Back to Journals » Clinical Ophthalmology » Volume 15
Long-Term Favorable Visual Outcomes in Patients with Large Submacular Hemorrhage
Authors Iyer PG, Brooks HL Jr, Flynn HW Jr ![]()
Received 21 January 2021
Accepted for publication 19 February 2021
Published 18 March 2021 Volume 2021:15 Pages 1189—1192
DOI https://doi.org/10.2147/OPTH.S300662
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Prashanth G Iyer,1 H Logan Brooks Jr,2 Harry W Flynn Jr1
1Department of Ophthalmology, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, FL, USA; 2Southern Vitreoretinal Associates, Tallahassee, FL, USA
Correspondence: Harry W Flynn Jr
Southern Vitreoretinal Associates, 900 NW 17th Street, Miami, FL, 33136, USA
Tel +1 305 326-6148
Fax +1 305 326-6417
Email [email protected]
Abstract: Submacular hemorrhage (SMH) has been reported to be toxic to the retina based on animal studies. However, observational studies of patients with neovascular-related SMH and those treated with intravitreal anti-vascular growth factor (anti-VEGF) therapy have shown many favorable visual acuity outcomes. We report two cases of neovascular-related SMH with ten or more years of follow-up. The first case was an 83-year old female with a history of nonexudative age-related macular degeneration in both eyes presenting with sudden decrease in vision (20/400) in her right eye due to a large SMH, treated with anti-VEGF therapy. Over the next following months, there was resolution of the hemorrhage and return of good visual acuity. At 10-year follow-up, visual acuity was 20/30 in the right eye. The second case was a 49-year old female with a history of presumed ocular histoplasmosis syndrome (POHS), presenting with sudden vision loss (20/400) in her right eye due to large, thick SMH. With observation and intermittent anti-VEGF therapy, there was resolution of the hemorrhage. At 30-year follow-up, visual acuity was 20/20 in the right eye.
Keywords: choroidal neovascularization, submacular hemorrhage, anti-VEGF, retinal toxicity, age-related macular degeneration, presumed ocular histoplasmosis syndrome
Introduction
Submacular hemorrhage (SMH) secondary to choroidal neovascularization (CNV) has been described in conditions such as exudative age-related macular degeneration (AMD), myopic maculopathy, angioid streaks, presumed ocular histoplasmosis syndrome (POHS), polypoidal choroidal vasculopathy and others. Animal studies have speculated that submacular hemorrhage may be toxic to the retina.1,2 However, observational studies of patients with SMH from all causes have shown some favorable visual acuity outcomes despite nonsurgical and nonmedical treatments.3,4 We report two such patients with SMH due to underlying CNV who have been followed for many years.
Cases
Case 1
An 83-year old female with a history of nonexudative AMD in both eyes presented with a sudden decrease in vision of her right eye. Visual acuity was 20/400 in the right eye and 20/20 in the left eye. Examination revealed large, thick SMH in the right eye and drusen in the left eye (Figure 1A–C). She was treated with intravitreal anti-vascular growth factor (anti-VEGF) agent bevacizumab injection to the right eye. One month later, there was some resolution of the SMH with persistent dehemoglobinized blood and visual acuity improving to 20/100 (Figure 1D). Six months later while the hemorrhage had resorbed, there was inferior subretinal fibrosis and visual acuity was 20/30 (Figure 1E). Over time, the patient was switched to intravitreal ranibizumab. Inferior subretinal fibrosis developed pigmentation and the OCT remained stable without subretinal fluid. At ten-year follow-up, the patient had a favorable visual acuity of 20/25 in the right eye with stable fundus examination and OCT (Figure 1F and G).
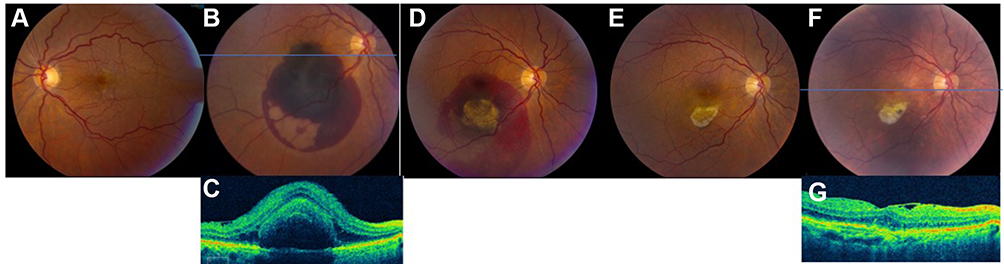 |
Figure 1 83-year old female with exudative age-related macular degeneration of the right eye. (A) Fundus photograph of the left eye showed macular drusen at the time of presentation. (B) The right fundus photograph revealed large, thick submacular hemorrhage at the time of presentation (SMH). (C) OCT of the right eye from presentation revealed subretinal hemorrhage. (D)At one-month follow-up after receiving intravitreal bevacizumab, there was some resolution of the SMH with persistent dehemoglobinzied blood. (E) Six months later with continuation of anti-VEGF treatment, the hemorrhage had been completely resolved, with inferior subretinal fibrosis that was away from the fovea. (F) At ten-year follow-up, the inferior subretinal fibrosis developed pigmentation; (G) corresponding OCT was stable without subretinal fluid. |
Case 2
A 49-year old female presented with sudden vision loss in her right eye. Four years prior, she had undergone laser treatment in the left eye for juxtafoveal CNV secondary to POHS. She presented with a visual acuity of 20/400 in the right eye and 20/20 in the left eye. Fundus examination of the right eye revealed a large, thick SMH (Figure 2A). The SMH was observed. On one-month follow-up, the patient had some resorption of the hemorrhage with persistent dehemoglobinized blood, with a visual acuity of 20/50 (Figure 2B). At three-month follow-up, the hemorrhage had mostly reabsorbed with minimal retinal pigment epithelial changes, and visual acuity was 20/30 in the right eye (Figure 2C). Approximately two years after, hemorrhage was resolved with some pigment changes and visual acuity returned to 20/20 (Figure 2D). Fifteen years after her hemorrhage, the patient intermittently required intravitreal bevacizumab and aflibercept injections to the right eye for intraretinal and subretinal fluid. Fundus examination at 30-year follow-up demonstrated localized pigmented subretinal fibrosis and OCT was flat without subretinal fluid (Figure 2E). Visual acuity remained 20/20.
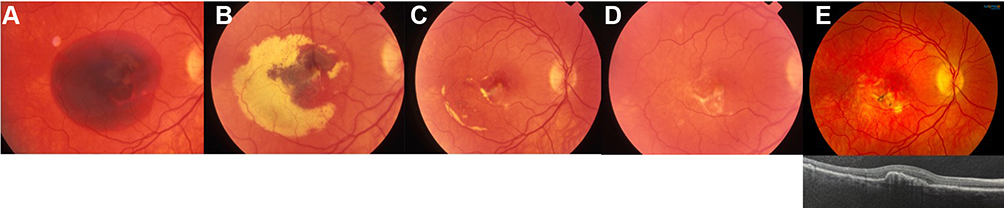 |
Figure 2 49-year old female with presumed ocular histoplasmosis syndrome (POHS) of the right eye. (A) On presentation, fundus photograph of the right eye revealed a large, thick SMH. There was no OCT imaging or anti-VEGF treatment agents available in 1989. (B) During one-month follow-up, while some of the hemorrhage had been resorbed, there was persistent dehemoglobinized blood. (C) At three-month follow-up, the hemorrhage had mostly resolved with minimal retinal pigment epithelial changes. (D) Two years later, hemorrhage was resolved completely with inferior subretinal fibrosis. (E) At 30-year follow-up, fundus photograph demonstrated pigmented fibrosis and the OCT showed a shallow RPE detachment without subretinal fluid. |
Discussion and Conclusions
Animal studies have reported that SMH may cause damage to retinal photoreceptors. Glatt and Machemer in 1982 injected autologous blood beneath the retina in a rabbit model to demonstrate irreversible photoreceptor damage and toxic effects on the retina during the first 24 hours of exposure.1 Toth et al in 1991 demonstrated using a cat model that there was photoreceptor damage 1 hour after the onset of SMH, and significant outer retinal damage within 1 week.2 These findings encouraged prompt removal of large, thick SMH early-on via surgery in order to optimize visual acuity outcomes. However, even with prompt surgical removal, Wade et al reported that patients with exudative AMD still had poor visual acuity outcomes.5 They compared AMD versus non-AMD groups in assessing subretinal surgery to remove the SMH clot, and reported better anatomic success and visual acuity in patient without AMD compared to those patients with a CNV-related subretinal hemorrhage.5
In addition, other studies reviewing the natural history of SMH such as Berrocal et al6 demonstrated that in patients with non-AMD-related SMH, almost half had a visual acuity of 20/40 or better, but only 15% of patients with SMH in the AMD study arm achieved similar visual acuity. Chaudhry et al also demonstrated a case report of spontaneous resolution of SMH in patient with CNV and excellent visual acuity despite large, thick SMH.4 Prior to anti-VEGF treatment, Avery et al reported in patients with exudative AMD with SMH that there was an average of 3.5 lines lost in 3 years, emphasizing that vision loss may be progressive in AMD due to the actual disease and not necessarily the SMH itself.7
In terms of management, some studies have reported variable and disappointing visual outcomes with surgical intervention for SMH in patients with AMD.5,8 The SMH trials in patients with AMD concluded that there was no advantage of surgical removal of the SMH clot over observation in achieving stable visual acuity.9 Surgical removal has adverse events such as recurrent bleeding, retinal detachment, cataract formation, proliferative vitreoretinopathy, and others.9 Heriot first described the method of pneumatic displacement of SMH at the American Academy of Ophthalmology in 1997 (San Francisco, AAO 1997). Haupert et al’s study in 2001 was one of the first studies evaluating displacement of thick SMH using vitrectomy, subretinal tissue plasminogen activator (tPA), fluid-air exchange and prone positioning.10 While a small study, subretinal hemorrhage was successfully displaced in all cases with final visual acuity improvement in the majority of cases.10 Recurrent hemorrhage was a frequent complication.10 With the advent of anti-VEGF therapy, Chang et al studied vitrectomy and subretinal tPA with and without anti-VEGF.11 They reported that while vitrectomy, subretinal tPA and tamponade could successfully displace thick SMH, adding anti-VEGF postoperatively could help maintain visual acuity gains after surgery.11
In the era of pharmacotherapies for exudative AMD, management considerations in these patients have shifted to anti-VEGF monotherapy. Sheinbaum et al reported patients with exudative AMD and SMH treated with anti-VEGF therapy alone.12 This study demonstrated visual acuity gains and OCT thickness improvements in one year without systemic or ocular complications in 19 eyes.12 Altaweel et al analyzed patients with exudative AMD enrolled in the Comparison of Age-Related Macular Degeneration Treatment Trials (CATT).13 In anti-VEGF monotherapy treated patients with SMH (defined as >50% of lesion composed of blood) compared to the rest of the patients enrolled in the trial, visual acuity and morphologic outcomes were equally improved in both groups. The CATT study investigators concluded that patients with SMH from AMD can be managed similarly to those who have less or no blood.13
In the current report of two patients with large, thick SMH, visual acuity improved from 20/400 to 20/30 or better with anti-VEGF monotherapy and observation during long-term follow-up. In addition to visual acuity, OCT is an excellent tool in assessing the outer retinal damage that may occur following SMH. We demonstrate in both cases that the fovea was unaffected on OCT despite SMH. Contrary to the earlier reported animal studies, there was no direct clinical evidence that SMH was toxic to the retina in these two cases. Final visual acuity outcomes are often determined by the associated macular pathology and may be more favorable when the CNV complex is eccentric to the fovea. Patients treated with anti-VEGF therapy may benefit from stabilization of the active CNV without mechanical removal of the blood. This method can avoid surgical complications including retinal detachment, proliferative vitreoretinopathy, and cataract formation. In the future, larger studies with similar long-term follow-up as ours may provide insight into risk factors that predict final visual outcomes in patients with large, thick SMH.
Statement of Ethics
The authors have no ethical conflicts to disclose. Institutional approval was not required to publish this case series.
Patient Consent
Consent to publish was obtained from the patients in this case series.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Glatt H, Machemer R. Experimental subretinal hemorrhage in rabbits. Am J Ophthalmol. 1982;94(6):762–773. doi:10.1016/0002-9394(82)90301-4
2. Toth CA, Morse LS, Hjelmeland LM, Landers MB
3. McCabe CM, Flynn HW
4. Chaudhry NA, Flynn HW
5. Wade EC, Flynn HW
6. Berrocal MH, Lewis ML, Flynn HW Jr. Variations in the clinical course of submacular hemorrhage. Am J Ophthalmol. 1996;122(6):920. doi:10.1016/s0002-9394(14)72107-5
7. Avery RL, Fekrat S, Hawkins BS, Bressler NM. Natural history of subfoveal subretinal hemorrhage in age-related macular degeneration. Retina. 1996;16(3):183–189. doi:10.1097/00006982-199616030-00001
8. Ibanez HE, Bloom SM, Olk RJ, et al. External argon laser choroidotomy versus needle drainage technique in primary scleral buckle procedures. A prospective randomized study. Retina. 1994;14(4):348–350. doi:10.1097/00006982-199414040-00010
9. Bressler NM, Bressler SB, Childs AL, et al. Surgery for hemorrhagic choroidal neovascular lesions of age-related macular degeneration: ophthalmic findings: SST report no. 13. Ophthalmology. 2004;111(11):1993–2006.
10. Haupert CL, McCuen BW
11. Chang W, Garg SJ, Maturi R, et al. Management of thick submacular hemorrhage with subretinal tissue plasminogen activator and pneumatic displacement for age-related macular degeneration. Am J Ophthalmol. 2014;157(6):1250–1257. doi:10.1016/j.ajo.2014.02.007
12. Shienbaum G, Garcia Filho CA, Flynn HW
13. Altaweel MM, Daniel E, Martin DF, et al. Outcomes of eyes with lesions composed of >50% blood in the Comparison of Age-related Macular Degeneration Treatments Trials (CATT). Ophthalmology. 2015;122(2):391–398.e395.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.