Back to Journals » Drug Design, Development and Therapy » Volume 20
Low-Dose Sevoflurane Restores Prefrontal Excitatory/Inhibitory Balance and Improves Autism-Like Social Behavior: A Preclinical and Pilot Clinical Study
Authors Xu H ![]() , Shi Z, Guo X, Deng S, Wu M, Chen B, Qin J, Xu N, Zhao T, Chang Y, Song X
, Shi Z, Guo X, Deng S, Wu M, Chen B, Qin J, Xu N, Zhao T, Chang Y, Song X
Received 15 April 2025
Accepted for publication 3 February 2026
Published 25 February 2026 Volume 2026:20 534484
DOI https://doi.org/10.2147/DDDT.S534484
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Tin Wui Wong
Haiping Xu,1,2,* Ziwen Shi,1,* Xinying Guo,1,* Shiqi Deng,1 Manhong Wu,3 Baoling Chen,1 Jingwen Qin,1 Ning Xu,3 Tianyun Zhao,1 Yanqun Chang,3 Xingrong Song1,2
1Department of Anesthesiology, Guangzhou Women and Children’s Medical Center, Guangzhou Medical University, Guangzhou, People’s Republic of China; 2Guangdong-Hong Kong-Macau Institute of CNS Regeneration, Ministry of Education CNS Regeneration Collaborative Joint Laboratory, Jinan University, Guangzhou, People’s Republic of China; 3Department of Rehabilitation Medicine, Guangdong Women and Children’s Hospital, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xingrong Song; Yanqun Chang, Email [email protected]; [email protected]
Background: Medications aimed at modulating excitatory/inhibitory (E/I) balance have shown promise in alleviating the behavioral manifestations of autism spectrum disorder (ASD). We therefore aimed to investigate the potential of low-concentration sevoflurane, a GABAA agonist, to modulate E/I balance and affect autism-like behavior deficit in BTBR mice and ASD patients.
Methods: In the preclinical study, BTBR mice were exposed to 1% sevoflurane for 30 minutes daily, 5 days per week, from postnatal weeks 4 to 6. Behavioral and electrophysiological assessments were performed. In the clinical trial, ASD patients received 1% sevoflurane treatments for 2 hours per session, 3– 5 times during the first two weeks, followed by 2– 3 sessions per week for a total of 12 weeks. Assessments were conducted at baseline and the 14th week. The primary outcomes were evaluated using the Childhood Autism Rating Scale (CARS) and Clinical Global Impressions-Improvement (CGI-I) scale, while secondary outcomes were assessed using the Autism Diagnostic Observation Schedule-2 (ADOS-2), Clinical Global Impression-Severity Scale (CGI-S), Autism Treatment Evaluation Checklist (ATEC), and Autism Behavior Checklist (ABC).
Results: Our preclinical results demonstrated that repeated exposure to low-concentration sevoflurane restored E/I balance and improved social interaction and social memory without affecting repetitive behaviors. Accordingly, an open-label and single-arm clinical trial enrolled 20 ASD patients in Guangzhou Women and Children’s Medical Center. Significant reduction in CARS score of 4.7 points was observed between baseline and the end of treatment, which is both statistically and clinically significant. Additionally, 61% of ASD children demonstrated a positive response as measured by the CGI-I scale. Furthermore, analysis of secondary outcomes revealed that sevoflurane treatment primarily improved social impairments in ASD patients. Importantly, no significant safety concerns were observed during the one-year follow-up.
Conclusion: Low-concentration sevoflurane shows promise as a novel therapeutic strategy for improving social deficits in ASD by modulating E/I balance.
Trial Registration: Chinese Clinical trial Number: ChiCTR1900027459.
Keywords: sevoflurane, autism, excitatory/inhibitory balance, social behavior
Background
Autism spectrum disorder (ASD) is a neurological and developmental disorders with a rising incidence worldwide, now affecting as many as 1 in 36 children.1–3 The primary symptoms of ASD are characterized by impairments in social communication/interaction, repetitive behaviors and restricted interests.4 The condition results from a complex interaction between genetic elements and environmental influences, which remain not fully elucidated.5 Although numerous drugs are under investigation for the treatment of ASD, no effective pharmacotherapy exists for addressing its core symptoms.6 Thus, extensive research efforts currently have been dedicated to investigating numerous pharmaceutical agents, extending beyond traditional psychotropic medications, to treat core ASD symptoms and accompanying neuropsychiatric conditions.
Disturbed excitatory and inhibitory (E/I) balances have been implicated in various brain disorders, including ASD.7 An increased E/I ratio in sensory, mnemonic, social, and emotional systems has been identified in both ASD patients and ASD mouse model.8,9 Targeting this imbalance, researchers have explored various pharmacological and non-pharmacological approaches to restore the E/I ratio.9 GABAergic system is critical for maintaining the E/I balance necessary for normal neural circuitry and brain functionality.10 This understanding has led to the emergence of pharmacological agents and modulators for GABAergic system as potential treatments for ASD and associated behavioral disturbances.11–13
Sevoflurane, a potentiator of GABAARs, has long been employed for surgical anesthesia in Japan since 1990 and increasingly adopted for sedative in intensive care units and outpatient settings, owing to its advantageous pharmacodynamic and pharmacokinetic characteristics.14–16 These include a rapid onset of action, minimal accumulation in the body, few adverse effects, and short recovery times.14–16 Recent discoveries have revealed that sevoflurane, beyond its established use as anesthetic, may serve as a therapeutic agent for multiple neuropsychiatric and neurodevelopmental disorders, such as depression,17,18 schizophrenia19 and ASD,20 by restoring the E/I balance in the brain. We previously discovered that repeated low concentration of sevoflurane was sufficient to modulate the E/I balance in the brain, improve behavioral abnormalities in schizophrenia, and demonstrate a favorable safety profile.19
This study aims to explore the effect of low concentrations sevoflurane on core abnormal behaviors in BTBR mice and the E/I balance in the brain. Accordingly, we aim to explore the efficacy and safety of repeated low-concentration sevoflurane inhalation in ASD children in a preliminary, small-scale study, paving the way for large-scale randomized controlled trials in the future.
Methods
Preclinical Methods
Mouse Husbandry
The experiments received approval from the Institutional Animal Care and Use Committees at Guangzhou Women and Children’s Medical Center, Guangzhou, China. All animal procedures were performed in strict accordance with the Guide for the Care and Use of Laboratory Animals. Both female and male C57BL/6 mice were acquired from SPF (Beijing) Biotechnology Company Limited. BTBR T+ Itpr3tf/J (Strain #:002282) was purchased from The Jackson Laboratory. All animals were cohabitated in sanitized acrylic cages with weekly bedding changes and provided unrestricted access to food and water.
Experimental Design of Mouse Experiment
Experimental timeline was shown in Figure 1A. In total, the B6+Con group included 9 mice (5 males, 4 females), while the BTBR+Con and BTBR+Sev groups each included 12 mice (6 males, 6 females). In detail, the experimental process began at postnatal week 4, where baseline behavioral assessments were first conducted on these mice. Following this, the sevoflurane treatment was exposed to 1% sevoflurane for 30min daily with a gas mixture containing 30% oxygen and 70% nitrogen for 5 consecutive days. This exposure was repeated at week 5 and week 6. This exposure conducted under the supervision of an anesthesia gas monitor following established protocol.21,22 The B6+Con and BTBR+Con groups served as control groups and were exposed to the same carrier gas mixture (30% O2 / 70% N2) in the anesthesia chamber, without sevoflurane, whereas the BTBR+Sev group received 1% sevoflurane in the same gas mixture. During each 30-min exposure, animals were continuously observed and gently repositioned as needed to maintain a patent airway and normal breathing pattern. No higher induction concentration was used, and no animal was excluded due to excessive cardiorespiratory suppression. After the final sevoflurane exposure at week 6, behavioral tests assessments including three-chamber social interaction and social novelty recognition tests, assessment of stereotyped behaviors (jumping, self-grooming, digging), and the marble-burying test were performed at week 7 and 10. The electrophysiological assessment was performed at week 7.
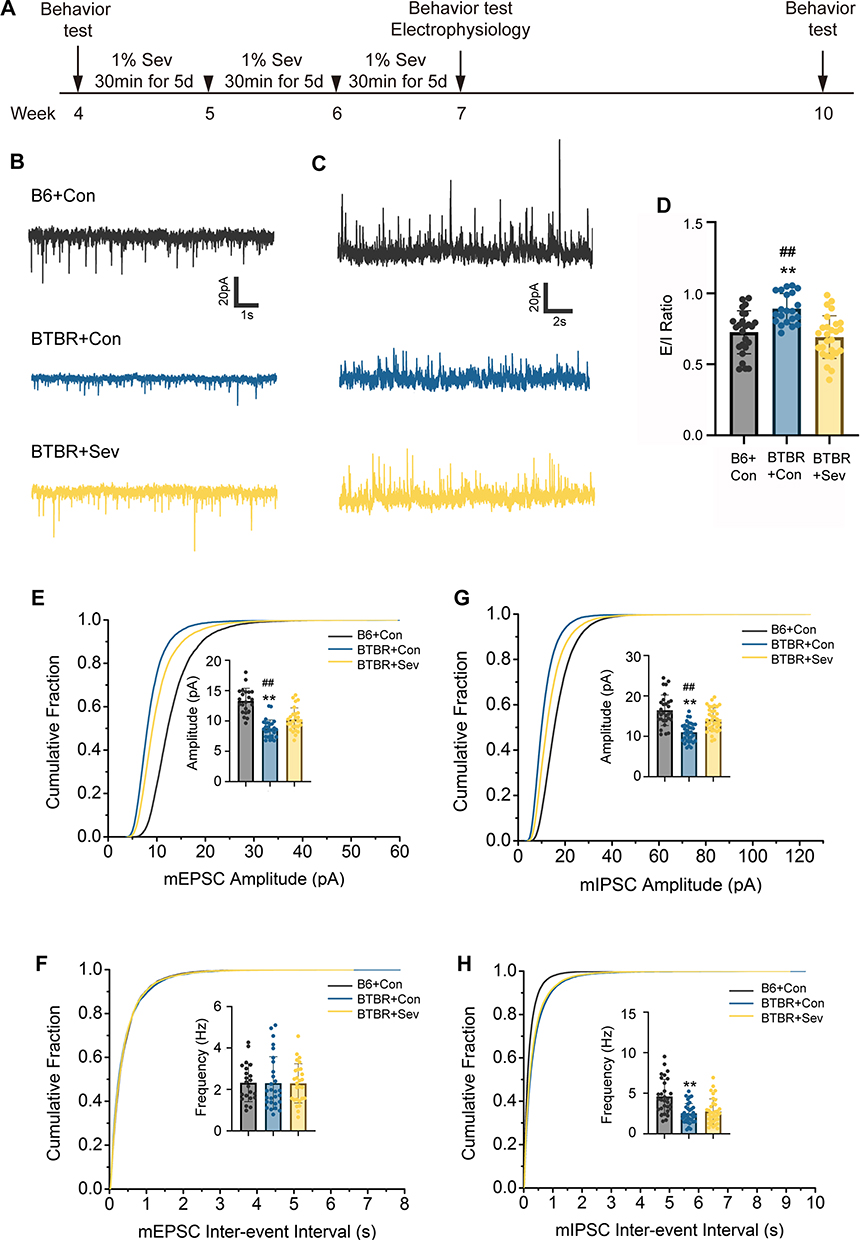 |
Figure 1 Low concentration sevoflurane reversed alterations of electrophysiological profiles and E/I balance in the mPFC of BTBR mice. (A) Experiment timeline. Sev, sevoflurane. D, days. (B and C) Representative mEPSC (B) and mIPSC (C) recording traces of pyramidal neurons in laminae II/III of the mPFC from the B6+Con, BTBR+Con and BTBR+Sev mice. (D) The E/I ratio in laminae II/III of the mPFC from different groups (B6+Con group: 25 cells, 6 mice; BTBR+Con group: 21 cells, 4 mice; BTBR+Sev group: 27 cells, 4 mice). (E and F) Cumulative distribution of mEPSC amplitudes and inter-event intervals recorded from pyramidal neurons in laminae II/III of the mPFC. The bar chart indicated the mean amplitude and frequency of mEPSC. (G and H) Cumulative distribution of mIPSC amplitudes and inter-event intervals recorded from pyramidal neurons in laminae II/III of the mPFC. The bar chart indicated the mean amplitude and frequency of mIPSC. One-way ANOVA followed by Bonferroni’s post-hoc tests were used for analysis. Data are represented as mean ± SD; ** P < 0.01 compared with B6+Con; ## P < 0.01 compared with BTBR+Sev. |
Behavioral Testing
All behavioral recordings were analyzed offline by experimenters who were blinded to genotype and treatment group.
Social Interaction and Social Novelty Test
Mice were introduced into a three-chamber setup following established protocol.23 To evaluate social interaction, mice were placed in the presence of a stranger mouse confined in a cage with bars, alongside an empty cage. This setup enabled the mice to navigate three chambers without constraints for 10 min. The social novelty testing involved presenting a cage with a familiar mouse and another with a novel mouse for 10 min. The record was measured using the TopScan Version 3.0 software.
Repetitive Behavior
Mice were measured the frequency of repetitive behaviors over a 10-min period. The observed behaviors included jumping, self-grooming, and digging. Jumping was defined as the mouse standing on its hind legs in a corner or along the side walls of the cage and then leaping with both hind legs leaving the ground simultaneously. Grooming was defined as the mouse using its forelimbs to stroke or scratch its face, head, or body, or licking parts of its body. Digging was defined as the coordinated use of the forelimbs or hind limbs to excavate or displace the bedding material.
Marble Buried
Mice subjected to the grooming behavior test were also evaluated using the marble burying test. Mice were placed individually in a plastic container (40 cm x 30 cm x 22 cm) filled with clean wood chip bedding. The mice were allowed to freely explore the container for 30 minutes without interference, allowing them to acclimate to the environment. Following this testing period, 20 glass marbles were arranged in 5 rows of 4 marbles each on the surface of the bedding. A marble was considered buried if more than two-thirds of its surface area was covered by the bedding. The total number of buried marbles was recorded.
Electrophysiology
Acute brain slices were prepared from C57BL/6J and BTBR mice at postnatal week 7. Coronal slices (250 μm) containing the medial prefrontal cortex (mPFC) were cut in ice-cold cutting solution containing (in mM): 75 sucrose, 85 NaCl, 2.5 KCl, 1.25 NaH2PO4, 4 MgSO4, 0.5 CaCl2, 24 NaHCO3, 25 D-glucose, bubbled with 95% O2/5% CO2 using a vibratome (VT1200S, Leica). Slices were recovered for 30 min at 32°C in artificial cerebrospinal fluid (aCSF) containing (in mM): 119 NaCl, 2.5 KCl, 1.25 NaH2PO4, 2 MgCl2, 2 CaCl2, 26 NaHCO3, 10 D-glucose, bubbled with 95% O2/5% CO2, and then maintained at room temperature. The pyramidal neurons of PFC layer II/III were viewed with an Olympus microscope equipped with infrared DIC optics. Patch pipettes (4–6 MΩ) were filled with internal solution containing (in mM): 135 cesium methanesulfonate, 8 CsCl, 10 HEPES, 7 Na2-phosphocreatine, 2.168 MgATP, 0.34 NaGTP, 0.25 EGTA, pH 7.25 (adjusted with CsOH), 290–295 mOsm. Whole-cell voltage-clamp recordings were performed using a Multiclamp 700B amplifier and digitized with Digidata 1550A (Molecular Devices). Signals were filtered at 2 kHz (Bessel) and sampled at 10 kHz. Series resistance was <30 MΩ and compensated; cells were discarded if series resistance changed >20%. A liquid junction potential of +9.5 mV was calculated according to Barry (1994) and all reported holding potentials have been corrected for this value. mEPSCs were recorded at −70 mV (LJP-corrected, actual command −79.5 mV) and mIPSCs at 0 mV (LJP-corrected, actual command −9.5 mV) in aCSF containing 1 μM tetrodotoxin (TTX). The entire 3-minute trace was used for analysis. On average, >300–400 events per cell were analyzed for mEPSCs and mIPSCs.
Statistical Methods
Statistical analysis and graph plotting were performed using GraphPad Prism 9 (GraphPad, San Diego, CA, USA). Individual data points are plotted in the figure The statistic details are listed in the figure legend. The significance threshold was established at P-value < 0.05.
Clinical Methods
Study Design and Ethical Approval
This open-labelled and single arm study (registered in Chinese Clinical trial: ChiCTR1900027459) was conducted from November 14, 2019, to November 15, 2023 in the Guangzhou Women and Children’s Medical Center. All research involving human participants was conducted in accordance with the Declaration of Helsinki. Informed written consent was obtained from parents, and consent from the children was also secured when they have the comprehensive and expressive ability to provide it.
Study Participants
Telephone contact was initiated by parents to the study coordinator or principal investigator (Xingrong Song). Participants were diagnosed and evaluated by two pediatric neurologists (Manhong Wu and Ning Xu). Key inclusion and exclusion criteria are presented in Supplementary Table 1. All participants met DSM-5 criteria for ASD based on comprehensive clinical evaluation and standardized assessments (including ADOS-2 and CARS). The majority of cases were idiopathic; however, one child had a specific underlying genetic mutation and two had co-occurring epilepsy, reflecting the clinical heterogeneity of ASD.
Sevoflurane Treatment
After obtaining informed written consent, participants were arranged to receive sevoflurane treatment in a designated anesthesia resuscitation room at the department of anesthesiology, administered by two trained and experienced anesthetists. Fasting and intravenous access were not required. Sevoflurane was delivered in an air-oxygen mixture at 2 L/min through a face mask for the induction of sedation. The initial concentration was 6–8% to induce rapid loss of consciousness, and it was gradually adjusted between 0.5–1.2% as needed to maintain deep sedation. During sevoflurane treatment, participants were accompanied by parents or guardians and monitored with pulse oximetry, blood pressure, electrocardiography, and end-tidal carbon dioxide. After discontinuation of sevoflurane, participants were observed for another hour before departing. This treatment was repeated 3–5 times in the first two weeks and 2–3 times every week for a total of 12 weeks.
Efficacy Outcomes and Assessments
Safety and tolerability assessments included electrocardiograms, vital signs, physical examination, and clinical laboratory tests (hematology, chemistry, urinalysis) were carried out both before and after the last treatment session. Careful monitoring of potential symptoms related to abuse, dependence, and withdrawal was diligently undertaken throughout the treatment and followed-up period. Evaluations of treatment efficacy were performed at two key points: baseline and after the last sevoflurane inhalation. Efficacy assessments including childhood autism rating scale (CARS), Clinical Global Impression-Severity Scale (CGI-S), Clinical Global Impressions Improvement (CGI-I), Autism Behavior Checklist (ABC) and Autism Treatment Evaluation Checklist (ATEC) were executed by two trained, research-certified independent evaluators blinded to treatment condition. The primary outcome measures were the CARS and CGI-I scale. Secondary outcomes included assessment of total and subscales score of the ABC and the ATEC, the CGI-S scale, and ADOS-2.
Statistical Methods
To examine treatment effect, first, Shapiro–Wilk test was used to check the normality. If the data is normally distributed, a two-tailed paired t-test was used to test the treatment effect. If the data is not normally distributed, Wilcoxon signed-rank test was used. P<0.05 was considered as significant change.
Result
Pre-Clinical Data
Low Concentration Sevoflurane Reversed Alterations of Electrophysiological Profiles and E/I Balance in the mPFC of BTBR Mice
Imbalances between excitation and inhibition are frequently observed in animal model of ASD, and their correction normalizes key autistic-like phenotypes in these animals.7 Given that low concentration sevoflurane exposure can induce long-lasing alteration in E/I balance, primarily manifested as a decrease in the E/I ratio,19,20 in the mPFC, a key brain region associated with autism-related behavior, we first explore whether repeated low concentration sevoflurane could alter E/I ratio in the laminar II/III of mPFC. We found the E/I ratio in mPFC, measured as the mEPSC/mIPSC amplitude of the same pyramidal neuron, was significantly increased in BTBR mice, indicating a shift towards hyperexcitation, consistent with previous reports.13 Notably, repeated sevoflurane exposure significantly decreased the E/I ratio in BTBR mice, suggesting a corrective effect on this imbalance (Figure 1A–D). Specifically, we found the amplitude but not frequency of mEPSC was significantly lower in BTBR mice, which was reelevated after low-concentration sevoflurane exposure (Figure 1E and F). However, although both the amplitude and frequency of mIPSC were reduced in BTBR mice, repeated low-concentration sevoflurane exposure only reversed the amplitude of mIPSC (Figure 1G and H). Taken together, these findings indicate that low-concentration sevoflurane effectively normalizes the E/I balance in the mPFC, thereby offering potential therapeutic value in treating ASD-related behavioral deficits.
Low Concentration Sevoflurane Exposure Improves Social Interaction and Social Memory in BTBR Mice, but Not Repetitive Behavior
Given that the correction of E/I imbalance is closely associated with the improvement of key autistic-like phenotypes,7 we further investigated whether exposure to low concentrations of sevoflurane could alter the autism-related phenotypes in BTBR mice. Baseline behavioral assessments at postnatal week 4 included the three-chamber social interaction and social novelty tests, stereotyped behaviors (jumping, self-grooming, digging), and the marble-burying test. There were no significant differences between BTBR+Con and BTBR+Sev groups at baseline in any behavioral measure, whereas both BTBR groups showed impaired social behavior and increased repetitive behaviors compared with B6+Con (data not shown). In addition, assessments of locomotor and olfactory function showed that BTBR mice exhibited normal locomotor activity but reduced odor investigation across stimuli, a phenotype not altered by low-dose sevoflurane (Figure S1A–C). These findings indicate that the improvement in social behavior is unlikely to be explained by changes in locomotion or basic olfactory detection. Consistent with previous reports, BTBR mice exhibited social behavior deficits and significantly increased stereotypic behavior at postnatal week 6 compared to wild-type mice (Figure 2A–G). However, in three-chamber social interaction assay, BTBR mice treated with low concentration sevoflurane show substantial recoveries in social interaction (Figure 2A–C) and social novelty recognition (Figure 2D and E). Notably, low concentration sevoflurane did not rescue stereotyped behavior, including spontaneous motor stereotypes (Figure 2F) and marble burying (Figure 2G), suggesting that sevoflurane selectively rescues social behaviors.
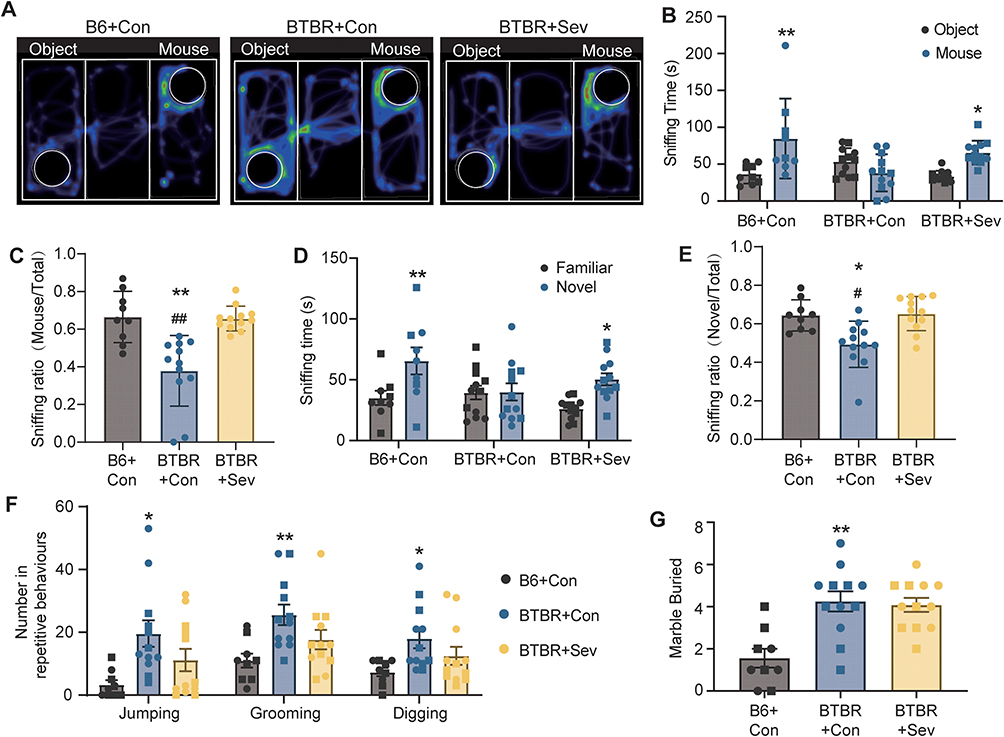 |
Figure 2 Low concentration sevoflurane exposure improves social interaction and social memory in BTBR mice. (A) Examples of recording trials from B6+Con, BTBR+Con and BTBR+Sev group as indicated. (B) Social interaction was evaluated using the 3-chamber paradigm by measuring the time spent in each side chambers. **p<0.01 and *p<0.05 two-way ANOVA followed by Sidak’s post hoc test between cages. (C) Sniffing ration (sniffing time (mouse) versus total sniffing time). **p<0.01 compared with B6+Con group, and ##: p<0.01 compared with BTBR+Sev group; one-way ANOVA followed by Tukey’s post hoc test. (D) Social memory was evaluated using the 3-chamber paradigm by measuring the time spent in each side chambers. **p<0.01 and *p<0.05 two-way ANOVA followed by Sidak’s post hoc test between cages. Data are shown as mean±SEM. (E) Sniffing ration (sniffing time (Novel) versus total sniffing time). *p<0.05 compared with B6+Con group, and #: p<0.05 compared with BTBR+Sev group; one-way ANOVA followed by Tukey’s post hoc test. (F) Stereotypical behaviors in different group. *p<0.05, **p<0.01 compared with B6+Con group; one-way ANOVA followed by Tukey’s post hoc test. (G) The number of buried marbles in different group. **p<0.01 compared with B6+Con group; one-way ANOVA followed by Tukey’s post hoc test. |
Carry-Over Effects Were Maintained in BTBR Mice, with Social Parameters Being Still Recovered Three Weeks After Sevoflurane Exposure Withdrawal
To further understand the carry-over effects of sevoflurane on autistic-like behavior in BTBR mice, particularly social behavior, after the cessations of treatment, we conducted behavioral assessments three weeks after the treatment had ended (Figure 1A). As regards social behavior, low concentration sevoflurane exposure-induced rescue of deficit in social interaction and social novelty recognition in BTBR mice persisted up to 3 weeks after the end of treatment (Figure 3A–D). However, three weeks after discontinuing sevoflurane exposure, the stereotypic behavior in BTBR mice remained unchanged ((Figure 3E and F). Thus, repeated low concentration sevoflurane exposure efficiently and long-lastingly relieved social interaction and social novelty recognition deficit in BTBR mice. Results from this classic autism mouse model suggest that exposure to low concentrations of sevoflurane can effectively improve social behavior deficit in mice. These preclinical findings, combined with the known safety profile of sevoflurane, provide a rationale for advancing to human trials.
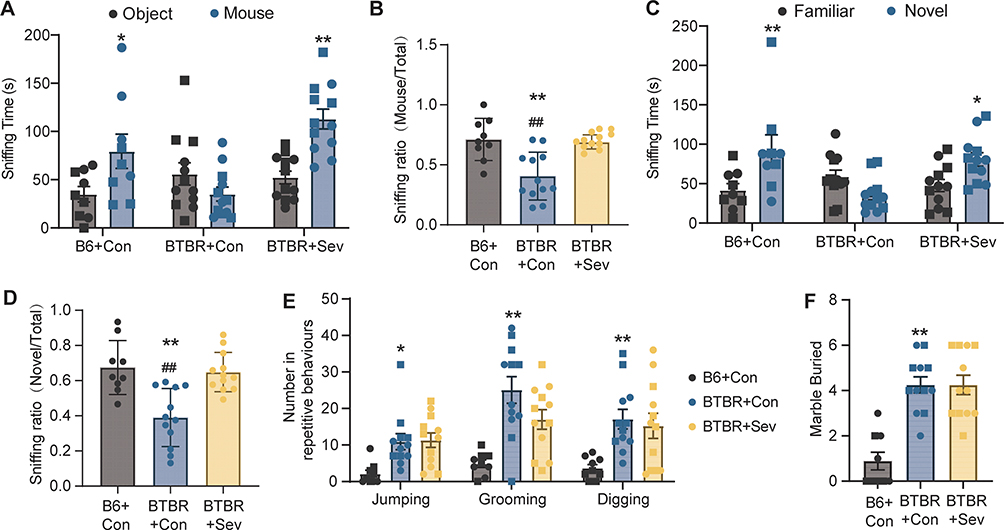 |
Figure 3 Carry-over effects were maintained in BTBR mice, with social parameters being still recovered three weeks after sevoflurane exposure withdrawal. (A) Social interaction was evaluated using the 3-chamber paradigm by measuring the time spent in each side chambers. **p<0.01 and *p<0.05 two-way ANOVA followed by Sidak’s post hoc test between cages. (B) Sniffing ration (sniffing time (mouse) versus total sniffing time). **p<0.01 compared with B6+Con group, and ##: p<0.01 compared with BTBR+Sev group; one-way ANOVA followed by Tukey’s post hoc test. (C) Social memory was evaluated using the 3-chamber paradigm by measuring the time spent in each side chambers. **p<0.01 and *p<0.05 two-way ANOVA followed by Sidak’s post hoc test between cages. Data are shown as mean+±SEM. (D) Sniffing ration (sniffing time (Novel) versus total sniffing time). **p<0.01 compared with B6+Con group, and ##: p<0.01 compared with BTBR+Sev group; one-way ANOVA followed by Tukey’s post hoc test. (E) Stereotypical behaviors in different group. *p<0.05, **p<0.01 compared with B6+Con group; one-way ANOVA followed by Tukey’s post hoc test. (F) The number of buried marbles in different group. **p<0.01 compared with B6+Con group; one-way ANOVA followed by Tukey’s post hoc test. |
Clinical Data
Clinical Trial Design
We designed and conducted an open-label, single arm clinical trial at Guangzhou Children and Women’s Medical Center with primary endpoints for efficacy as determined by CARS and CGI-I scale. Secondary endpoints included ADOS-2, CGI-S, ATEC, and ABC scale (Figure 4A–C). This trial initially screened 25 individuals for eligibility, and ultimately twenty children (17 males and 3 females, age 3–18 years) were included in the study after meeting the inclusion criteria as outlined in Supplementary Table 1. After enrollment, each participant was administrated baseline behavioral assessments using CARS, ADOS-2, ATEC, ABC and CGI-S, and liver and kidney function was evaluated by laboratory results. All inclusion and exclusion criteria can be found in Supplementary Table 1. Of these 20 patients, 18 participants (15 males and 3 females) completed the full 3-month trial treatments. One participant discontinued the trial due to lockdown policies of COVID-19 pandemic after receiving 18 treatments and another participant had to cease participation due to a traffic accident that occurred three days after 25th treatment. The mean (SD) number of sevoflurane treatments was 33.1 (8.71). Table 1 displays the demographics and initial characteristics of the participants. Baseline severity of ASD is shown in Table 1 including ADOS-2 score and CGI-S scales. According to the ADOS-2 score, out of the 20 children, 7 were moderate and 13 were severe. In the CGI-S assessment, 6 were rated as moderate, 7 as marked ill, and 7 as severely ill (Table 1). The intellectual levels varied widely and some of them can not cooperate to complete the intelligence test (data not shown). One of the children had a specific underlying genetic mutation, and two others presented with co-occurring epilepsy. CARS, CGI-I, ADOS-2 and CGI-S evaluation were performed by trained clinical pediatric neurologists, while ATEC and ABC assessments were completed by primary caregivers, who were predominantly parents and grandparents. Thus, there was minimal variability in raters for caregiver-completed assessments throughout the trial. All participants took no concomitant medications during treatment.
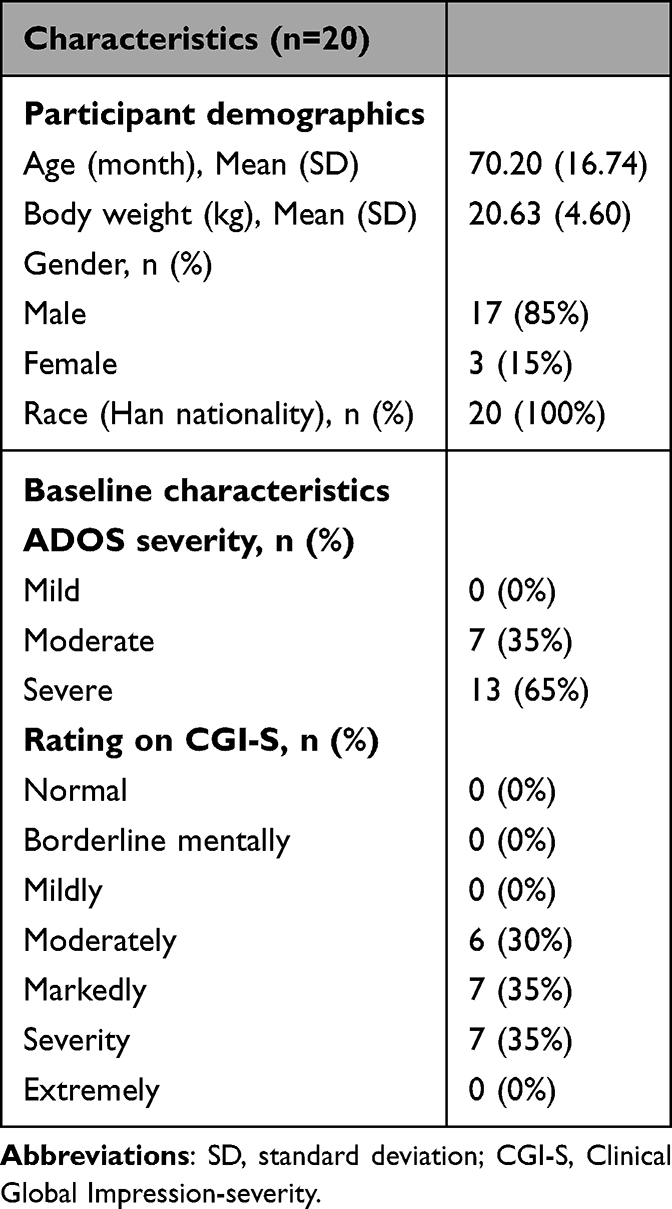 |
Table 1 Participant Demographics and Baseline Clinical Characteristics |
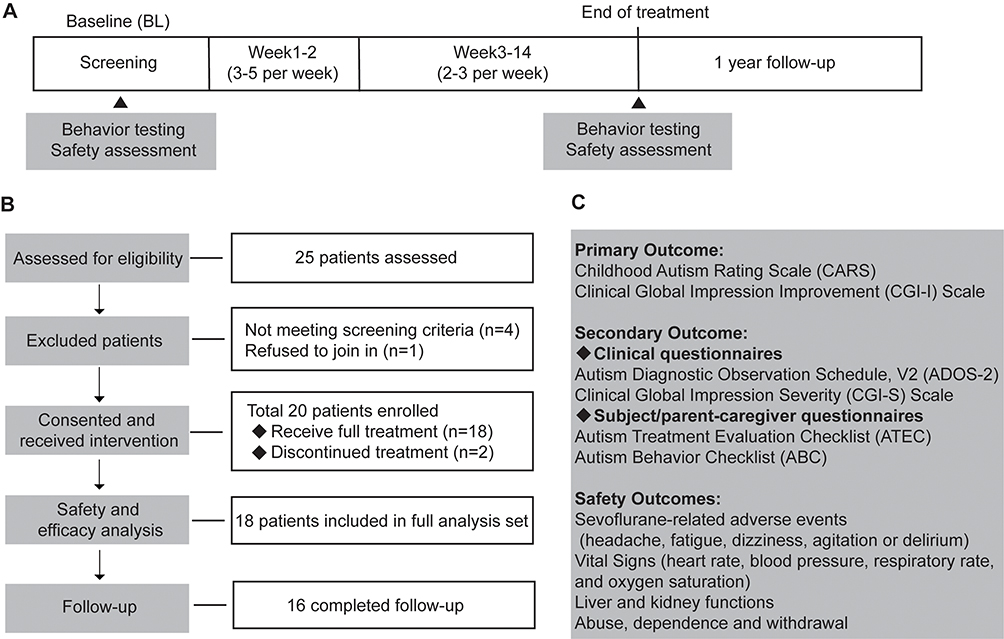 |
Figure 4 Trial design and procedures response to low concentration sevoflurane exposure in patients with ASD. (A) Clinical trial schedule. Participants were were screened in run-in period, followed by repeated 3–5 times during the initial two weeks and subsequently 2–3 times every week for a total of 12 weeks, with a follow-up 1 year after trial. Assessments were performed at baseline and again at the 14-week. (B) A total of 25 patients were screen for eligibility across trial. 20 patient were enrolled following meeting predefined criteria for study. 18 participants completed treatments and 16 completed the follow up. (C) Primary outcomes, secondary outcomes and safety outcomes were indicated. |
Primary Efficacy Outcomes
As shown in Figure 5A, from baseline to week 14, the overall CARS score exhibited a notable reduction with a p-value of less than 0.01, decreasing from 40.61 ± 4.19 at baseline to 35.89 ± 3.80, resulting in a significant difference value of 4.72 ± 1.36, which is considered clinically meaningful according to established consensus that define a reduction of 4.5 points on the CARS scale as significant.24 Among the 18 patients who completed the treatment, 12 showed a CARS reduction greater than 4.5 points, representing 66.7% of the group (Figure 5B). Additionally, 61% of the children demonstrated a positive response, classified as either much improved or very much improved on the CGI-I scale (Figure 5C). The remaining 39% of patients exhibited only minimal improvement (Figure 5C). The study, therefore, met its primary efficacy outcomes in ASD population, with a significant reduction in CARS score and a majority of patients showing meaningful clinical improvements.
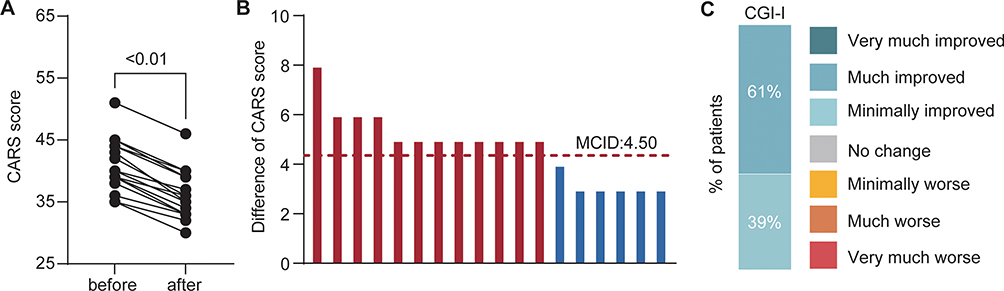 |
Figure 5 Primary outcomes after low concentration sevoflurane exposure in ASD patients. (A) Summary statistics of CARS score in patients before and after treatments with sevoflurane (n=18 patients). P<0.01. (B) Bar plot of difference of CARS scores for each patient (each bar represents one patients). (C) Percentage of patients in CGI-I score at the end of treatment. Abbreviation: MCID, minimal clinically important difference. |
Secondary Efficacy Outcomes
In the secondary efficacy outcomes, we categorized assessments into those conducted by professionally trained clinicians, including CGI-S and ADOS-2, and those completed by primary caregivers, including ATEC and ABC. Across all assessment tools, significant reductions in scores were observed with statistically difference, indicating improvements after low concentration sevoflurane exposure in ASD patients (Table 2). Specifically, CGI-S scores decreases from 5.06 to 4.17, ADOS-2 scores dropped from 22.28 to 19.78, ATEC scores reduced from 91.28 to 78.39, and ABC scores fell from 81.39 to 68.94.
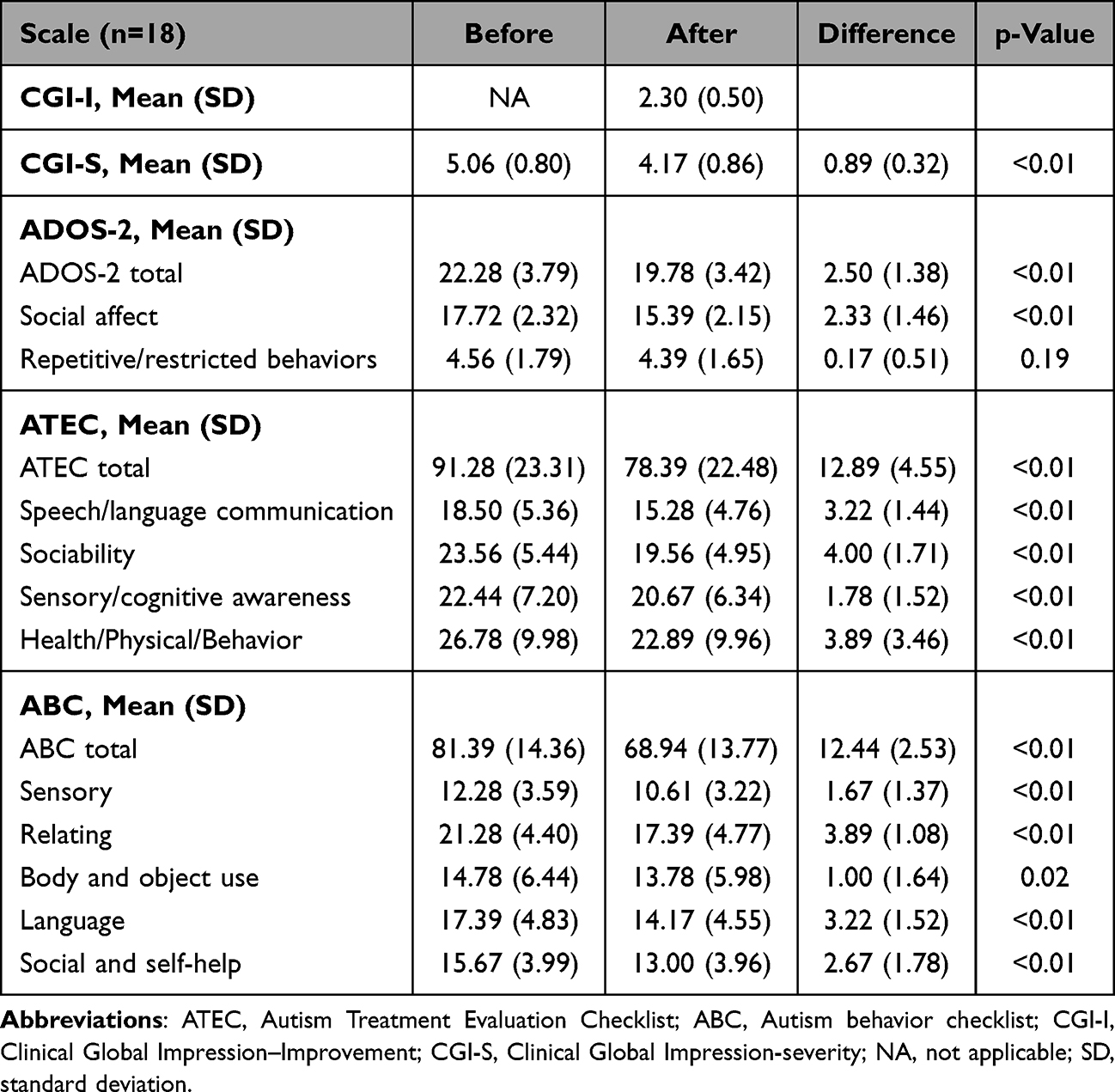 |
Table 2 Outcome Measures Before and After Treatment |
Further analysis of patient behavior improvement focused on the ADOS-2 assessments conducted by clinical professionals. The reduction in ADOS-2 scores was primarily driven by improvements in social behavior, with social affect (SA) scores decreasing from 17.72 to 15.39, which was statistically significant (Table 2). However, no significant improvement was observed in the restricted and repetitive behaviors (RRB) domain of ADOS-2, consistent with our findings in animal studies.
However, the evaluations completed by caregivers using the ATEC and ABC scales revealed somewhat different patterns. As shown in Table 2, ATEC subscales showed significant improvements across several domains: Speech/Language/Communication (from 18.50 ± 5.36 at baseline to 15.28 ± 4.76 at week 14), Sociability (from 23.56 ± 5.44 to 19.56 ± 4.95), Sensory/ Cognitive awareness (from 22.44 ± 7.20 to 20.67 ± 6.34) and Health/Physical/Behavior (from 26.78 ± 9.98 to 22.89 ± 9.96). Similarly, ABC subscales indicated significant reductions in sensory, relating, body/object use, language, and social self-help, with decreases of 1.67, 3.89, 1.00, 3.22 and 2.67 points, respectively.
Safety Outcomes
One participant experienced irritable cough during the inducing phase, and an additional two participants developed irritability during the treatment phase. Notably, these symptoms promptly resolved upon increasing the concentration of sevoflurane. A single participant reported brief episodes of mild nausea and vomiting approximately five minutes after awakening. Importantly, none of participants exhibited other sevoflurane-related adverse events including headache, fatigue, dizziness, agitation or delirium neither during their hospital nor throughout the entire treatment procedure, as detailed in Table 3.
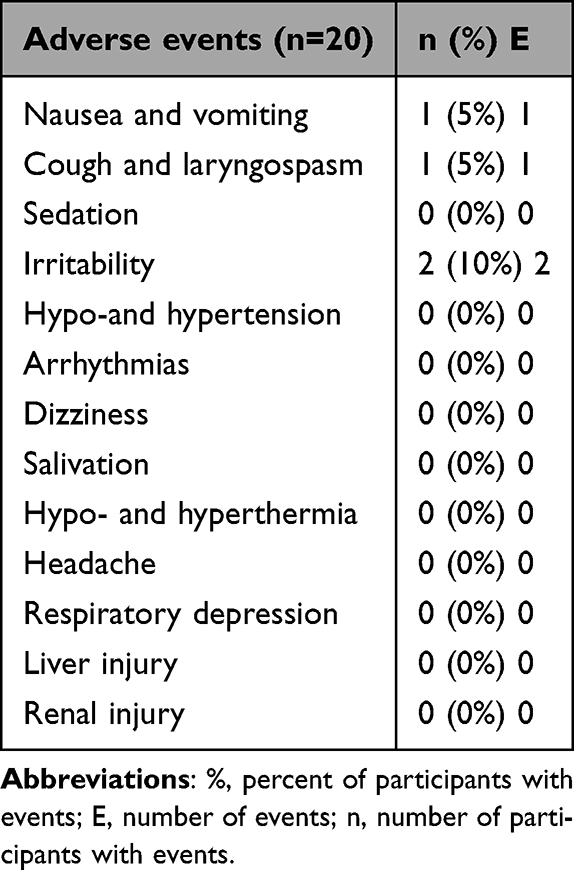 |
Table 3 Treatment-Emergent Adverse Events |
Furthermore, vital signs remained stable during treatment, including heart rate, blood pressure, respiratory rate, and oxygen saturation, all of which promptly returned to baseline value after discontinuing sevoflurane inhalation. No abnormal physiological parameters or medically meaningful changes, including liver and kidney functions, were observed when compared to the baseline (Supplementary Table 2).
Importantly, there were no reports of symptoms related to abuse, dependence and withdrawal during both the treatment and followed-up periods, and no participants withdrew from the study because of an adverse event.
One-Year Follow-Up Observation
Out of the 18 participants who completed entire treatment, 16 completed the one-year follow-up, resulting in a follow-up rate of approximately 89% (Figure 4B). Among those lost to follow-up, one participant could not be contacted by their primary caregivers, and one participant unfortunately pass away due to an accident.
Long term safety profile was the primary focus of our follow-up assessment. None of 16 participants exhibited sevoflurane-related adverse events including headache, dizziness, agitation or delirium during the follow-up period (Supplementary Table 3). Additionally, no caregivers reported signs of abuse, dependence, or withdrawal in the children (Supplementary Table 3). These findings suggest that the long-term safety profile of repeated low-concentration sevoflurane exposure in children with ASD remains favorable.
ABC scale was the sole behavioral evaluation during one-year follow-up period. While the total ABC score showed a significant reduction after treatment, the one-year follow-up revealed that the scores did not significantly change compared to either pre-treatment or post-treatment levels (Figure S2A). Most other subscales, including sensory, body and object use, and language, followed a similar trend (Figure S2B, D and E). It is noteworthy that the Relating and Social/Self-Help subscale scores were maintained during the one-year follow-up (Figure S2C and F). Nevertheless, we must interpret these results with caution. The fact that over 90% of the ASD children received additional behavioral therapies during the follow-up period, coupled with the natural developmental changes that occur as children’s brain mature, could also contribute to the sustained improvements.
Discussion
To the best of our knowledge, this is the first study to investigate the effects of low concentration sevoflurane exposure on autistic-like behaviors and electrophysiological profiles in BTBR mice, and preliminarily explore the safety and efficacy of low-concentration sevoflurane in small ASD cohort. Our results demonstrate that repeated exposure to low concentration sevoflurane effectively restores E/I balance in the mPFC of BTBR mice and, importantly, selectively ameliorates deficits in social interaction and social memory in BTBR mice. Moreover, these improvements in social deficits were sustained over the long term. These findings were consistent with the results from our clinical trial, where significant improvements in social interaction and communication were observed among children with ASD following sevoflurane treatment, although no remarkable improvement was observed in repetitive behaviors. Further, repeated 2-hrs low-concentration sevoflurane treatment for ASD children exhibited an acceptable safety profile. These findings suggest that modulating E/I balance with low-concentration sevoflurane could be a valuable therapeutic strategy for addressing social communication deficits in ASD.
Efficacy and Safety of Low-Concentration Sevoflurane Treatment in ASD
ASD is a complex heterogeneous consortium of pervasive development disorders characterized by a spectrum of neuropsychological and behavioral deficits, making diagnosis and treatment challenging. In our study, we employed widely recognized assessment scales including CARS, CGI-I, CGI-S, ABC and ATEC, to evaluate the efficacy of repeated low concentration sevoflurane. The treatment resulted in a 4.72-point improvement in CARS scores as the primary outcome, aligning with the consensus that a 4.5-point improvement is clinically meaningful for ASD interventions.24 In addition, the responders rate for CARS and CGI-I in our study (66.7% and 61%, respectively) were higher than those reported in previous reports.25,26 Importantly, assessments by primary caregivers using the ATEC and ABC scale also consistently indicated improvements in the core symptoms of autism with low-concentration sevoflurane treatment. This is significant because caregiver evaluations play a crucial role in autism assessment, offering unique insights into the daily behaviors and challenges faced by individuals with ASD—insights that may not always be fully captured in clinical settings.27,28
In this study, 19 children with ASD were exposed to sevoflurane more than 20 times, and no sevoflurane-related safety issues, particularly hepatorenal toxicity, were observed. No participants withdrew from the trial due to adverse reactions, and a one-year follow-up revealed no obvious sevoflurane-related safety concerns. This finding is significant given the cautious approach typically taken toward repeated anesthetic exposure in developing brains.29,30 Despite recent clinical studies affirming safety following short-term anesthesia exposure, typically averaging close to 1hrs for single doses, in children,31,32 some studies suggest that children exposed to repeated and longer cumulative durations of general anesthesia may face an elevated risk of developmental abnormalities.33,34 However, there remains a scarcity of studies focusing on the neurotoxicity of developing brain caused by repeated exposure of sedative doses of general anesthetics. Fortunately, two preclinical studies have shown that low-concentration sevoflurane (at concentrations of 1.2% and 1.8%, respectively) can promote cognition function and neuronal proliferation.35,36 Furthermore, an extensive body of clinical studies have shown that sevoflurane sedation in ICU, lasting for a minimum of 48hrs, can substantially improve the clinical outcomes and exhibit has protective properties in many organs such as brain, myocardium and lung.37–39 Our previous study has established a favorable safety and tolerability profile when exposing patients to repeated sedative dosage of sevoflurane for treatment of schizophrenia patients.19 Our study provides new evidence that repeated low-concentration sevoflurane exposure does not exacerbate core autism symptoms or cause other sevoflurane-related safety issues, as confirmed by the follow-up period.
The Mechanism of Low Concentration Sevoflurane on Social Deficits in ASD
Our study results indicate that the overall improvement in ADOS-2 scores was primarily driven by enhanced social interactions, with a significant reduction observed in the SA domain scores, while the RRB domain remained unchanged. This pattern closely mirrors our observations in BTBR mice, suggesting that sevoflurane may preferentially modulate neural processes specifically related to social behaviors. One plausible explanation is the ability of low-dose sevoflurane to reduce the elevated E/I ratio in the mPFC, as demonstrated in our preclinical work and by other.19,20 In fact, the E/I imbalance in the mPFC is closely associated with social deficits in rodents and human studies.40–42 Increased E/I ratio in this region can reliably induce social impairments,42 and conversely, experimental reduction of the E/I ratio rescues social deficits in multiple ASD mouse models.43 These converging findings support the concept that restoring prefrontal E/I balance may represent a viable therapeutic mechanism.
However, the mechanism by which sevoflurane modulates E/I balance is complex. Sevoflurane acts as a broad-spectrum positive modulator of GABAA receptors, and enhancement of GABAergic inhibition—through pharmacological agents or genetic manipulation—has been shown to ameliorate social deficits in both clinical44 and preclinical13 studies. Yet, sevoflurane is not selective for a particular GABAA receptor α-subunit. For example, previous studies report that enhancement of α2/α3-containing GABAA receptors can improve social behavior, whereas potentiation of α1-containing receptors may worsen it in BTBR mice.13 This raises an important mechanistic question about how a non-selective agent such as sevoflurane yields a net therapeutic effect. One possibility is that at low concentrations, sevoflurane produces dose- and circuit-dependent effects, preferentially influencing mPFC interneuron networks—which are enriched in α2/α3-containing receptors and critically regulate social behavior—while exerting comparatively weaker effects on α1-dominated thalamocortical or arousal pathways associated with sedation.
Importantly, general anesthesia with sevoflurane affects the entire brain, and it is unlikely that behavioral improvements arise solely from changes within the mPFC. Sevoflurane modulates activity in several regions implicated in social and affective processing, including the amygdala, hippocampus, striatum, and thalamocortical circuits. Low-dose sevoflurane has been shown to alter large-scale neural synchrony, oscillatory dynamics, and long-range connectivity—mechanisms that could independently or synergistically contribute to improved social behavior. Thus, while mPFC E/I restoration provides a compelling mechanistic link, additional circuit- and systems-level effects are likely involved.
Additionally, sevoflurane has off-target actions on other neurotransmitter systems, including NMDA receptors45 and AMPA receptors,46 which may also contribute to the normalization of cortical network activity. Despite acting through multiple molecular pathways, the convergent functional outcome observed across studies is a reduction in E/I ratio,19,20 providing a plausible mechanistic foundation for the behavioral improvements reported here. Nevertheless, our study does not identify the specific molecular or circuit targets through which low-dose sevoflurane exerts its effects. Future experiments employing receptor-subunit–specific modulation, genetic approaches, or cell-type–specific interrogation will be required to delineate the precise mechanisms underlying sevoflurane-induced restoration of E/I balance and social behavior.
The Effect of Low Concentration Sevoflurane on Repetitive Behaviors in ASD
Despite the positive outcomes observed in this study, it is important to note a key discrepancy: while the ADOS-2 RRB scores remained unchanged, reductions were noted in the ATEC fourth subscale (Health/Physical/Behavior) (p<0.01) and the ABC Body/Object Use subscale (p=0.02), both of which are related to restrictive and repetitive behaviors as reported by primary caregivers. This suggests that improvements in these behaviors were only captured in caregiver reports. Previous clinical studies have similarly found that outcomes reported by primary caregivers often show greater improvements compared to those reported by clinicians.47 This discrepancy may be attributed to the possibility that primary caregivers may have higher expectations for treatment outcomes, leading them to perceive and report more significant improvements, particularly when they are deeply invested in the intervention. These differences in reporting raise concerns about the reliability of subjective assessments and highlight the need for more objective quantitative measures, such as EEG48,49 or eye-tracking,50 to reduce expectation bias and provide a more accurate assessment of treatment efficacy.
In preclinical study, we also found that low-concentration sevoflurane exposure did not alter repetitive behaviors. Regarding the impact of sevoflurane on repetitive behaviors in autism, there is one study, to our knowledge, that reported 2% sevoflurane exposure effectively alleviated both social and repetitive behaviors in BTBR mice.20 This discrepancy may be due to differences in sevoflurane concentration. It is also possible that higher or differently timed doses of sevoflurane could affect repetitive behaviors, but such doses might carry additional risks or unintended effects, making them less viable in a therapeutic context. Given the unknown effects of high-concentration sevoflurane on the developing brain and other potential adverse reactions, our study adhered to use 1% sevoflurane for ASD treatment, as our previous research has already demonstrated that 1% sevoflurane exposure was sufficient to modulate the E/I ration in the brain and alleviate MK801-induced social deficits.19 Therefore, future research exploring different concentrations, timings, and even different autism mouse models will be necessary to further understand the therapeutic potential of sevoflurane in this context.
Limitations
It is important to acknowledge some inherent limitations of this study. First, the sample size of 20 participants is relatively small, and the potential for gender bias may limit the generalizability of the findings to the broader ASD population. Second, the complex classification and phenotypic heterogeneity of ASD make it challenging to generalize results across different subtypes, as the effects of interventions like sevoflurane may vary depending on individual characteristics. Third, the study relied solely on subjective assessment scales, which could introduce bias and may not fully capture nuanced changes in behavior and brain function. The development of objective measures, such as digital biomarkers, neuroimaging, or wearable technology, will be crucial in providing more accurate assessments of treatment outcomes in the future. Fourth, and most importantly, the study design must be improved from a single-arm design to a randomized controlled trial in future research. Without a control group, it is difficult to attribute the observed improvements solely to sevoflurane treatment, as these effects could potentially be due to placebo effects or other confounding factors. Lastly, because electrophysiological recordings and behavioral assessments were not systematically paired at the individual mouse level, we were unable to perform a robust correlation analysis between the magnitude of E/I ratio change and the degree of behavioral improvement within the BTBR+Sev group. Future studies that combine within-subject longitudinal electrophysiology and behavior will be important to directly test whether larger E/I normalization predicts greater amelioration of social deficits.
Conclusion
In summary, this pilot study demonstrates that exposure to low concentrations of sevoflurane improves social behavior in both BTBR mice and children with ASD, while leaving repetitive behaviors largely unchanged. At the mechanistic level, sevoflurane reduced the elevated E/I ratio in the mPFC of BTBR mice, suggesting that modulation of prefrontal inhibitory–excitatory balance may contribute to the observed behavioral benefits. Future randomized controlled trials and circuit-specific mechanistic studies will be necessary to establish causal relationships and to determine whether low-dose sevoflurane or related approaches can be developed into a targeted therapeutic strategy for ASD. Nevertheless, the present work provides initial proof-of-concept evidence that modulation of cortical E/I balance through low-dose anesthetic exposure may represent a promising avenue for improving social deficits in ASD.
Data Sharing Statement
The authors do not intend to share individual deidentified participant data from this study because of patient privacy protection and restrictions imposed by institutional regulations. However, the following study-related documents will be available upon reasonable request: study protocol, statistical analysis plan, informed consent form template, ethics approval letter. Requests for access to these materials can be made by contacting the corresponding author at: [email protected]. These documents will be available beginning 6 months after publication and will remain accessible for 5 years following publication.
Ethics Approval and Consent to Participate
The study was approved by the Ethics committee of Guangzhou Women and Children’s Medical Center, Guangzhou, China and written informed consent from patient or family member and registered in Chinese Clinical trial (ChiCTR1900027459). Written informed consents were obtained from patients or family members.
Consent for Publication
Written informed consent was obtained from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the grants from National Natural Science Foundation (Grant number 8247054228, Xingrong Song), Plan on enhancing scientific research in GMU (Grant number GMUCR2025-01011, Xingrong Song) and the grants from Guangzhou Municipal Science and Technology Programs (Grant numbers 2023A03J0899, Tianyun Zhao).
Disclosure
The authors declare no conflict of interest, financial or otherwise.
References
1. Hodges H, Fealko C, Soares N. Autism spectrum disorder: definition, epidemiology, causes, and clinical evaluation. Transl Pediatr. 2020;9(S1):S55–17. doi:10.21037/tp.2019.09.09
2. Thom RP, Pereira JA, Sipsock D, McDougle CJ. Recent Updates in Psychopharmacology for the Core and Associated Symptoms of Autism Spectrum Disorder. Curr Psychiatry Rep. 2021;23(12):79. doi:10.1007/s11920-021-01292-2
3. Maenner MJ, Warren Z, Williams AR, et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years — autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2020. MMWR Surveill Summ. 2023;72(2):1–14. doi:10.15585/mmwr.ss7202a1
4. Regier DA, Kuhl EA, Kupfer DJ. The DSM-5: classification and criteria changes. World Psychiatry. 2013;12(2):92–98. doi:10.1002/wps.20050
5. Bhandari R, Paliwal JK, Kuhad A. Neuropsychopathology of Autism Spectrum Disorder: complex Interplay of Genetic, Epigenetic, and Environmental Factors. In: Essa MM, Qoronfleh MW, editors. Personalized Food Intervention and Therapy for Autism Spectrum Disorder Management. Vol. 24. Cham: Springer International Publishing; 2020: 97–141. doi:10.1007/978-3-030-30402-7_4.
6. Persico AM, Ricciardello A, Lamberti M, et al. The pediatric psychopharmacology of autism spectrum disorder: a systematic review - Part I: the past and the present. Progress in Neuro-Psychopharmacology and Biological Psychiatry. 2021;110:110326. doi:10.1016/j.pnpbp.2021.110326
7. Lee E, Lee J, Kim E. Excitation/Inhibition Imbalance in Animal Models of Autism Spectrum Disorders. Biological Psychiatry. 2017;81:838–847. doi:10.1016/j.biopsych.2016.05.011
8. Rubenstein JLR, Merzenich MM. Model of autism: increased ratio of excitation/inhibition in key neural systems. Genes Brain and Behavior. 2003;2:255–267. doi:10.1034/j.1601-183X.2003.00037.x
9. Uzunova G, Pallanti S, Hollander E. Excitatory/inhibitory imbalance in autism spectrum disorders: implications for interventions and therapeutics. The World Journal of Biological Psychiatry. 2016;17:174–186. doi:10.3109/15622975.2015.1085597
10. Ko J, Choii G, Um JW. The balancing act of GABAergic synapse organizers. Trends in Molecular Medicine. 2015;21:256–268. doi:10.1016/j.molmed.2015.01.004
11. Henneberry E, Lamy M, Dominick KC, Erickson CA. Decades of Progress in the Psychopharmacology of Autism Spectrum Disorder. J Autism Dev Disord. 2021;51:4370–4394. doi:10.1007/s10803-021-05237-9
12. Brondino N, Fusar-Poli L, Panisi C, Damiani S, Barale F, Politi P. Pharmacological Modulation of GABA Function in Autism Spectrum Disorders: a Systematic Review of Human Studies. J Autism Dev Disord. 2016;46:825–839. doi:10.1007/s10803-015-2619-y
13. Han S, Tai C, Jones CJ, Scheuer T, Catterall WA. Enhancement of Inhibitory Neurotransmission by GABA A Receptors Having α 2,3 -Subunits Ameliorates Behavioral Deficits in a Mouse Model of Autism. Neuron. 2014;81:1282–1289. doi:10.1016/j.neuron.2014.01.016
14. Jerath A, Panckhurst J, Parotto M, et al. Safety and Efficacy of Volatile Anesthetic Agents Compared With Standard Intravenous Midazolam/Propofol Sedation in Ventilated Critical Care Patients: a Meta-analysis and Systematic Review of Prospective Trials. Anesthesia & Analgesia. 2017;124:1190–1199. doi:10.1213/ANE.0000000000001634
15. Sondekoppam RV, Narsingani KH, Schimmel TA, McConnell BM, Buro K, Özelsel TJ-P. The impact of sevoflurane anesthesia on postoperative renal function: a systematic review and meta-analysis of randomized-controlled trials. Can J Anesth/J Can Anesth. 2020;67:1595–1623. doi:10.1007/s12630-020-01791-5
16. MacIver MB. Anesthetic Agent-Specific Effects on Synaptic Inhibition. Anesthesia & Analgesia. 2014;119:558–569. doi:10.1213/ANE.0000000000000321
17. Guo F, Zhang B, Shen F, et al. Sevoflurane acts as an antidepressant by suppression of GluN2D‐containing NMDA receptors on interneurons. British J Pharmacology. 2024:16420. doi:10.1111/bph.16420.
18. Wu M, Li A, Guo Y, et al. GABAergic neurons in the nucleus accumbens core mediate the antidepressant effects of sevoflurane. European Journal of Pharmacology. 2023;946:175627. doi:10.1016/j.ejphar.2023.175627
19. Zhao T, Shi Z, Ling N, et al. Sevoflurane Ameliorates Schizophrenia in a Mouse Model and Patients: aPre-Clinical and Clinical Feasibility Study. CN. 2022;20:2369–2380. doi:10.2174/1570159X20666220310115846
20. Cui J, Park J, Ju X, et al. General Anesthesia During Neurodevelopment Reduces Autistic Behavior in Adult BTBR Mice, a Murine Model of Autism. Front Cell Neurosci. 2021;15:772047. doi:10.3389/fncel.2021.772047
21. Roque PS, Thörn Perez C, Hooshmandi M, et al. Parvalbumin interneuron loss mediates repeated anesthesia-induced memory deficits in mice. Journal of Clinical Investigation. 2023:133e159344. doi:10.1172/JCI159344.
22. Zhang W, Chen Y, Qin J, et al. Prolonged sevoflurane exposure causes abnormal synapse development and dysregulates beta-neurexin and neuroligins in the hippocampus in neonatal rats. Journal of Affective Disorders. 2022;312:22–29. doi:10.1016/j.jad.2022.05.115
23. Rey CC, Robert V, Bouisset G, et al. Altered inhibitory function in hippocampal CA2 contributes in social memory deficits in Alzheimer’s mouse model. IScience. 2022;25:103895. doi:10.1016/j.isci.2022.103895
24. Jurek L, Baltazar M, Gulati S, et al. Response (minimum clinically relevant change) in ASD symptoms after an intervention according to CARS-2: consensus from an expert elicitation procedure. Eur Child Adolesc Psychiatry. 2022;31:1–10. doi:10.1007/s00787-021-01772-z
25. Bolognani F, Del Valle Rubido M, Squassante L, et al. A Phase 2 clinical trial of a vasopressin V1a receptor antagonist shows improved adaptive behaviors in men with autism spectrum disorder. Sci Transl Med. 2019:
26. Wood JJ, Kendall PC, Wood KS, et al. Cognitive Behavioral Treatments for Anxiety in Children With Autism Spectrum Disorder: a Randomized Clinical Trial. JAMA Psychiatry. 2020;77:474. doi:10.1001/jamapsychiatry.2019.4160
27. Fewster DL, Uys C, Govender P. Interventions for Primary Caregivers of Children with Autism Spectrum Disorder: a cross-sectional study of current practices of stakeholders in South Africa. S Afr j Occup Ther. 2020;50. doi:10.17159/2310-3833/2020/vol50no1a7
28. Nordahl-Hansen A, Hart L, Øien RA. The Scientific Study of Parents and Caregivers of Children with ASD: a Flourishing Field but Still Work to be Done. J Autism Dev Disord. 2018;48:976–979. doi:10.1007/s10803-018-3526-9
29. Liu X, Ji J, Zhao G-Q. General anesthesia affecting on developing brain: evidence from animal to clinical research. J Anesth. 2020;34:765–772. doi:10.1007/s00540-020-02812-9
30. Robinson EJ, Lyne TC, Blaise BJ. Safety of general anaesthetics on the developing brain: are we there yet? BJA Open. 2022;2:100012. doi:10.1016/j.bjao.2022.100012
31. Davidson AJ, Disma N, De Graaff JC, et al. Neurodevelopmental outcome at 2 years of age after general anaesthesia and awake-regional anaesthesia in infancy (GAS): an international multicentre, randomised controlled trial. The Lancet. 2016;387:239–250. doi:10.1016/S0140-6736(15)00608-X
32. Sun LS, Li G, Miller TLK, et al. Association Between a Single General Anesthesia Exposure Before Age 36 Months and Neurocognitive Outcomes in Later Childhood. JAMA. 2016;315:2312. doi:10.1001/jama.2016.6967
33. Feng Y-P, Yang T-S, Chung C-H, Chien W-C, Wong C-S. Early childhood general anesthesia exposure associated with later developmental delay: a national population-based cohort study. PLoS One. 2020;15e0238289. doi:10.1371/journal.pone.0238289
34. Warner DO, Zaccariello MJ, Katusic SK, et al. Neuropsychological and Behavioral Outcomes after Exposure of Young Children to Procedures Requiring General Anesthesia. Anesthesiology. 2018;129:89–105. doi:10.1097/ALN.0000000000002232
35. Chen X, Zhou X, Yang L, et al. Neonatal Exposure to Low-Dose (1.2%) Sevoflurane Increases Rats’ Hippocampal Neurogenesis and Synaptic Plasticity in Later Life. Neurotox Res. 2018;34:188–197. doi:10.1007/s12640-018-9877-3
36. Chen C, Shen F-Y, Zhao X, et al. Low-Dose Sevoflurane Promotes Hippocampal Neurogenesis and Facilitates the Development of Dentate Gyrus-Dependent Learning in Neonatal Rats. ASN Neuro. 2015;7:175909141557584. doi:10.1177/1759091415575845
37. Jabaudon M, Zhai R, Blondonnet R, Bonda WLM. Inhaled sedation in the intensive care unit. Anaesthesia Critical Care & Pain Medicine. 2022;41:101133. doi:10.1016/j.accpm.2022.101133
38. Soukup J, Michel P, Christel A, Schittek GA, Wagner N-M, Kellner P. Prolonged sedation with sevoflurane in comparison to intravenous sedation in critically ill patients – a randomized controlled trial. Journal of Critical Care. 2023;74:154251. doi:10.1016/j.jcrc.2022.154251
39. Beck-Schimmer B, Restin T, Muroi C, Roth Z’Graggen B, Keller E, Schläpfer M. Sevoflurane sedation attenuates early cerebral oedema formation through stabilisation of the adherens junction protein beta catenin in a model of subarachnoid haemorrhage: a randomised animal study. European Journal of Anaesthesiology. 2020;37:402–412. doi:10.1097/EJA.0000000000001161
40. Bicks LK, Koike H, Akbarian S, Morishita H. Prefrontal Cortex and Social Cognition in Mouse and Man. Front Psychol. 2015;6:1. doi:10.3389/fpsyg.2015.01805
41. Trakoshis S, Martínez-Cañada P, Rocchi F, et al. Intrinsic excitation-inhibition imbalance affects medial prefrontal cortex differently in autistic men versus women. eLife. 2020;9:e55684. doi:10.7554/eLife.55684
42. Yizhar O, Fenno LE, Prigge M, et al. Neocortical excitation/inhibition balance in information processing and social dysfunction. Nature. 2011;477:171–178. doi:10.1038/nature10360
43. Selimbeyoglu A, Kim CK, Inoue M, et al. Modulation of prefrontal cortex excitation/inhibition balance rescues social behavior in CNTNAP2 -deficient mice. Sci Transl Med. 2017:
44. Veenstra-VanderWeele J, Cook EH, King BH, et al. Arbaclofen in Children and Adolescents with Autism Spectrum Disorder: a Randomized, Controlled, Phase 2 Trial. Neuropsychopharmacol. 2017;42:1390–1398. doi:10.1038/npp.2016.237
45. Zhang X, Shen F, Xu D, Zhao X. A lasting effect of postnatal sevoflurane anesthesia on the composition of NMDA receptor subunits in rat prefrontal cortex. Intl J of Devlp Neuroscience. 2016;54:62–69. doi:10.1016/j.ijdevneu.2016.01.008
46. Jiao Y, Fan H, Wang K, Lu S. Sevoflurane Impairs Short-Term Memory by Affecting PSD-95 and AMPA Receptor in the Hippocampus of a Mouse Model. Behav Neurol. 2019;2019:1068260. doi:10.1155/2019/1068260
47. Hacohen M, Stolar OE, Berkovitch M, et al. Children and adolescents with ASD treated with CBD-rich cannabis exhibit significant improvements particularly in social symptoms: an open label study. Transl Psychiatry. 2022;12:375. doi:10.1038/s41398-022-02104-8
48. Finn CE, Han GT, Naples AJ, Wolf JM, McPartland JC. Development of peak alpha frequency reflects a distinct trajectory of neural maturation in autistic children. Autism Research. 2023;16:2077–2089. doi:10.1002/aur.3017
49. Takarae Y, Zanesco A, Keehn B, Chukoskie L, Müller R, Townsend J. EEG microstates suggest atypical resting‐state network activity in high‐functioning children and adolescents with autism spectrum development. Developmental Science. 2022;25e13231. doi:10.1111/desc.13231
50. Avni I, Meiri G, Bar‐Sinai A, et al. Children with autism observe social interactions in an idiosyncratic manner. Autism Research. 2020;13:935–946. doi:10.1002/aur.2234
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.