Back to Journals » International Medical Case Reports Journal » Volume 19
Low-Grade Appendiceal Mucinous Neoplasm Presenting as Small Intestine Obstruction Due to Internal Hernia: A Case Report
Authors Karrabi AM ![]() , Tavasolizadeh M
, Tavasolizadeh M
Received 8 November 2025
Accepted for publication 15 February 2026
Published 18 February 2026 Volume 2026:19 579236
DOI https://doi.org/10.2147/IMCRJ.S579236
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Amir Mohammad Karrabi,1 Morteza Tavasolizadeh2
1Student Research Committee, Sabzevar University of Medical Sciences, Sabzevar, Iran; 2Department of General Surgery, Shahid Beheshti Hospital, Sabzevar University of Medical Sciences, Sabzevar, Iran
Correspondence: Morteza Tavasolizadeh, Department of General Surgery, Shahid Beheshti Hospital, Sabzevar University of Medical Sciences, Sabzevar, Iran, Tel +989159369030, Email [email protected]
Background: Appendiceal mucinous neoplasms (AMNs) are rare tumors that are often discovered incidentally and may present with non-specific symptoms such as abdominal pain, ascites, or features mimicking appendicitis.
Case Presentation: A 72-year-old male presented with small intestine obstruction secondary to an internal hernia. CT scan imaging initially suggested adhesive bands; however, surgical exploration revealed an inflamed, tumor-bearing appendix tip adherent to the mesentery, forming a hernia orifice that trapped a loop of small intestine. The patient underwent appendectomy, mesenteric mass resection, and hernia repair. Histopathology confirmed a low-grade appendiceal mucinous neoplasm (LAMN) with mucinous invasion of the mesentery, explaining the mass formation and mechanism of herniation.
Conclusion: This case illustrates that a locally invasive LAMN, even in the absence of peritoneal dissemination, can act as a lead point for an internal hernia and should be considered in the differential diagnosis of bowel obstruction and internal hernia, particularly in elderly patients.
Keywords: appendiceal mucinous neoplasms, AMNs, intestinal obstruction, internal hernia, surgery
Introduction
Appendiceal mucinous neoplasms (AMNs) are considered one of the most common primary epithelial neoplasms of the appendix and comprise a heterogeneous group of diagnostically challenging neoplasms.1,2 AMNs are often asymptomatic or presenting with nonspecific or appendicitis-like symptoms and usually discovered incidentally during surgical procedures.1,3 Their manifestation as a lead point for an internal hernia is unexpected.4
An internal hernia, a protrusion of abdominal viscera, typically the small intestine, through congenital or acquired peritoneal apertures, is a rare but serious etiology of intestinal obstruction.5,6 Due to asymptomatic patients or non-specific and vague symptoms, including abdominal pain, nausea, vomiting, distention, and constipation, Clinical diagnosis is considered very challenging.6,7 The computed tomography (CT) scan is considered the first-line and most frequent imaging technique for diagnosing internal hernia.8 The presentation of an appendiceal tumor causing intestinal obstruction and internal hernia is highly uncommon;4 nevertheless, it should be included in the differential diagnosis to ensure accurate clinical management.
In this case report, we describe a 71-year-old patient who presented with an unusual cause of intestinal obstruction, an internal hernia, followed by a low-grade appendiceal mucinous neoplasm (LAMN) located at the appendix tip. This rare manifestation highlights the critical importance of a thorough diagnostic evaluation to identify uncommon predisposing factors for common surgical presentations.
Case Presentation
A 72-year-old male presented to the emergency department with a 4-day history of intermittent abdominal pain, accompanied by nausea, vomiting, and anorexia. He additionally mentioned the absence of defecation and gas passing since the abdominal pain started. The patient reported no prior medical history and no family history suggestive of any related medical conditions, including gastrointestinal cancer and inflammatory bowel syndrome (IBS). He also denied a history of previous abdominal surgery. Physical examination revealed a soft abdomen with evidence of abdominal distension. Mild periumbilical tenderness was noted without any signs of rebound tenderness or guarding. An abdominopelvic CT scan with both oral and intravenous contrast administration, along with aortic CT angiography, was requested for further investigations. A small amount of free intraperitoneal fluid was observed, accompanied by dilatation of small bowel loops containing air–fluid levels, with a maximal diameter of 35 mm, suggesting small bowel obstruction in the context of possible adhesive bands (Figure 1). On surgical exploration, the intraoperative findings confirmed the radiological assessment; the small intestine was markedly dilated up to near the ileocecal valve, while the colon appeared collapsed. The appendix was seen inflamed with a mass which was located at its tip and adherent to the mesentery of the small intestine (Figure 2A). This condition created an internal herniation of the small intestine through the appendix mass. The herniated bowel was found to be ischemic but had not progressed to gangrene (Figure 2B). A mesenteric release with appendectomy and internal hernia repair of the small intestine was performed along with other necessary reconstructive procedures. The appendix and a mesenteric mass (Figure 2C)—initially presumed to be a lymph node—were submitted for pathological analysis. Histopathology revealed a margin-free low-grade appendix mucinous neoplasm (LAMN) with serosal involvement (pT4a) along with acute appendicitis and peritonitis, and no mitotic activity (Figure 3). The mass previously identified as a lymph node was determined to be an acellular mucin accommodation with mesothelial hyperplasia, rather than nodal tissue, which is confirming local extension and invasion of the LAMN into the adjacent mesenteric fat. Crucially, there was no evidence of tumor cells or mucin dissemination into the free peritoneal cavity (Figure 4). As the mucinous tumor exhibited no evidence of peritoneal dissemination, secondary surgical interventions and hyperthermic intraperitoneal chemotherapy (HIPEC) were not indicated. The patient was followed up at 6 months postoperatively; he did not report any abdominal pain, weight loss, fatigue, or bowel symptoms with an unremarkable physical examination.
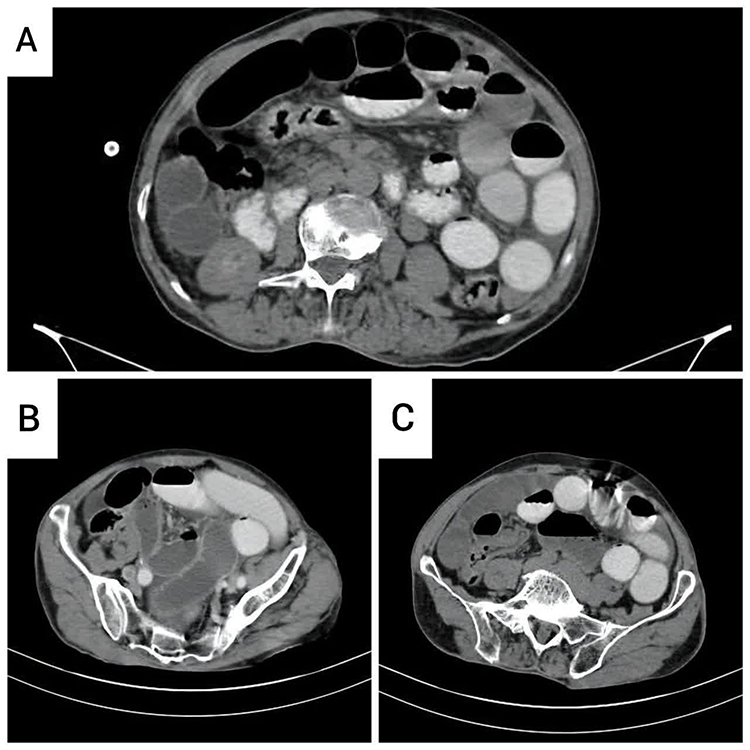 |
Figure 1 Abdominopelvic Computed Tomography (CT scan); (A) dilation of small intestine loops containing air–fluid levels indicating intestinal obstruction; (B) Adhesion of small intestine loops to the pelvic wall and fluid accumulation in the peritoneal space; (C) Twisted appendix and mass at its tip. |
 |
Figure 2 Intraoperative view: (A) inflamed and tumor-containing appendix, creating an obstructive loop; (B) bowel ischemia due to internal herniation; (C) mesenteric mucinous mass. |
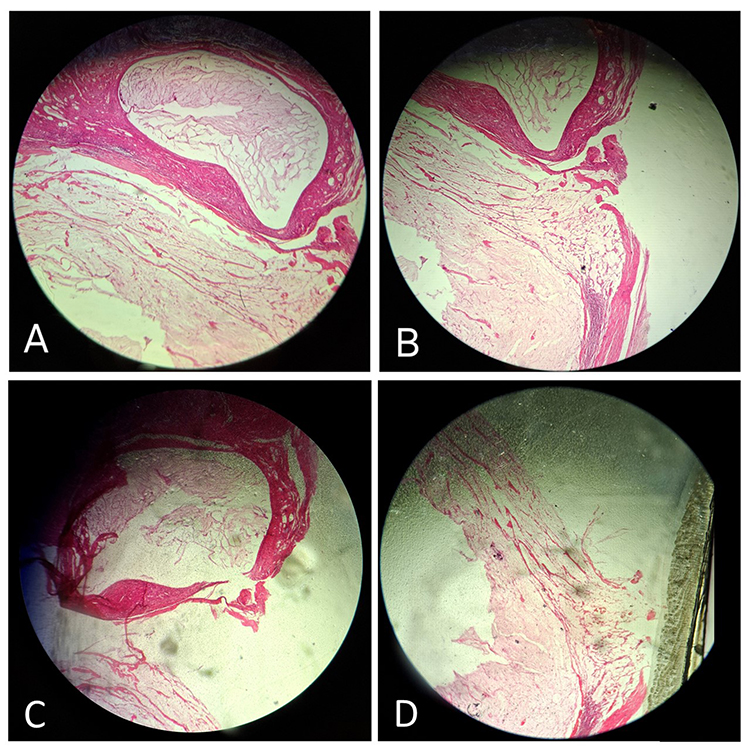 |
Figure 3 Histology of the appendix tumor; H&E staining; 40X magnification: (A) pool of mucin containing inflammatory cells accompanied by rare bland cells invades muscularis propria; (B and C) perforation and serosal involvement; (D) Mucinous deposits outside the appendiceal lumen confirm transmural invasion of the tumor. |
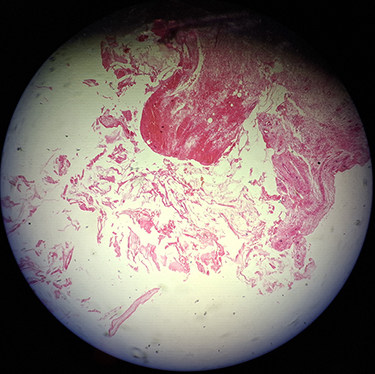 |
Figure 4 Histology of a mesenteric nodal mass; H&E staining; 40X magnification; acellular mucin accommodation with mesothelial hyperplasia. |
Discussion
AMNs are rare epithelial tumors, accounting for less than 1% of all gastrointestinal malignancies. They are often discovered incidentally, among appendectomy specimens. When symptoms do occur, they typically mimic acute appendicitis9,10 or manifest latently as ascites, abdominal pain, weight loss, anemia, or even hernia formation.9 In our case, the tumor presentation was atypical, as the tumor initially manifested with features of small intestine obstruction secondary to an internal herniation.
According to the WHO criteria (2019), appendiceal mucinous neoplasms are categorized as low-grade appendiceal mucinous neoplasm (LAMN), high-grade appendiceal mucinous neoplasm (HAMN), and mucinous adenocarcinoma, defined by the absence or presence of infiltrative invasion.11 LAMNs typically present as a dilated and mucin-filled appendix with wall calcification.10 Histopathologically, LAMNs are characterized by low-grade cytological atypia, usually with a monolayer of mucin-producing epithelial cells, hyperchromatic nuclei, and a low nuclear-to-cytoplasmic ratio due to intracellular mucin accumulations. Mitotic activity is uncommon, and invasion usually follows a “pushing” pattern rather than the destructive invasion growth seen in mucinous adenocarcinomas.10,12,13 In our patient, histopathology confirmed these classic features, with a LAMN located at the tip of the appendix demonstrating a low-grade nearby local mesenteric invasion. This direct mesenteric involvement explains the mechanism of internal herniation observed in our case, where the inflamed, mass-forming appendix created an obstructive loop leading to small intestine herniation.
Imaging plays a crucial role in the evaluation and management of AMNs as it aids in characterizing the lesion, assessing invasion, and identifying potential comorbidities. Multidetector computed tomography (MDCT) is considered the most accurate modality for evaluating AMNs. Mucoceles can be visualized as a cystic mass with variable calcification in the wall. Also, the presence of mural irregularity or soft tissue mass greater than 1.5 mm raises suspicion for mucinous neoplasia. In this imaging modality, the presence of any extra-appendiceal mucin deposition is considered a sign of LAMN or mucinous adenocarcinoma rather than an adenomatous process.1,14 Magnetic resonance imaging (MRI) can provide complementary information, particularly in differentiating mucinous tumors from other peritoneal pathologies, whereas ultrasonography may demonstrate the “onion-skin” sign of mucin accumulation. Plain radiography with or without a barium enema is also used; however, it provides negligible information.1 In our case, a contrast-enhanced abdominopelvic CT scan was performed. Imaging revealed dilated bowel loops with air–fluid levels and a small volume of free peritoneal fluid, but no obvious appendiceal mass was identified at first. This emphasizes the challenge of radiologic diagnosis when AMNs present atypically, as in our patient.
AMNs’ Management requires a multidisciplinary approach due to their heterogeneity in biological behavior. In the early stage, a simple appendectomy is generally sufficient for low-risk lesions, whereas right hemicolectomy may be indicated for larger tumors. For advanced cases with evidence of peritoneal dissemination, cytoreductive surgery is recommended, combined with adjuvant chemotherapy for lymph node involvement. In addition, HIPEC involves destroying any remaining cancer cells by the injection of chemotherapy drugs into the peritoneal cavity after surgery.9,15,16 Our patient underwent an appendectomy with resection of the adherent local mesenteric mass, and internal hernia repair was performed, which was appropriate given the localized nature of the disease. There was no radiological or surgical evidence of peritoneal carcinomatosis or pseudomyxoma peritonei. Therefore, extensive surgery or HIPEC was not indicated.
Conclusion
This case highlights a very rare presentation of LAMN manifesting as small intestine obstruction followed by internal herniation. Surgical exploration not only confirmed the underlying etiology but also enabled definitive treatment through appendectomy, mesenteric mass excision, and hernia repair. This presentation highlights that appendiceal neoplasms must be considered in the differential diagnosis of bowel obstruction, particularly when no common cause is identified.
Abbreviations
AMN, Appendiceal Mucinous Neoplasm; CT, Computed Tomography; HIPEC, Hyperthermic Intraperitoneal Chemotherapy; LAMN, Low-Grade Appendiceal Mucinous Neoplasm; MDCT, Multidetector Computed Tomography; MRI, Magnetic Resonance Imaging.
Data Sharing Statement
All data supporting the findings of this study are included within the article. Additional details related to the patient’s anonymized clinical or histopathological data are available from the corresponding author upon reasonable request.
Ethical Consideration
Ethical approval for the publication of this case report, including patient details and images, was obtained from the Ethical Committee of Sabzevar University of Medical Sciences, Sabzevar, Iran (reference number: IR.MEDSAB.REC.1404.152). Written informed consent was obtained from the patient and his son prior to submission.
Consent for Publication
Written informed consent was obtained from the patient and his son for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Acknowledgment
The authors would like to thank the staff of Shahid Beheshti Hospital for their support and collaboration in preparing this case report.
Funding
Sabzevar University of Medical Sciences has supported this study.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Tirumani SH, Fraser-Hill M, Auer R, et al. Mucinous neoplasms of the appendix: a current comprehensive clinicopathologic and imaging review. Cancer Imaging. 2013;13(1):14–6. doi:10.1102/1470-7330.2013.0003
2. Matias-García B, Mendoza-Moreno F, Blasco-Martínez A, Busteros-Moraza JI, Diez-Alonso M, Garcia-Moreno Nisa F. A retrospective analysis and literature review of neoplastic appendiceal mucinous lesions. BMC Surgery. 2021;21(1):79. doi:10.1186/s12893-021-01091-9
3. Chang H-C, Kang J-C, Pu T-W, Su R-Y, Chen C-Y, Hu J-M. Mucinous neoplasm of the appendix: a case report and review of literature. World J Gastrointest Surg. 2024;16(3):944. doi:10.4240/wjgs.v16.i3.944
4. Ye M, Bai B, Lu L, Xiang D, Li Z. Appendiceal mucinous cystadenoma presenting as abdominal internal hernia: a case report. Transl Cancer Res. 2019;8(7):2667–2671. doi:10.21037/tcr.2019.10.10
5. Husain A, Bhat S, Roy AK, Sharma V, Dubey SA, Faridi MS. Internal hernia through paraduodenal recess with acute intestinal obstruction: a case report. Indian J Surg. 2012;74(4):354–355. doi:10.1007/s12262-011-0243-4
6. Martin LC, Merkle EM, Thompson WM. Review of internal hernias: radiographic and clinical findings. Am J Roentgenol. 2006;186(3):703–717. doi:10.2214/AJR.05.0644
7. Salar O, El-Sharkawy A, Singh R, Speake W. Internal hernias: a brief review. Hernia. 2013;17(3):373–377. doi:10.1007/s10029-012-1023-1
8. Lanzetta MM, Masserelli A, Addeo G, et al. Internal hernias: a difficult diagnostic challenge. review of CT signs and clinical findings. Acta Biomed. 2019;90(5–s):20–37. doi:10.23750/abm.v90i5-S.8344
9. Shaib WL, Assi R, Shamseddine A, et al. Appendiceal mucinous neoplasms: diagnosis and management. Oncologist. 2017;22(9):1107–1116. doi:10.1634/theoncologist.2017-0081
10. Carr NJ, Bibeau F, Bradley RF, et al. The histopathological classification, diagnosis and differential diagnosis of mucinous appendiceal neoplasms, appendiceal adenocarcinomas and pseudomyxoma peritonei. Histopathology. 2017;71(6):847–858. doi:10.1111/his.13324
11. Assarzadegan N, Montgomery E. What is new in the 2019 World Health Organization (WHO) classification of tumors of the digestive system: review of selected updates on neuroendocrine neoplasms, appendiceal tumors, and molecular testing. Arch Pathol Lab Med. 2021;145(6):664–677. doi:10.5858/arpa.2019-0665-RA
12. González Bayón L, Martín Román L, Lominchar PL. Appendiceal mucinous neoplasms: from clinic to pathology and prognosis. Cancers. 2023;15(13):3426. doi:10.3390/cancers15133426
13. Gündoğar Ö, Kımıloğlu E, Komut N, et al. Evaluation of appendiceal mucinous neoplasms with a new classification system and literature review. Turk J Gastroenterol. 2018;29(5):532. doi:10.5152/tjg.2018.17605
14. Van Hooser A, Williams TR, Myers DT. Mucinous appendiceal neoplasms: pathologic classification, clinical implications, imaging spectrum and mimics. Abdom Radiol. 2018;43(11):2913–2922. doi:10.1007/s00261-018-1561-9
15. Gündoğar Ö, Kımıloğlu E, Komut N, et al. Evaluation of appendiceal mucinous neoplasms with a new classification system and literature review. Turk J Gastroenterol. 2018;29(5):533–542.
16. Rymer B, Forsythe RO, Husada G. Mucocoele and mucinous tumours of the appendix: a review of the literature. Int J Surg. 2015;18:132–135. doi:10.1016/j.ijsu.2015.04.052
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.