Back to Journals » International Journal of Women's Health » Volume 17
Longitudinal Pain Patterns and Cardiovascular Disease Risk in Chinese Menopausal Women: The Mediating Roles of Depression and Body Mass Index
Authors Ding F, Han Y, Huang J, Sun Y ![]() , Zhang K, Xu Y, Xu H
, Zhang K, Xu Y, Xu H
Received 29 June 2025
Accepted for publication 6 November 2025
Published 2 December 2025 Volume 2025:17 Pages 5063—5077
DOI https://doi.org/10.2147/IJWH.S550346
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Matteo Frigerio
Fangfang Ding,1 Yan Han,2 Jiajun Huang,1 Yiye Sun,1 Ke Zhang,1 Yujie Xu,1 Hua Xu3
1Department of Anesthesiology, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 2Department of Neurology, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 3Department of Algology, Xinhua Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China
Correspondence: Hua Xu, Department of Algology, Xinhua Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China, Email [email protected]
Purpose: Cardiovascular disease (CVD) and chronic pain substantially affect menopausal women. However, evidence is scarce regarding how the course of pain over time—specifically, whether it is persistent and affects multiple body sites—influences the future risk of CVD in this population. This study aimed to investigate the longitudinal association between these novel pain phenotypes and incident CVD, and to evaluate the mediating roles of depressive symptoms and body mass index (BMI).
Patients and Methods: This prospective analysis included 4,890 postmenopausal women from the China Health and Retirement Longitudinal Study (CHARLS). Pain status (location, intensity) and CVD were assessed at baseline (2013) and follow-up (2018). Persistent pain was defined as pain reported at both time points. We used regression models to examine the association between pain patterns and incident CVD, and mediation analysis to quantify the contribution of depressive symptoms and BMI.
Results: At baseline (cross-sectional), pain presence, intensity, and multisite distribution were associated with higher CVD prevalence. Over five years (longitudinal), persistent pain phenotypes predicted incident CVD after adjustment: general persistent pain (OR = 1.05, 95% CI: 1.00– 1.08, p = 0.012), persistent low back pain (OR = 1.08, 95% CI: 1.03– 1.13, p = 0.001), and persistent multisite pain (OR = 1.06, 95% CI: 1.00– 1.11, p = 0.020). Depressive symptoms mediated 21.6% of the association for persistent pain; for persistent low back pain, depressive symptoms (14.5%) and BMI (5.4%) were significant mediators.
Conclusion: Among postmenopausal women, long-standing and multisite pain is associated with higher future CVD risk. A modest portion of these associations was statistically accounted for by depressive symptoms and, for low back pain, BMI. Assessing pain persistence and distribution may help identify women who could benefit from integrated appraisal of pain, mood, and metabolic health.
Keywords: menopausal women, chronic pain, CVD, depressive symptoms, China Health and Retirement Longitudinal Study, CHARLS, BMI
Introduction
Cardiovascular disease (CVD) is the leading cause of death among women globally, accounting for approximately one-third of all female mortality.1–4 Menopausal women exhibit particularly alarming trends, demonstrating higher incidence and case-fatality rates for CVD than other groups—a pattern closely linked to the menopausal transition.4 In China, this burden is particularly acute, with the prevalence of CVD among women having surged by 7.5% since 1990.5 Despite this, gender-specific CVD risk factors remain under-recognized, leading to disparities in treatment.5,6 Furthermore, the management of CVD risk is complicated by its frequent co-occurrence with other chronic conditions, such as chronic pain.
Compounding the burden of CVD in this demographic, chronic pain represents another highly prevalent and debilitating public health issue. Defined by the International Association for the Study of Pain (IASP) as discomfort lasting over three months, it impacts about one-third of the global population.7 Supporting this global picture, Chinese epidemiological evidence from the China Health and Retirement Longitudinal Study (CHARLS) showed that 28.6% to 37.3% of adults in middle and later life stages reported recurrent daily pain.8 Chronic pain is linked not only to an increased risk of functional impairments,9 sleep problems,10 and depression,11 but also frequently coexists with other common chronic illnesses such as CVD.12 European epidemiological investigations confirm that chronic pain elevates both CVD incidence and mortality risk.13,14
Previous studies have characterized the pain-CVD association in broad populations, such as the UK Biobank and general Chinese adults.15 However, these investigations have typically treated pain as a binary construct (present vs absent), overlooking the potential importance of its persistence and distribution across multiple sites.
Beyond mere presence, the specific patterns of chronic pain—such as involving multiple sites or demonstrating persistence over time—may be critically important. These phenotypes are thought to reflect central sensitization and systemic burden,16,17 potentially serving as stronger CVD markers than binary pain status. The underlying pathophysiology may involve amplified neuroendocrine and autonomic nervous system dysregulation, and sustained systemic inflammation, which mutually potentiate each other to accelerate atherosclerosis.18–20 Within this conceptual framework, the selection of specific mediators requires theoretical justification. Depressive symptoms emerge as a plausible mediator, operating through shared neurobiological pathways that exacerbate stress responses and inflammation.11,21 Concurrently, body mass index (BMI) may mediate the relationship through dual pathways: metabolic dysregulation related to visceral adipose tissue, and biomechanical stress particularly relevant to low back pain.20
However, it remains unknown whether these longitudinal pain phenotypes predict CVD specifically in Chinese postmenopausal women, a population with unique vulnerabilities due to estrogen decline and its impact on both pain perception22 and cardiovascular health.23 Furthermore, the concomitant mediation by depressive symptoms and BMI remains unexamined, as prior research has focused on single mediators.15
This study therefore aims to determine whether multisite and persistent pain phenotypes predict incident CVD in Chinese postmenopausal women, testing the specific hypotheses that (H1) such pain patterns are associated with higher CVD risk after comprehensive adjustment, and (H2) these associations are partially mediated concurrently by depressive symptoms and BMI.
Materials and Methods
Data Source and Study Population
The analysis used data from the China Health and Retirement Longitudinal Study (CHARLS), a nationally representative prospective cohort of Chinese adults aged ≥45 years. CHARLS employed multistage, stratified, probability-proportional-to-size sampling across 28 provincial-level divisions (150 county-level units) with proportional urban–rural representation. The CHARLS protocol was approved by the Peking University Institutional Review Board (IRB00001052-11015) in accordance with the Declaration of Helsinki, and all participants provided written informed consent. This secondary analysis of publicly available, de-identified data was granted exemption from additional review by the Institutional Review Board of Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, under the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (effective February 18, 2023), Article 32, items (1) and (2). Standardized interviewer-administered questionnaires were implemented by trained field staff.24 The 2013 survey wave served as baseline (n = 18,650), with follow-ups conducted in 2015 and 2018. Study profile details: http://www.icpsr.umich.edu/icpsrweb/NACDA/studies/36179.
Terminology note (population). In this study, the term “menopausal women” refers to women who reported being postmenopausal at the 2013 CHARLS baseline; therefore, all analyses pertain to postmenopausal women.
For the cross-sectional analysis, we began with 18,650 baseline participants. After excluding premenopausal women (n=13,348) and participants with missing data on pain characteristics (n=330), CVD status (n=42), or age (n=40), a total of 4,890 postmenopausal women were included.
For the longitudinal analysis of incident CVD, we began with 4,890 women who had complete baseline information on pain and CVD status. We then excluded those who either had CVD at baseline or lacked CVD outcome data at follow-up (n = 684), as well as those missing pain data at follow-up (n = 680). The final analytic sample for the incident CVD analysis was 3,526 women who were free of CVD at baseline and had complete follow-up data (Figure 1).
 |
Figure 1 Flowchart of participant selection in CHARLS, 2013–2018. The analytic sample for the longitudinal incident CVD analysis included 3,526 postmenopausal women who were free of CVD at baseline and had complete follow-up data. Abbreviation: CVD, cardiovascular disease. |
Variables
All variables were assessed using the standardized questionnaires from the China Health and Retirement Longitudinal Study (CHARLS). The specific items used are described below.
Pain
Pain was assessed by two CHARLS items: “Do you often experience pain in your body?” and “Which body parts are painful? (head, neck, chest, stomach, shoulders, back, waist, hips, arms, legs, knees, wrists, fingers, ankles, toes).”25 In CHARLS, “waist” is distinct from “back”; consistent with prior CHARLS-based work, we treated “waist” as low back pain and used this term uniformly. We first dichotomized pain presence (absent/present). Among those with pain, the number of sites was counted and classified as single-site vs multisite (≥2 sites); we use the spelling “multisite” throughout.26 Pain severity was coded using the CHARLS response categories: none, slight, some, quite a bit, a lot. For terminology, we use chronic pain in the conceptual sense per the IASP definition (≥3 months). For longitudinal analyses, persistent pain denotes pain reported at both the 2013 and 2018 waves (general presence and/or specific locations/distribution). To characterize distribution trajectories, we integrated baseline and 5-year follow-up and defined four phenotypes: (1) absent or unifocal pain at both waves; (2) progression from absent/unifocal to multisite pain; (3) multisite pain at both waves (persistent multisite); and (4) regression from baseline multisite to resolution or unifocal pain. These operationalizations follow established observational methods.27,28
CVD Diagnosis
Our primary endpoint encompassed incident CVD events ascertained over the 5-year surveillance window (2013–2018). The 2013 CHARLS data served as the baseline survey given its high response rate and comprehensive menopause data. Physician-diagnosed CVD histories were collected via standardized questionnaires using the item:
Have you ever been diagnosed by a physician with [myocardial infarction, coronary artery disease, angina pectoris, congestive heart failure, or other heart conditions] or stroke?
Rigorous quality control (including double data entry and logic checks) ensured data accuracy.
Mediators
Depressive Symptoms
Depressive symptomatology was evaluated using the 10-item Center for Epidemiologic Studies Depression Scale (CES-D-10).29 This instrument evaluates depressive states through 10 items related to the participants’ experiences during the preceding week, including: feeling depressed, difficulty concentrating, other symptoms (eg, sleep disturbances, loss of appetite).30 Total scores range 0–30, with scores ≥10 establishing clinically significant depressive symptoms.
BMI
Qualified nursing staff measured participants’ height and weight. BMI was computed as weight in kilograms divided by height in meters squared (kg/m2).
Covariates
Based on the relevant questions in Wave 2, we screened postmenopausal women by including female respondents who reported being in a postmenopausal state. Multidimensional covariates were systematically documented, encompassing demographic characteristics (age, educational attainment, marital status), clinical measurements (menopausal status, systolic/diastolic blood pressure, anthropometrics), behavioral factors (tobacco use, alcohol consumption, sleep disturbances), and comorbidity profiles including hypertension, diabetes mellitus, and hyperlipidemia history. Details on the specific questionnaire items for all covariates are available in the publicly accessible CHARLS baseline questionnaire.
Statistical Analysis
Using CHARLS 2013–2018 data, we conducted (1) a cross-sectional analysis of baseline pain–CVD associations and (2) a longitudinal analysis of whether persistent pain phenotypes predict incident CVD. Continuous variables are summarized as mean ± SD and compared using Student’s t tests; categorical variables are summarized as counts (percentages) and compared using chi-square tests.
We fit multivariable logistic regression with hierarchical adjustment: Model 1 (unadjusted); Model 2 (sociodemographic and behavioral factors); Model 3 (Model 2 plus cardiometabolic factors, depressive symptoms, and age at menopause). Because depressive symptoms and BMI may lie on the pathway, Model 2 estimates are interpreted as approximating the total association, whereas Model 3 is shown to assess robustness and is not interpreted as a causal direct effect. In the longitudinal models, 566 incident CVD events yielded an events-per-variable well above common thresholds, reducing overfitting risk.
For mediation, we used the product-of-coefficients approach with nonparametric bootstrapping (5,000 resamples) to estimate indirect effects of depressive symptoms and BMI. Effect modification by age, age at menopause, smoking, alcohol use, and sleep duration was tested with likelihood-ratio (interaction) tests; detailed results appear in Supplementary Table S1. Multicollinearity was assessed using GVIF, with all GVIF^(1/(2×df)) < 2.5 (Supplementary Table S2). Missing data were handled using multiple imputation by chained equations (MICE; 5 imputed datasets, 10 iterations each) including all exposures, mediators, covariates, and outcomes as predictors. Imputed results closely matched complete-case analyses (Supplementary Tables S3–S4). All analyses used R 4.4.2; code is available from the corresponding author upon reasonable request.
Results
A total of 4,890 postmenopausal women were included at baseline; follow-up information in 2018 was available for the majority. After prespecified exclusions, 3,526 women without baseline CVD comprised the longitudinal cohort. The baseline characteristics of the cross-sectional sample are presented in Table 1. The mean age of the participants was 62.8 ± 8.3 years, and the mean age at menopause was 48.9 ± 4.4 years. Compared to participants who reported no pain, those with baseline pain were more likely to have lower education levels, a younger age at menopause, reside in rural areas, and be single. The group with baseline pain had older age, higher smoking prevalence, shorter nighttime sleep duration, elevated depression scores, and greater comorbidity burden (p < 0.05) (Table 1).
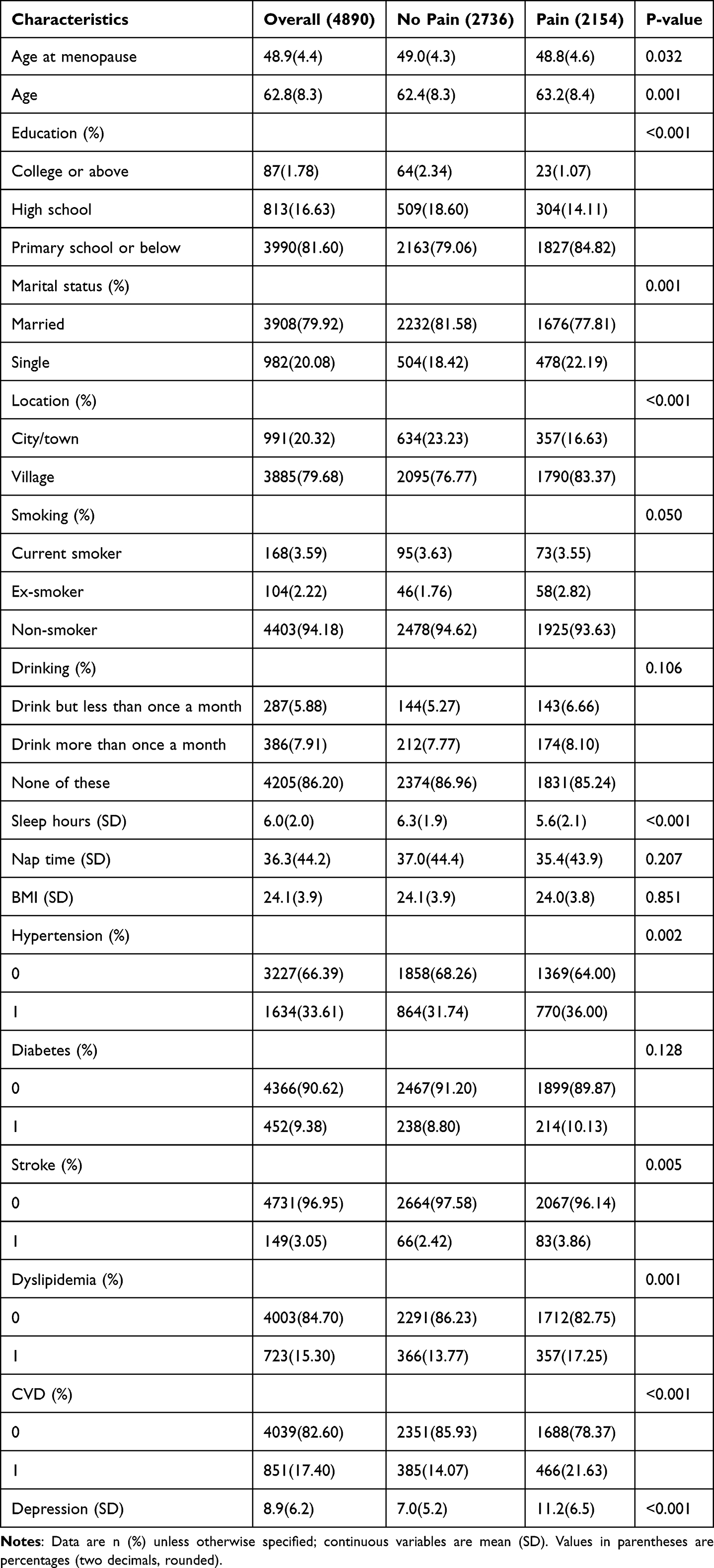 |
Table 1 Baseline Characteristics by Baseline Pain Status |
Cross-Sectional Association Between Pain and CVD
In the cross-sectional analysis, the prevalence of CVD among the total sample, individuals with pain, and those without pain was 17.40%, 21.63%, and 14.07%, respectively. As shown in Table 2, baseline pain was significantly associated with CVD. After adjusting for demographics, health behaviors, and chronic diseases (Model 3), baseline pain was significantly associated with CVD (OR: 1.06; 95% CI: 1.03–1.09, p < 0.001). Additionally, as detailed in Table 2, pain at several specific sites—including headache, chest pain, low back pain, and knee pain—showed particularly strong and statistically significant associations with prevalent CVD in the fully adjusted model (all p < 0.01).
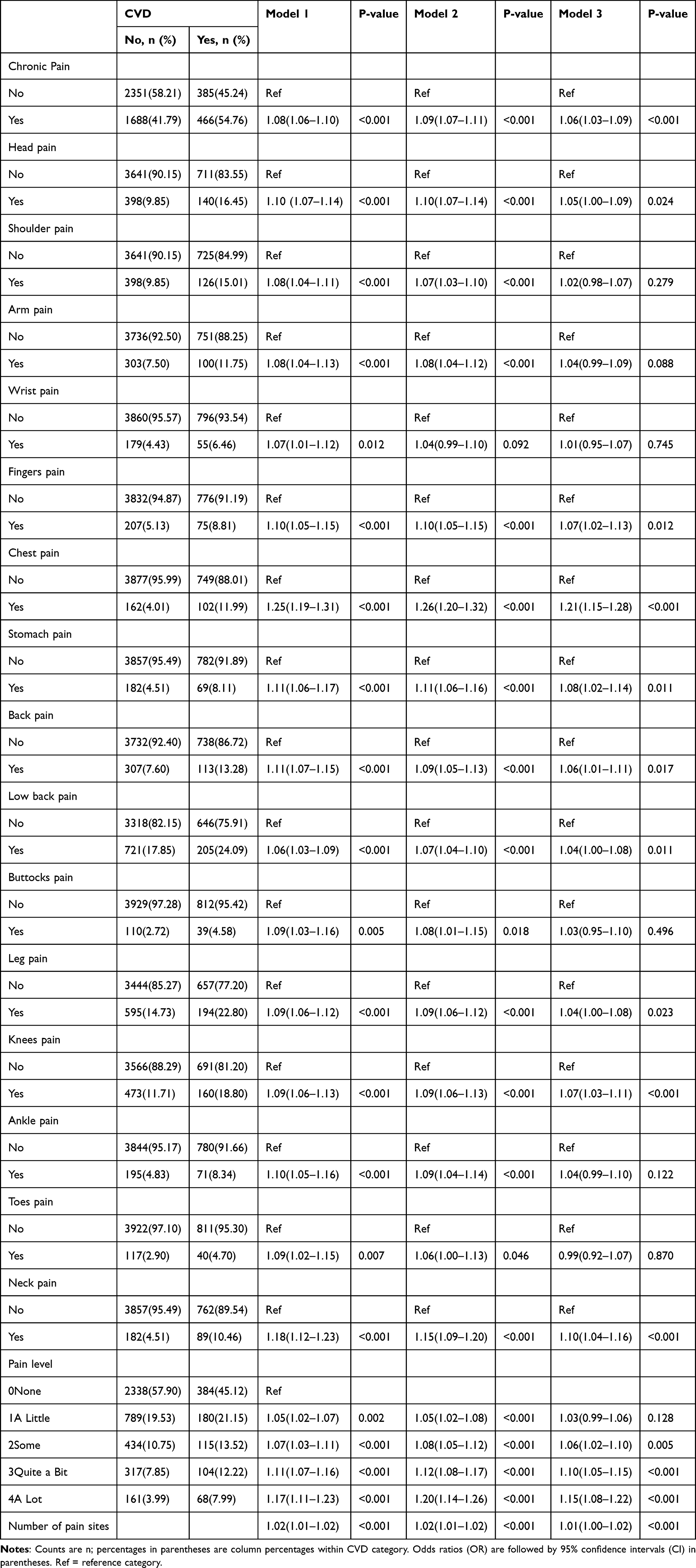 |
Table 2 Odds Ratios and 95% Confidence Intervals for CVD by Pain in the Cross-Sectional Analysis |
Longitudinal Association Between Persistent Pain and Incident CVD
Among 3,526 CVD-free participants, 933 (26.46%) had persistent pain. Over five years, 566 (16.06%) developed CVD—200 (35.34%) with persistent pain and 366 (64.66%) without persistent pain. The associations between pain and CVD events are presented in Table 3. After adjusting for covariates in Model 3, both persistent pain (OR = 1.05, 95% CI: 1.00–1.08; p = 0.012) and persistent low back pain (OR = 1.08, 95% CI: 1.03–1.13; p = 0.001) were associated with an increased risk of CVD events. Regarding pain severity and duration, both persistent multisite pain (OR = 1.06, 95% CI: 1.00–1.11; p = 0.020) and relatively severe pain levels (Quite a Bit vs none; OR = 1.08, 95% CI: 1.02–1.14; p = 0.013) were associated with an increased risk of CVD events. No significant associations were observed between persistent pain at other sites and CVD. It is noteworthy that a substantial proportion of participants with persistent low back pain also met the criteria for persistent multisite pain, indicating the overlapping nature of these pain phenotypes. By contrast, transitional pain trajectories — progression to or recovery from multisite pain between waves — were not significantly associated with incident CVD (Table 3).
 |
Table 3 Odds Ratios and 95% Confidence Intervals for CVD by Persistent Chronic Pain in the Longitudinal Analysis |
Mediation Analysis
In the longitudinal analysis, compared with subjects who did not develop CVD, those who developed CVD exhibited significantly higher CES-D-10 scores (10.41 ± 6.68 vs 8.08 ± 6.17) and body mass index (BMI) (24.7 ± 3.9 vs 23.8 ± 3.8). Figure 2 illustrates the mediating roles in the relationships of persistent pain, persistent low back pain, and incident CVD events. Depression emerged as a consistent psychological mediator in both associations: the proportion mediated by depression was 14.5% for persistent low back pain and 21.6% for persistent pain (both p < 0.05). Notably, depression exerted a stronger mediating effect for general persistent pain (proportion mediated: 21.6%) than for persistent low back pain (14.5%). The effect of pain on depressive symptoms (path a) was similar for both phenotypes (β ≈ 3.85), but the association between depression and CVD (path b) was more pronounced in the low back pain model. In contrast, BMI mediated only 5.4% of the association for persistent low back pain, with a statistically significant but relatively smaller proportion mediated compared to depressive symptoms. Analysis of the total effects revealed a stronger direct effect of persistent low back pain on CVD (Figure 2).
 |
Figure 2 Mediation models: (A) persistent multisite pain; (B) persistent low back pain; (C) overall model. a: effect of pain on the mediator (depressive symptoms or BMI). b: effect of the mediator on CVD (adjusting for pain). c: total effect of pain on CVD; c′: direct effect after accounting for the mediator. Numbers on arrows are unstandardized β coefficients; for paths to the binary outcome (CVD), βs are on the log-odds (logit) scale. *p < 0.05; **p < 0.01; ***p < 0.001. Estimates are adjusted for covariates as specified in Methods. |
Sensitivity Analysis
To assess robustness, we conducted sensitivity analyses using multiple imputation for missing data, which yielded results consistent with the original complete-case analysis (Supplementary Table S3−4) Subgroup analyses stratified by age, menopausal age, smoking, alcohol use, and sleep patterns showed no significant heterogeneity in the persistent pain-CVD associations (Figure 3). Formal interaction tests were non-significant across subgroups (all LRT p > 0.05; see Supplementary Table S1).
 |
Figure 3 Stratified subgroup analysis of the association between persistent pain and CVD risk. The subgroup analysis is based on Model 3. Abbreviations: OR, odds ratio; CI, confidence interval. |
Discussion
This cohort study of 4,890 Chinese postmenopausal women demonstrates that multisite and persistent pain—specifically, persistent multisite pain and persistent low back pain—are associated with a significantly elevated CVD risk, after adjustment for traditional risk factors, socioeconomic status, and comorbidities. Notably, episodic pain or transitions in pain patterns showed no significant association, which supports the hypothesis that CVD risk is more closely linked to sustained, cumulative exposure to pain stimuli rather than transient episodes. This finding aligns with the concept of “allostatic load”, where the physiological burden of sustained multisystem stress could overwhelm resilience.31
Our findings resonate with large-scale cohort studies in European populations, such as the UK Biobank study,14 which identified chronic pain as an independent risk factor for CVD. However, our study extends this by highlighting that in Chinese postmenopausal women, it is specifically the multisite and persistent nature of pain, rather than pain per se, that carries the strongest risk.
Although statistically significant, several ORs were close to 1.0. This pattern likely reflects rigorous covariate adjustment and the predominance of indirect rather than large direct effects. Our mediation findings are consistent with this interpretation, identifying depressive symptoms—and, for low back pain, BMI—as small but significant mediators. Therefore, the modest ORs are consistent with indirect pathways—psychological (depressive symptoms) and, for low back pain, metabolic/biomechanical (BMI)—within a broader risk profile.
It is speculated that the observed cumulative effect of multisite and persistent pain might operate through amplified neuroinflammatory and neuroendocrine pathways.13,17,32 The sustained stress of persistent pain may involve neuroinflammatory and neuroendocrine pathways that, over time, are proposed to adversely affect cardiovascular health.19,21 Thus, persistent multisite pain might serve as a clinical marker of such underlying, system-wide physiological strain.
Furthermore, the mediating role of depressive symptoms suggests an important psychological pathway. Our finding aligns with research in the Chinese population, which reported a similar mediating effect.15 The interplay between chronic pain, depression, and CVD risk likely involves shared neurobiological pathways. Supporting this, recent interventional research indicates that neuromodulation therapies like deep transcranial magnetic stimulation (dTMS), which target underlying neural circuits, can effectively alleviate both depression and comorbid chronic pain.33 These observations are consistent with the possibility that depression lies on a mediating pathway between persistent pain and CVD risk, although causality cannot be inferred from our observational data.
Transitional states (emergent/resolved multisite pain) were not associated with incident CVD, reinforcing the relevance of chronicity over fluctuation. This contrast with the significant findings for persistent pain strengthens our interpretation that the chronicity and stability of the pain burden over time, rather than its mere presence or short-term fluctuation, is most relevant to CVD risk pathogenesis. This pattern also reduces the likelihood of reverse causality being the primary driver of our results.
The specific mediation role of BMI in the persistent low back pain-CVD association (5.4%), though modest, underscores a tangible biomechanical and metabolic interplay.34,35 In our cohort, even within the normal-to-overweight range, higher BMI likely contributes to the pain-CVD link through dual pathways. Firstly, metabolic dysregulation related to visceral adipose tissue may foster a pro-inflammatory state and insulin resistance that promote atherosclerosis.36 It is corroborated by large-scale epidemiological studies in women, which have identified a strong link between hyperandrogenism, elevated BMI, and metabolic syndrome, a key precursor to CVD.37 Secondly, biomechanical stress from excess weight, especially abdominal obesity, increases spinal load, which may perpetuate low back pain and could contribute to higher CVD risk.20,38 This is particularly relevant as low back pain, a leading global cause of disability, exhibits a higher prevalence in women, with postmenopausal women being particularly susceptible.39–41 The vulnerability of this group is evidenced by research linking longer menopause duration (>5 years) and adverse body composition to substantially increased metabolic risk.42 Furthermore, postmenopausal estrogen decline is thought to contribute to this risk, likely by amplifying pain perception, stress responses, and promoting central adiposity.43
Our study advances the existing literature by specifically focusing on menopausal women and demonstrating that the cumulative burden of pain over time and across sites is associated with CVD risk. Moreover, we simultaneously quantify the mediating roles of both depressive symptoms and BMI, revealing their shared and specific pathways. However, several limitations should be considered. First, menopausal status, pain, and CVD were self-reported, which may introduce misclassification bias. While CHARLS employs validated instruments, any misclassification is likely non-differential, which would generally attenuate the observed effect estimates toward the null. Therefore, our reported associations might be conservative. Second, despite extensive adjustment for a wide range of covariates, residual confounding from unmeasured or imperfectly measured factors (eg, physical activity intensity, specific dietary components, genetic predisposition) remains possible. This means we cannot rule out the possibility that unaccounted factors explain part of the observed associations. Third, because the various pain phenotypes exhibit substantial conceptual and statistical overlap, we did not apply a formal multiple-testing correction. This strategy reduces the risk of Type II errors, though it increases the potential for Type I errors. Consequently, associations for specific pain sites should be considered exploratory.
Future research should prioritize several specific directions: (1) studies incorporating objective measures of physical activity, inflammatory biomarkers, and pain-related functional limitations to validate the proposed pathways; (2) prospective studies enrolling younger perimenopausal women to track the evolution of pain, mood, metabolic factors, and CVD risk from the menopausal transition onward; and (3) randomized controlled trials to investigate whether managing depressive symptoms and weight in menopausal women with chronic pain can ultimately reduce the risk of CVD. While our findings cannot support specific clinical recommendations, they suggest that women with persistent, multisite pain might benefit from comprehensive assessment that includes mood and metabolic health.
Conclusion
In this prospective cohort of Chinese postmenopausal women, several persistent pain phenotypes were associated with an increased risk of CVD. Notably, the association for persistent low back pain was consistent and statistically significant. Taken together, these findings suggest that the long-term trajectory of pain may be more relevant than short-term fluctuations. A modest portion of these associations was statistically accounted for by depressive symptoms and, for persistent low back pain, by BMI. While residual confounding cannot be ruled out, these results highlight depressive symptoms and BMI as potential mechanistic pathways worthy of further investigation. Future research should delineate these mechanisms and, in randomized trials, evaluate whether targeting these mediators can improve cardiovascular outcomes.
Acknowledgments
We would like to thank the CHARLS team for providing valuable data, and each study team member and each respondent for their time and effort.
Funding
This work was supported by the Shanghai Natural Science Foundation Medical Innovation Project of China, [Grant/Award Number: 21Y11906100].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zeng G, Wang H, Cao P, Zhao J, Liu L, Guo H. Changing patterns of cardiovascular diseases and subtypes induced by kidney dysfunction among 25–64 years in China from 1992 to 2021. BMC Public Health. 2025;25(1):26. doi:10.1186/s12889-024-21183-4
2. Martin SS, Aday AW, Almarzooq ZI, et al. 2024 heart disease and stroke statistics: a report of US and global data from the American heart association. Circulation. 2024;149(8):e347–e913. doi:10.1161/CIR.0000000000001209
3. Woodruff RC, Tong X, Khan SS, et al. Trends in cardiovascular disease mortality rates and excess deaths, 2010-2022. Am J Prev Med. 2024;66(4):582–589. doi:10.1016/j.amepre.2023.11.009
4. Vogel B, Acevedo M, Appelman Y, et al. The lancet women and cardiovascular disease commission: reducing the global burden by 2030. Lancet Lond Engl. 2021;397(10292):2385–2438. doi:10.1016/S0140-6736(21)00684-X
5. Wang H, Zhang H, Zou Z. Changing profiles of cardiovascular disease and risk factors in China: a secondary analysis for the global burden of disease study 2019. Chin Med J. 2023;136(20):2431–2441. doi:10.1097/CM9.0000000000002741
6. Bairey Merz CN, Andersen H, Sprague E, et al. Knowledge, attitudes, and beliefs regarding cardiovascular disease in women: the women’s heart alliance. J Am Coll Cardiol. 2017;70(2):123–132. doi:10.1016/j.jacc.2017.05.024
7. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet Lond Engl. 2021;397(10289):2082–2097. doi:10.1016/S0140-6736(21)00393-7
8. Qiu Y, Li H, Yang Z, et al. The prevalence and economic burden of pain on middle-aged and elderly Chinese people: results from the China Health and Retirement Longitudinal Study. BMC Health Serv Res. 2020;20(1):600. doi:10.1186/s12913-020-05461-6
9. Wu SH, Lin CF, Lu IC, Yeh MS, Hsu CC, Yang YH. Association between pain and cognitive and daily functional impairment in older institutional residents: a cross-sectional study. BMC Geriatr. 2023;23(1):756. doi:10.1186/s12877-023-04337-8
10. Seiger AN, Penzel T, Fietze I. Chronic pain management and sleep disorders. Cell Rep Med. 2024;5(10):101761. doi:10.1016/j.xcrm.2024.101761
11. Frank P, Batty GD, Pentti J, et al. Association between depression and physical conditions requiring hospitalization. JAMA Psychiatry. 2023;80(7):690–699. doi:10.1001/jamapsychiatry.2023.0777
12. Lin L, Lin J, Qiu J, et al. Genetic liability to multi-site chronic pain increases the risk of cardiovascular disease. Br J Anaesth. 2023;131(2):373–384. doi:10.1016/j.bja.2023.04.020
13. Rodríguez-Sánchez I, Ortolá R, Graciani A, et al. Pain characteristics, cardiovascular risk factors, and cardiovascular disease. J Gerontol A Biol Sci Med Sci. 2022;77(1):204–213. doi:10.1093/gerona/glab079
14. Rönnegård AS, Nowak C, Äng B, Ärnlöv J. The association between short-term, chronic localized and chronic widespread pain and risk for cardiovascular disease in the UK biobank. Eur J Prev Cardiol. 2022;29(15):1994–2002. doi:10.1093/eurjpc/zwac127
15. Miao E, Wu Q, Cai Y. Mediating effect of depressive symptoms on the relationship of chronic pain and cardiovascular diseases among Chinese population: evidence from the CHARLS. J Psychosom Res. 2024;180:111639. doi:10.1016/j.jpsychores.2024.111639
16. Chen Y, Sun Y, Wang L, Xu K, Wang DW. Genetic insights into associations of multisite chronic pain with common diseases and biomarkers using data from the UK biobank. Br J Anaesth. 2024;132(2):372–382. doi:10.1016/j.bja.2023.11.007
17. Fang XX, Zhai MN, Zhu M, et al. Inflammation in pathogenesis of chronic pain: foe and friend. Mol Pain. 2023;19:17448069231178176. doi:10.1177/17448069231178176
18. Onan D, Ulger O. Investigating the relationship between body mass index and pain in the spine in children or adolescents: a systematic review. Child Obes. 2021;17(2):86–99. doi:10.1089/chi.2020.0266
19. Kolijn D, Pabel S, Tian Y, et al. Empagliflozin improves endothelial and cardiomyocyte function in human heart failure with preserved ejection fraction via reduced pro-inflammatory-oxidative pathways and protein kinase gα oxidation. Cardiovasc Res. 2021;117(2):495–507. doi:10.1093/cvr/cvaa123
20. Kong P, Cui ZY, Huang XF, Zhang DD, Guo RJ, Han M. Inflammation and atherosclerosis: signaling pathways and therapeutic intervention. Signal Transduction Targeted Ther. 2022;7(1):131. doi:10.1038/s41392-022-00955-7
21. Xiong HY, Hendrix J, Schabrun S, et al. The role of the brain-derived neurotrophic factor in chronic pain: links to central sensitization and neuroinflammation. Biomolecules. 2024;14(1):71. doi:10.3390/biom14010071
22. Chen Q, Zhang W, Sadana N, Chen X. Estrogen receptors in pain modulation: cellular signaling. Biol Sex Differ. 2021;12(1):22. doi:10.1186/s13293-021-00364-5
23. El Khoudary SR, Aggarwal B, Beckie TM, et al. Menopause transition and cardiovascular disease risk: implications for timing of early prevention: a scientific statement from the American heart association. Circulation. 2020;142(25):e506–e532. doi:10.1161/CIR.0000000000000912
24. Zhao Y, Hu Y, Smith JP, Strauss J, Yang G. Cohort profile: the China Health and Retirement Longitudinal Study (CHARLS). Int J Epidemiol. 2014;43(1):61–68. doi:10.1093/ije/dys203
25. Huang J, Wang X. Association of depressive symptoms with risk of incidence low back pain in middle-aged and older Chinese adults. J Affect Disord. 2024;354:627–633. doi:10.1016/j.jad.2024.03.081
26. Zhu X, Zhang X, Ding L, et al. Associations of pain and sarcopenia with successful aging among older people in China: evidence from CHARLS. J Nutr Health Aging. 2023;27(3):196–201. doi:10.1007/s12603-023-1892-2
27. Chen J, Yan L, Chu J, Wang X, Xu Z. Pain characteristics and progression to sarcopenia in Chinese middle-aged and older adults: a 4-year longitudinal study. J Gerontol A Biol Sci Med Sci. 2024;79(5):glae080. doi:10.1093/gerona/glae080
28. Li W, Shen C, Kong W, et al. Association between the triglyceride glucose-body mass index and future cardiovascular disease risk in a population with cardiovascular-kidney-metabolic syndrome stage 0-3: a nationwide prospective cohort study. Cardiovasc Diabetol. 2024;23(1):292. doi:10.1186/s12933-024-02352-6
29. Fan S, Wang Q, Zheng F, et al. Depression as a mediator and social participation as a moderator in the bidirectional relationship between sleep disorders and pain: dynamic cohort study. JMIR Public Health Surveillance. 2023;9:e48032. doi:10.2196/48032
30. Wang W, Liu Y, Ji D, et al. The association between functional disability and depressive symptoms among older adults: findings from the China health and retirement longitudinal study (CHARLS). J Affect Disord. 2024;351:518–526. doi:10.1016/j.jad.2024.01.256
31. Sonino N, Fava GA, Lucente M, Guidi J. Allostatic load and endocrine disorders. Psychother Psychosom. 2023;92(3):162–169. doi:10.1159/000530691
32. Mei F, Li JJ, Lin J, Xing D, Dong S. Multidimensional characteristics of musculoskeletal pain and risk of Hip fractures among elderly adults: the first longitudinal evidence from CHARLS. BMC Musculoskelet Disord. 2024;25(1):4. doi:10.1186/s12891-023-07132-z
33. Ju P, Zhao D, Ma L, Chen J. Biomarker development perspective: exploring comorbid chronic pain in depression through deep transcranial magnetic stimulation. J Transl Intern Med. 2024;12(2):123–128. doi:10.2478/jtim-2023-0145
34. Weeldreyer NR, De Guzman JC, Paterson C, Allen JD, Gaesser GA, Angadi SS. Cardiorespiratory fitness, body mass index and mortality: a systematic review and meta-analysis. Br J Sports Med. 2025;59(5):339–346. doi:10.1136/bjsports-2024-108748
35. Zhang C, Zi S, Chen Q, Zhang S. The burden, trends, and projections of low back pain attributable to high body mass index globally: an analysis of the global burden of disease study from 1990 to 2021 and projections to 2050. Front Med. 2024;11:1469298. doi:10.3389/fmed.2024.1469298
36. Xu C, Fu Z, Wang J, Wu B, Wang XQ. Differences and correlations of anxiety, sleep quality, and pressure-pain threshold between patients with chronic low back pain and asymptomatic people. Pain Res Manage. 2022;2022:8648584. doi:10.1155/2022/8648584
37. Luo X, Wang Y, Wang L, Shen Y, Ren M. Association between female androgen levels, metabolic syndrome, and cardiovascular disease: an NHANES analysis (2013-2016). Int J Women’s Health. 2024;16:2087–2101. doi:10.2147/IJWH.S475149
38. Zhou J, Mi J, Peng Y, Han H, Liu Z. Causal associations of obesity with the intervertebral degeneration, low back pain, and sciatica: a two-sample mendelian randomization study. Front Endocrinol. 2021;12:740200. doi:10.3389/fendo.2021.740200
39. Zhang S, Ma X, Yao Y, Pan H, Zou L. Global, regional, and national burdens of low back pain in women of childbearing age from 1990 to 2021: an analysis based on the global burden of disease study 2021. BMC Public Health. 2025;25(1):515. doi:10.1186/s12889-025-21659-x
40. Cheng M, Xue Y, Cui M, et al. Global, regional, and national burden of low back pain: findings from the global burden of disease study 2021 and projections to 2050. Spine. 2025. doi:10.1097/BRS.0000000000005265
41. Li Y, Zou C, Guo W, et al. Global burden of low back pain and its attributable risk factors from 1990 to 2021: a comprehensive analysis from the global burden of disease study 2021. Front Public Health. 2024;12:1480779. doi:10.3389/fpubh.2024.1480779
42. Erdoğan K, Sanlier N. Metabolic syndrome and menopause: the impact of menopause duration on risk factors and components. Int J Women’s Health. 2024;16:1249–1256. doi:10.2147/IJWH.S460645
43. Vervoort D, Wang R, Li G, et al. Addressing the global burden of cardiovascular disease in women: JACC state-of-the-art review. J Am Coll Cardiol. 2024;83(25):2690–2707. doi:10.1016/j.jacc.2024.04.028
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.