Back to Journals » Journal of Blood Medicine » Volume 12
Macrophage Activation Led Acute Heart Failure Managed Successfully with Immunosuppression
Authors Seegobin K ![]() , Alhaj Moustafa M
, Alhaj Moustafa M ![]() , Majeed U, Ray JC, Shaikh M, Jiang L
, Majeed U, Ray JC, Shaikh M, Jiang L ![]() , Tun HW
, Tun HW ![]()
Received 21 September 2021
Accepted for publication 23 November 2021
Published 7 December 2021 Volume 2021:12 Pages 1037—1043
DOI https://doi.org/10.2147/JBM.S340361
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Supplementary video 1 of "MAS managed with immunosuppression" [ID 340361].
Views: 105
Karan Seegobin,1 Muhamad Alhaj Moustafa,1 Umair Majeed,1 Jordan C Ray,2 Marwan Shaikh,1 Liuyan Jiang,3 Han W Tun1
1Department of Hematology and Medical Oncology, Mayo Clinic, Jacksonville, FL, 32224, USA; 2Departmentof Cardio-Oncology, Mayo Clinic, Jacksonville, FL, 32224, USA; 3Department of Pathology, Mayo Clinic, Jacksonville, FL, 32224, USA
Correspondence: Han W Tun
Department of Hematology and Medical Oncology, Mayo Clinic Hospital, Jacksonville, FL, 32224, USA
Email [email protected]
Abstract: Macrophage activation leading to multi-organ dysfunction/failure has been described in various hematologic disorders like hemophagocytic lympho-histiocytosis (HLH), also known as macrophage activation syndrome (MAS) and macrophage activation like syndrome (MALS). Congestive heart failure (CHF) appears to be an uncommon manifestation of macrophage activation. This novel entity of macrophage activation-associated cytokine-mediated CHF has not been well reported in the medical literature. We report two young female patients with acute CHF secondary to macrophage activation-associated cytokine storm. An extensive diagnostic workup was negative for other etiologies, such as ischemia, myocarditis, or infections. Their clinical, laboratory, and pathologic findings did not meet the diagnostic criteria for hemophagocytic syndrome (HPS)/MAS. However, both had laboratory and pathologic findings which were consistent with macrophage activation and cytokine storm. One patient met criteria for MALS. Therapeutically, our patients were promptly treated with steroids with or without anti-cytokine therapy with rapid restoration of cardiac function. Macrophage activation-induced disease may not always fulfil the diagnostic criteria for the currently known macrophage activation disorders. We suggest that markers of macrophage activation and cytokine levels should be part of the diagnostic workup in patients with otherwise unexplained acute CHF. Additional research is warranted to further elucidate the underlying mechanism of this disorder.
Keywords: macrophage activation syndrome, MAS, macrophage activation like syndrome, MALS, cytokine release storm, CRS, reversible systolic heart failure, immunosuppression
Plain Language Summary
Macrophages are cells that surround and kill microorganisms, remove dead cells, and stimulate the action of other immune system cells. These macrophages are found in many organs and produce cytokines which is a chemical that can drive inflammation. In excess these cytokines can affect other organs such as the heart and result in heart failure. Some laboratory tests that can indicate macrophage activation include elevated ferritin, triglyceride, and CRP. Steroids and other anti-inflammatory medications can suppress this inflammation and improve symptoms and organ function in these patients with macrophage activation and organ dysfunction. We report two cases with unexplained heart failure who were found to have features of macrophage activation after further workup. They both responded promptly to immunosuppressive treatment. We suggest that markers of macrophage activation should be evaluated in patients with unexplained CHF. In some proven cases of heart failure, secondary to macrophage activation, prompt treatment with immunosuppressants could lead to clinical improvement, and such treatment should be sought only after other causes of heart failure have been clearly ruled out and must be done by physicians with expertise in managing heart failure.
Introduction
Macrophage activation leading to multi-organ dysfunction/failure has been described in various hematologic disorders including hemophagocytic lympho-histiocytosis (HLH)/macrophage activation syndrome (MAS), and macrophage activation like syndrome (MALS).1,2 Congestive heart failure (CHF) appears to be an uncommon manifestation of macrophage activation.3 We found seven case reports of HLH presenting with systolic heart failure in the medical literature (Table 1), six of whom had complete recovery of cardiac function with immunosuppressive therapy; post treatment cardiac function was not reported in one case. Here we report two cases of acute CHF associated with laboratory and pathologic evidence of macrophage activation and cytokine storm without meeting the diagnostic criteria for MAS/HLH. One patient met the criteria for MALS. Both cases had increased M2 macrophages in the bone marrow. Both cases had a dramatic response to immunosuppressive therapy with full recovery of cardiac function.
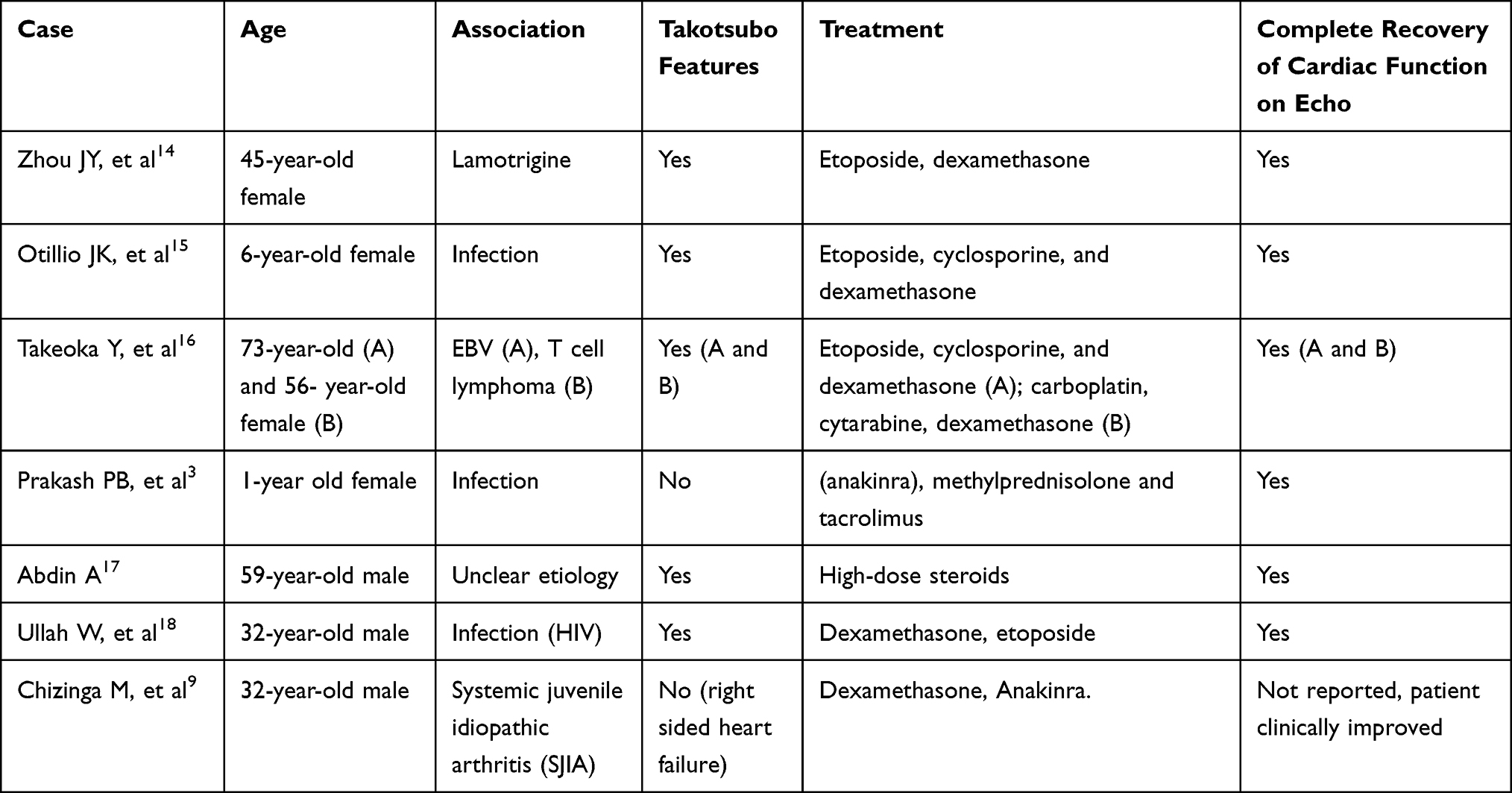 |
Table 1 Literature Review of Prior Cases with HLH Systolic Heart Failure |
Case 1
A 37-year-old female without any prior co-morbidity was hospitalized with acute onset of severe shortness of breath and fatigue. The initial examination showed blood pressure 102/96 mmHg, pulse 121 bpm, temperature 36.8 °C, respiratory rate 35 bpm and SpO2 94% on 2LO2. Bilateral inspiratory crackles were present on chest auscultation with normal heart sounds, S1 and S2, with added S3. Initial workup (Table 2) showed hemoglobin 9.3 g/dL (11.6–15), hematocrit 54% (35.5–44.9), platelet 76×109 (157–371), white cell count 2.4×109 (3.4–9.6), absolute neutrophil count 0.11×109 (1.56–6.45), absolute monocyte 3.0×109 (0.26–0.81), NT proBNP 17,280 pg/mL (<140), troponin T 11 (<10 ng/L), triglyceride 556 mg/dL (H), fibrinogen 312 mg/dL (200–393), ferritin 568 (11–307 mcg/L), CRP 92.4 (<8.0 mg/L), LDH 261 (122–222 U/L), presence of heterozygous prothrombin G20210A gene mutation, and interleukin-6, 8.6 pg/mL (<1.8), creatine kinase 80 U/L (26–192). Serial troponin T levels were 10 ng/L (6 hours after), and 8 ng/L (on day 2). Her HScore was 98 points based on the above results. Other lab workup including renal function panel, liver function panel, and autoimmune screen were unremarkable. Blood smear showed absolute neutropenia with left-shifted neutrophils and markedly increased immature monocytes. Electrocardiogram (EKG) showed sinus tachycardia with T inversion in the inferior leads. CT chest showed moderate bilateral pleural effusions, interstitial edema and central perivascular ground-glass opacities. Echocardiogram showed ejection fraction of 25%, with severe generalized left ventricular hypokinesis; normal left ventricular chamber size and thickness; normal right ventricular chamber size with reduced systolic function; right ventricle pressure 23 mmHg; right and left atrium was of normal size; mild mitral valve regurgitation, mild tricuspid valve regurgitation; normal aortic and pulmonary valve; small pericardial effusion (video 1). Abdominal ultrasound showed normal spleen and liver size. Initially she was started on broad-spectrum antibiotics (vancomycin, piperacillin and tazobactam) and diuretics. Her oxygen requirements increased within 24 hours of admission necessitating non-invasive positive-pressure ventilation with BIPAP at 50% FiO2, and ICU monitoring. She remained hemodynamically stable in the ICU and did not require inotropic support. After 72 hours, extensive workup for underlying infection including bacterial, viral, fungal and mycobacterial organisms were all negative; and despite antibiotics, interleukin-6 and ferritin continued to increase to 11.4, and 731 respectively, with increasing liver enzymes. Bone marrow biopsy showed hypercellularity with diffuse infiltration by CD68+ macrophages and atypical megakaryocytes; the macrophages are predominantly type 2 macrophages since they are negative for pSTAT1 and positive for CD163 (Figure 1). Chromosome analysis, acute myeloid leukemia (AML) FISH panel, next generation sequencing (NGS) for myeloid neoplasms (11 gene panel), and myeloproliferative neoplasm (MPN) panel (JAK2, CALR, MPL) were all negative. Macrophage activation associated cytokine-mediated disease process was suspected in the absence of evidence for ischemia, myocarditis, autoimmune disorders, and infections. She was treated with dexamethasone 40 mg daily and had significant clinical improvement, no longer requiring oxygen after 5 days of steroids. Furthermore, echocardiogram after 5 days of steroids showed significant improvement in EF to 55% with normal left ventricular chamber size, wall thickness and regional wall motion; normal left ventricular diastolic function; normal right ventricular chamber size and function; estimated right ventricular systolic pressure 23 mmHg; mild mitral valve regurgitation and mild tricuspid valve regurgitation; normal pulmonary valve systolic velocity and small circumferential pericardial effusion (video 2). There was also resolution of hematologic abnormalities.
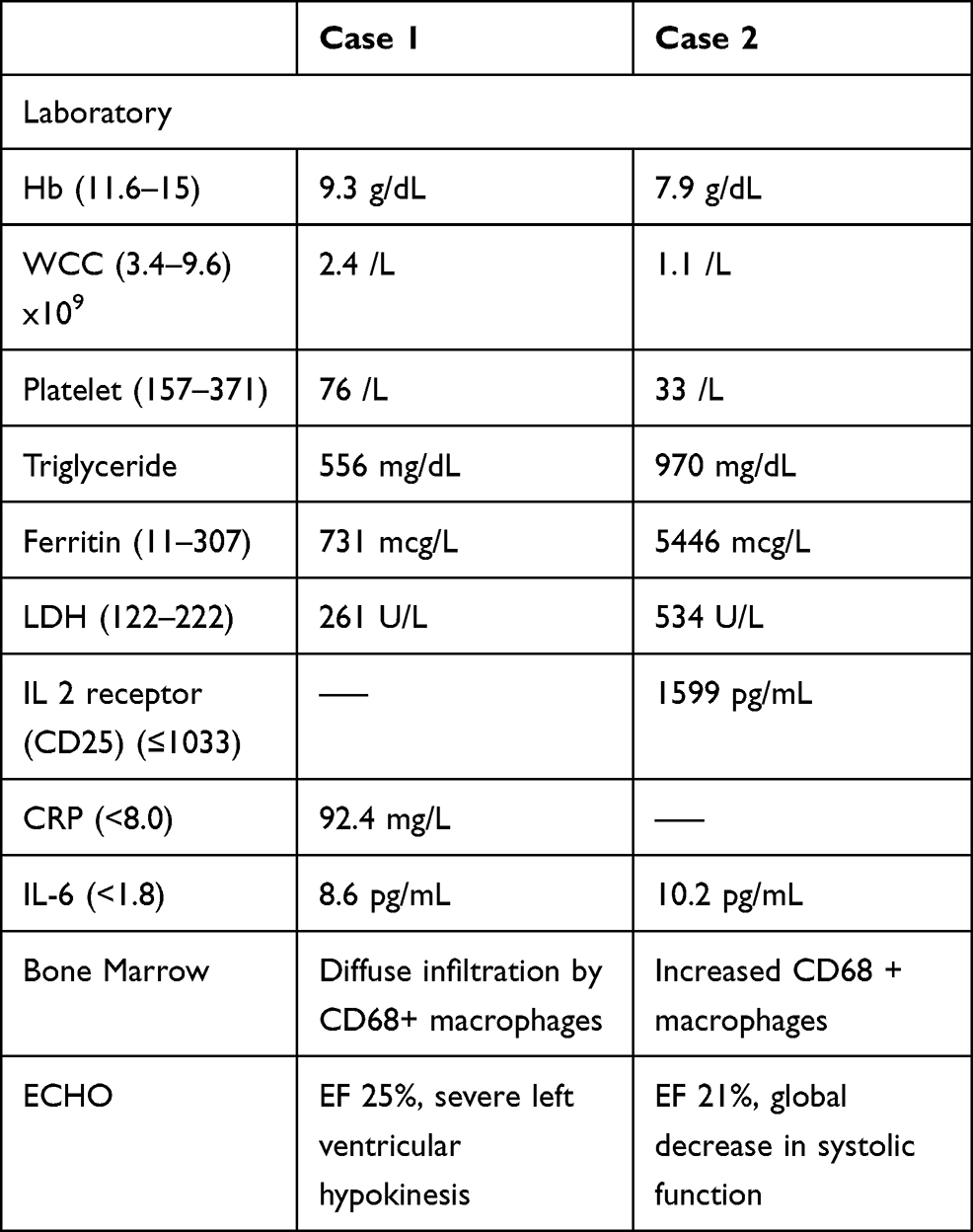 |
Table 2 Laboratory, Bone Marrow and ECHO Findings of Case 1 and 2 |
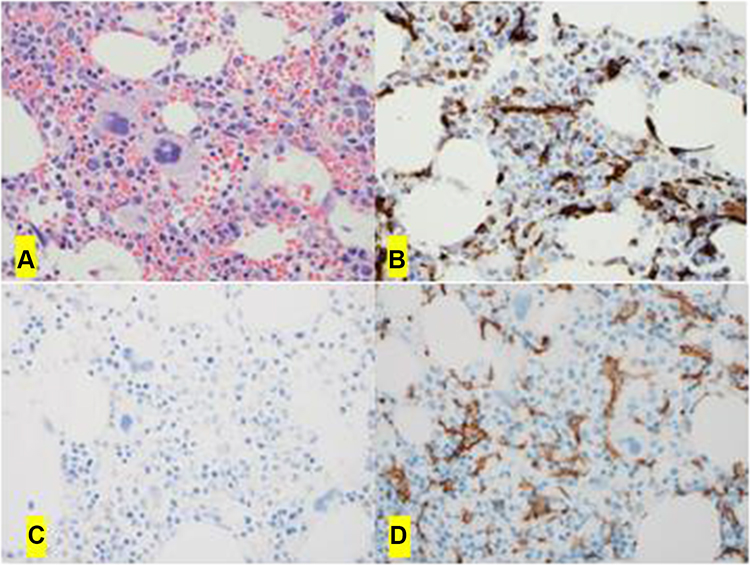 |
Figure 1 The bone marrow biopsy shows hypercellularity with increased megakaryocytes (A, H&E x40). The immunohistochemical studies show increased interstitial macrophages by CD68 (PGM1) (B, x40); and they are type 2 macrophages negative for pSTAT1 (C, x 0) but positive for CD163 (D, x40). |
She was discharged on a 6-week steroid taper. One month later, ejection fraction was 62% and at 2-month follow-up she was clinically doing well. Unfortunately, several months later she was found to have avascular necrosis of the bilateral distal femur and proximal tibia and is currently followed by orthopedics for further care. She was started on Eliquis 10 mg twice daily for 7 days then 5 mg twice daily for 21 days, then 2.5 mg twice daily for 6 months in light of the possible association of her prothrombin gene mutation and development of avascular necrosis. Her pain symptom subjectively improved with the initiation of anticoagulation.
Case 2
A 41-year-old female was hospitalized with subjective fever, nausea, vomiting, and abdominal pain which were present for 3 weeks. Initial examination showed blood pressure 66/39 mmHg, pulse 135 bpm, temperature 36.6 °C, respiratory rate 35 bpm and SpO2 99%. Normal heart sounds and breath sounds were heard on auscultation. Initial workup (Table 2) showed hemoglobin 7.9 g/dL (11.6–15), hematocrit 24.7% (35.5–44.9), platelet 33×109 (157–371), white cell count 1.1×109 (3.4–9.6), absolute neutrophil count 0.5×109 (1.56–6.45), troponin T 17 (<10 ng/L), triglyceride 970 mg/dL, fibrinogen 601 mg/dL (200–393), ferritin 5446 (11–307 mcg/L), LDH 534 (122–222 U/L), interleukin 2 receptor (CD25) soluble 1599 pg/mL (≤1033), IL-6 10.2 pg/mL, prothrombin time 14.4 (9.4–12.5 sec), INR 1.3 (0.9–1.1), activated partial prothrombin time 35 (25–37 sec) and elevation of liver enzymes (total bilirubin 3.1 mg/dL (<1.2), direct bilirubin 2.7 mg/dL (0–0.3), alanine aminotransferase 81 U/L (7–45), aspartate aminotransferase 241 U/L (8–43), alkaline phosphatase 117 U/L (35–104). Serial troponin T levels were 13 ng/L (day 2) and 18 ng/L D3 (day 3). Other laboratory workup included renal function panel and autoimmune screen were unremarkable. Her HScore was 152 based on the above results. Blood smear showed absolute leukopenia and lymphopenia. EKG showed sinus tachycardia with T inversions in V1.
Echocardiogram showed left ventricular ejection fraction 21% with a normal size and thickness left ventricle with multiple regional wall motion abnormalities in non−coronary distribution and associated global decrease in systolic function; grade 3/4 left ventricular diastolic dysfunction, consistent with severely elevated left ventricular filling pressure; normal right ventricular chamber size with mild global decrease in systolic function, right ventricular systolic pressure 42 mmHg, tricuspid annular plane systolic excursion (TAPSE) was 11 mm (20–22); mitral valve was normal with moderate mitral valve regurgitation and severe tricuspid valve regurgitation. Aortic and pulmonary valves were normal. No pericardial effusion. Normal size of both right and left atrium (video 3). Abdominal ultrasound did not show splenomegaly/hepatomegaly. She was started on broad spectrum antibiotics (vancomycin, piperacillin and tazobactam) and admitted to ICU as she required inotropic support with milrinone starting at 0.375 mcg/kg/min and then titrated as needed to maintain blood pressure. Extensive workup for underlying infection including bacterial, viral, fungal and mycobacterial organisms were all negative. Bone marrow biopsy showed hypocellularity with left-shifted myelopoiesis, increased clusters of immature myeloid precursors, and increased CD68+ macrophages, which were predominantly type 2 macrophages negative for pSTAT1 and positive CD163 (Figure 2). Chromosome analysis, AML FISH, NGS for myeloid neoplasms (11 gene panel), MPN panel (JAK2, CALR, and MPL), immunoglobulin gene rearrangement, and T-cell receptor gene rearrangements were all unremarkable. Macrophage activation associated cytokine-mediated systemic disease process was suspected and treated with anakinra (anti-IL1) 100 mg subcutaneous for 7 days, and dexamethasone 10 mg once daily for 7 days followed by a 6-week steroid taper. She clinically improved rapidly and was completely off inotropic support after 6 days of immunosuppression treatment. Repeat echocardiogram after 7 days of immunosuppressive treatment showed significantly improved left ventricular function with ejection fraction 70%; normal left ventricular chamber size and wall thickness with hyperdynamic systolic function; normal right ventricular chamber size and function; no regional wall motion abnormalities; no pericardial effusion (video 4). Complete resolution of cytopenias and normalization of liver function was also seen. At 8 months follow up she has no clinical features of heart failure.
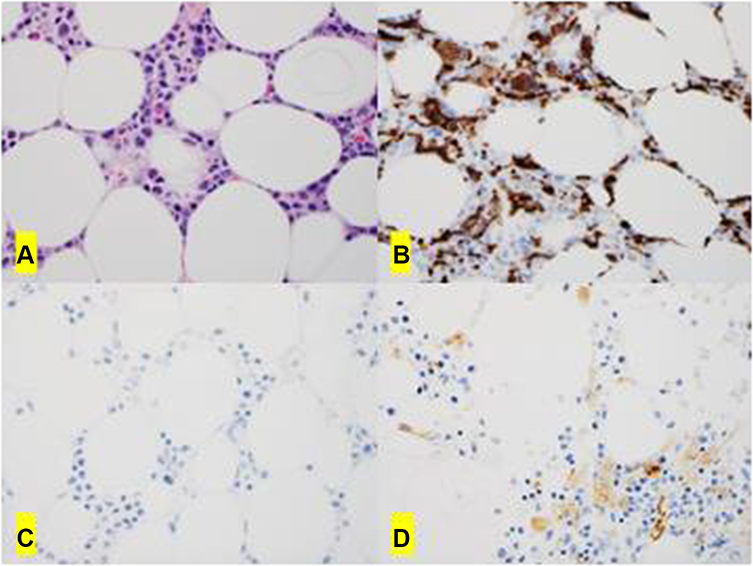 |
Figure 2 The bone marrow biopsy shows hypocellularity with left-shifted myelopoiesis (A, H&E x 0). Immunohistochemical studies shows increased interstitial macrophages by CD68 (PGM1) (B, x40); they are type 2 macrophages (M2) negative for pSTAT1 (C, x 0) and positive for CD163 (D, x40). |
Discussion
Our two young patients represent unique cases of acute CHF secondary to macrophage activation-associated cytokine storm with one patient meeting criteria for MALS. It is interesting that they did not meet the diagnostic criteria for known macrophage activation disorders such as HLH, also known as MAS.2,4,5 They clearly had laboratory evidence of macrophage activation which includes elevated ferritin, triglyceride, CRP, IL-6, and CD25.2 The other prominent finding is infiltration of the bone marrow by CD68+ type 2 macrophages, associated with pancytopenia which can be seen in HLH/MAS.2 It appears that activated macrophages are located in the bone marrow compromising hematopoiesis and mediating CHF via cytokine storms. In our cases the underlying mechanism for macrophage activation is not clear, negative extensive genetic and molecular testing together with rapid response to immune suppression would indicate a reactive process inciting macrophage activation. They both had increased M2 macrophages in the bone marrow. M2 macrophages which can be seen in MAS, are heterogeneous in comparison to M1 macrophages.6 In these cells the production of proinflammatory mediators are downregulated.6 While they are mostly described as anti-inflammatory, there is some data to suggest they may act as an innate immune sensor for bacteria and trigger production of pro-inflammatory cytokines.6,7
HLH/MAS is diagnosed if at least five of the eight criteria of the International Histiocyte Society (2004-HLH criteria), published in 2007, are met: (a) fever, (b) splenomegaly, (c) cytopenia of at least two lineages; (d) fasting triglycerides ≥265 mg/dl and fibrinogen ≤150 mg/dl; (e) hemophagocytosis in the bone marrow; (f) low or absent NK-cell activity; (g) ferritin ≥500 ng/mL; and soluble CD25 ≥2400 units/mL.2 Presence of bone marrow hemophagocytosis is one of the criteria taken into consideration for the diagnosis of MAS.8 MALS, which is often described in the setting of sepsis, came about due to the difficulty of performing a bone marrow biopsy in every critically ill patient and is defined as an HS score more than 151 or patients with both hepatobiliary dysfunction (HBD) and disseminated intravascular coagulation (DIC). Both cases did not meet the criteria for HLH/MAS (they both had two out of the five criteria for HLH/MAS). We did not have NK cell activity or soluble CD 25 levels available in both cases. An HS score of case 2 met the criteria for MALS, further supporting the presence of macrophage activation. Our second case had more evidence of multiorgan dysfunction characterized by liver dysfunction, heart failure and lower degrees of cytopenias (with respect to case 1) and overall was more critically ill and required inotropic support. It is possible that she may have been on the more severe end of the disease spectrum of macrophage activating disorders; while our first patient who did not have liver dysfunction, less severe cytopenias and not requiring inotropic support may have been on a milder end of the spectrum characterizing this novel entity of macrophage activation-associated cytokine-mediated CHF. Bone marrow features of macrophage activation were present in both cases. One hypothesis is that macrophage activation in the bone marrow may be the first sign of the disease and if not diagnosed early may propagate from macrophage associated cytokine storm to the more severe end of the spectrum (manifesting as MALS or HLH) with HLH being the most severe of these entities.
The other unique aspect of our two patients is CHF as a prominent organ dysfunction. In our medical literature search, we identified only seven case reports of HLH with systolic heart failure (Table 1). Of note right ventricle failure without involvement of the left ventricle can also be involved.9 It appears that CHF is uncommon in macrophage activation disorders.3 In those cases and our two patients, immunosuppressive therapy worked very well with rapid restoration of cardiac function. The ECHO findings in both cases and non-rising troponin levels helped rule out other conditions such as takotsubo cardiomyopathy, myocarditis and acute myocardial infarction. Cardiac catheterization was not pursued considering their quick recovery with immunosuppressive medications.
We used steroid monotherapy in our first patient and steroid with anakinra (Anti-IL-1 monoclonal antibody) in our second patient with excellent therapeutic outcomes. Dexamethasone is a standard steroid used in management of HLH.10 We chose to use anakinra in our second patient as her clinical status was rapidly deteriorating. IL-1 is an important cytokine which can activate an innate immune response with activation of macrophages.11 In both patients, IL-6 was elevated. It would have also been reasonable to try anti-IL-6 monoclonal antibody therapy. In some cases while patients respond to immunosuppressive medications additional supportive care, such as veno-arterial extracorporeal membrane oxygenation (VA-ECMO), may be needed and can be lifesaving.9
Unfortunately, our first patient developed avascular necrosis several months after she recovered from her episode of heart failure. There are many short-term and long-term side effects of high dose steroids, avascular necrosis is one such reported side effect. We felt other factors may have contributed to her avascular necrosis, such as the presence of her prothrombin G20210A gene mutation. Hypercoagulable states have been reported to be associated with avascular necrosis and anticoagulation has been reported to help in some cases. This was our rationale using Eliquis in this patient.12,13 It is unclear if macrophage activation would have had a role in the pathogenesis of her avascular necrosis. Monitoring for adverse effects of steroids during the short- and long-term follow up of these patients is also important.
In conclusion, we report a novel macrophage activation-induced disease entity which does not fulfil the diagnostic criteria for HLH/MAS and is clinically characterized prominently by acute CHF and pancytopenia. We suggest that macrophage activation should be entertained as a differential diagnosis in patients with acute, otherwise unexplained, CHF. Markers of macrophage activation and hematologic parameters including complete blood counts and bone marrow biopsy should be evaluated to diagnose this entity. Therapeutically, patients with this disorder should be promptly treated with steroids and anti-cytokine therapy after considering the risk of the therapy vs benefit and only patients with proven cases should be treated with immunosuppressants. The clinical outcome could be better if the disease is recognized early in the course and appropriate therapy, such as immunosuppressants, started early with consideration of advanced therapies such as ECMO in refractory cases. Additional research is warranted to further elucidate the underlying disease mechanism.
Ethics Approval
Institutional approval was not required to publish the case details.
Consent
Written and informed consent was obtained from both patients for publication of this manuscript.
Acknowledgments
We thank the patients for providing consent to publish this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
All authors have no conflicts of interest to declare.
References
1. Bracaglia C, Prencipe G, De Benedetti F. Macrophage activation syndrome: different mechanisms leading to a one clinical syndrome. Pediatr Rheumatol Online J. 2017;15(1):5. doi:10.1186/s12969-016-0130-4
2. Karakike E, Giamarellos-Bourboulis EJ. Macrophage activation-like syndrome: a distinct entity leading to early death in sepsis. Front Immunol. 2019;10:55. doi:10.3389/fimmu.2019.00055
3. Prakash PB, Raj S. Cytokine induced myocardial dysfunction in a patient with hemophagocytic lymphohistiocytosis. J Am Coll Cardiol. 2016;67(13_Supplement):1061. doi:10.1016/S0735-1097(16)31062-2
4. Ravelli A, Minoia F, Davi S, et al. Classification criteria for macrophage activation syndrome complicating systemic juvenile idiopathic arthritis: a European League Against Rheumatism/American College of Rheumatology/Paediatric Rheumatology International Trials Organisation Collaborative Initiative. Ann Rheum Dis. 2016;75(3):481–489. doi:10.1136/annrheumdis-2015-208982
5. Henter JI, Horne A, Arico M, et al. HLH-2004: diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2007;48(2):124–131. doi:10.1002/pbc.21039
6. Grom AA, Mellins ED. Macrophage activation syndrome: advances towards understanding pathogenesis. Curr Opin Rheumatol. 2010;22(5):561–566. doi:10.1097/01.bor.0000381996.69261.71
7. Rőszer T. Understanding the mysterious m2 macrophage through activation markers and effector mechanisms. Mediators Inflamm. 2015;2015:816460. doi:10.1155/2015/816460
8. Kyriazopoulou E, Leventogiannis K, Norrby-Teglund A, et al. Macrophage activation-like syndrome: an immunological entity associated with rapid progression to death in sepsis. BMC Med. 2017;15(1):172. doi:10.1186/s12916-017-0930-5
9. Chizinga M, Kalra SS, Innabi A, Rackauskas M, Ataya A, Emtiazjoo A. Macrophage activating syndrome causing decompensated right heart failure. Respir Med Case Rep. 2021;33:101409. doi:10.1016/j.rmcr.2021.101409
10. Lerkvaleekul B, Vilaiyuk S. Macrophage activation syndrome: early diagnosis is key. Open Access Rheumatol. 2018;10:117–128. doi:10.2147/OARRR.S151013
11. Mehta P, Cron RQ, Hartwell J, Manson JJ, Tattersall RS. Silencing the cytokine storm: the use of intravenous anakinra in haemophagocytic lymphohistiocytosis or macrophage activation syndrome. Lancet Rheumatol. 2020;2(6):e358–e67. doi:10.1016/S2665-9913(20)30096-5
12. Björkman A, Burtscher IM, Svensson PJ, Hillarp A, Besjakov J, Benoni G. Factor V Leiden and the prothrombin 20210A gene mutation and osteonecrosis of the knee. Arch Orthop Trauma Surg. 2005;125(1):51–55. doi:10.1007/s00402-004-0760-8
13. Björkman A, Svensson PJ, Hillarp A, Burtscher IM, Rünow A, Benoni G. Factor V Leiden and prothrombin gene mutation: risk factors for osteonecrosis of the femoral head in adults. Clin Orthop Relat Res. 2004;425:168–172. doi:10.1097/00003086-200408000-00023
14. Zhou JY, Martinez JA, Shen JP. Lamotrigine-induced hemophagocytic lymphohistiocytosis with Takotsubo cardiomyopathy: a case report. Journal of Medical Case Reports. 2019;13(1):345.
15. Otillio JK, Harris JK, Tuuri R. A 6-year-old girl with undiagnosed hemophagocytic lymphohistiocytosis and takotsubo cardiomyopathy: a case report and review of the literature. Pediatr Emerg Care. 2014;30(8):561–565.
16. Takeoka Y, Nakamae M, Nakamae H, et al. Two cases of ampulla (takotsubo-shaped) cardiomyopathy associated with hemophagocytic lymphohistiocytosis. Acta Haematol. 2007;117(4):205–210.
17. Abdin A. Takotsubo Cardiomyopathy Due to Hemophagocytic Lymphohistiocytosis. CHEST. 2016;150(4):435A.
18. Ullah W, Hamid M, Grover H, Figueredo VM, Inayat F. Takotsubo cardiomyopathy secondary to haemophagocytic lymphohistiocytosis in HIV patients: a comprehensive review. BMJ Case Rep. 2019;12(4).
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.