Back to Journals » Clinical Ophthalmology » Volume 20
Longitudinal Biometric Changes and Intraocular Lens Calculation Formula Accuracy in Delayed Cataract Surgery Cases
Authors Nishida S, Hirata A ![]() , Inomata Y
, Inomata Y
Received 9 October 2025
Accepted for publication 8 January 2026
Published 14 January 2026 Volume 2026:20 571750
DOI https://doi.org/10.2147/OPTH.S571750
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Shohei Nishida,1 Akira Hirata,2 Yasuya Inomata1
1Department of Ophthalmology, Inomata Eye Clinic, Kumamoto City, Kumamoto, Japan; 2Department of Ophthalmology, Hayashi Eye Hospital, Fukuoka City, Fukuoka, Japan
Correspondence: Yasuya Inomata, Inomata Eye Clinic, 4-1-21, Simoezu, Higasi-ku, Kumamoto City, Kumamoto, Japan, Tel +81962738823, Fax +81962738825, Email [email protected]
Purpose: To compare postoperative refractive error (PE) calculated using intraocular lens (IOL) calculation formulas based on initial and remeasured ocular parameters in cases of delayed cataract surgery.
Patients and Methods: Patients who underwent delayed cataract surgery (ie, postponed for > 3 months) between February 2017 and April 2025 were included. Initial and remeasured ocular parameters were compared, namely axial length, mean keratometric power, anterior chamber depth (ACD), and lens thickness (LT). Expected refractions were calculated using the Sanders-Retzlaff-Kraff/Theoretical (SRK/T), Haigis, Barrett Universal II (BU II), Kane, and Emmetropia Verifying Optical (EVO) formulas. PEs were compared between the initial and remeasured data for each IOL calculation formula.
Results: The study included 57 eyes from 57 patients. Cataract surgery was delayed for an average of 14 months. Comparing the initial versus remeasured data, ACD deeper significantly and LT thinner significantly among the ocular parameters. The mean PE indicated a significant myopic shift for both the Haigis formula (0.02 D to − 0.05 D) and EVO formula (0.00 D to − 0.06 D) (paired t-test: p = 0.04, 0.03), while the other formulas had no significant differences. The mean absolute error and median absolute error showed no significant differences among the IOL calculation formulas. Based on the remeasured data, the results of the multiple regression analysis showed that only LT was a significant associated factor in the Haigis formula (estimate = 0.56, p = 0.02), whereas no significant associated factors were identified for the EVO formula.
Conclusion: It was suggested that the characteristics of each IOL calculation formula must be taken into consideration when selecting IOL power for delayed surgery.
Keywords: phacoemulsification, ocular parameters, postoperative refractive error, lens thickness
Introduction
In cataract surgery, recent advancements in surgical instruments1 and biometric technology,2 as well as new-generation intraocular lens (IOL) calculation formulas,3 have markedly improved the postoperative refractive accuracy.4 IOL power is calculated using various formulas based on preoperative ocular parameters, and the choice of formula used is an important factor affecting postoperative refractive accuracy. These ocular parameters are obtained prior to surgery and include axial length (AL), keratometric power (K), anterior chamber depth (ACD), lens thickness (LT), and white-to-white (WTW). The third-generation Sanders-Retzlaff-Kraff/Theoretical (SRK/T)5 formula uses AL and K, while the fourth-generation Haigis6 formula uses AL, K, and ACD. New-generation IOL calculation formulas3,7 incorporate LT and WTW in addition to AL, K, and ACD as optional elements to improve postoperative accuracy. These baseline ocular parameters are measured when cataract surgery is scheduled. However, in reality, surgery can sometimes be postponed for several months to years due to patient circumstances, financial reasons, or other factors. At that time, a clinical judgment must be made as to whether the initial data remain appropriate for IOL power calculation. Since ocular parameters and cataracts change with age,8,9 these ocular parameters should be remeasured in order to properly recalculate IOL power if surgery is postponed. However, at present, there are still no clear guidelines regarding the most appropriate ocular parameters to use in cases of delayed cataract surgery. Unfortunately, reports that describe these changes over time in the same patients are rare, and thus its impact on the IOL calculation formulas and corresponding postoperative refractive error (PE) remains unclear. This issue is particularly important for new-generation IOL calculation formulas that incorporate multiple ocular parameters, as their sensitivity to temporal changes in ocular parameters may differ among IOL calculation formulas. In other words, if cataract surgery is delayed, selecting an IOL based on initial data can result in PEs due changes ocular parameters. Conversely, selecting an IOL based on remeasured parameters can theoretically account for any changes in these ocular parameters. However, in advanced cataracts, the shape of the eye differs from the original LT and ACD, which may also cause PE.10,11 Therefore, changes in ACD and LT associated with cataract progression do not necessarily lead to improved accuracy simply by remeasurement. To address this knowledge gap, this study measured changes in ocular parameters in patients with delayed cataract surgery, predicted refraction based on initial and remeasured data, and compared the PE between various IOL calculation formulas.
Material and Methods
This study is a retrospective paired study of cases in which cataract surgery was delayed.
Ethics Approval and Informed Consent
This study was conducted in accordance with the provisions of the Declaration of Helsinki and was approved by the Kumamoto Clinical Ophthalmology Ethics Review Board (approval number: 2025–6). Informed consent was waived because only anonymized data was used.
Patient Selection
This study included cases wherein delayed cataract surgery (ie, postponed for more than 3 months) was performed between February 2017 and April 2025, with follow-up for 4 weeks after surgery. In-the-bag implantation was performed using a non-toric one-piece hydrophobic acrylic IOL (HOYA iSert Micro [HOYA Surgical Opticals, Inc.,] Tecnis OptiBlue [Johnson & Johnson Surgical Vision, Inc.,]) or a three-piece hydrophobic acrylic IOL (Eternity Fine Natural [Santen Pharmaceutical Co., Ltd.,]). The exclusion criteria included diseases that could influence PE other than cataracts, a history of diabetes mellitus (DM) that could influence the cornea or lens,12,13 previous anterior or posterior segment surgery, and best corrected visual acuity of less than 20/25 at 4 weeks postoperatively. If surgery was postponed for both eyes, then either the left or right eye was included in the analysis, selected at random. A swept-source optical coherence tomography-based biometer (OA-2000TM [TOMEY Corp. Nagoya-City, Aichi, Japan]) was used to measure ocular parameters (ie, AL, K, ACD [from the corneal epithelium to the lens], and LT) before surgery postponement and after the decision to reschedule surgery. Ocular parameters were measured by multiple experienced orthoptists, and only measurements with a signal-to-noise ratio of ≥3 and no warning indications were included. Remeasured data was obtained within two weeks before surgery, after the decision to operate was made.
IOL Calculation Formulas
The following formulas were used for IOL calculation: SRK/T,5 a vergence-based, thin-lens theoretical formula; Haigis,6 which is also vergence-based and incorporates thin-lens theory with a regression approach; Barrett Universal II (BU II),14 a ray-tracing-based, thick-lens theoretical formula; Kane,15 a hybrid model combining regression and artificial intelligence; and Emmetropia Verifying Optical (EVO),16 which is based on the theory of achieving emmetropia. The BU II formula was used to calculate the implanted IOL power. A-constants were adopted from the User Group for Laser Interference Biometry. For each IOL model, the constants were set as follows. For the HOYA iSert Micro (HOYA Surgical Opticals, Inc.,), the A-constant was 118.5 with a0 = −0.542, a1 = 0.161, and a2 = 0.204. For the Tecnis OptiBlue (Johnson & Johnson Surgical Vision, Inc.,), the A-constant was 119.5 with a0 = −0.329, a1 = 0.332, and a2 = 0.203. For the Eternity Fine Natural (Santen Pharmaceutical Co., Ltd.,), the A-constant was 119.6 with a0 = 1.860, a1 = 0.400, and a2 = 0.100.
PE
The expected refraction of each formula was subtracted from the spherical equivalent of the objective refraction using an autorefractometer (model ARK-1a from Nidek Co., Ltd. Nagoya-City, Aichi, Japan) at 4 weeks postoperatively17 and evaluated as the refractive error. For the mean PE (ME), positive and negative values represent refractive error for hyperopia and myopia, respectively. The ME, mean absolute error (MAE), median absolute error (MedAE), and the proportion of PE were compared between the different IOL calculation formulas using both the initial and remeasured data. A modified version of the method proposed by Fernandes et al18 was used to rank the IOL calculation formulas based on multiple accuracy metrics, including the ME, standard deviation, MedAE, root mean square error (RMSE),19 and the percentage of eyes with a PE within ±0.25, ±0.50, and ±1.00 diopters (D). Additionally, for the IOL calculation formulas in which a significant difference in PE was observed, multiple regression analysis was performed with the PE as the dependent variable and each ocular parameter as the independent variables.
Statistical Analysis
Statistical analyses were performed using RStudio (version 2025.05.1 Build 513)20 following previously published protocols.17 Data normality was assessed using the Kolmogorov–Smirnov test. The χ2 test was used to compare ages between the initial and remeasured data. The paired t-test was used to compare ME and MAE between each IOL calculation formula (initial and remeasured data), while the Wilcoxon signed-rank test was used to compare MedAE. McNemar’s test was used to compare the percentage of PEs. Statistical significance was set at p < 0.05.
Results
Table 1 shows the subjects and changes in ocular parameters based on the initial and remeasured data. The study included a total of 57 eyes from 57 patients, with a mean postponement period of 14 months (range: 3–54). Regarding the ocular parameters, there were no significant changes in AL or Mean K, but there was a significant deeper in ACD (3.13 ± 0.40 vs 3.16 ± 0.36 mm, paired t-test: p = 0.04) and a significant thinner in LT (4.69 ± 0.44 vs 4.63 ± 0.39 mm, paired t-test: p = 0.04).
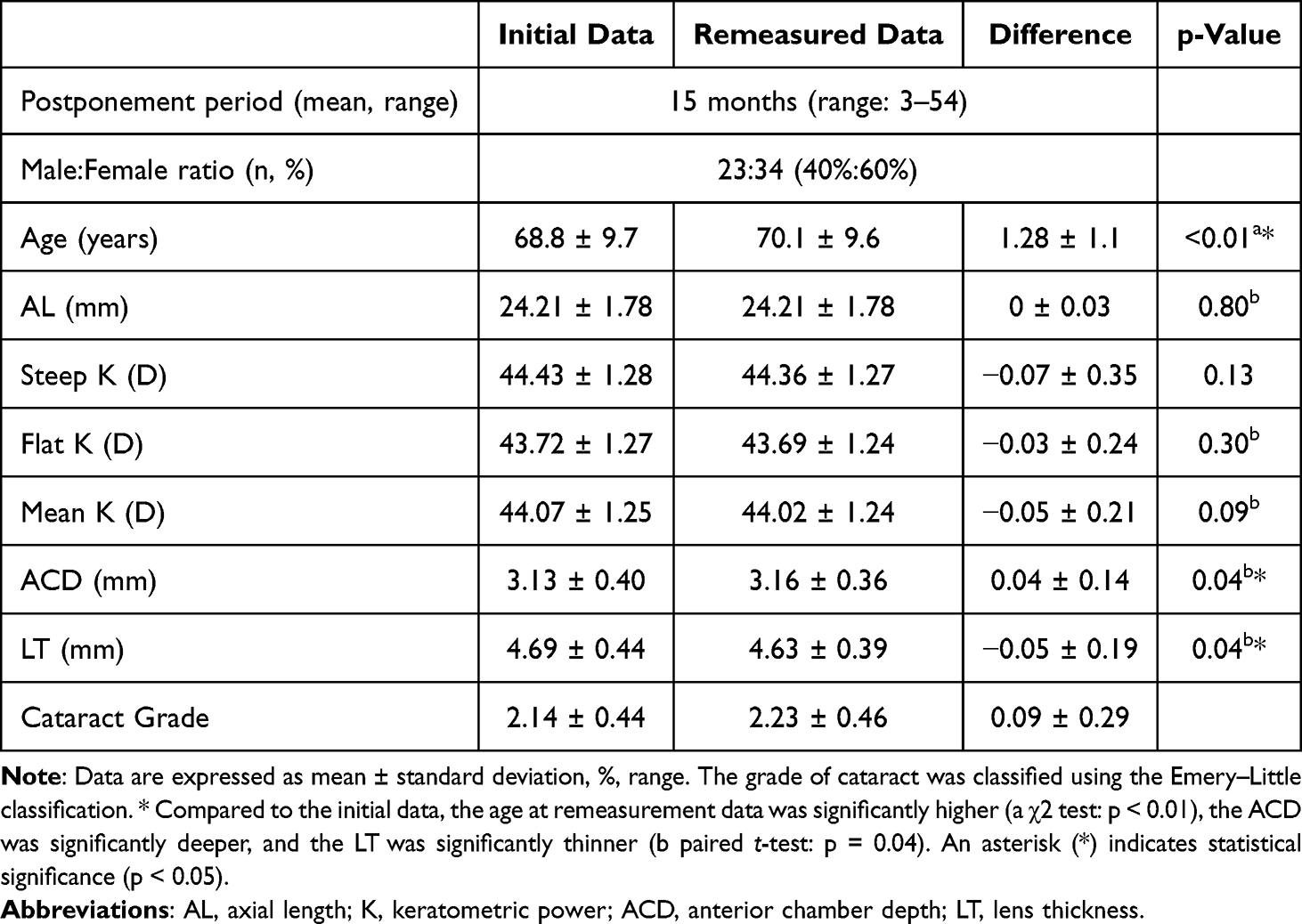 |
Table 1 Subjects and Changes in Ocular Parameters |
Table 2 shows a comparison of the ME based on the initial and remeasured data. The ME demonstrated a significant myopic shift when using both the Haigis formula (0.02 D to −0.05 D) and EVO formula (0.00 D to −0.06 D) (paired t-test: p = 0.04, 0.03). The other IOL calculation formulas demonstrated no statistically significant differences.
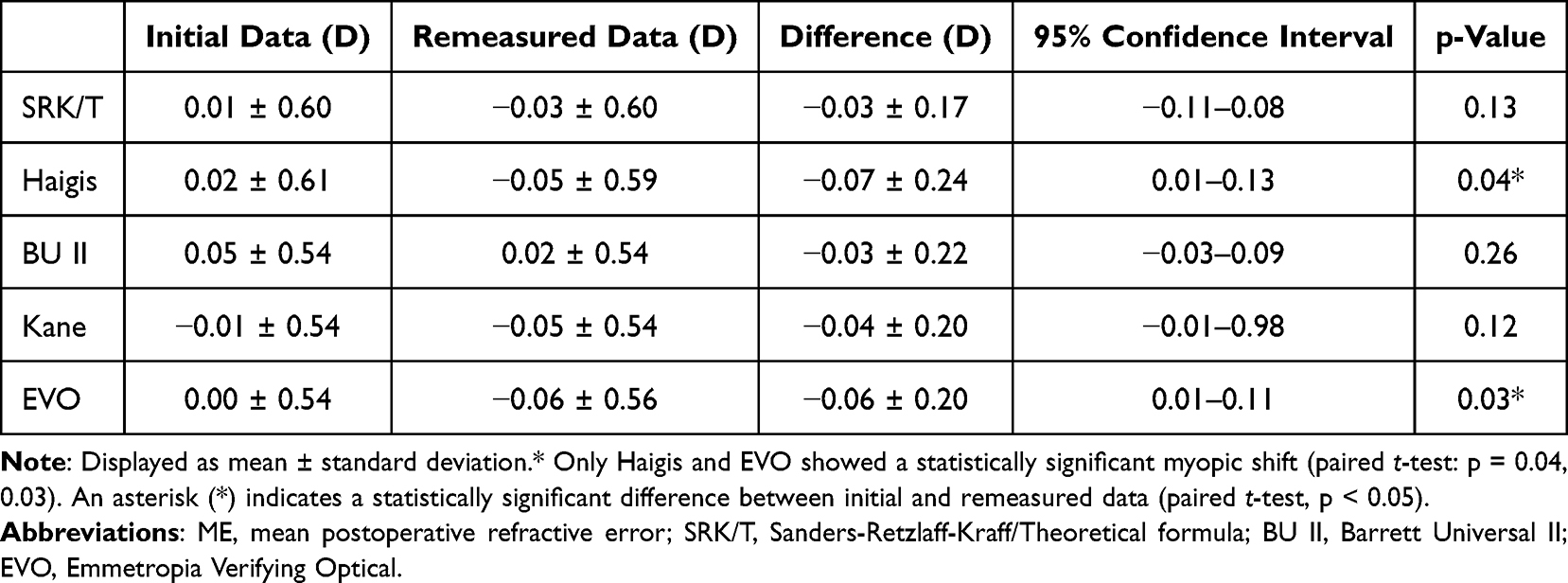 |
Table 2 Comparison of the Mean Postoperative Refractive Error Based on the Initial and Remeasured Data |
Table 3 compares the MAE and MedAE based on the initial and remeasured data. No significant differences were observed among all IOL calculation formulas in MAE or MedAE (paired t-test: p > 0.05, Wilcoxon signed-rank test: p > 0.05).
 |
Table 3 Comparison of the Mean and Median Absolute Errors Based on the Initial and Remeasured Data |
Table 4 shows the percentage of PE. No significant differences were observed among all IOL calculation formulas in the percentages of eyes within ±0.25 D, ±0.50 D, and ±1.00 D (McNemar’s test: all p > 0.05).
 |
Table 4 Distrubution of Postoperative Refractive Error |
Table 5 ranks the IOL calculation formulas based on the initial and remeasured data. New-generation IOL calculation formulas (EVO and Kane) tended to demonstrate higher accuracy based on the initial data.
 |
Table 5 Ranking of the Intraocular Lens Calculation Formulas Based on the Initial and Remeasured Data |
Table 6 shows the results of the multiple regression analysis for the Haigis and EVO formulas based on the remeasured data. In the Haigis formula, only LT was a significant associated factor (estimate = 0.56, p = 0.02), whereas no significant associated factors were identified for the EVO formula.
 |
Table 6 Multiple Regression Analysis Results for Haigis and EVO Based on Remeasured Data |
Discussion
This study compared the PEs of IOL calculation formulas based on the initial and remeasured ocular parameter data in cases of delayed cataract surgery. The main reasons for surgical delay were cases in which patients experienced improved vision after surgery in one eye and therefore judged that surgery in the fellow eye was not urgent, as well as personal factors such as work-related circumstances and anxiety about surgery. There was a significant myopic shift in ME when using the remeasured data in the Haigis and EVO formulas. Among the ocular parameters, LT demonstrated a statistically significant decrease. A negative correlation between cortical cataract and LT has been previously documented,21 which is in line with our findings. Regarding the PE based on the initial and remeasured data, Yun et al22 reported that the remeasured data had a higher accuracy of IOL power calculation, in contrast with the findings of this study. This difference in results can be attributed to differences in LT associated with DM, since patients with DM have a significantly thicker LT.23 Although the overall results of previous studies showed no significant difference in LT, their supplementary information indicated that LT was significantly thinner among patients without DM, which is consistent with the changes in ocular parameters observed in this study. Although previous studies did not compare the PE specifically among patients without DM, it is still possible that LT thickening associated with DM masked the LT thinning observed in patients without DM. A significant myopic shift in ME was seen using remeasured data with the Haigis and EVO formulas only. For the Haigis formula, this result can be attributed to the discrepancy between the predicted effective lens position (ELP) and the actual postoperative IOL position. Since the Haigis formula is a thin-lens theoretical formula, it is affected by changes in LT.24 With thinner LT values, the ELP tends to be overestimated, leading to the selection of a higher-power IOL and a subsequent myopic shift in ME. Meanwhile, the EVO formula is known to have a high predictive accuracy.7,24–27 While the EVO formula also demonstrated high accuracy based on the remeasured data in this study, it showed even higher accuracy when based on the initial data. (Table 5). In the multiple regression analysis based on the remeasured data, LT was a significant factor in the Haigis formula (estimate = 0.56, p = 0.02), showing a tendency toward a hyperopic shift with thicker LT and a myopic shift with thinner LT, whereas no significant associated factors were identified for the EVO formula. The specific algorithm of EVO formula has not been disclosed, and the sample size of this study was small. Thus, the factors contributing to this myopic shift when using the remeasured data in the EVO formula could not be ascertained. The limitations of this study are as follows: the observed change in LT may fall within the range of measurement variability of the biometric device and therefore should be interpreted with caution as a true anatomical change; progression of cataract opacity may impair not only the accuracy of biometric measurements but also fundus visualization, potentially increasing measurement errors, particularly in eyes with posterior staphyloma; and the limited sample size resulted in insufficient statistical power, preventing the identification of definitive factors contributing to the myopic shift. In the supplementary linear regression analysis examining the association between the delay period and changes in ocular parameters, all p values were > 0.05, and no significant associations were observed. The results of this study suggest that IOL power calculations based on the initial and remeasured ocular parameters may yield different PEs depending on the IOL calculation formula used. Not all IOL calculation formulas demonstrated consistent behavior, and statistically significant differences were observed in some formulas. These findings indicate that, in cases of delayed cataract surgery, the characteristics of each IOL calculation formula should be taken into consideration when determining IOL power. Further studies involving larger and more homogeneous cohorts are warranted.
Conclusion
In cases of postponed cataract surgery, a significant myopic shift was observed when remeasured data were used with the Haigis and EVO formulas. Therefore, it is suggested that IOL power selection in delayed surgery should take into account the characteristics of each IOL calculation formula.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available due to patient privacy concerns and restrictions imposed by the institutional ethics committee, but are available from the corresponding author on reasonable request.
Acknowledgments
The authors would like to thank Enago (www.enago.com) for the English language.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lin H-Y, Chuang Y-J, Lin P-J, Ho Y-J. Novel method for preventing cyclorotation in Ziemer Femto LDV Z8 femtosecond laser-assisted cataract surgery with Verion image-guided system. Clin Ophthalmol. 2019;13:415–8. doi:10.2147/opth.s177219
2. Sorkin N, Achiron A, Abumanhal M, et al. Comparison of two new integrated SS-OCT tomography and biometry devices. J Cataract Refract Surg. 2022;48(11):1277–1284. doi:10.1097/j.jcrs.0000000000000974
3. Stopyra W, Langenbucher A, Grzybowski A. Intraocular lens power calculation formulas-a systematic review. Ophthalmol Ther. 2023;12(6):2881–2902. doi:10.1007/s40123-023-00799-6
4. Nishida S, Inomata Y, Hirata A. Risk factors for postoperative refractive error in new-generation intraocular lens calculation formulas. Clin Ophthalmol. 2024;18:2253–2259. doi:10.2147/opth.s471393
5. Retzlaff JA, Sanders DR, Kraff MC. Development of the SRK/T intraocular lens implant power calculation formula. J Cataract Refract Surg. 1990;16(3):333–340. doi:10.1016/s0886-3350(13)80705-5
6. Langenbucher A, Szentmáry N, Wendelstein J, Cayless A, Fassbind B, Hoffmann P. Considerations on the Haigis formula: are better outcomes possible with tuning? Acta Ophthalmol. 2025;103(5):e298–e309. doi:10.1111/aos.17491
7. Pomberger L, Tasch L, Mayer-Xanthaki C, Reifeltshammer SA, Bolz M, Hirnschall N. Clinical feasibility of the ESCRS IOL power calculator. J Cataract Refract Surg. 2025;51(6):504–510. doi:10.1097/j.jcrs.0000000000001637
8. Hashemi H, Khabazkhoob M, Iribarren R, Emamian MH, Fotouhi A. Five-year change in refraction and its ocular components in the 40- to 64-year-old population of the Shahroud eye cohort study. Clin Exp Ophthalmol. 2016;44(8):669–677. doi:10.1111/ceo.12753
9. Lei Q, Tu H, Feng X, Ortega-Usobiaga J, Cao D, Wang Y. Distribution of ocular biometric parameters and optimal model of anterior chamber depth regression in 28,709 adult cataract patients in China using swept-source optical biometry. BMC Ophthalmol. 2021;21(1):178. doi:10.1186/s12886-021-01932-4
10. Yesilkaya EC, Garip R. Accuracy of different lens power calculation formulas in patients with mature cataracts. Cureus. 2023;15(10):e47053. doi:10.7759/cureus.47053
11. Zhao J-F, Yang C, Zhou J, Zhang H-Y, Geng Y. Assessment of the variability and correlation of biometric measurements in eyes with cataracts. Photodiagnosis Photodyn Ther. 2025;51:104453. doi:10.1016/j.pdpdt.2024.104453
12. Khan A, Petropoulos IN, Ponirakis G, Malik RA. Visual complications in diabetes mellitus: beyond retinopathy. Diabet Med. 2017;34(4):478–484. doi:10.1111/dme.13296
13. Ljubimov AV. Diabetic complications in the cornea. Vision Res. 2017;139:138–152. doi:10.1016/j.visres.2017.03.002
14. Barrett Universal. Formula version1.05. Available from: http://calc.apacrs.org/barrett_universal2105/.
15. Kane Formula. Kane formula official page. Available from: https://www.iolformula.com/.
16. EVO Formula. Emmetropia verifying optical formula: IOL calculator v2.0. Available from: https://www.evoiolcalculator.com/calculator.aspx.
17. Hoffer KJ, Savini G. Update on intraocular lens power calculation study protocols: the better way to design and report clinical trials. Ophthalmology. 2021;128(11):e115–e120. doi:10.1016/j.ophtha.2020.07.005
18. Hipólito-Fernandes D, Elisa Luís M, Maleita D, et al. Intraocular lens power calculation formulas accuracy in combined phacovitrectomy: an 8-formulas comparison study. Int J Retina Vitreous. 2021;7(1):47. doi:10.1186/s40942-021-00315-7
19. Hill WE, Abulafia A, Wang L, Koch DD. Pursuing perfection in IOL calculations. II. Measurement foibles: measurement errors, validation criteria, IOL constants, and lane length. J Cataract Refract Surg. 2017;43(7):869–870. doi:10.1016/j.jcrs.2017.07.006
20. Ariel de Lima D, Helito CP, de Lima LL, Clazzer R, Gonçalves RK, de Camargo OP. How to perform a meta-analysis: a practical step-by-step guide using R Software and RStudio. Acta Ortop Bras. 2022;30(3):e248775. doi:10.1590/1413-785220223003e248775
21. Klein BE, Klein R, Moss SE. Lens thickness and five-year cumulative incidence of cataracts: the Beaver dam eye study. Ophthalmic Epidemiol. 2000;7(4):243–248. doi:10.1076/opep.7.4.243.4176
22. Yun YI, Oh R, Oh JY, Choi HJ, Kim MK, Yoon CH. Longitudinal changes in ocular biometry and their effect on intraocular lens power calculation accuracy in cataract patients. Graefes Arch Clin Exp Ophthalmol. 2025;263(7):1915–1924. doi:10.1007/s00417-025-06775-z
23. Fledelius HC, Miyamoto K. Diabetic myopia--is it lens-induced? An oculometric study comprising ultrasound measurements. Acta Ophthalmol. 1987;65(4):469–473. doi:10.1111/j.1755-3768.1987.tb07025.x
24. Hipólito-Fernandes D, Luís ME, Serras-Pereira R, et al. Anterior chamber depth, lens thickness and intraocular lens calculation formula accuracy: nine formulas comparison. Br J Ophthalmol. 2022;106(3):349–355. doi:10.1136/bjophthalmol-2020-317822
25. Voytsekhivskyy OV, Hoffer KJ, Cooke DL, Savini G. IOL Power calculation project: accuracy of 36 formulas. Am J Ophthalmol. 2025;277:45–56. doi:10.1016/j.ajo.2025.05.004
26. Kothari SS, Reddy JC. Recent developments in the intraocular lens formulae: an update. Semin Ophthalmol. 2023;38(2):143–150. doi:10.1080/08820538.2022.2094712
27. Sorkin N, Zadok R, Totah H, et al. Analysis of the ESCRS calculator’s prediction accuracy. J Cataract Refract Surg. 2024;50(11):1109–1116. doi:10.1097/j.jcrs.0000000000001512
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.