Back to Journals » Patient Preference and Adherence » Volume 8
Lost to follow-up for appointments in a dedicated dry eye clinic
Authors Poon KH, Yeo S, Tong L
Received 21 May 2014
Accepted for publication 5 June 2014
Published 9 October 2014 Volume 2014:8 Pages 1409—1418
DOI https://doi.org/10.2147/PPA.S68147
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Video abstract presented by Sharon Yeo
Views: 131
Kip Hoe Poon,1 Sharon Yeo,1 Louis Tong1–4
1Singapore Eye Research institute, Singapore; 2Singapore National Eye Centre, Singapore; 3Yong Loo Lin School of Medicine, Singapore; 4Duke-NUS Graduate Medical School, Singapore
Objective: Dry eye is a prevalent condition with significant socioeconomic burden. This study evaluates the extent and reasons for loss to follow-up (LTF) in a dedicated dry eye clinic. LTF refers to patient who discontinued visits for >2 years.
Method: The proportion of patients LTF and the demographics in a cohort of dry eye patients (2006 to 2010) were determined. A telephone survey was prospectively conducted for patients who were LTF.
Results: Of 505 patients, 240 (47.5%) were LTF. Associated demographic factors for LTF were male sex, non-Chinese ethnicity, and age group <30 years old (all P<0.05). The reasons for LTF through the telephone survey (response rate 77.9%) were categorized into three broad groups, stabilized dry eye condition (47%), personal/social factors (25%) and perceived insufficiency of healthcare delivery (28%). Only two (1.1%) were considered as management failures. The younger patients (age <50 years) were more likely to become LTF (P<0.001) due to stabilized dry eye disease, compared to older patients who were more likely to be LTF due to personal/social reasons (P=0.02). Poor communication and service factors under healthcare delivery were found to be higher (P=0.002) in those who visited once before they were LTF (8.5%) compared to those who visited multiple times before they were LTF (0.1%).
Conclusion: LTF was relatively common in hospital-based dry eye management. Female and older patients were less likely to stop consultation. Stabilized dry eye condition, common in younger patients, was the most common reason for LTF. Elderly patients have difficulty attending clinics due to nonmedical problems, which may require a more holistic approach.
Keywords: public health, health services utilization, human, cohort study, clinical study
Introduction
Dry eye is defined as a chronic and multifactorial disease of the tear and ocular surface resulting in symptoms of discomfort, visual disturbances, and ocular surface damage.1 The disease is highly prevalent in many parts of the world. Demographic risk factors include Asian ethnicity, female sex, and old age.2,3 In the United States alone, the accumulated approximated consumer spending on artificial tears for dry eye treatment reached up to $32 million United States dollars (US$32 million) per year.3 In a single hospital pharmacy in Singapore, spending on dry eye lubricants and related medications amounted to US$1.5 million over 1 year.4
Dry eye disease is the most common ocular surface dysfunction encountered in a general ophthalmic clinic.5 In 2006, Singapore National Eye Center (SNEC) established a specialized dry eye clinic in order to improve management of dry eye patients.6 There is currently no definitive cure for dry eye disease. The mainstay for dry eye treatment focuses on palliative relief7 and use of immunosuppressive drugs, which may not be effective in treatment of more chronic and severe dry eye.
These facts suggest that the accumulation of dry eye patients may continue perpetually in the clinic. If this is true, it will be essential to determine the rate of the increase and allocate healthcare resources accordingly. On the other hand, if the overall number of dry eye patients does not increase, it is important to find out what proportion is lost to follow-up (LTF). Patients may be LTF for different reasons. These reasons could indicate success of disease management, or reveal risk factors that obstruct them from visiting the clinic. Therefore, understanding the reasons for the LTF is crucial. As far as we know, no studies have examined LTF for dry eye patients in a dry eye clinic.
There are various reasons why patients do not remain in a dry eye service. The disease condition itself may be explanatory for the LTF. Dry eye is known to fluctuate in severity and presenting symptoms.1 The patient may cease visits if there is a substantial symptom-free period. In addition, patients suffering from mild dry eye may stop clinic consultations if they perceived the symptoms to be tolerable in daily life. One study has reported that most cases of dry eye in the community are mild (54%),8 though this proportion may not apply to a hospital scenario.
Secondly, personal/social factors may deter further visits. These factors may include, for example, the direct and indirect costs incurred by the patient for treatment,8 as well as the inconvenience of commuting, since there is only one national center that has a dedicated dry eye service in Singapore. Moreover, dry eye disease may be associated with anxiety and depression,9,10 and these conditions may affect a decision to visit the dry eye clinic. Since dry eye is predominantly present in aging people, many patients in the dry eye clinic also have other pressing systemic diseases such as rheumatoid arthritis, heart disease, liver cirrhosis, or malignancies.11,12 Such patients will consider dry eye to have a lower priority in their hospital visits.
Lastly, there may be reasons pertaining to healthcare services or providers. Health care providers refer to health care professionals directly involved in the diagnosis, management, and care of the patients; these include ophthalmologists, optometrists, receptionists, pharmacists, and nurses at the eye center. Dry eye patients suffering from severe dry eye symptoms or anxiety may require more consultations for immediate symptoms relief or reassurance, respectively. However, the availability of healthcare resources13 may not be adequate to accommodate all patients, therefore resulting in patients frequently switching providers and become LTF.
In this clinic-based study, we reported the proportion of a cohort of patients referred to the dry eye clinic between the years 2006 and 2010 that were LTF. Next, through a structured phone survey, we recorded and analyzed the underlying reasons for patients being LTF. A tertiary aim was to explore the possible demographic factors associated with patients being LTF.
Materials and methods
Ethical consideration
The research study was conducted in accordance with good clinical practice guidelines and obtained approval from the Central Institutional Review Board of Singapore Healthcare Services. Informed verbal consent was obtained from the patients during the telephone survey before proceeding with the study. Contact and background information were collected from each patient only for the purpose of this study.
Study population
The clinic-based survey comprised the cohort of patients registered during the period of August 2006 to December 2010 at the SNEC private and subsidized dry eye clinic. This is a tertiary referral clinic run by a single ophthalmologist on two fixed mornings every week. Patients visiting the dry eye clinic are primarily dry eye referrals from SNEC and other hospitals.
The majority of dry eye patients attended repeat visits at different time intervals after the initial consultation, depending on the severity of the dry eye disease and taking into consideration the patient’s circumstances. For example, after the first consultation, severe cases were reviewed after 3–6 months, moderate cases were reviewed after 6–9 months, and mild cases were reviewed after 9 months to 1 year. Dry eye cases requiring topical corticosteroid treatment or other special circumstances, like treatment trials, could be seen again in 4–6 weeks.
Patients who did not have an appointment 2 years after their last consultation at the dry eye clinic were considered to be LTF, and eligible for enrollment into this study. From the prospective database of all dry eye patients who attended the clinic, a list of 505 patients was obtained, and 240 (47%) patients, considered to be LTF, were enrolled. Out of these individuals (Figure S1), 187 participated in the telephone survey, giving an overall response rate of 77.9%. The other 53 eligible patients cannot be contacted.
From a previous study, patients who visited this dry eye clinic in SNEC had differing degrees of severity of dry eye.14 The mean Schirmer’s I test without anesthesia (standard deviation) was 12.7 (8.8) mm at 5 minutes, whereas the mean fluorescein tear breakup time was 3.0 (1.5) seconds.14
Study procedure
We analyzed the demographic factors, including sex, ethnicity, and age group of each individual who visited the dry eye clinic between the years 2006 to 2010. From the SNEC computerized appointment system, the frequencies of visits of the dry eye patients before discontinuing follow-up treatment were also recorded.
Each participant of the phone survey was questioned on why they had stopped visiting the clinic. The primary reasons were grouped into three categories: disease-related, personal/social, and healthcare service factors.
Statistical analysis
Analysis was carried out for demographic factors, stratified for patients who were LTF visits with the clinic and patients who were still visiting the clinic. An online statistical calculator was used for chi square analysis of categorical variables. Chi-square test was used to assess statistical significance. Fisher’s exact test was used if the expected value was less than 5. A P-value less than 0.05 was considered statistically significant.
Results
Participants in the study population
Five hundred and five patients were referred to and reviewed at the dry eye service between 2006 and 2010. Subsequent to their clinic review, 240 of these patients (47.5%) were considered to be LTF according to our definition (Table 1). Males and younger patients were more likely to be LTF (P<0.001). The mean age was 49 (±15.8) years, compared to 57 (±11.2) years for patients still visiting the clinic. There was a greater proportion of non-Chinese (17.9%) patients in the LTF group (P<0.001), compared to 6.8% in the follow-up group. Among the 505 patients who attended the clinic, the percentage of patients afflicted with systemic diseases, apart from diabetes, was not different between the LTF group and patients still attending the clinic (Table S1). There was an overrepresentation of patients with diabetes mellitus in the LTF group.
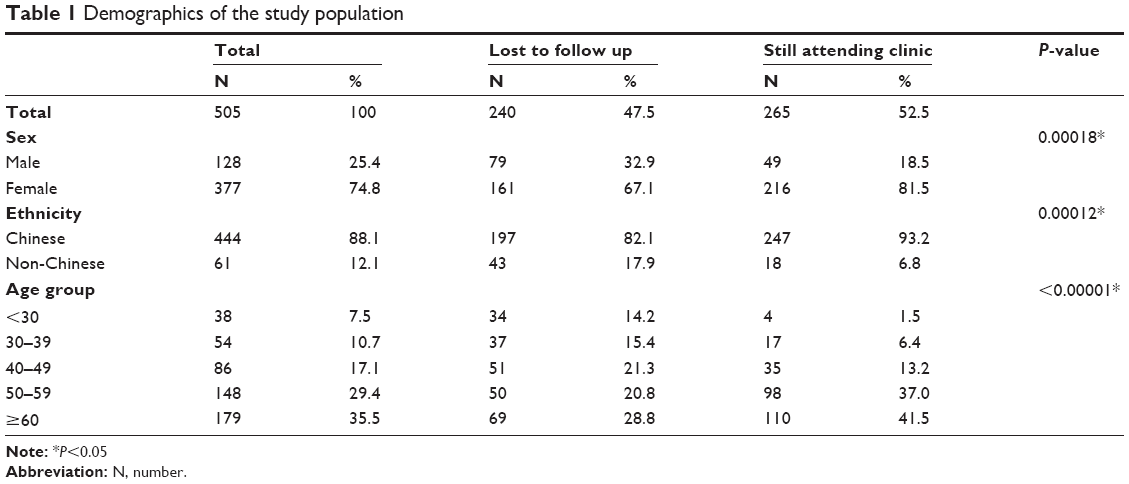 | Table 1 Demographics of the study population |
One hundred and eighty-seven patients responded to the telephone survey (Figure S1). Of the 240 shortlisted patients, seven patients did not have a Singapore address, and 53 cases of Singapore residents could not be contacted by telephone and were considered as nonrespondents in this study (Table 2). The respondents and nonrespondents did not differ in terms of sex or age. There was a significantly higher proportion of foreigners or non-Singapore residents in the nonresponding group compared to responders (P=0.002).
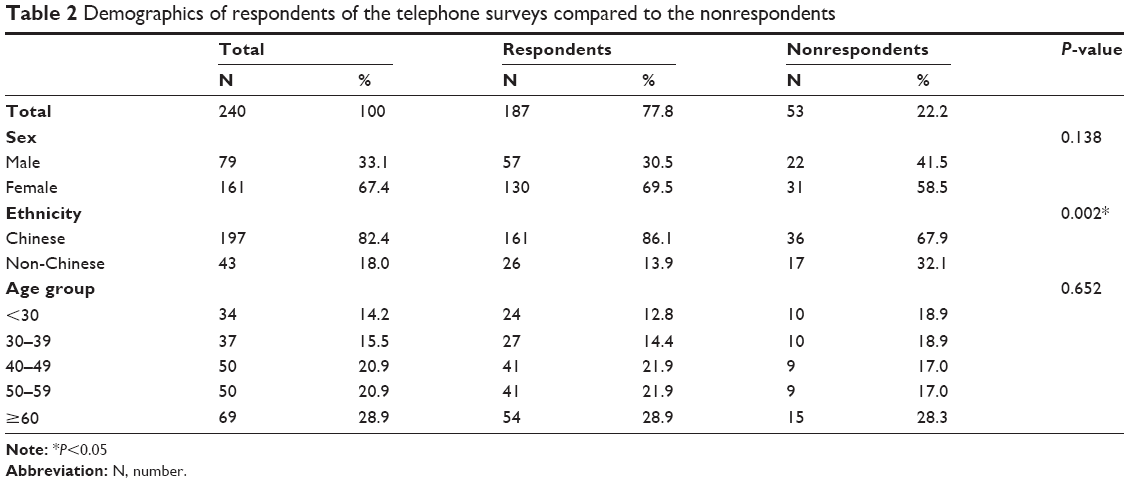 | Table 2 Demographics of respondents of the telephone surveys compared to the nonrespondents |
It was important to determine which patients were consulted only once at the dry eye service, since their reasons might differ from patients who returned for follow-up visits. One hundred and nine (45.4%) of the 240 patients had only one clinic visit before they were LTF (adding up leftmost bars of Figure S2A and B). The number of patients who had one visit was similar between respondents and nonrespondents (P>0.05).
Reasons for LTF
Out of the 187 respondents to the telephone survey, two patients experienced major social impacts in their daily lives due to dry eye disease (one changed jobs and another was forced into unforeseen retirement) and are considered to be treatment failures. They will be described below.
We were able to classify the reasons for patients being LTF into three broad groups for the remaining 185 patients (Figure 1A). These groups were 1) disease factors; 2) patient personal factors; and 3) hospital or system factors (Table 3). The bulk of these patients (47%) did not need to attend further visits and fell into the first group as their dry eye conditions can be self-managed. The others did not want to attend due to personal/social reasons (second group, 28%) or were in the third group: health service delivery insufficiencies (25%). The proportions of these reasons were similar amongst patients who had been through multiple consultations and patients who consulted only once (Figure 1B).
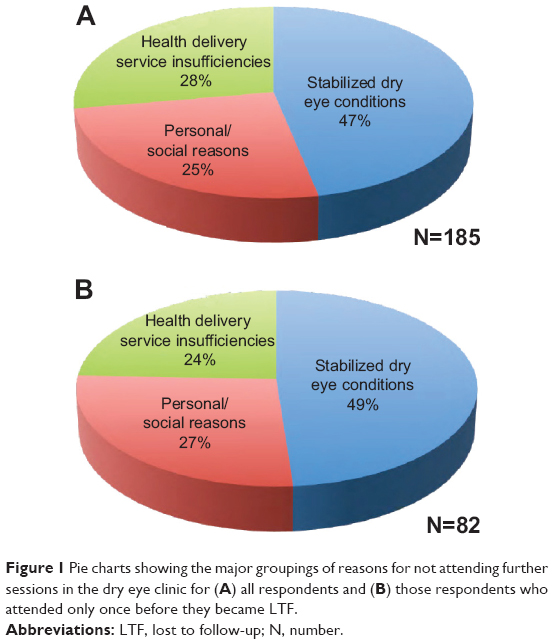 | Figure 1 Pie charts showing the major groupings of reasons for not attending further sessions in the dry eye clinic for (A) all respondents and (B) those respondents who attended only once before they became LTF. |
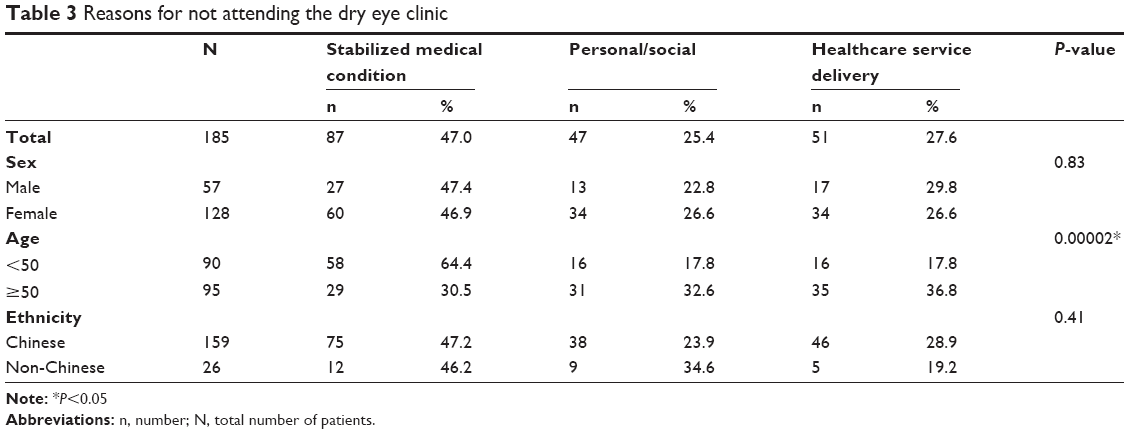 | Table 3 Reasons for not attending the dry eye clinic |
Demographic factors were examined for the three groups for the reasons for discontinuing clinic visits (Table 3). Age group was significantly associated with stabilization of the disease (P<0.001) (Group 1) or personal/social factors (P=0.02) (Group 2). Patients who were younger than 50 years were more likely to cope with their dry eye condition without visiting the clinic (Group 1). On the other hand, patients 50 years of age or older were more susceptible to LTF due to personal/social factors (Group 2).
Patients with stabilized dry eye conditions (group 1)
Eighty-seven patients were not required to attend the clinic when their dry eye conditions stabilized and the disease could be self-managed. The impact of the dry eye disease did not significantly affect their daily lives. Among participants with stabilized dry eye conditions (blue area in Figure 1A), about one-third did not have any further dry eye symptoms (Figure 2A). The proportion was similar among those who had only one visit (Figure 2B) or more than one visit (Figure 2C). Although 23 (27%) out of 87 patients did not perceive any improvement in symptoms, they did not need to attend the clinic because, through counseling and other measures, they had learned to cope without requiring further consults (Figure 2A).
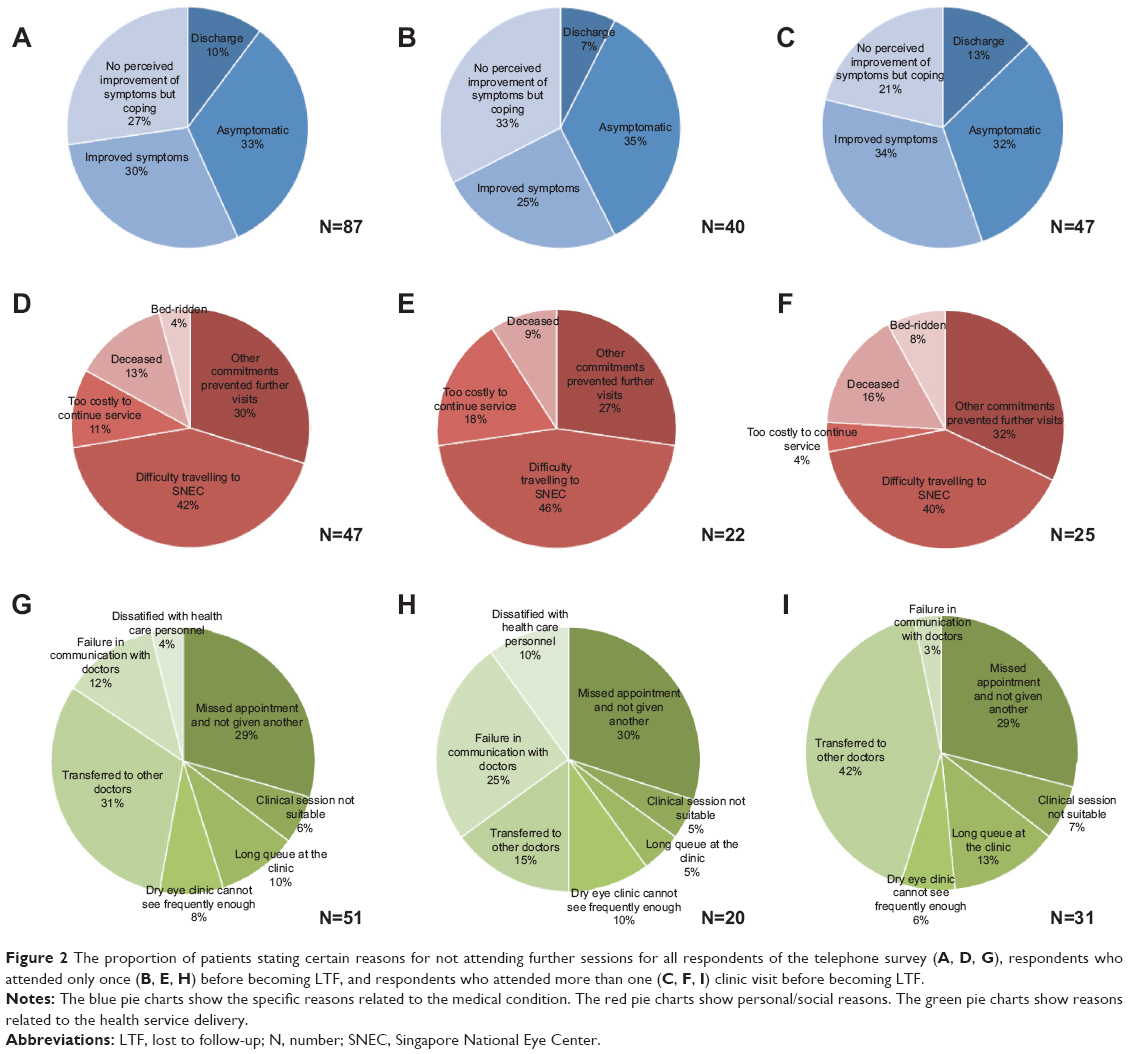 | Figure 2 The proportion of patients stating certain reasons for not attending further sessions for all respondents of the telephone survey (A, D, G), respondents who attended only once (B, E, H) before becoming LTF, and respondents who attended more than one (C, F, I) clinic visit before becoming LTF. |
Patients who could not attend for personal/social reasons (group 2)
Personal and social reasons include perceived obstacles to attending further visits. In this group of patients (25%, red area in Figure 1A), the most common reason (more than one-third of patients) was physical inability to go to the center or a preference for another healthcare center that was more geographically accessible (Figure 2D). The second most common reason in this group was having other commitments during the course of treatment (Figure 2D).
Not surprisingly, patients who came for only one visit were more likely to cite the affordability or expenses associated with the consultation as reasons compared to patients who came for more than one visit, although this difference was not statistically significant (P=0.235) (Figure 2E and F). There were no bed-ridden patients amongst those who attended only once.
Health service delivery was unable to meet the patient’s requirements (group 3)
Reasons pertaining to this group encompass various perceived health service delivery insufficiencies. In this category, 51 (27.6%) of the 185 respondents in Figure 1A, several reasons were cited (Figure 2G–I). All dry eye patients were seen in the service on Wednesday and Friday mornings only. The reasons within this group were further subcategorized, and the proportion of patients in each category was shown in percentages out of a total of 51 patients. In one subcategory, 12 (24%) patients were either unhappy with the frequency, timing, or waiting times of these clinics.
Another 15 (29%) patients had missed appointment(s) and did not obtain further appointment dates for some reason. The hospital’s policy was to send out three further dates. We could not rule out failure to send out these reminders, but it was also possible that the patients have forgotten about the appointments despite reminders.
A third subcategory of 16 (31%) patients had been moved to another clinic for a different medical problem (eg, glaucoma) either in the same center or elsewhere, but had not yet been given further appointments to the dry eye clinic. These patients currently might have further management related to dry eye at these clinics, and it was also possible that they may return to the dry eye service in the future.
A minority of eight (16%) patients was unwilling to be seen at the dry eye clinic because of service factors related to healthcare personnel and failure in communication with doctors. These reasons include failure of healthcare providers to offer sufficient counseling, or explanation on the need for continuation of treatment and the perceived lack of empathy of healthcare providers. These factors were significantly higher (P=0.002) in patients who visited the clinic only once compared to those with more than one visit before becoming LTF (Figure 2H and Figure I), suggesting that patients who considered these factors to be important may decide to drop out as early as after the first visit.
Patients with unsatisfactory treatment outcomes directly related to dry eye
Two patients suffered from persistence of dry eye symptoms that have significantly impacted their daily lives. The effects included reduced ability to work and perform daily activities. Unlike the other patients in the survey, the nonattendance was deemed directly related to the dry eye condition.
One patient, a 45-year-old Chinese woman, had to retire prematurely from her admin assistant job due to the severity of her dry eye condition, which affected her ability to work in an intensive computer-usage environment. As a result of the loss of income, she was unable to afford further consultation expenses. In this hospital, the usual practice for financial help is through a physician referral to the in-house medical social worker.
Another patient, a 46-year-old Chinese woman, had to change from a desk-bound job to one which required lesser hours of computer use. This patient felt that the treatment given was not able to help her to function in her work even after four visits and was discouraged from seeking further treatment from the clinic.
Discussion
In the cohort, 47.5% of patients were LTF in the dry eye clinic over 5 years; 45.4% had only visited the clinic once. Up to 50% of the patient’s LTF occurred early after the initial visit to the clinic. Associated factors for patient’s being LTF were male sex, non-Chinese ethnicity, and an age of <30 years old. The most common reason was related to dry eye condition having stabilized (47%), especially for the younger patients. Older patients were more likely to be LTF due to personal/social factors. Patients unhappy with communication with healthcare providers or system were more likely to be LTF after one visit than after more visits. Only two (1.1%) participants were considered as management failures.
As far as we are aware, there were no clinic-based studies on the extent of LTF in dry eye patients. Previous studies have reported that dry eye reduced patient’s quality of life (QOL).15,16 Although it has been found that the decrease in QOL may be related to aberrations and difficulty performing daily activities,17 other aspects, such as the contribution of socioeconomic burden to QOL, have not been quantified. In addition, the possible relationship between a decrease in QOL and LTF has not been explored.
One would expect that the patients with only one visit to be more likely to have reasons such as being transferred to other doctors, since they might have been referred for a confirmed diagnosis only and not future management. Not surprisingly, some of the patients who came to the clinic only once included foreigners who came for an opinion and left Singapore afterwards. However, when comparing patients with only one visit and those with more than one visit before becoming LTF, our findings showed that apart from the perceived healthcare insufficiencies, the reasons for becoming LTF were similar.
We found men were more likely to be LTF and women more likely to attend dry eye clinics. Interestingly, in the Singapore general population, the prevalence of dry eye was found to be equal in both sexes,18,19 but among dry eye patients seeking treatment at the clinic, there was a female preponderance.20–22 This may suggest that male patients are either less likely to consult or more likely to leave after consultation. This may be due to either a faster control of dry eye in men, or that the impact of dry eye on daily activities is less significant in males. These underlying reasons cannot be easily determined by the current protocol; we intend to explore these in future qualitative research using focus groups. Regardless of the underlying explanation, the sex composition of dry eye disease in the current clinic was similar to those studies in other parts of the world, where the majority of people suffering from dry eyes were female.3
Ethnicity analysis revealed significantly more non-Chinese were LTF compared to ongoing patients. This result is expected, as the non-Chinese group may consist of non-Singapore residents who came to Singapore for consultation or who only resided for a short duration in Singapore.
Young people (younger than 30 years of age) may be more likely than older people to be LTF. Young people’s dry eye conditions were related to environmental factors such as computer use or contact lens wear.23,24 These dry eye conditions may be managed by lifestyle changes and do not require frequent examination of the eye.
On the other hand, older patients (≥50 years of age) were more inclined to become LTF due to social/personal factors. Older people could experience age-related problems such as lowered physical strength, reduced spending power (in the case of retired individuals), and concomitant diseases. There were twice as many patients with diabetes mellitus amongst the LTF patients compared to those who returned for follow-up visits. This may be due to hospital visits related to systemic diabetic complications in diabetic patients being regarded as more urgent and medically important than dry eye.
Clinical significance
This study shows a relatively high proportion of LTF in patients from the dry eye clinic overall. It was reassuring that the most common reason (47%) for becoming LTF was related to the improved dry eye condition or satisfactorily coping with the condition; ie, the patient feels there was no medical need to continue treatment. This type of LTF may in fact be beneficial to the system overall, as the clinic burden will not build up excessively over time.
The results of this study hinted that perhaps more healthcare resources may be required for older and female patients, since they are more likely to remain in the dry eye service. Up to a quarter of LTF patients were unhappy with the healthcare delivery. If the resources do not permit sufficient physicians to attend to dry eye, perhaps some of the roles of the physician (ie, counseling) can be delegated to allied health professionals such as optometrists or nurse counselors. Some of these professionals may be housed in satellite clinics or even perform home visits in order to attend to patients who are unable to travel to the more crowded and more inaccessible national center.
Strengths
Studies that examine LTF patients are common for other chronic diseases like tuberculosis and genitourinary disease.25,26 However, the current study is the first to report on dry eye in a clinical setting. Our study on dry eye used a similar categorization of reasons for LTF as a previous study for LTF in tuberculosis.26 Lastly, the study was conducted by one trained individual, ensuring uniformity in the interpretation of answers for the conversations. Voice recordings were used for training purposes before the study was conducted.
Limitations
Since only two patients had failure of dry eye management, the study was not sufficiently powered to explore reasons that contributed to failure of management. The reasons elicited could be inaccurate due to difficulty recalling an event that happened a long time ago. The analysis also did not consider the interaction between disease severity and personal/social factors. The results of this study may not apply to a clinic which is dominated by very severe dry eye patients or predominantly patients with systemic autoimmune diseases.
Singapore, being a small city-state, may have a uniquely accessible health care system. Nevertheless, there are some issues about payment and affordability which cannot be probed on a telephone survey.
As there was a possibility for dry eye patients to return to the clinic after a long absence, patients who had their first appointments in the later period of the study (eg, 2009 and 2010), compared to earlier period of study (eg, 2006–2008), will have a higher chance of being incorrectly considered LTF.
Study participants were predominantly Chinese, and it is unclear if results can be extrapolated to other racial or cultural contexts. Since only 26 non-Chinese patients were in the LTF group, we did not compare the proportion of those with autoimmune disease in this group compared to LTF patients who are Chinese. We did not evaluate possible differences in LTF in paying patients compared to subsidized patients, and did not measure specific socioeconomic factors such as monthly income.
Future studies
We would like to determine if the clinical severity of dry eye condition affects LTF, or if some subtypes of dry eye are predisposed to LTF. We will explore this issue by conducting focus groups for patients with different kinds of dry eye, such as those with particular systemic diseases.
In conclusion, we found that the proportion of LTF in the dry eye service over 5 years was relatively high, but only a small percentage was due to failure of dry eye treatment. The study also found that female and older patients were more likely to continue the consultations. Younger patients were likely to be LTF primarily because of medical control. On the other hand, a significant number of older patients were LTF due to personal and social constraints. These findings suggested that more resources should be targeted to older dry eye patients.
Conclusion
Dry eye is a prevalent condition in the community and in eye care centers. It may represent a significant health care burden. There is no definitive cure for dry eye, and multiple modalities may need to be used. There is a large range of severity in dry eye. Often several visits may be required to achieve control of symptoms.
Compliance is a major issue in chronic diseases like dry eye. In chronic diseases, patients may stop coming to the clinic. Patients with dry eye have a high level of anxiety and depression, which may contribute to treatment cessation.
This study found that LTF is quite common in dry eye clinics (47.5% over 5 years). Associated factors for becoming LTF were male sex, non-Chinese ethnicity, and an age of <30 years old. A very small proportion of patients that were LTF was due to failure coping or management failure. The main reasons for patient’s being LTF are divided into disease factors, personal/social factors, and health service related reasons. The reason why patients or the physician did not feel a need to continue the consultations was largely related to good control with over-the-counter medications or the relative mild nature of the condition (disease factors).
Acknowledgments
Funding for this study was provided by the National Medical Research Council (NMRC/CSA/045/2012) and the Biomedical Research Council (BMRC 10/1/35/19/670).
Disclosure
The authors report no conflicts of interest in this work.
References
The definition and classification of dry eye disease: report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. Apr 2007;5(2):75–92. | ||
Pflugfelder SC. Prevalence, burden, and pharmacoeconomics of dry eye disease. Am J Manag Care. 2008;14(3 Suppl):S102–S106. | ||
Gayton JL. Etiology, prevalence, and treatment of dry eye disease. Clin Ophthalmol. 2009;3:405–412. | ||
Waduthantri S, Yong SS, Tan CH, et al. Cost of dry eye treatment in an Asian clinic setting. PLoS One. 2012;7(6):e37711. | ||
O’Brien PD, Collum LM. Dry eye: diagnosis and current treatment strategies. Curr Allergy Asthma Rep. 2004;4:314–319. | ||
Zagórski Z, Molenda K, Kudasiewicz-Kardaszewska A, Piecyk-Sidor M. Experience from running the first dry eye clinic in Poland 2013; http://www.tfos2013.orgprograms/Taormina%202013%20Conference%20Scientific%20Program%20-%20Final,%20September%206.pdf | ||
Lemp MA. Management of dry eye disease. Am J Manag Care. 2008;14(3 Suppl):S88–S101. | ||
Yu J, Asche CV, Fairchild CJ. The economic burden of dry eye disease in the United States: a decision tree analysis. Cornea. 2011;30(4):379–387. | ||
Li M, Gong L, Sun X, Chapin WJ. Anxiety and depression in patients with dry eye syndrome. Curr Eye Res. 2011;36(1):1–7. | ||
Li M, Gong L, Chapin WJ, Zhu M. Assessment of vision-related quality of life in dry eye patients. Invest Ophthalmol Vis Sci. 2012;53(9):5722–5727. | ||
Fujita M, Igarashi T, Kurai T, Sakane M, Yoshino S, Takahashi H. Correlation between dry eye and rheumatoid arthritis activity. Am J Ophthalmol. 2005;140:808–813. | ||
Lemp MA. Advances in understanding and managing dry eye disease. Am J Ophthalmol. 2008;146(3):350–356. | ||
Clegg JP, Guest JF, Lehman A, Smith AF. The annual cost of dry eye syndrome in France, Germany, Italy, Spain, Sweden and the United Kingdom among patients managed by ophthalmologists. Ophthalmic Epidemiol. 2006;13(4):263–274. | ||
Tong L, Chaurasia SS, Mehta JS, Beuerman RW. Screening for meibomian gland disease: its relation to dry eye subtypes and symptoms in a tertiary referral clinic in singapore. Invest Ophthalmol Vis Sci. 2010;51(7):3449–3454. | ||
Uchino M, Schaumberg DA. Dry Eye Disease: Impact on Quality of Life and Vision. Curr Ophthalmol Rep. 2013;1(2):51–57. | ||
Yamada M, Mizuno Y, Shigeyasu C. Impact of dry eye on work productivity. Clinicoecon Outcomes Res. 2012;4:307–312. | ||
Miljanović B, Dana R, Sullivan DA, Schaumberg DA. Impact of dry eye syndrome on vision-related quality of life. Am J Ophthalmol. 2007;143(3):409–415. | ||
Tong L, Waduthantri S, Wong TY, et al. Impact of symptomatic dry eye on vision-related daily activities: the Singapore Malay Eye Study. Eye (Lond). 2010;24(9):1486–1491. | ||
Siak JJ, Tong L, Wong WL, et al. Prevalence and risk factors of meibomian gland dysfunction: the Singapore Malay eye study. Cornea. 2012;31(11):1223–1228. | ||
Waduthantri S, Yong SS, Tan CH, Htoon HM, Tong L. Lubricant with gelling agent in treating dry eye in adult Chinese patients. Optom Vis Sci. 2012;89(11):1647–1653. | ||
Tong L, Chaurasia SS, Mehta JS, Beuerman RW. Screening for meibomian gland disease: its relation to dry eye subtypes and symptoms in a tertiary referral clinic in singapore. Invest Ophthalmol Vis Sci. 2010;51(7):3449–3454. | ||
Lee SY, Petznick A, Tong L. Associations of systemic diseases, smoking and contact lens wear with severity of dry eye. Ophthalmic Physiol Opt. 2012;32(6):518–526. | ||
Nichols JJ, Sinnott LT. Tear film, contact lens, and patient-related factors associated with contact lens-related dry eye. Invest Ophthalmol Vis Sci. 2006;47(4):1319–1328. | ||
Moschos MM, Chatziralli IP, Siasou G, Papazisis L. Visual problems in young adults due to computer use. Klin Monbl Augenheilkd. 2012;229(4):379–381. | ||
Ross J, Mclver A, Blakely A, Dalrymple J, Peacock W, Wallis C. Why do patients default from follow-up at a genitourinary clinic?: a multivariate analysis. Genitourin Med 1995;71:393–395. | ||
Rutherford ME, Hill PC, Maharani W, Sampurno H, Ruslami R. Risk factors for treatment default among adult tuberculosis patients in Indonesia. Int J Tuberc Lung Dis. 2013;17(10):1304–1309. |
Supplementary materials
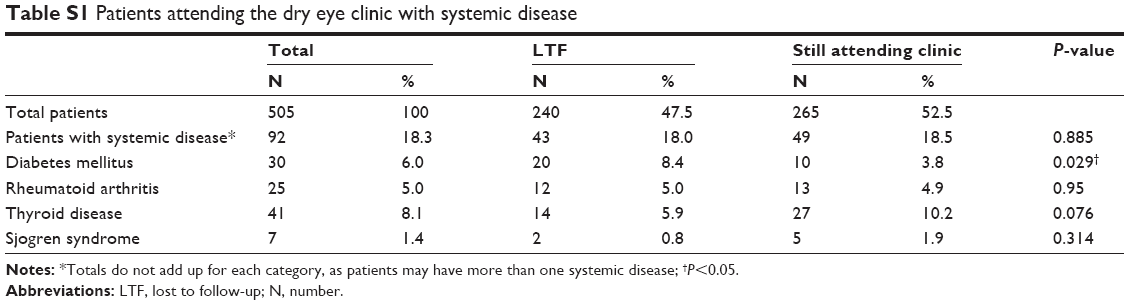 | Table S1 Patients attending the dry eye clinic with systemic disease |
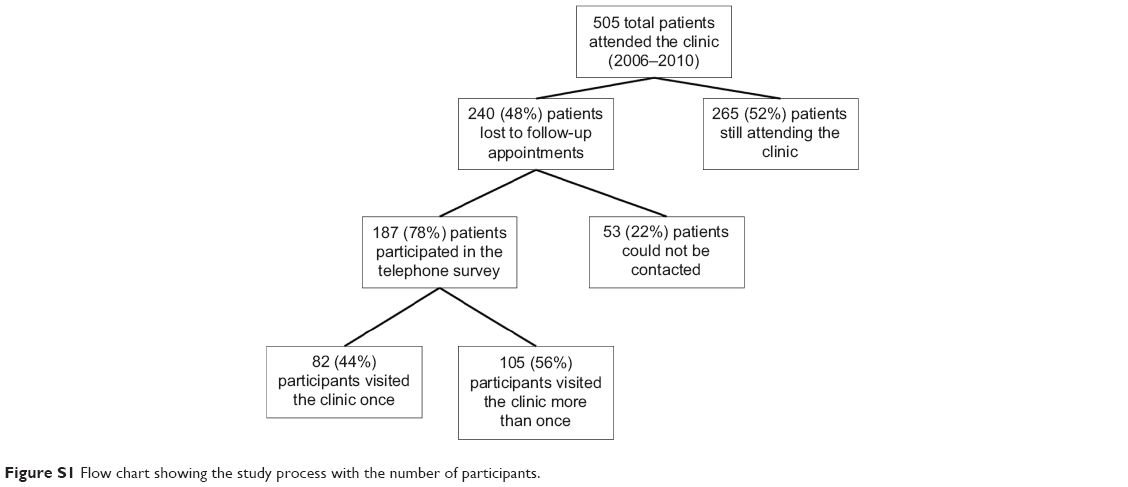 | Figure S1 Flow chart showing the study process with the number of participants. |
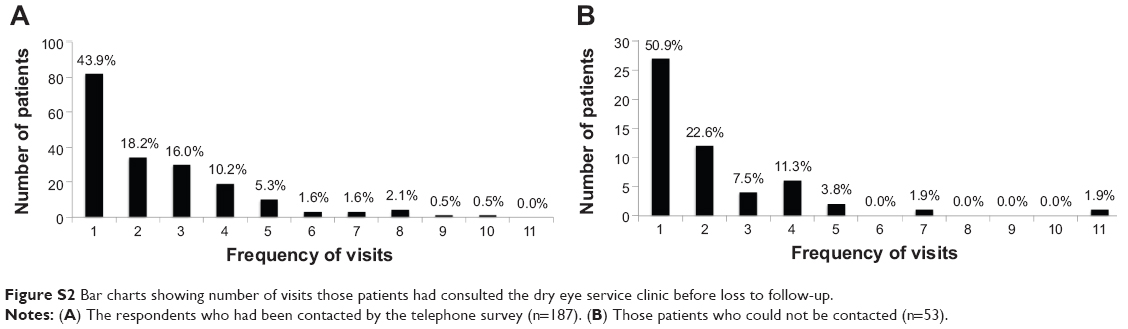 | Figure S2 Bar charts showing number of visits those patients had consulted the dry eye service clinic before loss to follow-up. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.