Back to Journals » Clinical Ophthalmology » Volume 14
Long-Term Visual, Refractive and Topographic Outcomes of “Epi-off” Corneal Collagen Cross-Linking in Pediatric Keratoconus: Standard versus Accelerated Protocol
Authors Amer I, Elaskary A, Mostafa A, Hazem HA ![]() , Omar A
, Omar A ![]() , Abdou A
, Abdou A ![]()
Received 12 August 2020
Accepted for publication 29 September 2020
Published 3 November 2020 Volume 2020:14 Pages 3747—3754
DOI https://doi.org/10.2147/OPTH.S275797
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ibrahim Amer,1 Abdelhakeem Elaskary,1 Ali Mostafa,2 Hazem A Hazem,2 Ahmed Omar,2,3 Ahmed Abdou2
1Ophthalmology Department, Faculty of Medicine, AL-Azhar University, Assiut, Egypt; 2Ophthalmology Department, Faculty of Medicine, Assiut University, Assiut, Egypt; 3University Hospitals Eye Institute and the Department of Ophthalmology and Visual Sciences, Case Western Reserve University School of Medicine, Cleveland, Ohio, USA
Correspondence: Ahmed Abdou
Ophthalmology Department, Faculty of Medicine, Assiut University, Assiut 71515, Egypt
Tel +201004343388
Email [email protected]
Purpose: To compare the visual, refractive and topographic outcomes of standard and accelerated corneal collagen cross-linking (CXL) in pediatric keratoconus patients.
Methods: Prospective, comparative observational study on 68 eyes of 35 pediatric keratoconus patients (< 18 years). Patients were classified into two groups, group (I) included 34 eyes and received standard “Epi-Off” CXL (3 mW/cm2, 30 min.) and group (II) included 34 eyes and received accelerated “Epi-Off” CXL (9 mW/cm2, 10 min.). Uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), spherical equivalent (SE), simulated keratometry (Sim K-1, Sim K-2, K-max, K-mean), cylindrical (CYL), pachymetry and Q-value were evaluated preoperatively and for 3 years postoperatively.
Results: Postoperative UDVA and CDVA did not significantly change in both groups after 3 years. Postoperative SE was increased significantly in accelerated CXL (p=0.012) with no significant change in the postoperative cylinder in both procedures. Standard CXL had greater “significant” effect in decreasing Sim K-1, K-max and K-mean. The mean reduction in postoperative corneal pachymetry (at thinnest location) was significant in standard CXL (18.4 μm) (p=0.001). No significant change was noticed in postoperative Q-value.
Conclusion: Standard and accelerated CXL protocols are efficient in pediatric keratoconus management with better outcomes in the standard procedure.
Keywords: standard CXL, accelerated CXL, corneal collagen cross-linking, pediatric keratoconus
Introduction
Visual impairment has a broad deleterious impact on children and their quality of life and this consequently will affect their social development and education. A degenerative disorder, keratoconus is a progressive and regularly asymmetric corneal ectasia distinguished by localized corneal steepening and thinning, and reduction in visual acuity.1 In general, keratoconus begins at puberty and its progression continues up to the age of 35–40 years.2 Pediatric keratoconus forms about 88% of keratoconus cases and is often diagnosed in a more advanced stage (stage 4) compared with adult keratoconus (27.8% vs 7.8%).3 Thus, the progression of pediatric keratoconus is aggressive with an increased rate of acute hydrops in comparison with the adult population.4,5 The rapid and effective stopping of the progression of the corneal ectasia in pediatric patients is vital to avoid the need for corneal transplantation which is seven-fold higher in pediatric keratoconus patients.6
Corneal cross-linking (CXL) is a procedure that causes photopolymerization of the corneal stromal collagen fibers using ultraviolet-A (UVA) (370 nm) and riboflavin.7,8 For years, this procedure has been widely utilized for the treatment of corneal ectatic disorders such as progressive keratoconus and post-refractive corneal ectasia.1 Corneal collagen cross-linking has been used effectively in the treatment of progressive keratoconus in younger patients.9,10
The original standard CXL procedure involves 5.4 J/cm2 energy with an intensity of 3 mW/cm2 administered for 30 min.11 Many studies have investigated the efficacy and safety of standard CXL. It has been reported that standard CXL stabilized visual acuity along with a marked reduction of maximum keratometry (by 2 diopters) and a progression rate of 22% in pediatric keratoconus patients.12,13
The long operative time of the standard CXL procedure (30 min) is a major drawback, especially in pediatric patients, which favors the application of an accelerated protocol with less duration but more UVA intensity.14,15 Comparable results of both protocols in adult KC treatment were published16,17 but few studies have investigated the two procedures in pediatric KC.
The objective of this study is to evaluate the two different protocols of corneal collagen cross-linking (CXL) in pediatric keratoconus management for a follow-up period of 3 years.
Patients and Methods
This is a prospective, randomized, comparative, observational (cohort) study which was carried out in a refractive eye surgery center (Modern eye center), in Egypt. The study included a total of 68 eyes of 35 pediatric keratoconus patients (<18 years) who underwent standard CXL (n=34 eyes) or accelerated CXL (n=34 eyes). CXL protocol type was decided according to surgeon preference and not at the discretion of the researchers. Keratoconus eyes were suspected clinically in high cylinder patients, not fully corrected visual acuity and family history of vernal keratoconjunctivitis, which were confirmed by topography. Patients were excluded if they had an age of >18 years, corneal thickness <400 μm, previous history of herpetic keratitis, central or paracentral corneal scar and active ophthalmic infection or inflammation. Written informed consent was obtained from the parents of all included patients that was approved by the ethical board committee (IRB) of Faculty of Medicine, AL-Azhar University (Assiut), and followed the tenets of Declaration of Helsinki.18
For all included patients, a complete ophthalmological examination was completed including spherical equivalent (SE), uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), intraocular pressure, slit-lamp examination, fundoscopic examination and corneal topographic analysis using Pentacam HR (WaveLight Allegro Oculyzer II, Erlangen, Germany). Topographic corneal analysis was done including simulated keratometry measurements (Sim K-1, Sim K-2, K-max), cylindrical (CYL) value in addition to corneal thickness at the thinnest point (thCT) and Q-value was recorded. Visual acuity was measured by decimal Snellen chart. These measurements were done at baseline and for 3 years postoperatively.
Surgical Techniques
Topical anesthesia using benoxinate hydrochloride 0.4% eye drops (Benox 0.4%; Eipico Inc., Cairo, Egypt) or general anesthesia (in some cases) was used before CXL. In both standard and accelerated CXL procedures, corneal epithelium was removed mechanically with a Hockey epithelium removal knife at an intended 8.5 mm zone after loosening the epithelium with a 20% alcohol solution applied for 20 s over the cornea within an 8.5 mm alcohol well. Riboflavin drops (0.1% riboflavin, saline with hydroxypropyl methylcellulose “HPMC” solution, VibeX Rapid™, Avedro, USA) were applied to the center of the cornea every 3 min for 30 min. The UVA irradiation was applied using a UVA system (VEGA CBM X-Linker, CSO, Italy).
In the standard CXL procedure, before the UVA treatment, we calibrated the intended 3 mW/cm2 surface irradiance for 30 min using a UVA meter. In the accelerated procedure, 9 mW/cm2 irradiance was applied for 10 min. Both protocols deliver 5.4 J/cm2 surface dosage. A silicone hydrogel bandage contact lens was applied at the end of the surgery until full reepithelialization of the cornea (3–5 days). Postoperatively, the treatment included Gatifloxacin eye drops q.i.d. for 1 week, fluorometholone eye drops q.i.d. on a tapering schedule for 2 months, and artificial tears q.i.d. for 2 months.
Statistical Analysis
Data were analyzed using SPSS software (version 21; International Business Machines Co, Armonk, NY, USA). Data were expressed as the mean ± standard deviation (SD). Paired sample t-test was used for the comparisons between preoperative and postoperative after both CXL procedures. However, independent samples t-test was used to calculate the significance of the difference between CXL procedures. Qualitative data were compared by Chi-square test/Fisher’s exact test when appropriate. P-value less than 0.05 was deemed statistically significant, however, P-value of less than 0.01 was considered as highly significant.
Results
In this study, 34 eyes of 18 patients received standard CXL and 34 eyes of 17 patients received accelerated CXL. In the standard CXL group, there were 7 males (38.9%) and 11 females (61.1%) with a mean age of 15.3 ± 2.0 years. In the accelerated CXL group, there were 7 males (41.2%) and 10 females (58.8%) with a mean age of 15.2 ± 2.5 years. No significant differences were found between the two groups regarding age (p=0.836) and sex (p=0.890). There were no statistically significant differences between groups regarding the preoperative cylinder, spherical equivalent and uncorrected distance visual acuity (p >0.05 for all). Three years postoperatively, significant differences were observed between both procedures regarding sphere (p=0.011), spherical equivalent (p=0.039) and corrected distance visual acuity (p=0.015).
In standard CXL group (group I), within 3 years postoperatively there was an improvement in the mean preoperative sphere and cylinder from −3.24 ± 3.56 D and −3.30 ± 2.46 D to −3.09 ± 3.86 D and −3.15 ± 2.49 D, respectively. But this improvement was not statistically significant (p > 0.05 for all). The mean preoperative UDVA and CDVA were 0.22 ± 0.23 and 0.56 ± 0.26, respectively. However postoperatively, there was a statistically significant change in the mean UDVA (0.23 ± 0.21, p=0.043), whilethe change in CDVA was not significant (0.59 ± 0.25, p=0.119).
In eyes which received accelerated CXL (group II), the postoperative cylinder, UDVA and CDVA remained almost unchanged compared with their preoperative values (p=0.094, p=0.261 and p=0.972, respectively), but a significant change was recorded in the postoperative sphere and spherical equivalent compared with preoperative values (p=0.007 for sphere and p=0.012 for SE). (Table 1).
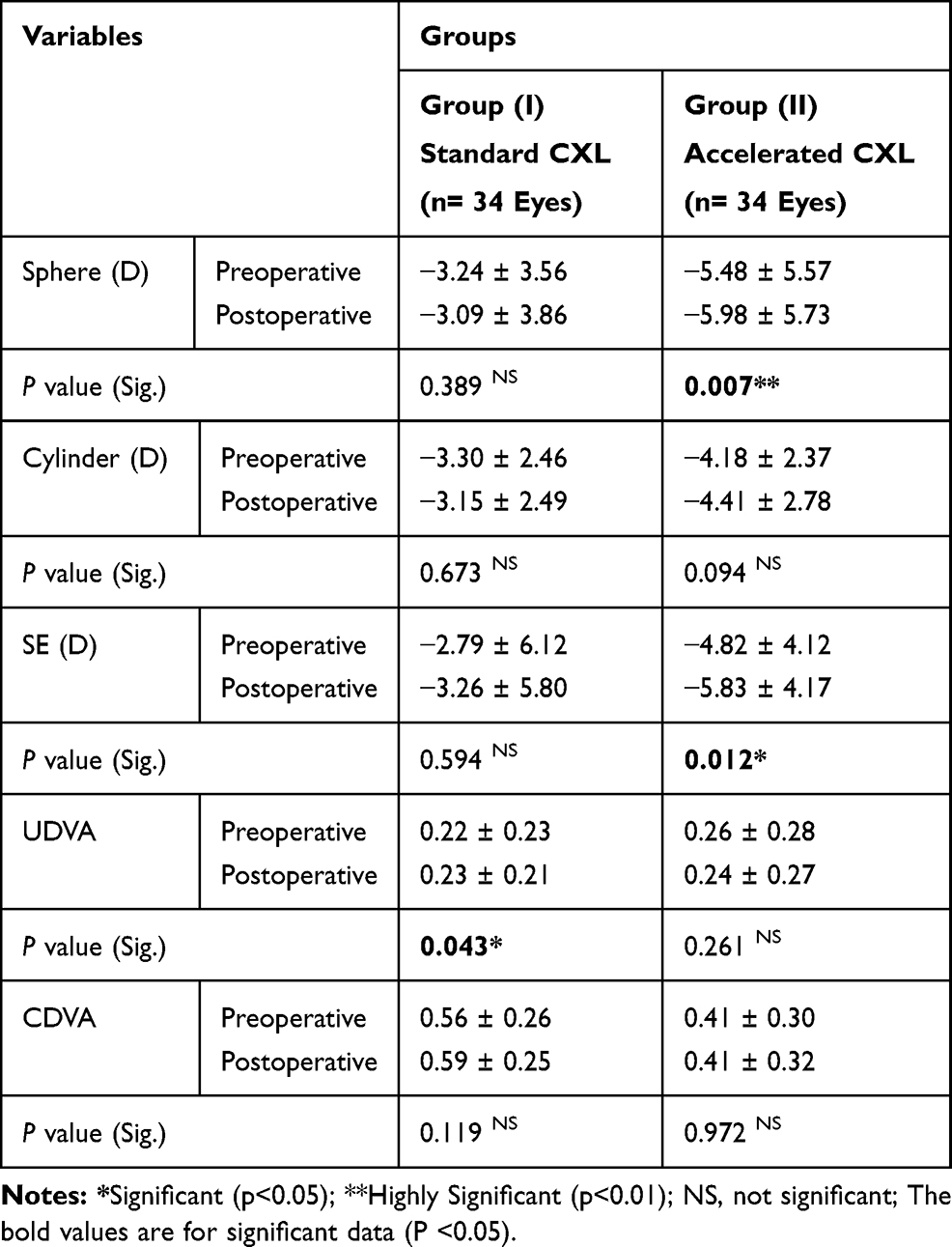 |
Table 1 Visual and Refractive Parameters Between Studied Groups Preoperatively and Postoperatively |
The results presented in Table 2 show that there were no significant differences between the two groups in preoperative Sim K-1, Sim K-2, K-max, thCT and Q-value. In the standard CXL group (group I) postoperatively, there was a flattening of 0.8 D in the mean Sim K-1, 0.5 D in the mean Sim K-2, 1.4 D in the mean K-max and 0.6 D in the K-mean, which was statistically significant (p < 0.05 for all). As regards thCT values, there was a significant reduction in pachymetry (P=0.001), the mean thinnest location value reduced from 458.4 ± 49.5 μm preoperatively to 440.4 ± 52.3 μm postoperatively. However, a non-significant reduction was noticed in Q-value from 0.56 ± 0.45 preoperatively to 0.52 ± 0.47 postoperatively (p=0.287).
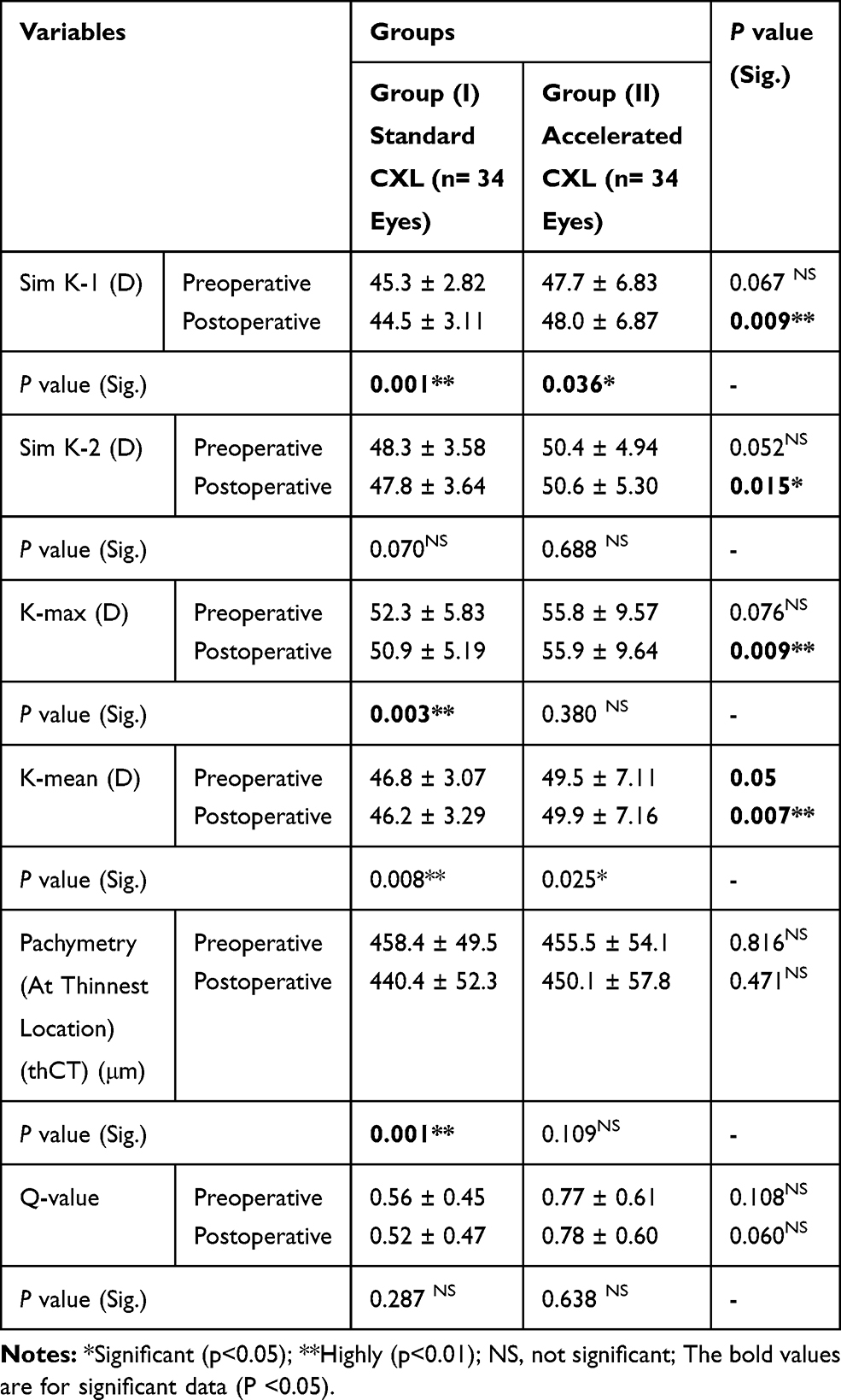 |
Table 2 Topographic Parameters Between Studied Groups Preoperatively and Postoperatively |
In the accelerated CXL group (group II), a significant change was noticed in postoperative Sim K-1 and K-mean (p=0.036 and p=0.025, respectively). However, non-significant changes were observed in postoperative values of Sim K-2 and K-max (p=0.688 and p=0.380, respectively). In the same group, the mean thCT value reduced from 455.5 ± 54.1 μm preoperatively to 450.1 ± 57.8 μm postoperatively, but this reduction was not statistically significant (p=0.109) and Q-value remained almost unchanged postoperatively.
Postoperatively, the accelerated CXL group had significantly higher Sim K-1, Sim K-2, K-max and K-mean compared with standard CXL group (p=0.009, p=0.015, p=0.009 and p=0.007, respectively). However, the differences between groups did not reach significance regarding thCT and Q-value (p=0.471 and p=0.060, respectively). Figures 1 and 2 present preoperative and 3 years postoperative Pentacam maps in patients who underwent standard CXL (Figure 1) and accelerated CXL (Figure 2) which reveal stable topographic readings.
 |
Figure 1 Pentacam maps of a patient of Group (I): Preoperatively (upper maps) and 3 years postoperatively (lower maps). |
 |
Figure 2 Pentacam maps of a patient of Group (II): Preoperatively (upper maps) and 3 years postoperatively (lower maps). |
Discussion
The progression of keratoconus in pediatric patients is aggressive and does not discontinue on its own.17 Treatment of these patients as early as possible can ensure good visual function and avoid keratoplasty complications.19 Corneal collagen cross-linking is a mainstay in keratoconus treatment in pediatric patients20,21 with favorable outcomes.1,9 The standard CXL procedure involves 3 mW/cm2 UVA intensity with 30 min duration which is a major disadvantage22 that encouraged the application of accelerated protocols with much shorter duration.23 In the present study, we compared the results of accelerated CXL (9 mW/cm2, 10 min) with the standard CXL protocol (3 mW/cm2, 30 min) in pediatric keratoconus patients. To our knowledge, few studies have compared the effectiveness of these two protocols in pediatric patients.24,25
The present results revealed that in eyes which received standard CXL, postoperatively there was a slight insignificant improvement in sphere and cylinder, while a slight significant change in UDVA was noticed; however, CDVA remained unchanged. In addition, a statistically significant flattening of the K values was noticed and up to 1.5 reduction in the mean K-max. A significant reduction was recorded in postoperative thCT values, however, the mean Q-value reduced insignificantly. In the accelerated CXL group, the results were conflicting and not as clear as those of standard CXL. A slight insignificant change was noticed in postoperative UDVA, however, CDVA was stable and a significant change was recorded in the postoperative sphere and spherical equivalent compared with preoperative values. In addition, a significant change was observed in postoperative Sim K-1 and K-mean however, non-significant changes were observed in postoperative Sim K-2 and K-max. Furthermore, the mean postoperative thCT reduced insignificantly and Q-value almost remained unchanged.
The results of published studies have been conflicting. As with our results, Waszczykowska and Jurowski26 studied the outcomes of accelerated CXL in patients with progressive keratoconus and did not find any significant improvement in visual acuity. Also, many studies reported that standard CXL was more effective in clinical and topographic outcomes compared with accelerated CXL with a total energy of 5.4 J/cm2 “in adult patients”.27,28 Caporossi et al.29 performed a prospective study which included 152 eyes of 77 younger patients (<18 years) with 3 years follow-up period. They found that after standard CXL, keratoconus stabilized and they demonstrated rapid and significant improvement of visual function. It has been reported that the mechanism by which CXL improves vision is not fully understood; it might be caused by the reduction in corneal steepness and astigmatism, rather than the improvement of different KC topographic indices.30
On the other hand, some studies reported similar outcomes for accelerated CXL in comparison to the standard technique regarding the visual acuity and keratometric indices.31 Mrochen32 reported that the biomechanical stiffening effect on corneal tissue with standard protocol can be achieved using energies up to 10 mW/cm2 with less UVA exposure time. Also, Ozgurhan et al.14 studied the effects of accelerated CXL protocol in pediatric keratoconus patients for 2-year follow-up and found significant improvement of visual, keratometric and aberrometric indices. In addition, Shetty et al.15 studied accelerated CXL (9 mW/cm2 for 10 min) for the treatment of progressive keratoconus in children <14 years. At 2-year follow-up, they found that there was a statistically significant improvement in the mean UDVA, CDVA, cylindrical refraction and keratometry. They concluded that the higher energy and shorter treatment duration of accelerated CXL present a good choice in children; this benefit is especially important in pediatric patients in which cooperation and compliance are the main problems during the surgical procedures. In addition, the fitting of contact lenses was better, amblyopia was prevented and early penetrating keratoplasty was successfully deterred. Similar results were also reported by Badawi with 1-year follow-up period.22 Recently, Henriquez et al.24 found that accelerated epi-on CXL is as safe and effective as standard epi-off CXL in preventing the progression of pediatric keratoconus at one year postoperatively. They found non-significant changes in UDVA, CDVA, keratometry, pachymetry and posterior elevation. Similar results were also published by Sarac et al.25 for up to 2 years postoperatively.
Although the main objective of CXL is to stabilize the cornea rather than to improve its shape, reduction of the keratometric values is used to assess the efficacy of the procedure. In the present study, the obtained results regarding the stability and the non-significant change of Sim-K2 and K-max values in accelerated CXL were partly in agreement with previous studies.14,33 While, Shetty et al.15 found approximately 2 D flattening in both K1 and K2 after 2 years following accelerated CXL. Also, Badawi22 found a statistically significant decrease in the mean anterior surface keratometry in steep and flat axes with flattening of 0.76 D in K1, 1.1 D in K2 and 1.2 D in K-max mean (at 1-year postoperatively).
It has been reported that K-max is an important parameter to reveal disease progression.34 Also, K-max is a significant indicator of the success of CXL; it significantly reduced after CXL (up to 2.01 D).11 In the present study, a highly significant reduction was recorded in postoperative K-max in standard CXL (p=0.003) however, almost no change was recorded in postoperative K-max in accelerated CXL. These findings partly agreed with Saraca et al.1 who found that K-max values “2 years postoperative” were reduced significantly in standard CXL in pediatric patients. Also, Ozgurhan et al.14 reported a significant improvement in keratometric values in accelerated CXL, which was not fully reported in our study. These results were comparable to other studies that evaluated the standard CXL procedure9,21 and studies utilizing accelerated CXL.15 However, Duncan et al.35 published that K-max is a poor parameter for both progression and cross-linking efficacy, because K-max fails to reflect the degree of ectasia, so noticeable progression can happen without a change in K-max.36
In the existing study, the mean reduction in postoperative thCT was higher in standard CXL “18.4 μm” compared with accelerated CXL “5.4 μm” (p=0.001). Changes that occurred in the corneal thickness after CXL procedures may be due to various reasons such as the keratocyte restoration process, corneal lamellae rescheduling, corneal stroma changes, reduction in the proteoglycan, corneal ischemia, structural and anatomical changes in collagen fibers and the new epithelium arrangement.8,37 Caporossi et al.20 reported reduction after long-term follow-up (more than 4 years) using standard CXL. Badawi22 and Saraca et al.25 reported similar results using the accelerated procedure with significant reduction in corneal pachymetry, while Tian et al. found no significant difference between TCT (thinnest corneal thickness) before and after accelerated pediatric CXL.38 Non-significant change of Q-value in both techniques is another sign of stopping keratoconus progression. Badawi22 described the importance of Q-value in evaluating the progression of keratoconus and reported its significant improvement after accelerated CXL in pediatric keratoconus.
There were no complications noted in our study such as infectious keratitis and stromal opacity in any of the patients after both CXLs, indicating the safety of both procedures. Similarly, Saraca et al.1 did not find any postoperative complications in pediatric patients who underwent standard CXL. Similar results were obtained using the accelerated technique.14,15
This study has strengths and limitations. A strong point is the relatively good sample number of patients with long-term evaluation after 3 years of CXL. One of the limitations is the failure to study the course of the disease after CXL due to the lack of regular follow-ups and frequent evaluation (we usually suffer from this problem in upper Egypt with low socioeconomic status). A larger number of patients and tri-monthly evaluation are strongly recommended.
Conclusion
In conclusion, standard and accelerated CXL are safe and effective in treatment of pediatric keratoconus with better outcomes with the standard procedure (standard CXL has a greater effect in decreasing Sim K-1, Sim K-2, K-max and K-mean). The lack of regular follow-up was the main limitation of our study. Compliance problems, higher energy and shorter duration of treatment are the main advantages of accelerated CXL procedure that make it recommended especially for pediatric patients. Finally, our obtained results need to be supported by subsequent studies.
Ethical Consideration
All patient data collected comply with the relevant data protection and privacy regulations.
Disclosure
None of the authors have any financial or proprietary interests to disclose. The authors report no conflicts of interest for this work. Early results of the study were presented at the ESCRS meeting, Paris 2019.
References
1. Sarac O, Caglayan M, Cakmak HB, Cagil N. Factors Influencing Progression of Keratoconus 2 Years After Corneal Collagen Cross-Linking in Pediatric Patients. Cornea. 2016;35(12):1503–1507. doi:10.1097/ICO.0000000000001051
2. Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42(4):297–319. doi:10.1016/S0039-6257(97)00119-7
3. Leoni-Mesplie S, Mortemousque B, Touboul D, et al. Scalability and severity of keratoconus in children. Am J Ophthalmol. 2012;154(1):56–62. doi:10.1016/j.ajo.2012.01.025
4. Li X, Yang H, Rabinowitz YS. Longitudinal study of keratoconus progression. Exp Eye Res. 2007;85(4):502–507. doi:10.1016/j.exer.2007.06.016
5. Arora R, Lohchab M. Pediatric keratoconus misdiagnosed as meridional amblyopia. Indian J Ophthalmol. 2019;67(4):551–552. doi:10.4103/ijo.IJO_1496_18
6. Reeves SW, Stinnett S, Adelman RA, Afshari NA. Risk factors for progression to penetrating keratoplasty in patients with keratoconus. Am J Ophthalmol. 2005;140(4):607–611. doi:10.1016/j.ajo.2005.05.029
7. Wollensak G. Crosslinking treatment of progressive keratoconus: new hope. Curr Opin Ophthalmol. 2006;17(4):356–360. doi:10.1097/01.icu.0000233954.86723.25
8. Blackburn BJ, Jenkins MW, Rollins AM, Dupps WJ. A Review of Structural and Biomechanical Changes in the Cornea in Aging, Disease, and Photochemical Crosslinking. Fron Bioeng Biotechnol. 2019;7:66. doi:10.3389/fbioe.2019.00066
9. Chatzis N, Hafezi F. Progression of Keratoconus and Efficacy of Corneal Collagen Cross-linking in Children and Adolescents. J Refractive Surgery. 2012;28(11):753–758. doi:10.3928/1081597X-20121011-01
10. Perez-Straziota C, Gaster RN, Rabinowitz YS. Corneal Cross-Linking for Pediatric Keratcoconus Review. Cornea. 2018;37(6):802–809. doi:10.1097/ICO.0000000000001579
11. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a–induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135(5):620–627. doi:10.1016/S0002-9394(02)02220-1
12. Padmanabhan P, Rachapalle Reddi S, Rajagopal R, et al. Corneal Collagen Cross-Linking for Keratoconus in Pediatric Patients—Long-Term Results. Cornea. 2017;36(2):138–143. doi:10.1097/ICO.0000000000001102
13. Godefrooij DA, Soeters N, Imhof SM, Wisse RPL. Corneal Cross-Linking for Pediatric Keratoconus: long-Term Results. Cornea. 2016;35(7):954–958. doi:10.1097/ICO.0000000000000819
14. Ozgurhan EB, Kara N, Cankaya KI, Kurt T, Demirok A. Accelerated corneal cross-linking in pediatric patients with keratoconus: 24-month outcomes. J Refractive Surgery. 2014;30(12):843–849. doi:10.3928/1081597X-20141120-01
15. Shetty R, Nagaraja H, Jayadev C, Pahuja NK, Kurian Kummelil M, Nuijts RMMA. Accelerated corneal collagen cross-linking in pediatric patients: two-year follow-up results. Biomed Res Int. 2014;2014:894095. doi:10.1155/2014/894095
16. Cinar Y, Cingu AK, Turkcu FM, et al. Comparison of accelerated and conventional corneal collagen cross-linking for progressive keratoconus. Cutan Ocul Toxicol. 2014;33(3):218–222. doi:10.3109/15569527.2013.834497
17. Ertan A, Muftuoglu O. Keratoconus clinical findings according to different age and gender groups. Cornea. 2008;27(10):1109–1113. doi:10.1097/ICO.0b013e31817f815a
18. World Medical A. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194.
19. Vanathi M, Panda A, Vengayil S, Chaudhuri Z, Dada T. Pediatric keratoplasty. Surv Ophthalmol. 2009;54(2):245–271.
20. Caporossi A, Mazzotta C, Baiocchi S, Caporossi T. Long-term results of riboflavin ultraviolet a corneal collagen cross-linking for keratoconus in Italy: the Siena eye cross study. Am J Ophthalmol. 2010;149(4):585–593. doi:10.1016/j.ajo.2009.10.021
21. Zotta PG, Moschou KA, Diakonis VF, et al. Corneal collagen cross-linking for progressive keratoconus in pediatric patients: a feasibility study. J Refractive Surgery. 2012;28(11):793–799. doi:10.3928/1081597X-20121011-08
22. Badawi AE. Accelerated corneal collagen cross-linking in pediatric keratoconus: one year study. Saudi j Ophthalmol. 2017;31(1):11–18. doi:10.1016/j.sjopt.2017.01.002
23. Kymionis G, Yoo S, Diakonis VF, Kankariya V. Management of pediatric keratoconus - evolving role of corneal collagen cross-linking: an update. Indian J Ophthalmol. 2013;61(8):435–440. doi:10.4103/0301-4738.116070
24. Henriquez MA, Rodriguez AM, Izquierdo L. Accelerated Epi-On Versus Standard Epi-Off Corneal Collagen Cross-Linking for Progressive Keratoconus in Pediatric Patients. Cornea. 2017;36(12):1503–1508. doi:10.1097/ICO.0000000000001366
25. Sarac O, Caglayan M, Uysal BS, Uzel AGT, Tanriverdi B, Cagil N. Accelerated versus standard corneal collagen cross-linking in pediatric keratoconus patients: 24 months follow-up results. Contact Lens Anterior Eye. 2018;41(5):442–447. doi:10.1016/j.clae.2018.06.001
26. Waszczykowska A, Jurowski P. Two-year accelerated corneal cross-linking outcome in patients with progressive keratoconus. Biomed Res Int. 2015;2015:325157. doi:10.1155/2015/325157
27. Tomita M, Mita M, Huseynova T. Accelerated versus conventional corneal collagen crosslinking. J Cataract Refract Surg. 2014;40(6):1013–1020. doi:10.1016/j.jcrs.2013.12.012
28. Shetty R, Pahuja NK, Nuijts RMMA, et al. Current Protocols of Corneal Collagen Cross-Linking: visual, Refractive, and Tomographic Outcomes. Am J Ophthalmol. 2015;160(2):243–249. doi:10.1016/j.ajo.2015.05.019
29. Caporossi A, Mazzotta C, Baiocchi S, Caporossi T, Denaro R, Balestrazzi A. Riboflavin-UVA-induced corneal collagen cross-linking in pediatric patients. Cornea. 2012;31(3):227–231. doi:10.1097/ICO.0b013e31822159f6
30. Greenstein SA, Fry KL, Hersh PS. Corneal topography indices after corneal collagen crosslinking for keratoconus and corneal ectasia: one-year results. J Cataract Refract Surg. 2011;37(7):1282–1290. doi:10.1016/j.jcrs.2011.01.029
31. Madeira C, Vasques A, Beato J, et al. <p>Transepithelial accelerated versus conventional corneal collagen crosslinking in patients with keratoconus: a comparative study. <![CDATA[Clinical Ophthalmology]]>. 2019;13:445–452. doi:10.2147/OPTH.S189183
32. Mrochen M. Current status of accelerated corneal cross-linking. Indian J Ophthalmol. 2013;61(8):428–429. doi:10.4103/0301-4738.116075
33. Ulusoy DM, Goktas E, Duru N, et al. Accelerated corneal crosslinking for treatment of progressive keratoconus in pediatric patients. Eur J Ophthalmol. 2017;27(3):319–325. doi:10.5301/ejo.5000848
34. Wittig-Silva C, Chan E, Islam FMA, et al. A randomized, controlled trial of corneal collagen cross-linking in progressive keratoconus: three-year results. Ophthalmology. 2014;121(4):812–821. doi:10.1016/j.ophtha.2013.10.028
35. Duncan JK, Belin MW, Borgstrom M. Assessing progression of keratoconus: novel tomographic determinants. Eye Vision. 2016;3(1):6. doi:10.1186/s40662-016-0038-6
36. Mahmoud AM, Nunez MX, Blanco C, et al. Expanding the cone location and magnitude index to include corneal thickness and posterior surface information for the detection of keratoconus. Am J Ophthalmol. 2013;156(6):1102–1111.
37. Croxatto JO, Tytiun AE, Argento CJ. Sequential in vivo confocal microscopy study of corneal wound healing after cross-linking in patients with keratoconus. J Refractive Surgery. 2010;26(9):638–645. doi:10.3928/1081597X-20091111-01
38. Tian M, Jian W, Sun L, Shen Y, Zhang X, Zhou X. One-year follow-up of accelerated transepithelial corneal collagen cross-linking for progressive pediatric keratoconus. BMC Ophthalmol. 2018;18(1):75. doi:10.1186/s12886-018-0739-9
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.