Back to Journals » Journal of Blood Medicine » Volume 16
Long-Term Survival Following Cladribine Containing Pretransplant Regimen for Autologous Hematopoietic Stem Cell Transplantation in Disseminated Interdigitating Dendritic Cell Sarcoma: A Case Report and Literature Review
Authors Zhou P ![]() , Nie L, Ma R, Wang X, Wu G, Zhu Z
, Nie L, Ma R, Wang X, Wu G, Zhu Z ![]() , Yuan X
, Yuan X
Received 23 January 2025
Accepted for publication 15 April 2025
Published 1 May 2025 Volume 2025:16 Pages 197—203
DOI https://doi.org/10.2147/JBM.S515776
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Pan Zhou,1 Lu Nie,1 Rongjun Ma,1 Xiaoyan Wang,2 Guangyin Wu,3 Zunmin Zhu,1 Xiaoli Yuan1
1Department of Hematology, Henan Provincial People’s Hospital, People’s Hospital of Zhengzhou University, Zhengzhou, 450003, People’s Republic of China; 2Department of Pathology, Henan Provincial People’s Hospital, People’s Hospital of Zhengzhou University, Zhengzhou, 450003, People’s Republic of China; 3Department of Radiotherapy, Henan Provincial People’s Hospital, People’s Hospital of Zhengzhou University, Zhengzhou, 450003, People’s Republic of China
Correspondence: Xiaoli Yuan, Email [email protected] Zunmin Zhu, Email [email protected]
Abstract: Interdigitating dendritic cell sarcoma (IDCS) is an exceedingly rare hematological neoplasm arising from dendritic cells that presents significant diagnostic and therapeutic challenges, particularly in cases of disseminated disease. Here, a 33-year-old woman presented with discomfort of the left pharynx accompanied by nasopharyngeal and cervical mass for 3 months. The histopathology confirmed the diagnosis of IDCS as the neoplastic cells were spindle or ovoid in shape, forming fascicles or whorls, and were positive for S-100, vimentin and CD163 but negative for CD21, CD23, CD35 and CD1a. The patient underwent autologous hematopoietic stem cell transplantation (auto-HSCT) after achieving partial remission (PR) from six courses of chemotherapy based on the ABVD regimen and one cycle of radiotherapy. Encouragingly, the mass disappeared after cladribine containing regimen pretreated auto-HSCT and the patient has been in complete remission (CR) state for over 5 years. Therefore, the long survival of this patient might suggest that ABVD regimen with a sequential cladribine-containing preparative regimen prior to auto-HSCT may improve the prognosis of disseminated IDCS. However, this represents only a single-case experience, and further studies with larger sample sizes are required for validation.
Keywords: disseminated interdigitating dendritic cell sarcoma, autologous hematopoietic stem cell transplantation, ABVD regimen, cladribine, survival
Introduction
Interdigitating dendritic cell sarcoma (IDCS) is an exceedingly rare and highly invasive hematopoietic neoplasm that mainly originates from interdigitating dendritic cells (IDCs). To date, few cases of IDCS have been reported, and knowledge of this disease is limited.1,2 Due to the rarity of IDCS, there is no consensus on a standard treatment strategy and current treatments are disappointing. Usually, surgical resection or radiotherapy has a role in the treatment for localized IDCS, whereas chemotherapy is preferred in disseminated IDCS.3 In this study, we successfully treated a patient who was diagnosed with disseminated IDCS without recurrence for over 5 years using the ABVD chemotherapy regimen in combination with cladribine containing regimen pretreated autologous hematopoietic stem cell transplantation (auto-HSCT) and report as follows.
Case Presentation
Clinical History
A 33-year-old pregnant woman presented to the Otolaryngology Department of our hospital with a 3-month history of left pharynx discomfort accompanied by nasopharyngeal and cervical mass. Physical examination revealed lychee-like neoplasms in bilateral middle nasal passages, and a palpable mass of approximately 4 cm × 5 cm in the left neck, which was tough, smooth, and inflexible, with significant tenderness. Laryngoscopy showed a large amount of off-white caseating deposition in the nasopharynx, blocking both sides of the posterior nostril. Histologic sections of the neoplasm showed diffuse replacement of the normal architecture by a spindle or ovoid cells. The atypical cells were arranged in the form of fascicles or whorls. Further immunohistochemistry was performed and proved that the tumor cells were strongly and diffusely positive for S-100, vimentin and CD163, and negative for CD21, CD23, CD35 and CD1a. Those immunohistochemical features excluded follicular dendritic cell sarcoma (FDCS) and confirmed IDCS diagnosis (Figure 1).
 |
Figure 1 Biopsy pathology of the nasopharyngeal tumor. (A) (HE 400x) Diffuse short spindle or round tumor cells were arranged in fuzzy bundles with neutrophils and eosinophil infiltration. The nuclei of tumor cells had light chromatin, slight folds, and occasional furrows with small nucleoli. (B) (200×) Immunohistochemistry showed that the tumor cells were strongly and diffusely positive for S-100, Ki67 and CD163, and negative for CD21, Langerin and CD1a. |
The patient visited our department on the 11th day after cesarean section. Her blood test showed as following: WBC 8.09×109/L, RBC 4.9×1012/L, Hb 84 g/L, PLT 265×109/L and β-2 microglobulin 2.7 mg/L. Her EBV-DNA load was increased at 1.78E+03 IU/mL. The PET-CT scan exhibited enhanced fluorodeoxyglucose (FDG) metabolism activity in an irregular soft tissue mass in the left nasopharynx involving bilateral oropharynx, which was consistent with the appearance of sarcoma. Besides, multiple enlarged lymph nodes were found in the bilateral neck and left supraclavicular region and retroperitoneum, and slightly lower-density nodules were suspected in the tail of the pancreas. These above sites also showed high FDG uptake and were considered sarcoma metastasis (Figure 2). Bone marrow biopsy revealed no significant abnormality. Thus, the patient was finally diagnosed as disseminated IDCS.
 |
Figure 2 The whole-body imaging of PET-CT at initial diagnosis on 2017-10-8. (A) Irregular soft tissue mass could be seen in the left nasopharynx, with the length and diameter of about 50mm, increased radioactive uptake, SUVmax29.43, involving bilateral oropharynx, disappeared pharyngeal crypt, and narrow pharyngeal cavity. (B) Increased FDG uptake were revealed in multiple enlarged lymph nodes involved the bilateral neck (SUVmax29.75) and left supraclavicular area (SUVmax28.53). (C) Foci of high FDG uptake were shown in pancreas (SUVmax4.11), mesentery and intestinal wall (SUVmax18.96). |
Treatment Process
The patient was initially treated with a GDP regimen (gemcitabine 1.2 g, oxaliplatin 150 mg, and dexamethasone 15 mg) but had no obvious response. Subsequently, we changed the treatment with ABVD (epirubicin 50 mg, bleomycin 15 mg, vinorelbine 40 mg, and dacarbazine 500 mg) combined with dexamethasone (15 mg) regimen for 4 courses. Surprisingly, the patient achieved partial remission (PR) with the smaller tumor and disappearance of some enlarged lymph nodes. Thereafter, we repeated the administration of the ABVD regimen combined with asparaginase (3750 IU) for 2 courses, followed by 1 cycle of radiotherapy. The curative effect of above mentioned chemoradiotherapy was evaluated as PR by PET-CT. Specifically, the soft tissue on the left wall of the nasopharynx seemed to be disappeared with slightly thickened mucosa, which displayed no obvious increase in FDG metabolism. Lymph nodes on the left neck were shrinked with reduced FDG uptake compared to pretreatment.
Afterward, the patient underwent autologous hematopoietic stem cell transplantation (auto-HSCT). Arabinoside chemotherapy plus granulocyte colony-stimulating factor (G-CSF) were used to mobilize peripheral blood stem cells (PBSCs), and the subsequent pretreatment scheme of auto-HSCT was as follows: cladribine 7.6 mg/d (−7~−3d), cytarabine 3 g/d (−7~−6d), busulfan 164 mg/d (−5~−2d). The patient received 28.3×106/kg CD34+ cells and 17.76×108/kg mononuclear cells (MNCs). Granulocytes and platelets were engrafted on days 11 and 13. On the 20th day after transplantation, routine blood test showed WBC 3.11×109/L with NEUT 1.99×109/L, Hb 81 g/L, PLT 158×109/L. Urinalysis, hepatic and renal function test results were within normal limits. In addition, hepatitis B virus DNA and Epstein–Barr virus DNA were negative.
Survival Outcome
Three months after transplantation, the patient eventually achieved CR by PET-CT evaluation, which showed disappearance of the nasopharyngeal mass and normal metabolism of the left supraclavicular lymph node and mesentery (Figure 3). Encouragingly, this patient has now obtained over 5 years of disease-free survival by annual follow-up.
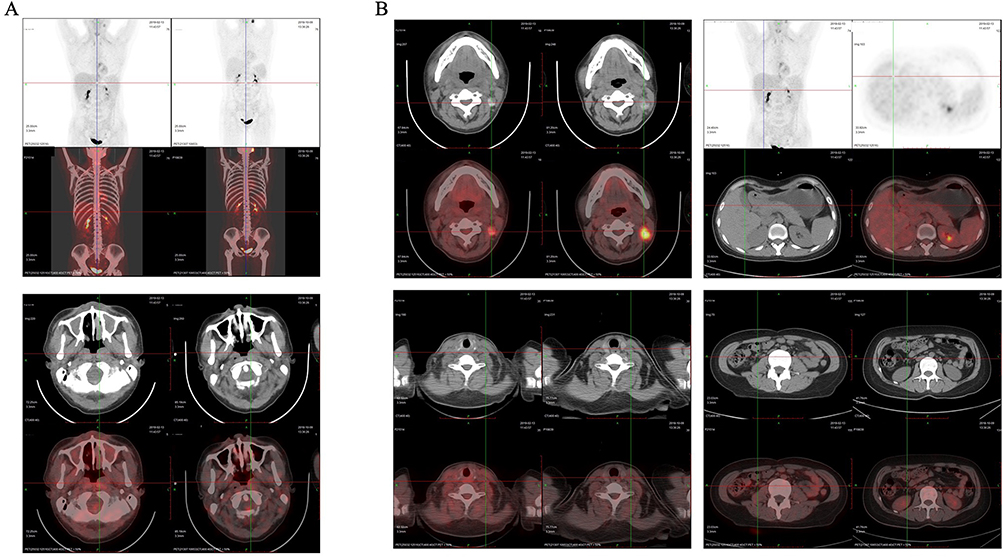 |
Figure 3 A follow-up PET-CT after three months of auto-HSCT on 2019-2-13 (left) compared to 2018-10-19 (right) before transplantation. (A) After treatment, the mass in the left nasopharynx was complete disappeared and bilateral nasopharyngeal was symmetrical with no abnormal FDG uptake. (B) The enlarged lymph nodes in the left neck, left supraclavicular and mesenteric regions were shrunk to normal size with no obvious metabolism. |
Discussion
Dendritic cells (DCs) are the immune system’s accessory cells, which functions as the key factor in antigen capture, presentation, and immune response and regulation.4,5 IDCs are a type of dendritic cells (DCs) originated from hematopoietic precursors and are mainly located in the T-zone of lymphoid organs. Their primary functions are antigen capture, presentation, and immune response and regulation.6 IDCS is an extremely rare, aggressive and highly fatal malignant proliferative disease with spindular to ovoid cells similar to the IDCs phenotype. It is generally believed that IDCS originated from IDCs, whereas some recent studies suggest that IDCS may be transdifferentiated from lymphoid or myeloid tumors.7–9
At yet, the diagnosis of IDCS is still challenging because of its nonspecific clinical presentation and confusing cytomorphologic and immunohistochemical features.2 IDCS generally occurs in adults with male predominance and usually present with painless localized lymphadenectasis (especially cervical lymph node involvement). Other manifestations like systemic symptoms including fever, weight loss, fatigue or night sweats are rarely reported. One-third of IDCS have extranodal involvement and the common sites of extranodal invasion are nasopharynx, liver, skin, gastrointestinal tract (GIT), bladder, nervous system.10–12 Microscopically, most neoplastic cells are spindle or ovoid, forming diffuse, fascicular, whorled, or storiform structures surrounded by small lymphocytes, plasma cells, or other inflammatory cells. The neoplastic cells show abundant and slightly eosinophilic cytoplasm, with unclear cell boundaries, oval or irregular central nuclei, chromatin dispersed in vacuoles, thin nuclear membrane and eosinophilic nucleolus. The main immunohistochemical characteristics of IDCS are positive staining for S-100, vimentin, with weak and variable CD68 expression and negative staining for CD21, CD23 and CD35, which are markers of FDCs. They are characterized by variable staining for CD45RO, CD4, CD43, CD163 and SMA and negative staining for Melan-A, HMB-45, cytokeratin, epithelial membrane antigen (EMA), CD30, CD34, ALK, langerin, B cell markers, T cell markes and myeloperoxidase (MPO).13–16 The Ki-67 labeling index is usually low (10–20%) though more aggressive proliferation.1
The etiopathogenesis of IDCS is yet to be elucidated. Epstein–Barr virus (EBV) and human herpes virus (HHV) 8 infection were usually considered useless for the disease.17,18 However, the patients with IDCS attending our hospital was diagnosed with EBV infection at her first visit. Whether this is related to lower immunity in the third trimester or opportunistic infections remains to be further studied. It is worth noting that about 20% IDCS cases have immunosuppression and other hematological or nonhematological malignancies.2 Several studies have shown that IDCS may transdifferentiate from mature B-cell lymphoma (follicular lymphoma and CLL/SLL) in consideration of the same molecular alterations (BCL-2/IgH translocation) and monoclonal immunoglobulin heavy-chain gene (IgH gene) rearrangement.19,20 It has also been considered that IDCS may be directly related to the BCL-2 gene.21 Other genetic alterations like MYC gene translocation, BRAF-V600E, ARID2, TET2, TP53 mutations, RAS-BRAF signal transduction (NF1 mutation) and NF-κB activation (TNFAIP3) are also reported associated with this transdifferentiation.9,22–25
Although IDCS prognosis is known to be aggressive, no standard strategy has yet been developed because of its infrequency. Generally, localized disease was found to be related with a better prognosis, while the young age, measuring more than 5 cm in diameter, disseminated lesions involvement indicated a poor outcome of patients.10 The main treatments of IDCS include surgical management, radiotherapy, chemotherapy and targeted therapy. Complete surgical resection is preferred for patients with localized IDCS. Adjuvant chemotherapy or radiotherapy after surgery is usually not needed for its ineffectiveness.2,18 Chemotherapy is usually recommended for patients with disseminated IDCS. The most frequently used regimens are CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone), ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine). Other reported regimens include ESHAP (etoposide, methylprednisolone, cytosine arabinoside, platinum), DHAP (dexamethasone, cisplatin, high-dose cytarabine), EPOCH (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin), ICE (ifosfamide, carboplatin, etoposide), gemcitabine/docetaxel, Alkylating agent/platinum/anthracycline combinations with methotrexate, etoposide, L-asparaginase or bleomycin combinations of cisplatin, epirubicin, and high-dose methotrexate, among others.2,26,27 Of these regimens, the ABVD regimen has proven to be an effective treatment for IDCS.28–30 However, the efficacy of other regimens is not very satisfactory. In this case, during the first visit the patient had extensive metastasis, and the therapeutic effect of the GDP regimen was not desired. After 4 courses of chemotherapy based on the ABVD regimen, the patient achieved PR. Therefore, the ABVD regimen is effective in the treatment of IDCS.
In addition to the treatment strategies mentioned above, stem cell transplantation (including autologous and allogeneic stem cell transplant) had been reported for IDCS, although the number of reported cases is limited. Thereinto, autologous stem cell transplant has been reported mostly.2 Considering that the patient at our center was relatively young with distant spread but no bone marrow invasion and had not achieved CR after 7 courses of chemotherapy (1 GDP+6 ABVD) and 1 course of radiotherapy, we chose auto-HSCT after a comprehensive evaluation. High-dose conditioning regimens for eradicating resistant tumor and making room for the stem cell allografts prior to autologous transplantation are critical to patients’ clinical outcomes. So far, there is no standardized conditioning regimen for IDCS. The lymphoma pretreatment regimen BEAM (BCNU, cytarabine, etoposide and melphalan) was the mostly reported chemotherapy.27 Unfortunately, outcomes remain poor in disseminated patients undergoing autologous stem cell transplantation after BEAM high-dose chemotherapy.31 Since IDCS is a bone marrow hematopoietic stem cell-derived tumor, we tried to choose a myelogenous malignancies pretreatment regimen containing cladribine, cytarabine, and busulfan. Cladribine is a deoxyadenosine analog resistant to adenosine deaminase (ADA), which has broad-spectrum activity against lymphocytes and myeloid cells.32 The use of bifunctional DNA alkylating agent busulfan-based conditioning is also extending rapidly to hematopoietic stem cell transplantation (HSCT) for lymphoid malignancies.33 This conditioning regimen received by this patient has resulted in a good myeloablative effect without serious adverse reactions. This patient showed a fast neutrophils and platelets engraftment and fortunately achieved CR after transplantation. The patient receives regular checkups in the outpatient department and has now obtained a disease-free survival over 5 years. The pooled analysis by Shi et al showed that patients with diffused lesion had median PFS of 3 months and a median OS of 9 months.11 Recently, Fugere et al reported that IDCS patients with metastatic disease at diagnosis had a poor prognosis with a median OS of 5 months.34 To our knowledge, this disseminated IDCS patient attended at our center achieved a quite long survival. Therefore, we speculate that the use of conditioning therapy containing cladribine, cytarabine, and busulfan prior to auto-HSCT could improve the prognosis of these patients.
This study has some limitations. First, cladribine has been reported to lead cell death by interfering with DNA repair, induce cell apoptosis by both caspase-dependent and caspase-independent mechanisms, prevent DNA methylation, synergize with cytarabine, exhibit antitumor immunity.35,36 The precise mechanism underlying the successful outcomes achieved by the cladribine-containing pretransplant strategy in this case remains unclear. Second, the high economic burden is indeed an important factor influencing patients’ choice of cladribine-containing regimens. Third, immune checkpoint inhibitors like anti-PD-1 monoclonal antibodies might be promising in patients with FDCS.37 Although we have not attempted this immunotherapy approach, a previously reported IDCS patient appears to be unresponsive to treatment with PD-1 inhibition.38 Finally, since this represents only a successful case report, further studies with larger sample sizes will be required to validate our therapeutic experience.
In conclusion, the long-term survival of the case in our center might indicate that the ABVD regimen is effective for disseminated IDCS patients, while further cladribine, cytarabine, and busulfan as a preparative regimen before auto-HSCT for patients without CR could result in better prognosis. Therefore, further studies with larger IDCS case series are needed to verify these preliminary findings.
Ethics and Consent
The patient voluntarily provided written informed consent for publication of their medical data and images. There was no institutional approval that required for publication.
Funding
The Youth Program of the National Natural Science Foundation of China (No. 82100222); Henan Natural Science Foundation (162300410287).
Disclosure
No potential conflict of interest was reported by the authors.
References
1. Zhou J, Li Q, Fu X, Feng D, Yang K, Wang J. Interdigitating dendritic cell sarcoma: analysis of two original extra-nodal cases and review of literature. Virchows Arch. 2022;481(1):101–110. doi:10.1007/s00428-022-03320-9
2. Muhammed A, Ahmed ARH, Maysa H, Mohamed AES, Abd-ElLateef AA, Elnakib E. New insights inside the interdigitating dendritic cell sarcoma-pooled analysis and review of literature. Ann Hematol. 2019;98(12):2641–2651. doi:10.1007/s00277-019-03824-6
3. Tanaka A, Uemura H, Matsuoka M, Takeda M, Kitahara T. An extremely rare case of interdigitating dendritic cell sarcoma of the parotid gland with a 40‑month disease‑free survival time after only surgery: a case report. Oncol Lett. 2023;25(3):130. doi:10.3892/ol.2023.13716
4. Mellman I. Dendritic cells: master regulators of the immune response. Cancer Immunol Res. 2013;1(3):145–149. doi:10.1158/2326-6066.CIR-13-0102
5. Balan S, Saxena M, Bhardwaj N. Dendritic cell subsets and locations. Int Rev Cell mol Biol. 2019;348:1–68. doi:10.1016/bs.ircmb.2019.07.004
6. Waisman A, Lukas D, Clausen BE, Yogev N. Dendritic cells as gatekeepers of tolerance. Semin Immunopathol. 2017;39(2):153–163. doi:10.1007/s00281-016-0583-z
7. Shao H, Xi L, Raffeld M, et al. Clonally related histiocytic/dendritic cell sarcoma and chronic lymphocytic leukemia/small lymphocytic lymphoma: a study of seven cases. Mod Pathol. 2011;24(11):1421–1432. doi:10.1038/modpathol.2011.102
8. Jiang YZ, Dong NZ, Wu DP, Xue SL. Interdigitating dendritic cell sarcoma presenting simultaneously with acute myelomonocytic leukemia: report of a rare case and literature review. Int J Hematol. 2013;97(5):657–666. doi:10.1007/s12185-013-1336-6
9. Ochi Y, Hiramoto N, Yoshizato T, et al. Clonally related diffuse large B-cell lymphoma and interdigitating dendritic cell sarcoma sharing MYC translocation. Haematologica. 2018;103(11):e553–e556. doi:10.3324/haematol.2018.193490
10. Xue T, Jiang XN, Wang WG, Zhou XY, Li XQ. Interdigitating dendritic cell sarcoma: clinicopathologic study of 8 cases with review of the literature. Ann Diagn Pathol. 2018;34:155–160. doi:10.1016/j.anndiagpath.2018.03.008
11. Shi F, Song Q, Wang L, Gao Y, Chang H. Diffuse lesion and necrosis tied to poorer prognosis of interdigitating dendritic cell sarcoma: cases report and a pooled analysis. Sci Rep. 2017;7(1):667. doi:10.1038/s41598-017-00719-2
12. Zhou J, Zhou W, Bai C, Zhou Y, Wang Y. Interdigitating dendritic cell sarcoma: case report with review of the literature. Onkologie. 2011;34(11):634–637. doi:10.1159/000334212
13. Yao ZG, Wang YK, Qin YJ, Zhao MQ, Li X. A rare case of rectal interdigitating dentritic cell sarcoma presenting with a polypoid appearance. Pathology. 2016;48(7):744–746. doi:10.1016/j.pathol.2016.07.013
14. Pan M, Gong Q, Fan Q, Zhang Z, Li Y, Wang C. [Interdigitating dendritic cell sarcoma/tumor: a clinicopathologic study]. Zhonghua Bing Li Xue Za Zhi. 2014;43(2):99–102.
15. Yoon SO. Pathologic characteristics of histiocytic and dendritic cell neoplasms. Blood Res. 2024;59(1):18. doi:10.1007/s44313-024-00015-9
16. Jain P, Patel KP, Futreal A, et al. Clinico-pathological characteristics, treatments and outcomes of patients with dendritic cell sarcoma (DS). Blood. 2015;126(23):2700.
17. Barwell N, Howatson R, Jackson R, Johnson A, Jarrett RF, Cook G. Interdigitating dendritic cell sarcoma of salivary gland associated lymphoid tissue not associated with HHV-8 or EBV infection. J Clin Pathol. 2004;57(1):87–89. doi:10.1136/jcp.57.1.87
18. Pokuri VK, Merzianu M, Gandhi S, Baqai J, Loree TR, Bhat S. Interdigitating dendritic cell sarcoma. J Natl Compr Canc Netw. 2015;13(2):128–132. doi:10.6004/jnccn.2015.0020
19. Feldman AL, Arber DA, Pittaluga S, et al. Clonally related follicular lymphomas and histiocytic/dendritic cell sarcomas: evidence for transdifferentiation of the follicular lymphoma clone. Blood. 2008;111(12):5433–5439. doi:10.1182/blood-2007-11-124792
20. Fraser CR, Wang W, Gomez M, et al. Transformation of chronic lymphocytic leukemia/small lymphocytic lymphoma to interdigitating dendritic cell sarcoma: evidence for transdifferentiation of the lymphoma clone. Am J Clin Pathol. 2009;132(6):928–939. doi:10.1309/AJCPWQ0I0DGXBMHO
21. Nayer H, Murphy KM, Hawkins AL, et al. Clonal cytogenetic abnormalities and BCL2 rearrangement in interdigitating dendritic cell sarcoma. Leuk Lymphoma. 2006;47(12):2651–2654. doi:10.1080/10428190600879896
22. Di Liso E, Pennelli N, Lodovichetti G, et al. Braf mutation in interdigitating dendritic cell sarcoma: a case report and review of the literature. Cancer Biol Ther. 2015;16(8):1128–1135. doi:10.1080/15384047.2015.1057359
23. Hillen U, Grabellus F, Franklin C, Sucker A, Schadendorf D, Schilling B. Oncogene status of an interdigitating dendritic cell sarcoma: recurrent mutations in NF1, TP53, and ARID2 shared with melanoma. Am J Surg Pathol. 2016;40(12):1721–1723. doi:10.1097/PAS.0000000000000746
24. Massoth LR, Hung YP, Ferry JA, et al. Histiocytic and dendritic cell sarcomas of hematopoietic origin share targetable genomic alterations distinct from follicular dendritic cell sarcoma. Oncologist. 2021;26(7):e1263–e1272. doi:10.1002/onco.13801
25. Erich SA, Teske E. One health: therapies targeting genetic variants in human and canine histiocytic and dendritic cell sarcomas. Vet Comp Oncol. 2024. doi:10.1111/vco.12988
26. Dainese E, Cimetti L, Pozzi B, et al. Primary cutaneous interdigitating dendritic cell sarcoma (IDCS): report of a new case and literature review. Pathol Res Pract. 2023;247:154559. doi:10.1016/j.prp.2023.154559
27. Adam Z, Vesely K, Krejci M, et al. [Interdigitating dendritic cell sarcoma of lower extremities resistant to high dose chemotherapy BEAM with peripheral blood stem cell transplantation]. Vnitr Lek. 2009;55(2):147–157.
28. Lee SY, Lee SR, Chang WJ, Kim HS, Kim BS, Kim IS. Successful treatment of disseminated interdigitating dendritic cell sarcoma with Adriamycin, bleomycin, vinblastine, and dacarbazine chemotherapy. Korean J Hematol. 2012;47(2):150–153. doi:10.5045/kjh.2012.47.2.150
29. Helbig G, Wichary R, Pajak J, et al. Sustained remission after ABVD treatment for interdigitating dendritic cell sarcoma. Contemp Oncol. 2015;19(1):83–85. doi:10.5114/wo.2014.43974
30. Kyogoku C, Seki M, Ogawa S, et al. Complete remission in systemic skin interdigitating dendritic cell sarcoma after ABVD chemotherapy. J Clin Exp Hematop. 2015;55(1):33–37. doi:10.3960/jslrt.55.33
31. Adam Z, Pour L, Vesely K, et al. Interdigitating dendritic cell sarcoma of the leg. Onkologie. 2009;32(6):364–365. doi:10.1159/000217796
32. Bryson HM, Sorkin EM. Cladribine. A review of its pharmacodynamic and pharmacokinetic properties and therapeutic potential in haematological malignancies. Drugs. 1993;46(5):872–894. doi:10.2165/00003495-199346050-00007
33. Ciurea SO, Andersson BS. Busulfan in hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2009;15(5):523–536. doi:10.1016/j.bbmt.2008.12.489
34. Fugere T, Fugere B, Amisha F, et al. Interdigitating dendritic cell sarcoma and indeterminate dendritic cell tumor: patient characteristics, prognostic factors, and survival outcomes for rare dendritic cell neoplasms. Blood. 2023;142:5346.
35. Molica M, Breccia M, Capria S, et al. The role of cladribine in acute myeloid leukemia: an old drug up to new tricks. Leuk Lymphoma. 2020;61(3):536–545. doi:10.1080/10428194.2019.1672060
36. Kohnke PL, Mactier S, Almazi JG, Crossett B, Christopherson RI. Fludarabine and cladribine induce changes in surface proteins on human B-lymphoid cell lines involved with apoptosis, cell survival, and antitumor immunity. J Proteome Res. 2012;11(9):4436–4448. doi:10.1021/pr300079c
37. Assi T, Cesne AL. Immune checkpoint inhibitors in follicular dendritic cell sarcoma. Immunotherapy. 2024;16(6):341–344. doi:10.2217/imt-2023-0230
38. Chen HZ, Bonneville R, Yu L, et al. Genomic characterization of metastatic ultra-hypermutated interdigitating dendritic cell sarcoma through rapid research autopsy. Oncotarget. 2019;10(3):277–288. doi:10.18632/oncotarget.26352
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.