Back to Journals » Research and Reports in Tropical Medicine » Volume 11
Low Knowledge and Attitude Towards Visceral Leishmaniasis Among Migrants and Seasonal Farm Workers in Northwest Ethiopia
Authors Gelaye KA ![]() , Demissie GD
, Demissie GD ![]() , Ayele TA, Wami SD
, Ayele TA, Wami SD ![]() , Sisay MM
, Sisay MM ![]() , Akalu TY
, Akalu TY ![]() , Teshome DF, Wolde HF
, Teshome DF, Wolde HF ![]()
Received 18 October 2020
Accepted for publication 30 November 2020
Published 15 December 2020 Volume 2020:11 Pages 159—168
DOI https://doi.org/10.2147/RRTM.S286212
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Mario Rodríguez-Pérez
Kassahun Alemu Gelaye,1 Getu Debalkie Demissie,2 Tadesse Awoke Ayele,1 Sintayehu Daba Wami,3 Malede Mequanent Sisay,1 Temesgen Yihunie Akalu,1 Destaw Fetene Teshome,1 Haileab Fekadu Wolde1
1Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Health Education and Behavioral Science, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3Department of Environmental and Occupational Health and Safety, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Haileab Fekadu Wolde Email [email protected]
Objective: Ethiopia has the second highest burden of visceral leishmaniasis (VL) next to Sudan. North West Ethiopia alone accounts for 60% of the national burden. Migrant and seasonal farmworkers were the riskiest groups. Good knowledge and attitude on VL is a precursor for successful control of the disease. Therefore, this study was aimed to determine knowledge and attitude towards VL and its associated factors among migrants and seasonal farmworkers in West Gondar zone, Northwest Ethiopia.
Methods: A community-based cross-sectional study was conducted from October to November 2018 in Metema and West Armachiho districts. Two-stage cluster sampling was used to select 950 migrant and seasonal farmworkers. A binary logistic regression model was fitted and variables having a P-value< 0.05 were considered to have a significant association with the outcome variable. Odds ratio (OR) with 95% confidence interval (CI) was used as a measure of association. The goodness of fit test was assessed by Hosmer–Lemeshow test.
Results: Of the total participants, 33.2% (95% CI=30.2– 36.2) and 30.2% (95% CI=27.4– 33.2) were found to have good knowledge and favorable attitude towards VL, respectively. Factors associated with good knowledge include having health information (AOR=3.2, 95% CI=2.3– 4.4), previous history of VL (AOR=6.8, 95% CI=3.7– 12.8), and higher age (AOR=1.58, 95% CI=1.12– 2.23). Moreover, factors associated with favorable attitude include having health information (AOR=2.8, 95% CI=2.0– 3.9), previous history of VL (AOR=2.3, 95% CI=1.3– 4.1), good knowledge (AOR=2.4, 95% CI=1.7– 3.3), and larger number of visits to the farm area (AOR=2.5, 95% CI=1.5– 4.1).
Conclusion: In this study, knowledge and attitude of migrants and seasonal farmworkers towards VL were low. Having health information and previous history of VL had increased the odds of both knowledge and attitude. Tailored interventions for the migrant seasonal farmworkers focusing on knowledge and attitude of VL would be supremely important.
Keywords: attitude, knowledge, VL, migrants and seasonal farmworkers, West Gondar
Introduction
Visceral leishmaniasis (VL) is a sandfly born disease caused by protozoan parasite in genus Leishmania and characterized by fever, splenomegaly, lymphadenopathy, pancytopenia, weakness, and weight loss, and it may end up with death if left untreated.1 Ethiopia is one of the WHO recognized countries which recognize 90% of the global burden of VL, and Ethiopia has the second largest number of VL cases form Sub-Saharan Africa (SSA) next to Sudan.2,3 VL is one of the most neglected and emerging diseases in Ethiopia,4 about 32 million people are estimated to be at risk and one-third of the landmass in northwestern, northeastern, southeastern, and western parts of the country is highly suitable for VL transmission.5
Visceral leishmaniasis is a major public health problem in Metema and West Armachiho districts, where hundreds of thousands of migrant farmworkers migrate for work every year during the planting and harvesting seasons, which is when the majority of the outbreaks occur. Studies have reported that there are 1,000–2,000 human cases of VL in Humera and Metema and the disease rate in northwest Ethiopia accounted for 60% of the national burden.3,6,7 Migration of non-immune migrants and seasonal farmworkers from non-endemic highlands into VL endemic farmlands in the areas is responsible for the higher rate of the disease.8 Likewise, the majority of the migrant farmworkers perform agricultural activities at night time, when the vectors become active, and they also sleep outdoor where appropriate vector control is absent.8–11 They may also be exposed to additional risk factors for the disease, like malnutrition, poor housing condition, and weak immunity.12
The participation of the affected community is very crucial for the implantation of tailored programs for the prevention of many diseases.13 So far, the success of control programs against VL is the most important prerequisite to assess the knowledge, attitude, and practice (KAP) towards VL and its predictors.14 However, few community based attempts have been made to study KAP13–20 but the majority of these studies only focus on the level of KAP without considering the possible predictors. In addition, there is no study that assesses KAP among this highly affected group (migrant farm workers) by disease in Ethiopia.
It is, therefore, this study which mainly aimed to estimate the level of KAP among migrant farmworkers in Metema and West Armachiho and the possible predictors for their knowledge and attitude.
Methods
Study Design and Setting
A community-based crossectional study design was conducted from October to November 2018 among seasonal and migrant farmworkers in Metema and West Armachiho district. In West Armachiho, the average temperature and humidity are 38°C and 78%, respectively, and the daytime temperature is very high from March to May, reaching up to 43°C. Except some mountain tops falling outside, almost all of the lands in this district are in the lowlands and 638 meters above sea level. The second study setting was Metema, located at a latitude and longitude of 12°58′N 36°12′E with an elevation of 685 meters above sea level. Metema is bordered by Sudan in the west, Chilga in the East, Tach Armacho in the Northeast, and West Armacho in the North. These districts are one of the development corridors of the Amhara region as the farms are fertile with a large scale of farming of cash crops like sesame, maize, cotton, and sorghum. As a result, hundred thousands of migrants and seasonal farmworkers travel to these areas to work, especially in the weeding (July to August) and harvesting (September to November) seasons. Both districts are endemic for VL, and migrant workers are the most affected populations.
Sampling Procedure and Sample Size Determination
The sample size was determined using a single population proportion formula with assumptions of 95% CI, 0.05 margin of error, and 5% non-response rate, and a design effect of 2. In addition, a pilot study was conducted among 50 migrant farmworkers in Quara district aimed to estimate the expected proportions of knowledge (41%) and attitude (53%). Then the sample size was 794 and 804 for knowledge and attitude, respectively. The sample size for the predictors was computed using assumptions of power, 80%, 95% CI, odds ratio 1.5–1.8 health information, occupation, and knowledge from previous studies. From this, the largest and final sample size was found to be 976.
Data Collection Procedures and Quality Control
The source population for this study was all seasonal and migrant farmworkers working in west Gondar zone development corridors. The data was collected using a face-to-face interviewer administered structured questionnaire which was developed by the team based on previous literature. The questionnaire comprised socio-demographic, knowledge on VL, attitude towards VL, practice towards prevention of VL, and the health-seeking behavior of respondents towards VL.
Knowledge on VL was assessed using 12 item questions. Each correct answer was given a score of 1, or else scored 0, and the total score ranged between 0–12. Therefore, participants who scored ≥6 were considered as having good knowledge. Attitude towards VL was measured using six items in likert scale questions. The responses for each item were given a score between 1 and 5 by giving a higher score for correct responses, and the total score ranged between 6 and 30. Therefore, participants who scored ≥24 were considered as having a favorable attitude.
The factors assessed were age, sex, original place of residence, religion, marital status, educational status, the main occupation before departure, family size, number of visits, length of stay in the current visit, and income per day. Income was categorized into two based on the median score (120). Low income was defined as a respondent who earns ≤120 birr ($3–4) per day. Ten BSc nurses and four public health professionals (MPH) collected and supervised the data collection process, respectively. Two days of training was given to data collectors and supervisors to keep the data quality. In addition, the filled questionnaires were checked for completeness and consistency daily by the supervisors.
Data Processing and Analysis
Data was entered using Epi Data 3.1 and analyzed using STATA version 14. Data cleaning was done by identifying and correcting missed values and inconsistencies. Descriptive statistics like frequency, percentage, median, and interquartile range (IQR) were done to describe the study population in relation to different variables. Chi-square test was done for all variables to check the assumptions. Multi-collinearity was checked using variance inflation factor (VIF). Binary logistic regression model was fitted, and variables having a P-value ≤0.2 were chosen as a candidate for the final multivariable logistic regression model anda P-value<0.05 in the multivariable model was used to declare a significant association with the outcome variable. Odds ratio with 95% CI was used as a measure of the direction and strength of association. The model goodness of fit was assessed by Hosmer-Lemeshow test.
Ethical Considerations
Ethical clearance was obtained from the ethical committee of University of Gondar and Amhara Public Health Institute. A formal permission letter was obtained from respective health office administrators. The purpose and importance of the study was explained to the participants and, since most of the participants could not read and write, verbal consent was obtained from each participant at and above the age of 18. Consent was also obtained from the heads of the farming area for participants below the age of 18 and this was approved by the ethics review board. Subjects were told that they had the full right not to participate or quit participation at any stage of the study if they wished to. Privacy of the patients was maintained, Names were not included, and questionnaires kept locked. Finally, the study was carried out in accordance with the Helsinki Declaration.
Result
Socio-Demographic Characteristics of the Participants
A total of 950 migrant farmworkers were included with a response rate of 95%. Almost all (943; 99.3%) of the participants were males and the median age was 25 (IQR=20–29) years old. The majority (832; 87.6%) of the seasonal migrant workers came from rural areas, and were Orthodox Christians (932; 98.1%) in religion. More than half (503; 52.9%) of the seasonal migrant workers attended formal education and 649 (68.3) were single by marital status. Regarding their number of visits to the farm area, 772 (81.3%) came for the second or more time and the majority (576; 60.3) of the participants stayed for less than 2 months in the current visit (Table 1).
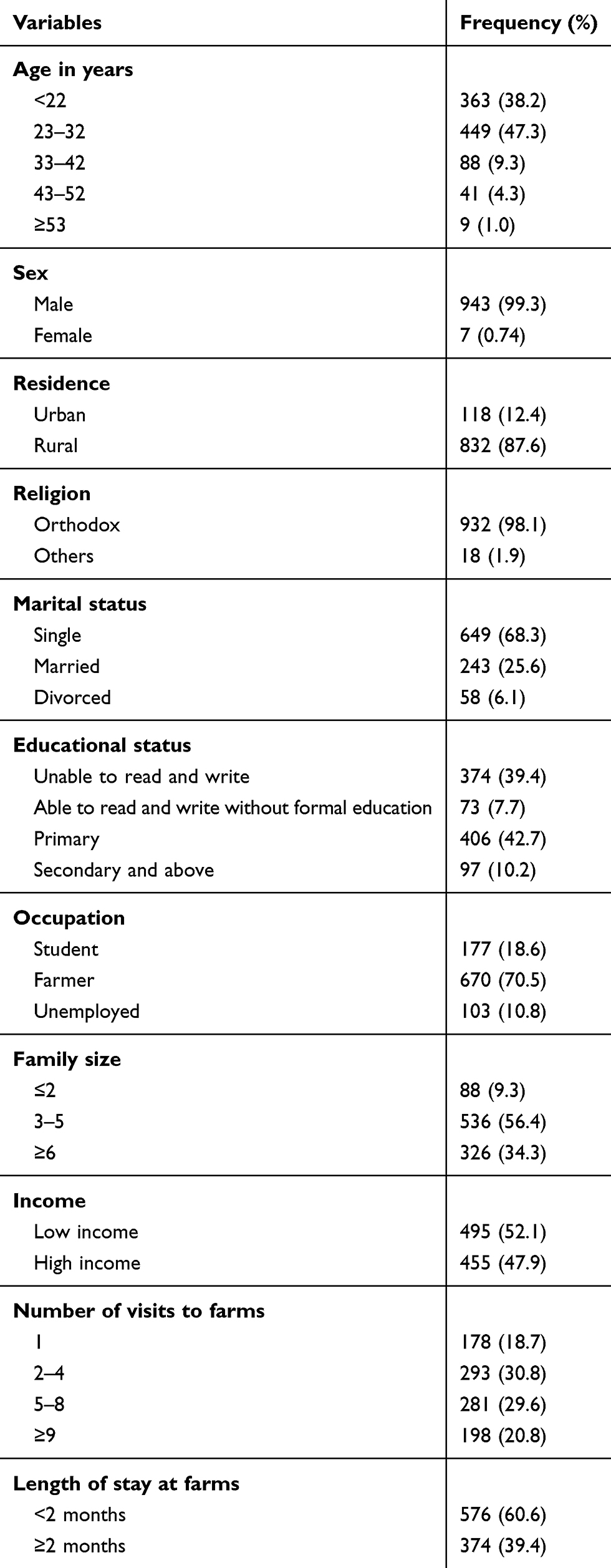 |
Table 1 Socio-Demographic Characteristics of Migrant Farmworkers in North-West Ethiopia, 2018 (n=950) |
Source of Health Information
Of the total 950 participants, 566 (59.6%) had heard about health information. Of these, 328 (58.0%), 509 (90.1%), 270 (47.9%), 90 (16.0%), and 145 (25.71) found the information from mass media, health workers, friends or family, posters, and schools, respectively.
Knowledge on VL Among Study Participants
Among the total participants, 606 (63.8%) knew that VL can be transmitted and 669 (70.4%) mentioned sand fly is a vector involved in a mode of transmission. More than half (495; 52.1%) knew that VL is preventable and 589 (62%) and 689 (73.5%) responded that environmental cleaning and insecticide spraying were ways of prevention, respectively. Concerning the symptoms, 500 (52.6%), 586 (61.7%), and 700 (73.7%) knew abdominal swelling, weight loss, and anemia were the symptoms of VL, respectively. Regarding the overall knowledge, 33.2% (95% CI=30.2–36.2) had a good knowledge on VL (Table 2).
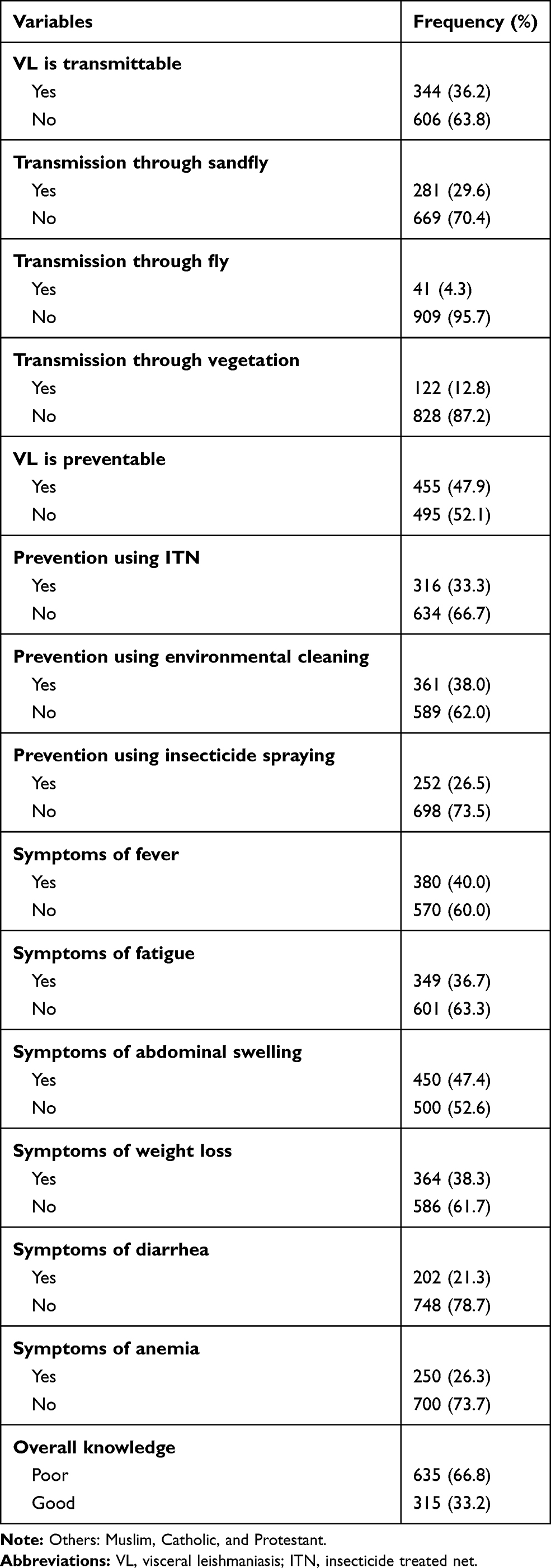 |
Table 2 Knowledge on Visceral Leishmaniasis Among Migrant Farmworkers in North West Ethiopia, 2018 (n=950) |
Attitude Towards VL Among the Study Participants
Of the total respondents, 620 (65.3%) and 593 (62.42%) believed that VL is treatable and the outcome could be death if left untreated. Of all respondents, 393 (41.4%) and 304 (32.0%) believed that VL cannot be transmitted through close contact with an infected person and through bathing, respectively. With regard to the overall attitude, 30.2% (95% CI=27.4–33.2) had a favorable attitude towards VL (Table 3).
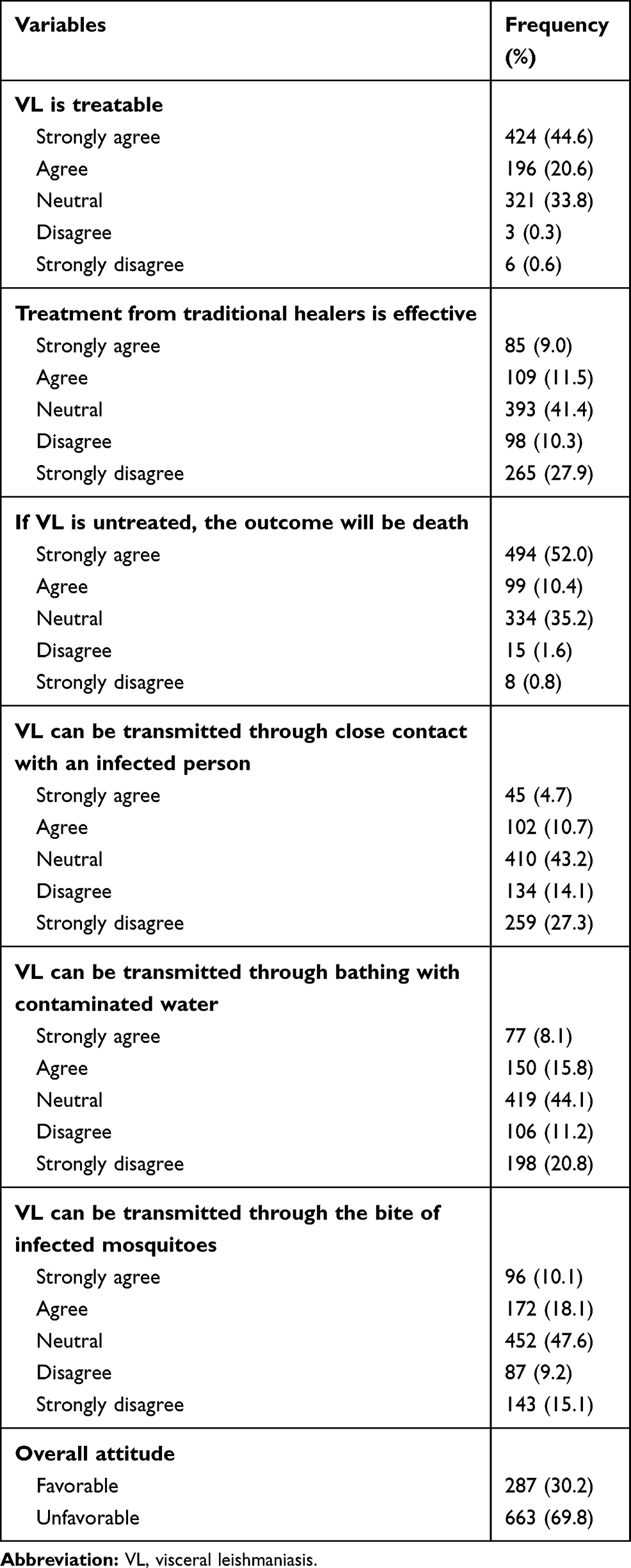 |
Table 3 Attitude Towards VL Among Migrant Farmworkers in North West Ethiopia, 2018 (n=950) |
Practice Towards VL Prevention and Health Seeking Behavior of Study Participants
Among all the participants, 104 (11.0%), 115 (12.11), and 336 (35.4%) used bed net, spray insecticides, and clean their living environment to prevent VL, respectively. However, more than half (565; 59.5%) of the participants did not use any of those methods of prevention. With regard to participants health seeking behavior, only 61 (6.42%) had a history of VL. Among the participants who had a history of VL, 56 (91.8%) sought treatment for the diseases; of these, 51 went to health facilities for treatment while others went to traditional healers, took self treatment with herbal medicine or holy water. In addition, 46 (82.1%) only sought treatment after the disease reached a serious stage.
Factors Associated with Knowledge on VL
In bi-variable logistic regression, knowledge on VL was significantly associated with age, residence, family size, health information, and history of VL. However, in the multivariable model only age, income, health information, and history of VL were found to be significantly associated with good knowledge. The odds of having good knowledge is increased by 58% among participants in the age group of 23–32 years compared with 13–22 (AOR=1.58, 95% CI=1.12–2.23). Respondents who had health information about VL had 3.2-times increased odds of having good knowledge compared to their counterparts (AOR=3.2, 95% CI=2.33–4.44). The odds of having good knowledge was 6.83-times higher among participants who had a history of VL compared to their counterparts (AOR=6.83, 95% CI=3.65–12.77). On the other hand, the odds of good knowledge were decreased by 31% among participants who had high income compared to their counterparts (AOR=0.69, 95% CI=0.51–0.93) (Table 4).
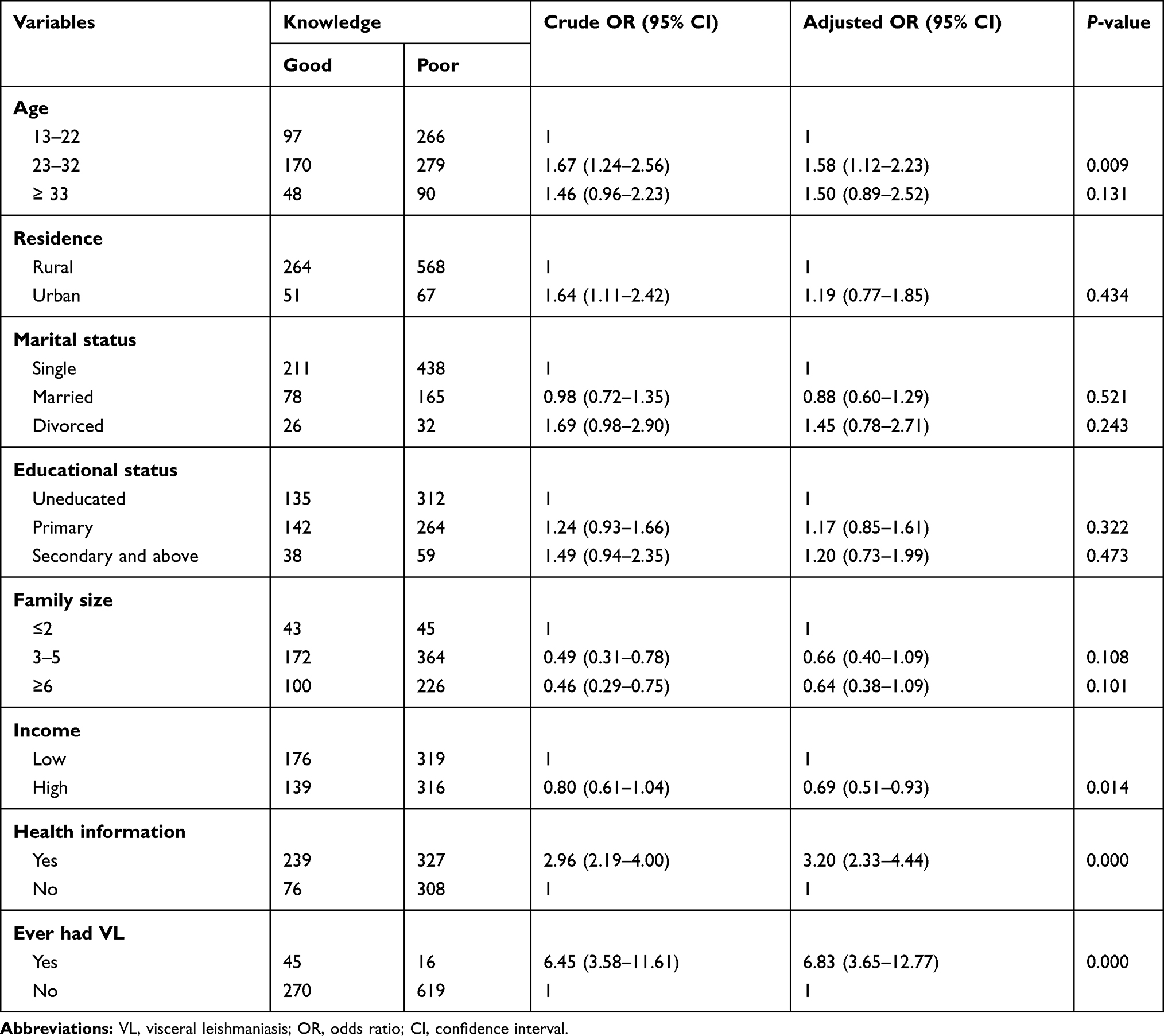 |
Table 4 Multivariable Logistic Regression Output for the Factors Associated with Knowledge on VL Among Migrant Farmworkers in North-West Ethiopia, 2018 (n=950) |
Factors Associated with Attitude Towards VL
From the final multivariable logistic regression model, participants who came to the farm areas nine or more times had 2.50-times increased odds of having a favorable attitude towards VL compared to those who came for the first time (AOR=2.5, 95% CI=1.5–4.1). Participants who had health information about VL had 2.77-times increased odds of having a favorable attitude towards VL compared to their counterparts (AOR=2.8, 95% CI=2.0–3.9). The odds of having a favorable attitude towards VL was 2.30-times (AOR=2.3, 95% CI=1.3–4.1) higher among participants who had a history of VL compared to those who did not. Migrants with a good knowledge on VL had 2.39-times (AOR=2.4, 95% CI=1.7–3.3) increased odds of having a favorable attitude towards VL compared to their counterparts (Table 5).
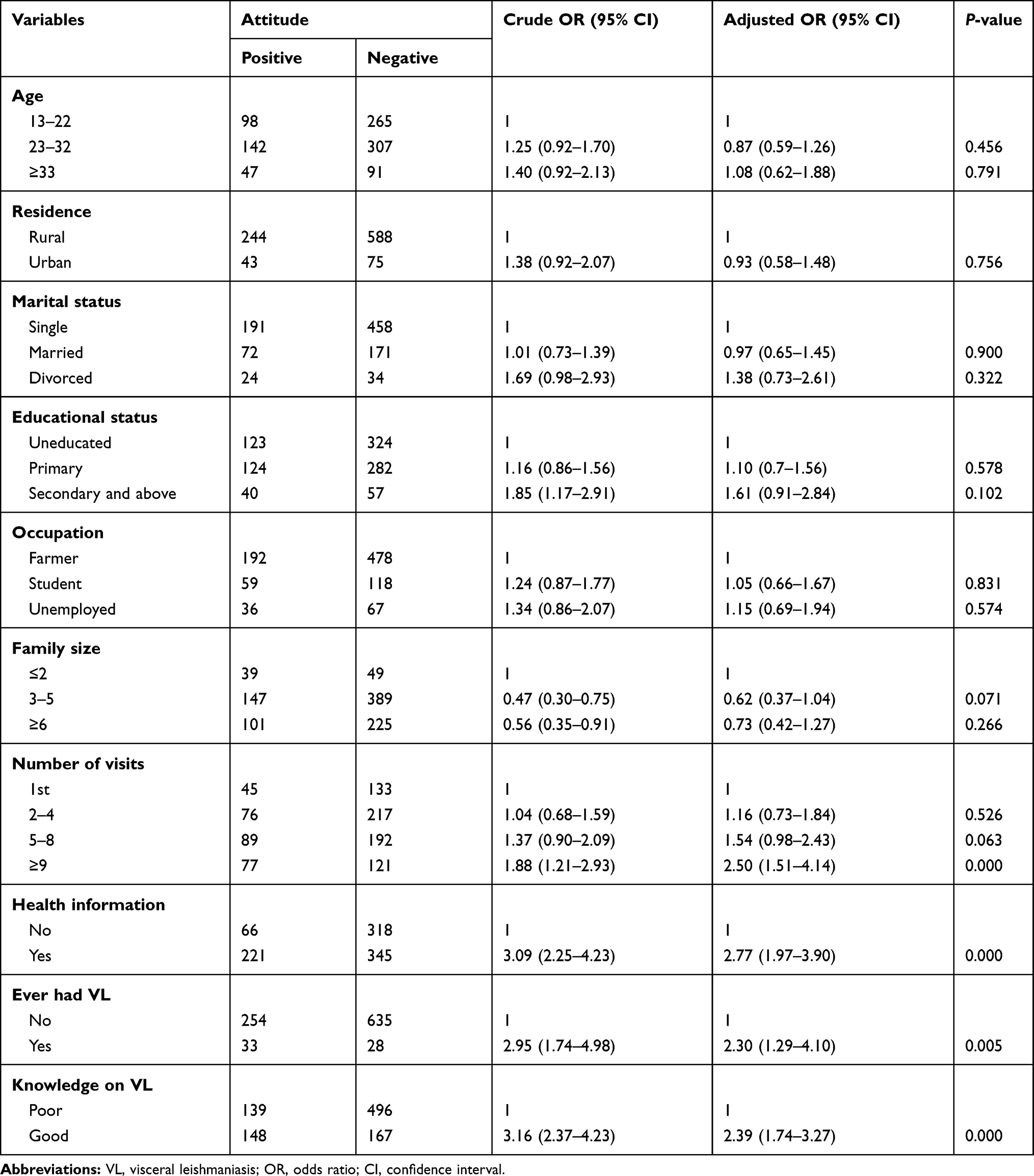 |
Table 5 Multivariable Logistic Regression Output for the Factors Associated with Attitude Towards VL Among Migrant Farmworkers in North-West Ethiopia, 2018 (n=950) |
Discussion
In this study, the overall knowledge, and attitude of the seasonal and migrant farmworkers were found to be low and the majority of the workers did not use any of the methods for prevention of the vector. Age, income, history of VL, and having health information were found to be significant factors of knowledge. In addition, the number of visits to the farm area, history of VL, health information, and knowledge were significantly associated with attitude towards VL.
This study indicates that 33.2% and 30.2% of the participants had good knowledge and a favorable attitude towards VL, respectively. This result was much lower than the finding from a study conducted in Addis Zemen, Ethiopia which showed 89.4% good knowledge and 87.1% favorable attitude towards VL13 and a study conducted in Western Tigray, Ethiopia illustrated that 59% and 95% for a good knowledge and favorable attitude, respectively.3 In addition, the finding is lower than a study conducted in India which showed that 43.9% and 48.6% of respondents had good knowledge and a favorable attitude, respectively.21 This could be due to the difference in the study population because the study in Addis Zemen was conducted among residents of the town, which have better access to mass media and different health information. In addition, the majority (42.4%) of the participants in the Addis Zemen’s study have secondary and above education and the study in West Tigray also included health professionals, which might have a better knowledge and attitude about the disease.3,17 However, in our study only migrant and seasonal farmworkers were included; which have low access to health information and the majority (89.6%) had primary or no education. As a result, migrants and seasonal farmworkers could result in poor knowledge and unfavorable attitude.
Age is significantly affecting the odds of having good knowledge. Adults whose age was 23–32 years were at higher odds of good knowledge than 13–22 years. This finding is in agreement with a study conducted in Paraguay among health professionals and the community which showed an increased odds of having heard about leishmaniasis among higher age groups.22 The possible reason for this could be most migrant farmworkers with higher age groups come to this VL endemic farming areas many times so they may have better information and knowledge about the diseases than younger age groups who came for the first time to the area.3
Having health information about VL was associated with increased odds of good knowledge and attitude. The positive effect of having health information from media, health professionals, schools, and posters has an important role in improving the respondent’s knowledge towards the disease.23–25 Likewise, good knowledge has a significant implication to have a positive attitude towards the diseases.
History of VL was significantly associated with good knowledge and favorable attitude. This finding is concurrent with a longitudinal study from Ethiopia; family’s with a previous history of VL had better overall knowledge.19 This result was also similar with a study conducted in India which showed a positive association between attitude towards VL and previous history of VL.21 This could be attributed to the experience of those patients about the disease symptoms and treatment. In addition, they might also have frequent contact with health professionals and get health education about the disease when they go for treatment, so this may increase their knowledge and attitude towards the diseases.
In this study, participants who had a good knowledge about VL had increased odds of having a favorable attitude. This result was in line with a study conducted in India.21 This finding could be considered as an interesting implication to the public health practice because by only improving the knowledge on the diseases we can enhance favorable attitude and having a favorable attitude can have a big role in enhanced good practice towards prevention control of the disease.
This study estimates the KAP and associated factors among seasonal and migrant farmworkers who are vulnerable to any type of infectious disease. The findings of this study would have a contribution in reducing the burden of diseases among seasonal and migrant farmworkers by improving their knowledge and attitude towards the disease by identifying different public health interventions tailored to migrant and seasonal farmworkers which can increase their knowledge and attitude towards the diseases transmission, prevention, and control.
Limitations of the Study
The study could not establish a cause and effect relationship because of the cross-sectional nature of the study. The study might also be affected by social desirability bias and recall bias, though strong efforts have been made to minimize these biases during data collection.
Conclusion and Recommendations
In this study, the knowledge and attitude of migrants and seasonal farmworkers towards VL were low. Having health information and a previous history of VL had increased the odds of both knowledge and attitude. Tailored interventions for the migrant seasonal farmworkers focusing on knowledge and attitude of VL would be supremely important.
Data Sharing Statement
Data will be available from the corresponding author upon request.
Ethical Consideration
Ethical clearance was obtained from the ethical committee of University of Gondar and Amhara Public Health Institute (Ref No: VP/RCS/05/478/2017). A formal permission letter was obtained by respective health office administrators. The purpose and importance of the study was explained to the participants and since most of the participants couldn’t read and write, verbal consent was obtained from each participant at and above the age of 18. The Consent was also obtained from the heads of the farming area for participants below the age of 18. The verbal informed consent procedure was approved by the ethics board of University of Gondar and Amhara Public Health Institute. Subjects were told that they have full right not to participate or quit participation at any stage of the study if they wish to. Privacy of the patients was maintained, Names were not included, and questionnaires kept locked. Finally, the study was carried out in accordance with the Helsinki Declaration.
Acknowledgments
Firstly, we would like to forward our kindest regards to our study participants. We extend our thanks to data collectors and supervisors without them the report will not be materialized. Last but not least, the authors would forward great thanks to the University of Gondar for financial support.
Author Contributions
KAG, SDW, GDD, and TAA: contributed to the study design, data collection, data analysis, interpretations of the results, and manuscript write-up. HFW, MMS, DFT, TYA: to the study design, data collection, data analysis, interpretations of the results, and manuscript review. All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
All authors declared that they have no conflicts of interest. The abstract of this paper was presented at the 31st EPHA annual conference as a poster presentation. The poster’s abstract can be found at https://www.etpha.org/conference/index.php/31stConference/31stConference/paper/view/2814.
References
1. Chappuis F, Sundar S, Hailu A, et al. Visceral leishmaniasis: what are the needs for diagnosis, treatment and control? Nat Rev Microbiol. 2007;5(11supp):S7. doi:10.1038/nrmicro1748z
2. Organization WH. Investing to Overcome the Global Impact of Neglected Tropical Diseases: Third WHO Report on Neglected Tropical Diseases 2015. World Health Organization; 2015.
3. Berhe M, Bsrat A, Taddele H, et al. Knowledge attitude and practice towards visceral leishmaniasis among residents and health professionals in Welkait District, Western Tigray, Ethiopia. J Trop Dis. 2018;6:257. doi:10.4172/2329-891X.1000257
4. Alvar J, Aparicio P, Aseffa A, et al. The relationship between leishmaniasis and AIDS: the second 10 years. Clin Microbiol Rev. 2008;21(2):334–359. doi:10.1128/CMR.00061-07
5. Tsegaw T, Gadisa E, Seid A, et al. Identification of environmental parameters and risk mapping of visceral leishmaniasis in Ethiopia by using geographical information systems and a statistical approach. Geospat Health. 2013;7(2):299–308. doi:10.4081/gh.2013.88
6. Ayehu A, Aschale Y, Lemma W, et al. Seroprevalence of asymptomatic leishmania donovani among laborers and associated risk factors in agricultural camps of West Armachiho District, Northwest Ethiopia: a cross-sectional study. J Parasitol Res. 2018;2018.
7. Kassahun A, Sadlova J, Dvorak V, et al. Detection of Leishmania donovani and L. tropica in Ethiopian wild rodents. Acta Trop. 2015;145:39–44. doi:10.1016/j.actatropica.2015.02.006
8. Leta S, Dao THT, Mesele F, et al. Visceral leishmaniasis in Ethiopia: an evolving disease. PLoS Negl Trop Dis. 2014;8(9):e3131. doi:10.1371/journal.pntd.0003131
9. Argaw D, Mulugeta A, Herrero M, et al. Risk factors for visceral leishmaniasis among residents and migrants in Kafta-Humera, Ethiopia. PLoS Negl Trop Dis. 2013;7(11):e2543. doi:10.1371/journal.pntd.0002543
10. Bashaye S, Nombela N, Argaw D, et al. Risk factors for visceral leishmaniasis in a new epidemic site in Amhara Region, Ethiopia. Am J Trop Med Hyg. 2009;81(1):34–39. doi:10.4269/ajtmh.2009.81.34
11. Aschale Y, Ayehu A, Worku L, et al. Malaria-visceral leishmaniasis co-infection and associated factors among migrant laborers in West Armachiho district, North West Ethiopia: community based cross-sectional study. BMC Infect Dis. 2019;19(1):239. doi:10.1186/s12879-019-3865-y
12. Gebremichael Tedla D, Bariagabr FH, Abreha HH. Incidence and trends of leishmaniasis and its risk factors in Humera, Western Tigray. J Parasitol Res. 2018;2018:1–9. doi:10.1155/2018/8463097
13. Alemu A, Alemu A, Esmael N, et al. Knowledge, attitude and practices related to visceral leishmaniasis among residents in Addis Zemen town, South Gondar, Northwest Ethiopia. BMC Public Health. 2013;13:382. doi:10.1186/1471-2458-13-382
14. Siddiqui N, Kumar N, Ranjan A, et al. Awareness about kala-azar disease and related preventive attitudes and practices in a highly endemic rural area of India. Southeast Asian J Trop Med Public Health. 2010;41(1):1.
15. Mondal D, Singh SP, Kumar N, et al. Visceral leishmaniasis elimination programme in India, Bangladesh, and Nepal: reshaping the case finding/case management strategy. PLoS Negl Trop Dis. 2009;3(1):e355. doi:10.1371/journal.pntd.0000355
16. Ahluwalia IB, Bern C, Costa C, et al. Visceral leishmaniasis: consequences of a neglected disease in a Bangladeshi community. Am J Trop Med Hyg. 2003;69(6):624–628. doi:10.4269/ajtmh.2003.69.624
17. de Amorim CF, Santos Albano Amora S, Kazimoto TA, et al. Knowledge of the population about visceral leishmaniasis transmission in endemic areas near the banks of the Mossoro River in northeastern Brazil. Int J Environ Res Public Health. 2015;12(3):3343–3357. doi:10.3390/ijerph120303343
18. Koirala S, Parija SC, Karki P, et al. Knowledge, attitudes, and practices about kala-azar and its sandfly vector in rural communities of Nepal. Bull World Health Organ. 1998;76(5):485–490.
19. Lopez-Perea N, Sordo L, Gadisa E, et al. Knowledge, attitudes and practices related to visceral leishmaniasis in rural communities of Amhara State: a longitudinal study in northwest Ethiopia. PLoS Negl Trop Dis. 2014;8(4):e2799. doi:10.1371/journal.pntd.0002799
20. Srinivasan R, Ahmad T, Raghavan V, et al. Positive influence of behavior change communication on knowledge, attitudes, and practices for visceral Leishmaniasis/Kala-azar in India. Glob Health Sci Pract. 2018;6(1):192–209. doi:10.9745/GHSP-D-17-00087
21. Govil D, Sahoo H, Pedgaonkar SP, et al. Assessing knowledge, attitudes, and preventive practices related to Kala-A: a study of rural Madhepura, Bihar, India. Am J Trop Med Hyg. 2018;98(3):857–863. doi:10.4269/ajtmh.16-0978
22. Ruoti M, Oddone R, Lampert N, et al. Mucocutaneous leishmaniasis: knowledge, attitudes, and practices among paraguayan communities, patients, and health professionals. J Trop Med. 2013;2013:1–10. doi:10.1155/2013/538629
23. Koirala S, Parija S, Karki P, et al. Knowledge, attitudes, and practices about kala-azar and its sandfly vector in rural communities of Nepal. Bull World Health Organ. 1998;76(5):485.
24. Sarkari B, Qasem A, Shafaf MR. Knowledge, attitude, and practices related to cutaneous leishmaniasis in an endemic focus of cutaneous leishmaniasis, Southern Iran. Asian Pac J Trop Biomed. 2014;4(7):566–569. doi:10.12980/APJTB.4.2014C744
25. Wang M, Han X, Fang H, et al. Impact of health education on knowledge and behaviors toward infectious diseases among students in Gansu Province, China. Biomed Res Int. 2018;2018.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.