Back to Journals » Cancer Management and Research » Volume 7
Long-term survival in advanced melanoma patients using repeated therapies: successive immunomodulation improving the odds?
Authors Coventry B ![]() , Baume D, Lilly C
, Baume D, Lilly C
Received 21 October 2014
Accepted for publication 14 January 2015
Published 29 April 2015 Volume 2015:7 Pages 93—103
DOI https://doi.org/10.2147/CMAR.S76163
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Kenan Onel
Brendon J Coventry, Dominique Baume, Carrie Lilly
Discipline of Surgery, Royal Adelaide Hospital, University of Adelaide, Adelaide, SA, Australia
Background: Patients with advanced metastatic melanoma are often confronted with little prospect of medium- to longer-term survival by any currently available therapeutic means. However, most clinicians are aware of exceptional cases where survival defies the notion of futility. Prolonged survival from immunotherapies, including interleukin-2, vaccines and antibodies to cytotoxic lymphocyte antigen-4, and programmed death-1 receptor inhibitory monoclonal antibody, implies a role for immune system modulation. We aimed to identify cases where exceptional survival from advanced melanoma occurred prior to recent novel therapies to facilitate better understanding of this phenomenon.
Methods: Cases of long-term survival of ≥3 years' duration (from diagnosis of metastatic disease) were identified from the database of one clinician; these cases were treated before the availability of newer immunotherapies, and they were documented and examined. A literature search for reported outcome measures from published studies using older and recent therapies for advanced melanoma was conducted to enable the comparison of data.
Results: Eighteen cases were identified that identified survival of ≥3 years' duration from metastatic disease (12 American Joint Committee on Cancer [AJCC] Stage IV cases; six AJCC III cases) diagnosis. These were assessed and reported to detail the clinical course. Standard clinical prognostication methods predicted high risk of early mortality in those patients. No identifiable differences could be detected between these and other patients with similar patterns of disease. At evaluation, 17 patients (94%) had survived ≥5 years, and eleven patients (61%) had survived ≥10 years (range: 3–15 years). The median survival duration with metastatic disease was 11 years; 15 remained alive and three had died. Published studies of melanoma therapies were tabled for comparison.
Conclusion: The fact that 18 cases of exceptional survival in advanced melanoma were identified is remarkable in itself. Even with recent therapies, the factors for improved survival remain enigmatic; however, one apparent common denominator in most cases was the persistent use of repeated therapies to reduce tumor bulk, induce tumor necrosis, and/or cause immunostimulation. These cases are instructive, suggesting manipulation of an established, endogenous, existing immune response. These observations provide practical evidence that the course for any patient with advanced melanoma at the outset should be considered unpredictable, open to immunomanipulation, and thus not uniformly fatal. The findings were compared and interpreted with reported newer immunotherapeutic approaches.
Keywords: advanced melanoma, clinical responses, immunotherapy, prolonged survival
Background
Remarkable cases of complete regression of metastatic melanoma and other cancers with prolonged survival, with or without therapeutic intervention, are noteworthy events and represent highly instructive natural clinical experiments. The immune system is again being considered the likely contributor to such events following successful results from the recent use of immunomodulatory agents.
Metastatic malignant melanoma represents a highly aggressive form of skin cancer, with an overall 5-year survival of less than 2% and a median survival time of 6–9 months for stage IV disease.1–3 The incidence of melanoma is rising, affecting over 150,000 new patients per year worldwide. This is likely due to both increased levels of exposure to ultraviolet radiation and improved diagnostic awareness and detection procedures.
Although primary melanoma is often curable, the risk of metastasis directly increases with Breslow depth.4 Other poor prognostic factors include ulceration, high mitotic rate, increasing Clark level, increased age, elevated lactate dehydrogenase levels, and lymph node involvement, as these are associated with a higher potential for metastasis.5
Current standard therapy for primary melanoma is wide local excision (WLE) of the skin and subcutaneous tissues around the primary lesion with surgical margins determined by Breslow thickness.6,7 Lymphatic tracing and sentinel node biopsy is recommended for melanomas >1 mm in thickness for staging and therapy because regional draining lymph nodes are typically the first site of metastases.8 The status of the sentinel nodes is the most important prognostic factor in patients with primary melanoma. Patients with regional or local lymphatic spread have a high risk of widespread disseminated disease and poorer survival rates.7 Observed patterns of metastases are, however, highly variable.
While localized disease can be effectively managed with surgery, there is currently no effective treatment for disseminated disease. Management options differ depending on the sites and rate of progression of the disease and usually involve a multidisciplinary approach. Surgical resection of operable metastases has been shown to significantly improve the patient’s survival rate, but is predominantly employed only if one or few metastases are present and resectable.3,9–11
Adjuvant radiotherapy may be employed postoperatively; however, several studies have demonstrated no improvement in survival when used after nodal dissection in stage III patients,12–14 while one showed improved local disease control.15 In advanced disease, radiotherapy plays a larger role in effective symptom palliation, especially for bone metastases.
Standard approved chemotherapy with single-agent dacarbazine, fotemustine, or temozolomide has been used for the treatment of late-stage melanoma; however, overall response rates (ORR) remain uniformly low (5%–20%) and are often short lived.2,3 Complete responses (CRs) from chemotherapy are rare. Isolated limb perfusion or infusion chemotherapy techniques are effective for recurrent disease localized to the arm or the leg and have reported regional CR rates of between 40% and 60%.12,16,17
Recent advances in the development of inhibitory agents, which target key checkpoint molecules within metabolic pathways of melanoma cells, have led to a range of new experimental therapies. These include B-raf and mitogen-activated protein kinase inhibitors, which offer much promise for the more effective treatment of selected B-raf mutation-positive advanced melanoma.17,18 However, despite some impressive initial clinical responses, these seldom translate into CRs or durable long-term survival.
Immunotherapy has also emerged over the last three decades as a potentially viable field of therapy. In particular, interleukin-2 (IL-2), cytotoxic lymphocyte antigen-4 (CTLA-4), and programmed death receptor-1 (PD-1), and programmed death-1 receptor ligand inhibitory monoclonal antibody (PDL-1) therapies, vaccines, and other cytokine-based therapies have been a major area of research.18–20 Notably, IL-2 therapy has stood the test of time, with some 5%–10% of patients achieving CRs and long-term survival.21,22 More recently, studies have demonstrated a 17% CR rate from combined CTLA-4 inhibitor and IL-2 therapy and similar CR rates using a melanoma lysate vaccine therapy.17,20,23
In contrast to the pathway inhibitors, immunotherapeutic strategies produce higher reported rates of CRs and are associated with a higher proportion of long-term survivors.20,23 Importantly, almost irrespective of the therapy type considered, when CRs occur, these often translate into long-term survival beyond 5 years, especially for immunotherapies.
Objectives
The primary objective of this study was to identify and document advanced melanoma cases where longer-term survival of at least 3 years was observed, in one clinician’s experience. A second objective was to evaluate the published literature to date for reported clinical outcomes from advanced melanoma therapies.
Methods
The case records of patients under the care of one clinician (BJC) were carefully reviewed and those with a survival of ≥3 years from the date of diagnosis of metastatic disease were identified. Treatment modalities and event timelines were recorded and investigated for each patient. For the purposes of the study, data collection was ceased in April 2013. The literature was surveyed using PubMed and other databases for published clinical trials of agents that have been successfully used for the systemic treatment of metastatic melanoma from 1984. Search terms included: “metastatic melanoma”; “advanced melanoma”; “systemic therapy”; “complete response”; “CR”; “chemotherapy”; “DTIC”; “dacarbazine”; “temozolomide”; “fotemustine”; “IL-2”; “interleukin-2”; “pathway inhibitors”; “immunotherapy”; “vaccine”; “B-raf”; “Braf”; “CTLA-4”; and “PD-1”. Reported studies that utilized chemotherapy and other therapies for the treatment of advanced or metastatic melanoma were identified and included.
Results
The median age was 55 years at melanoma presentation, with ages ranging from 33 to 83 years. The median duration of survival from the initial diagnosis of primary melanoma was 13.5 years. All individuals were Caucasian. Fourteen were male and three were female. American Joint Committee on cancer (AJCC) staging determined that there were 12 cases with stage IV and six with advanced stage III disease present at the time of initial therapy or observation. At the time of data collection closure, 18 patients were identified who had survived for ≥3 years after the diagnosis of advanced melanoma, ranging from 3 to 15 years in duration. Seventeen patients (94%) had survived 5 years or more and eleven patients (61%) had survived 10 years or more.
The median survival duration with metastatic disease was 11 years. At evaluation, 15 remained alive and three were dead (Table 1).
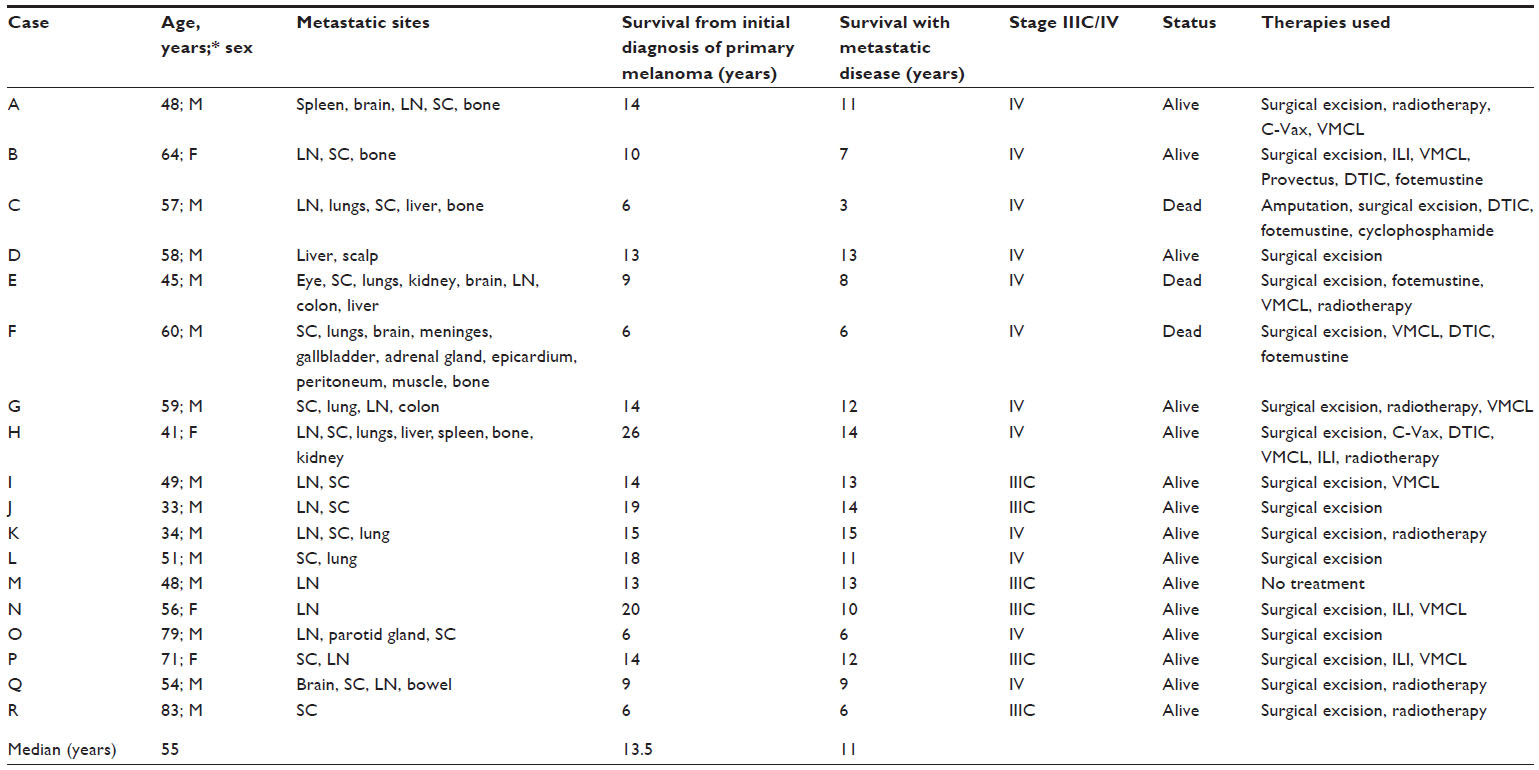 | Table 1 Patient characteristics, metastatic sites, survival times, and therapies used |
Detailed case series
Case A (Status: alive and disease-free; survival: 11 years)
A 48-year-old male presented in 1999 for WLE of a left paraumbilical melanoma, Clark level III, Breslow 0.95 mm. The patient remained disease-free for 2 years, until left groin metastatic melanoma nodal enlargement occurred in late 2001, and a left pelvic and inguinal nodal dissection was performed. The patient commenced a Phase III Canvaxin or Cancer Vax (C-Vax) trial for resected stage III melanoma in 2002; however, in June 2002, a solitary left cerebellar metastasis developed. This was treated with surgical resection and adjuvant whole-brain radiotherapy, and he was changed to the stage IV C-Vax trial protocol. In 2003, a splenectomy for multiple metastases was performed and the patient was then reinduced with C-Vax vaccine. Subsequent to C-Vax trial closure in April 2005, two cerebral nodules developed and were managed with surgical and stereotactic radiosurgical treatment. In 2006, radical right inguinal and pelvic nodal dissection for further metastases was performed. Later in 2006, WLE of a left buttock metastasis was performed. In 2007, the patient underwent palliative radiotherapy for a right sixth rib metastatic deposit. A left buttock recurrence occurred in January 2008 and vaccinia melanoma cell lysate (VMCL) vaccine trial therapy was commenced.
Case B (Status: alive and disease-free; survival: 7 years)
A 64-year-old female presented in early 2003 for WLE of melanoma of her left foot, Clark level IV, Breslow 2.2 mm, and subsequent radical left inguinal dissection. She remained disease-free until February 2006, when large pigmented nodules over the anterior aspect of her lower left leg were detected. Isolated limb infusion chemotherapy was performed in April 2006, with good initial control, but she experienced four further episodes of local cutaneous/subcutaneous recurrences over 1.5 years, treated surgically. In March 2008, multiple nonresectable nodules developed over the thigh and leg, and VMCL vaccine trial therapy was commenced, which continued for 8 months. Subcutaneous metastases over her left medial thigh and left lower leg decreased notably in size. In December 2008, regrowth occurred, and a Rose Bengal (PV-10; Provectus Pharmaceuticals, Inc., Knoxville, TN, USA) trial therapy was commenced for 5 months with some initial effect, but deposits eventually grew and further nodules appeared. Further surgical resection of deep soft tissue limb metastases was performed in May 2009, and again in September. VMCL therapy was recommenced in September 2009, with some clinical effect. In November 2009, left inguinal, external iliac, and common iliac lymphadenopathy developed. In January 2010, positron emission tomography (PET) imaging revealed progression of disease with abnormal fluorodeoxyglucose uptake in several retroperitoneal lymph nodes and further local subcutaneous metastases in her left leg. She was commenced on a “timed” schedule of VMCL vaccine therapy synchronized with immune fluctuations identified by monitoring high-sensitivity C-reactive protein levels, and similarly synchronized with dacarbazine (DTIC) chemotherapy in February 2010. Some stability of disease resulted (with regression of an enlarged high left inguinal lymph node) until April 2010, when disease progression was evident. In May 2010, “palliative” left radical high pelvic retroperitoneal lymph node dissection was performed. The combined timed vaccine and chemotherapy regimen was recommenced, until DTIC was ceased in December 2010 due to bone marrow suppression and low blood counts. All metastases regressed completely and repeated regular computed tomography (CT) scans have revealed no evidence of metastatic disease since.
Case C (Status: died in April 2011; survival: 3 years)
A 57-year-old male presented in May 2005 for amputation of his right middle finger for advanced subungual acral lentiginous melanoma, Clark level IV, Breslow depth 2.5 mm. In January 2008, he was found to have bilateral pulmonary metastases and he was commenced on six cycles of DTIC, which successfully reduced the size of these tumors by November 2008. In June 2009, CT scans showed progression of a right hilar mass and the patient was commenced on fotemustine, which was not effective. In February 2010, he began a trial of timed administration of the VMCL vaccine with oral cyclophosphamide (2×50 mg doses per day intermittently) with immune monitoring based on high-sensitivity C-reactive protein levels. Stability of disease was observed for 2 months. In April 2010, a left ischiorectal fossa melanoma metastasis was surgically resected. In August 2010, a CT scan revealed further pulmonary, hepatic, and bony metastases. Radiotherapy was given to the right hilar metastatic deposit and mediastinum, with some success. In September 2010, he developed a metastasis to his left buttock, which was completely excised, and in October he went on to develop multiple subcutaneous metastases to his scalp, neck, and jaw. He recommenced palliative treatment with DTIC chemotherapy in November, but failed to respond. In January 2011, he was noted to have an increasingly severe cough and had developed subsequent pneumonia with pleural effusions. The pleural effusions were drained but he recovered incompletely and died.
Case D (Status: alive and disease-free; survival: 13 years)
A 58-year-old male presented in 2000 with malignant melanoma in the liver, with no identified primary tumor. This was completely resected, and he went on to develop metastases to his scalp in 2001, which were also completely excised. Chemotherapy was declined. He has remained well since. No other treatment apart from self-termed “positive thinking” was instituted.
Case E (Status: died in March 2010; survival: 8 years)
A 45-year-old male presented in late 2000 for WLE of a melanoma of his right ear, Clark level III, and Breslow depth 0.45 mm. In 2002, he re-presented for excision of a metastasis to his right eye and adjuvant chemotherapy. In early 2007, he developed a subcutaneous metastasis to his left buttock, as well as pulmonary and renal secondaries. He commenced VMCL vaccine therapy, which was initially effective, but he went on to develop a metastasis to a left groin lymph node later that year, for which he received radiotherapy. In 2009, he underwent several cycles of fotemustine chemotherapy with some decrease in the size of his pulmonary metastases. However, in early 2010, the patient deteriorated quickly, developing multiple brain metastases that were not responsive to whole-brain radiotherapy. In addition, he required sigmoid colon resection and stoma formation after mesenteric metastases caused colonic obstruction. Imaging in February 2010 revealed progression with pulmonary, hepatic, gastrointestinal, and lymphatic metastases.
Case F (Status: died in October 2009; survival: 6 years)
A 60-year-old male presented in 2003 with two primary melanomas: left flank Clark level IV, Breslow depth 2.91 mm; and lower back Clark level IV, Breslow depth 1.01 mm. Metastatic disease was diagnosed on sentinel node biopsy in 2003, with radical axillary dissection, then multiple subcutaneous in-transit metastases to his anterior chest wall occurred over 5 years, all of which were completely excised. Pulmonary/pleural metastases were noted in March 2008, prompting the commencement of the VMCL vaccine in April 2008. A further subcutaneous metastasis to his left thigh was noted in July, but it was not excised. He commenced concurrent DTIC chemotherapy in January 2009. In August 2009, a cerebellar metastasis was excised, and radiotherapy was commenced for leptomeningeal seeding. Later CT scans revealed disseminated disease of the lungs, gallbladder, left adrenal gland, peritoneum, epicardium, muscle, bone, and spine. The patient recommenced the VMCL vaccine trial and chemotherapy with fotemustine with some initial stabilization of disease, but he died later that year.
Case G (Status: alive and disease-free; survival: 12 years)
A 59-year-old male presented in 1999 for WLE of a primary Clark IV, Breslow 4.5 mm melanoma of his central back. In 2001, recurrences in the right neck and right lung were surgically excised and radiotherapy was delivered to those areas. In 2005, further metastases to the left buttock and back were fully excised and targeted radiotherapy was delivered to the buttock. Further to this, resection of a malignant right retrocrural mass encircling the esophagus was performed, but residual melanoma was documented on the pathology report. In 2006, the patient underwent a sigmoid colectomy for metastatic bowel deposits, and later that same year, underwent resection of cutaneous metastasis of the scalp and a radical right axillary dissection. In November of 2006, the patient commenced VMCL vaccine trial therapy, and he has remained disease-free since.
Case H (Status: alive and disease-free; survival: 14 years)
A 41-year-old female presented in 1987 for excision of what was reported to be a benign Spitz nevus of her left calf. In 1999, excision of a nodule adjacent to the scar revealed melanoma. A WLE and sentinel node dissection was then performed. Review of the previous pathology revealed the initial lesion to be a malignant Spitzoid melanoma. Over the following 2 years, the patient required multiple excisions for in-transit recurrences near the original site, and in August of 2000, she required a radical left inguinal and pelvic lymph node dissection and was commenced on the C-Vax vaccine from October 2000 to February 2001, when further local subcutaneous recurrences occurred and were excised. She was commenced on VMCL vaccine in March 2001. CT scans in early 2001 showed multiple pulmonary deposits, and in November 2001, hepatic metastases. In late 2002, CT scans demonstrated disseminated disease involving the mediastinum, lungs, liver, and spleen. In September 2002, DTIC chemotherapy was commenced. Further CT scans in April 2003 demonstrated a marked reduction in the size of her pulmonary nodules and no evidence of metastatic disease elsewhere. The patient remained well until 2006, when she was diagnosed with a deep, lobulated, large, soft tissue calf metastasis involving the left tibia for which she underwent isolated limb infusion chemotherapy with melphalan and actinomycin-C, and radiotherapy. The mass stabilized then gradually regressed, and medullary reamings from orthopedic stabilization for a pathological fracture revealed no malignancy. In August 2007, right sacroiliac joint metastases were treated with radiotherapy, and she recommenced the VMCL vaccine in February 2008, after a PET scan showed persistent bony metastases. CT and PET imaging demonstrated a renal metastasis in June 2008. The VMCL vaccine was ceased in September 2008, as the renal metastasis was regressing. The initial partial responses developed into a CR by late 2009. CT scans to date have shown no metastatic disease.
Case I (Status: alive and disease-free; survival: 13 years)
A 49-year-old male presented in 1999 for WLE of a primary melanoma of his back, Clark level V, Breslow depth 10 mm, and left axillary clearance for metastases. Over the next year, the patient required several further excisions for multiple subcutaneous and chest wall metastases of his back, left axilla, and chest, and subsequently underwent radiotherapy to his left axilla in late 2000. Further multiple subcutaneous and chest wall metastases developed. The patient commenced VMCL vaccine in November of 2000 and demonstrated an excellent clinical response within three doses, with resolution of all subcutaneous metastases within 6 weeks.
Case J (Status: alive and disease-free; survival: 14 years)
A 33-year-old Caucasian male initially presented in 1994 for WLE of a Clark level III, Breslow thickness 0.9 mm melanoma of his back. In early 1999, secondary deposits developed in the lymph nodes of the right axilla, for which right radical axillary clearance was performed. Further deep subcutaneous in-transit nodular recurrence at the edge of the right axillary lymph node basin required further surgical resection several months later. No further therapy was given. He has remained disease-free on CT scanning.
Case K (Status: alive and disease-free; survival: 15 years)
A 34-year-old Caucasian male presented with an amelanotic melanoma of his scalp, Breslow thickness 7 mm, in 1998, and underwent WLE and in-continuity modified radical left neck dissection for an overt 3 cm metastatic left midcervical lymph node mass. Pathology showed three of 12 lymph nodes to be involved with the melanoma with extranodal spread, and the patient subsequently underwent adjuvant local radiotherapy to the left neck. He remained well until December of 2006, when a CT scan revealed a secondary metastasis to his left lung, which was fully resected in 2007. He has remained disease-free on CT scanning.
Case L (Status: alive and disease-free; survival: 11 years)
A 51-year-old Caucasian male presented in 1995 for wide excision of a Clark level IV, 1.3 mm nodular melanoma of his back. He re-presented in April 2002 for resection of a further subcutaneous deposit of his lower back and underwent a left thoracotomy in July 2002 for resection of a pulmonary metastasis. In 2005, further CT scans revealed a new lesion in the left lower lobe of the lung, which was completely excised. He has since remained disease-free to clinical and CT follow-up.
Case M (Status: alive and disease-free; survival: 13 years)
A 48-year-old Caucasian male presented in 2000 with a 4 cm diameter right axillary lump present for 7 months with no primary melanoma site identified. A fine-needle biopsy confirmed metastatic melanoma and he was booked for a right radical axillary lymph node dissection, but this was deferred so the patient could attend the Sydney Olympic Games. On review 6 weeks later, the mass had markedly reduced in size. The mass continued to decrease in size without treatment, and a CT scan at that time showed no evidence of disease. On recent repeat CT scanning in 2010, no metastatic disease was evident, and clinically he continues to be disease-free.
Case N (Status: alive and disease-free; survival: 10 years)
A 56-year-old Caucasian female presented in early 1993 for WLE of a malignant melanoma of the left leg, Clark level II, Breslow thickness 0.4 mm. She re-presented 10 years later with locally recurrent nodules over the left leg that were excised, some incompletely due to difficulty of location. She developed further local metastases over her limb within the next 2 years. She subsequently underwent isolated limb infusion chemotherapy in April 2004, but developed further local metastases in July, which were excised. In August 2004, the patient commenced the VMCL melanoma vaccine, and in November underwent a second isolated limb infusion therapy procedure due to further local recurrences. Several further recurrences were excised in 2005, and in December 2005, she underwent a third isolated limb infusion chemotherapy, which led to significant ulceration of her skin. In July 2006, CT scans showed lymphadenopathy in the left groin, and fine-needle biopsy confirmed metastatic melanoma. Radical left pelvic and inguinal lymph node dissections were performed in August 2006. She has been maintained on VMCL therapy since, and has developed a complete clinical response with no evidence of disease present clinically or on serial CT scans to date.
Case O (Status: alive and disease-free; survival: 6 years)
A 79-year-old man presented in early May 2007 for WLE of a Clark level IV, Breslow thickness 5.1 mm amelanotic melanoma from his right forehead. Sentinel node biopsy demonstrated metastatic disease, and a subsequent right modified radical neck dissection and right parotidectomy were performed. He re-presented 1 year later with a single metastasis to his scalp, which was completely excised, and then again with further metastatic deposits in the left parotid gland, for which a left parotidectomy and left modified radical neck dissection were performed. In early 2009, the patient re-presented with an enlarged metastatic right axillary lymph node, for which he underwent right radical axillary dissection. In January 2011, WLE of a second primary in situ melanoma of his left cheek was performed. He has remained disease-free on clinical and CT scan criteria since.
Case P (Status: alive and disease-free; survival: 12 years)
A 71-year-old female presented in March 1999 for WLE of a Clark level IV, Breslow 1.53 mm melanoma of the left leg. She re-presented for WLE of in-transit recurrence in late 2000 and again in November 2001 with multiple local recurrences of the left leg, which were surgically excised. Further recurrences were treated using isolated limb infusion chemotherapy with a CR. Local recurrences again occurred throughout 2002 and she commenced the VMCL melanoma vaccine in March 2003. In April 2003, she developed left groin lymph node metastases and underwent radical dissection of the left groin and pelvis, followed by continuous VMCL vaccine therapy. She has remained disease-free by clinical and CT scan criteria to date.
Case Q (Status: alive and disease-free; survival: 9 years)
A 54-year-old Caucasian male initially presented with neurological symptoms in December of 2004, and underwent resection of hemorrhagic right frontal cerebral melanoma metastasis of unknown primary site. Adjuvant whole-brain radiotherapy was given. Shortly thereafter, he presented for resection of a left lower back subcutaneous metastatic deposit. He remained disease-free until October 2005, when he was noted to have a low hemoglobin level, and upper and lower endoscopies revealed no cause for this. A small bowel capsule camera study demonstrated a nonobstructing bleeding mass in the lower small intestine. He was also noted to have a mass in the right inguinal region, for which he underwent a right radical inguinal and pelvic lymph node dissection in December 2005. In February 2006, a small bowel resection and primary anastomosis removed the two previously noted metastatic melanoma deposits. He has had no further recurrence of melanoma.
Case R (Status: alive and disease-free; survival: 6 years)
An 83-year-old male presented in May 2007 with a Clark level V, Breslow 3.95 mm melanoma of the scalp, with perineural invasion. Multiple extensive satellite lesions developed covering half of his scalp, and they were treated by extensive wide excision and grafting, with adjuvant radiotherapy. In February 2009, the patient re-presented with a second primary Clark level IV, Breslow 0.85 mm thick metastasis to his right thigh, which was surgically excised.
For the purposes of comparison, the reported relevant clinical outcome measures for a range of different published treatment modalities for metastatic melanoma are shown in Table 2.
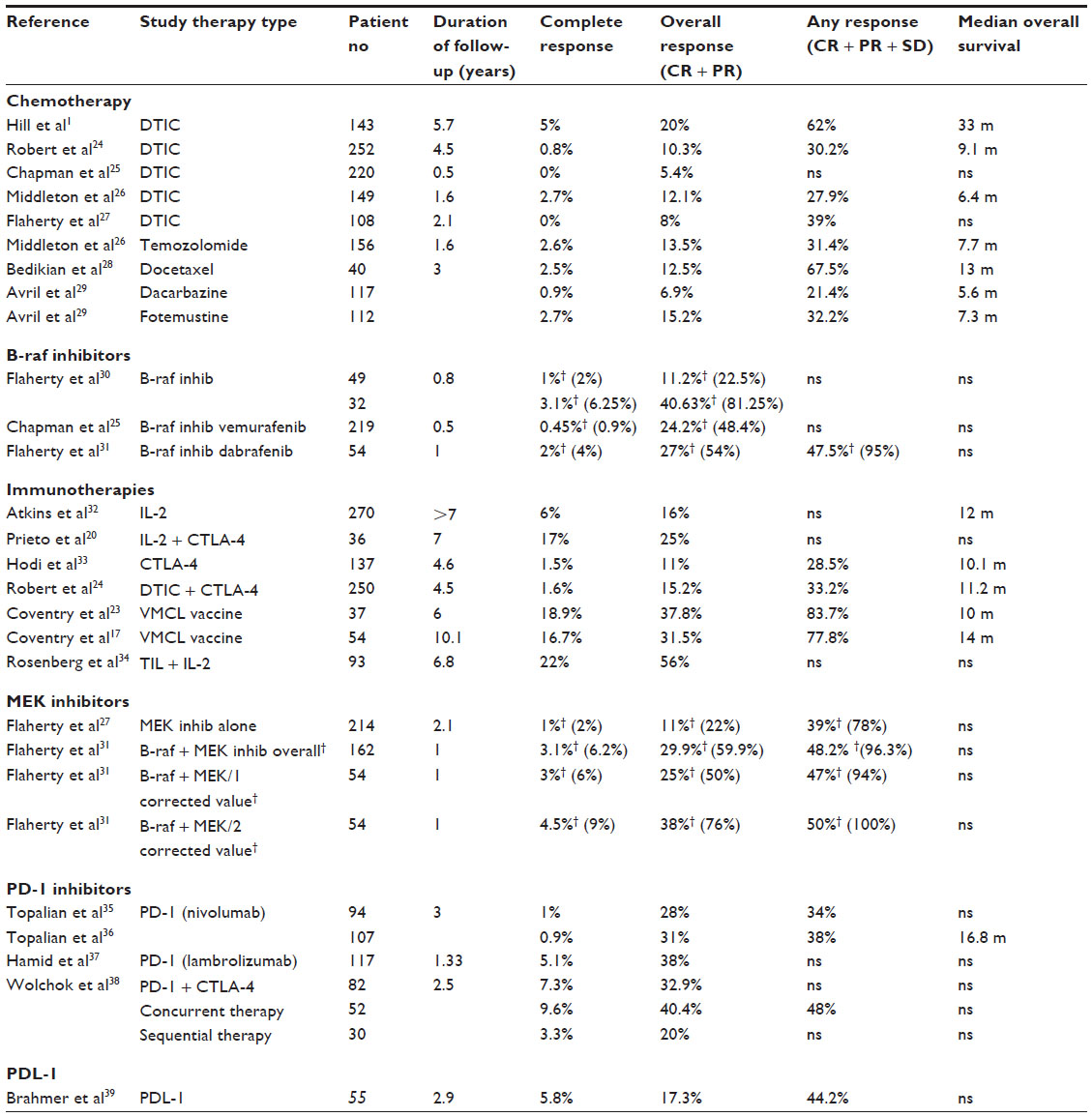 | Table 2 Response rates from previous studies using different modalities of treatment for advanced melanoma |
Discussion
The finding that 18 patients with metastatic melanoma had remained alive for ≥3 years’ duration, and that 17 had survived ≥5 years, was both unusual and notable. Despite considerable research into multiple areas of treatment, the overall usual prognosis of stage IV melanoma still remains poor. Median survival time ranges from 6 to 9 months, with a 5-year survival rate of <2%.1–3 Although there have been recent encouraging therapeutic approaches using pathway and checkpoint blockade approaches and some indication of prolongation of survival, in many centers, the typical treatment options for disseminated disease still remain seriously limited in their ability to induce long-term survival.24–41 Surgical resection can be very effective in selected cases if the metastases are solitary or few in number, or if they are sequential in their clinical appearance,9–11 but this is unpredictable with recurrence being commonplace.
Until recently, DTIC has often been considered the first-line treatment for patients with disseminated disease, conferring response rates of 10%–20% and producing initial complete remission in 0%–5% of patients.14,24 Despite this, the 5-year survival rate for patients using this therapy remains under 2%, and three separate randomized controlled trials conducted by the European Organization for Research and Treatment of Cancer, the World Health Organization, and the Central Oncology Group demonstrated no significant difference in survival after treatment with DTIC compared with placebo.6
Combination chemotherapy has offered little over single-agent chemotherapy for metastatic melanoma. Studies of nitrosourea- and DTIC-based chemotherapy, taxane-based chemotherapy, and cisplatin-based chemotherapy have found no convincing evidence to support improved efficacy.6
Immunotherapy has been an emerging area of research over the past two decades with mixed results.40 Several studies have examined the value of combined chemotherapy and immunotherapy, again with mixed results. Studies have looked at the role of interferon-α in combination with DTIC, cisplatin, vinca alkaloids, and nitrosoureas and found that the results were comparable to single-agent chemotherapy.6 Similarly, treatment with IL-2 and DTIC has not been shown to be superior to single-agent therapy. In contrast, Phase II trials directed toward the combination of cisplatin and high-dose IL-2 or low-dose IL-2 with the addition of interferon-α showed initial promising results with response rates of 10%–20% and an overall 2-year survival rate of 10% in selected patients.6 Unfortunately, due to the long inpatient hospital stays, high expense, and substantial toxicity, further Phase III investigations were considered not feasible.
Historically, meta-analyses focusing on the use of chemotherapy and immunotherapy in stage IV melanoma have shown their role to be largely palliative rather than curative. However, the concept of vaccines to directly target melanoma cells is particularly attractive. Several vaccine therapies have been investigated, with mixed results. One such example is the polyvalent allogenic whole-cell vaccine, CancerVax. Though early Phase I and II trials were encouraging, Phase III trials of the vaccine in both stage III and IV melanoma patients were discontinued due to negative findings.40
Similarly, neither of the two lysate vaccines that entered Phase III clinical trials – the viral melanoma oncolysate vaccine and the aforementioned VMCL vaccine – have shown statistically significant survival benefit in surgically resected high-risk stage II/III melanoma patients19 although, remarkably, VMCL has shown CR rates of 17% with a 15% 5-year survival rate for advanced stage III/IV metastatic melanoma.23,42
Recent reports using B-raf inhibitors (vemurafenib, dabrafenib) and CTLA-4 blocking antibody therapies (ipilimumab) had promised new hope for improving survival with stage IV melanoma. However, although overall response rates were 69% and 7%, the CR rates have remained very low at 0.9% and 0.5%, respectively.26,27,41 It should be noted that, B-raf V600E expression has been found in 30%–60% of melanomas and that some 69% of these showed a response to B-raf inhibitory antibody therapy, then the true response rate for statistically valid comparison with the unselected melanoma patient population was about 31% (ie, 69% of 45%) overall.26,27
Despite the numerous discouraging results from studies of many therapies for advanced melanoma, some patients defy the usual predicted course of the disease. Those cases cited and detailed in this study represent extraordinary and informative cases. Close evaluation of these patients indicated that their pattern of disease was not uniform. Many of the patients had disease that was indistinguishable from other patients who subsequently encountered progressive disease and died. The main distinguishing feature for many of the patients cited here seemed to be the utilization of a range of therapies, often in sequence. This persistence and repetition in the clinical application of therapies appears to be a vitally important factor for determining patient survival.42–44 The wide disparity between the multitude of variables in those cases reported here was far too divergent to permit useful correlative analysis. That wide divergence further adds to our contention that these cases most likely represent in vivo immunomanipulation of a pre-existing endogenous immune response against the cancer in the patient, often by multiple means, to create successful outcomes.44
The investigation of multiple other pathways, such as neuroendocrine, glucocorticoid, melanogenic, and immunomodulatory influences, may offer associated approaches for overcoming the “resistance” mechanisms that appear to be evident with current therapies.45
The interesting findings emerging from recent immunotherapeutic agents and strategies appear to be strongly indicative that modulation of a pre-existing, underlying, endogenous immune response is naturally occurring within the patient against their cancer. It is therefore highly likely that both the findings arising from the repeated therapies reported in our present series, and those being reported using current repetitious immunotherapeutic and pathway blockade therapy approaches, appear to cause progressive immunomodulation, perhaps by effectively “synchronising”, “directing”, or “re-focussing” the patient’s in vivo immune response against their cancer.42,43 Better serial blood biomarker analysis and improvement of the accuracy of the timing of therapeutic intervention(s) both appear to be very promising approaches toward obtaining better “synchronization” of therapies with pre-existing in vivo immune responses to thereby improve clinical efficacy.21,22,42–44
Conclusion
Some patients show long-term survival despite advanced melanoma having the reputation of being associated with a particularly dismal prognosis. Clinical course data for 18 cases demonstrates that some patients do defy the odds, in some cases even without therapy, to mount an effective response against their cancer. A combination of selective and combined therapies tailored to the individual patient appears to be capable of modulating the immune response and disease level in a favorable direction for a better outcome. These remarkable cases provide clinical insight into the mechanisms that underpin the better clinical control of metastatic melanoma, and perhaps cancer more generally. Even after failed treatment attempts, long-term patient survival may still be evidenced in a remarkable number of cases in clinical practice. Recent data from the treatment of patients using “pure” immunotherapeutic approaches, such as IL-2, CTLA-4/PD-1 antibody therapies, and repetitive vaccination, would reinforce the notion that restimulation of the immune response in the patient can be remarkably effective in inducing long-term survival.
Although the outlook on metastatic melanoma may seem dismal, cases such as those reported should provide patients with tangible evidence and some hope that their fight against advanced melanoma is not uniformly, nor irrevocably, futile. Physicians, while being realistic, should encourage patients not to become disheartened by failed treatment attempts. Some individuals, even after multiple failed treatment attempts, do ultimately defy their metastatic disease to outlive their initial predicted prognosis, as our findings demonstrate. Continued persistent therapies appear remarkably pivotal. Moreover, newer immunotherapies and new approaches for applying these clinically offer the very tangible prospects of improving the manipulation of endogenous immune responses in patients with advanced cancer.42–44
Disclosure
The authors report no conflicts of interest in this work.
References
Hill GL 2nd, Krementz ET, Hill HZ. Dimethyl triazeno imidazole carboxamide and combination therapy for melanoma. IV. Late results after complete response to chemotherapy (Central Oncology Group protocols 7130, 7131, and 7131A). Cancer. 1984;53(6):1299–1305. | |
Bonnet-Duquennoy M, Papon J, Mishellany F, et al. Promising pre-clinical validation of targeted radionuclide therapy using a [131I] labelled iodoquinoxaline derivative for an effective melanoma treatment. J Cancer Sci Ther. 2009;1(1):1–7. | |
Brand CU, Ellwanger U, Stroebel W, et al. Prolonged survival of 2 years or longer for patients with disseminated melanoma. An analysis of related prognostic factors. Cancer. 1997;79(12):2345–2353. | |
Lanitis S, Papaioannou N, Sgourakis G, Seitz A, Zacharakis E, Karaliotas C. Prolonged survival after the surgical management of a solitary malignant melanoma lesion within the pancreas: a case report of curative resection. J Gastrointestin Liver Dis. 2010;19(4):453–455. | |
Homsi J, Kashani-Sabet M, Messina JL, Daud A. Cutaneous melanoma: prognostic factors. Cancer Control. 2005;12(4):223–229. | |
Balch C, Houghton A, Sober A, Soong S. Cutaneous Melanoma. 4th ed. St Louis, MO: Quality Medical Publishing, Inc.; 2013. | |
Algazi AP, Soon CW, Daud AI. Treatment of cutaneous melanoma: current approaches and future prospects. Cancer Manag Res. 2010;2:197–211. | |
Morton DL, Thompson JF, Cochran AJ, et al; MSLT Group. Final trial report of sentinel-node biopsy versus nodal observation in melanoma. N Engl J Med. 2014;370(7):599–609. | |
Wasif N, Bagaria SP, Ray P, Morton DL. Does metastasectomy improve survival in patients with Stage IV melanoma? A cancer registry analysis of outcomes. J Surg Oncol. 2011;104(2):111–115. | |
Howard JH, Thompson JF, Mozzillo N, et al. Metastasectomy for distant metastatic melanoma: analysis of data from the first Multicenter Selective Lymphadenectomy Trial (MSLT-I). Ann Surg Oncol. 2012; 19(8):2547–2555. | |
Ollila DW, Gleisner AL, Hsueh EC. Rationale for complete metastasectomy in patients with stage IV metastatic melanoma. J Surg Oncol. 2011;104(4):420–424. | |
Balch CM, Morton DL, Gershenwald JE, et al. Sentinel node biopsy and standard of care for melanoma. J Am Acad Dermatol. 2009;60(5):872–875. | |
Moncrieff MD, Martin R, O’Brien CJ, et al. Adjuvant postoperative radiotherapy to the cervical lymph nodes in cutaneous melanoma: is there any benefit for high-risk patients? Ann Surg Oncol. 2008;15(11):3022–3027. | |
Atkins MB. The role of cytotoxic chemotherapeutic agents either alone or in combination with biological response modifiers. In: Kirkwood JK, editor. Molecular Diagnosis, Prevention and Therapy of Melanoma. New York, NY: Marcel Dekker; 1997:219–225. | |
Burmeister BH, Henderson MA, Ainslie J, et al. Adjuvant radiotherapy versus observation alone for patients at risk of lymph-node field relapse after therapeutic lymphadenectomy for melanoma: a randomised trial. Lancet Oncol. 2012;13(6):589–597. | |
Giles MH, Coventry BJ. Isolated limb infusion chemotherapy for melanoma: an overview of early experience at the Adelaide Melanoma Unit. Cancer Manag Res. 2013;5:243–249. | |
Coventry BJ, Kroon HM, Giles MH, et al. Australian multi-center experience outside of the Sydney Melanoma Unit of isolated limb infusion chemotherapy for melanoma. J Surg Oncol. 2014;109(8):780–785. | |
Menzies AM, Long GV. New combinations and immunotherapies for melanoma: latest evidence and clinical utility. Ther Adv Med Oncol. 2013;5(5):278–285. | |
Safa M, Foon K. Cancer vaccines. In: Oldham RK, editor. Principles of Cancer Biotherapy. 4th ed. Dordrecht, the Netherlands: Kluwer Academic Publishers; 2013. | |
Prieto PA, Yang JC, Sherry RM, et al. CTLA-4 blockade with ipilimumab: long-term follow-up of 177 patients with metastatic melanoma. Clin Cancer Res. 2012;18(7):2039–2047. | |
Coventry BJ, Ashdown ML. The 20th anniversary of interleukin-2 therapy: bimodal role explaining longstanding random induction of complete clinical responses. Cancer Manag Res. 2012;4:215–221. | |
Dutcher JP, Wiernik PH. Deconstructing and reinventing the IL-2 paradigm: can alternate dosing schedules enhance tumor effect. Kidney Cancer Journal. 2013;11(1):22–28. | |
Coventry B, Hersey P, Halligan AM, Michele A. Immuno-chemotherapy using repeated vaccine treatment can produce successful clinical responses in advanced metastatic melanoma. J Cancer Ther. 2010;1(4):205–213. | |
Robert C, Thomas L, Bondarenko I, et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N Engl J Med. 2011;364(26):2517–2526. | |
Chapman PB, Hauschild A, Robert C, et al; BRIM-3 Study Group. Improved survival with vemurafenib in melanoma with BRAF V600E mutation. N Engl J Med. 2011;364(26):2507–2516. | |
Middleton MR, Grob JJ, Aaronson N, et al. Randomized phase III study of temozolomide versus dacarbazine in the treatment of patients with advanced metastatic malignant melanoma. J Clin Oncol. 2000;18(1):158–166. | |
Flaherty KT, Robert C, Hersey P, et al; METRIC Study Group. Improved survival with MEK inhibition in BRAF-mutated melanoma. N Engl J Med. 2012;367(2):107–114. | |
Bedikian AY, Weiss GR, Legha SS, et al. Phase II trial of docetaxel in patients with advanced cutaneous malignant melanoma previously untreated with chemotherapy. J Clin Oncol. 1995;13(12):2895–2899. | |
Avril MF, Aamdal S, Grob JJ, et al. Fotemustine compared with dacarbazine in patients with disseminated malignant melanoma: a phase III study. J Clin Oncol. 2004;22(6):1118–1125. | |
Flaherty KT, Puzanov I, Kim KB, et al. Inhibition of mutated, activated BRAF in metastatic melanoma. N Engl J Med. 2010;363(9):809–819. | |
Flaherty KT, Infante JR, Daud A, et al. Combined BRAF and MEK inhibition in melanoma with BRAF V600 mutations. N Engl J Med. 2012;367(18):1694–1703. | |
Atkins MB, Kunkel L, Sznol M, Rosenberg SA. High-dose recombinant interleukin-2 therapy in patients with metastatic melanoma: long-term survival update. Cancer J Sci Am. 2000;6 Suppl 1:S11–S14. | |
Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363(8):711–723. | |
Rosenberg SA, Yang JC, Sherry RM, et al. Durable complete responses in heavily pretreated patients with metastatic melanoma using T-cell transfer immunotherapy. Clin Cancer Res. 2011;17(13):4550–4557. | |
Topalian SL, Hodi FS, Brahmer JR, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med. 2012;366(26):2443–2454. | |
Topalian SL, Sznol M, McDermott DF, et al. Survival, durable tumor remission, and long-term safety in patients with advanced melanoma receiving nivolumab. J Clin Oncol. 2014;32(10):1020–1030. | |
Hamid O, Robert C, Daud A, et al. Safety and tumor responses with lambrolizumab (anti-PD-1) in melanoma. N Engl J Med. 2013;369(2):134–144. | |
Wolchok JD, Kluger H, Callahan MK, et al. Nivolumab plus ipilimumab in advanced melanoma. N Engl J Med. 2013;369(2):122–133. | |
Brahmer JR, Tykodi SS, Chow LQ, et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N Engl J Med. 2012;366(26):2455–2465. | |
Finke LH, Wentworth K, Blumenstein B, Rudolph NS, Levitsky H, Hoos A. Lessons from randomized phase III studies with active cancer immunotherapies – outcomes from the 2006 meeting of the Cancer Vaccine Consortium (CVC). Vaccine. 2007;25 Suppl 2:B97–B109. | |
Ernstoff MS. Been there, not done that – melanoma in the age of molecular therapy. N Engl J Med. 2011;364(26):2547–2548. | |
Coventry BJ, Lilly CA, Hersey P, Michele A, Bright RJ. Prolonged repeated vaccine immune-chemotherapy induces long-term clinical responses and survival for advanced metastatic melanoma. J Immunother Cancer. 2014;2:9. | |
Ashdown M, Coventry B. Window of opportunity [cover story]. Australasian Science. Jun 2014. | |
Coventry BJ, Ashdown ML. Complete clinical responses to cancer therapy caused by multiple divergent approaches: a repeating theme lost in translation. Cancer Manag Res. 2012;4:137–149. | |
Slominski AT, Carlson JA. Melanoma resistance: a bright future for academicians and a challenge for patient advocates. Mayo Clin Proc. 2014;89(4):429–433. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.