Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 14
Longitudinal comparison of outcomes in patients with smoking-related asthma-COPD overlap and in non-smoking asthmatics with incomplete reversibility of airway obstruction
Authors Boulet LP, Boulay ME, Milot J ![]() , Lepage J, Bilodeau L
, Lepage J, Bilodeau L ![]() , Maltais F
, Maltais F ![]()
Received 24 October 2018
Accepted for publication 1 February 2019
Published 27 February 2019 Volume 2019:14 Pages 493—498
DOI https://doi.org/10.2147/COPD.S192003
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Louis-Philippe Boulet, Marie-Eve Boulay, Joanne Milot, Johane Lepage, Lara Bilodeau, François Maltais
Research Center, Quebec Heart and Lung Institute-Laval University, Quebec, QC, Canada
Background: There is a need to characterize the impact of the smoking status on the clinical course of asthmatics with incomplete reversibility of airway obstruction (IRAO).
Objective: To compare longitudinal health care use, symptom control, and medication needs between smoking and non-smoking asthmatics with IRAO.
Materials and methods: This was a 12-month follow-up of a cross-sectional study comparing asthmatics with IRAO according to their tobacco exposure. One group had a tobacco exposure ≥20 pack-years and was considered to have asthma-COPD overlap (ACO) and the second with a past tobacco exposure
Results: A total of 111 patients completed all follow-up telephone calls: 71 ACO and 40 NS-IRAO. The number of exacerbations per patient over the 12-month follow-up was similar in both groups. However, ACO reported worse symptom control throughout the follow-up as compared to NS-IRAO, although no significant variations within a group were observed over the study period.
Conclusion: Although asthma control scores were poorer in ACO patients over 1 year compared to NS-IRAO, exacerbation rate was similar and low in both groups of asthmatics. These observations suggest that poorer asthma control in ACO was not driven by the number of exacerbations but may reflect the influence of chronic airway changes related to the COPD component.
Keywords: asthma-COPD overlap, symptoms, exacerbations, smoking history, fixed airflow limitation
Introduction
Asthma may be associated with an incomplete reversibility of airway obstruction (IRAO). When patients demonstrate features of both asthma and COPD, they are often considered to have asthma-COPD overlap (ACO).1,2 We previously showed that patients with ACO, defined as asthmatic patients with an IRAO and a significant smoking history, had a different phenotype compared to non-smoking asthmatic patients with IRAO.3
The clinical course of patients with smoking-related ACO remains, however, to be compared to that of non-smokers with IRAO (NS-IRAO), and these observations may have important implications for the clinical management of these patients. The present analysis is a 12-month longitudinal follow-up of patients with ACO or NS-IRAO who were the subject of an extensive cross-sectional phenotypic characterization.3 The present investigation was intended to specifically focus on the clinical outcomes of these two groups of asthmatics with emphasis on the frequency of exacerbations and symptom control.
Materials and methods
Subjects
Two groups of asthmatic subjects with an IRAO were recruited from the asthma outpatient clinic of the Institut universitaire de cardiologie et de pneumologie de Québec-Université Laval (IUCPQ-UL), a tertiary care center in Quebec city: 1) one composed of current smokers or ex-smokers (≥20 pack-years history of cigarette smoking), ACO and 2) one involving never-smokers or ex-smokers with a non-significant smoking history of less than five pack-years who had quitted smoking more than 12 months before study inclusion, NS-IRAO. Inclusion criteria and baseline evaluation have been reported previously.3 Briefly, we included patients aged 40 years and over, with a previous diagnosis of asthma based on the Canadian Thoracic Society criteria,4 who required inhaled corticosteroids with or without additional asthma medication, and who showed IRAO, as defined by persistence of a post-bronchodilator FEV1/FVC ratio <0.7 in addition to a FEV1 less than 80% of predicted value on at least two occasions while on a treatment considered as optimal by a respirologist.4 Patients with any other respiratory conditions than asthma (including previous diagnosis of COPD without a confirmed diagnosis of asthma), an unstable respiratory or non-respiratory condition, previous bronchial thermoplasty, who experienced a respiratory infection in the 4 weeks preceding study entry, or who changed respiratory medication in the 4 weeks before baseline visit were excluded. This study was conducted in accordance with the Declaration of Helsinki. All subjects signed an informed consent form and the study was approved by the Ethics committee of the IUCPQ-UL (CER21047).
Study design
This was a 12-month longitudinal study. Following baseline assessment, telephone calls were made by the study coordinators (JM and JL) at 3-month intervals to gather information related to exacerbations and asthma control. The study was registered on Clinical Trials (NCT03817333).
Outcomes
Patients were asked about events related to asthma exacerbations including: 1) unscheduled medical visits, 2) emergency department visits (<24 hours in the emergency room), 3) hospitalizations (>24 hours in the emergency room or formal hospitalization), 4) increase in maintenance dose of inhaled corticosteroids (ICSs) for at least 3 consecutive days, 5) oral corticosteroids use, including new therapy or increased maintenance dose for at least 2 consecutive days as a consequence of exacerbation,5 and 6) antibiotic treatments for bronchitis or pneumonia. In addition, study coordinators administered the validated French version of the asthma control questionnaire-6 (ACQ-6 [0–6], a lower score indicating better asthma control and scores >1.5 suggesting uncontrolled asthma)6,7 and the clinical subsection of the asthma control scoring system (ACSS [20–100], a higher score indicating better asthma control).8,9 Lastly, patients answered questions about changes in maintenance medication, allergen exposure, and smoking habit at each phone call.
Statistical analyses
Results are presented as mean ± SD. The outcomes were analyzed using a generalized linear mixed model. Statistical thresholds were set at P-values<0.05 for number of exacerbations (primary end point) and P<0.01 for control scores (secondary end points). All analyses were conducted using the statistical package SAS, version 9.4 (SAS Institute Inc, Cary, NC, USA) and R (R Core Team [2016], Foundation for Statistical Computing, Vienna, Austria).
Results
From the initial cohort of 75 patients with ACO and 40 patients with NS-IRAO who were the subject of the cross-sectional study,3 71 patients with ACO and all patients with NS-IRAO completed this 12-month follow-up study. The main characteristics are available in Table S1 of the online supplement while detailed phenotypic assessment of these patients have been published elsewhere.3
Very few exacerbation events were reported in this population over the 12-month follow-up. No significant differences in the number of asthma exacerbations per patient at 12 months were observed between ACO and NS-IRAO: 1) total events per year: 2.0 vs 2.3, respectively, 2) number of unscheduled medical visits per year: 0.33 vs 0.30, respectively, 3) number of emergency department visits per year: 0.11 vs 0.25, respectively, 4) number of hospitalizations per year: 0.06 vs 0, respectively, 5) number of increases in maintenance dose of ICS for at least 3 consecutive days per year: 0.92 vs 1.2, respectively, 6) number of oral corticosteroid uses per year: 0.42 vs 0.38, respectively, and 7) number of antibiotic treatments for bronchitis or pneumonia per year: 0.15 vs 0.18, respectively.
Consistent with better asthma control in patients with NS-IRAO, there was strong tendency for ACQ-6 scores to be lower in the NS-IRAO as compared to the ACO group (P=0.016), while ACSS clinical scores were significantly higher (P=0.004) in the NS-IRAO as compared to the ACO group (Figure 1) throughout the study. However, the time course of symptom scores followed a similar pattern in both groups of asthmatics. No significant change in life habits or environment was reported in either group.
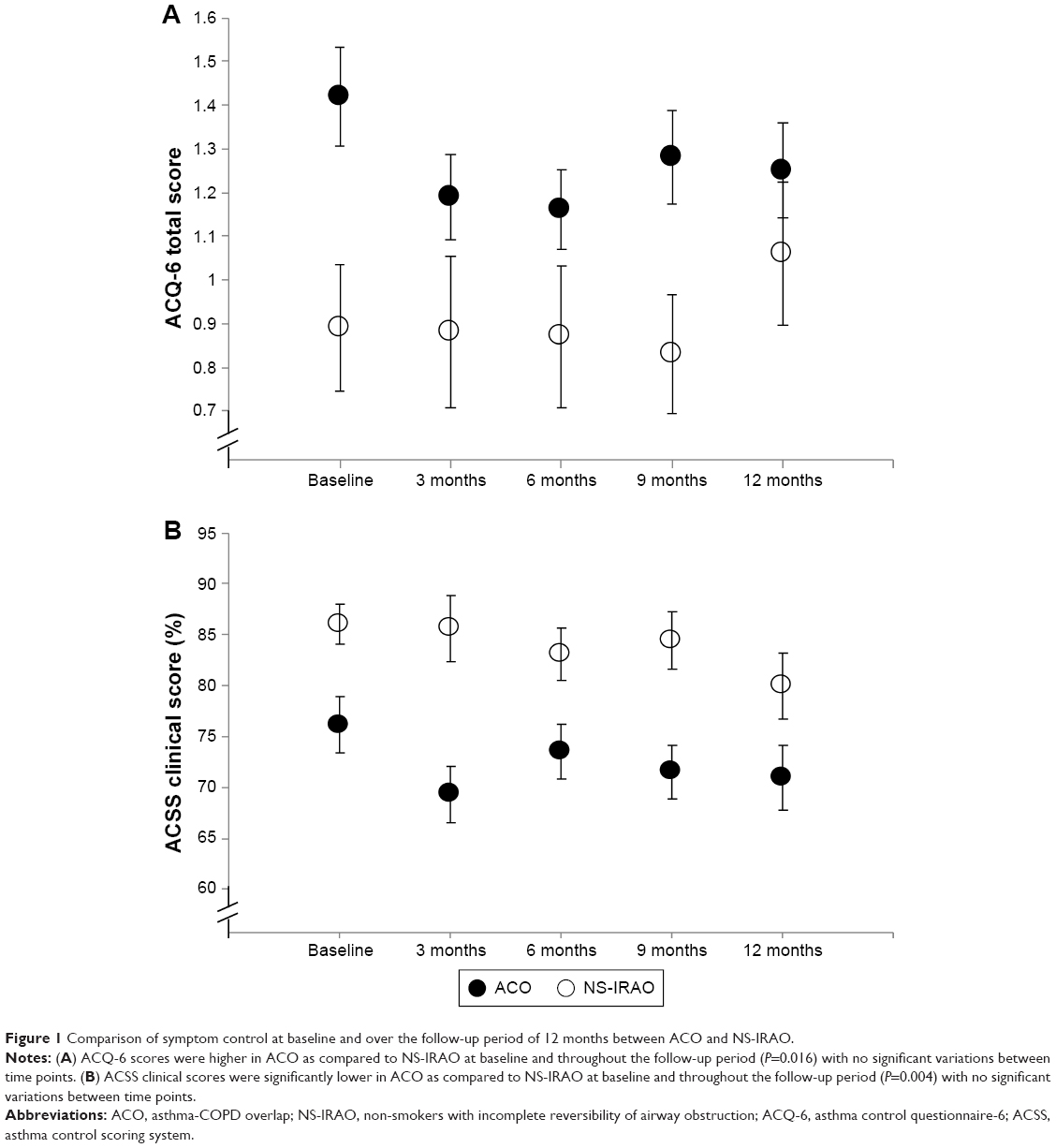 | Figure 1 Comparison of symptom control at baseline and over the follow-up period of 12 months between ACO and NS-IRAO. |
Discussion
In this study, patients with ACO and NS-IRAO experienced a similar low number of exacerbation events over 12 months. Despite this, symptom control was poorer in ACO as compared to NS-IRAO throughout the 12-month follow-up, although the time course of asthma control showed a similar pattern between the two groups.
Our results are at variance with several studies reporting a higher frequency of exacerbations10–12 and increased health care use13–16 in patients with ACO compared to those with asthma or patients with COPD, although this is not a universal finding.17–19 Several factors may explain the low exacerbation event rates in the present cohort of patients with ACO. First, patients with ACO who were involved in this study were former smokers, while current but not past smoking has been associated with a greater risk of hospitalization and hospital-based care for asthma,20 more unscheduled health care visits,21 and more rescue courses of oral steroids as compared to ex-smokers.21 Second, as our patients were followed in a tertiary care practice, they may have benefited from optimal management, with better access to asthma/COPD education and optimal therapy. Indeed, although this was not part of the study, all study patients were seen and followed by a qualified asthma educator to assess inhalator technique and review self-management strategies, including asthma control, smoking cessation, use of an action plan, and environmental control which may also have contributed to lowering the exacerbation event rates in the present study. Hence, clinicians should insist not only on optimal pharmacotherapy but also on the accessibility to self-management strategies for their patients.
Our findings suggest that there could be a dissociation between asthma control scores which indicated better asthma control in patients with NS-IRAO and the exacerbation rates which was similar between the two groups. The clinical implication of this observation is that the exacerbation rates should not be used as a surrogate for asthma control. Also, lower asthma control in ACO than in NS-IRAO was likely driven by worse symptoms that were unrelated to exacerbations. This indicates the importance of focusing on improving symptoms such as dyspnea and functional limitation and not solely on reducing exacerbation rates when treating patients with IRAO. From a mechanistic point of view, the lower asthma control scores in patients with ACO were possibly related to the persistence of smoking-induced chronic changes in the airways (as in COPD), contributing to symptom generation. For example, glandular hyperplasia, increased/different airway remodeling, or factors associated with lung air trapping (loss of elastic recoil) could all be worse in ACO compared to NS-IRAO group, although this needs to be further studied.
Conclusion
Our results suggest that although symptom control is poorer in patients with ACO as compared to NS-IRAO, the few exacerbations observed in each group do not suggest a higher risk of such events in patients with ACO when appropriately managed. Finally, focusing on symptom control seems equally important than reducing the exacerbation rate in this population.
Acknowledgments
The authors thank Serge Simard for performing all statistical analyses and Justine Veilleux for data entry. We also thank the patients who participated to the study. This study received a non-restrictive investigator-initiated grant from AstraZeneca Canada Inc.
Disclosure
The authors report no conflicts of interest in this work.
References
Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention; 2018. Available from: https://ginasthma.org/wp-content/uploads/2018/04/wms-GINA-2018-report-V1.3-002.pdf. Accessed April 30, 2018. | ||
Postma DS, van den Berge M. The different faces of the asthma-COPD overlap syndrome. Eur Respir J. 2015;46(3):587–590. | ||
Boulet LP, Boulay ME, Dérival JL, et al. Asthma-COPD overlap phenotypes and smoking: comparative features of asthma in smoking or non-smoking patients with an incomplete reversibility of airway obstruction. COPD. 2018;15(2):130–138. | ||
Lougheed MD, Lemiere C, Ducharme FM, et al. Canadian Thoracic Society 2012 guideline update: diagnosis and management of asthma in preschoolers, children and adults. Can Respir J. 2012;19(2):127–164. | ||
Reddel HK, Taylor DR, Bateman ED, et al. An official American thoracic Society/European Respiratory Society statement: asthma control and exacerbations: standardizing endpoints for clinical asthma trials and clinical practice. Am J Respir Crit Care Med. 2009;180(1):59–99. | ||
Juniper EF, O’byrne PM, Guyatt Gh, Ferrie PJ, King DR. Development and validation of a questionnaire to measure asthma control. Eur Respir J. 1999;14(4):902–907. | ||
Juniper EF, Svensson K, Mörk AC, Ståhl E. Measurement properties and interpretation of three shortened versions of the asthma control questionnaire. Respir Med. 2005;99(5):553–558. | ||
Boulet LP, Boulet V, Milot J. How should we quantify asthma control? A proposal. Chest. 2002;122(6):2217–2223. | ||
Leblanc A, Robichaud P, Lacasse Y, Boulet LP. Quantification of asthma control: validation of the asthma control scoring system. Allergy. 2007;62(2):120–125. | ||
Hardin M, Cho M, Mcdonald ML, et al. The clinical and genetic features of COPD-asthma overlap syndrome. Eur Respir J. 2014;44(2):341–350. | ||
Menezes AMB, Montes de Oca M, Pérez-Padilla R, et al. Increased risk of exacerbation and hospitalization in subjects with an overlap phenotype. Chest. 2014;145(2):297–304. | ||
Bai JW, Mao B, Yang WL, Liang S, Lu HW, Xu JF. Asthma-COPD overlap syndrome showed more exacerbations however lower mortality than COPD. QJM. 2017;110(7):431–436. | ||
Andersén H, Lampela P, Nevanlinna A, Säynäjäkangas O, Keistinen T. High Hospital burden in overlap syndrome of asthma and COPD. Clin Respir J. 2013;7(4):342–346. | ||
Gerhardsson de Verdier M, Andersson M, Kern DM, Zhou S, Tunceli O. Asthma and chronic obstructive pulmonary disease overlap syndrome: doubled costs compared with patients with asthma alone. Value Health. 2015;18(6):759–766. | ||
Rhee CK, Yoon HK, Yoo KH, et al. Medical utilization and cost in patients with overlap syndrome of chronic obstructive pulmonary disease and asthma. COPD. 2014;11(2):163–170. | ||
Vaz Fragoso CA, Murphy TE, Agogo GO, Allore HG, McAvay GJ. Asthma-COPD overlap syndrome in the US: a prospective population-based analysis of patient-reported outcomes and health care utilization. Int J Chron Obstruct Pulmon Dis. 2017;12:517–527. | ||
Ding B, Dibonaventura M, Karlsson N, Ling X. Asthma-chronic obstructive pulmonary disease overlap syndrome in the urban Chinese population: prevalence and disease burden using the 2010, 2012, and 2013 China National Health and wellness surveys. Int J Chron Obstruct Pulmon Dis. 2016;11:1139–1150. | ||
Caillaud D, Chanez P, Escamilla R, et al. Asthma-COPD overlap syndrome (ACOS) vs “pure” COPD: a distinct phenotype? Allergy. 2017;72(1):137–145. | ||
Contoli M, Baraldo S, Marku B, et al. Fixed airflow obstruction due to asthma or chronic obstructive pulmonary disease: 5-year follow-up. J Allergy Clin Immunol. 2010;125(4):830–837. | ||
Eisner MD, Iribarren C. The influence of cigarette smoking on adult asthma outcomes. Nicotine Tob Res. 2007;9(1):53–56. | ||
Thomson NC, Chaudhuri R, Heaney LG, et al. Clinical outcomes and inflammatory biomarkers in current smokers and exsmokers with severe asthma. J Allergy Clin Immunol. 2013;131(4):1008–1016. |
Supplementary material
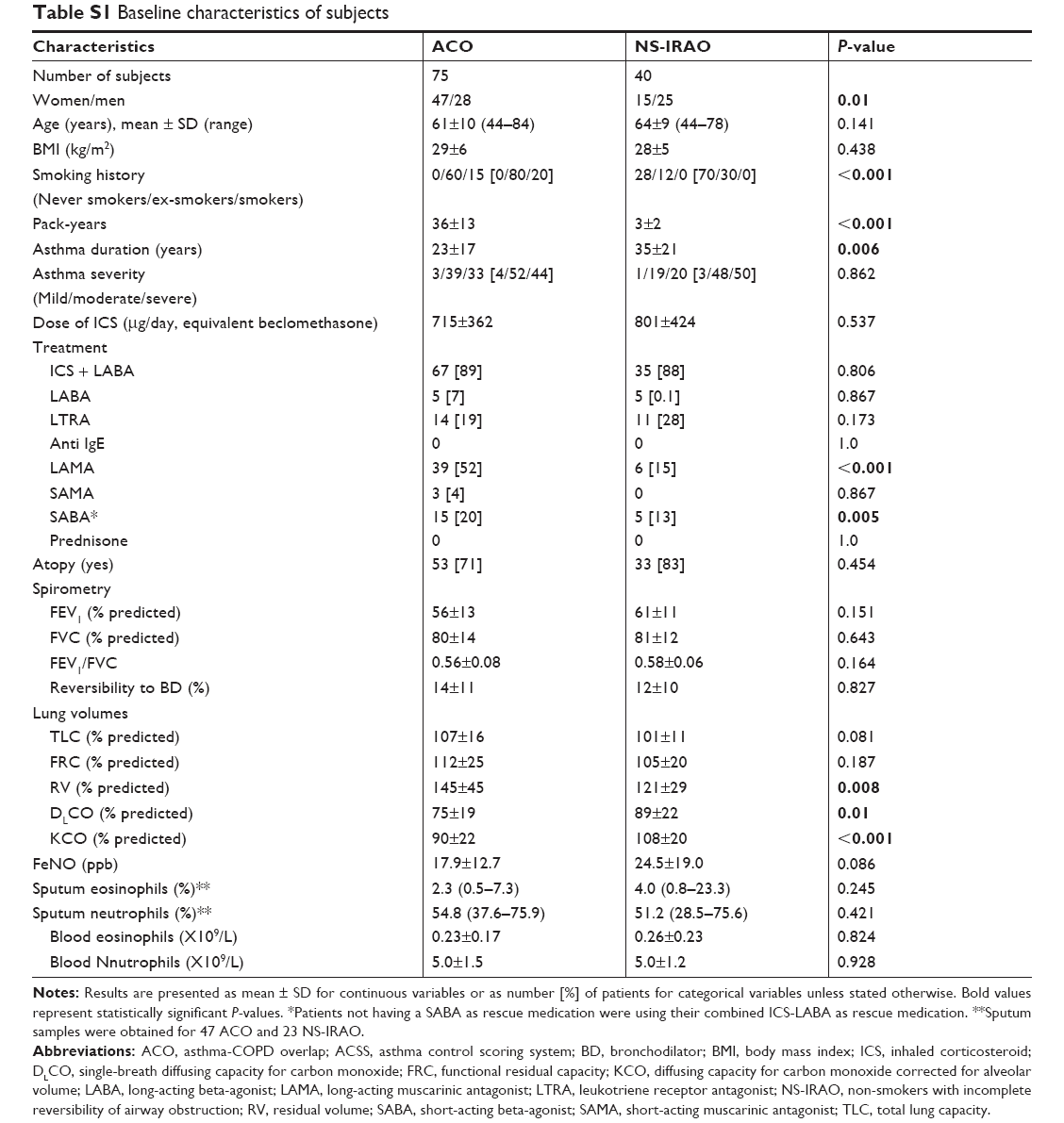 | Table S1 Baseline characteristics of subjects |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.