Back to Journals » International Journal of Women's Health » Volume 17
Low Bone Mineral Density Is Associated with Higher Venous Thromboembolism Risk Scores in Postmenopausal Women
Authors Gong C, Ling F, Mao Y, Zhu X, Lu X, Wang J
Received 24 July 2025
Accepted for publication 4 November 2025
Published 17 November 2025 Volume 2025:17 Pages 4565—4575
DOI https://doi.org/10.2147/IJWH.S556076
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Everett Magann
Chen Gong,1,2,* Feng Ling,1,* Yichao Mao,3,* Xianyang Zhu,1 Xiao Lu,2 Jiaxing Wang1,3
1Department of Orthopedics, Taizhou School of Clinical Medicine, The Affiliated Taizhou People’s Hospital of Nanjing Medical University, Taizhou, Jiangsu, 225300, People’s Republic of China; 2Department of Rehabilitation, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, 210029, People’s Republic of China; 3Department of Orthopedics, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, 210029, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiaxing Wang, Email [email protected] Xiao Lu, Email [email protected]
Background: Venous thromboembolism (VTE) and osteoporosis are both prevalent and clinically significant conditions in postmenopausal women. These disorders share common risk factors, including estrogen deficiency and age-related physiological changes. Although emerging evidence suggests a link between reduced bone mineral density (BMD) and thrombotic events, current VTE risk assessment models do not incorporate BMD. This study aimed to investigate the association between BMD and VTE risk in postmenopausal women.
Methods: A total of 511 postmenopausal women hospitalized at the First Affiliated Hospital of Nanjing Medical University between January and December 2024 were enrolled. BMD was measured using dual-energy X-ray absorptiometry (DXA) and classified according to World Health Organization criteria. VTE risk was assessed using the Caprini Risk Assessment Score.
Results: Patients with osteoporosis had significantly higher Caprini scores compared to those with normal BMD (6.20 ± 3.20 vs 5.40 ± 2.60; p = 0.019). Additionally, levels of D-dimer 2 (DD2) and fibrinogen (FIB) increased as BMD decreased. Multivariate analysis identified the lowest BMD value as an independent predictor of elevated VTE risk (odds ratio = 0.02; 95% CI: 0.003– 0.164; p < 0.01). A negative correlation was observed between BMD and Caprini score (r = − 0.241; p < 0.01).
Conclusion: Lower BMD is independently associated with increased VTE risk in postmenopausal women. These findings suggest that BMD may serve as a novel biomarker for VTE risk. Incorporating BMD into existing risk assessment models and considering thromboprophylaxis for individuals with low BMD are recommended.
Keywords: postmenopausal women, venous thromboembolism, caprini score, bone mineral density
Introduction
Venous thromboembolism (VTE) and osteoporosis are two major global health concerns, each affecting millions of individuals worldwide.1,2 VTE, characterized by abnormal thrombus formation in the deep veins of the lower extremities, carries a substantial risk of pulmonary embolism—a life-threatening condition that ranks among the top five most common vascular diseases globally.3 Osteoporosis, defined by a progressive loss of bone mass and deterioration of bone microarchitecture, increases susceptibility to fragility fractures. Clinically, osteoporosis is primarily diagnosed through bone mineral density (BMD) assessment using dual-energy X-ray absorptiometry (DXA). With global population aging, the incidence of postmenopausal osteoporosis is expected to rise markedly, placing a growing burden on healthcare systems.4 Both VTE and osteoporosis represent significant public health challenges with overlapping epidemiological features. Understanding their potential pathophysiological connections is essential for integrated risk management.
The Caprini score, a widely validated clinical tool for VTE risk assessment, enables quantitative risk stratification by integrating several multidimensional risk factors, including age, surgical type, immobility status, and cancer history.5 It has been proven as an effective approach for individualized thromboprophylaxis selection following total hip arthroplasty. In addition, the score incorporates other key risk factors such as hormone therapy history, prior thrombotic events, and renal insufficiency—factors that highly overlap with established high-risk elements for osteoporosis.6 The Caprini score is an independent risk factor for all-cause mortality in patients with acute coronary syndrome, and the risk of all-cause death is significantly increased in high-risk patients with a score of 5 or higher.7
The scientific rationale for exploring associations between VTE and BMD is grounded in their shared risk factors—such as advanced age, female sex, and immobility—and supported by emerging mechanistic evidence. Crosstalk between vascular and bone biology is increasingly recognized. For example, warfarin-mediated inhibition of γ-carboxylation affects vitamin K–dependent osteocalcin activity, impairing bone integrity.8 Reduced mobility not only increases the risk of VTE by promoting venous stasis but also suppresses osteoblast activity due to inadequate mechanical loading on bone tissue, thereby establishing a self-perpetuating cycle of bone loss, impaired mobility, and heightened VTE risk.9,10 Moreover, osteoblasts and osteocytes regulate endothelial function and angiogenesis via mechanosensitive paracrine signaling.11 Prolonged immobilization further exacerbates thrombosis risk by promoting venous stasis, endothelial dysfunction, and a hypercoagulable state—core elements of Virchow’s triad.12
Given these interconnected mechanisms, investigating the relationship between BMD and thrombotic risk, particularly in elderly postmenopausal women, may provide valuable insights for identifying high-risk subpopulations. We hypothesize that in postmenopausal women, lower BMD is negatively associated with the Caprini score. Specifically, as BMD declines progressively from normal to osteopenia and then to osteoporosis, the Caprini score is expected to rise correspondingly. In this cross-sectional study, we examined the association between Caprini scores and BMD measurements at the lumbar spine (L1–L4) and bilateral femoral sites. This study seeks to enhance clinical insights into bone-vascular crosstalk, underscoring how low bone mineral density may signal thrombotic risk in women and thereby informing preventive strategies—such as integrated screening protocols and targeted thromboprophylaxis—to mitigate VTE and osteoporosis-related complications in female populations.
Methods
Study Design and Population
This study was approved by the Institutional Review Board (IRB) of the First Affiliated Hospital of Nanjing Medical University (Registration No.: 2025SR-616) and complies with the Declaration of Helsinki. Due to the retrospective nature of the data collection, the IRB waived the requirement for individual informed consent and all patient data were anonymized prior to analysis. Data were obtained from female patients who visited the Department of Orthopedics at the First Affiliated Hospital of Nanjing Medical University between January and December 2024. An initial cohort of 2153 patient records was retrieved from the hospital’s database.
Inclusion and Exclusion Criteria
Eligible participants were female patients who underwent orthopedic surgery during the study period and had complete medical records, including demographic information, laboratory test results, BMD measurements, and clinical variables required for Caprini score calculation. Exclusion criteria were as follows: premenopausal status (confirmed by menstrual and reproductive history); use of medications known to affect BMD, such as glucocorticoids, bisphosphonates, or selective estrogen receptor modulators; and incomplete or missing medical records. After applying these criteria, a total of 511 postmenopausal women were included in the final analysis, as illustrated in Figure 1.
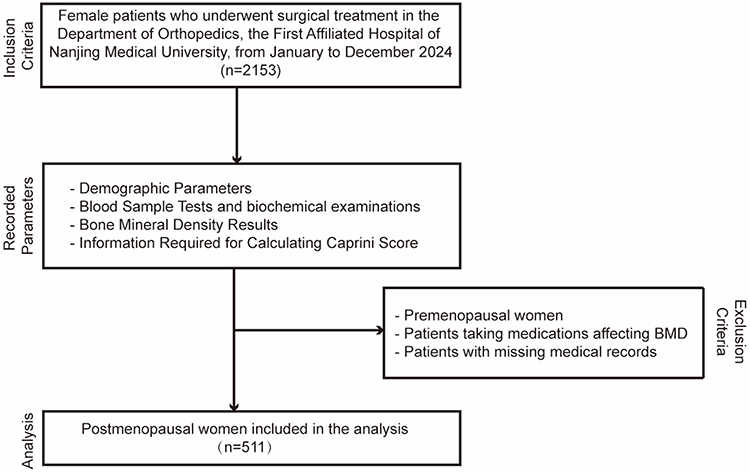 |
Figure 1 Flowchart Showing the Inclusion and Exclusion Criteria for Postmenopausal Women in This Study. |
Recorded Parameters
Demographic data collected included age, height, weight, menopausal duration, and self-reported comorbidities such as diabetes, hypertension, and osteoporosis. Laboratory assessments encompassed coagulation markers and lipoprotein(a) (Lpa), which was included due to its recognized association with thrombotic diseases. BMD measurements of the lumbar spine (L1–L4) and bilateral femoral sites were obtained using DXA and interpreted by certified technicians. Based on L1–L4 T-scores, patients were classified into three groups according to World Health Organization (WHO) criteria: normal BMD (T-score ≥ −1.0), osteopenia (−2.5 < T-score < −1.0), and osteoporosis (T-score ≤ −2.5). Clinical information relevant to venous thromboembolism (VTE) risk—including type of surgery, immobilization status, and cancer history—was extracted to calculate Caprini scores.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics (version 27.0) and GraphPad Prism (version 9.0). The distribution of continuous variables was assessed with the Shapiro–Wilk test. Normally distributed data are presented as mean ± standard deviation, while categorical variables are expressed as frequencies and percentages. Group comparisons were conducted using one-way ANOVA for normally distributed continuous variables, the Kruskal–Wallis test for non-normally distributed variables, and chi-square tests for categorical variables. Pearson correlation and linear regression analyses were performed to evaluate associations between Caprini scores and clinical parameters, including BMD. Logistic regression was used to identify independent predictors of high VTE risk (defined as Caprini score >5), adjusting for age and body mass index (BMI). Results are reported as odds ratios (OR) with corresponding 95% confidence intervals (CI). Statistical significance was set at p < 0.05.
Results
Baseline Characteristics and DXA Results
The study included 511 postmenopausal women categorized into normal BMD (n = 124), osteopenia (n = 205), and osteoporosis (n = 182) groups (Table 1). DXA results demonstrated significant differences in T-scores and BMD among the groups: femoral neck T-scores were 0.31 ± 0.48 for the normal group, −1.09 ± 0.66 for osteopenia, and −1.44 ± 0.73 for osteoporosis, with corresponding BMD values of 0.70 ± 0.17, 0.55 ± 0.13, and 0.43 ± 0.08, respectively (p < 0.01). The osteoporosis group exhibited the lowest lumbar spine T-score (−2.46 ± 1.75) and BMD (0.43 ± 0.08), confirming severe bone loss. Clinically, age, menopausal duration, smoking status, and blood pressure did not differ significantly between groups; however, BMI showed a significant decrease from normal (25.23 ± 3.13) to osteopenia (24.73 ± 3.42), while unexpectedly, the osteoporosis group had a higher BMI (25.77 ± 2.79, p < 0.01). These findings confirm a gradient of bone loss across BMD categories, with osteoporosis demonstrating the most pronounced skeletal deficits.
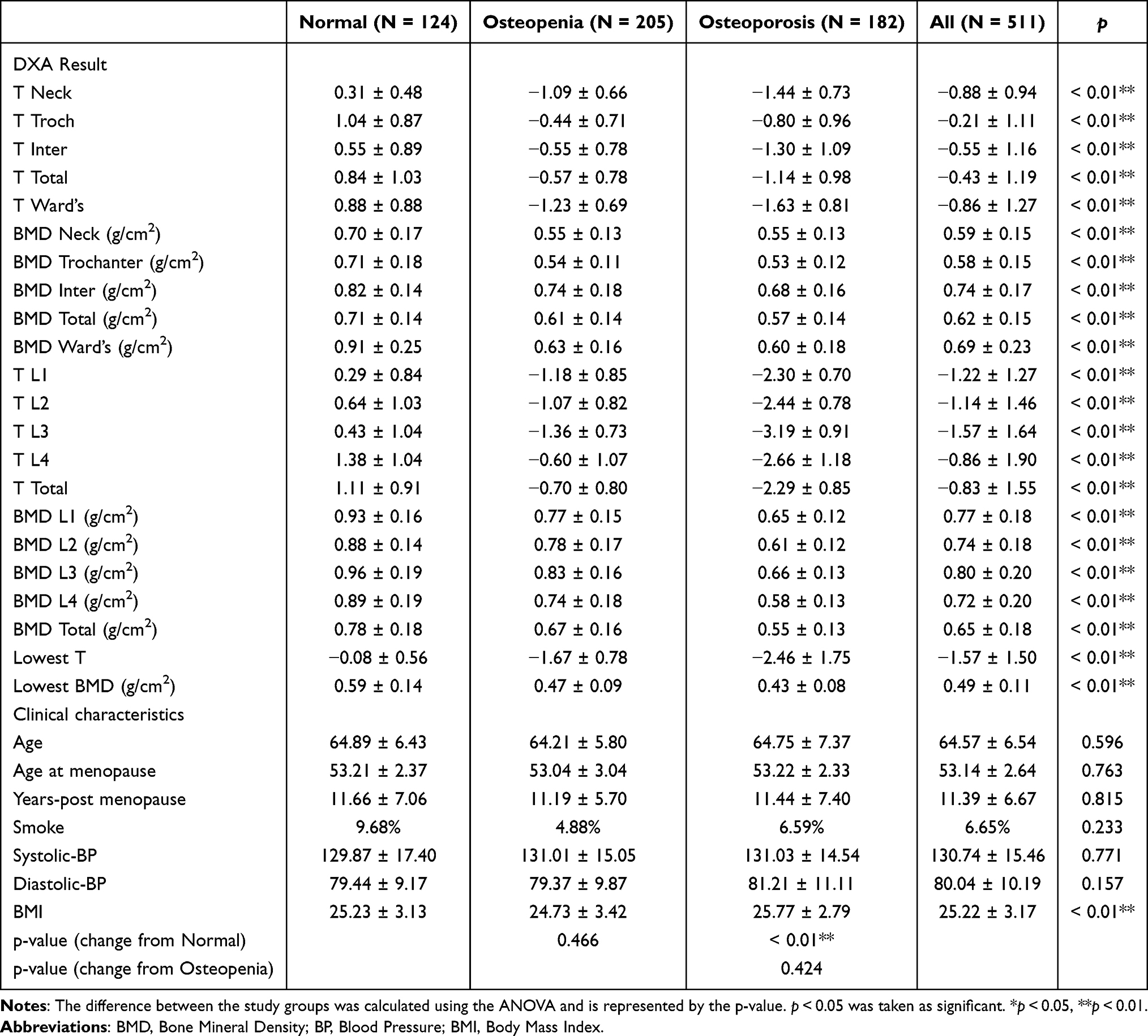 |
Table 1 Baseline Characteristics and DXA Results |
Coagulation Function Indices and VTE Risk Scores
Coagulation function indices and VTE risk scores differed significantly across BMD groups (Table 2), with prothrombin time (PT) and PT-INR showing only marginal overall differences (p = 0.069 and p = 0.053, respectively) and limited pairwise significance. In contrast, activated partial thromboplastin time (APTT) progressively shortened with declining BMD (overall p < 0.01), from 28.02 ± 1.35 s (normal) to 27.26 ± 1.71 s (osteopenia) and 26.88 ± 1.50 s (osteoporosis), with significant reductions in both osteopenia and osteoporosis versus normal (p < 0.01) and a marginal further decrease in osteoporosis versus osteopenia (p = 0.053). Fibrinogen (FIB) levels rose stepwise (overall p < 0.01), from 2.39 ± 0.57 g/L (normal) to 2.50 ± 0.47 g/L (osteopenia) and 2.61 ± 0.49 g/L (osteoporosis), with significance only between osteoporosis and normal (p < 0.01), linking elevated substrate reserves to heightened thrombus formation risk in advanced osteoporosis. Thrombin time (TT) exhibited a nonlinear pattern (overall p < 0.01), with a significant shortening in osteoporosis (15.18 ± 0.90 s) versus osteopenia (15.54 ± 1.12 s; p < 0.01). D-dimer (DD2) surged sharply (overall p < 0.01), from 0.29 ± 0.12 μg/mL (normal) to 0.50 ± 1.00 μg/mL (osteopenia) and 1.61 ± 1.99 μg/mL (osteoporosis), with significant elevations in osteoporosis versus both normal and osteopenia (p < 0.01), underscoring markedly increased thrombotic activity. Lipoprotein(a) [Lp(a)] trended inversely (overall p < 0.01), dropping significantly from 206.63 ± 104.00 (normal) to 151.31 ± 87.82 (osteopenia) and 163.24 ± 95.17 (osteoporosis; p < 0.01 versus normal for both, no difference between osteopenia and osteoporosis; p = 0.648), potentially serving as an intermediary marker in BMD-coagulation dysregulation. The Caprini score, reflecting VTE risk, increased progressively (overall p = 0.019), from 5.40 ± 2.60 (normal) to 5.60 ± 2.60 (osteopenia) and 6.20 ± 3.20 (osteoporosis), with significance between osteoporosis and normal (p = 0.026). These findings suggest that postmenopausal women with lower BMD exhibit prothrombotic alterations in coagulation function and an increased risk of VTE.
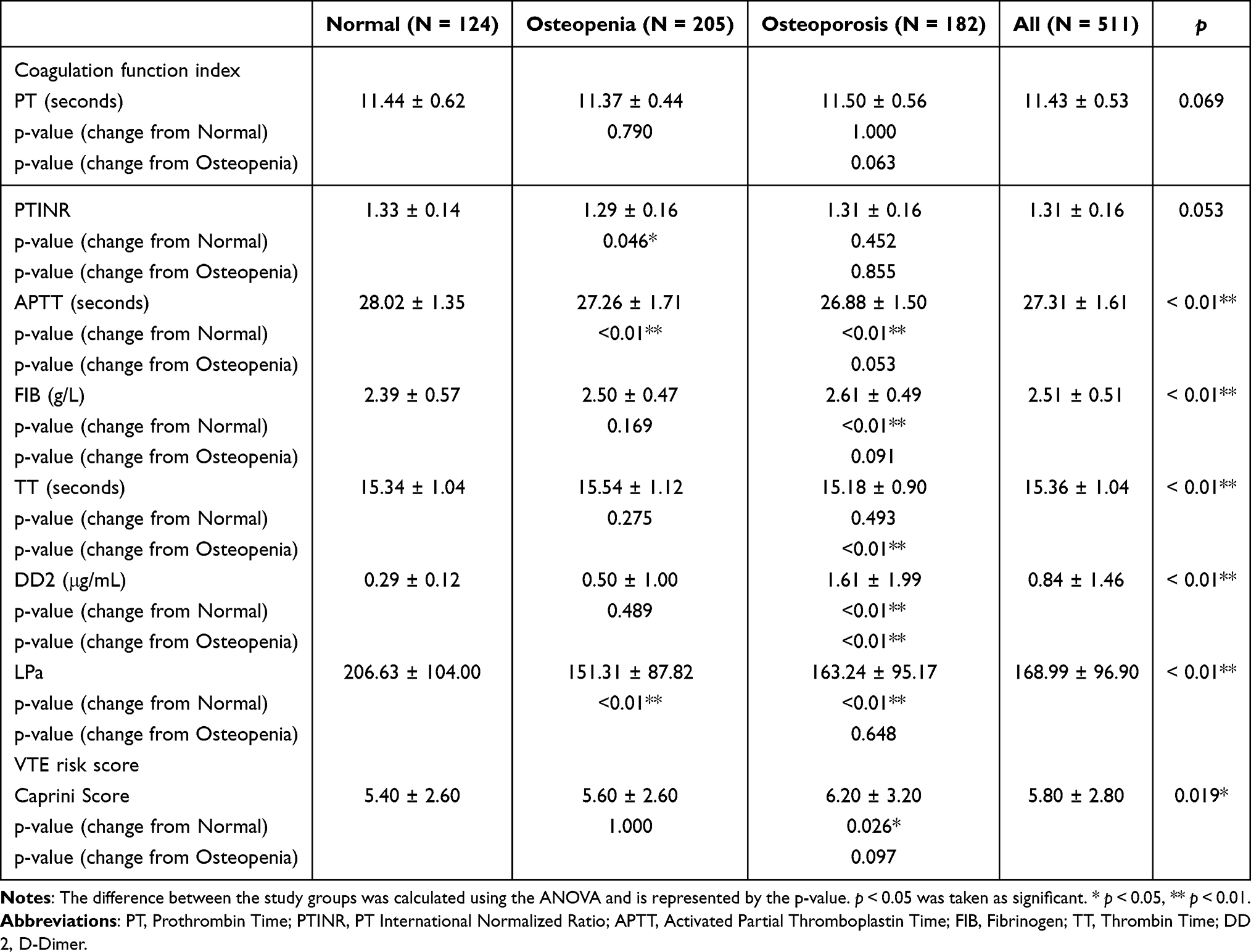 |
Table 2 Coagulation Function Indices and VTE Risk Scores |
Comparison Between High and Low VTE Risk Groups
The Caprini score classifies individuals with scores ≥5 as “very high risk” for VTE.13 Accordingly, we divided the cohort into two groups based on this cutoff (≥5 vs <5) for analysis (Table 3). DXA results revealed that participants with Caprini scores ≥5 had significantly lower BMD and more negative T-scores at multiple skeletal sites compared to those with scores <5. The intertrochanteric T-score in the high-risk group was significantly lower than that in the low-risk group (−0.65 ± 1.15 vs −0.39 ± 1.16, p = 0.013). There were no significant differences in T-scores at other sites (femoral neck T-score: −0.93 ± 0.94 vs −0.80 ± 0.95, p = 0.122; trochanter T-score: −0.26 ± 1.10 vs −0.14 ± 1.13, p = 0.247; Ward’s area T-score: −0.90 ± 1.21 vs −0.76 ± 1.25, p = 0.148; lowest total T-score: −1.64 ± 0.57 vs −1.54 ± 0.46, p = 0.722). BMD was significantly lower in the high-risk group at multiple skeletal sites. Femoral neck BMD (0.57 ± 0.14 vs 0.61 ± 0.17, p < 0.01), trochanter BMD (0.55 ± 0.14 vs 0.61 ± 0.16, p < 0.01), total BMD (0.59 ± 0.14 vs 0.67 ± 0.15, p < 0.01), and Ward’s area BMD (0.67 ± 0.22 vs 0.71 ± 0.24, p = 0.025) were all significantly lower than in the low-risk group. The lowest BMD (0.46 ± 0.10 vs 0.52 ± 0.13, p < 0.01) was also significantly lower. There were no significant differences in lumbar spine L1-L4 BMD (L1: 0.70 ± 0.17 vs 0.71 ± 0.19, p = 0.189; L2: 0.73 ± 0.18 vs 0.76 ± 0.19, p = 0.166; L3: 0.79 ± 0.19 vs 0.81 ± 0.20, p = 0.297; L4: 0.71 ± 0.20 vs 0.74 ± 0.21, p = 0.136). These results indicate a consistent pattern of reduced hip and total BMD in postmenopausal women at high VTE risk. Clinically, age (p = 0.389), menopausal duration (p = 0.869), and BMI (p = 0.578) did not differ significantly between groups. Regarding coagulation indices, PT-INR was higher in the ≥5 group (1.33 ± 0.16 vs 1.28 ± 0.14, p < 0.01), while TT was shorter (15.24 ± 1.02 s vs 15.55 ± 1.04 s, p < 0.01). Other markers including Lpa, APTT, FIB, and DD2 showed no significant differences. These results indicate that postmenopausal women with elevated VTE risk, as reflected by higher Caprini scores, exhibit lower BMD and certain alterations in coagulation parameters, suggesting a potential link between thrombotic risk and bone health.
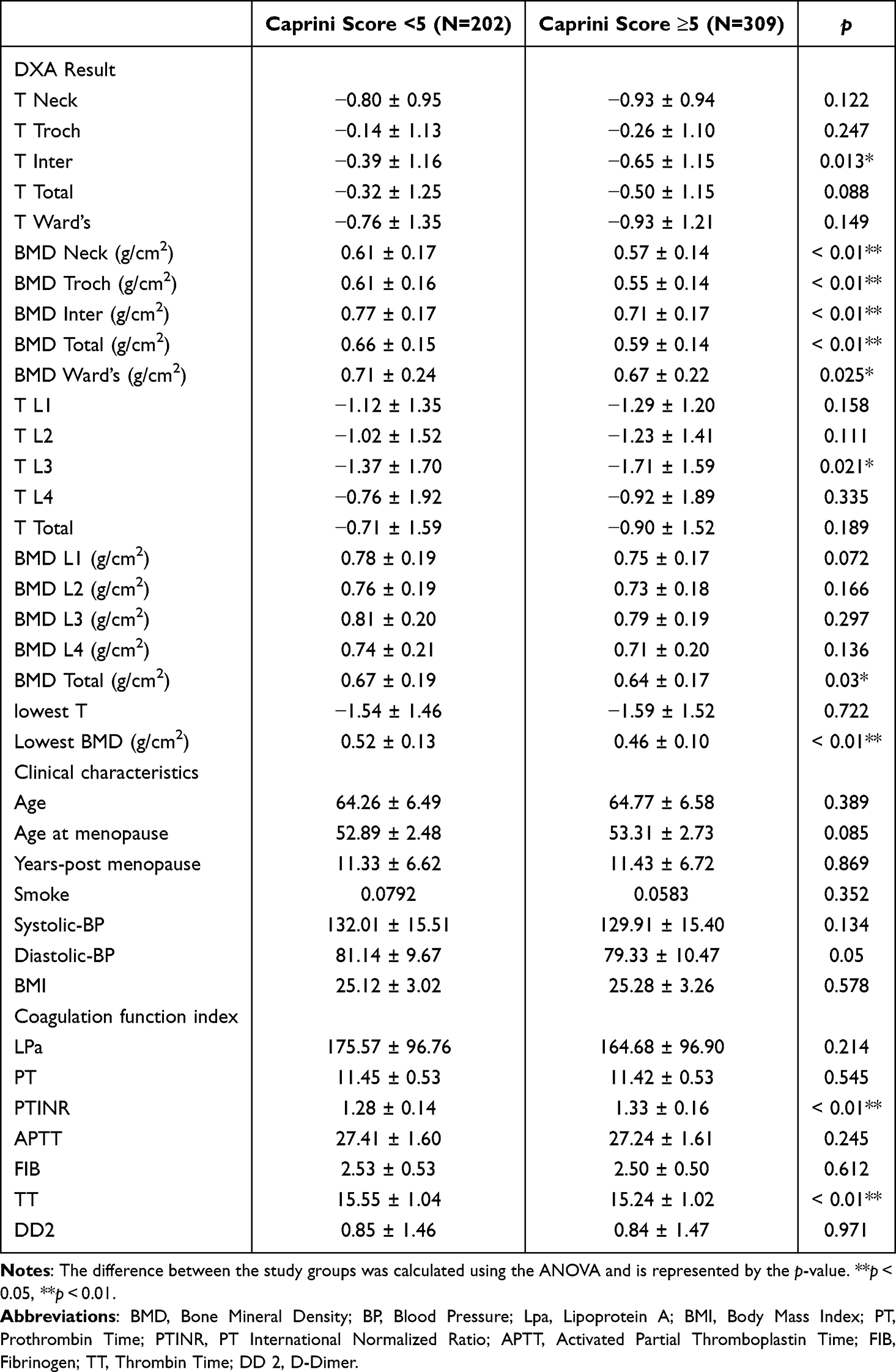 |
Table 3 Comparison Between High and Low VTE Risk Groups |
Univariate and Multivariate Logistic Regression of VTE Risk Groups
Univariate and multivariate logistic regression analyses were performed to examine the association between BMD, coagulation function indices, and VTE risk, adjusting for covariates including BMI, age, blood pressure, and smoking status (Table 4). The lowest BMD emerged as a strong independent predictor of VTE risk, with univariate analysis yielding an OR of 0.011 (95% CI: 0.002–0.061, p < 0.01) and multivariate analysis confirming this association (OR = 0.02; 95% CI: 0.003–0.164; p < 0.01), indicating that lower BMD significantly elevates VTE risk. In contrast, coagulation parameters such as Lpa, PT, APTT, FIB, TT, and DD2 did not show significant independent associations with VTE risk in multivariate models. Although TT showed a significant negative correlation with VTE risk in univariate analysis (OR = 0.745, p < 0.01), this association lost significance after adjusting for confounders. These results highlight BMD as a potentially valuable biomarker for VTE risk stratification in postmenopausal women, whereas traditional coagulation markers have limited predictive value once clinical variables are accounted for.
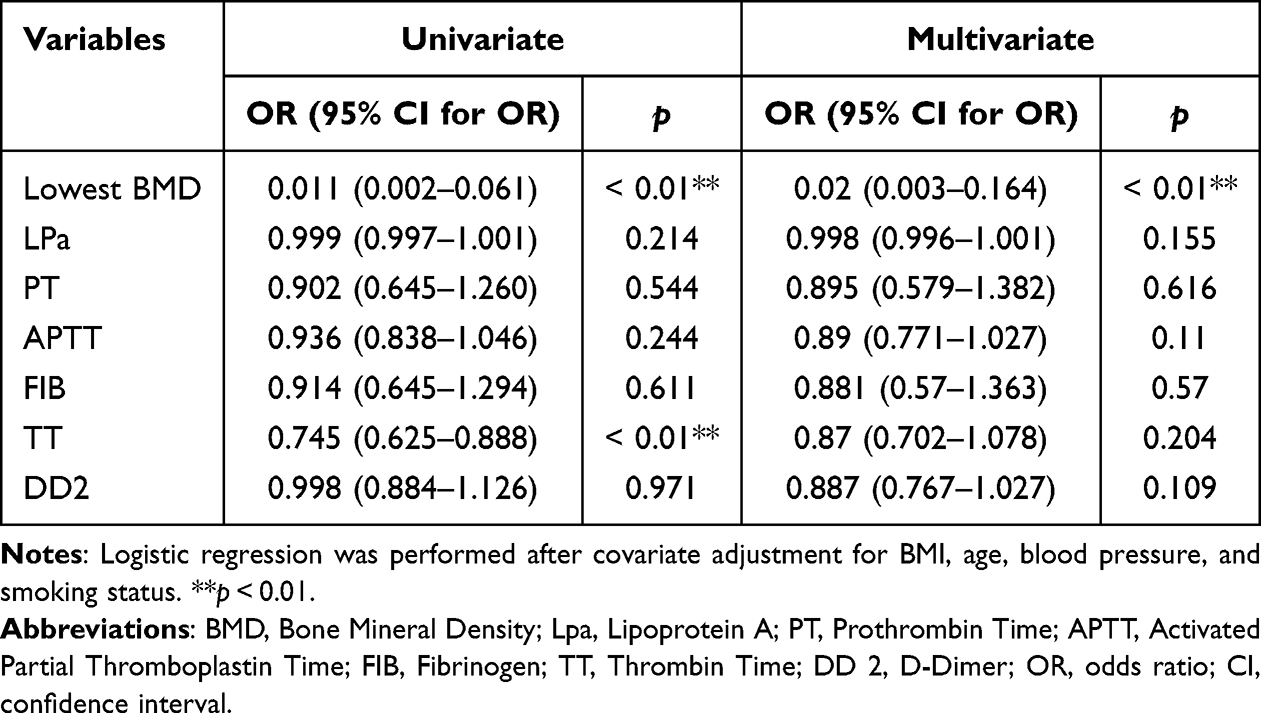 |
Table 4 Univariate and Multivariate Logistic Regression of VTE Risk Groups |
Pearson Correlation and Linear Regression Analysis of Caprini Score
To investigate factors influencing the Caprini score, Pearson correlation analysis was performed. A significant negative correlation was observed between the lowest BMD and the Caprini score (r = −0.241, p < 0.01) (Table 5), indicating that lower BMD is associated with a higher risk of thromboembolism. Among the coagulation indices, TT also showed a significant negative correlation with the Caprini score (r = −0.142, p < 0.01), whereas other markers—including PT, APTT, FIB, DD2, and Lpa—exhibited weak or non-significant associations. Interestingly, the lowest BMD was positively correlated with both TT (r = 0.450, p < 0.01) and Lpa (r = 0.216, p < 0.01), suggesting a potential physiological link between bone metabolism and coagulation pathways. The results provided partial support for the core hypothesis that, in postmenopausal women, lower bone mineral density (BMD) is negatively associated with the Caprini score, with the score expected to increase progressively as BMD declines from normal to osteopenia and then to osteoporosis. Specifically, linear regression analyses across all three bone health groups revealed significant negative correlations between BMD and Caprini scores. In the normal bone mass group, each 1 g/cm2 increase in BMD was associated with an average decrease of 4.356 points in the Caprini score (slope = −4.356, p = 0.0163, R2 = 0.046). In the osteopenia group, this association was more pronounced, with 8.865-point decrease per 1 g/cm2 BMD increase (slope = −8.865, p < 0.0001, R2 = 0.085). In the osteoporosis group, the score decreased by 7.043 points for each 1 g/cm2 BMD increase (slope = −7.043, p = 0.0237, R2 = 0.028) (Figure 2), indicating a significant but attenuated relationship. While the overall negative correlation between BMD and Caprini score was consistently confirmed, the anticipated continuous escalation of the score with progressive BMD decline exhibited stage-specific variations: the impact of BMD was most evident during the osteopenia stage, whereas in the osteoporosis stage, confounding factors—such as inflammation and immobilization—diminished the explanatory power of BMD,14–16 resulting in a less linear progression of the score. Collectively, these findings reinforce the independent predictive value of BMD for thromboembolic risk and highlight a potential interaction between bone health and coagulation function.
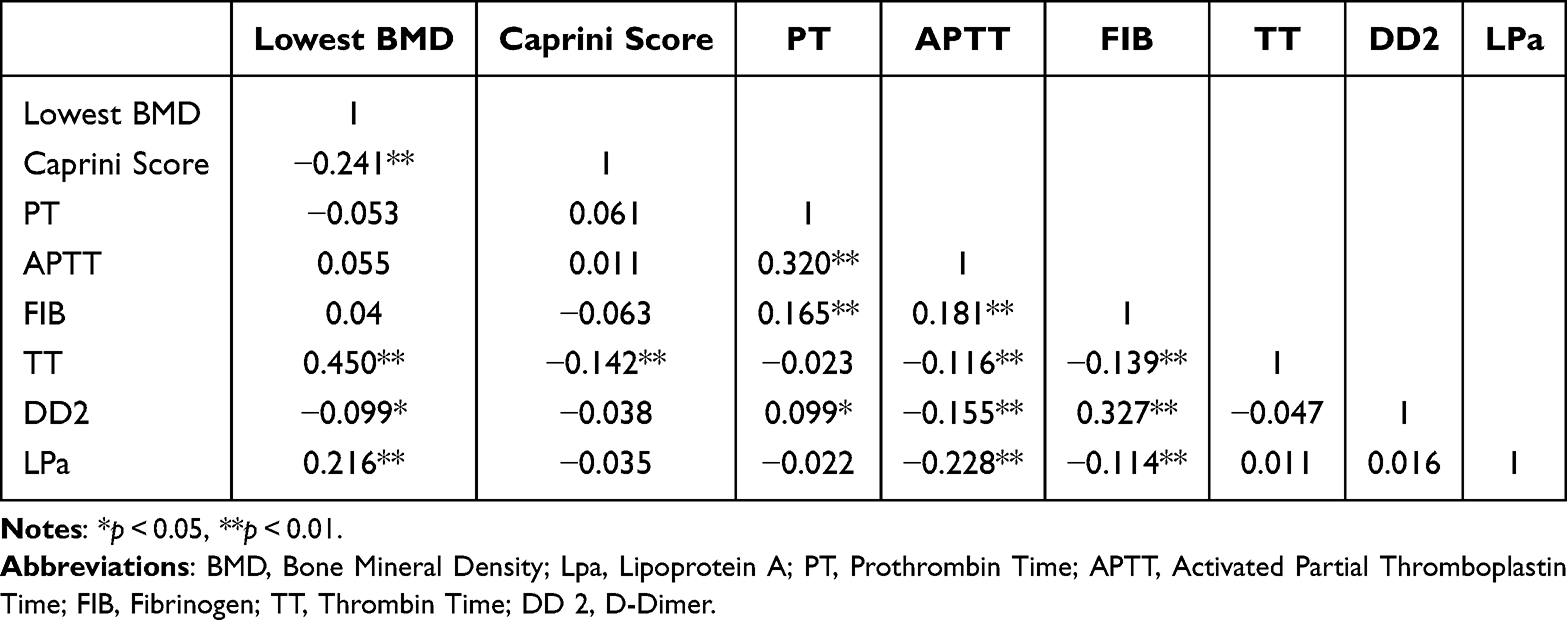 |
Table 5 Pearson Analysis of Caprini Score |
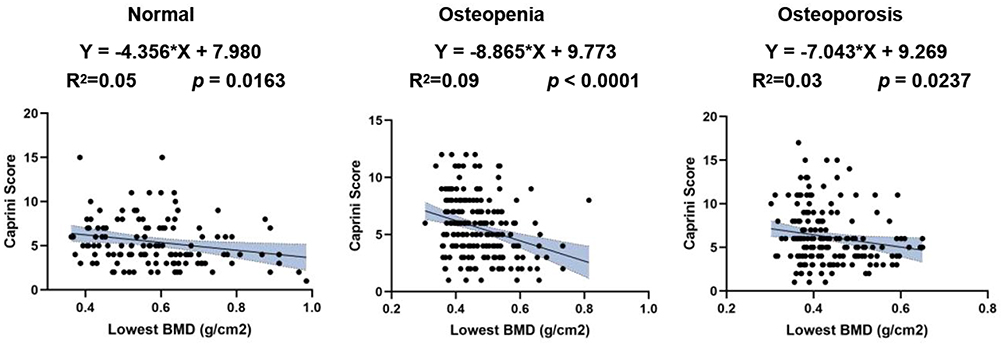 |
Figure 2 Subgroup linear regression analyses revealed that Caprini scores exhibit differing patterns across different BMD categories. |
Discussion
This study clarifies the significant clinical association between low bone mineral density (BMD) and elevated risk of deep vein thrombosis (VTE) in postmenopausal women. Multivariate logistic regression analysis confirmed that the lowest tertile of BMD, across femoral neck, trochanter, and lumbar spine sites, independently predicts a moderate-to-high VTE risk (OR=0.02, 95% CI: 0.003–0.164, p < 0.01) even after adjusting for age, BMI, and comorbidities. This finding is consistent with the gradient increase in Caprini scores from the normal BMD group (5.40±2.60) to the osteoporosis group (6.20±3.20, p = 0.019), accompanied by prothrombotic changes in coagulation markers (reduced APTT, elevated FIB and DD2) in the low-BMD group, which is of great reference value for clinical risk assessment.
The inverse correlation between BMD and VTE risk provides a new perspective for the clinical assessment of VTE in postmenopausal women. Clinical studies have confirmed that the vitamin K-dependent pathway plays a key role in both bone metabolism and the coagulation system, and the researchers provided evidence for this association.17 In clinical practice, postmenopausal estrogen deficiency is an important common risk factor. Previous studies reveal its impact from the perspectives of bone metabolism and vascular function respectively, suggesting that in clinical practice, the dual effect of this factor on BMD and VTE risk should be considered comprehensively.18,19 These mechanisms involve a complex interplay between pro‑inflammatory cytokines, complement activation, and endothelial dysfunction, all of which may contribute to both bone resorption and thrombus formation.20,21
Inflammatory mechanisms play a significant role in the clinical link between bone mineral density BMD and VTE, with existing evidence supporting the involvement of immune-mediated cross-activation in this association.22 Inflammatory mechanisms may be the potential mechanism underlying the significant differences observed in coagulation indices (APTT, FIB, TT, DD2, LPa) among different bone status subgroups. This study did not directly include traditional inflammatory markers (such as C-reactive protein), which requires follow-up studies. Notably, in this study, the body mass index (BMI) in the osteoporosis group was elevated (25.77 ± 2.79), significantly higher than in the osteopenia group (24.73 ± 3.42) and the normal bone mass group (25.23 ± 3.13; overall p < 0.01). Although elevated BMI is a well-established risk factor for thrombosis—and osteoporosis itself confers additional thrombotic risk—the osteopenia group paradoxically exhibited a relative decrease in BMI, underscoring the complex interplay between adiposity, bone health, and vascular outcomes in postmenopausal women.23 This paradox may reflect underlying metabolic adaptations or chronic inflammation, indicating that BMI alone may not reliably indicate either protection against bone loss or a reduced risk of thrombotic events.24,25
From a clinical perspective, the results of this study extend previous findings on the relationship between BMD and vascular health. Prior evidence supports the association between BMD and vascular-related risks, including cardiovascular diseases such as VTE, from multiple pathophysiological perspectives.26,27 This study uniquely establishes lowest BMD as an independent predictor of VTE risk in postmenopausal women, via univariate and multivariate logistic regression analysis. Univariate analysis revealed a significant association (OR = 0.011; 95% CI: 0.002–0.061; p < 0.01), which persisted after multivariate adjustment for traditional coagulation markers and confounders (OR = 0.02; 95% CI: 0.003–0.164; p < 0.01), confirming that lower BMD strongly elevates VTE risk. In contrast, traditional markers showed limited multivariate predictive value: DD2 (OR = 0.887; 95% CI: 0.767–1.027; p = 0.109) and FIB (OR = 0.881; 95% CI: 0.57–1.363; p = 0.57) lacked significance, likely due to confounders like inflammation or trauma, as noted in prior studies.28,29
Clinically relevant limitations of this study include potential selection bias inherent in the hospital-based sample, which may limit the generalizability of findings to the broader population. Additionally, the cross-sectional design precludes causal inference, which should be taken into account when applying the findings to clinical practice. Future clinical studies should prioritize multicenter prospective cohort studies with expanded sample coverage and long-term follow-up to systematically validate the clinical value of BMD as a biomarker for VTE risk. Meanwhile, exploring VTE risk assessment and intervention strategies based on BMD will help improve the clinical management of bone-vascular comorbidities in postmenopausal women.
Conclusion
This study is the first to confirm that lower BMD in postmenopausal women serves as an independent predictor of VTE risk, outperforming traditional coagulation markers. These findings substantiate our hypothesis that the Caprini score rises progressively as BMD declines from normal to osteopenia and then to osteoporosis. Clinically, integrating BMD into tools like the Caprini score enables streamlined bone-thrombosis risk stratification, optimizing personalized preventive strategies and facilitating early identification of high-risk patients.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Abdulwehab S, Kedir F. Deep vein thrombosis in Ethiopia: a systematic review and meta-analysis, 2025. Thromb J. 2025;23(1):68. doi:10.1186/s12959-025-00760-6
2. Albrecht AP, Kistler-Fischbacher M, De Godoi Rezende Costa Molino C, et al. Prevalence and incidence of osteoporotic vertebral fractures in community-dwelling European older adults: an observational analysis of the DO-HEALTH trial. Osteoporos Int. 2025;36(6):1077–1088. doi:10.1007/s00198-025-07489-y
3. Wendelboe AM, Raskob GE. Global burden of thrombosis: epidemiologic aspects. Circ Res. 2016;118(9):1340–1347. doi:10.1161/CIRCRESAHA.115.306841
4. Reginster J-Y, Burlet N. Osteoporosis: a still increasing prevalence. Bone. 2006;38(2 Suppl 1):S4–9. doi:10.1016/j.bone.2005.11.024
5. Leikin JB. Venous thromboembolism prophylaxis using the Caprini score. Dis Mon. 2019;65(8):248. doi:10.1016/j.disamonth.2018.12.004
6. Krauss ES, Segal A, Dengler N, Cronin M, Pettigrew J, Simonson BG. Utilization of the caprini score for risk stratification of the arthroplasty patient in the prevention of postoperative venous thrombosis. Semin Thromb Hemost. 2022;48(4):407–412. doi:10.1055/s-0042-1742739
7. Li W, Wang Y, Li D, et al. The caprini risk score for early prediction of mortality in patients with acute coronary syndrome. J Cardiovasc Nurs. 2023;38(5):472–480. doi:10.1097/JCN.0000000000000949
8. Ding W, Xu C, Zhang Y, Chen H. Advances in the understanding of the role of type-H vessels in the pathogenesis of osteoporosis. Arch Osteoporos. 2020;15(1):5. doi:10.1007/s11657-019-0677-z
9. Patel MJ, Chang KH, Sykes MC, Talish R, Rubin C, Jo H. Low magnitude and high frequency mechanical loading prevents decreased bone formation responses of 2T3 preosteoblasts. J Cell Biochem. 2009;106(2):306–316. doi:10.1002/jcb.22007
10. Zouhal H, Jayavel A, Parasuraman K, et al. Effects of exercise training on anabolic and catabolic hormones with advanced age: a systematic review. Sports Med. 2022;52(6):1353–1368. doi:10.1007/s40279-021-01612-9
11. Shen N, Maggio M, Woods I, et al. Mechanically activated mesenchymal-derived bone cells drive vessel formation via an extracellular vesicle mediated mechanism. J Tissue Eng. 2023;14:20417314231186918. doi:10.1177/20417314231186918
12. van Duijnhoven NTL, Bleeker MWP, de Groot PCE, et al. The effect of bed rest and an exercise countermeasure on leg venous function. Eur J Appl Physiol. 2008;104(6):991–998. doi:10.1007/s00421-008-0854-z
13. Cronin M, Dengler N, Krauss ES, et al. Completion of the updated caprini risk assessment model (2013 Version). Clin Appl Thromb Hemost. 2019;25:1076029619838052. doi:10.1177/1076029619838052
14. Zhang L, Zheng Y-L, Wang R, Wang X-Q, Zhang H. Exercise for osteoporosis: a literature review of pathology and mechanism. Front Immunol. 2022;13:1005665. doi:10.3389/fimmu.2022.1005665
15. Alele JD, Kamen DL. The importance of inflammation and vitamin D status in SLE-associated osteoporosis. Autoimmun Rev. 2010;9(3):137–139. doi:10.1016/j.autrev.2009.05.001
16. Khoury MI. Osteoporosis and inflammation: cause to effect or comorbidity? Int J Rheum Dis. 2024;27(10):e15357. doi:10.1111/1756-185X.15357
17. Theuwissen E, Smit E, Vermeer C. The role of vitamin K in soft-tissue calcification. Adv Nutr. 2012;3(2):166–173. doi:10.3945/an.111.001628
18. Heshmati HM, Khosla S, Robins SP, O’Fallon WM, Melton LJ, Riggs BL. Role of low levels of endogenous estrogen in regulation of bone resorption in late postmenopausal women. J Bone Miner Res. 2002;17(1):172–178. doi:10.1359/jbmr.2002.17.1.172
19. Reckelhoff JF. Cardiovascular disease, estrogen deficiency, and inflammatory cytokines. Hypertension. 2006;48(3):372–373. doi:10.1161/01.HYP.0000235866.97871.9d
20. Foley JH, Conway EM. Cross Talk Pathways Between Coagulation and Inflammation. Circ Res. 2016;118(9):1392–1408. doi:10.1161/CIRCRESAHA.116.306853
21. Zhou P, Zheng T, Zhao B. Cytokine-mediated immunomodulation of osteoclastogenesis. Bone. 2022;164:116540. doi:10.1016/j.bone.2022.116540
22. Cheng C-H, Chen L-R, Chen K-H. Osteoporosis due to hormone imbalance: an overview of the effects of estrogen deficiency and glucocorticoid overuse on bone turnover. Int J Mol Sci. 2022;23(3):1376. doi:10.3390/ijms23031376
23. Weitz JI, Farjat AE, Ageno W, et al. Influence of body mass index on clinical outcomes in venous thromboembolism: insights from GARFIELD-VTE. J Thromb Haemost. 2021;19(12):3031–3043. doi:10.1111/jth.15520
24. Arjunan D, Prasad TN, Das L, Bhadada SK. Osteoporosis and Obesity. Indian J Orthop. 2023;57(Suppl 1):218–224. doi:10.1007/s43465-023-01052-9
25. Gkastaris K, Goulis DG, Potoupnis M, Anastasilakis AD, Kapetanos G. Obesity, osteoporosis and bone metabolism. J Musculoskelet Neuronal Interact. 2020;20(3):372–381.
26. Wani K, Sabico S, Veronese N, Al-Masri AA, Al-Daghri NM. Ten-year atherosclerotic cardiovascular disease risk score in post-menopausal women with low bone mineral density. Aging Clin Exp Res. 2025;37(1):56. doi:10.1007/s40520-025-02957-1
27. Kanis JA, Oden A, Johnell O, Jonsson B, de Laet C, Dawson A. The burden of osteoporotic fractures: a method for setting intervention thresholds. Osteoporos Int. 2001;12(5):417–427. doi:10.1007/s001980170112
28. Mahmoodi BK, Cushman M, Anne Næss I, et al. Association of traditional cardiovascular risk factors with venous thromboembolism: an individual participant data meta-analysis of prospective studies. Circulation. 2017;135(1):7–16. doi:10.1161/CIRCULATIONAHA.116.024507
29. Tsai AW, Cushman M, Rosamond WD, Heckbert SR, Polak JF, Folsom AR. Cardiovascular risk factors and venous thromboembolism incidence: the longitudinal investigation of thromboembolism etiology. Arch Intern Med. 2002;162(10):1182–1189. doi:10.1001/archinte.162.10.1182
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.