Back to Journals » International Medical Case Reports Journal » Volume 15
Long-Acting Fluocinolone Acetonide Intravitreal Implant for Recurrent Bilateral Non-Infectious Posterior Uveitis
Authors Babel AT, Chin EK ![]() , Almeida DRP
, Almeida DRP ![]()
Received 2 August 2022
Accepted for publication 10 November 2022
Published 22 November 2022 Volume 2022:15 Pages 665—669
DOI https://doi.org/10.2147/IMCRJ.S384356
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Adrian T Babel,1,2 Eric K Chin,3,4 David RP Almeida2
1Boonshoft School of Medicine, Dayton, OH, USA; 2Erie Retinal Surgery, Erie, PA, USA; 3Retina Consultants of Southern California, Redlands, CA, USA; 4Loma Linda Eye Institute, Veterans Affair Hospital, Loma Linda, CA, USA
Correspondence: David RP Almeida, Erie Retinal Surgery, Erie Retina Research, 300 State Street, Suite 201, Erie, PA, 16507, USA, Tel +1 814 456-4241, Fax +1 814 453 3354, Email [email protected]
Purpose: Our case emphasizes the utility of long-acting intravitreal fluocinolone implants (YUTIQ) for managing recalcitrant forms of non-infectious posterior uveitis, NIPU.
Patient: We present a case of bilateral NIPU refractory to topical corticosteroids and intravitreal triamcinolone and dexamethasone.
Results: Management with bilateral YUTIQ improved local ocular inflammatory control with improved vision and anatomical outcomes.
Conclusion: NIPU can develop into recurrent forms resistant to short-acting therapeutics. Long-acting efficacy with YUTIQ emphasizes the need to recognize such refractory NIPU cases.
Keywords: non-infectious uveitis, NIU, fluocinolone acetonide implant
Introduction
Uveitis is inflammation of the vascular layer connecting the sclera and neurosensory retina; the uveal tract includes the iris, ciliary body, and choroid.1–3 Anterior uveitis is most common and primarily involves inflammation of the iris (iritis), pars plicata of the ciliary body (anterior cyclitis), or both (iridocyclitis).2,3 Intermediate uveitis primarily involves the vitreous (vitritis).2 Posterior uveitis is the second most common uveitis and primarily involves the choroid (choroiditis), retina (retinitis), or both (chorioretinitis and retinochoroiditis); it can also involve the optic nerve (neuroretinitis).2,3 Inflammation’s foci can be either single, multiple, or diffuse.2 In panuveitis, all structures of the uveal tract are inflamed.2
Uveitis can be categorized into infectious or non-infectious uveitis.1–3 Non-infectious posterior uveitis is a significant cause of vision loss, and its prevalence varies by race and ethnicity.1–3 Macular edema associated with uveitis is the most common cause of visual impairment.2 Although the etiology of NIPU remains unclear, the involvement of both genetic and environmental factors is considered significant.1–3 Genes coding for major histocompatibility complexes, MHCs, and the interleukin 23 receptor, IL-23R, are two susceptible pathways that are commonly associated with NIPU pathogenesis.1 For example, non-infectious uveitic diseases such as Adamantiades–Behçet’s disease and acute anterior uveitis are associated with IL-23R and MHC class I mutations, Vogt-Koyanagi-Harada disease and sarcoidosis are associated with IL-23R and MHC class II mutations, and birdshot chorioretinopathy is associated with MHC class I mutations.1–3 Environmental factors contributing to NIPU development are not as well understood, although aberrant immunological responses (Th1/Th17 mediated) to viral infections have been implicated in NIPU onset for individuals with predisposing factors.1
NIPU is typically treated with ocular (local therapy) or systemic corticosteroids. The addition of systemic immunosuppressants may be required to mitigate visual impairment.4–6 Adverse effects associated with systemic corticosteroid use (eg, osteoporosis, poor glycemic control in diabetes, mood changes, cataract formation) and steroid-sparing immunosuppressants can complicate disease management, which highlights the importance of local (ie, ocular) control with intravitreal therapeutics whenever possible.5
Longer-acting sustained-release intravitreal corticosteroid implants such as the 0.7mg dexamethasone implant (Ozurdex; Allergan/AbbVie, Irvine, CA, USA) and the recently-approved 0.18mg fluocinolone acetonide, FA, implant (YUTIQ; EyePoint Pharmaceuticals, Watertown, MA, USA) demonstrate improved efficacy over older agents.4–7 Here, we present a case of a 59-year-old female with bilateral recalcitrant NIPU. Initial treatment revealed suboptimal control, and the patient was subsequently successfully treated with YUTIQ intravitreal implants OU.
Observation
A 59-year-old white female presented with a three-month history of recalcitrant bilateral NIPU. The patient had a non-contributory past medical history; past ocular history was significant for pseudophakia OU. Upon referral, the patient had a history of topical corticosteroid drops OU (declined systemic corticosteroid treatment) and previous intravitreal triamcinolone (Triesence; Alcon Laboratories, Ft. Worth, TX, USA) OS (Figure 1). The patient had undergone previous vitrectomy and membranectomy for visually-significant epiretinal membrane OS. The patient continued with recurrent active posterior uveitis and was treated with a dexamethasone 0.7mg implant (Ozurdex) OU.
 |
Figure 1 Topical corticosteroid drops OU and previous intravitreal triamcinolone OS, widefield fluorescein angiography (Optos) and optical coherence tomography. Bright green line indicates section of image provided and green arrow has no significance. |
At just 6 weeks after Ozudex OD and 8 weeks after Ozurdex OS, follow-up revealed BCVA improved from 20/80 to 20/60 OD, but worsened from 20/70 to 20/200 OS (IOP was stable and within normal limits) (Figure 2). Despite local treatment as above, widefield fluorescein angiography (Optos, Marlborough, MA, USA) showed persistent inflammation. After discussing the risks and benefits, the decision to proceed with bilateral YUTIQ implants was planned. Follow-up showed improvement in vision, macular edema, and macular leakage on fluorescein angiography imaging (Figure 3): at 3 months after YUTIQ OD and 1 month after YUTIQ OS, BCVA improved from 20/60 to 20/50 OD and 20/70 to 20/40 OS. The patient did not have systemic steroid therapy during the course of treatment and IOP remained stable with no IOP elevations following YUTIQ injections OU.
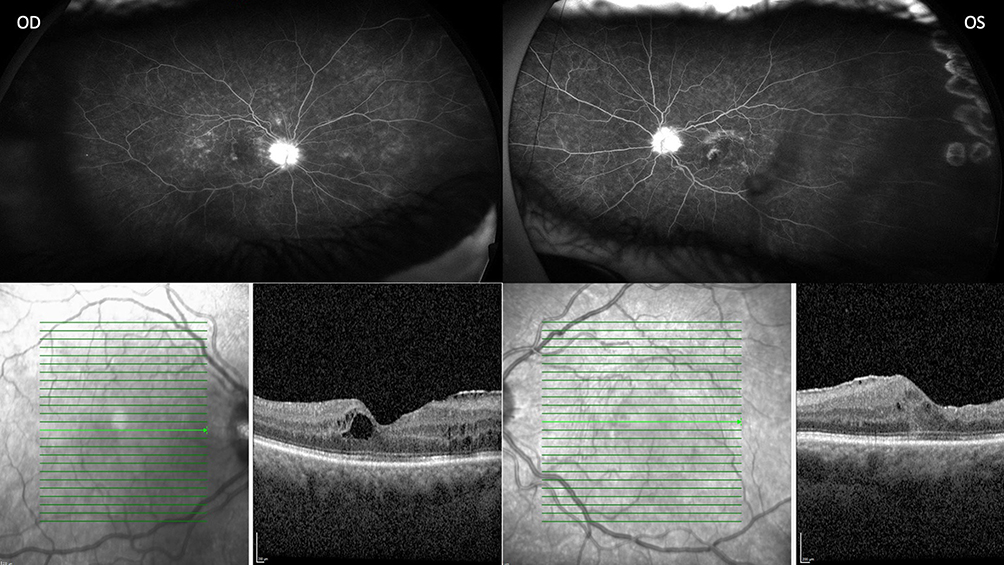 |
Figure 2 Persistent inflammation 6 weeks after Ozudex OD and 8 weeks after Ozurdex OS, widefield fluorescein angiography (Optos) and optical coherence tomography. Bright green line indicates section of image provided and green arrow has no significance. |
 |
Figure 3 Improved macular edema 3 months after YUTIQ OD and 1 month after YUTIQ OS, widefield fluorescein angiography (Optos) and optical coherence tomography. Bright green line indicates section of image provided and green arrow has no significance. |
Discussion
The most common cause of intraocular inflammation is idiopathic, which is responsible for at least 50% of all uveitis cases.2,3 NIPU is the third most common type of idiopathic intraocular inflammation in the United States, accounting for 10% of all cases in adults with severe vision loss without proper diagnosis and management.1,2,6,8,9 NIPU classically presents as periodic flares of inflammation leading to worsening non-reversible vision loss over time.6 While the etiology of NIU is uncertain, it is linked to certain systemic diseases (eg sarcoidosis, Adamantiades–Behçet’s disease) and several genes identified in the pathogenesis of NIU.1–3 Two common genetic associations are with human leukocyte antigen, HLA, alleles, which code for MHC class I and class II molecules, and with the IL-23R gene, which codes for IL-23R.1–3
MHC class I and class II molecules present intracellular and extracellular antigens essential for cell-mediated (CD8-positive cytotoxic T cells) and humoral (CD4-positive helper T cells) immunity, respectively.1,3 Mutations in genes encoding these MHC molecules predisposes patients to autoimmune and exaggerated immune responses implicated in the pathogenesis of NIU.1,3 The IL-23R gene produces the IL-23R which is found on the Th17 cell surface and is the second most common susceptibility gene for NIU.1,3 This receptor, when bound to its IL-23 ligand, plays an integral role in Th17 homeostasis, differentiation to pathological Th17 cells, and production of inflammatory cytokines (IL-17, IL-6, interferon- γ) which are observed in certain non-infectious uveitic diseases such as Adamantiades–Behçet’s disease, Vogt-Koyanagi-Harada disease, and sarcoidosis.1,3
The inflammatory nature of NIU pathogenesis indicates anti-inflammatory agents as ideal treatments, particularly agents that act locally.1,2,5,9 One such intravitreal corticosteroid was developed in 2005: a 0.57mg FA (Retisert; Bausch & Lomb, Rochester, NY, USA) surgically placed intravitreal implant.5,6,9,10 However, this sizable and nonbiodegradable device requires invasive surgical removal.9 YUTIQ was developed in 2018 and is a nonbiodegradable intravitreal implant containing 0.18mg FA which showed superior effects in reducing inflammation and improving vision in our case of NIPU compared to other options.5–7 Two randomized, double blinded, placebo-controlled Phase 3 clinical trials concluded that YUTIQ (0.18mg FA implant) significantly reduced the recurrence of posterior uveitis compared to placebo at 6 months and at 3 years.11,12
A recent systemic review and network meta-analysis comparing efficacy and safety of intravitreal therapeutic agents for NIU concluded that YUTIQ (FA implant 0.2 µg/day, calculated delivered dose) improved BCVA as much as Ozurdex (0.7 mg dexamethasone implant) at 6 months, but no 12 month data was provided for Ozurdex and this meta-analysis does not highlight the efficacy of YUTIQ over Ozurdex in patients refractory to topical corticosteroids and Ozurdex treatment.13 Additionally, YUTIQ was ranked higher in probability of being the most efficacious drug for improving BCVA at 6 months over Ozurdex.13 Unlike Ozurdex, the YUTIQ implant is made of an inert non-biodegradable material that does not require surgical removal.5,7 Furthermore, the active compound FA in YUTIQ is more potent than dexamethasone, but is in a lower dose compared to its predecessor Retisert to minimize the side effects and is placed through a less invasive intravitreal injection.5–7
Ocular and systemic corticosteroids pose potential ocular risks such as IOP elevations and cataract progression, yet they serve as a mainstay for the treatment of NIPU.1,5–7,9 In order to minimize the long-term side effects associated with corticosteroids, it is often recommended to use immunomodulators for maintenance therapy and corticosteroids to counter flare-ups and acute inflammation.1,5–7,9 Through this case study, we highlight the local control of ocular inflammation and encourage further head-to-head comparisons on various corticosteroid implants to research their effectiveness and safety profiles. Additionally, with the role of IL-23 and Th-17 in the development of NIPU we recommend further investigation of the efficacy and durability of intraocular implants such as YUTIQ, in combination with steroid-sparing immunomodulators.
Abbreviations
NIPU, non-infectious posterior uveitis; NIU, non-infectious uveitis; MHC, major histocompatibility complex; IL-23R, interleukin 23 receptor; HLA, human leukocyte antigen.
Ethics and Consent Statements
Consent to publish this case report has been obtained from the patient in writing, the data has been anonymized, and institutional approval is not required to publish the case details.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Dr Eric K Chin was involved in research and clinical trials for Opthea, Genentech, Novartis, Iveric, Chendgu Kanghong Biosciences, Kodiak Sciences, and Bayer, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Takeuchi M, Mizuki N, Ohno S. Pathogenesis of non-infectious uveitis elucidated by recent genetic findings. Front Immunol. 2021;12:640473. doi:10.3389/fimmu.2021.640473
2. Massa H, Pipis SY, Adewoyin T, Vergados A, Patra S, Panos GD. Macular edema associated with non-infectious uveitis: pathophysiology, etiology, prevalence, impact and management challenges. Clin Ophthalmol. 2019;13:1761–1777. doi:10.2147/OPTH.S180580
3. Huang XF, Brown MA. Progress in the genetics of uveitis. Genes Immun. 2022;23(2):57–65. doi:10.1038/s41435-022-00168-6
4. Kempen JH, Altaweel MM; Multicenter Uveitis Steroid Treatment (MUST) Trial Research Group. Benefits of systemic anti-inflammatory therapy versus fluocinolone acetonide intraocular implant for intermediate uveitis, posterior uveitis, and panuveitis: fifty-four-Month Results of the Multicenter Uveitis Steroid Treatment (MUST) trial and follow-up study. Ophthalmology. 2015;122(10):1967–1975. doi:10.1016/j.ophtha.2015.06.042
5. Kuppermann BD, Zacharias LC, Kenney MC. Steroid differentiation: the safety profile of various steroids on retinal cells in vitro and their implications for clinical use (an American Ophthalmological Society thesis). Trans Am Ophthalmol Soc. 2014;112:116–141.
6. Testi I, Pavesio C. Preliminary evaluation of YUTIQ™ (fluocinolone acetonide intravitreal implant 0.18 mg) in posterior uveitis. Ther Deliv. 2019;10(10):621–625. doi:10.4155/tde-2019-0051
7. Uveitis treatment. Fluocinolone acetonide intravitreal implant. YUTIQ®. Available from: https://yutiq.com/downloads/YUTIQ%20Patient%20Brochure_21070601.pdf.
8. Thorne JE, Suhler E, Skup M, et al. Prevalence of non-infectious uveitis in the United States: a claims-based analysis. JAMA Ophthalmol. 2016;134(11):1237–1245. doi:10.1001/jamaophthalmol.2016.3229
9. Tan HY, Agarwal A, Lee CS, et al. Management of non-infectious posterior uveitis with intravitreal drug therapy. Clin Ophthalmol. 2016;10:1983–2020. doi:10.2147/OPTH.S89341
10. Arcinue CA, Cerón OM, Foster CS. A comparison between the fluocinolone acetonide (Retisert) and dexamethasone (Ozurdex) intravitreal implants in uveitis. J Ocul Pharmacol Ther. 2013;29(5):501–507. doi:10.1089/jop.2012.0180
11. Jaffe GJ, Pavesio CE; Study Investigators. Effect of a fluocinolone acetonide insert on recurrence rates in noninfectious intermediate, posterior, or panuveitis: three-year results. Ophthalmology. 2020;127(10):1395–1404. doi:10.1016/j.ophtha.2020.04.001
12. Safety and efficacy study of a FAI insert in subjects with chronic non-infectious posterior uveitis - study results. Study Results - ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/results/NCT02746991.
13. Liao W, Zhong Z, Su G, Feng X, Yang P. Comparative efficacy and safety of advanced intravitreal therapeutic agents for noninfectious uveitis: a systematic review and network meta-analysis. Front Pharmacol. 2022;13:749312. doi:10.3389/fphar.2022.749312
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.