Back to Journals » International Journal of Women's Health » Volume 18
Long-Term Management and Prevention Strategies for Adolescent Primary Dysmenorrhea: From Precision Diagnosis to Comprehensive Intervention
Authors Zhao M ![]() , Zhou F, Qiu C
, Zhou F, Qiu C
Received 20 March 2026
Accepted for publication 25 June 2026
Published 3 July 2026 Volume 2026:18 610913
DOI https://doi.org/10.2147/IJWH.S610913
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Mei Zhao 1,2, Fuhua Zhou1, ChunMei Qiu1
1Department of Gynecology, Sanming Hospital of Integrated Medicine, Sanming, Fujian, People’s Republic of China; 2Department of Gynecology, Longhua Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China
Correspondence: ChunMei Qiu, Department of Gynecology, Sanming Hospital of Integrated Medicine, Building 13, Shazhou New Village, Sanyuan District, Sanming, Fujian, People’s Republic of China, Email [email protected]
Abstract: Adolescent primary dysmenorrhea (PD) is one of the most prevalent gynecological issues in adolescent females, and its long-term management and prevention are crucial for improving quality of life, preventing secondary complications, and safeguarding future reproductive health. This narrative review examines the pathophysiological mechanisms, key points of differential diagnosis, long-term pharmacological and non-pharmacological management strategies, lifestyle interventions, psychosocial support, and evidence-based prevention frameworks for adolescent PD. It particularly emphasizes the importance of accurately distinguishing rare organic conditions, such as Obstructed Hemivagina and Ipsilateral Renal Anomaly (OHVIRA) syndrome, which can mimic primary dysmenorrhea, during long-term management to avoid misdiagnosis and delayed treatment. This narrative review synthesizes current evidence on adolescent primary dysmenorrhea. Its primary objective is to provide clinicians with a comprehensive, staged, and individualized long-term management framework that integrates pharmacological, non-pharmacological, lifestyle, and psychosocial interventions, while emphasizing the importance of accurate differential diagnosis and patient empowerment through health education. Key outcome measures assessed in this review include pain severity, pain duration, quality of life, school absenteeism, medication use, and adverse effects.
Keywords: adolescent, primary dysmenorrhea, long-term management, prevention strategies, differential diagnosis, comprehensive intervention
Introduction
Dysmenorrhea represents one of the most prevalent gynecological complaints among adolescents, with a substantial proportion of young females experiencing menstrual pain that adversely impacts their daily functioning, academic performance, and psychological well-beingPrimary dysmenorrhea (PD),1 defined as painful menstruation in the absence of identifiable pelvic pathology, is the most commonly encountered menstrual issue in this demographic and is a leading cause of recurrent school absenteeism.2 The core pathophysiological mechanism involves the excessive synthesis and release of prostaglandins, particularly prostaglandin F2α (PGF2α), from the endometrium during menstruation, which induces intense, spasmodic uterine contractions and resultant ischemia, culminating in cramping lower abdominal pain.3 However, the clinical presentation of PD extends beyond isolated pain, often encompassing a spectrum of systemic symptoms and imposing a significant burden on quality of life. Research indicates a strong positive correlation between the severity of dysmenorrhea, as measured by tools like the Visual Analog Scale (VAS), and its negative impact on adolescents’ physical activities, social engagements, and school attendance.2 The economic and societal costs are considerable, with dysmenorrhea accounting for billions in economic impact annually in some countries and contributing to recurrent short-term school absences.4,5 Therefore, effective long-term management and prevention strategies are imperative, necessitating a shift from merely addressing acute episodes to implementing comprehensive, sustained interventions that improve symptom control, functional capacity, and overall health outcomes.
A critical foundation for any long-term management plan is a precise initial assessment to distinguish true primary dysmenorrhea from secondary causes, a step where misdiagnosis remains a significant concern. The diagnosis of PD fundamentally relies on the exclusion of underlying pelvic pathologies, with a detailed patient history playing a pivotal role.1 Alarmingly, factors such as adolescents’ reluctance to seek care, reliance on non-professional advice, or incomplete clinical evaluations by healthcare providers can contribute to diagnostic errors and delays in appropriate management.1 This is particularly dangerous as some adolescents presenting with what appears to be primary dysmenorrhea may harbor occult reproductive tract anomalies or other conditions. A notable example is Obstructed Hemivagina and Ipsilateral Renal Anomaly (OHVIRA) syndrome, which is frequently misdiagnosed as PD, leading to delayed intervention and preventable complications.5,6 The detailed discussion of OHVIRA syndrome, along with other secondary causes such as endometriosis, is provided in the differential diagnosis section (Key Differential Diagnosis: Vigilance for Organic Diseases Masquerading as “Primary”). The long-term management of confirmed primary dysmenorrhea necessitates a multidimensional and integrative approach that extends beyond pharmacological analgesia to encompass nutritional, lifestyle, psychological, and complementary interventions aimed at modulating underlying pathophysiology and improving coping mechanisms. While non-steroidal anti-inflammatory drugs (NSAIDs) and hormonal contraceptives remain first-line pharmacological therapies by inhibiting prostaglandin synthesis or suppressing ovulation, there is increasing interest in adjuvant and alternative strategies to limit medication use and address root causes.7 Nutritional factors, particularly vitamin D and calcium status, have emerged as significant modulators of dysmenorrhea severity.4,8,9 Lifestyle factors, including body mass index (BMI) and physical activity, are also intricately linked to PD.10–12 Furthermore, the bidirectional relationship between dysmenorrhea and psychological health cannot be overstated, with studies demonstrating associations with anxiety, depression, poor sleep quality, and stress coping ability.13–15
The primary aim of this narrative review is to provide clinicians with a comprehensive, evidence-informed framework for the long-term management and prevention of adolescent primary dysmenorrhea. Unlike existing reviews that often focus narrowly on acute pain relief or isolated therapeutic modalities, this review integrates findings across pharmacological, non-pharmacological, lifestyle, and psychosocial domains to support a staged, individualized, and sustainable management approach. From a clinical perspective, this review addresses several key gaps: (1) the frequent misdiagnosis of secondary causes as primary dysmenorrhea; (2) the lack of clear guidance on transitioning from episodic pain control to long-term preventive strategies; (3) the underutilization of evidence-based non-pharmacological interventions; and (4) the need to empower adolescents through health education and self-management. By synthesizing current evidence and highlighting practical recommendations, this review aims to improve clinical decision-making, reduce diagnostic delays, prevent long-term complications, and ultimately enhance the quality of life for adolescents suffering from dysmenorrhea.
This article is a narrative review, not a systematic review. It does not follow PRISMA guidelines or include a formal, systematic search strategy. Literature was identified through searches of PubMed, Web of Science, and CNKI databases up to February 5, 2026, using search terms including “adolescent primary dysmenorrhea”, “long-term management”, “differential diagnosis”, “OHVIRA syndrome”, and “non-pharmacological interventions”. The studies cited in this review encompass a range of publication types, including randomized controlled trials (RCTs), systematic reviews and meta-analyses, prospective and retrospective cohort studies, cross-sectional studies, case series, and narrative reviews. Whenever available, priority was given to high-quality evidence sources such as RCTs and meta-analyses, particularly for therapeutic interventions. For rare conditions such as OHVIRA syndrome, case series and case reports were also included due to the paucity of higher-level evidence. The selection of articles was guided by clinical relevance and quality, without the application of systematic eligibility criteria or formal quality assessment tools, consistent with the nature of a narrative review. The review synthesizes key findings based on the authors’ expertise and critical evaluation, aiming to provide a broad, clinically oriented overview of long-term management strategies for adolescent primary dysmenorrhea.
Pathophysiology and Differential Diagnosis of Primary Dysmenorrhea: The Starting Point for Long-Term Management
Prostaglandin-Mediated Pain Mechanisms and Their Long-Term Effects
The synthesis and metabolism of endometrial prostaglandins (PGs) during the menstrual cycle are central to the pathophysiology of primary dysmenorrhea. Following progesterone withdrawal in the late luteal phase, the release of arachidonic acid from phospholipid membranes is catalyzed by phospholipase A2. This arachidonic acid is subsequently metabolized via the cyclooxygenase (COX) pathway, predominantly COX-2, leading to the production of prostaglandins, including PGF2α and PGE2.16 An imbalance in the ratio of these prostaglandins, specifically elevated PGF2α relative to PGE2, is a key driver of dysmenorrheic pain. PGF2α potently stimulates uterine smooth muscle contraction by increasing intracellular calcium concentration, leading to excessive, painful uterine contractions and ischemia.17 Concurrently, PGE2, while often considered pro-inflammatory, can exhibit complex, context-dependent roles. In some inflammatory settings, PGE2 signaling through specific receptors like EP4 can exert anti-inflammatory effects by inhibiting pathways such as IKK/NF-κB.18 However, in the context of primary dysmenorrhea, the dysregulated local milieu favors the hyper-contractile effects of PGF2α. This imbalance not only causes direct cramping pain but also contributes to vascular spasm and heightened peripheral nociceptor sensitivity, a process known as peripheral sensitization.19 The direct link between high urinary levels of PGF2α and the incidence of primary dysmenorrhea in adolescents underscores its pathogenic role.3 Furthermore, interventions that reduce PGF2α, such as extra virgin olive oil’s active compound oleocanthal, which inhibits PGF2α-induced uterine hyper-contraction and associated pain signaling pathways, validate this mechanism as a therapeutic target.16 Photobiomodulation with red light has also been shown to effectively decrease PGF2α levels while upregulating PGE2, resulting in pain inhibition in dysmenorrhea models.19
Long-term exposure to high levels of prostaglandins, particularly the inflammatory milieu they sustain, may have profound implications for uterine innervation and pain chronicity. Persistent inflammation and oxidative stress, driven by repeated cycles of elevated PGs, can lead to neuroplastic changes. This includes potential alterations in the density and sensitivity of nerve fibers within the uterine myometrium. The state of chronic inflammation can promote peripheral and central sensitization, where the nervous system becomes hyper-responsive to pain stimuli.20 This shares mechanistic pathways with other chronic pain conditions, including endometriosis-associated pain, suggesting a potential continuum or shared vulnerability.20 The concept of central sensitization is supported by neuroimaging studies in primary dysmenorrhea patients showing structural and functional changes in brain regions involved in pain perception and modulation, even during pain-free phases, indicating long-term neuroadaptive changes.21 The inflammatory cascade in dysmenorrhea, characterized by elevated cytokines like IL-6 and IL-1β, can further exacerbate this sensitization process.22 Over time, this may lower the pain threshold and contribute to the chronicity of dysmenorrhea, transforming it from a cyclical event into a persistent pain state. The role of prostaglandins extends beyond the uterus; for instance, in neuroinflammatory contexts, PGE2 is involved in regulating immune cell function and inflammatory responses within the central nervous system, analogous to how it might influence pain pathways originating from the pelvis.23–25 Consequently, targeting prostaglandin synthesis remains the cornerstone of long-term pharmacological management for primary dysmenorrhea. Non-steroidal anti-inflammatory drugs (NSAIDs) work by inhibiting COX enzymes, thereby reducing the production of both PGF2α and PGE2. However, due to the potential cardiovascular and gastrointestinal side effects from non-selective inhibition of prostaglandins, there is interest in more targeted approaches.26 For example, inhibiting microsomal prostaglandin E2 synthase-1 (mPGES-1), a downstream enzyme specifically involved in PGE2 synthesis, is being explored as a strategy to block the overexpression of PGE2 in inflammatory diseases while sparing other prostanoids.26 Nutritional and supplemental interventions also act on this axis. Vitamin D supplementation has been shown to significantly reduce dysmenorrhea severity, potentially by modulating inflammatory cytokine and prostaglandin synthesis, given the expression of vitamin D receptors in the female reproductive tract.4 Similarly, calcium absorption, which is vitamin D-dependent, is implicated, as abnormal calcium metabolism can affect muscle contractility.4 Other strategies like high-intensity interval training (HIIT) have demonstrated efficacy in reducing pain severity and menstrual distress, partly through modulation of hormone levels and decreased inflammation, including reductions in PGE2 and PGF2α.27 These multifaceted interventions targeting the prostaglandin pathway provide a robust theoretical foundation for comprehensive, long-term management strategies aimed not only at symptom relief but also at potentially mitigating the risk of pain chronicity and central sensitization (Figure 1).
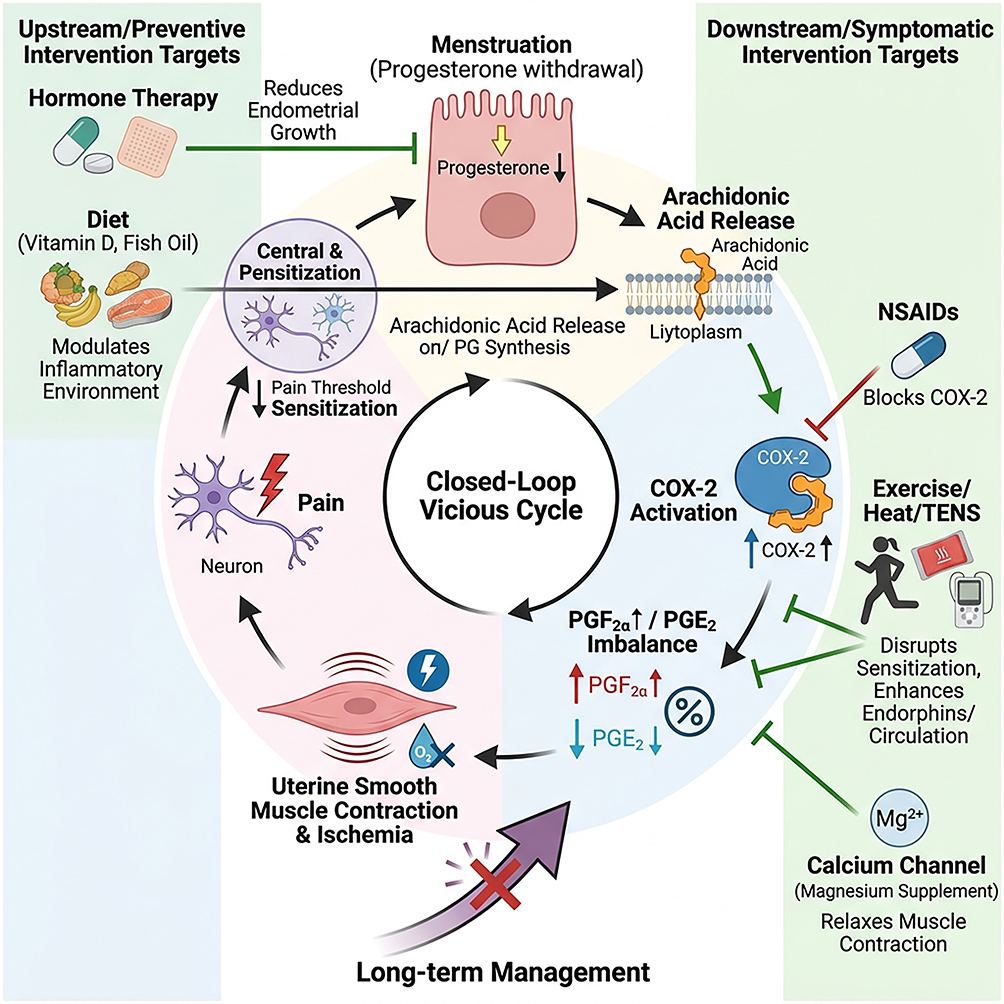 |
Figure 1 Pathophysiology and Intervention Targets of Primary Dysmenorrhea. This diagram illustrates the central “vicious cycle” of prostaglandin-mediated pain in primary dysmenorrhea, from progesterone withdrawal to uterine hypercontraction, ischemia, and central sensitization. It maps the mechanisms of key long-term interventions: upstream strategies (hormonal therapy, diet) target the inflammatory environment, while downstream approaches (NSAIDs, exercise/heat/TENS, magnesium) work to block prostaglandin synthesis, relieve muscle contraction, disrupt pain sensitization, and enhance endogenous pain relief, ultimately aiming to break the cycle through comprehensive long-term management. Abbreviations: TENS, transcutaneous electrical nerve stimulation; NSAIDs, non-steroidal anti-inflammatory drugs; COX, cyclooxygenase; PGF2α, prostaglandin F2α. |
Key Differential Diagnosis: Vigilance for Organic Diseases Masquerading as “Primary”
A comprehensive clinical evaluation is paramount in adolescents presenting with dysmenorrhea to distinguish primary from secondary causes. A detailed history and, when appropriate, a pelvic examination are essential first steps. Clinicians must maintain a high index of suspicion and actively seek “red flag” symptoms that suggest an underlying organic pathology. These warning signs include: (1) Dysmenorrhea that is progressive in severity over time; (2) Poor response to conventional first-line therapies (eg, NSAIDs); (3) Non-cyclic pelvic pain (pain occurring outside the menstrual period); (4) Associated gastrointestinal or urinary symptoms (eg, dyschezia, dysuria, urinary frequency); (5) Onset of pain more than 12 months after menarche (late-onset dysmenorrhea); (6) Presence of a palpable pelvic mass on examination.
Endometriosis stands as the most common cause of secondary dysmenorrhea in adolescents and young women.28 A long diagnostic delay for endometriosis increases the risk of chronic pain and future fertility issues, highlighting the critical importance of early recognition.29 Studies suggest that adolescents with severe dysmenorrhea have a significantly higher likelihood of ultrasound-detectable endometriosis or adenomyosis, with one investigation finding such signs in approximately 40% of adolescents with severe pain.30 A history of dysmenorrhea, particularly with onset more than 12 months after menarche or persistent pain refractory to treatment, is a strong predictor for a later diagnosis of endometriosis.31,32
OHVIRA Syndrome as a Critical Differential Diagnosis
Obstructed Hemivagina and Ipsilateral Renal Anomaly (OHVIRA) syndrome, also known as Herlyn-Werner-Wunderlich syndrome, is a Müllerian duct anomaly characterized by the triad of uterine didelphys (or bicorporeal uterus), an obstructed hemivagina, and ipsilateral renal agenesis.33 This syndrome typically manifests after menarche with progressively worsening dysmenorrhea due to the obstruction of menstrual outflow from one hemivagina, leading to accumulation of blood (hematocolpos).34 OHVIRA syndrome is frequently misdiagnosed as primary dysmenorrhea, leading to a dangerous delay in intervention that can result in serious complications, including: (1) Hematocolpos (blood accumulation in the obstructed vaginal canal); (2) Pelvic inflammatory disease and tubo-ovarian abscess; (3) Endometriosis (due to chronic retrograde menstruation); (4) Permanent, irreversible damage to the ipsilateral adnexa, compromising future reproductive potential.34
Clinicians should maintain a high index of suspicion for OHVIRA syndrome in adolescents with severe, progressive, or treatment-refractory dysmenorrhea, particularly when accompanied by a palpable pelvic mass or known solitary kidney (incidentally detected). The syndrome may also present with non-specific symptoms such as recurrent vulvovaginitis or chronic pelvic pain.35
Role of Imaging in Differential Diagnosis
Imaging plays a central and definitive role in the differential diagnosis of dysmenorrhea when secondary causes are suspected.
Transabdominal or transperineal ultrasound is the recommended first-line imaging tool due to its wide availability, non-invasiveness, and lack of ionizing radiation. It can effectively identify findings suggestive of obstructive anomalies, such as a distended, fluid-filled vaginal canal (hematocolpos) or uterine cavity (hematometra), and the presence of a uterine or vaginal septum.36
Magnetic resonance imaging (MRI) is considered the gold standard for elucidating complex genital tract anatomy. MRI provides superior soft-tissue contrast and multi-planar capabilities, allowing for detailed characterization of Müllerian duct anomalies, precise mapping of septa, and confirmation of obstruction.37 Crucially, MRI also enables a comprehensive evaluation of associated anomalies, particularly in the renal system. Given the high association between Müllerian anomalies and renal tract abnormalities (as seen in OHVIRA), MRI can simultaneously assess for ipsilateral renal agenesis, ectopia, or dysplasia, providing a complete anatomical picture essential for pre-surgical planning.38
This integrated imaging approach ensures accurate diagnosis, prevents misclassification of secondary dysmenorrhea as primary, and guides appropriate surgical intervention to relieve obstruction and preserve fertility (Figure 2).
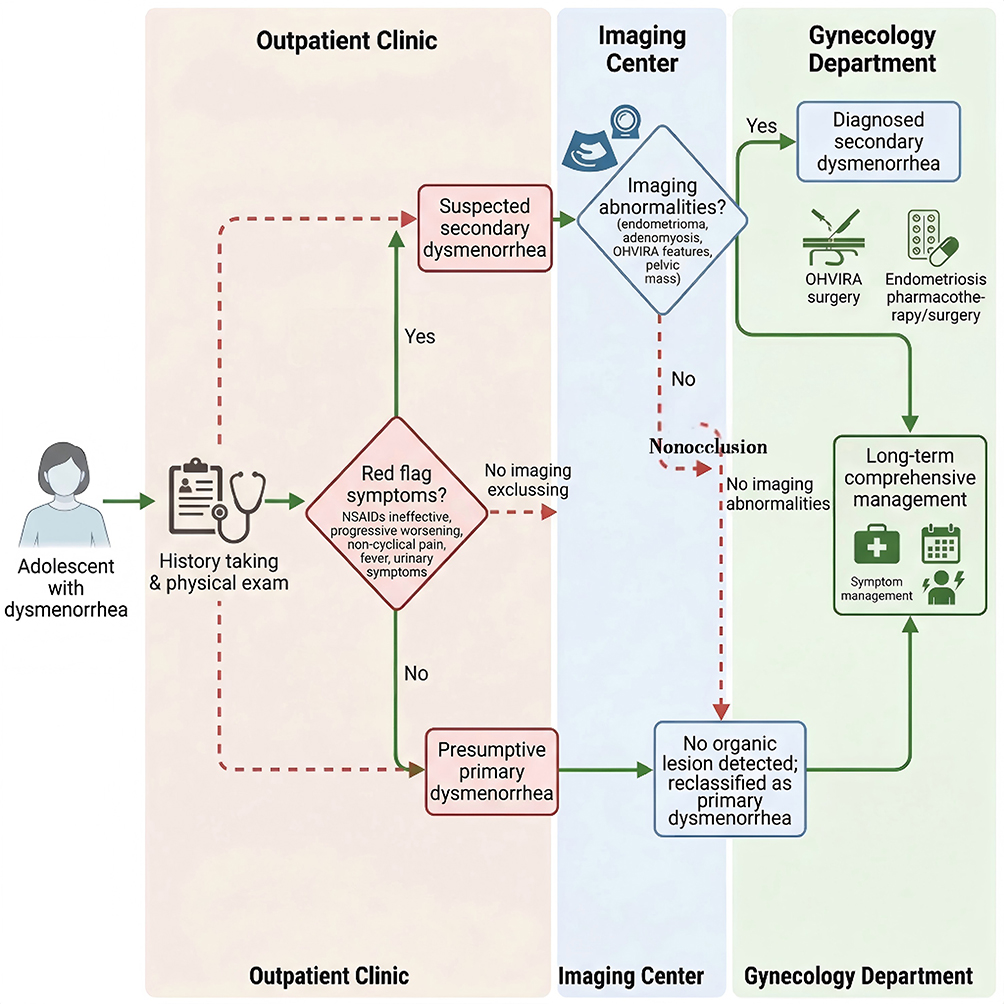 |
Figure 2 Precision Diagnosis and Triage Management Chart for Adolescent Dysmenorrhea. This flowchart illustrates the clinical workflow for evaluating adolescents presenting with dysmenorrhea, from initial assessment to definitive diagnosis and triage to appropriate management pathways. The algorithm emphasizes the identification of “red flag” symptoms that warrant further investigation, the role of noninvasive imaging (ultrasound and MRI) in detecting structural anomalies, and the differentiation between primary dysmenorrhea and secondary causes such as endometriosis or OHVIRA syndrome. Abbreviation: OHVIRA, Obstructed Hemivagina and Ipsilateral Renal Anomaly. |
Evidence-Based Long-Term Pharmacotherapy Strategies
First-Line Medications: Optimized Use of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
Non-steroidal anti-inflammatory drugs (NSAIDs) are established as the first-line pharmacological treatment for primary dysmenorrhea, primarily due to their mechanism of action in inhibiting cyclooxygenase (COX) enzymes, thereby reducing the synthesis of prostaglandins which are the key mediators of uterine cramping and pain.39 The pharmacodynamic profiles of different NSAIDs, such as ibuprofen, naproxen, and mefenamic acid, are central to their clinical application. A network meta-analysis evaluating over-the-counter analgesics for primary dysmenorrhea found that diclofenac and ibuprofen were ranked as the most and second most effective agents, respectively, based on efficacy outcomes, with both being significantly more effective than placebo.27 This analysis, which included naproxen and ketoprofen, supports the comparative effectiveness of various NSAIDs, although aspirin was found to be less effective than ibuprofen and diclofenac.27 The efficacy of specific agents like mefenamic acid is further supported by trials comparing it to other treatments, such as tranexamic acid for heavy menstrual bleeding associated with intrauterine device use, where it resulted in less volume of blood loss.40 For long-term management, a strategic shift from “as-needed” use to “preemptive” or anticipatory dosing is recommended to more effectively control the prostaglandin surge that precipitates pain. This approach involves initiating medication 1–2 days before the expected onset of menses and continuing for 2–3 days. While direct evidence for this specific schedule from the provided references is limited, the principle of proactive management is implicit in the recognition of NSAIDs as a cornerstone of treatment.41 The goal is to prevent the peak of prostaglandin production and the ensuing pain cascade, rather than attempting to suppress it after it has begun.
The long-term use of NSAIDs necessitates vigilant safety monitoring due to well-documented risks, including gastrointestinal (eg, nausea, indigestion), renal, and cardiovascular adverse effects.42 These drawbacks are a primary reason patients and clinicians seek alternative therapies.43,44 Strategies to mitigate these risks are crucial for safe long-term administration. Preventive measures include taking NSAIDs with food to reduce gastric irritation and using the lowest effective dose for the shortest necessary duration.41,45 The safety profile is a key differentiator between treatments; for instance, a systematic review on heat therapy found it probably reduced the risk of adverse effects compared with NSAIDs.46 Furthermore, studies on complementary therapies often highlight the adverse events associated with conventional NSAID use as a rationale for exploration. For example, ginger was found to be equally effective as NSAIDs for pain severity in primary dysmenorrhea, implying a potential for a better safety profile, though the specific adverse events of NSAIDs were not detailed in that meta-analysis.47 Similarly, a meta-analysis on the Chinese herbal formula Siwutang suggested it may be safer than conventional medicine in terms of the incidence of adverse events.48 Monitoring for side effects is particularly important in adolescents, who may use these medications over many years. The common practice of self-medication with NSAIDs, as observed in populations like nursing students, underscores the need for professional guidance to ensure appropriate and safe use.49 Ultimately, while NSAIDs remain highly effective, their optimization involves not only selecting the appropriate agent and dosing strategy but also implementing consistent safety measures to allow for sustainable long-term management of dysmenorrhea.
Long-Term Management and Individualized Selection of Hormonal Medications
Hormonal therapies, particularly combined oral contraceptives (COCs), are a cornerstone for the long-term management of primary dysmenorrhea, especially when NSAIDs are insufficient, contraindicated, or when contraception is desired. Their therapeutic mechanism is multifactorial, primarily involving the suppression of ovulation, which leads to a thinner endometrial lining and a consequent reduction in the production of prostaglandins and leukotrienes, the key inflammatory mediators of menstrual pain.50 This makes COCs an effective first-line medical option, independent of or in combination with NSAIDs. The evidence supports their use, as they are considered an effective treatment for both primary and secondary dysmenorrhea.41 The efficacy of COCs can be enhanced when used in combination with other therapies; for instance, one randomized controlled trial revealed a beneficial impact of oral contraceptives used in combination with the herbal medicine Tao-Hong Siwu Tang compared to OCs alone.42 This highlights the potential for integrative approaches in hormonal management.
The choice of hormonal regimen requires individualization. Traditional cyclic regimens (eg, 21 days of active pills followed by a 7-day hormone-free interval) are commonly used. However, extended-cycle or continuous-use regimens, which reduce or eliminate the hormone-free interval, may offer superior symptom control by preventing the withdrawal bleed and associated pain entirely. The provided references do not directly compare these regimens for dysmenorrhea, but the principle of using hormonal contraceptives for dysmenorrhea management is well-established.51 Long-term use of COCs, particularly in adolescents, necessitates consideration of potential effects on bone mineral density and lipid metabolism. While the specific references provided do not detail these effects for dysmenorrhea treatment, the importance of monitoring is a general principle in hormonal therapy. The selection of a progestin or estrogen-progestin combination should consider secondary indications, such as acne or hirsutism, alongside contraceptive needs.51 For adolescents with dysmenorrhea unresponsive to initial medical therapy, COCs are a standard part of the treatment algorithm.50
For individuals with contraindications to estrogen or those who desire a long-acting, low-maintenance option, progestin-only therapies are valuable alternatives. The levonorgestrel-releasing intrauterine system (LNG-IUS) is highlighted as a particularly suitable option for adolescents with both contraceptive needs and dysmenorrhea, including cases related to endometriosis.29 Other progestin-only options include subdermal implants and progestin-only pills, which are also effective for managing dysmenorrhea.52 The LNG-IUS is specifically mentioned as a hormonal contraceptive option for treating dysmenorrhea.32 In the context of intrauterine devices, the LNG-IUD is associated with irregular bleeding rather than increased menstrual flow, and medical therapies can be used to manage associated pain or bleeding.53 In cases of secondary dysmenorrhea, such as that caused by endometriosis, hormonal suppressive therapy is a mainstay of treatment following surgical diagnosis, with the goal of relieving symptoms and protecting fertility.52,53 Progestins are among the many drug classes used to treat adolescent endometriosis.43 Therefore, the individualized selection of hormonal therapy depends on a careful assessment of the patient’s symptoms, contraceptive requirements, medical history, risk factors, and personal preferences, ensuring a tailored approach to long-term dysmenorrhea management.
The Long-Term Role of Non-Pharmacological Interventions and Complementary and Alternative Therapies
The Role of Regular Physical Exercise and Physical Therapy
Regular physical exercise, particularly aerobic activities, is a cornerstone of long-term management for primary dysmenorrhea (PD) in adolescents, with a robust evidence base supporting its efficacy. Systematic reviews and meta-analyses of randomized controlled trials (RCTs) confirm that aerobic exercise significantly alleviates both the pain intensity and duration of PD in adolescents and young women.11 The physiological mechanisms underpinning this benefit are multifaceted. Exercise is known to stimulate the release of endogenous opioids like endorphins, which act as natural analgesics. Furthermore, it improves systemic and pelvic circulation, potentially reducing uterine ischemia—a key contributor to menstrual pain—and modulates stress hormones, thereby lowering overall stress levels which can exacerbate pain perception. A specific meta-analysis highlighted that various forms of aerobic exercise, including Pilates, are effective, with optimal parameters suggesting benefits from low-intensity sessions lasting 31–45 minutes, performed up to twice weekly over at least two menstrual cycles.54 Comparative studies show that both aquatic (eg, swimming) and land-based aerobic exercises lead to significant reductions in dysmenorrhea severity scores and pain intensity, while also improving pressure pain thresholds and quality of life, with aquatic exercise potentially offering superior gains in quality-of-life metrics.11 Beyond general aerobic activity, targeted exercise programs, including functional or combined exercise regimens, have been shown to effectively reduce abdominal and low back pain severity and improve associated menstrual symptoms and sleep quality over an 8-week period.55 High-intensity interval training (HIIT) has also demonstrated promise, significantly reducing premenstrual symptoms, menstrual distress, and pain severity, likely through modulation of hormonal profiles (eg, estradiol, progesterone, cortisol) and reduction of inflammatory mediators like prostaglandins.56
Physical therapy techniques offer another vital, non-pharmacological avenue for long-term management. Among these, pelvic floor muscle training has gained attention. A quasi-experimental study comparing Kegel exercises (pelvic floor strengthening) with pelvic rocking exercises over four menstrual cycles found that both significantly reduced pain, but Kegel exercises provided superior pain relief, facilitating a greater shift from severe to mild pain categories.57 This suggests that targeted pelvic floor relaxation and strengthening, rather than just mobilization, may be particularly beneficial. Heat therapy is one of the most widely used and evidence-supported physical modalities. Heat therapy, which involves the application of superficial heat to the lower abdomen, is a widely used physical modality that promotes local vasodilation, improves blood flow, and modulates pain gate mechanisms. A comprehensive systematic review and meta-analysis concluded that heat therapy is likely to reduce pain intensity both as a prophylactic measure over months and during acute episodes within 24 hours.58 When compared to NSAIDs, heat therapy may provide comparable or slightly superior analgesic efficacy while exhibiting a significantly superior safety profile with fewer adverse effects.58 The physiological rationale includes local vasodilation, improved blood flow, and potential modulation of pain gate mechanisms. Other manual and device-based therapies show promise but require further robust evidence. Sacroiliac joint manipulation, for instance, was found in an RCT to be more effective than superficial heat therapy in improving autonomic nervous system balance and alleviating lower abdominal pain and menstrual distress, with effects sustained over 8 weeks.59 Extracorporeal shock wave therapy (ESWT) applied to abdominal acupuncture points significantly reduced pain severity and duration over three cycles, with efficacy comparable whether applied during the follicular or luteal phase.60 Similarly, electromagnetic field therapy (EMFT) has shown statistically significant progress in reducing pain, improving work ability, and minimizing the need for analgesic drugs in young women with severe dysmenorrhea.61
Behavioral interventions involving neuromodulation, such as transcutaneous electrical nerve stimulation (TENS), represent a feasible long-term self-management tool. The mechanism involves delivering electrical currents to the skin, which inhibits pain transmission, releases endogenous opioids, and may reduce uterine muscle ischemia. An updated Cochrane review found that both high-frequency and low-frequency TENS may reduce pain compared to placebo or no treatment, though the certainty of evidence is low due to risk of bias in studies.62 High-frequency TENS application at the root level (spinal nerves) has shown significant improvement in managing lower abdominal, low back, and referred thigh pain in adolescents.63 While evidence comparing TENS directly to medications like NSAIDs or acetaminophen is uncertain, its favorable safety profile and potential for home use make it a viable option. Ongoing and planned RCTs are further investigating protocols for transcutaneous electrical acupoint stimulation (TEAS), a variant of TENS, and incorporating economic evaluations to assess its cost-effectiveness as a long-term management strategy.64,65 The feasibility of TENS as a home-based tool is underscored by its non-invasive nature and the ability for patients to self-administer during painful episodes, offering a sense of control over symptom management. Surveys indicate that alongside heat therapy and massage, many women actively seek and use such non-pharmacological strategies, highlighting the importance of integrating evidence-based physical and behavioral interventions into comprehensive adolescent health programs to reduce reliance on analgesics and improve overall quality of life.66
Evidence Assessment of Nutritional Supplements and Phytotherapy
The use of nutritional supplements for managing primary dysmenorrhea is a common area of interest, with several micronutrients evaluated in randomized controlled trials. Among these, omega-3 fatty acids, vitamin B1 (thiamine), vitamin E, and magnesium are frequently studied. The proposed mechanisms often involve anti-inflammatory pathways or modulation of muscle activity. For instance, omega-3 fatty acids may compete with arachidonic acid, leading to the production of less inflammatory prostaglandins. Magnesium is thought to act as a calcium antagonist, helping to relax uterine smooth muscle. However, while some individual studies show positive effects, the overall evidence base from high-quality systematic reviews specifically focusing on these supplements for PD in adolescents is not extensively detailed in the provided references. The references emphasize that dietary supplements are among the non-pharmacologic options with limited evidence, and they are typically suggested as adjuncts or alternatives for patients seeking such options, rather than as first-line treatments.67 A broad review on dysmenorrhea therapeutic options notes that behind first-line pharmacologic treatments, there are less evidence-based data for modalities like dietary supplements, and these methods should be used in conjunction with first-line therapy after discussing risks and benefits.7 This indicates that while specific RCTs exist for supplements like vitamin B1, vitamin E, and magnesium, the evidence is not as robust or consistent as for interventions like exercise or heat therapy. Therefore, recommendations for their use must be cautious and dose-specific, ideally guided by evidence from well-designed trials targeting the adolescent population, acknowledging that more research is needed to solidify dosing guidelines and efficacy.
Traditional plant-based therapies, including herbs and herbal formulas, are widely used globally for dysmenorrhea. Common examples include ginger, cinnamon, fennel, and traditional Chinese medicine (TCM) formulations like Wen Jing Tang. The mechanisms of action for these botanicals are diverse, often encompassing anti-inflammatory, antispasmodic, and prostaglandin-inhibiting properties. For instance, ginger contains gingerols, which have demonstrated anti-inflammatory effects. Evidence from clinical studies is emerging but varies in quality. Surveys of self-management practices show that a significant proportion of women use herbal teas to alleviate menstrual pain.68 However, the literature review accompanying one survey noted that the evidence for these methods remains limited. Within the TCM paradigm, various acupuncture-related therapies that often incorporate herbal elements (eg, acupoint patching with herbal preparations, herb-partitioned moxibustion) have been evaluated. A network meta-analysis of RCTs on acupuncture-related therapies for PD found that techniques combining massage with acupoint patching, acupuncture with acupoint patching, and acupoint patching alone ranked highly for improving clinical effective rates and reducing pain scores.69 Specific TCM external therapies like herb-partitioned moxibustion (HPM) at the Shenque (CV8) acupoint are used for syndromes like “cold coagulation and blood stasis”, combining heat, herbal, and acupoint stimulation to promote Qi circulation and relieve pain.70 Similarly, Zhuang medicine thread moxibustion, which integrates drug, acupoint, and moxibustion, has been applied in experimental models of PD, showing analgesic effects.71 While these practices are promising, the long-term safety considerations of continuous use of plant medicines are paramount. Potential issues include herb-drug interactions, variability in preparation and potency, and a lack of standardized dosing. The safety profile of many herbal remedies is not as thoroughly documented as that of conventional pharmaceuticals, necessitating caution.
When recommending complementary and alternative therapies, including both nutritional supplements and phytotherapies, it is crucial to base advice on the best available evidence and maintain a patient-centered approach. The overarching principle is that these interventions should not replace first-line pharmacologic treatments (NSAIDs, hormonal contraceptives) unless contraindicated or by patient preference, but can be considered as part of a multimodal management plan. A narrative review on therapeutic options stresses that methods with less evidence-based data, such as dietary supplements and acupuncture, should be used in conjunction with first-line therapy after a discussion of risks and benefits.7 Particular attention must be paid to potential interactions with conventional medications; for example, some herbs may affect cytochrome P450 enzymes, altering the metabolism of drugs like NSAIDs or oral contraceptives. Furthermore, the quality and sourcing of supplements and herbal products are often unregulated, posing risks of contamination or inconsistent active ingredient levels. Therefore, healthcare providers should inquire about patients’ use of these therapies, educate them on the evidence (or lack thereof), and emphasize the importance of disclosing all supplements to avoid adverse interactions. The goal is to integrate safe, evidence-informed complementary strategies into a holistic long-term management plan for adolescent dysmenorrhea, always prioritizing interventions with stronger evidence like exercise and heat therapy while cautiously navigating areas where evidence is still evolving.
Lifestyle Adjustment and the Construction of Preventive Health Behaviors
Long-Term Effects of Dietary Patterns on Weight Management
The long-term management of primary dysmenorrhea (PD) necessitates a focus on dietary patterns and weight management, as these factors significantly influence the underlying inflammatory and hormonal milieu. A diet rich in fiber and antioxidants, such as those found in fruits and vegetables, and low in fat, is posited to exert beneficial effects by modulating systemic inflammation and estrogen metabolism. For instance, the consumption of dried figs, a food high in fiber and antioxidants, was shown in a randomized controlled trial to significantly reduce pain severity and duration, menstrual distress, and perceived stress in individuals with PD compared to placebo and cinnamon groups.72 This suggests that specific dietary components can directly alleviate dysmenorrhea symptoms, potentially by lowering inflammatory mediators like prostaglandins. Conversely, certain dietary elements may exacerbate symptoms. A study investigating risk factors in adolescent basketball players found that higher susceptibility to disordered eating attitudes was associated with an increased risk of PD.73 While this study did not directly measure caffeine, salt, or alcohol intake, it highlights the complex interplay between dietary habits, psychological stress, and hormonal markers like elevated prolactin and cortisol, which are known to influence pain perception. Therefore, practical dietary advice should emphasize increasing intake of whole foods like fruits, vegetables, and legumes while recommending moderation or avoidance of potential triggers like excessive caffeine and alcohol, which may indirectly worsen symptoms through effects on stress and fluid balance. The relationship between body weight and PD severity is complex and bidirectional. A systematic review and meta-analysis concluded that being underweight may increase the risk of PD, whereas overweight and obesity might not be consistently associated with its development.74 However, other evidence points to a more nuanced picture. A cross-sectional study specifically in adolescents found that both underweight and obese groups had statistically higher visual analogue scale (VAS) pain scores compared to normal-weight and overweight groups.10 This indicates that deviations from a healthy weight range at both extremes are problematic. The mechanism linking obesity to potential exacerbation of pain may involve increased aromatase activity in adipose tissue, leading to higher estrogen levels, which can promote uterine prostaglandin production and cramping. Furthermore, obesity is often associated with a state of chronic low-grade inflammation, which could lower pain thresholds. Thus, maintaining a healthy weight through balanced nutrition and regular physical activity is a cornerstone of long-term PD management, not only for potential direct hormonal benefits but also for improving overall metabolic health and reducing systemic inflammation.
Comprehensive Strategies for Stress Management and Sleep Hygiene
Effective long-term strategies for primary dysmenorrhea must address the significant roles of chronic stress and poor sleep, both of which can exacerbate pain perception through distinct yet interconnected physiological pathways. Chronic stress activates the hypothalamic-pituitary-adrenal (HPA) axis and the sympathetic nervous system, leading to the release of cortisol and catecholamines. Elevated cortisol levels have been directly implicated in PD; a study on adolescent athletes found that higher cortisol levels were associated with an increased risk of dysmenorrhea.75 This hormonal response can heighten sensitivity to pain, increase muscle tension, and potentially dysregulate other reproductive hormones. Furthermore, stress can amplify the perception of menstrual pain through central nervous system mechanisms, making pain feel more intense and debilitating. Therefore, implementing long-term stress management techniques suitable for adolescents is crucial. These include mindfulness meditation, deep-breathing exercises, yoga, and cognitive-behavioral therapy (CBT). The efficacy of such holistic approaches is supported by research; for example, a randomized controlled trial on the naturopathic lifestyle practice Arogya Rakshak Panchatantra (ARP), which incorporates principles of stress reduction and healthy living, showed significant improvements in heart rate variability (an indicator of autonomic balance and stress resilience) and reductions in pain scores among young women with PD.76 Similarly, consuming dried figs was found to significantly reduce perceived stress levels alongside dysmenorrhea symptoms.72 Highlighting how dietary interventions can also modulate stress response. Sleep constitutes another critical pillar of management. Sleep deprivation or poor sleep quality negatively impacts pain thresholds and amplifies inflammatory responses. While the provided references do not contain direct studies on sleep and PD, the general principle is well-established in pain literature: inadequate sleep lowers the pain tolerance and can increase the production of pro-inflammatory cytokines. The ARP trial also monitored general well-being, and participants reported on various symptoms, underscoring the importance of a comprehensive lifestyle approach.76 Practical guidance for improving sleep hygiene includes maintaining a consistent sleep schedule, creating a dark and quiet sleep environment, limiting screen time before bed, and avoiding caffeine and heavy meals in the evening. Integrating these stress and sleep management strategies into a long-term plan can help break the cycle where pain causes stress and sleep disturbance, which in turn worsens pain, thereby improving overall coping and quality of life for adolescents with PD.
The Core Role of Psychosocial Support and Health Education in Long-Term Management
Long-Term Impact of Dysmenorrhea on Adolescent Mental Health and Quality of Life
Primary dysmenorrhea (PD) exerts a profound and enduring negative impact on the mental health and overall quality of life (QoL) of adolescent girls, extending far beyond the days of menstrual pain. The chronic, recurrent nature of the pain leads to significant functional impairments, including frequent school absenteeism, social withdrawal, and restriction of daily activities, which collectively precipitate and exacerbate psychological distress. A cross-sectional study in Zambia directly linked PD with a diminished health-related QoL among adolescent girls.77 The disruption is substantial; research indicates that PD leads to significant gynecological consultations, school absenteeism, and disrupted daily activities, adversely affecting overall QoL.11 The severity of this impact is dose-dependent; a study found a significant positive correlation between PD severity and its negative effect on adolescents’ physical activities, social activities, and school attendance, with higher odds of impairment in those with moderate to severe pain.2 This cycle of pain and disability fosters anxiety, depression, and a reduced sense of self-efficacy. Evidence robustly supports a bidirectional relationship between pain and emotional disorders. Studies consistently show that stress, depression, and anxiety are positively associated with menstrual pain and symptoms in adolescents.78 Furthermore, adolescents with PD affecting daily activities exhibit worse sleep quality, more symptoms of inattention and hyperactivity-impulsivity (linked to ADHD), and higher levels of anxiety, depression, somatization, and hostility compared to their peers.12 A large-scale phenome study and Mendelian randomization analysis in female college students provided genetic-level evidence, identifying an increased risk of depression and anxiety associated with PD.78 This complex interplay underscores the critical necessity of integrating psychological assessment and support into the long-term management paradigm for adolescent dysmenorrhea. To effectively capture this multifaceted burden, standardized assessment tools are essential. Clinical evaluation often utilizes pain diaries to track patterns, the Visual Analog Scale (VAS) or Numeric Pain Rating Scale (NPRS) to quantify pain intensity, and validated QoL instruments like the EuroQol-5 Dimension (EQ-5D).78 The Cox Menstrual Symptom Scale (CMSS) is another tool used to assess a broader range of symptoms.79 Employing these tools allows clinicians to move beyond a singular focus on pain severity, enabling a holistic understanding of how dysmenorrhea disrupts an adolescent’s life and informing comprehensive, personalized intervention strategies that address both physical and psychological dimensions.
Empowering Health Education: Transitioning from Patient to Self-Manager
Empowerment through structured health education is a cornerstone of effective long-term management for adolescent primary dysmenorrhea, facilitating a crucial transition from a passive patient to an active self-manager. The primary goal of such education is to equip both adolescents and their parents with accurate, evidence-based knowledge about the physiological mechanisms of menstruation and dysmenorrhea, available treatment options (both pharmacological and non-pharmacological), and realistic expected outcomes. This demystification process is vital for reducing unnecessary fear, dispelling myths, and combating the stigma often associated with menstrual pain, which can prevent help-seeking. A narrative review highlighted that parental knowledge about adolescent menstrual problems, including dysmenorrhea, is often limited, particularly in recognizing severity and appropriate management, underscoring the need for targeted family education.80 Education should be structured and comprehensive, covering key self-management skills. This includes teaching adolescents how to perform accurate pain self-assessment using tools like pain diaries or rating scales, ensuring the correct use of medications like NSAIDs (including timing and dosage), and instructing on non-pharmacological skills such as heat application, relaxation techniques, or specific exercises.81 Crucially, education must also define clear “red flag” or “warning signals” that indicate the need for medical re-evaluation, such as pain unresponsive to first-line treatment, worsening symptoms, or signs suggestive of secondary dysmenorrhea like endometriosis.1 This empowers adolescents to navigate their care proactively. The feasibility and effectiveness of this educational model can be significantly enhanced by leveraging digital health tools. Mobile applications offer promising platforms for symptom tracking, providing reminders for medication or non-drug interventions, and delivering accessible, reliable educational information. This digital support system can reinforce learning, promote adherence to management plans, and foster sustained self-management over time, ultimately improving long-term outcomes and quality of life for adolescents with dysmenorrhea.
Long-Term Management of Special Cases: Insights from OHVIRA Syndrome as an Example (Figure 3)
As discussed in Key Differential Diagnosis: Vigilance for Organic Diseases Masquerading as “Primary”, Obstructed Hemivagina and Ipsilateral Renal Anomaly (OHVIRA) syndrome is a critical differential diagnosis that must be excluded before confirming primary dysmenorrhea. Once diagnosed, however, the management paradigm shifts fundamentally from symptomatic treatment to definitive surgical intervention and structured long-term follow-up. This section focuses on the long-term management of OHVIRA syndrome following diagnosis, including surgical principles, postoperative surveillance, and reproductive health protection.
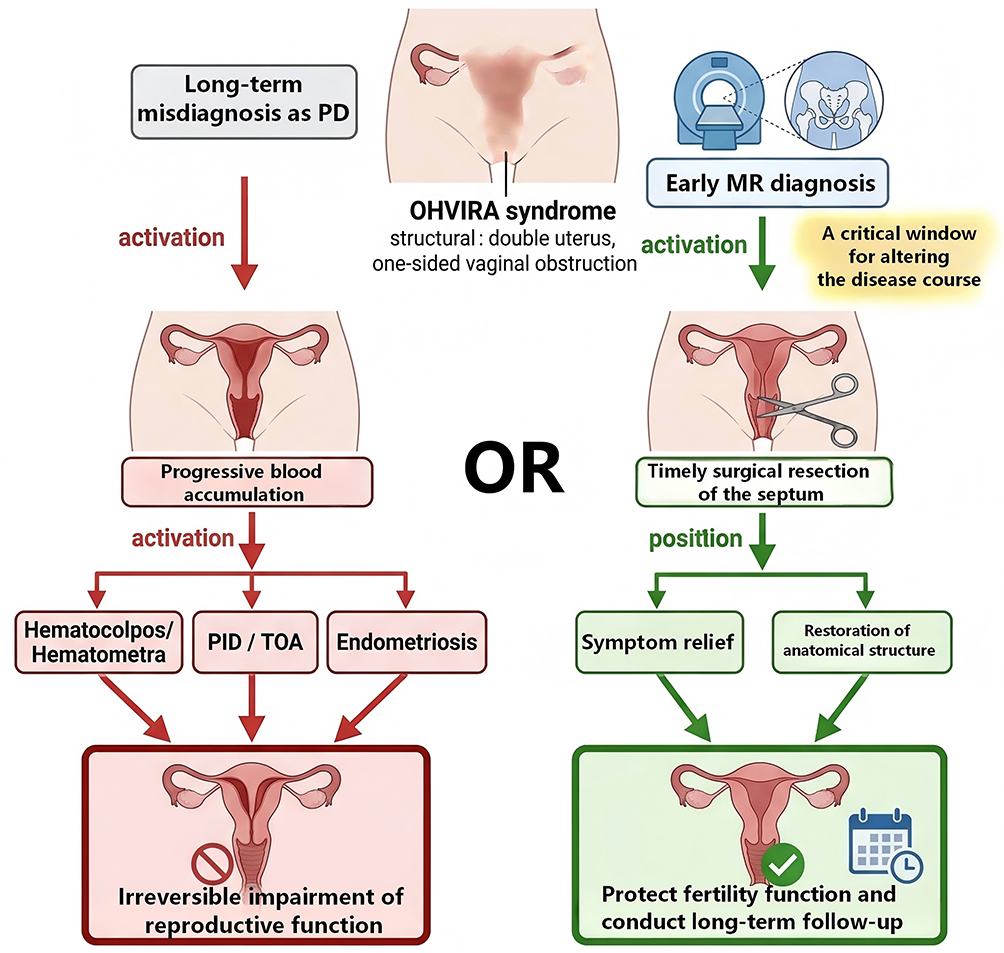 |
Figure 3 Pathological Evolution and Intervention Timing of OHVIRA Syndrome. This figure illustrates the progressive pathological changes in OHVIRA syndrome from menarche to late complications, including hematocolpos, endometriosis, and adnexal damage, as well as the critical window for timely surgical intervention. Abbreviations: PID, pelvic inflammatory disease; TOA, tubo-ovarian abscess. |
Definitive Surgical Management: Principles and Approaches
The definitive treatment for OHVIRA syndrome is the resection of the obstructive longitudinal vaginal septum, with the primary goal being the immediate relief of obstruction and drainage of accumulated hematocolpos.82 This procedure aims to create a patent vaginal canal, allowing normal menstrual egress and resolving the acute symptoms of dysmenorrhea and pelvic pain.
Contemporary surgical approaches emphasize minimally invasive techniques. Vaginoscopic resection using a mini-resectoscope under ultrasound guidance has been described as an effective, hymen-sparing option that is particularly suitable for adolescents.82 Key surgical principles include: (1) Complete excision of the obstructive septum to prevent re-obstruction; (2) Preservation of unaffected anatomy, including the cervix and vaginal wall; (3) Meticulous hemostasis to reduce the risk of postoperative adhesion formation; (4) Confirmation of adequate drainage of hematocolpos intraoperatively. Timely surgical intervention is essential not only for symptom relief but also for halting the pathological progression that can lead to endometriosis, pelvic inflammatory disease, and irreversible adnexal damage.
Long-Term Follow-Up and Reproductive Health Protection
Surgical resection of the obstructive septum marks the beginning, not the end, of comprehensive patient management. A structured, long-term follow-up protocol is essential to ensure sustained success and protect future reproductive health. The postoperative management plan should include: (1) Regular clinical assessments to confirm complete and lasting resolution of dysmenorrhea and abnormal bleeding; Monitoring for potential complications such as vaginal adhesion or stenosis at the resection site, which may require additional intervention. (2) Follow-up ultrasound to assess the developmental status of the previously obstructed uterine horn and adnexa; Monitoring for any residual collections, hematometra, or signs of endometriosis. (3) Endometriosis is a known sequela of obstructive Müllerian anomalies due to chronic retrograde menstruation;82 If endometriosis is diagnosed (either preoperatively or postoperatively), appropriate medical or surgical management should be initiated. (4) Patients with Müllerian anomalies may have associated subfertility factors and increased obstetric risks (eg, preterm labor, malpresentation); Ongoing counseling regarding future reproductive options and the need for specialized obstetric care is a fundamental component of comprehensive care. (5) As affected adolescents transition to adulthood, coordinated transfer to adult gynecology or reproductive medicine services ensures continuity of care.
This holistic, lifespan-oriented approach ensures that successful surgical correction of an anatomical defect in adolescence translates into optimized reproductive health and informed life choices in adulthood, fulfilling the core objective of preserving fertility and quality of life (Table 1).
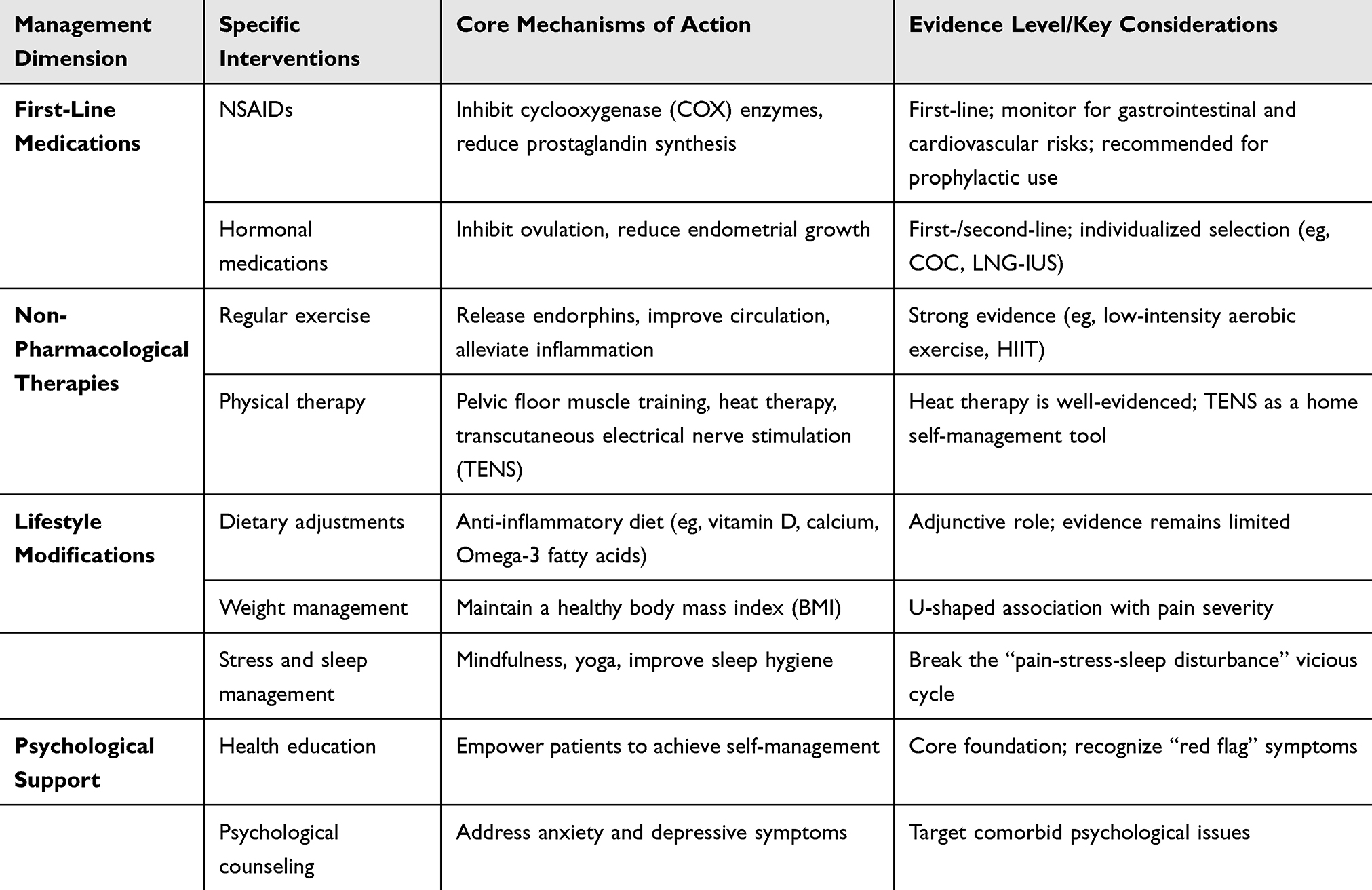 |
Table 1 Summary of Treatment Strategies: Stepped Long-Term Management Strategy for Primary Dysmenorrhea |
Discussion
The findings synthesized in this narrative review support a multidimensional, stepped-care approach to the long-term management of adolescent primary dysmenorrhea (PD). The outcome measures used in the studies cited in this review (including VAS, NPRS, EQ-5D, SF-36, and CMSS) have demonstrated acceptable reliability and validity in adolescent populations, as established in their respective validation studies. Below, we discuss key observations in relation to the evidence reviewed.
Integrating Pharmacological and Non-Pharmacological Strategies
The evidence consistently demonstrates that first-line pharmacological agents—NSAIDs and hormonal contraceptives—are effective for pain relief in PD.1,83 However, long-term reliance on medication alone is limited by concerns over adverse effects (eg, gastrointestinal, cardiovascular) and variable adherence.6,17 This review found growing evidence supporting the integration of non-pharmacological interventions. For example, a 2025 meta-analysis of RCTs confirmed that aerobic exercise significantly reduces pain intensity and duration in adolescents and young women with PD.11 Heat therapy, which is safe, low-cost, and patient-administered, was shown in a 2025 systematic review and meta-analysis to provide analgesic effects similar to NSAIDs while exhibiting a superior safety profile.81 These findings suggest that combining pharmacotherapy with physical modalities can enhance pain control while reducing medication burden—a particularly important consideration for adolescents requiring long-term management.
Mechanisms of Action for Key Interventions
The therapeutic effects of the interventions discussed in this review are mediated through distinct but potentially complementary biological mechanisms. Regular aerobic exercise alleviates dysmenorrhea primarily by stimulating the release of endogenous opioids (eg, endorphins), which act as natural analgesics; improving systemic and pelvic circulation to reduce uterine ischemia; and modulating stress hormones such as cortisol. Heat therapy promotes local vasodilation, increases blood flow to the uterine region, and activates spinal pain-gating mechanisms, thereby reducing the perception of cramping pain without systemic adverse effects. Transcutaneous electrical nerve stimulation (TENS) delivers low-voltage electrical currents to peripheral nerves, which is thought to inhibit pain transmission via the gate control theory of pain and to stimulate the release of endogenous opioids at both spinal and supraspinal levels. Nutritional supplements such as vitamin D and calcium may reduce prostaglandin synthesis and modulate uterine smooth muscle contractility through their roles in inflammatory regulation and calcium-dependent muscle relaxation. A summary of these mechanisms is also illustrated in Figure 1.
The Role of Lifestyle and Psychological Factors
Beyond direct pain relief, this review identified lifestyle modifications as important modulators of dysmenorrhea severity. Vitamin D and calcium status show an inverse relationship with pain scores, supported by a 2023 systematic review9 and multiple RCTs,4,9 although most studies are small and heterogeneous. Body mass index exhibits a U-shaped association with PD severity: a 2023 study in adolescents reported that both underweight and obese groups had significantly higher VAS pain scores than normal-weight peers.10 The relationship between psychological health and dysmenorrhea appears bidirectional. A 2025 school-based cross-sectional study found that adolescents with PD had higher rates of anxiety, depression, and poor sleep quality,13 while a 2025 RCT demonstrated that a stress-reduction lifestyle intervention significantly improved pain outcomes and heart rate variability.76 Although evidence for psychological interventions specifically in adolescent PD remains limited, extrapolation from adult chronic pain literature supports their inclusion as adjunctive strategies.75
Differentiating Primary from Secondary Causes
A critical clinical message from this review is the importance of systematic exclusion of secondary causes. OHVIRA syndrome, though rare (estimated prevalence <1%), is emblematic of the diagnostic challenges in this population. A 2026 case series and literature review found that delayed recognition of OHVIRA leads to preventable complications including endometriosis, tubo-ovarian abscess, and permanent adnexal damage.83 High-resolution ultrasound and MRI now allow accurate non-invasive diagnosis,36 and a 2024 study confirmed that definitive surgical resection of the obstructive septum can be curative when performed in a timely manner.37 These findings underscore that initial diagnostic evaluation is not merely an academic exercise but a prerequisite for appropriate long-term management.
Limitations
As a narrative review, this article has several inherent limitations. First, the literature search was not systematic, and we did not apply formal eligibility criteria or quality assessment tools, which may introduce selection bias. Second, the heterogeneity of study designs, outcome measures, and populations across the included literature precludes quantitative synthesis. Third, some recommendations are based on single studies or extrapolated from adult data, as high-quality evidence specifically in adolescents remains limited. Fourth, potential publication bias may have influenced the availability of positive findings. Finally, the review does not include a formal assessment of evidence certainty (eg, GRADE).
Future Directions
Future research should prioritize: (1) large-scale, high-quality randomized controlled trials of multi-modal intervention programs specifically in adolescents; (2) validation of standardized, age-appropriate long-term management pathways across diverse healthcare settings; (3) investigation of digital health tools (eg, mobile apps for symptom tracking and self-management support) to enhance engagement and adherence; (4) prospective studies on the natural history of primary dysmenorrhea and its transition to chronic pain conditions; and (5) cost-effectiveness analyses of integrated care models compared to conventional episodic care. Additionally, international consensus on core outcome sets for dysmenorrhea research in adolescents would facilitate meta-analyses and cross-study comparisons.
Conclusion
The long-term management of adolescent primary dysmenorrhea requires a systematic, multidimensional approach that extends beyond acute pain relief. Accurate differential diagnosis to exclude secondary causes such as OHVIRA syndrome is the essential first step. Evidence supports a stepped care model: first-line pharmacotherapy (NSAIDs, hormonal contraceptives) combined with non-pharmacological interventions (regular exercise, heat therapy, TENS) and foundational lifestyle modifications (healthy diet, weight management, stress reduction, adequate sleep). Empowering adolescents through health education to become active self-managers is a core determinant of long-term success. This integrated, patient-centered framework offers the greatest potential to reduce symptom burden, prevent chronicity, and preserve quality of life and future reproductive health.
Ethics
No human participants/research was involved in the production of this article.
Acknowledgments
The figures in the article as well as the material Created in BioRender. https://BioRender.com. Sincere thanks to BioRender.
Funding
Jointly Funded Project of Medical and Health Field in Sanming City (2025-S-116, 2025-S-125); Fujian Provincial Natural Science Foundation Project (2026J0011992).
Disclosure
The authors declare no competing interests in this work.
References
1. Panova DI, Boshku AA, Stankovic ZB. Primary dysmenorrhea in adolescents. Best Pract Res Clin Obstet Gynaecol. 2026;106:102717. doi:10.1016/j.bpobgyn.2026.102717
2. Donayeva A, Amanzholkyzy A, Abdelazim I, et al. The impact of primary dysmenorrhea on adolescents’ activities and school attendance. J Med Life. 2023;16(10):1462–19. doi:10.25122/jml-2023-0247
3. Jusuf EC, Octaviani D, Husain MG, Jumrah. The influence of physical activity, body mass index and urinary levels of prostaglandin (PGF2α) with the incidence of primary dysmenorrhea in adolescents. J Obstet Gynaecol Res. 2024;50(5):909–913. doi:10.1111/jog.15914
4. Donayeva A, Amanzholkyzy A, Abdelazim I, et al. The effects of vitamin D and calcium on primary dysmenorrhea: a systematic review. J Med Life. 2023;16(11):1597–1605. doi:10.25122/jml-2023-0248
5. Liu T, Qi D, Zhang L, et al. Academic stress and irregular menstruation influence the dysmenorrhea, school absenteeism and healthcare seeking among adolescent girls in junior high school in Shanghai: a cross-sectional study. Front Reprod Health. 2025;7:1574195. doi:10.3389/frph.2025.1574195
6. Akay E, Uzun Gül AD. OHVIRA syndrome: a case report treated with delayed diagnosis and multidisciplinary approaches. Taiwan J Obstet Gynecol. 2025;64(4):693–699. doi:10.1016/j.tjog.2024.08.014
7. Kirsch E, Rahman S, Kerolus K, et al. Dysmenorrhea, a narrative review of therapeutic options. J Pain Res. 2024;17:2657–2666. doi:10.2147/JPR.S459584
8. Donayeva A, Amanzholkyzy A, Nurgaliyeva R, et al. Vitamin D and vitamin D receptor polymorphism in Asian adolescents with primary dysmenorrhea. BMC Womens Health. 2023;23(1):414. doi:10.1186/s12905-023-02569-9
9. Abdi F, Amjadi MA, Zaheri F, Rahnemaei FA. Role of vitamin D and calcium in the relief of primary dysmenorrhea: a systematic review. Obstet Gynecol Sci. 2021;64(1):13–26. doi:10.5468/ogs.20205
10. Donayeva A, Amanzholkyzy A, Nurgaliyeva R, Gubasheva G, Abdelazim IA, Samaha II. The relation between primary dysmenorrhea in adolescents and body mass index. Prz Menopauzalny. 2023;22(3):126–129. doi:10.5114/pm.2023.131314
11. Abdelrahman AY, El-Kosery SM, Abbassy AH, Botla AM. Effect of aquatic exercise versus aerobic exercise on primary dysmenorrhea and quality of life in adolescent females: a randomized controlled trial. Physiother Res Int. 2024;29(3):e2095. doi:10.1002/pri.2095
12. Kabukçu C, Kabukçu Başay B, Başay Ö. Primary dysmenorrhea in adolescents: association with attention deficit hyperactivity disorder and psychological symptoms. Taiwan J Obstet Gynecol. 2021;60(2):311–317. doi:10.1016/j.tjog.2021.01.033
13. Gambadauro P, Hadlaczky G, Wasserman D, Carli V. Dysmenorrhea and adolescent mental health: a school-based cross-sectional study. BJOG. 2025;132(9):1278–1284. doi:10.1111/1471-0528.18187
14. Cameron L, Mikocka-Walus A, Stanley K, et al. The relationship between menstrual pain in adolescence and mental health in adolescence and early adulthood. J Psychosom Res. 2025;192:112122. doi:10.1016/j.jpsychores.2025.112122
15. Liu H, Han D, Hu Y, Huang L, Wang J, Zhu D. Association between stress and dysmenorrhea among Chinese female adolescent students: a cross-sectional epidemiology study. Sci Rep. 2025;15(1):22180. doi:10.1038/s41598-025-05152-4
16. Chiang YF, Hung HC, Chen HY, et al. The inhibitory effect of extra virgin olive oil and its active compound oleocanthal on prostaglandin-induced uterine hypercontraction and pain-ex vivo and in vivo study. Nutrients. 2020;12(10):3012. doi:10.3390/nu12103012
17. Tang Y, Pan W, Ding W, et al. Prostaglandin E2 alleviates inflammatory response and lung injury through EP4/cAMP/IKK/NF-κB pathway. Biochim Biophys Acta Mol Basis Dis. 2025;1871(5):167801. doi:10.1016/j.bbadis.2025.167801
18. Clemenza S, Vannuccini S, Capezzuoli T, Meleca CI, Pampaloni F, Petraglia F. Is primary dysmenorrhea a precursor of future endometriosis development? Gynecol Endocrinol. 2021;37(4):287–293. doi:10.1080/09513590.2021.1878134
19. Fu Q, Yang J, Jiang H, et al. Effect of photobiomodulation on alleviating primary dysmenorrhea caused by PGF2α. J Biophotonics. 2024;17(5):e202300448. doi:10.1002/jbio.202300448
20. Su X, Liu H, Wang H, et al. Brain morphological changes and associated functional connectivity and lag structures in women with primary dysmenorrhea during the pain-free periovulatory phase. J Pain. 2025;31:105419. doi:10.1016/j.jpain.2025.105419
21. Xia F-Y, Liu Y, Zhong Y, et al. Effect of electroacupuncture on cannabinoid-related receptor CB2R and TRPV1 and spinal microglial polarization in rats with primary dysmenorrhea. Zhen Ci Yan Jiu. 2025;50(11):1248–1256. doi:10.13702/j.1000-0607.20250615
22. Song HH, Song TC, Yang T, et al. High mobility group box 1 mediates inflammatory response of astrocytes via cyclooxygenase 2/prostaglandin E2 signaling following spinal cord injury. Neural Regen Res. 2021;16(9):1848–1855. doi:10.4103/1673-5374.303039
23. Gorica E, Calderone V. Arachidonic acid derivatives and neuroinflammation. CNS Neurol Disord Drug Targets. 2022;21(2):118–129. doi:10.2174/1871527320666210208130412
24. Zhang YY, Yao YD, Luo JF, et al. Microsomal prostaglandin E2 synthase-1 and its inhibitors: molecular mechanisms and therapeutic significance. Pharmacol Res. 2022;175:105977. doi:10.1016/j.phrs.2021.105977
25. Yang MY, Chen HY, Ho CH, Huang WC. Impact of probiotic supplementation and high-intensity interval training on primary dysmenorrhea: a double-blind, randomized controlled trial investigating inflammation and hormonal modulation. Nutrients. 2025;17(4):622. doi:10.3390/nu17040622
26. Gutman G, Nunez AT, Fisher M. Dysmenorrhea in adolescents. Curr Probl Pediatr Adolesc Health Care. 2022;52(5):101186. doi:10.1016/j.cppeds.2022.101186
27. Nie W, Xu P, Hao C, Chen Y, Yin Y, Wang L. Efficacy and safety of over-the-counter analgesics for primary dysmenorrhea: a network meta-analysis. Medicine. 2020;99(19):e19881. doi:10.1097/MD.0000000000019881
28. Dai Y, Luo H, Zhu L, et al. Dysmenorrhea pattern in adolescences informing adult endometriosis. BMC Public Health. 2024;24(1):373. doi:10.1186/s12889-024-17825-2
29. de Kok L, Boersen Z, Coppus S, et al. Diagnostic delay in endometriosis: is there any progress? Reprod Biomed Online. 2025;53(1):105405. doi:10.1016/j.rbmo.2025.105405
30. Rohan P, Common M, Ryan J, Mulholland D, O’Shea A. Multimodality imaging findings in secondary dysmenorrhea. Clin Radiol. 2025;86:106927. doi:10.1016/j.crad.2025.106927
31. Martire FG, Piccione E, Exacoustos C, Zupi E. Endometriosis and adolescence: the impact of dysmenorrhea. J Clin Med. 2023;12(17):5624. doi:10.3390/jcm12175624
32. Begum IA. The connection between endometriosis and secondary dysmenorrhea. J Reprod Immunol. 2025;168:104425. doi:10.1016/j.jri.2025.104425
33. Gudapati S, Chaudhari K, Dave A, Shinde D. An incidental diagnosis of Herlyn-Werner-Wunderlich syndrome in a young female: a case report of a rare entity. Cureus. 2024;16(1):e53227. doi:10.7759/cureus.53227
34. Zarfati A, Lucchetti MC. OHVIRA (Obstructed Hemivagina and Ipsilateral Renal Anomaly or Herlyn-Werner-Wunderlich syndrome): is it time for age-specific management? J Pediatr Surg. 2022;57(11):696–701. doi:10.1016/j.jpedsurg.2022.04.002
35. Monteiro Dos Santos Figueiredo J, Figueiredo J. Herlyn-Werner-Wunderlich (HWW) syndrome in an adolescent. Cureus. 2025;17(11):e96788. doi:10.7759/cureus.96788
36. Fazecas T, Paiva Lopes F, Gedeon B, Daltro P, Goulart Corrêa D. Utility of non-contrast transperineal ultrasound for the evaluation of pediatric disorders. Pediatr Radiol. 2025;55(13):2730–2744. doi:10.1007/s00247-025-06432-x
37. Ball S, Fisher J. Adolescent abdominal pain due to rare mullerian duct anomaly. Am J Emerg Med. 2022;59:218.e1–218.e3. doi:10.1016/j.ajem.2022.06.032
38. Fontana V, Aboud GS, Sabbaj L. Síndrome de Herlyn-Werner Wünderlich: reporte de dos casos [Herlyn-Werner-Wünderlich syndrome: two case report]. Arch Argent Pediatr. 2024;122(4):e202310138. doi:10.5546/aap.2023-10138.eng
39. Ferries-Rowe E, Corey E, Archer JS. Primary dysmenorrhea: diagnosis and therapy. Obstet Gynecol. 2020;136(5):1047–1058. doi:10.1097/AOG.0000000000004096
40. Christelle K, Norhayati MN, Jaafar SH. Interventions to prevent or treat heavy menstrual bleeding or pain associated with intrauterine-device use. Cochrane Database Syst Rev. 2022;8(8):CD006034. doi:10.1002/14651858.CD006034.pub3
41. Guimarães I, Póvoa AM. Dismenorreia primária: avaliação e tratamento [Primary Dysmenorrhea: assessment and Treatment]. Rev Bras Ginecol Obstet. 2020;42(8):501–507. doi:10.1055/s-0040-1712131
42. Itani R, Soubra L, Karout S, Rahme D, Karout L, Khojah HMJ. Primary dysmenorrhea: pathophysiology, diagnosis, and treatment updates. Korean J Fam Med. 2022;43(2):101–108. doi:10.4082/kjfm.21.0103
43. Ma W, Qiu L, Dong Y, Zhou H. Complementary and alternative therapies in the treatment of primary dysmenorrhea. Front Reprod Health. 2026;7:1730164. doi:10.3389/frph.2025.1730164
44. Mardon AK, Whitaker L, Farooqi T, et al. Investigational drugs for the treatment of dysmenorrhea. Expert Opin Investig Drugs. 2024;33(4):347–357. doi:10.1080/13543784.2024.2326627
45. Schettino MT, Vastarella MG, Riemma G, Dores E, Turco F, De Franciscis P. Acmella oleracea and Boswellia serrata for symptom relief and reduced analgesic use in women with dysmenorrhea. Womens Health Rep. 2025;6(1):652–659. doi:10.1089/whr.2025.0056
46. Yuan D, Liu Y, Chen Z, et al. Heat therapy for primary dysmenorrhea: a systematic review and meta-analysis. Front Med. 2026;12:1730505. doi:10.3389/fmed.2025.1730505
47. Negi R, Sharma SK, Gaur R, Bahadur A, Jelly P. Efficacy of ginger in the treatment of primary dysmenorrhea: a systematic review and meta-analysis. Cureus. 2021;13(3):e13743. doi:10.7759/cureus.13743
48. Li G, Liu A, Lin M, Liao S, Wen Z. Chinese herbal formula siwutang for treating primary dysmenorrhea: a systematic review and meta-analysis of randomized controlled trials. Maturitas. 2020;138:26–35. doi:10.1016/j.maturitas.2020.03.009
49. Ramos-Pichardo JD, Ortega-Galán ÁM, Iglesias-López MT, Abreu-Sánchez A, Fernández-Martínez E. Why do some Spanish nursing students with menstrual pain fail to consult healthcare professionals? Int J Environ Res Public Health. 2020;17(21):8173. doi:10.3390/ijerph17218173
50. McKenna KA, Fogleman CD. Dysmenorrhea. Am Fam Physician. 2021;104(2):164–170.
51. Schroll JB, Black AY, Farquhar C, Chen I. Combined oral contraceptive pill for primary dysmenorrhoea. Cochrane Database Syst Rev. 2023;7(7):CD002120. doi:10.1002/14651858.CD002120.pub4
52. Wang J, Deng K, Li L, Dai Y, Sun X. Levonorgestrel-releasing intrauterine system vs. systemic medication or blank control for women with dysmenorrhea: systematic review and meta-analysis of randomized controlled trials. Front Glob Womens Health. 2022;3:1013921. doi:10.3389/fgwh.2022.1013921
53. Samy A, Taher A, Sileem SA, et al. Medical therapy options for endometriosis related pain, which is better? A systematic review and network meta-analysis of randomized controlled trials. J Gynecol Obstet Hum Reprod. 2021;50(1):101798. doi:10.1016/j.jogoh.2020.101798
54. Cai J, Liu M, Jing Y, Yin Z, Kong N, Guo C. Aerobic exercise to alleviate primary dysmenorrhea in adolescents and young women: a systematic review and meta-analysis of randomized controlled trials. Acta Obstet Gynecol Scand. 2025;104(5):815–828. doi:10.1111/aogs.15042
55. Navinbhai PD, B M, N SS. Comparative effect of Kegel and Pelvic rocking exercises on primary dysmenorrhea: a quasi-experimental study. Bioinformation. 2025;21(10):3531–3535. doi:10.6026/973206300213531
56. Huang WC, Chiu PC, Ho CH. The sprint-interval exercise using a spinning bike improves physical fitness and ameliorates primary dysmenorrhea symptoms through hormone and inflammation modulations: a randomized controlled trial. J Sports Sci Med. 2022;21(4):595–607. doi:10.52082/jssm.2022.595
57. Deodato M, Grosso G, Drago A, et al. Efficacy of manual therapy and pelvic floor exercises for pain reduction in primary dysmenorrhea: a prospective observational study. J Bodyw Mov Ther. 2023;36:185–191. doi:10.1016/j.jbmt.2023.07.002
58. Teoh BK, Romero SSB, Quach TVB, Chung HY, Chen YH. The synergistic effect of heat therapy and electroacupuncture treatment in inflammatory pain mouse models. Brain Sci. 2025;15(8):822. doi:10.3390/brainsci15080822
59. Park S, Kim H, Jung J, Lee S. Effects of sacroiliac joint manipulation on autonomic nervous system and lower abdominal pain in women with primary dysmenorrhoea: a randomized controlled trial. Medicina. 2024;60(12):2068. doi:10.3390/medicina60122068
60. Xing R, Yang J, Wang R, Wang Y. Extracorporeal shock wave therapy for treating primary dysmenorrhea: a randomized controlled trial. Medicine. 2021;100(5):e23798. doi:10.1097/MD.0000000000023798
61. Al Hassan RM, Abdullah NM, Al Tawry AMJ. Evaluation of electromagnetic therapy in the treatment of severe dysmenorrhea in young women of Basrah. Ann Afr Med. 2024;23(2):189–193. doi:10.4103/aam.aam_46_23
62. Han S, Park KS, Lee H, et al. Transcutaneous electrical nerve stimulation (TENS) for pain control in women with primary dysmenorrhoea. Cochrane Database Syst Rev. 2024;7(7):CD013331. doi:10.1002/14651858.CD013331.pub2
63. Manisha U, Anuradha L. Effect of high frequency transcutaneous electrical nerve stimulation at root level menstrual pain in primary dysmenorrhea. J Bodyw Mov Ther. 2021;26:108–112. doi:10.1016/j.jbmt.2020.12.025
64. Rodrigues JC, Avila MA, Driusso P. Transcutaneous electrical nerve stimulation for women with primary dysmenorrhea: study protocol for a randomized controlled clinical trial with economic evaluation. PLoS One. 2021;16(5):e0250111. doi:10.1371/journal.pone.0250111
65. Liu W, Ding Y, Xie H, Liu H, Liang C. Efficacy and safety of transcutaneous electrical acupoint stimulation for the management of primary dysmenorrhoea: protocol for a randomised controlled trial in China. BMJ Open. 2024;14(6):e078895. doi:10.1136/bmjopen-2023-078895
66. Rodrigues JC, de Arruda GT, de Moraes PC, Firão CB, Avila MA, Driusso P. Self-management of primary dysmenorrhea-related pain: cross-sectional study on non-pharmacological interventions. Pain Manag. 2024;14(5–6):265–272. doi:10.1080/17581869.2024.2376519
67. MacGregor B, Allaire C, Bedaiwy MA, Yong PJ, Bougie O. Disease Burden of Dysmenorrhea: impact on Life Course Potential. Int J Womens Health. 2023;15:499–509. doi:10.2147/IJWH.S380006
68. Bansal K, Sharma S, Bajpai M. Herbal medicines - a fruitful approach to periodic illness dysmenorrhoea: evidence-based review. Curr Pharm Biotechnol. 2023;25:179–195. doi:10.2174/1389201024666230623161113
69. Chen B, Liu S, Jin F, et al. Efficacy of acupuncture-related therapy in the treatment of primary dysmenorrhea: a network meta-analysis of randomized controlled trials. Heliyon. 2024;10(10):e30912. doi:10.1016/j.heliyon.2024.e30912
70. Xu WW, Teng ZQ, Wan QQ, Shao XM, Tian HF. Herbs-partitioned moxibustion on the navel in a rat model of primary dysmenorrhea with cold coagulation and blood stasis. J Vis Exp. 2024;(212):e66622. doi:10.3791/66622
71. Sitong X, Chenglong W, Caiyue L, Deyuan Q, Zujie Q, Chen L. Medicated thread moxibustion therapy of Zhuang medicine and its application in a rat model of cold-congealing syndrome of primary dysmenorrhea. J Vis Exp. 2024;(203):e65669. doi:10.3791/65669
72. Amanak K. Effects of dry figs on primary dysmenorrhea symptoms, perceived stress levels and the quality of life. P R Health Sci J. 2020;39(4):319–326.
73. Mizgier M, Więckowska B, Sansoni V, et al. Risk factors of primary dysmenorrhea in female adolescent basketball players related to dietary, hormonal, and immuno-metabolic factors and disordered eating attitudes. Nutrients. 2025;17(7):1190. doi:10.3390/nu17071190
74. Wu L, Zhang J, Tang J, Fang H. The relation between body mass index and primary dysmenorrhea: a systematic review and meta-analysis. Acta Obstet Gynecol Scand. 2022;101(12):1364–1373. doi:10.1111/aogs.14449
75. Lee H, Kim J. Direct and indirect effects of stress and self-esteem on primary dysmenorrhea in Korean adolescent girls: a cross-sectional survey study. Iran J Public Health. 2024;53(1):116–125. doi:10.18502/ijph.v53i1.14688
76. Silwal K, Kodali PB, Sharma H, et al. Efficacy of Arogya Rakshak Panchatantra (Five Lifestyle Principles) on heart rate variability and menstrual symptoms in primary dysmenorrhea: a randomized controlled trial. J Integr Complement Med. 2025;31(5):471–482. doi:10.1089/jicm.2024.0216
77. Jiangzhou H, Xu H, Wen Y, et al. Association between primary dysmenorrhea and mental health traits: a study based on multi-phenotype correlation network and Mendelian randomization analysis in female college students. Phenomics. 2025;5(5):502–517. doi:10.1007/s43657-024-00213-6
78. Silva GD, Canova NAH, Bortoletto P, Wutzke MLS, Dos Santos Soares F, Bertolini GRF. Cryotherapy produces pain relief in young people with primary dysmenorrhea. Ther Hypothermia Temp Manag. 2022;12(2):57–60. doi:10.1089/ther.2021.0002
79. Khalajinia Z, Falahieh FM, Aghaali M. The effects of chamomile and flaxseed on pelvic pain, dyspareunia, and dysmenorrhea in endometriosis: a controlled randomized clinical trial. Iran J Nurs Midwifery Res. 2024;29(6):731–736. doi:10.4103/ijnmr.ijnmr_110_23
80. Weng N, Munro C, Grover SR. Parental understanding of menstrual problems in their adolescent child: a narrative review✰. J Pediatr Adolesc Gynecol. 2026;S1083–3188(26)00314–1. doi:10.1016/j.jpag.2026.02.004
81. Wang Y, Li S, Zhang Y, et al. Heat and cold therapy reduce pain in patients with delayed onset muscle soreness: a systematic review and meta-analysis of 32 randomized controlled trials. Phys Ther Sport. 2021;48:177–187. doi:10.1016/j.ptsp.2021.01.004
82. Moufawad G, Giannini A, D’Oria O, et al. Obstructed hemivagina and ipsilateral renal anomaly syndrome: a systematic review about diagnosis and surgical management. Gynecol Minim Invasive Ther. 2023;12(3):123–129. doi:10.4103/gmit.gmit_103_22
83. Yang JS, Park JE, Jo HC. Recurrent vulvovaginitis as an unusual presentation of diagnosed Obstructed Hemivagina and Ipsilateral Renal Anomalies (OHVIRA) syndrome in an adolescent: a case report and review of the literature. J Clin Med. 2026;15(2):440. doi:10.3390/jcm15020440
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.