Back to Journals » Therapeutics and Clinical Risk Management » Volume 12
Long-term safety of tiotropium delivered by Respimat® SoftMist™ Inhaler: patient selection and special considerations
Authors Tan CK, Say GQ, Geake J
Received 22 March 2016
Accepted for publication 17 June 2016
Published 21 September 2016 Volume 2016:12 Pages 1433—1444
DOI https://doi.org/10.2147/TCRM.S109011
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Ching Kuo Tan, Gui Quan Say, James B Geake
Department of Respiratory Medicine, Lyell McEwin Hospital, Elizabeth Vale, SA, Australia
Abstract: Tiotropium bromide is a long-acting inhaled muscarinic antagonist used in patients with chronic respiratory disease. It has been available since 2002 as a single-dose dry powder formulation via the HandiHaler® dry powder inhaler (DPI) device, and since 2007 as the Respimat® SoftMist™ Inhaler (SMI). The latter is a novel method of medication delivery that utilizes a multidose aqueous solution to deliver the drug as a fine mist. Potential benefits include more efficient drug deposition throughout the respiratory tract, reduced systemic exposure, and greater ease of use and patient satisfaction compared with the use of HandiHaler DPI. Although tiotropium bromide delivered via the HandiHaler DPI has been clearly shown to improve lung function, dyspnea, and quality of life and to reduce exacerbations in patients with chronic obstructive pulmonary disease (COPD), there is accumulating evidence regarding the use of tiotropium HandiHaler in other respiratory diseases characterized by airflow limitation, such as asthma and cystic fibrosis. Developed more recently, tiotropium delivered via the Respimat SMI appears to have a similar efficacy and safety profile to the HandiHaler DPI, and early data raising the possibility of safety concerns with its use in COPD have been refuted by more recent evidence. The benefits over the HandiHaler DPI, however, remain unclear. This paper will review the evidence for tiotropium delivered via the Respimat SMI inhaler, in particular as an alternative to the HandiHaler DPI, and will focus on the safety profile for each of the chronic lung diseases in which it has been trialed, as well as an approach to appropriate patient selection.
Keywords: tiotropium, Respimat, safety, COPD, asthma, HandiHaler
Introduction
Tiotropium bromide (Spiriva®, Boehringer Ingelheim Pharma GmbH & Co KG, Ingelheim am Rhein, Germany) is an inhaled long-acting muscarinic antagonist. It acts via competitively binding predominantly to M3 receptors contained within bronchial smooth muscle, attenuating cholinergic-mediated bronchoconstriction.1 It was approved by the US Food and Drug Administration (FDA) in 2004 for the treatment of chronic obstructive pulmonary disease (COPD) via the HandiHaler® dry power inhaler (DPI, Boehringer Ingelheim International GmbH),2 and has subsequently been approved across many health care jurisdictions worldwide for this indication. There is convincing evidence that this treatment results in improved lung function and quality of life and reduced breathlessness and exacerbations in patients with COPD.3–6 It has also been trialed in other obstructive lung diseases, and in particular there is now also increasing evidence that it has favorable effects on chronic suboptimally controlled asthma.7–9 The HandiHaler DPI device delivers tiotropium via an inhaled dry powder mechanism, using lactose powder as a carrier.10 This mechanism relies on the inspiratory airflow generated by the patient to deposit the drug particles in the lungs. Many variables influence the amount of drug inhaled into the lungs, including inspiratory flow profile of the device, inspiratory airflow volume generated by the patient, and the amount of moisture in the oropharynx.11 Therefore, it is possible that drug deposition varies considerably between patients and is likely to be compromised in patients who have severe respiratory disease with already limited inspiratory capacity.
In attempts to improve drug deposition, particularly for patients with severe chronic lung disease who are unable to generate sufficient inspiratory flow rates, the Respimat® SoftMist™ Inhaler (SMI; Boehringer Ingelheim International GmbH) was developed. It was approved by the FDA in September 201412 and dispenses a 5-μg dose. In this novel delivery device, mechanical energy (via a spring that is actuated by the patient) is used to convert a liquid drug solution to a transient mist, which can then be inhaled by the patient.13 This means that the delivered drug dose is independent of inspiratory effort, and the increased time for which the drug remained in the oropharynx provided greater opportunity to coordinate device actuation and patient inhalation. In addition, the Respimat SMI inhaler results in high fine-particle fraction, as well as low ejection velocity and long spray duration. In combination, it is postulated that these features provide improved lung deposition, minimize loss of small diameter particles during exhalation, and reduce oropharyngeal deposition.11 Supporting evidence comes predominantly from trials using compounds other than tiotropium, in healthy patients without lung disease or in patients with mild-to-moderate asthma.13–16 The extent to which these theoretical benefits translate into improved clinical efficacy and acceptable safety profile remains controversial.
Search strategy
We performed a literature search from the databases Medline and Cochrane Library, with the assistance of an experienced librarian. The search terms and study flow diagram are included in the supplementary material (Table S1 and Figure S1).
Pharmacokinetics and pharmacodynamics
Tiotropium is an anticholinergic agent. Upon delivery to respiratory epithelium, it competitively and reversibly binds as an antagonist to the M3 subtype muscarinic receptors within bronchial smooth muscle, resulting in bronchodilation because of inhibition of cholinergic-mediated bronchoconstriction.1 As with any inhaled medication, not all of the dispensed medication reaches the intended airway mucosa. A proportion is lost through exhalation or coughing, and a portion is delivered directly to the systemic circulation after deposition in the upper aerodigestive tract. In vitro studies suggest that tiotropium does not undergo significant hepatic metabolism and is predominantly cleared by renal action.17 It is the small proportion of active drug reaching the systemic circulation that is responsible for many of the unwanted side effects of the drug, and therefore lower systemic exposures might be expected to result in fewer adverse and serious adverse events. Thus, the lower dose of tiotropium dispensed with Respimat SMI compared with the HandiHaler DPI, in combination with a possible greater efficiency of delivery, might result in a reduction in systemic exposure, and in turn an improved safety profile.
However, pharmacokinetic data from clinical trials have been conflicting. Some have shown generally similar profiles,18,19 others have suggested increased systemic exposure with the Respimat SMI,20 and still others have more recently demonstrated the opposite.21 In 2014, a crossover trial enrolled 154 COPD patients who were then randomized into five different treatment arms comprising placebo, tiotropium HandiHaler DPI 18 μg, and tiotropium Respimat SMI 1.25, 2.5, and 5 μg, respectively.19 This study found lower peak plasma concentrations (Cmax, ss) in the tiotropium Respimat SMI 5-μg solution group compared to the HandiHaler DPI group (Figure 1), although it was still greater than in the manufacturer’s report.1 On the other hand, plasma concentrations of tiotropium HandiHaler DPI were significantly less in pharmacological studies compared to the manufacturer’s reported value.10,20,21 Given the conflicting pharmacokinetic data, in vitro bioequivalence cannot be assumed between the HandiHaler and Respimat devices.21
 | Figure 1 (A) Mean tiotropium plasma concentration–time profile following inhalations as Respimat SMI solution or HandiHaler DPI. (B) Steady-state plasma concentrations (Cmax, ss) by dose and device. |
Tiotropium Respimat SMI in asthma
Efficacy
There is now an accumulating and reasonably substantial body of evidence supporting the use of tiotropium Respimat SMI in patients with suboptimally controlled asthma despite optimal treatment with moderate-to-high doses of inhaled corticosteroids (ICS), either in addition to ICS/long-acting β-2-agonist (LABA) combination, or in place of a LABA.22 Kerstjens et al23 was one of the first to demonstrate its benefit in a randomized controlled trial conducted in 2011, where they found significant spirometric and clinical benefits of tiotropium Respimat SMI compared to placebo. Since then, many other studies have shown similar results (Table 1). Perhaps more importantly, tiotropium Respimat SMI was shown to reduce the risk of asthma exacerbations compared to placebo, even with the use of adjunct therapies.7 Overall, tiotropium Respimat SMI has been shown to be beneficial in patients with asthma, regardless of age,24,25 baseline function,26 allergic status (as defined by serum Immunoglobulin E levels, or clinical evidence of allergic asthma),27 or phenotype.28 There are no studies that directly compare the efficacy between tiotropium HandiHaler DPI and tiotropium Respimat SMI in patients with asthma.
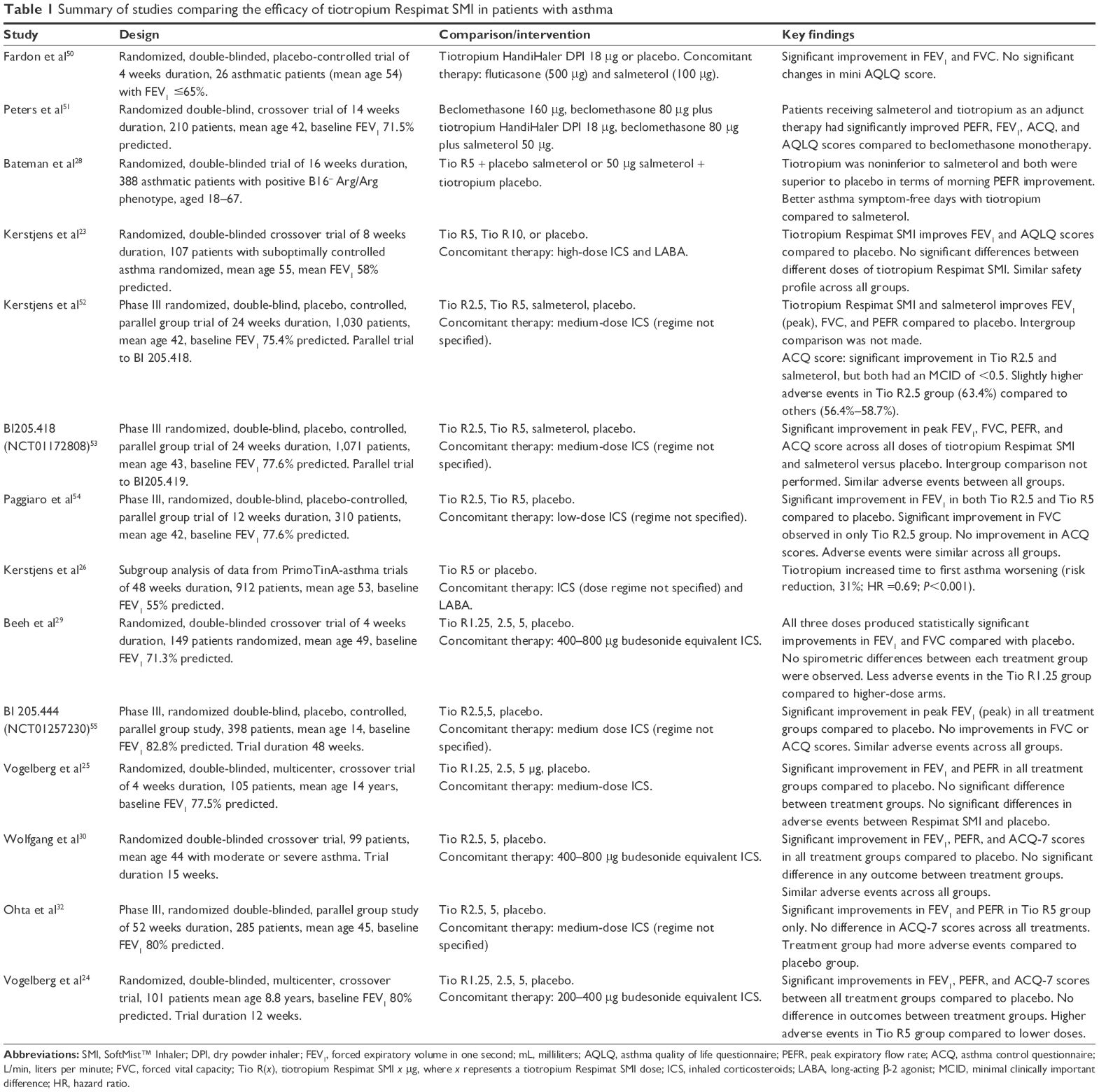 | Table 1 Summary of studies comparing the efficacy of tiotropium Respimat SMI in patients with asthma |
Safety and tolerability
Tiotropium Respimat SMI appears to be generally well tolerated in patients with asthma, and rates of discontinuation reported in clinical trials have been low (between 1% and 4%).28,29 Fatal events have been extremely rare, and no mortality signal to match the early concerns in the COPD population has emerged. However, the frequency of adverse events, in particular severe adverse events, does appear to increase with increasing doses of tiotropium.23,30,31 A large pooled analysis found that patients who are administered 5 μg tiotropium Respimat SMI are 1.5 times more likely to have an adverse event leading to discontinuation, and 2.28 times more likely to have a severe adverse event compared to those who receive 2.5-μg tiotropium Respimat SMI.31 Similarly, patients who are administered 10-μg tiotropium Respimat SMI are 1.15 times more likely to experience an adverse event compared to patients who are given 5-μg tiotropium Respimat SMI.23 The relationship between dose and adverse events appears to be constant in children.25 The most common severe adverse events are pneumonia and cardiac arrhythmias.7 Coronary artery disease was also reported in 0.8% of cases.7 The most common adverse events are exacerbation of asthma, nasopharyngitis, and upper respiratory tract infection.31 Cardiac adverse events are rare, ranging from 0.4%1 to 4.4%.32
Patient selection and special considerations
In most guidelines, tiotropium is suggested for asthmatic patients with persisting evidence of disease activity despite being established in alternative inhaled regimens. The GINA (Global Initiative for Asthma) guidelines recommend adding tiotropium if an adult patient’s symptoms are not controlled by medium- or high-dose ICS (2,000 μg beclomethasone equivalent) plus long-acting β-2-agonist therapy (Figure 2).33 The American Thoracic Society guidelines state that the use of long-acting muscarinic antagonists should be reserved only for moderate-to-severe asthmatics.34 Such recommendations are corroborated by the manufacturer’s recommendation.35 A meta-analysis conducted in 201522 found that the benefit of tiotropium is greatest in patients with poorly controlled asthma. They found that while tiotropium confers spirometric improvement in asthma patients regardless of severity, patients with severe asthma demonstrated larger benefits, particularly improvement in the quality of life.22 Although data from these trials and guidelines appear to encourage the use of tiotropium in poorly controlled asthmatics, it should be noted that these trials often have strict exclusion criteria. In particular, patients with underlying cardiac disorders are often excluded. Given the small increase in adverse events with increasing doses of tiotropium,36 caution should be exercised before prescribing tiotropium in patients with underlying cardiac disease. Attempts should also be made to ensure compliance with existing therapy prior to adding further agents to existing therapy regimes, as it has been reported that up to 80% of patients with poorly controlled asthma have poor compliance rates.36
 | Figure 2 GINA guidelines for management of asthma. |
In summary, tiotropium Respimat SMI should be considered in patients with asthma having persistent disease activity as measured by lung function or symptom records, despite the use of moderate-to-high doses of ICS, with or without concomitant LABA.7 It should be avoided in patients with a history of acute myocardial infarction within the last 6 months, patients with a history of malignant cardiac arrhythmias, patients with New York Heart Association Class III or IV heart failure, patients with acute angle glaucoma, or in males with prostatic hypertrophy.17
Tiotropium Respimat SMI in COPD
Efficacy
Tiotropium HandiHaler DPI 18 μg improves lung function, dyspnea, and quality of life and reduces exacerbations in patients with COPD.3–6,37 There is now a fairly large volume of accumulated data demonstrating similar spirometric and clinical outcomes between the HandiHaler DPI and the Respimat SMI. Both direct randomized placebo-controlled trials comparing Respimat SMI with placebo and noninferiority trials comparing Respimat SMI with HandiHaler DPI support their use in stable COPD.38,39
Safety and tolerability
Dry mouth, constipation, and urinary tract infections38,40 are the most commonly reported adverse events in patients with COPD trials. The most common nonanticholinergic-mediated adverse events were nasopharyngitis, sinusitis, bronchitis, and exacerbations of COPD.19,38 Other less common side effects (<1%) include urinary retention, dry skin, angioedema, abnormal liver function test, and gastroesophageal reflux disease.
For several years, there were concerns regarding the safety of tiotropium Respimat SMI. Although many of the original trials showed no significant deaths or adverse events,19,38,40 initial aggregate data raised the possibility of a safety signal for Respimat SMI. In particular, two systematic reviews reported an increase in mortality6,20 with the Respimat SMI device. Shortly thereafter, a population-based longitudinal observational study was done in the Netherlands that showed an increased risk of death in patients using Respimat SMI compared to HandiHaler DPI, and that the risk was higher in patients with coexisting cardiovascular disease.41
Critiques pointed out that the reviews described earlier were confounded by imbalances in the randomization and higher dropouts in the placebo group, and the inclusion of the Respimat SMI 10 μg dose. Nonetheless, in the light of these findings, the FDA initially did not approve the use of tiotropium Respimat SMI in the USA.
The TIOSPIR study was conducted with the primary aim of addressing this concern and directly compared Respimat SMI and HandiHaler DPI in patients with COPD. This large double-blind study involved a total of 17,135 patients with COPD who were treated for a median duration of 835 days and followed up for a median of 2.3 years. The patients were randomized to receive either Respimat SMI 2.5 μg or Respimat SMI 5 μg, or a tiotropium HandiHaler DPI. Mortality rates were similar between tiotropium Respimat SMI 2.5 μg or 5 μg and tiotropium HandiHaler DPI (7.7% death from any cause in the Respimat SMI 2.5-μg group, 7.4% death in the Respimat SMI 5-μg group, and 7.7% in the HandiHaler DPI group). There was also no significant difference in cardiovascular deaths between the groups. In light of these data, the FDA approved tiotropium for use in stable COPD, and it has now been accepted for this indication across a number of health care jurisdictions around the world. It is important to note that although patients with concomitant cardiac disease were included, the patients with more acute cardiac disease were excluded from the trial (myocardial infarction within 6 months, NYHA Class III and IV heart failure admissions within 12 months, and unstable arrhythmias). Patients with unstable COPD were also excluded from the trial (recent exacerbation within 4 weeks, awaiting surgical intervention, and chronic use of corticosteroids >10 mg/d of prednisolone). They also excluded patients with other significant lung diseases (interstitial lung disease, bronchiectasis, asthma, cystic fibrosis [CF], or pulmonary thromboembolism).39 Finally, a stratified analysis of patients with and without chronic renal impairment from a partial cohort of the TIOSPIR study also demonstrated an increase in mortality associated with the use of tiotropium Respimat SMI in patients with Stage 3 to 5 chronic renal impairment, compared to placebo (adjusted hazard ratio [HR] =1.52, 95% confidence interval [CI] =1.02–2.28).42 Therefore, there is limited evidence to support the use of tiotropium Respimat in patients with other concurrent nonasthmatic pulmonary pathologies, or with significant renal impairment. Table 2 summarizes the studies comparing the safety and efficacy profile of tiotropium Respimat SMI compared to HandiHaler DPI and/or placebo in patients with COPD.
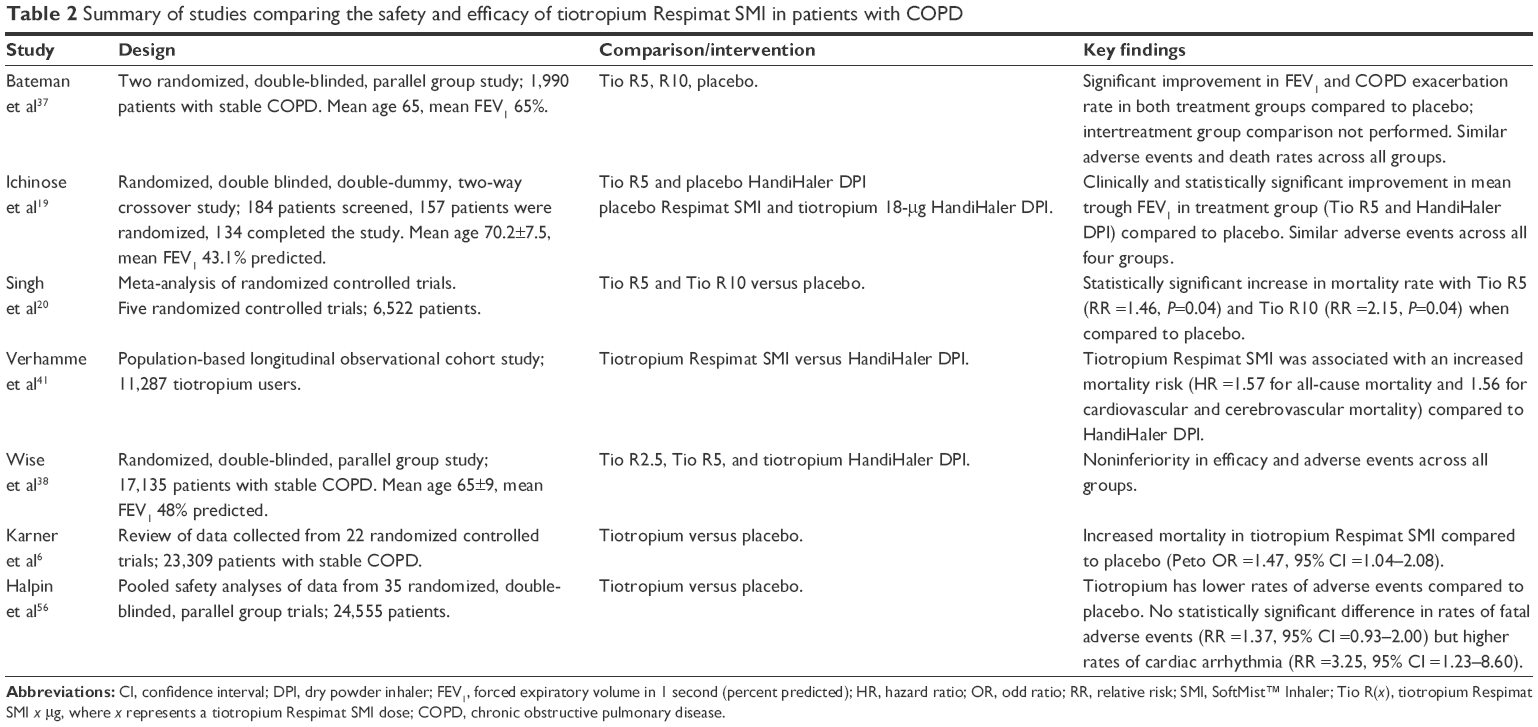 | Table 2 Summary of studies comparing the safety and efficacy of tiotropium Respimat SMI in patients with COPD |
Patient selection and special considerations
Overall, the data suggest fairly similar efficacy and safety profiles between Respimat SMI and HandiHaler DPI. Therefore, Respimat SMI should be considered for use in patients with stable COPD who are symptomatic or who suffer exacerbations. The use of both the devices should be carefully considered in patients with severe concomitant heart disease or other relative contraindications. However, there may be specific factors for patients with COPD that influence the use of one device over the other. Trotta et al43 conducted a retrospective, cohort, drug-utilization study to investigate factors that influence prescribers and patients to use tiotropium Respimat SMI or HandiHaler DPI. The study, conducted in 2011 in Italy, involved 9,920 COPD patients in a general hospital outpatient clinic, aged over 45 years with at least one prescription of tiotropium over a 2-year period. The researchers’ objectives were 1) to investigate what factors influence clinicians to prescribe a particular tiotropium formulation and 2) to investigate what factors led patients to switch from one formulation to another. They found that the HandiHaler DPI formed the majority (79.5%) of first prescriptions of tiotropium to patients; patients with underlying cardiac and neurological disorders were more likely to receive Respimat SMI as their first tiotropium prescription (odds ratio [OR] =1.29–1.65, respectively). When evaluating “switchers”, only 5.4% of the patients in the total cohort switched to the Respimat SMI formulation during the 2-year period, and 67% of the switches happened within the first 60 days of being prescribed HandiHaler DPI. The factors that were identified in increasing predisposition to switching from HandiHaler DPI to Respimat SMI are underlying cardiac disease (OR =1.76), severe respiratory disease requiring three (OR =1.96) or more (OR =4.62) other respiratory medications, and a younger age (OR =1.92).
Therefore, at present, patient and clinician preferences, as opposed to evidence from clinical trials, are likely to be the greatest drivers with regard to device choice in COPD, and the relatively high proportion of patients on HandiHaler DPI and the relatively low number of switchers in the aforementioned study suggest that the HandiHaler DPI remains popular among clinicians and patients alike. However, there may be niche roles for Respimat SMI, for example, in people with neurological disease who may have difficulty coordinating the steps in preparing and actuating the HandiHaler DPI device. Notably, there are a number of alternative antimuscarinic antagonists entering the market worldwide, and in at least one patient-preference study, both the HandiHaler DPI and Respimat SMI performed worse than alternatives.44,45
In conclusion, tiotropium Respimat SMI 5 μg appears to be efficacious and well tolerated when used in a selected COPD population. However, it should be used with caution in patients with COPD who have the following: a history of recent myocardial infarction (within 6 months); unstable/life-threatening cardiac arrhythmia (requiring intervention within 12 months), hospitalization for cardiac failure (within 12 months); moderate-to-severe renal impairment; other concurrent pulmonary pathology, including but not limited to interstitial lung disease, bronchiectasis, asthma, CF, or pulmonary thromboembolism because of the design of the trials, which excludes patients with other concurrent lung diseases.46
Tiotropium Respimat SMI in CF
Efficacy
Tiotropium delivered by the Respimat SMI has been trialed in patients with stable CF bronchiectasis, although to date its routine use is not supported by existing Phase III trials. Although spirometric improvements have been noted in both children and adults,47,48 these data have not been corroborated in larger Phase III trials, nor have any differences translated in clinically relevant outcomes.49 Boehringer Ingelheim, in its prescribing information for UK prescribers, does not recommend the use of tiotropium Respimat SMI in patients with CF.35
Safety and tolerability
There were no reported increase in adverse events across all three studies, and all of the studies demonstrated good tolerability of tiotropium Respimat SM, with low withdrawal rates. Adverse events were generally minor, with the most common being cough, pyrexia, and nasopharyngitis.47 However, Ratjen et al49 found a numerical, although not statistically significant, increase in the risk of infective exacerbations of CF in the tiotropium Respimat SMI group when compared to placebo. To the best of our knowledge, no studies have been performed to ascertain whether there is a similar signal with tiotropium HandiHaler DPI. There are no studies comparing the efficacy or safety of tiotropium Respimat SMI and HandiHaler DPI in patients with CF at the time of writing. Therefore, it is impossible to distinguish whether these observations might be related to the use of tiotropium itself, or the underlying delivery mechanism. However, it is possible the anticholinergic properties of tiotropium result in dehydration of airway secretions. Many of the inhaled treatments used in CF, which have been demonstrated to reduce exacerbations, work as airway hydrators, increasing the volume and composition of the airway surface liquid and improving sputum viscosity and airway clearance. Therefore, it is possible that the molecule itself may result in adverse outcomes such as exacerbations.
Patient selection
At present, the use of tiotropium via the Respimat SMI for patients with CF is not supported, in particular due to concerns around a possible increased risk of exacerbations of CF bronchiectasis. Although it is possible that this intervention might result in small spirometric improvements for some patients, given the relative paucity of robust data demonstrating clinical efficacy, combined with the aforementioned concerns around safety, Respimat SMI should not be recommended for patients with CF.
Conclusion
Tiotropium Respimat SMI appears to be efficacious, safe, and well tolerated in patients with asthma and COPD. Dose escalation beyond 5 μg has not been shown to improve spirometric or clinical outcomes, and in asthma, it has been associated with a small increase in adverse events. Although bioequivalence has not been convincingly demonstrated between Respimat SMI and HandiHaler DPI, clinical and spirometric outcomes appear comparable, at least for patients with COPD. There is no robust evidence that possible improvements in drug delivery result in improved clinical outcomes, and therefore selection of either the HandiHaler DPI or Respimat SMI should be made on a case-by-case basis, taking into account patient preferences, cost, individual patient tolerability, and potentially, the degree of impairment in lung function.
Most of the adverse effects of tiotropium Respimat SMI are consistent with its anticholinergic properties, for example, dry mouth and constipation. Importantly, early data suggesting an increase in mortality with Respimat SMI in COPD have not been corroborated in subsequent, large, well-conducted, head-to-head randomized controlled trials, and overall its use appears to be safe in COPD, where important contraindications have been excluded. Given the rigorous exclusion criteria from these clinical trials, tiotropium, delivered either via HandiHaler DPI or Respimat SMI, should be used with caution in patients with narrow-angle glaucoma, prostatic hyperplasia, bladder neck obstruction, severe renal impairment, and, particularly for Respimat SMI, those with cardiac rhythm disorders or recent myocardial infarction.35
In patients with CF, the use of tiotropium Respimat SMI may increase the risk of infective exacerbations, and therefore its use for this indication cannot be supported at present.
In summary, tiotropium delivered via the Respimat SMI device has been shown to have similar efficacy and safety profile as the older HandiHaler DPI device in patients with asthma and COPD. Trials comparing the two devices failed to demonstrate superiority of one over the other; however, it remains a viable alternative to the traditional HandiHaler DPI.
Acknowledgments
The authors are grateful to Ms Wanda Pomeroy and the other librarians of Lyell McEwin Hospital, South Australia, for their assistance in performing the literature search.
Disclosure
The authors report no conflicts of interest in this work.
References
McKeage K. Tiotropium Respimat®: a review of its use in asthma poorly controlled with inhaled corticosteroids and long-acting β2-adrenergic agonists. Drugs. 2015;75(7):809–816. | ||
FDA. Drug Approval Package: Spiriva HandiHaler (Tiotropium Bromide) Inhalation Powder. US Food and Drug Administration: Silver Spring, MD; 2004. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/nda/2004/21-395_Spiriva.cfm. Accessed November 28, 2015. | ||
Niewoehner DE, Rice K, Cote C, et al. Prevention of exacerbations of chronic obstructive pulmonary disease with tiotropium, a once-daily inhaled anticholinergic bronchodilator: a randomized trial. Ann Intern Med. 2005;143(5):317–326. | ||
Tashkin DP, Celli B, Senn S, et al. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med. 2008;359(15):1543–1554. | ||
Cheyne L, Irvin-Sellers MJ, White J. Tiotropium versus ipratropium bromide for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2013;(9):CD009552. | ||
Karner C, Chong J, Poole P. Tiotropium versus placebo for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014;(7):CD009285. | ||
Kerstjens HA, Engel M, Dahl R, et al. Tiotropium in asthma poorly controlled with standard combination therapy. N Engl J Med. 2012;367(13):1198–1207. | ||
Befekadu E, Onofrei C, Colice GL. Tiotropium in asthma: a systematic review. J Asthma Allergy. 2014;7:11–21. | ||
Lee SW, Kim HJ, Yoo KH, et al. Long-acting anticholinergic agents in patients with uncontrolled asthma: a systematic review and meta-analysis. Int J Tuberc Lung Dis. 2014;18(12):1421–1430. | ||
Boehringer Ingelheim Pharmaceuticals I. How To Use Your HandiHaler. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals; 2014:9. Available from: https://www.spiriva.com/pdf/SPIRIVA_HandiHaler_Instructions.pdf | ||
Dalby RN, Eicher J, Zierenberg B. Development of Respimat(®) Soft Mist Inhaler and its clinical utility in respiratory disorders. Med Devices (Auckl). 2011;4:145–155. | ||
Boehringer Ingelheim Pharmaceuticals I. Summary of Product Characteristics, Labelling and Package Leaflet. 2015. Available from: http://products.boehringer-ingelheim.com/products/prescription_medicines/respiratory/copd/spiolto/public/assets/spiriva_respimat_spc_published.pdf. Accessed December 28, 2015. | ||
Anderson P. Use of Respimat Soft Mist inhaler in COPD patients. Int J Chron Obstruct Pulmon Dis. 2006;1(3):251–259. | ||
Newman SP, Brown J, Steed KP, Reader SJ, Kladders H. Lung deposition of fenoterol and flunisolide delivered using a novel device for inhaled medicines: comparison of RESPIMAT with conventional metered-dose inhalers with and without spacer devices. CHEST J. 1998;113(4):957–963. | ||
Steed KP, Towse LJ, Freund B, Newman SP. Lung and oropharyngeal depositions of fenoterol hydrobromide delivered from the prototype III hand-held multidose Respimat nebuliser1. Eur J Pharm Sci. 1997;5(2): 55–61. | ||
Newman SP, Steed KP, Reader SJ, Hooper G, Zierenberg B. Efficient delivery to the lungs of flunisolide aerosol from a new portable hand-held multidose nebulizer. J Pharm Sci. 1996;85(9):960–964. | ||
Spiriva® MIMS Full [prescribing information]. Ingelheim am Rhein, Germany: Boehringer Ingelheim Pharmaceuticals; 2015. Available from: http://www.mimsonline.com.au/Search/FullPI.aspx?ModuleName=Product%20Info&searchKeyword=tiotropium&PreviousPage=~/Search/QuickSearch.aspx&SearchType=&ID=65230001_2. Accessed February 28, 2016. | ||
van Noord JA, Cornelissen PJ, Aumann JL, Platz J, Mueller A, Fogarty C. The efficacy of tiotropium administered via Respimat Soft Mist Inhaler or HandiHaler in COPD patients. Respir Med. 2009;103(1):22–29. | ||
Ichinose M, Fujimoto T, Fukuchi Y. Tiotropium 5 μg via Respimat and 18 μg via HandiHaler; efficacy and safety in Japanese COPD patients. Respir Med. 2010;104(2):228–236. | ||
Singh S, Loke YK, Enright PL, Furberg CD. Mortality associated with tiotropium mist inhaler in patients with chronic obstructive pulmonary disease: systematic review and meta-analysis of randomised controlled trials. BMJ. 2011;342:d3215. | ||
Hohlfeld J, Sharma A, Van Noord J, et al. Pharmacokinetics and pharmacodynamics of tiotropium solution and tiotropium powder in chronic obstructive pulmonary disease. J Clin Pharmacol. 2014;54(4):405–414. | ||
Rodrigo GJ, Castro-Rodríguez JA. What is the role of tiotropium in asthma? a systematic review with meta-analysis. Chest. 2015;147(2):388–396. | ||
Kerstjens HA, Disse B, Schröder-Babo W, et al. Tiotropium improves lung function in patients with severe uncontrolled asthma: a randomized controlled trial. J Allergy Clin Immunol. 2011;128(2):308–314. | ||
Vogelberg C, Engel M, Moroni-Zentgraf P, et al. Tiotropium in asthmatic adolescents symptomatic despite inhaled corticosteroids: a randomised dose-ranging study. Respir Med. 2014;108(9):1268–1276. | ||
Vogelberg C, Moroni-Zentgraf P, Leonaviciute-Klimantaviciene M, et al. A randomised dose-ranging study of tiotropium Respimat® in children with symptomatic asthma despite inhaled corticosteroids. Respir Res. 2015;16(1):20. | ||
Kerstjens H, Engel M, Moroni-Zentgraf P, Schmidt H, Bateman E. Tiotropium added to inhaled corticosteroids and long-acting beta (2)-agonists reduces episodes of asthma worsening, irrespective of selected patient baseline characteristics. Allergy. 2013;68:41. | ||
Dahl R, Paggiaro P, Engel M, et al. Once-daily tiotropium improves lung function and reduces risk of asthma exacerbation/worsening in patients with symptomatic asthma, regardless of allergic status. Allergy. 2013;68:40–41. | ||
Bateman ED, Kornmann O, Schmidt P, Pivovarova A, Engel M, Fabbri LM. Tiotropium is noninferior to salmeterol in maintaining improved lung function in B16-Arg/Arg patients with asthma. J Allergy Clin Immunol. 2011;128(2):315–322. | ||
Beeh KM, Moroni-Zentgraf P, Ablinger O, et al. Tiotropium Respimat® in asthma: a double-blind, randomised, dose-ranging study in adult patients with moderate asthma. Respir Res. 2014;15(1):61. | ||
Wolfgang TM-ZP, Cornelissen P, Unseld A, Pizzichini E, Buhl R. Once-daily tiotropium Respimat® 5 μg is an efficacious 24-h bronchodilator in adults with symptomatic asthma. Respir Med. 2014;109:329–338. | ||
Dusser D, Buhl R, Castro M, et al. Once-daily tiotropium Respimat® add-on to at least ICS in adult patients with symptomatic asthma: pooled safety analysis. Thorax. 2014;70:151–152. | ||
Ohta K, Ichinose M, Tohda Y, et al. Long-term once-daily tiotropium Respimat® is well tolerated and maintains efficacy over 52 weeks in patients with symptomatic asthma in Japan: a randomised, placebo-controlled study. PLoS One. 2015;10(4):e0124109. | ||
Global Initiative for Asthma (GINA) Teaching Slide Set, 2015 Update (Slide 63). Global Initiative for Asthma. Available from: medicina-ucr.com/quinto/wpcontent/uploads/2015/08/GINA_SlideSet_2015.ppt. Accessed January 29, 2016. | ||
Chung KF, Wenzel SE, Brozek JL, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43(2):343–373. | ||
Spiriva Respimat® (tiotropium bromide) 2.5 micrograms solution for inhalation [prescribing information] for UK prescribers. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals; 2012;17. Available from: http://docs.boehringer-ingelheim.com/Prescribing%20Information/PIs/Spiriva%20Respimat/spirivarespimat.pdf. Accessed Feberuary 29, 2016. | ||
Bel EH. Tiotropium for asthma – promise and caution. N Engl J Med. 2012;367(13):1257–1259. | ||
Yohannes AM, Connolly MJ, Hanania NA. Ten years of tiotropium: clinical impact and patient perspectives. Int J Chron Obstruct Pulmon Dis. 2013;8:117–125. | ||
Bateman E, Singh D, Smith D, et al. Efficacy and safety of tiotropium Respimat® SMI in COPD in two 1-year randomized studies. Int J Chron Obstruct Pulmon Dis. 2010;5:197. | ||
Wise RA, Anzueto A, Cotton D, et al. Tiotropium Respimat inhaler and the risk of death in COPD. N Engl J Med. 2013;369(16):1491–1501. | ||
Tang Y, Massey D, Zhong N. Evaluation of the efficacy and safety of tiotropium bromide (5 μg) inhaled via Respimat in Chinese patients with chronic obstructive pulmonary disease. Chin Med J (Engl). 2012;126(19):3603–3607. | ||
Verhamme KM, Afonso A, Romio S, Stricker BC, Brusselle GG, Sturkenboom MC. Use of tiotropium Respimat Soft Mist Inhaler versus HandiHaler and mortality in patients with COPD. Eur Respir J. 2013;42(3):606–615. | ||
Verhamme KM, van Blijderveen N, Sturkenboom MC. Tiotropium and the risk of death in COPD. N Engl J Med. 2014;370(5):481–482. | ||
Trotta F, Da Cas R, Rajevic M, Rossi M, Traversa G. Risk factors influencing the prescription of tiotropium Respimat formulation: a population-based cohort study. BMJ Open. 2015;5(5):e006619. | ||
van der Palen J, Ginko T, Kroker A, et al. Preference, satisfaction and errors with two dry powder inhalers in patients with COPD. Expert Opin Drug Deliv. 2013;10(8):1023–1031. | ||
Criner GJ, Bourbeau J, Diekemper RL, et al. Prevention of acute exacerbations of COPD: American College of Chest Physicians and Canadian Thoracic Society Guideline. Chest J. 2015;147(4):894–942. | ||
Mathioudakis AG, Chatzimavridou-Grigoriadou V, Evangelopoulou E, Mathioudakis GA, Siafakas NM. Comparative mortality risk of tiotropium administered via handihaler or respimat in COPD patients: are they equivalent? Pulm Pharmacol Ther. 2014;28(2):91–97. | ||
Bradley JM, Koker P, Deng Q, et al. Testing two different doses of tiotropium Respimat® in cystic fibrosis: phase 2 randomized trial results. PLoS One. 2014;9(9):e106195. | ||
Konstan MW, Sharma A, Moroni-Zentgraf P, Wang F, Koker P. Safety, tolerability, and plasma exposure of Tiotropium Respimat® in children and adults with cystic fibrosis. J Aerosol Med Pulm Drug Deliv. 2015;28(2):137–144. | ||
Ratjen F, Koker P, Geller DE, et al. Tiotropium Respimat in cystic fibrosis: phase 3 and pooled phase 2/3 randomized trials. J Cyst Fibros. 2015;14(5):608–614. | ||
Fardon T, Haggart K, Lee DK, Lipworth BJ. A proof of concept study to evaluate stepping down the dose of fluticasone in combination with salmeterol and tiotropium in severe persistent asthma. Respir Med. 2007;101(6):1218–1228. | ||
Peters SP, Kunselman SJ, Icitovic N, et al. Tiotropium bromide step-up therapy for adults with uncontrolled asthma. N Engl J Med. 2010;363(18):1715–1726. | ||
Kerstjens HA, Casale TB, Bleecker ER, et al. Tiotropium or salmeterol as add-on therapy to inhaled corticosteroids for patients with moderate symptomatic asthma: two replicate, double-blind, placebo-controlled, parallel-group, active-comparator, randomised trials. Lancet Respir Med. 2015;3(5):367–376. | ||
Boehringer Ingelheim. Evaluation of Tiotropium 2.5 and 5 mcg Once Daily Delivered Via the Respimat® Inhaler Compared to Placebo and Salmeterol HydroFluoroAlkane (HFA) Metered Dose Inhaler (MDI) (50 mcg Twice Daily) in Patient With Moderate Persistent Asthma I. Available from: https://clinicaltrials.gov/ct2/show/NCT01172808?term=NCT01172808&rank=1. NLM identifier: NCT01172808. Accessed February 28, 2016. | ||
Paggiaro P, Halpin DM, Buhl R, et al. The effect of tiotropium in symptomatic asthma despite low- to medium-dose inhaled corticosteroids: a randomized controlled trial. J Allergy Clin Immunol Pract. 2016;4(1):104–113.e102. | ||
Boehringer Ingelheim. Efficacy and Safety of 2 Doses of Tiotropium Via Respimat Compared to Placebo in Adolescents With Moderate Persistent Asthma. Available from: https://clinicaltrials.gov/ct2/show/NCT01257230?term=NCT+01257230&rank=1. NLM identifier: NCT01257230. Accessed February 28, 2016. | ||
Halpin DM, Dahl R, Hallmann C, Mueller A, Tashkin D. Tiotropium HandiHaler® and Respimat® in COPD: a pooled safety analysis. Int J Chron Obstruct Pulmon Dis. 2015;10:239. |
Supplementary materials
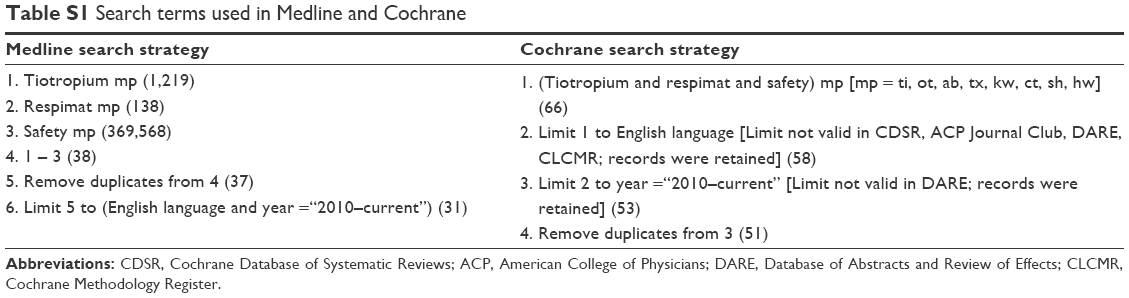 | Table S1 Search terms used in Medline and Cochrane |
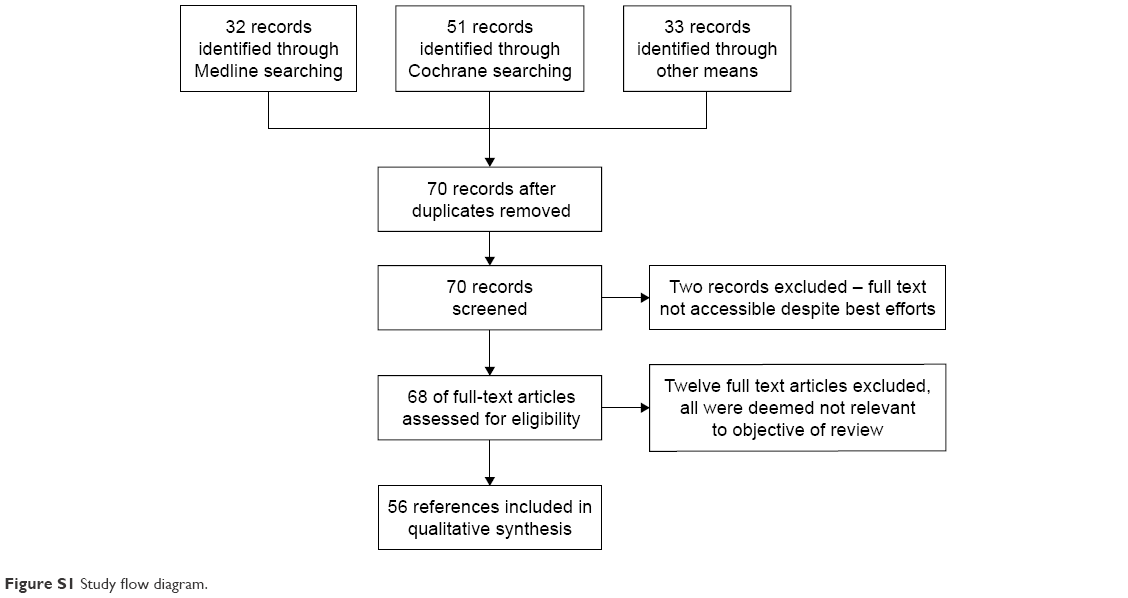 | Figure S1 Study flow diagram. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.