Back to Journals » Clinical and Experimental Gastroenterology » Volume 7
Long-term safety and efficacy of budesonide in the treatment of ulcerative colitis
Authors Iborra M, Álvarez-Sotomayor D, Nos P
Received 4 June 2013
Accepted for publication 5 August 2013
Published 5 February 2014 Volume 2014:7 Pages 39—46
DOI https://doi.org/10.2147/CEG.S34715
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Marisa Iborra,1 Diego Álvarez-Sotomayor,2 Pilar Nos1
1Gastroenterology Unit, Department of Digestive Disease, Centro de investigación biomédica en Red de Enfermedades Hepáticas y Digestivas (CIBEREHD), La Fe University and Polytechnic Hospital, Valencia, Spain; 2Gastroenterology Unit, Department of Digestive Disease, La Fe University and Polytechnic Hospital, Valencia, Spain
Abstract: Ulcerative colitis (UC) is a chronic, relapsing, and remitting inflammatory disease involving the large intestine (colon). Treatment seeks to break recurrent inflammation episodes by inducing and maintaining remission. Historically, oral systemic corticosteroids played an important role in inducing remission of this chronic disease; however, their long-term use is limited and can lead to adverse events. Budesonide is a synthetic steroid with potent local anti-inflammatory effects and low systemic bioavailability due to high first-pass hepatic metabolism. Several studies have demonstrated oral budesonide's usefulness in treating active mild to moderate ileocecal Crohn's disease and microscopic colitis and in an enema formulation for left sided UC. However, there is limited information regarding oral budesonide's efficacy in UC. A novel oral budesonide formulation using a multimatrix system (budesonide-MMX) to extend drug release throughout the colon has been developed recently and seems to be an effective treatment in active left sided UC patients. This article summarizes budesonide's long-term safety and efficacy in treating UC.
Keywords: budesonide, ulcerative colitis, Crohn's disease, safety
Introduction
Inflammatory bowel disease (IBD), including Crohn’s disease (CD) and ulcerative colitis (UC), is characterized by a relapsing and remitting course. Aminosalicylates (mesalazine), glucocorticoids, and biological therapies (anti-tumor necrosis factor-alpha [TNF-α] therapy) are the drugs used for inducing remission during acute disease flares, and aminosalicylates, immunomodulators, and anti-TNF-α therapy are also used to maintain IBD in remission.1 Currently, traditional corticosteroids are used more frequently to induce clinical remission of both CD and UC, despite their inability to achieve mucosal healing as well as the multiple adverse effects (AE) which limit their long-term use. A second generation of corticosteroids has been developed to reduce severe side effects and improve safety. Oral budesonide and beclomethasone are two types of locally active oral steroids used in clinical practice.2
Beclomethasone was initially used in enema form in UC treatment and has recently been formulated as an oral enteric coated compound which is released in the distal small bowel and throughout the colon.2 Budesonide is a synthetic steroid with high topical glucocorticoid activity and low systemic bioavailability due to its high first-pass hepatic metabolism.2 In this review, we analyze budesonide’s long-term safety and efficacy in treating gastrointestinal diseases and the drug’s role with regard to IBD patients, with an emphasis on UC patients.
Budesonide, a locally active oral drug, has an improved safety profile and constitutes an important alternative to the classic steroids in frequently encountered gastrointestinal conditions such as CD, microscopic colitis, and eosinophilic colitis.2,3 Several reviews have evaluated budesonide’s efficacy in treating inflammatory intestinal diseases.2–4 The European Crohn’s and Colitis Organization recommends using budesonide to induce remission in mild to moderate active ileocecal CD.5 Budesonide (9 mg per day) was the preferred treatment because it was associated with fewer side effects and demonstrated usefulness in replacing conventional systemic glucocorticoids in CD patients. However, budesonide’s efficacy in maintaining remission is controversial and published studies conclude that although this drug may delay relapse after medically induced remission, it is not effective at maintaining remission for 12 months.3,5–7
The efficacy of oral budesonide for active UC is controversial and it has been demonstrated to be less likely to induce clinical remission than oral mesalazine, while having no benefit over the placebo.8 Therefore, budesonide in its current formulation is not recommended in routine clinical practice. A novel budesonide multimatrix (MMX) preparation has recently completed phase III trials and the preliminary data suggests significant benefit over placebo for the induction of remission in UC.1,2,9
Budesonide’s efficacy in treating microscopic colitis in both histological forms, collagenous colitis, and lymphocytic colitis, has been demonstrated in several reviews2,3 and in the European Consensus.10 There has been a recent publication demonstrating budesonide’s higher response rate and lower risk of recurrence when compared to prednisone in patients with microscopic colitis.11
Pharmacology
Formulations
Budesonide is a potent glucocorticoid with a high local anti-inflammatory effect and low systemic bioavailability. The first trial published about the use of oral budesonide in CD patients was performed by Lofberg et al in 1993.12 Budesonide is available in three oral dose forms (Table 1): a controlled ileal release form, a pH-dependent release formulation, and a MMX formulation.8,13
Both controlled ileal and pH-dependent release use enteric coated (Eudragit®, Evonik Industries, Essen, Germany) pellets and have been approved for treating CD located in the terminal ileum and/or ascending colon. The controlled ileal release form (Entocort®, AstraZeneca, London, UK; Entocir®, Sofar SpA, Milan, Italy) contains L 100-55 Eudragit® granules, which are resistant to gastric acid degradation and dissolve at pH values above 5.5. A pH-dependent release formulation (Budenofalk®, Dr Falk Pharma, Freiburg, Germany) is an enteric coated locally acting glucocorticoid preparation whose pH- and time-dependent coating enables its release into the ileum and ascending colon. This oral formulation consists of a capsule containing L, S, LS, and RS Eudragit® granules that dissolve at pH values above 6.4.13,14
 | Table 1 Characteristics of the three oral budesonide formulations |
A new controlled release system, Budesonide MMX® (Cosmo Pharmaceuticals SpA, Lainate, Italy), has recently been developed and researched.15,16 MMX technology comprises hydrophilic and lipophilic excipients, both of which are enclosed within a gastroresistant and pH-dependent coating. This new once a day oral budesonide formulation is released when pH rises above 7 and consequently achieves homogeneous distribution throughout the ascending, transverse, and descending colon allowing it to treat UC more specifically.15–17 Budesonide MMX® is a promising new system that appears suitable for targeted colonic drug delivery and has been shown to increase the response and remission rates in patients with active left sided UC.9,18
Pharmacodynamics and metabolism
Budesonide is a potent glucocorticoid with high affinity for the glucocorticoid receptor, greater anti-inflammatory potency, and better solubility. Budesonide produces an anti-inflammatory effect through downregulation of cytokines with an important role in the inflammation pathways, including nuclear factor-KappaB, TNF-α, and the interleukins 1 and 6.8,19 Budesonide exerts its potent local effect because it has approximately 15 times higher binding affinity to the glucocorticoid receptor than prednisolone and is also more effective than triamcinolone.20 Following oral administration, the drug is absorbed from the intestinal lumen via the apical enterocyte drug transporting P-glycoprotein. The reason for budesonide’s minimal systemic absorption lies in the high first-pass effect (over 90%) which is carried out by hepatic cytochrome P450 (CYP3A4 and CYP3A5) enzymes. Once metabolized, it is transforms into two metabolites, 6β-hydroxybudesonide and 16α-hydroxyprednisolone, with negligible glucocorticoid activity (less than 1%) which does not contribute to budesonide’s therapeutic action.3,13,20
Side effects
Current UC treatments for an acute flare include aminosalicylates, glucocorticoids, and biological therapies. First line therapy for mild to moderately active UC is mesalazine; corticosteroids and anti-TNF-α therapies are administered in refractory disease. However, anti-TNF-α therapies are very expensive, their use implies a risk of latent infection reactivation, and the serological status (hepatitis B virus and tuberculosis) must be known. For this reason, corticosteroids are frequently the drug of choice in this situation.1 Conventional corticosteroids are associated with several AE such as hypertension, diabetes, osteoporosis, cataracts, and glaucoma. In contrast to systemic corticosteroids, budesonide has reduced systemic AE due to location specific delivery and a high first-pass metabolism with limited systemic bioavailability. However, it has been demonstrated that it can generate an impact on organs and metabolic activities of the body.3 The most common AE (>1/100 – <1/10 cases) associated with budesonide are Cushingoid features or hypokalaemia due to effects on the endocrine organs, psychiatric disorders, blurred vision, palpitations, dyspeptic symptoms, skin reactions such as urticaria or exanthema, muscle cramps, and menstrual disorders.3 Suppression of the hypothalamic-pituitary-adrenal axis is common and can be reversed using conventional corticosteroids, but not with newer topically acting corticosteroids.21 Effects on the nervous system are not common (>1/1,000 – <1/100), although in certain cases tremors may appear.3 Other rare effects include reduced growth speed and anaphylactic reactions, which occur in <1/10,000 cases.3
A study with data from five 1-year, double-blind, placebo-controlled trials in more than 200 CD patients showed that the highest incidence rates of AE were gastrointestinal and endocrine system related in both groups (budesonide 6 mg/day versus placebo).22 Incidence rates were similar in both groups; however, the budesonide group had a higher incidence of endocrine disorders than the placebo group (P = 0.0042) caused by a higher amount of cutaneous corticosteroid symptoms (P = 0.0036) in the budesonide group, without significant differences in individual symptoms. The budesonide group demonstrated a lower percentage of patients with normal adrenal function at 13 weeks (in three of the five analyzed trials) than placebo groups; however, at 52 weeks (in two of the five analyzed trials) this percentage was dissimilar among the groups. Clinically important or serious AE associated with systemic corticosteroids (sepsis, cataracts, or adrenal insufficiency) were very infrequent and similar between groups.22 D’Haens et al investigated the influence of budesonide (9 mg for 10 weeks) compared to methylprednisolone (32 mg for 3 weeks with subsequent tapering) on bone turnover and they demonstrated that budesonide does not impair osteoblast activity.23 Furthermore, while budesonide treatment during the follow-up period has not demonstrated a benefit in fracture reduction, it seems that corticosteroid naïve patients treated with budesonide showed better preservation of bone mass compared to patients treated with prednisolone.24
Safety in children and pregnancy
There is limited data regarding safety and efficacy of oral budesonide during pregnancy in IBD patients. Beaulieu et al25 reviewed their database and identified eight CD patients who received oral budesonide treatment (6 mg/day in six patients and 9 mg/day in two patients) during pregnancy. In this retrospective study, there were no cases of severe maternal side effects (adrenal suppression, glucose intolerance, ocular side effects, and hypertension) and there did not appear to be an increased risk of major congenital abnormalities.25 Data from allergy rhinitis and asthma patients have also demonstrated that inhaled budesonide is not incriminated as a teratogen in humans and can be used by pregnant women.26,27
A serious complication of corticosteroids in children is growth retardation and reduced final height. There are no studies in UC patients evaluating the use of budesonide in children. However, it seems that systemic exposure, systemic availability, and cortisol suppression are similar in children and adults with active CD treated with oral budesonide.28 Data from child CD patients have demonstrated the safety and efficacy of budesonide compared to systemic glucocorticosteroids.29–31 Although budesonide has demonstrated fewer side effects and lower adrenal suppression, prednisolone was more effective for inducing remission.31 Pediatric patients treated with budesonide had significantly fewer side effects than patients treated with prednisone with similar rates of clinical remission.29
Budesonide in UC
Efficacy for inducing remission
There are limited data about the role of budesonide in UC treatment (Table 2). A review for The Cochrane Collaboration explored all studies and abstracts of gastroenterology scientific meetings that analyzed the safety and efficacy of oral budesonide for the induction of remission of UC.8 Only three comparative studies and randomized trials met the inclusion criteria.8 The authors concluded that there is no evidence to recommend oral budesonide for inducing remission in active UC because it was no better than placebo and was inferior to mesalamine.8 The first study was a small double-blind controlled trial comparing 10 mg of budesonide per day and 40 mg of prednisolone per day. This pilot study did not show differences in endoscopic remission in active UC patients; however, suppression of plasma cortisol levels was less common with budesonide treatment.32
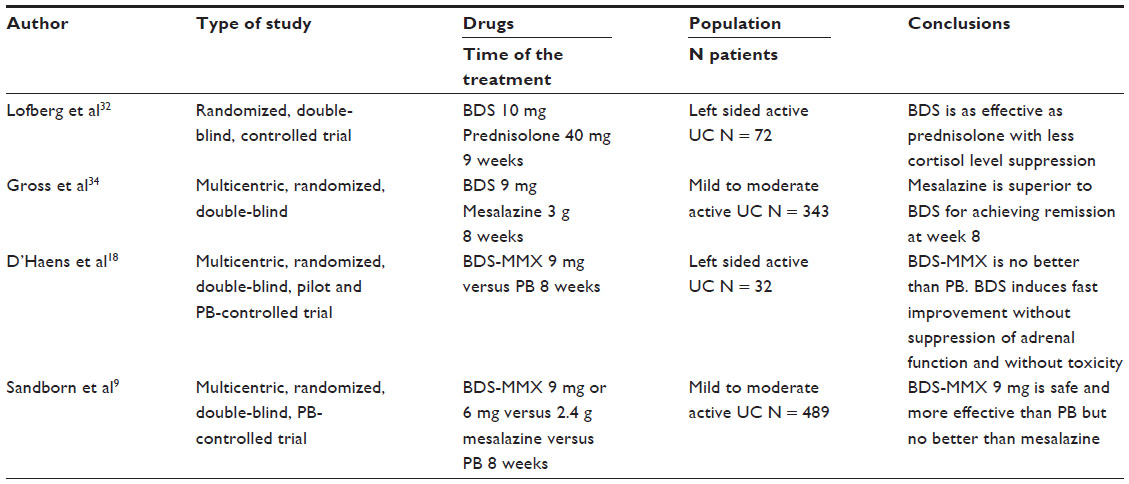 | Table 2 Published studies comparing budesonide’s safety and efficacy with other drugs as maintenance treatment for ulcerative colitis patients |
The second included study was performed by Gross et al in 2009 and has been published in abstract form.33 Researchers compared 9 mg of budesonide (in a pH-dependent release formulation, Budenofalk®) with 3 g of mesalazine (Salofalk®; Dr Falk Pharma, Freiburg, Germany). This mesalazine is an aminosalicylate formulation which combines both delayed- and extended-release mechanisms. Currently, mesalazine is the first line treatment in mild to moderately active UC disease, whereas systemic corticosteroids are appropriate if symptoms of active colitis do not respond to mesalazine (refractory disease) or in cases of high disease activity.1 These preliminary results demonstrated that oral mesalazine was significantly better at inducing clinical remission than budesonide after 8 weeks of therapy (relative risk 0.72, 95% confidence interval 0.57 to 0.91). More recently, Gross et al34 have published definitive results for 343 patients with mild to moderate active UC in which 177 were treated with budesonide 3 mg capsules 3 times per day (Budenofalk® 3 mg capsules) and 166 with mesalazine 1,000 mg granules 3 times per day (Salofalk® 1,000 mg granules). Clinical remission at week 8 was lower in the budesonide group versus the mesalazine group (70/177 [39.5%] versus 91/166 [54.8%], respectively). The Clinical Activity Index (CAI) and Endoscopic Index (EI) mean scores decreased from the baseline in both groups but the mean reduction in both scores at the concluding visit was higher in the mesalazine group. Similar median time to first resolution of symptoms and range of AE was observed in both mesalazine (11 days and 25.3% AE) and budesonide (14 days and 26.6% AE) groups. In conclusion, once daily 3 g mesalazine granules are superior to 9 mg oral budesonide for achieving remission in mild to moderate UC. However, budesonide induced clinical remission in about 40% of the patients with rapid resolution of symptoms (14 days) and endoscopic remission in about 50% of patients.34
The last study included in the Cochrane review was the first study to evaluate the new oral budesonide-MMX® 9 mg formulation’s safety and efficacy in inducing clinical remission at 4 weeks in active left sided UC patients.18 This randomized pilot study compared budesonide with a placebo for 4 weeks and after all patients received budesonide for 4 more weeks. Eighteen patients were included in each group and after 4 weeks of treatment, eight patients (47.06%) achieved a CAI reduction in the budesonide group compared with five subjects (33.33%) in the placebo group. Clinical improvement was also significantly faster in the budesonide-MMX® group than in the placebo group without suppression of adrenocortical functions (normal pituitary–adrenal axis function in 40% of budesonide versus 60% of placebo group) and without significant side effects. However, the mucosal normalization at 4 and 8 weeks measured by EI and histological remission were not parallel to the clinical symptoms and there were no statistically significant differences among the groups. The authors concluded that although the sample was small, budesonide-MMX® 9 mg might become an effective treatment in active left sided UC patients without suppressing adrenocortical functions and without significant toxicity.18
Sandborn et al9 have recently corroborated budesonide-MMX®’s efficacy. This double-blind, placebo-controlled trial evaluated budesonide-MMX®’s efficacy in inducing remission in patients with active mild to moderate UC.9 Almost 500 patients were randomized to receive budesonide-MMX (9 mg or 6 mg) or mesalazine 2.4 g and placebo for 8 weeks and remission rates were 17.9%, 13.2%, and 12.1%, respectively, compared with 7.4% for the placebo. Clinical and endoscopic improvement rates at week 8 among patients given budesonide-MMX® were 33.3% and 28.5% in the 9 mg group and 30.6% and 28.9% in the 6 mg group, respectively; in the mesalazine group, rates were 33.9% and 25.0%, respectively, and 24.8% and 16.5% for the placebo group. Clinical and endoscopic remission in the budesonide-MMX® 9 mg group was significantly higher than the placebo group at week 8. AEs occurred with similar frequencies among groups; however, the percentage of severe AEs was greatest in the placebo group (12.4% compared with 6.3%, 9.5%, and 5.5% in the budesonide 9 mg, budesonide 6 mg, and mesalazine group respectively). The authors concluded that budesonide-MMX® 9 mg was safe and more effective than the placebo in inducing remission in active mild to moderate UC patients.9
The pilot studies have demonstrated that budesonide-MMX is better than the placebo, but is less effective than mesalazine in active mild to moderate UC patients.9,18 Further studies are required to discover new drugs to improve the treatment and to avoid the use of immunosuppressive drugs in these patients, who could benefit from less aggressive treatments.
The available literature provides three independent and noncomparative studies about the use of budesonide in UC treatment. Keller et al published a pilot study to evaluate oral budesonide’s efficacy in a pH-modified release formulation in patients previously treated with conventional corticosteroids.35 In this study, 14 patients with steroid-dependent UC in the reduction phase of conventional corticosteroids following a severe flare up were treated with budesonide 9 mg (in three doses) for 6 months. Eleven patients achieved clinical remission and corticosteroid treatment was able to be withdrawn, and three patients experienced relapse and needed further corticosteroid treatment. In the relapse group, the dose of systemic corticosteroids and the CAI was significantly higher before starting budesonide than in the remission group. In conclusion, treatment with 9 mg of budesonide per day in steroid-dependent UC patients seems well tolerated, effective, and capable of reducing systemic corticosteroids use.35
An open phase II clinical trial evaluated the pharmacokinetics, the pharmacodynamics, and the safety of two dosage regimens of pH-dependent release budesonide capsules (9 mg once daily and 3 mg three times daily) in 15 patients with active distal UC for 8 weeks.36 Peak concentrations, systemic availability, and cortisol suppression were more pronounced in the 9 mg once per day group than in the 3 mg three times per day group. The pharmacodynamics profile (lymphocyte and neutrophil count) and the mucosal budesonide levels were similar in both groups. The response rates after treatment for 8 weeks were higher in the 9 mg once per day group than in the 3 mg three times per day group (71% versus 38%) and the EI improved significantly in both groups. This study suggests that budesonide 9 mg once per day is effective in distal colitis with fewer side effects.36
Finally, there is also a study seeking to determine the benefit of budesonide in clinical practice and identify any Food and Drug Administration unapproved uses that may warrant further study.37 In total, 225 patients were categorized by indication for therapy in three groups: ileocolonic CD (group one), CD elsewhere (group two), and other conditions (group three) including patients with microscopic colitis, pouchitis, UC, and celiac disease. A favorable outcome occurred in 61% of group one patients but in only 24% of patients in group two. In group three, only microscopic colitis patients and pouchitis patients experienced >50% response rates (77% and 60%, respectively). Although budesonide’s benefit in UC was not confirmed, small sample size (only 12 UC patients were included) cannot be excluded as being responsible for this.37
Budesonide has shown efficacy in inducing remission in mild to moderate active UC patients but this finding must be confirmed in controlled trials that compare effective induction doses of mesalazine.
Efficacy in maintaining remission
There are currently no published studies examining oral budesonide’s efficacy and safety in maintaining UC remission. To this end, there are published results in abstract form.38 This drug’s role as maintenance treatment in a placebo-controlled trial was evaluated based on the results of budesonide-MMX® in the Sandborn et al9 study. The efficacy of budesonide-MMX® 6 mg for up to 12 months in maintaining clinical remission was evaluated in 122 patients who were in clinical and endoscopic remission after two phase III studies or an open label study.9 Budesonide-MMX® 6 mg was not significantly different from placebo in maintaining clinical remission but the probability of clinical relapse at 12 months was reduced and the median time until clinical relapse was longer in the budesonide-MMX® group when compared to the placebo group. The AEs were similar between treatment groups (21.0%) and placebo (21.3%). They concluded that extended use of budesonide-MMX® 6 mg may be an option in long-term therapy for maintaining remission in UC patients.38 Budesonide’s role as maintenance therapy in UC patients is still very limited and more studies comparing it to mesalazine are required.
Budesonide in pouchitis
After colectomy, greater numbers of UC patients will develop pouchitis, a frequent complication following total proctocolectomy with ileal pouch-anal anastomosis. In addition, more than 15% will develop a chronic course that can be resistant to antibiotic therapy and that may lead to surgical pouch excision. Further therapeutic options are therefore needed and oral budesonide may be an alternative. There are two studies39,40 that evaluated oral budesonide efficacy in inducing remission and improving quality of life in patients with chronic refractory pouchitis after 8 weeks of treatment. Both studies found significant improvement in the pouchitis disease activity index, in the Disease Questionnaire score, as well as the clinical, endoscopic and histological subscores. Oral budesonide appears effective in inducing remission in active chronic refractory pouchitis.39,40
Topical treatment
Budesonide foams and enemas have also been used in treating distal colitis. Budesonide enemas have been found to be effective and well tolerated due to low systemic bioavailability (15%), with less effect on plasma cortisol level, thereby potentially minimizing steroid side effects.41 The drug is absorbed in the distal rectum and the hemorrhoid plexus.42 Two randomized trials compared rectal mesalazine and rectal budesonide in active distal UC and mesalazine was demonstrated to be better than budesonide.43,44 In the first study by Lemann et al,43 budesonide enema 2 mg/100 mL appears to be as efficient and well tolerated as 5-aminosalicylic acid enema in treating active distal UC and proctitis. Both enema forms resulted in significant improvement in endoscopy and histopathology scores as well as in clinical symptoms (number of bowel movements per day, quality of stools, presence of blood and mucus, and state of wellbeing). However, the clinical remission rate at 4 weeks was 38% for patients treated with budesonide enema but 60% for those treated with 5-aminosalicylic acid enema (P = 0.03).43
The most recent trial by Hartmann et al44 compared therapy with budesonide enema (2 mg/100 mg) and mesalazine enema (4 g/60 mL) in an open randomized study including 237 patients with active mild to moderate left sided UC. Clinical remission rates of 75% and 60% were achieved after 8 weeks of treatment with rectal mesalazine or budesonide, respectively (P < 0.02). The authors concluded that mesalazine enema was associated with a significantly higher remission rate, which was also supported by favorable trends in the secondary endpoints (Inflammatory Bowel Disease Questionnaire [IBDQ], endoscopic and histological remission).44
Conclusion
Oral systemic corticosteroids have been used to induce remission in active UC patients for over 50 years due to their potent anti-inflammatory effects. However, side effects are frequent and risks associated with long-term therapy outweigh the benefits of this treatment; alternative agents with fewer side effects are needed. Budesonide, a nonsystemic corticosteroid with high first-pass metabolism, may be a viable therapeutic option in patients with active mild to moderate UC. Current studies have failed to demonstrate higher efficacy of budesonide versus mesalazine for the induction of remission in active UC patients. Mesalazine is superior to budesonide for the treatment of active UC. Preliminary data from clinical trials with budesonide-MMX, a new oral formulation of budesonide with a controlled release system, have demonstrated promising efficacy in treating left sided UC patients and may also be an option in maintaining clinical remission. Large prospective and controlled trials are therefore needed. Insufficient data exist on the role of budesonide as maintenance therapy in UC patients and more comparison studies with mesalazine are required. Oral budesonide seems effective in inducing remission in active chronic refractory pouchitis; however, rectal budesonide in active distal UC patients has not demonstrated improvement over rectal mesalazine.
Disclosure
The authors report no conflict of interest in this work.
References
Dignass A, Lindsay JO, Sturm A, et al. Second European evidence-based consensus on the diagnosis and management of ulcerative colitis part 2: current management. J Crohns Colitis. 2012;6(10):991–1030. | |
Nunes T, Barreiro-de Acosta M, Marin-Jimenez I, Nos P, Sans M. Oral locally active steroids in inflammatory bowel disease. J Crohns Colitis. 2013;7(3):183–191. | |
O’Donnell S, O’Morain CA. Therapeutic benefits of budesonide in gastroenterology. Ther Adv Chronic Dis. 2010;1(4):177–186. | |
Gross V. Oral pH-modified release budesonide for treatment of inflammatory bowel disease, collagenous and lymphocytic colitis. Expert Opin Pharmacother. 2008;9(7):1257–1265. | |
Dignass A, Van Assche G, Lindsay JO, et al; European Crohn’s and Colitis Organisation (ECCO). The second European evidence-based Consensus on the diagnosis and management of Crohn’s disease: Current management. J Crohns Colitis. 2010;4(1):28–62. | |
Hanauer S, Sandborn WJ, Persson A, Persson T. Budesonide as maintenance treatment in Crohn’s disease: a placebo-controlled trial. Aliment Pharmacol Ther. 2005;21(4):363–371. | |
Sandborn WJ, Lofberg R, Feagan BG, Hanauer SB, Campieri M, Greenberg GR. Budesonide for maintenance of remission in patients with Crohn’s disease in medically induced remission: a predetermined pooled analysis of four randomized, double-blind, placebo-controlled trials. Am J Gastroenterol. 2005;100(8):1780–1787. | |
Sherlock ME, Seow CH, Steinhart AH, Griffiths AM. Oral budesonide for induction of remission in ulcerative colitis [review]. Cochrane Database Syst Rev. 2010(10):CD007698. | |
Sandborn WJ, Travis S, Moro L, et al. Once-daily budesonide MMX(R) extended-release tablets induce remission in patients with mild to moderate ulcerative colitis: results from the CORE I study. Gastroenterology. 2012;143(5):1218–1226. e1–e2. | |
Munch A, Aust D, Bohr J, et al; European Microscopic Colitis Group (EMCG). Microscopic colitis: Current status, present and future challenges: statements of the European Microscopic Colitis Group. J Crohns Colitis. 2012;6(9):932–945. | |
Gentile NM, Abdalla AA, Khanna S, et al. Outcomes of patients with microscopic colitis treated with corticosteroids: a population-based study. Am J Gastroenterol. 2013;108(2):256–259. | |
Lofberg R, Danielsson A, Salde L. Oral budesonide in active Crohn’s disease. Aliment Pharmacol Ther. 1993;7(6):611–616. | |
Marin-Jimenez I, Pena AS. Budesonide for ulcerative colitis. Rev Esp Enferm Dig. 2006;98(5):362–373. Spanish. | |
Patel NV, Patel JK, Shah SH, Patel JN. Central composite design for the formulation and optimization of a multi-unit potential colonic drug delivery system of budesonide for ulcerative colitis. Pharmazie. 2011;66(2):124–129. | |
Brunner M, Ziegler S, Di Stefano AF, et al. Gastrointestinal transit, release and plasma pharmacokinetics of a new oral budesonide formulation. Br J Clin Pharmacol. 2006;61(1):31–38. | |
Fiorino G, Fries W, De La Rue SA, Malesci AC, Repici A, Danese S. New drug delivery systems in inflammatory bowel disease: MMX and tailored delivery to the gut. Curr Med Chem. 2010;17(17):1851–1857. | |
De Cassan C, Fiorino G, Danese S. Second-generation corticosteroids for the treatment of Crohn’s disease and ulcerative colitis: more effective and less side effects? Dig Dis. 2012;30(4):368–375. | |
D’Haens GR, Kovacs A, Vergauwe P, et al. Clinical trial: Preliminary efficacy and safety study of a new Budesonide-MMX(R) 9 mg extended-release tablets in patients with active left-sided ulcerative colitis. J Crohns Colitis. 2010;4(2):153–160. | |
Barnes PJ. Molecular mechanisms and cellular effects of glucocorticosteroids. Immunol Allergy Clin North Am. 2005;25(3):451–468. | |
Silverman J, Otley A. Budesonide in the treatment of inflammatory bowel disease. Expert Rev Clin Immunol. 2011;7(4):419–428. | |
Ardizzone S, Bianchi Porro G. Comparative tolerability of therapies for ulcerative colitis. Drug Saf. 2002;25(8):561–582. | |
Lichtenstein GR, Bengtsson B, Hapten-White L, Rutgeerts P. Oral budesonide for maintenance of remission of Crohn’s disease: a pooled safety analysis. Aliment Pharmacol Ther. 2009;29(6):643–653. | |
D’Haens G, Verstraete A, Cheyns K, Aerden I, Bouillon R, Rutgeerts P. Bone turnover during short-term therapy with methylprednisolone or budesonide in Crohn’s disease. Aliment Pharmacol Ther. 1998;12(5):419–424. | |
Schoon EJ, Bollani S, Mills PR, et al; Matrix Study Group. Bone mineral density in relation to efficacy and side effects of budesonide and prednisolone in Crohn’s disease. Clin Gastroenterol Hepatol. 2005;3(2):113–121. | |
Beaulieu DB, Ananthakrishnan AN, Issa M, et al. Budesonide induction and maintenance therapy for Crohn’s disease during pregnancy. Inflamm Bowel Dis. 2009;15(1):25–28. | |
Piette V, Daures JP, Demoly P. Treating allergic rhinitis in pregnancy. Curr Allergy Asthma Rep. 2006;6(3):232–238. | |
Norjavaara E, de Verdier MG. Normal pregnancy outcomes in a population-based study including 2,968 pregnant women exposed to budesonide. J Allergy Clin Immunol. 2003;111(4):736–742. | |
Lundin PD, Edsbacker S, Bergstrand M, et al. Pharmacokinetics of budesonide controlled ileal release capsules in children and adults with active Crohn’s disease. Aliment Pharmacol Ther. 2003;17(1):85–92. | |
Levine A, Weizman Z, Broide E, et al; Israeli Pediatric Gastroenterology Association Budesonide Study Group. A comparison of budesonide and prednisone for the treatment of active pediatric Crohn disease. J Pediatr Gastroenterol Nutr. 2003;36(2):248–252. | |
Levine A, Kori M, Dinari G, et al; Israeli Pediatric Budesonide Study Group. Comparison of two dosing methods for induction of response and remission with oral budesonide in active pediatric Crohn’s disease: a randomized placebo-controlled trial. Inflamm Bowel Dis. 2009;15(7):1055–1061. | |
Escher JC; European Collaborative Research Group on Budesonide in Paediatric IBD. Budesonide versus prednisolone for the treatment of active Crohn’s disease in children: a randomized, double-blind, controlled, multicentre trial. Eur J Gastroenterol Hepatol. 2004;16(1):47–54. | |
Lofberg R, Danielsson A, Suhr O, et al. Oral budesonide versus prednisolone in patients with active extensive and left-sided ulcerative colitis. Gastroenterology. 1996;110(6):1713–1718. | |
Gross V, Bunganic I, Mikhailova TL, et al. Efficacy and tolerability of a once daily treatment with budesonide capsules versus mesalamine granules for the treatment of active ulcerative colitis: a randomized, double-blind, double-dummy, multicenter study. Gastroenterology. 2009;136(5 Suppl 1):A–15. | |
Gross V, Bunganic I, Belousova EA, et al; International BUC-57 Study Group. 3 g mesalazine granules are superior to 9 mg budesonide for achieving remission in active ulcerative colitis: a double-blind, double-dummy, randomised trial. J Crohns Colitis. 2011;5(2):129–138. | |
Keller R, Stoll R, Foerster EC, Gutsche N, Domschke W. Oral budesonide therapy for steroid-dependent ulcerative colitis: a pilot trial. Aliment Pharmacol Ther. 1997;11(6):1047–1052. | |
Kolkman JJ, Mollmann HW, Mollmann AC, et al. Evaluation of oral budesonide in the treatment of active distal ulcerative colitis. Drugs Today (Barc). 2004;40(7):589–601. | |
Chopra A, Pardi DS, Loftus EV Jr, et al. Budesonide in the treatment of inflammatory bowel disease: the first year of experience in clinical practice. Inflamm Bowel Dis. 2006;12(1):29–32. | |
Sandborn WJ, Danese S, Ballard ED, et al. Efficacy of budesonide MMx® 6 mg QD for the maintenance of remission in patients with ulcerative colitis: results from a phase III, 12 month safety and extended use study. Gastroenterology. 2012;142(5 Suppl 1):S–564. | |
Gionchetti P, Rizzello F, Poggioli G, et al. Oral budesonide in the treatment of chronic refractory pouchitis. Aliment Pharmacol Ther. 2007;25(10):1231–1236. | |
Cabriada Nuno JL, Hernandez Martin A, Bernal Martinez A, Zabalza Estevez I. Oral budesonide in the treatment of chronic refractory pouchitis. Gastroenterol Hepatol. 2008;31(8):485–489. Spanish. | |
Budesonide enema in distal ulcerative colitis. A randomized dose-response trial with prednisolone enema as positive control. The Danish Budesonide Study Group. Scand J Gastroenterol. 1991;26(12):1225–1230. | |
Gomollon F, Hinojosa J, Nos P. Budesonide and inflammatory bowel disease. Gastroenterol Hepatol. 1999;22(10):525–532. Spanish. | |
Lemann M, Galian A, Rutgeerts P, et al. Comparison of budesonide and 5-aminosalicylic acid enemas in active distal ulcerative colitis. Aliment Pharmacol Ther. 1995;9(5):557–562. | |
Hartmann F, Stein J; BudMesa-Study Group. Clinical trial: controlled, open, randomized multicentre study comparing the effects of treatment on quality of life, safety and efficacy of budesonide or mesalazine enemas in active left-sided ulcerative colitis. Aliment Pharmacol Ther. 2010;32(3):368–376. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.