Back to Journals » International Medical Case Reports Journal » Volume 19
Low-Grade Appendiceal Mucinous Neoplasm (LAMN) Presenting Acutely: A Case Report and Concise Review of Surgical Decision-Making
Authors Eghbali M, Gohari M, Mohebbi R ![]()
Received 6 September 2025
Accepted for publication 21 May 2026
Published 27 May 2026 Volume 2026:19 565810
DOI https://doi.org/10.2147/IMCRJ.S565810
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Mohammad Eghbali,1 Mohaddese Gohari,2 Reza Mohebbi3
1Department of Nursing, School of Nursing and Midwifery, Torbat Heydariyeh University of Medical Sciences, Torbat Heydariyeh, Iran; 2Student Research Committee, Torbat Heydariyeh University of Medical Sciences, Torbat Heydariyeh, Iran; 3Department of Operating Room, School of Nursing and Midwifery, Torbat Heydariyeh University of Medical Sciences, Torbat Heydariyeh, Iran
Correspondence: Reza Mohebbi, School of Nursing and Midwifery, Torbat Heydariyeh University of Medical Sciences, Torbat Heydariyeh, Iran, Email [email protected]
Abstract: The optimal surgical management of Low-Grade Appendiceal Mucinous Neoplasm (LAMN) remains nuanced, requiring a balance between recurrence risk and operative morbidity. Although right hemicolectomy is frequently recommended, accumulating evidence suggests that simple appendectomy is adequate in well-defined circumstances. We report the case of a 52-year-old man with common cardiac comorbidities who presented with symptoms resembling acute appendicitis and was found to have a 10 cm LAMN. Given the intraoperative findings an intact appendix, a healthy appendiceal base, and absence of extra-appendiceal mucin simple appendectomy was performed with curative outcome. Using this case as an anchor, we provide a concise and practical synthesis of the key intraoperative and pathological criteria that can assist surgeons in confidently selecting appendectomy over hemicolectomy in appropriately selected patients. Our objective is to offer a clear, actionable framework for surgical decision-making in the management of LAMN.
Keywords: appendiceal mucocele, low-grade appendiceal mucinous neoplasm, LAMN, case report, appendectomy, surgical decision-making
Introduction
Appendiceal mucoceles are rare cystic lesions of the appendix, with Low-Grade Appendiceal Mucinous Neoplasm (LAMN) representing a common pathological subtype. The primary clinical significance of LAMN lies in its potential, if ruptured, to lead to pseudomyxoma peritonei (PMP), a devastating condition. Therefore, the cornerstone of management is complete surgical resection without spillage.1–4
The choice of surgical procedure remains a subject of debate. While right hemicolectomy is traditionally recommended for many mucinous neoplasms, simple appendectomy may be sufficient for LAMNs confined to the appendix. This decision is critically important when balancing oncologic safety against operative morbidity.5
We present a case of a giant LAMN presenting acutely. This report highlights the critical importance of a tailored surgical strategy. We demonstrate that a simple appendectomy, guided by stringent intraoperative findings, can be curative. This approach avoids the unnecessary risks of a more extensive operation in selected patients.
Case Presentation
Patient History
A 52-year-old man presented to the emergency department with a 2-day history of right lower quadrant abdominal pain, accompanied by nausea, vomiting, and anorexia. Physical examination revealed tenderness in the right lower quadrant. His medical history included controlled hypertension and a stable right bundle branch block (RBBB), for which he was under routine follow-up and medical therapy. He was also a tobacco user, representing an additional perioperative risk factor (Table 1).
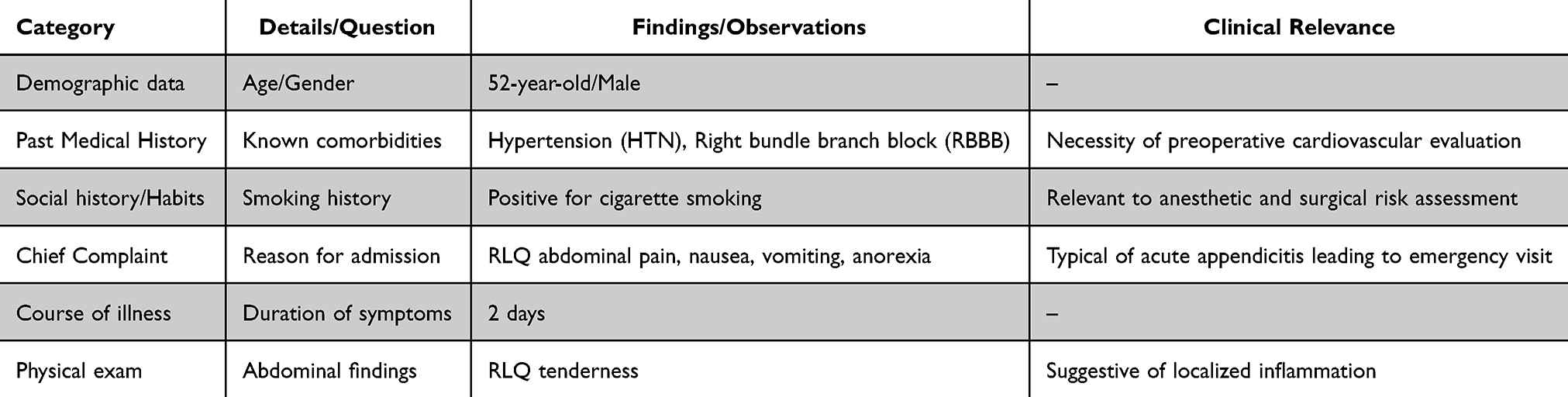 |
Table 1 Clinical Findings at Presentation |
Laboratory Findings
Neutrophilia: 81.3% (normal range: 40–75%) Lymphocytopenia: 16.0% (normal range: 20–45%) Urinalysis: abundant mucus Serum urea, creatinine, sodium, and potassium: within normal limits (Table 2).
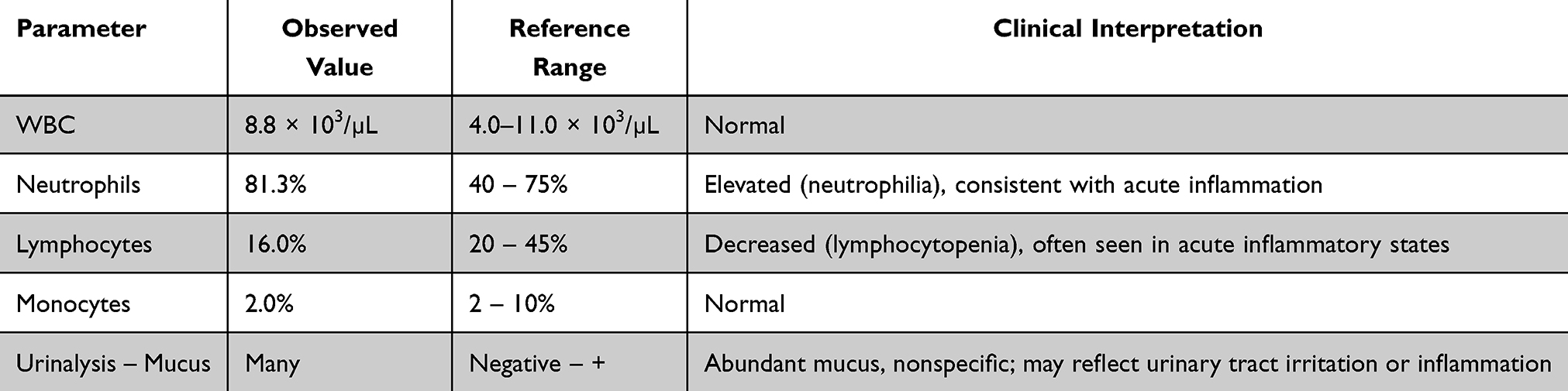 |
Table 2 Laboratory Findings |
Imaging Studies
Ultrasound: Well-defined hypoechoic tubular mass in the right lower quadrant, 39×30 × 106 mm, with no vascular flow on Doppler. Contrast-enhanced CT: Tubular, blind-ending lesion with smooth walls, 100×30 mm, no peri-lesional inflammation or adhesion (Table 3).
 |
Table 3 Imaging Findings |
Surgical Intervention
Following appropriate preoperative preparation, the patient underwent laparotomy via a right lower quadrant incision. Intraoperative findings included a markedly distended cystic appendix consistent with appendiceal mucocele. The appendix was carefully dissected without injury to the wall or spillage of mucinous contents. A stapled appendectomy was performed with negative margins. No perforation, mucin spillage, or peritoneal carcinomatosis was observed (Figure 1).
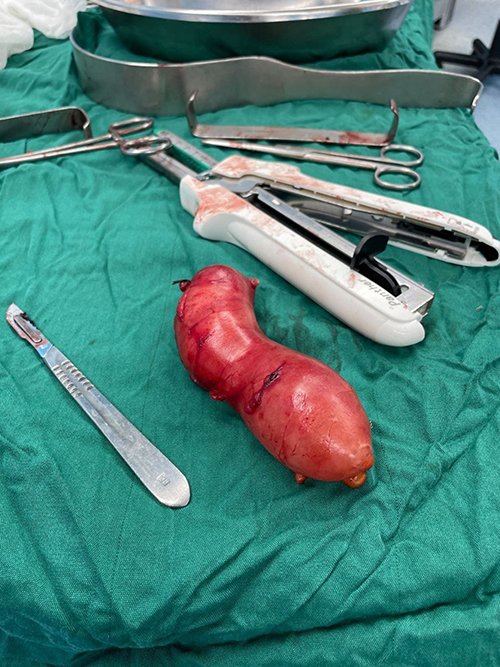 |
Figure 1 Gross specimen of the resected appendix showing cystic dilatation with mucinous content, consistent with low-grade appendiceal mucinous neoplasm (LAMN). |
Pathology
Gross: Appendix 12 cm × 4 cm, lumen filled with mucinous material, dull brown serosal surface. Microscopy: Flat proliferation of mucinous epithelial cells with low-grade nuclear atypia, consistent with LAMN. No mural invasion, negative margins, and no extra-appendiceal mucin. Coexisting acute appendicitis and periappendicitis were also noted (Table 4).
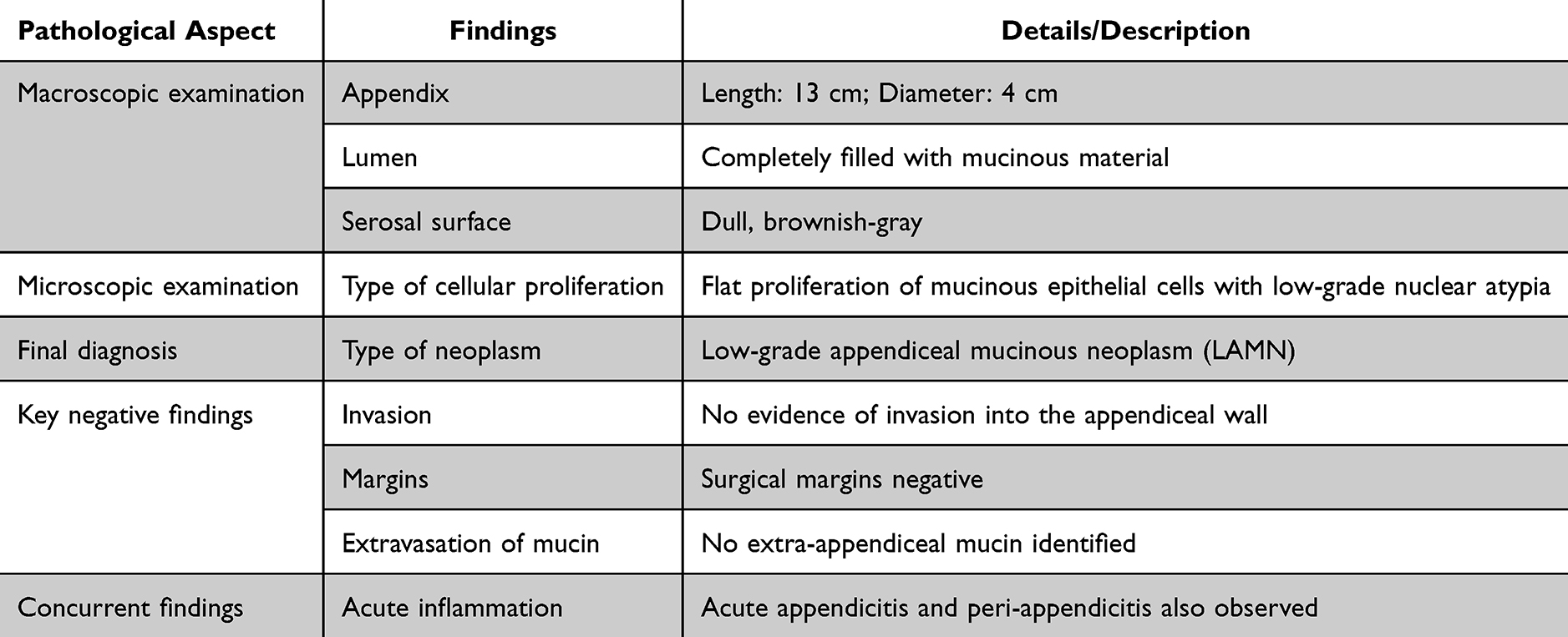 |
Table 4 Pathological Findings |
Outcome and Follow-Up
The patient was discharged in good condition two days postoperatively. Standard follow-up was advised based on pathology and surgical findings. At 4 months, no postoperative complications were observed.
Discussion
Low-grade appendiceal mucinous neoplasms (LAMNs) represent a rare but clinically significant subset of appendiceal tumors, with management strategies that continue to evolve. Although LAMNs are frequently discovered incidentally and may remain asymptomatic for long periods, they can also present acutely and mimic classical appendicitis, as demonstrated in our patient. In such scenarios, acute inflammation may obscure typical radiologic features of mucinous neoplasms, reinforcing the need for surgeons to maintain a high index of suspicion when encountering atypical or unusually distended appendices intraoperatively.6,7
A central challenge in the management of LAMN lies in determining the most appropriate surgical strategy. Historically, right hemicolectomy was recommended due to concerns regarding occult invasion or risk of recurrence.5 However, recent evidence indicates that simple appendectomy is sufficient—and equally safe—in patients who meet specific pathological and intraoperative criteria.8 Our case underscores this evolving paradigm. The intact appendiceal wall, normal cecal base, absence of extra-appendiceal mucin, and negative resection margins collectively supported the decision to perform appendectomy alone. These features align with contemporary recommendations that limit hemicolectomy to cases with perforation, invasive adenocarcinoma, positive margins, or extra-appendiceal mucin deposits.7,9
To provide practical guidance, the literature consistently emphasizes several factors that help surgeons determine whether appendectomy alone is sufficient or a more extensive resection is warranted. Key considerations include the integrity of the appendiceal wall, since perforation significantly increases the risk of peritoneal dissemination.5 The absence of extra-appendiceal mucin, which is a major predictor of pseudomyxoma peritonei; negative proximal margins, indicating complete excision of neoplastic mucosa; lack of infiltrative invasion on pathological evaluation7 and no evidence of regional lymphadenopathy or additional mucinous lesions elsewhere. Our patient met all of these criteria, supporting the decision to proceed with a conservative, low-morbidity appendectomy.
Although the patient’s comorbidities—hypertension and right bundle branch block—do not contribute directly to LAMN biology, they influenced perioperative planning and underscore a practical consideration: even common comorbidities necessitate coordinated multidisciplinary management when unexpected intraoperative findings arise.10 This reflects real-world surgical decision-making more accurately than emphasizing novelty in disease presentation.
Nevertheless, several limitations must be acknowledged. First, the combination of acute LAMN and common cardiac comorbidities does not constitute a novel pathologic entity, and therefore, the generalizability of this report is inherently limited. Second, the postoperative follow-up period of four months restricts any conclusions regarding long-term recurrence risk. Finally, because the diagnosis was made postoperatively, preoperative imaging and decision-making could not fully incorporate neoplastic considerations.
In summary, this case adds value not by introducing a new clinical variant, but by illustrating how established intraoperative and pathological criteria can guide surgeons toward safe, conservative management of LAMN, thereby avoiding unnecessary hemicolectomy. By synthesizing these decision-making principles, this report offers a concise and actionable framework that may support clinicians faced with similar intraoperative findings in the future.
Limitation
This case report is limited by its single-patient design, which restricts generalizability and precludes comparison with alternative surgical approaches. The relatively short follow-up period does not allow full assessment of long-term outcomes, including recurrence or development of pseudomyxoma peritonei. In addition, some preoperative data and biomarkers were not comprehensively available, and management decisions were influenced by the acute clinical setting and surgeon judgment, which may limit reproducibility in other contexts.
Conclusion
This case illustrates how established intraoperative and pathological criteria can be applied in real time to guide surgical decision-making in patients with appendiceal mucinous neoplasms presenting acutely. Although the patient’s symptoms initially suggested routine acute appendicitis, careful intraoperative assessment—combined with postoperative pathological confirmation of an intact LAMN with negative margins and no extra-appendiceal mucin—supported the use of simple appendectomy rather than more extensive resection. The successful outcome reinforces the growing evidence that appendectomy alone can be curative in well-selected patients. Rather than proposing a novel disease presentation, this report demonstrates the practical utility of a structured, criteria-based approach that may help surgeons avoid unnecessary hemicolectomy in similar clinical scenarios.
Implications
The primary implication of this case is not the recognition of LAMN as a differential diagnosis—which is already well established—but the clarification of how specific intraoperative and pathological findings can confidently direct surgeons toward a less morbid operative strategy. Incorporating criteria such as appendiceal wall integrity, absence of extra-appendiceal mucin, and negative proximal margins into real-time decision-making can reduce overtreatment without compromising oncologic safety. This case therefore supports the practical implementation of a selective appendectomy-based approach for appropriately screened patients, offering a clear and reproducible framework for surgical management.
Ethics Approval
This case report was conducted in accordance with the ethical standards of the institutional and national research committee Torbat Heydariyeh University of Medical Sciences Ethics Committee (Approval No: IR.THUMS.REC.1404.059). Following ethical approval, Imam Hossein Educational Hospital, Torbat Heydariyeh, Iran, was contacted for access and information dissemination. Written informed consent was obtained from the patient for participation in the study and for the publication of the clinical data and images included in this report.
Author Contributions
The authors made significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no specific funding for this work.
Disclosure
The authors declare no competing interests in this work.
References
1. Sima LV, Dan CA-M, Zara F, et al. Giant appendiceal mucocele with high grade mucinous neoplasm-case report and review of the literature. Diagnostics. 2024;14(21):2429. doi:10.3390/diagnostics14212429
2. von Rokitansky C, von Rokitanskyvon Rokitansky KF. A Manual of Pathological Anatomy. Vol. 3. Blanchard & Lea; 1855.
3. Higa E, Rosai J, Pizzimbono CA, et al. Mucosal hyperplasia, mucinous cystadenoma, and mucinous cystadenocarcinoma of the appendix. A re‐evaluation of appendiceal “mucocele”. Cancer. 1973;32(6):1525–6. doi:10.1002/1097-0142(197312)32:6<1525::AID-CNCR2820320632>3.0.CO;2-C
4. Aho AJ, Heinonen R, Laurén P. Benign and malignant mucocele of the appendix. Histological types and prognosis. Acta Chir Scand. 1973;139(4):392–400.
5. Istl AC, Gage MM, Esquivel J, et al. Management of Low-Grade Appendiceal Mucinous Neoplasms (LAMN): an International Survey of Surgeons Performing CRS and HIPEC. Ann Surg Oncol. 2021;28(7):3831–3837. doi:10.1245/s10434-020-09312-w
6. Cosyns S. New insights in the treatment of borderline ovarian tumours; 2025.
7. Carr NJ, Cecil TD, Mohamed F, et al. A consensus for classification and pathologic reporting of pseudomyxoma peritonei and associated appendiceal neoplasia: the results of the Peritoneal Surface Oncology Group International (PSOGI) modified Delphi process. Am J Surg Pathol. 2016;40(1):14–26. doi:10.1097/PAS.0000000000000535
8. Guner M, Aydın C. Low-grade appendiceal mucinous neoplasm: what is the best treatment? Cureus. 2023;15(10):e46591. doi:10.7759/cureus.46591
9. Turaga KK, Pappas S, Gamblin TC. Right hemicolectomy for mucinous adenocarcinoma of the appendix: just right or too much? Ann Surg Oncol. 2013;20(4):1063–1067. doi:10.1245/s10434-012-2783-7
10. Smilowitz NR, Berger JS. Perioperative management to reduce cardiovascular events. Circulation. 2016;133(11):1125–1130. doi:10.1161/CIRCULATIONAHA.115.017787
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.