Back to Journals » Clinical Ophthalmology » Volume 10
Long-term follow-up for bimanual microincision cataract surgery: comparison of results obtained by surgeons in training and experienced surgeons
Authors Cavallini G, Verdina T ![]() , Forlini M, Volante V, De Maria M
, Forlini M, Volante V, De Maria M ![]() , Torlai G, Benatti C, Delvecchio G
, Torlai G, Benatti C, Delvecchio G
Received 3 January 2016
Accepted for publication 3 March 2016
Published 26 May 2016 Volume 2016:10 Pages 979—987
DOI https://doi.org/10.2147/OPTH.S103540
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Gian Maria Cavallini, Tommaso Verdina, Matteo Forlini, Veronica Volante, Michele De Maria, Giulio Torlai, Caterina Benatti, Giancarlo Delvecchio
Institute of Ophthalmology, University of Modena and Reggio Emilia, Modena, Italy
Purpose: To determine the efficacy of bimanual microincision cataract surgery (B-MICS) performed by surgeons in training, evaluating clinical results, posterior capsule opacification (PCO) incidence, and clear corneal incision (CCI) architecture in a long-term follow-up and comparing results with those obtained by experienced surgeons.
Patients and methods: Eighty eyes of 62 patients operated on by three surgeons in training who used B-MICS technique for the first time were included in the study (Group A). Eighty eyes of 59 patients who underwent B-MICS by three experienced surgeons were included as a control group (Group B). Best corrected visual acuity, astigmatism, corneal pachymetry, and endothelial cell count were evaluated before surgery and at 1 month and 18 months after surgery. Anterior segment optical coherence tomography images were obtained to study the morphology of CCIs. PCO incidence was evaluated using EPCO2000 software.
Results: Out of 160 surgeries included in the study, mean best-corrected visual acuity improvement at 18 months was 0.343±0.246 logMAR for Group A, and 0.388±0.175 logMAR for Group B, respectively. We found no statistically significant induced astigmatism nor corneal pachymetry changes in either group, while we noticed a statistically significant endothelial cell loss postoperatively in both groups (P<0.05). In Group A, mean PCO score was 0.163±0.196, while for Group B, it was 0.057±0.132 (P=0.0025). Mean length and inclination of the CCIs for Group A and Group B were, respectively, 1,358±175 µm and 1,437±256 µm and 141.8°±6.4° and 148.7°±5.1°. As regards corneal architecture in the 320 CCIs considered, we found posterior wound retractions and endothelial gaps, respectively, 9.8% and 11.6% for Group A and 7.8% and 10.8% for Group B.
Conclusion: B-MICS performed by surgeons in training is an effective surgical technique even when assessed after a long-term follow-up. PCO incidence resulted in being higher for less experienced surgeons. Corneal incisions were shorter and less angled in surgeons in training in comparison with results obtained by expert surgeons.
Keywords: small incisions, learning curve, B-MICS, clear corneal incisions, posterior capsule opacification
Introduction
Bimanual microincision cataract surgery (B-MICS) is a microinvasive variant of the traditional coaxial phacoemulsification,1 and it is characterized by the separation of the aspiration and the infusion probes: this enables clear corneal incisions (CCIs) of ≤1.5 mm, the smallest incisions in cataract surgery.2–4
The article recently published by our group5 showed that B-MICS is a safe and effective technique even when performed by surgeons in training assessed in a 1-month follow-up, and it may be no more difficult to learn than the traditional coaxial technique. B-MICS features such as the increased stability of the anterior chamber, the chance to use both right and left hand for the procedures directing the instruments as required, the greater visibility of the surgical field due to the small size of the instruments, are extremely helpful, especially for surgeons approaching cataract surgery for the first time.6
We know that posterior capsule opacification (PCO) is still one of the main long-term complications and one of the most common causes of nonrefractive decreased postoperative vision following lens implantation, especially for hydrophilic intraocular lens (IOLs).7 According to the literature, there is some debate regarding the importance of an accurate posterior capsule cleaning for the prevention of this alteration.8
Even the architecture of the CCIs seems to be important for cataract surgery outcomes during the follow-up.9,10
Considering the results obtained in our previous study, we decided to re-examine a group of patients to evaluate the results in a long-term follow-up (18 months) considering the same preoperative parameters such as visual acuity, astigmatism, corneal thickness, and endothelial cell count. To date, there are no studies investigating the effectiveness of B-MICS in a group of surgeons in training with a long-term follow-up. Moreover, we evaluated PCO incidence and CCIs architecture with anterior segment optical coherence tomography (AS-OCT). There are no studies investigating these alterations for surgeons in training using B-MICS technique. We compared the results with those obtained by expert surgeons for a similar group of patients.
Patients and methods
We evaluated 80 eyes of 62 patients who underwent cataract extraction by three surgeons in training (VV, MF, and TV) during their first experience with B-MICS at the Institute of Ophthalmology, University of Modena & Reggio Emilia (Group A); all the surgeries had an 18-month follow-up. All the operations were carried out with B-MICS technique under the direct supervision of an expert surgeon (who had the task of guidance and possible intervention if required). The surgeons used B-MICS technique for the first time with very little previous experience in coaxial technique. We also evaluated 80 eyes of 59 patients operated by three expert surgeons (GMC, GD, and GN) as a comparison group (Group B). In both groups, surgeons used the same B-MICS technique. Patients in both groups were similar for age and cataract characteristics.
All the operated eyes had cataracts from grades 2 to 3 in the Lens Opacities Classification System III. Exclusion criteria were eyes with previous surgery, complicated cataract (eg, total cataract and traumatic cataract), concomitant pathologies (uveitis, glaucoma, and corneal opacities), insufficient mydriasis (<4 mm), low endothelial cell count (<1,500 cells/mm2), and patients with only one eye. We also excluded patients with any ocular pathology during follow-up not related to the surgery.
Prior to surgery, all patients underwent a careful clinical history evaluation, best-corrected visual acuity (BCVA) examination, anterior segment biomicroscopy, fundus examination, biometry (performed with both IOL Master; Carl Zeiss Meditec AG, Jena, Germany, and US500 Echoscan; Nidek Co., Ltd., Gamagori, Japan), corneal microscopy (Noncon Robo CA; Konan, Hyogo, Japan), corneal pachymetry (IOPac; Heidelberg Engineering, Heidelberg, Germany), and corneal topography (CT1000; Shin Nippon, Tokyo, Japan). Every surgeon performed operations using the same phaco machine (Stellaris, Bausch & Lomb, NY, USA).
Prophylactic strategies in preventing infections included applying topical antibiotic eyedrops before surgery, applying 5% povidone iodine to the conjunctival cul-de-sac, preparing the periocular skin with 10% povidone iodine, careful sterile draping of the eyelid margins and eyelashes, adding antibiotics to the irrigating solution, instilling intracameral antibiotics at the end of surgery, and applying topical antibiotic eyedrops after surgery.
Surgical technique
Prior to a consistent mydriasis obtained with instillation of 10% phenylephrine and 1% cyclopentolate and locoregional anasthesia with peribulbar block (2.5 mL of lidocaine 2% and 2.5 mL of bupivacaine 0.5%), two 1.4 mm trapezoidal incisions were performed in the clear cornea at 10 o’clock and 2 o’clock with a precalibrated diamond knife (ME 772 DA, E Janach, Como, Italy). A continuous curvilinear capsulorhexis was made with a cystotome and microforceps (E Janach); hydrodissection was performed with 26 G cannula and phacoemulsification with a 20 G, 30° angled sleeveless probe, and an irrigating chopper (Bragamele 19 G). Phacofracture was obtained by the stop-and-chop technique. Irrigation/aspiration was performed with a 21 G probe with an oval-shaped section (21 G irrigation handpiece smooth, Stellaris; 21 G aspiration handpiece rough, Bausch & Lomb). All surgeons in training used continued infusion during phacoemulsification and irrigation/aspiration (I/A). The 10 o’clock incision was enlarged to 1.8 mm with a precalibrated knife (Alio’s MICS “multi-incision knife”) and IOL was implanted; the incisions were hydrosutured and, if necessary, sutured with nylon 10/0.
Postoperative therapy consisted of tobramycin and dexamethasone eye drops four times a day for 15 days, followed by flurbiprofen eye drops three times a day for a further 15 days. The study adhered to the tenets of the Declaration of Helsinki and was approved by the University of Modena and Reggio Emilia ethics committee. All patients provided informed consent before surgery.
Long-term outcomes
Postoperative results have been evaluated at 30 days and 18 months in terms of BCVA, corneal pachymetry, corneal astigmatism, and endothelial microscopy with the instruments previously described. All these examinations have been performed by the same experienced physician.
PCO incidence
We evaluated PCO incidence using the computer-based software Evaluation of Posterior Capsule Opacification 2000 (EPCO2000). This software is based on morphological assessment of PCO and allows a quantitative and qualitative evaluation of the amount of IOL surface affected by opacification (Figure 1). For every patient, we took retroillumination images of the pseudophakic anterior segments of the eyes affected, following dilation of the pupil. We used a camera connected to the slit lamp. Then, we used EPCO2000 to evaluate each picture giving us a final PCO score for every eye examined. The PCO score for each eye is calculated by multiplying the density of the opacification, graded from 0 (none) to 4 (severe), by the fractional PCO area involved behind the entire IOL optics.11 Density areas are identified and marked interactively by the observer on the computer screen. The evaluation was always made by the same expert observer. The neodymium-doped yttrium aluminum garnet (Nd:YAG) laser capsulotomy rate was recorded.
 | Figure 1 PCO analysis with EPCO2000 software in two study cases. |
CCIs evaluation
For every patient, we performed an AS-OCT (Optos OCT SLO; Optos Inc., Marlborough, MA, USA) to evaluate CCIs. In particular, we evaluated length and inclination of the incisions by calculating the angle between the line passing through the incision and the line tangential to the corneal plane using specialized OCT software for both groups (Figure 2). We also evaluated the presence of other microstructural features such as endothelial gap, posterior wound retraction (PWR, defined as a step off or recession of the limbal edge of the posterior wound surface), epithelial gap, Descemet’s stripping (DS), and corneal misalignment, as previously described.9,10
 | Figure 2 Microincision length and angle as measured with AS-OCT. |
All data have been recorded in an Excel database (Microsoft Excel 2010, Microsoft Office Professional Plus 2010), and for analysis, we used Stata 13.1 software (StataCorp LP, College Station, TX, USA) with Student’s t-test and Wilcoxon rank sum test. A P-value <0.05 was considered to indicate statistical significance. For postoperative results analysis, we also used one-way analysis of variance with a Bonferroni correction for multiple testing; normality of data was verified by Shapiro–Wilk test.
Results
For Group A, 80 eyes (38 right eyes and 42 left eyes) of 62 patients (29 males and 33 females) were included in the study; the average age was 76.7±7.1 years (range 62–88 years). An Akreos MI60 IOL was implanted in every eye. Seventy-eight IOLs were implanted in the bag, while two were implanted in the sulcus due to intraoperative complications. We recorded a mean total surgical time of 27.32±6.18 minutes. Mean final size of the enlarged incision was 1.77±0.09 mm.
For Group B, 80 eyes (41 right eyes and 39 left eyes) of 59 patients (26 males and 33 females) were included in the study; the average age was 74.2±7.8 years (range 60–89 years). An Akreos MI60 IOL was implanted in every eye always in the bag. We recorded a mean total surgical time of 16.21±5.07 minutes. Mean final size of the enlarged incision was 1.73±0.10 mm.
Postoperative results
In Group A, we found a mean BCVA of 0.013±0.031 logMAR at 30 days and 0.066±0.161 logMAR at 18 months, with a statistically significant improvement from mean BCVA at baseline (0.408±0.183 logMAR). Visual acuity reduction during 17 months of follow-up was 0.053±0.161 logMAR, and this was statistically significant (P=0.004). In the control group (Group B), we found a mean BCVA improvement of 0.28±0.097 at 30 days and 0.037±0.108 logMAR at 18 months, with a statistically significant improvement from mean BCVA at baseline (0.410±0.130 logMAR). The reduction in visual acuity during the follow-up was 0.009±0.037 logMAR, and this was not statistically significant (P=0.61; Tables 1 and 2). Using Spearman correlation coefficients, we found that the improvement in visual acuity at 18 months was similar in the two groups (r=−0.19, P=0.029), while the reduction in visual acuity during the follow-up was significantly higher in the training group (r=−0.27, P=0.002).
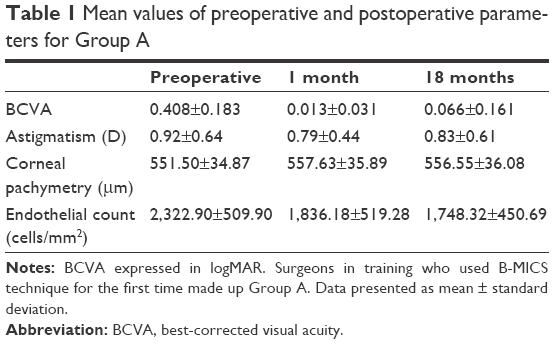 | Table 1 Mean values of preoperative and postoperative parameters for Group A |
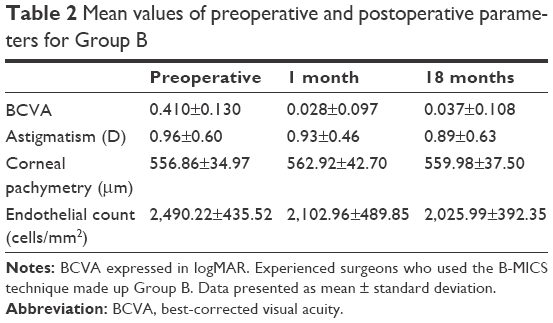 | Table 2 Mean values of preoperative and postoperative parameters for Group B |
With regard to astigmatism, in Group A, we found a mean decrease of 0.09±0.52 D at 18 months after surgery, while for Group B, this was 0.07±0.46 D, both not statistically significant. Regarding corneal pachymetry, we recorded final mean increase of 5.05±24.09 μm and of 3.12±21.75 μm at 18 months, respectively, for Group A and Group B; still not statistically significant for both groups.
Finally, with regard to the endothelial cell count in Group A, we obtained mean values of 1,836.18±450.69 cells/mm2 at 1 month and 1,748.32±450.69 cells/mm2 at 18 months as compared with a mean preoperative count of 2,322.90±509.90 cells/mm2. In Group B, we obtained mean values of 2,102.96±489.85 cells/mm2 at 1 month and 2,025.99±392.35 cells/mm2 at 18 months as compared with a mean preoperative count of 2,490.22±435.52 cells/mm2. Therefore, at 18-month follow-up, we found a mean endothelial cell loss of 574.58±530.39 cells/mm2 (21.7%, range 0%–46%) for Group A and of 464.23±511.98 cells/mm2 (16.4%, range 0%–38%) from surgery, a reduction that is statistically significant (P<0.05) in both groups. Using a nonparametric test, we found that the training group had a significantly superior endothelial cell loss than that found by the expert surgeons at 1 month (P=0.04). No statistically significant cell loss was found between the first and the 18th month from surgery in both groups.
Mean values obtained are reported in Tables 1 and 2.
PCO incidence
PCO score in Group A was higher (0.163±0.196) than that in group B (0.058±0.133), and the difference was statistically significant (P=0.002).
PCO was registered in 36 cases (45%) for Group A and 21 cases (27.5%) for Group B; however, visual axis was involved only in a few cases, and Nd:YAG laser capsulotomy at 18 months was necessary only in four cases (5%) for Group A and in two cases (2.5%) for Group B. Detailed results are reported in Table 3.
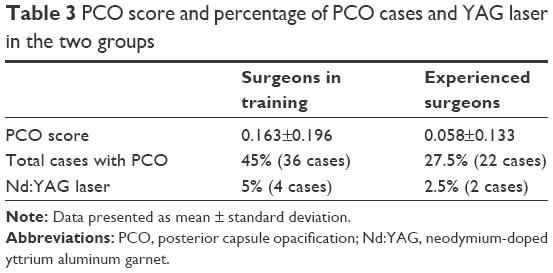 | Table 3 PCO score and percentage of PCO cases and YAG laser in the two groups |
CCIs evaluations
Using AS-OCT, we found that CCIs in Group A had lower values both for length (1,318±194 μm) and inclination (141.8°±6.4°) in comparison with those in Group B (respectively, 1,427±244 μm and 148.4°±5.4°), and the difference was statistically significant (P<0.05).
Moreover, within Group A, we divided the cases with iris prolapse from those without iris prolapse: in the first group (nine cases), CCIs were shorter and less angled (1,202±175 μm and 136.8°±7.6°) than in those cases (71 cases) without iris incarcerations (1,369±299 μm 144.4°±5.2°), and the difference was statistically significant (P<0.05).
Tables 4 and 5 show all CCIs mean values.
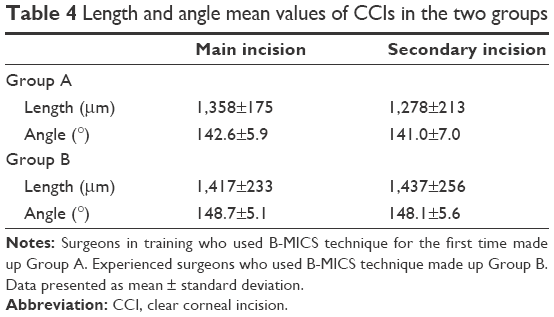 | Table 4 Length and angle mean values of CCIs in the two groups |
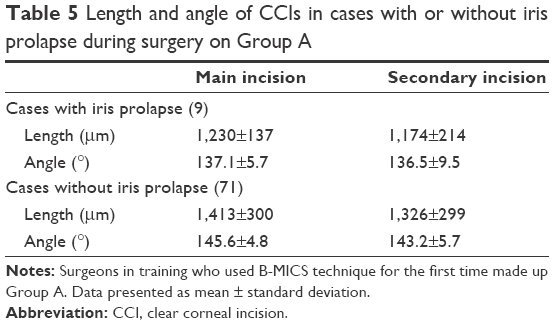 | Table 5 Length and angle of CCIs in cases with or without iris prolapse during surgery on Group A |
Finally, regarding morphological features of the CCIs at AS-OCT, we found mainly endothelial gaps and PWRs (respectively, 9.8% and 11.6% for Group A and 7.8% and 10.8% for Group B). Moreover, we found 0.8% epithelial gap, 0.8% DS, and 0.8% corneal misalignment in Group A (one case for each type of alterations); we did not find any of these features in Group B.
Figure 3 shows some cases, and in Table 6 all the alterations are reported for both groups considered.
 | Figure 3 Anterior segment OCT scans showing morphological alterations. |
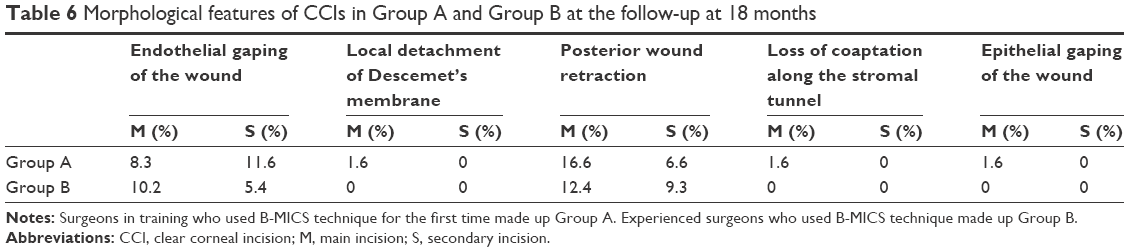 | Table 6 Morphological features of CCIs in Group A and Group B at the follow-up at 18 months |
Discussion
In this study, we investigated postoperative long-term results obtained by three surgeons in training using B-MICS technique for the first time in terms of visual outcomes at 18 months after surgery. Moreover, we evaluated PCO incidence and CCIs architecture. We compared results with those obtained by expert surgeons.
With regard to postoperative results at 18 months, we found a significant increase in BCVA in both groups as previously reported in the literature.4,12,13 In Group A, we found a statistically significant decrease in visual acuity between month 1 and month 18 (P=0.004), while this was not significant for the expert surgeon group (P=0.61). We supposed that this could be related to the presence of a higher PCO incidence in the trainers group.
We found a nonsignificant surgical-induced astigmatism in both groups as already shown for B-MICS technique.4–17 Moreover, corneal pachimetry resulted in a nonsignificant change between pre- and postoperative values for both groups, as expected.
Our findings on endothelial cell loss are statistically significant and similar to those published in traditional phacoemulsification cataract surgery performed by residents18 and for results with B-MICS for expert surgeons.19,20 We found a statistically significant lower cell loss in the expert surgeons’ group. Certainly, experienced surgeons are more confident with anterior chamber maneuvres and use less ultrasound during the surgery than surgeons in training. However, endothelial cell loss remained stable during 17 months of follow-up in both groups (Table 1).
PCO remains the most common complication in cataract surgery. Many studies have tried to find factors influencing PCO development.8,21–24 These factors include the IOL design, the use of specific therapeutic agents, the surgical technique itself, and other surgical interventions such as an accurate posterior capsule cleaning at the end of I/A. IOLs with sharp optic edges should be preferred to round-edged IOLs but there does not seem to be any significant difference using different optic materials or different types of anti-inflammatory treatments.8
There are very few reports on PCO incidence in B-MICS.25 In our study, we found a higher PCO score in Group A. To try to explain this finding, we carefully checked every video recording concerning the surgical maneuvres performed by each surgeon, and we noticed that expert surgeons always carried out an accurate cleaning of the posterior capsule at the end of I/A with a manual aspiration cannula or bimanual I/A (Figure 4). Surgeons in training never performed this delicate surgical intervention due to lack of skill with posterior capsules. We think that this could be the reason for the higher incidence of PCO in the training group. The lack of an accurate cleaning of the posterior capsule can lead to a proliferation, growth, migration, and transdifferentiation of residual lens epithelial cells as previously reported in the literature,24 and this process can be responsible for the higher rate of PCO incidence.
 | Figure 4 Posterior capsule scraping performed by an expert surgeon. |
In B-MICS, a correct execution of the CCIs is crucial for the subsequent surgical steps, and recently, AS-OCT has been identified as being the most useful method to detect changes in the architecture of CCIs.9,26–28 CCIs need to be correctly positioned and angled: they must be, respectively, 1.4 mm long and 145° angled. In case of too short and/or too perpendicular incisions, they may induce an increased risk of intraoperative iris prolapse in the surgical wound.29–31
In our case series, we found that CCIs performed by surgeons in training presented lower values both for length and inclination in comparison with those values found by expert surgeons. This could have been an important factor in determining a more frequent iris prolapse occurrence in the training group. In our previous study,5 we reported a high incidence of iris prolapse occurrence during B-MICS performed by surgeons in training. This value turned out to be higher than that found in other studies,14,18–20 and we thought it could be related to both the wrong inclination and length of the CCIs and the use of the nondominant hand.
We reanalyzed all the CCIs using AS-OCT separating the cases with iris prolapse from those without iris prolapse: interestingly, we noticed that in the first group, incisions were shorter and less angled than in those cases without iris incarceration. These results confirmed that CCIs architecture in B-MICS results in being a very important step in the technique. Interestingly, we noticed that in Group A, the CCIs in the dominant hand (main CCI) were longer than that in the nondominant hand, while we found the opposite for the expert surgeons. We suppose that for trainers, the use of the nondominant hand can be more difficult, especially in handling instruments, and the incision could be less angled and shorter in order to try to enter into the anterior chamber in the easiest way. For experienced surgeons, this maneuvre is certainly easier.
Finally, as regards ultrastructural alterations in the site of the incisions, we found mostly endothelial gaps and PWRs. In a previous study investigating CCIs architecture in B-MICS in a long-term follow-up for an expert surgeon,9 Calladine and Packard found only PWR and mostly in the dominant hand. In our study, we found some endothelial gaps in both groups, a case each for epithelial gap, DS, and corneal misalignment in the surgeons in training group, while we did not find any of these features in the expert surgeons group of patients. However, these alterations did not influence visual results.
Conclusion
B-MICS is an effective technique when performed by surgeons in training even assessed after a long-term follow-up. The lack of experience of the surgeons in training and a less accurate cleaning of the posterior capsule may lead to a more significant incidence of PCO in the postoperative period compared to expert surgeons. This may also lead to the presence of microstructural alterations at the incision site that, however, do not influence the efficacy of this surgery. Due to the relatively small data set, other investigations will be needed in the future to validate the effectiveness of this technique at long-term for surgeons in training.
Acknowledgments
The authors thank Gabriele Melegari for his help with the statistical analysis of the data. The abstract of this paper was preliminary presented as an oral presentation at the XXXIII Conference of ESCRS in Barcelona (Spain), September 2015: http://escrs.org/barcelona2015/programme/free-papers-details.asp?id=24921&day=0.
Disclosure
The authors report no conflicts of interest in this work.
References
Cavallini GM, Campi L, Masini C. B-MICS: Origini e Definizione. In: Cavallini GM, editor. B-MICS: Bimanual Micro Incision Cataract Surgery. Modena: Athena; 2014:1–5. | ||
Vasavada V, Vasavada V, Raj SM, Vasavada AR. Intraoperative performance and postoperative outcomes of microcoaxial phacoemulsification; observational study. J Cataract Refract Surg. 2007;33(6):1019–1024. | ||
Cavallini GM, Lugli N, Campi L, Lazzerini A, Longanesi L. Surgically induced astigmatism after manual extracapsular cataract extraction or after phacoemulsification procedure. Eur J Ophtalmol. 1996;6(3):257–263. | ||
Cavallini GM, Campi L, Masini C, Pelloni S, Pupino A. Bimanual microphacoemulsification versus coaxial miniphacoemulsification: prospective study. J Cataract Refract Surg. 2007;33(3):387–392. | ||
Cavallini GM, Volante V, Verdina T, et al. Results and complications of surgeons-in-training learning bimanual microincision cataract surgery. J Cataract Refract Surg. 2015;41(1):105–115. | ||
Verdina T, Forlini M, Volante V, Cavallini GM. Complicanze e Fase di Training nella B-MICS. In: Cavallini GM, editor. B-MICS: Bimanual Micro Incision Cataract Surgery. Modena: Athena; 2014:99–128. | ||
Khandwala MA, Marjanovic B, Kotagiri AK, Teinory M. Rate of posterior capsule opacification in eyes with the Akreos intraocular lens. J Cat Ref Surg. 2007;33(8):1409–1413. | ||
Findl O, Buehl W, Bauer P, Sycha T. Interventions for preventing posterior capsule opacification. Cochrane Database Syst Rev. 2010;(2):CD003738. | ||
Calladine D, Packard R. Clear corneal incision architecture in the immediate postoperative period evaluated using optical coherence tomography. J Cataract Refract Surg. 2007;33(8):1429–1435. | ||
Cavallini GM, Campi L, Torlai G, Forlini M, Fornasari E. Clear Corneal Incisions in bimanual microincision cataract surgery: long-term wound–healing architetture. J Cataract Refract Surg. 2012;38(10):1743–1748. | ||
Tetz MR, Auffarth GU, Sperker M, Blum M, Völcker HE. Photographic image analysis system of posterior capsule opacification. J Cataract Refract Surg. 1997;23(10):1515–1520. | ||
Can I, Takmaz T, Yildiz Y, Bayhan HA, Soyugelen G, Bostanci B. Coaxial, microcoaxial, and biaxial microincision cataract surgery. Prospective comparative study. J Cataract Refract Surg. 2010;36(5):740–746. | ||
Kahraman G, Amon M, Franz C, Prinz A, Abela-Formanek C. Intraindividual comparison of surgical trauma after bimanual microincision and conventional small-incision coaxial phacoemulsification. J Cataract Refract Surg. 2007;33(4):618–622. | ||
Carricondo PC, Fortes AC, Mourao Pde C, Hajnal M, Kara Jose NK. Senior resident phacoemulsification learning curve. Arq Bras Oftalmol. 2010;73(1):66–69. | ||
Woodfield AS, Gower EW, Cassard SD, Ramanthan S. Intraoperative phacoemulsification complication rates of second- and third year ophthalmology resident. Ophthalmology. 2011;118(5):954–958. | ||
Briszi A, Prahs P, Hillenkamp J, Helbig H, Herrmann W. Complication rate and risk factors for intraoperative complications in resident-performed phacoemulsification surgery. Graefes Arch Clin Exp Ophthalmol. 2012;250(9):1315–1320. | ||
Wilczyńska O, Wilczyński M, Omulecki W. Surgically induced astigmatism after bimanual phacoemulsification through microincision and after standard phacoemulsification. Klin Oczna. 2010;112(4–6):115–119. | ||
O’Brien PD, Fitzpatric P, Kilmartin DJ, Beatty S. Risk factor for endothelial cell loss after phacoemulsificaton surgery by a junior resident. J Cataract Refract Surg. 2004;30(4):839–843. | ||
Wilczynski M, Supady E, Loba P, Synder A, Palenga-Pydyn D, Omulecki W. Comparison of early corneal endothelial cell loss after coaxial phacoemulsification through 1.8 mm microincision and bimanual phacoemulsification through 1.7 mm microincision. J Cataract Refract Surg. 2008;35(9):1570–1574. | ||
Gonen T, Sever O, Horozoglu F, Yasar M, Keskinbora KH. Endothelial cell loss: Biaxial small-incision torsional phacoemulsification versus biaxial small-incision longitudinal phacoemulsification. J Cataract Refract Surg. 2012;38(11):1918–1924. | ||
Cavallini GM, Masini C, Campi L, Pelloni S. Capsulorhexis phimosis after bimanual microphacoemulsification and in-the-bag implantation of the Akreos MI60 intraocular lens. J Cataract Refract Surg. 2008;34(9):1598–1600. | ||
Svancarova R, Novak J, Adamkova H. The influence of lens capsule mechanical polishing to the secondary cataract development. Cesk Slov Oftalmol. 2010;66(1):21–25. | ||
Marcantonio JM, Vrensen GF. Cell biology of posterior capsular opacification. Eye. 1999;13(Pt 3b):484–488. | ||
Awasthi N, Guo S, Wagner BJ. Posterior capsular opacification: a problem reduced but not yet eradicated. Arch Ophthalmol. 2009;127(4):555–562. | ||
Podboraczynska-Jodko K, Lubinski W. Bimanual microincision cataract surgery with implantation of an Akreos MI60 lens – one year follow up. Klin Oczna. 2013;114(4):245–248. | ||
Dewey S, Beiko G, Braga-Mele R, et al. Microincisions in cataract surgery. J Cataract Refract Surg. 2014;40(9):1549–1557. | ||
Can I, Bayhan HA, Celik H, Ceran BB. Anterior segment optical coherence tomography evaluation and comparison of main clear corneal incisions in microcoaxial and biaxial cataract surgery. J Cataract Refract Surg. 2011;37(3):490–500. | ||
Wang L, Dixit L, Weikert MP, Jenkins RB, Koch DD. Healing changes in clear corneal cataract incisions evaluated using Fourier-domain optical coherence tomography. J Cataract Refract Surg. 2012;38(4):660–665. | ||
Rutar T, Porco TC, Naseri A. Risk factors for intraoperative complication in resident-performed phacoemulsification surgery. Ophthalmology. 2009;116(3):431–436. | ||
Chang DF, Braga-Mele R, Mamalis N, et al. ASCRS White Paper: clinical review of intraoperative floppy-iris syndrome. J Cataract Refract Surg. 2008;34(12):2153–2162. | ||
Hu YJ, Hou P. Managing Iris prolapse. J Cataract Refract Surg. 2010;36(6):1064. [author reply 1064–1065]. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.