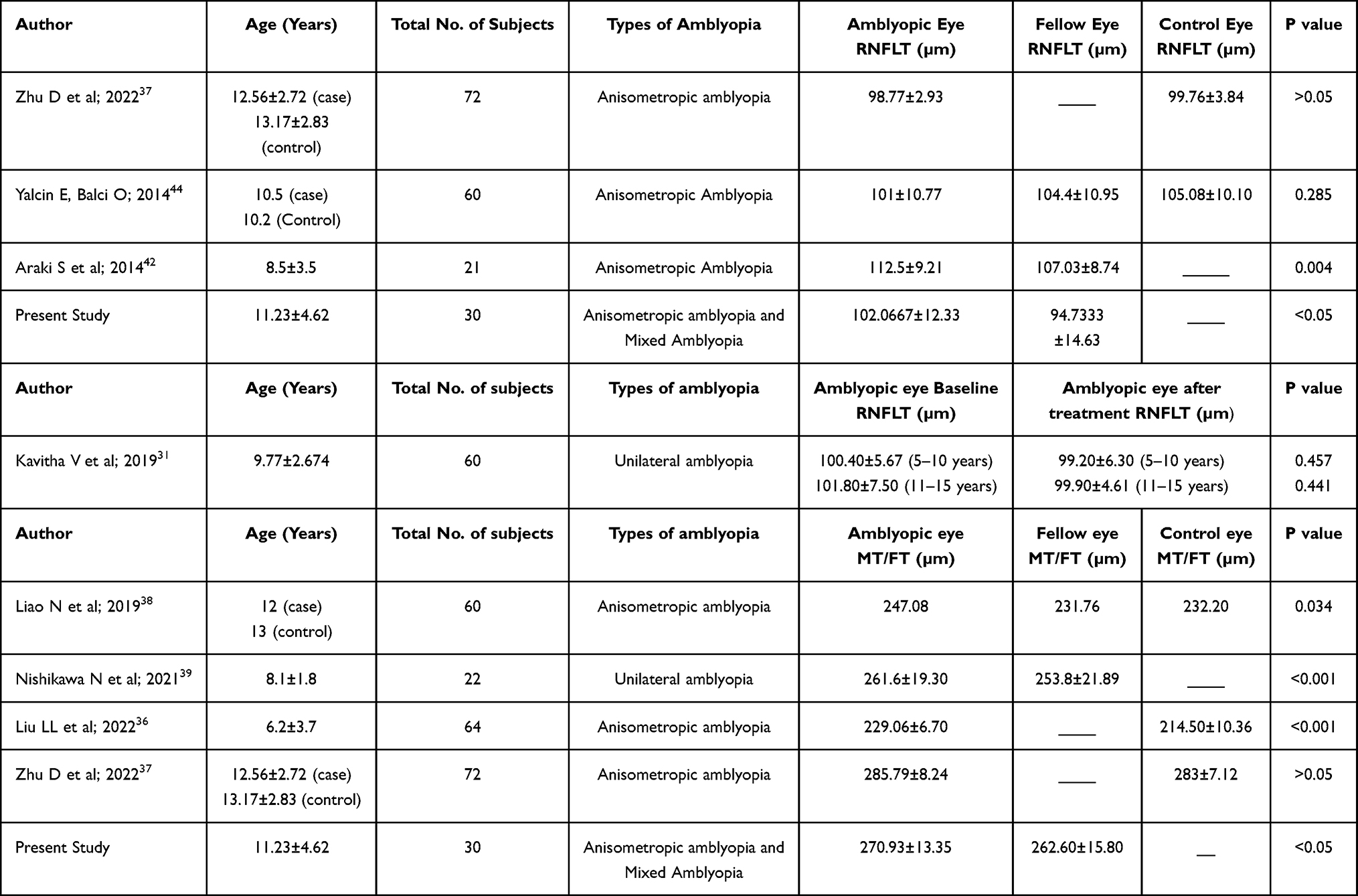 |
Table 6 Comparative Findings of Present Study with Previous Studies |
Future studies with larger cohorts, axial length correction, and incorporation of optical coherence tomography angiography (OCTA) may further elucidate the structural-functional relationship in amblyopia. Longitudinal data might also help determine whether subtle retinal changes precede or follow amblyopic development. The limitation of the study is not able to achieve the desired sample size.
Conclusion
In summary, our research supports the increasing evidence that amblyopia is not only associated with functional visual impairment but also structural retinal alterations, especially in the macula and RNFL. These alterations seem to be uniform irrespective of amblyopia type or gender. Although the exact pathophysiologic mechanisms are yet to be determined, our results underscore the value of OCT in clinical and research environments for amblyopia. Subsequent research should include axial length correction, investigate longitudinal changes after treatment, and continue to elucidate the functional significance of these structural abnormalities.
Human and Animal Rights
The authors didn’t violate the human rights during the research.
Study Limitations
The limitation of the study is not able to achieve the desired sample size and not considering the axial length corrections.
Abbreviations
BCVA, Best Corrected Visual Acuity; MAR, Minimum Angle of Resolution; RNFL, Retinal Nerve Fibre Layer; SD,OCT, Spectral Domain Optical Coherence Tomography; CMT, Central Macular Thickness; ETDRS, Early Treatment of Diabetic Retinopathy Study; ILM, Internal Limiting membrane; RPE, Retinal Pigment Epithelium; OCTA, Optical coherence tomography angiography.
Data Sharing Statement
The data that support the findings of this study are openly available whenever requested. The data that support the findings of this study are not publicly available due to containing information that could compromise the privacy of research participants but are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study is approved by The National University of Malaysia ethical committee (Ref. No. UKM/PPI/111/8/JEP-2021-176) and approval to collect the data was obtained from the hospital.
Consent for Publication
Both the authors have the consent for Publications.
Acknowledgments
We would like to thank the patients who had participated in the study and the hospital for allowing me to collect the data. We would also like to acknowledge Shankar Bhavan Netralaya for allowing us to collect data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no potential source of funding for the research.
Disclosure
The authors report no potential conflicts of interest in this work.
References
1. Blair K, Cibis G, Zeppieri M, Gulani A. Amblyopia. StatPearls; 2024.
2. Kaur S, Sharda S, Aggarwal H, Dadeya S. Comprehensive review of amblyopia: types and management. Indian J Ophthalmol. 2023;71(7):2677–13. doi:10.4103/IJO.IJO_338_23
3. Emmanuel BU, Burns JG, Thompson B, Thompson B. Amblyopia: a review of unmet needs, current treatment options, and emerging therapies. Survey Ophthalmol. 2023;68(3):507–525. doi:10.1016/j.survophthal.2023.01.001
4. Zhao PF, Zhou YH, Wang NL, Zhang J. Study of the wavefront aberrations in children with amblyopia. Chinese Med J. 2010;123(11):1431–1435.
5. Williams C. Amblyopia. BMJ Clin Eviden. 2009;2009:0709.
6. Fu Z, Hong H, Su Z, Lou B, Pan CW, Liu H. Global prevalence of amblyopia and disease burden projections through 2040: a systematic review and meta-analysis. Br J Ophthalmol. 2020;104(8):1164–1170. doi:10.1136/bjophthalmol-2019-314759
7. Hu B, Liu Z, Zhao J, et al. The global prevalence of amblyopia in children: a systematic review and meta-analysis. Front Pediatrics. 2022;10:819998. doi:10.3389/fped.2022.819998
8. Janti SS, Alluri VM, Kolavai RR, et al. Prevalence of amblyogenic risk factors among school children in India using the spot vision screener. Cureus. 2024;16(8).
9. Bamhane P, Singh P, Kumar K, et al. A prospective study of amblyopia and its risk factors in selected school going children of Bhopal region. Indian J Clin Experi Ophthalmol. 2022;8(1):24–29. doi:10.18231/j.ijceo.2022.006
10. Gopal SK, Kelkar J, Kelkar A, Pandit A. Simplified updates on the pathophysiology and recent developments in the treatment of amblyopia: a review. Indian J Ophthalmol. 2019;67(9):1392–1399. doi:10.4103/ijo.IJO_11_19
11. Julku H, Rouhinen S, Huttunen HJ, et al. Reduced evoked activity and cortical oscillations are correlated with anisometric amblyopia and impairment of visual acuity. Sci Rep. 2021;11(1):8310. doi:10.1038/s41598-021-87545-9
12. Wang Y, Wu Y, Luo L, Li F. Structural and functional alterations in the brains of patients with anisometropic and strabismic amblyopia: a systematic review of magnetic resonance imaging studies. Neural Regen Res. 2023;18(11):2348–2356. doi:10.4103/1673-5374.371349
13. Cruz OA, Repka MX, Hercinovic A, et al. Amblyopia preferred practice pattern. Ophthalmology. 2022;130(3):P136. doi:10.1016/j.ophtha.2022.11.003
14. Robitaille JM. Long-term visual outcomes in prematurely born children. J Binocular Vision Ocular Motility. 2024;74(1):1–8. doi:10.1080/2576117X.2023.2287633
15. Cao Y, Wang Y, Li B, et al. Analysis of risk factors associated with the high incidence of amblyopia in preterm infants at the corrected gestational age of 12 months. BMC Pediatric. 2023;23(1):136. doi:10.1186/s12887-023-03937-y
16. Toro MD, Bremond-Gignac D, Brézin AP, et al. COVID-19 outbreak and increased risk of amblyopia and epidemic myopia: insights from EUROCOVCAT group. Eur J Ophthalmol. 2022;32(1):17–22. doi:10.1177/11206721211053175
17. Panel SP, Sprunger DT, Lambert SR, et al. Pediatric ophthalmology/strabismus preferred practice pattern development process and participants. Ophthalmology. 2022;130(3):P179. doi:10.1016/j.ophtha.2022.11.002
18. Webber AL, Schmid KL, Baldwin AS, Hess RF. Suppression rather than visual acuity loss limits stereoacuity in amblyopia. Invest Ophthalmol Visual Sci. 2020;61(6):50. doi:10.1167/iovs.61.6.50
19. Song S, Levi DM, Pelli DG. A double dissociation of the acuity and crowding limits to letter identification, and the promise of improved visual screening. J Vis. 2014;14(5):3. doi:10.1167/14.5.3
20. Levi DM, McKee SP, Movshon JA. Visual deficits in anisometropia. Vision Research. 2011;51(1):48–57. doi:10.1016/j.visres.2010.09.029
21. Chinn RN, Michalak SM, Shoshany TN, Bishop K, Staffa SJ, Hunter DG. Effect of sequential and simultaneous patching regimens in unilateral amblyopia. Am J Ophthalmol. 2022;233:48–56. doi:10.1016/j.ajo.2021.07.012
22. Chen AM, Cotter SA. The amblyopia treatment studies: implications for clinical practice. Advanc Ophthalmol Optometry. 2016;1(1):287. doi:10.1016/j.yaoo.2016.03.007
23. Milla M, Molina-Martín A, Piñero DP. Long-term efficacy of the combination of active vision therapy and occlusion in children with strabismic and anisometropic amblyopia. Children. 2022;9(7):1012. doi:10.3390/children9071012
24. Lee SH, Erickson GB. Management of anisometropic amblyopia: a case report and brief review. Vision Dev Rehab. 2019;5(2):100–102.
25. Alotaibi AG, Al Enazi B. Unilateral amblyopia: optical coherence tomography findings. Saudi J Ophthalmol. 2011;25(4):405–409. doi:10.1016/j.sjopt.2011.06.001
26. Altintas Ö, Yüksel N, Özkan B, Çaglar Y. Thickness of the retinal nerve fiber layer, macular thickness, and macular volume in patients with strabismic amblyopia. J Pediatr Ophthalmol Strabismus. 2005;42(4):216–221. doi:10.3928/01913913-20050701-03
27. Walker RA, Rubab S, Voll AR, Erraguntla V, Murphy PH. Macular and peripapillary retinal nerve fibre layer thickness in adults with amblyopia. Can J Ophthalmol. 2011;46(5):425–427. doi:10.1016/j.jcjo.2011.07.013
28. Lekskul A, Wuthisiri W, Padungkiatsagul T. Evaluation of retinal structure in unilateral amblyopia using spectral domain optical coherence tomography. J AAPOS. 2018;22(5):386–389. doi:10.1016/j.jaapos.2018.05.014
29. Pang Y, Goodfellow GW, Allison C, Block S, Frantz KA. A prospective study of macular thickness in amblyopic children with unilateral high myopia. Invest Ophthalmol Visual Sci. 2011;52(5):2444–2449. doi:10.1167/iovs.10-5550
30. Dickmann A, Petroni S, Perrotta V, et al. A morpho-functional study of amblyopic eyes with the use of optical coherence tomography and microperimetry. J AAPOS. 2011;15(4):338–341.
31. Kavitha V, Heralgi MM, Harishkumar PD, Harogoppa S, Shivaswamy HM, Geetha H. Analysis of macular, foveal, and retinal nerve fiber layer thickness in children with unilateral anisometropic amblyopia and their changes following occlusion therapy. Indian J Ophthalmol. 2019;67(7):1016–1022. doi:10.4103/ijo.IJO_1438_18
32. Yen MY, Cheng CY, Wang AG. Retinal nerve fiber layer thickness in unilateral amblyopia. Invest Ophthalmol Visual Sci. 2004;45(7):2224–2230.
33. Francisconi CL, Wagner MB, Ribeiro RV, Freitas AM. Effects of axial length on retinal nerve fiber layer and macular ganglion cell-inner plexiform layer measured by spectral-domain OCT. Arquivos Brasileiros de Oftalmologia. 2020;83(4):269–276. doi:10.5935/0004-2749.20200039
34. Bennett AG, Rudnicka AR, Edgar DF. Improvements on Littmann’s method of determining the size of retinal features by fundus photography. Graefes Arch Clin Exp Ophthalmol. 1994;232(6):361–367. doi:10.1007/BF00175988
35. Öner V, Özgür G, Türkyilmaz K, Şekeryapan B, Durmuş M. Effect of axial length on retinal nerve fiber layer thickness in children. Eur J Ophthalmol. 2014;24(2):265–272. doi:10.5301/ejo.5000345
36. Liu LL, Wang YC, Cao M, et al. Analysis of macular retinal thickness and microvascular system changes in children with monocular hyperopic anisometropia and severe amblyopia. Dis. Markers. 2022;2022(1):9431044. doi:10.1155/2022/9431044
37. Zhu D, Sun Q, Yang H, Zou Y, Liu C, Xu Y. Macular and optic disc parameters in children with amblyopic and nonamblyopic eyes under optical coherence tomography fundus images. Comput Math Method Med. 2022;2022(1):9409749. doi:10.1155/2022/9409749
38. Liao N, Jiang H, Mao G, et al. Changes in macular ultrastructural morphology in unilateral anisometropic amblyopia. Am J Transl Res. 2019;11(8):5086.
39. Nishikawa N, Chua J, Kawaguchi Y, et al. Macular microvasculature and associated retinal layer thickness in pediatric amblyopia: magnification-corrected analyses. Invest Ophthalmol Visual Sci. 2021;62(3):39. doi:10.1167/iovs.62.3.39
40. Chen W, Xu J, Zhou J, et al. Thickness of retinal layers in the foveas of children with anisometropic amblyopia. PLoS One. 2017;12(3):e0174537. doi:10.1371/journal.pone.0174537
41. Xia Z, Chen H, Zheng S. Thicknesses of macular inner retinal layers in children with anisometropic amblyopia. Biomed Res Int. 2020;2020(1):6853258. doi:10.1155/2020/6853258
42. Araki S, Miki A, Yamashita T, et al. A comparison between amblyopic and fellow eyes in unilateral amblyopia using spectral-domain optical coherence tomography. Clin Ophthalmol. 2014;7:2199–2207. doi:10.2147/OPTH.S69501
43. Dickmann A, Petroni S, Salerni A, Dell’Omo R, Balestrazzi E. Unilateral amblyopia: an optical coherence tomography study. J AAPOS. 2009;13(2):148–150. doi:10.1016/j.jaapos.2008.10.009
44. Yalcin E, Balci O. Peripapillary retinal nerve fiber layer and foveal thickness in hypermetropic anisometropic amblyopia. Clin Ophthalmol. 2014;12:749–753.
45. Shen Y, Zhao J, Sun L, et al. The long-term observation in Chinese children with monocular myelinated retinal nerve fibers, myopia and amblyopia. Translational Pediatrics. 2021;10(4):860. doi:10.21037/tp-20-452
46. Repka MX, Kraker RT, Tamkins SM, Suh DW, Sala NA, Beck RW, Pediatric Eye Disease Investigator Group. Retinal nerve fiber layer thickness in amblyopic eyes. Am J Ophthalmol. 2009;148(1):143–147. doi:10.1016/j.ajo.2009.01.015
47. Szigeti A, Tátrai E, Varga BE, et al. The effect of axial length on the thickness of intraretinal layers of the macula. PLoS One. 2015;10(11):e0142383. doi:10.1371/journal.pone.0142383
48. Huynh SC, Samarawickrama C, Wang XY, et al. Macular and nerve fiber layer thickness in amblyopia: the sydney childhood eye study. Ophthalmology. 2009;116(9):1604–1609. doi:10.1016/j.ophtha.2009.03.013
49. Kee S-Y, Lee S-Y, Lee Y-C. Thicknesses of the fovea and retinal nerve fiber layer in amblyopic and normal eyes in children. Korean J Ophthalmol. 2006;20(3):177–181. doi:10.3341/kjo.2006.20.3.177
50. Al-Haddad, Christiane E, El Mollayess G, Cherfan C, Jaafar D, Bashshur Z. Retinal nerve fiber layer and macular thickness in amblyopia as measured by spectral domain optical coherence tomography. J Am Associat Pediatric Ophthalmol Strabismus. 2011;15(1):e11.
51. Levi DM. Rethinking amblyopia 2020. Vision Research. 2020;176:118–129. doi:10.1016/j.visres.2020.07.014
52. Hess RF, Thompson B, Gole G, Mullen KT. Deficient responses from the lateral geniculate nucleus in humans with amblyopia. Eur J Neurosci. 2009;29(5):1064–1070. doi:10.1111/j.1460-9568.2009.06650.x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.