Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Localized Infrared Hyperthermia as an Adjunctive Therapy for Long-Standing Hailey–Hailey Disease: A Case Report
Authors Wu H, Lu Y, Feng Y, Zhang L, Jiang C, Liao T ![]()
Received 17 February 2026
Accepted for publication 14 May 2026
Published 3 June 2026 Volume 2026:19 603844
DOI https://doi.org/10.2147/CCID.S603844
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Carlos A. Torres-Cabala
Hongye Wu, Yonghong Lu, Yanyan Feng, Liwen Zhang, Cunhuo Jiang, Tianzhi Liao
West China School of Medicine, Sichuan University, Sichuan University Affiliated Chengdu Second People’s Hospital, Chengdu Second People’s Hospital, Chengdu, People’s Republic of China
Correspondence: Yonghong Lu, West China School of Medicine, Sichuan University, Sichuan University Affiliated Chengdu Second People’s Hospital, Chengdu Second People’s Hospital, Chengdu, People’s Republic of China, Email [email protected]
Abstract: Hailey–Hailey disease (familial benign chronic pemphigus, HHD) is a rare, relapsing genodermatosis characterized by painful erosions in intertriginous areas. Management can be challenging in patients with long-standing, frequently relapsing disease, particularly when conventional therapies provide only partial or transient benefit. We describe a 45-year-old man with a 20-year history of HHD who was treated with localized infrared hyperthermia as an adjunctive therapy. Prior to presentation at our department, he had received multiple topical and systemic treatments with limited and temporary benefit, and continued to experience frequent relapses with substantial impairment in quality of life. A biphasic treatment regimen combining standard topical supportive care with localized infrared irradiation (1.0– 2.4 μm, 43 ± 1°C) was administered. Initial treatment of the right axilla achieved complete local clearance and was accompanied by improvement in untreated distant lesions. Subsequent treatment of the remaining involved sites resulted in sustained overall disease control, with the Physician Global Assessment score improving from 4 to 1 and the Dermatology Life Quality Index from 23 to 2. No thermal adverse events were observed, and the patient remained recurrence-free at 11 months. This case suggests that localized infrared hyperthermia may be a safe, well-tolerated, non-invasive adjunctive option for selected patients with long-standing, frequently relapsing Hailey–Hailey disease.
Keywords: familial benign chronic pemphigus, physician global assessment, dermatology life quality index, long-term follow-up
Introduction
Familial benign chronic pemphigus, also known as Hailey–Hailey disease, is a rare autosomal dominant genodermatosis affecting approximately 1 in 50,000 individuals.1,2 It presents with recurrent flaccid vesicles, erosions, fissures, and macerated plaques, mainly in intertriginous areas such as the axillae, groins, inframammary folds, and genital region. Pain, pruritus, malodor, exudation, and functional limitation can markedly impair quality of life, especially in extensive or frequently relapsing disease.3
Management is challenging because Hailey–Hailey disease typically follows a chronic relapsing course, with flares triggered by friction, heat, sweating, moisture, and secondary bacterial or fungal colonization.4 Standard treatment includes trigger avoidance, reduction of friction and sweating, topical anti-inflammatory agents, antiseptic measures, and antimicrobial therapy when needed. For long-standing disease, systemic treatments, botulinum toxin, photodynamic therapy, ablative laser, dermabrasion, and other procedures have been reported, but outcomes are variable, recurrence is common, and use may be limited by adverse effects, cost, access, wound care requirements, or practical challenges in flexural sites.5
Localized hyperthermia using infrared radiation has been explored as a non-pharmacologic dermatologic therapy, with potential effects on heat shock responses, local inflammation, microcirculation, and tissue repair. However, its use in Hailey–Hailey disease has rarely been reported, and its clinical value remains uncertain. Herein, we report a patient with long-standing, frequently relapsing Hailey–Hailey disease who showed marked and sustained improvement after localized infrared hyperthermia as an adjunct to standard topical supportive care. This case suggests that localized infrared hyperthermia may warrant further investigation as a non-invasive adjunctive option for selected patients with long-standing, frequently relapsing Hailey–Hailey disease.
Materials and Methods
Patient
A 45-year-old male bus driver presented to the Department of Dermatology at Chengdu Second People’s Hospital with a 20-year history of recurrent, painful skin lesions involving the bilateral axillae, inguinal regions, popliteal fossae, and perianal area. His work required prolonged sitting and repetitive arm movements, which likely aggravated symptoms by increasing friction, occlusion, moisture retention, and perspiration in affected intertriginous areas; disease activity was typically worse during warmer months. Over the preceding two decades, he had sought treatment at multiple institutions and had received repeated courses of systemic corticosteroids and immunosuppressive/immunomodulatory agents, including Tripterygium glycosides and total glucosides of paeony, in addition to a range of topical therapies. These included medium- to high-potency topical corticosteroids (eg, fluticasone propionate and halometasone), topical antibiotics (eg, fusidic acid and mupirocin), and other topical therapies. Despite these interventions, clinical benefit was limited and temporary, with frequent relapses that markedly impaired his quality of life. At presentation, his Dermatology Life Quality Index (DLQI) score was 23/30, and his pain score on the Visual Analogue Scale (VAS) was 5/10. Figure 1 shows erythematous plaques with maceration and erosions before treatment. Physical examination revealed ill-defined erythematous plaques with significant maceration, deep erosions, and serous exudation involving the bilateral axillae and groins (Figure 1). Scattered papules, vesicles, and crusts were visible at the periphery, accompanied by a foul odor consistent with secondary infection. The total Body Surface Area (BSA) involvement was estimated at 4%, with a Physician Global Assessment (PGA) score of 4 (severe). While complete blood count and liver/kidney function tests were normal, swabs from the erosions cultured positive for a mixed infection of penicillin-resistant Staphylococcus aureus and Candida albicans.
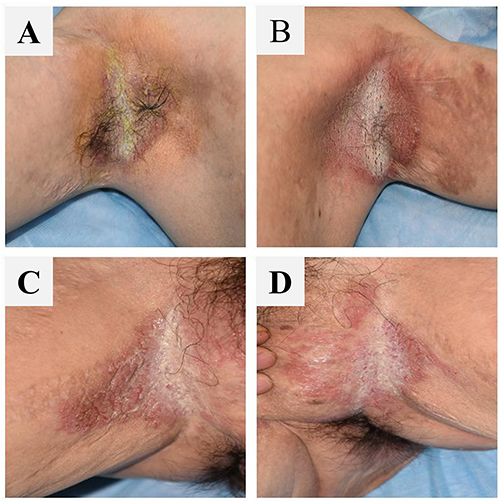 |
Figure 1 Baseline Clinical Presentation. (A) Right axilla; (B) Left axilla; (C) Right inguinal region; (D) Left inguinal region. |
A punch biopsy demonstrated hyperkeratosis, irregular acanthosis, and the characteristic “dilapidated brick wall” appearance of the epidermis, defined by extensive suprabasal acantholysis with intraepidermal bullae containing acantholytic cells. These histopathological findings (Figure 2), together with the clinical presentation and family history, supported the diagnosis of Hailey–Hailey disease (HHD).
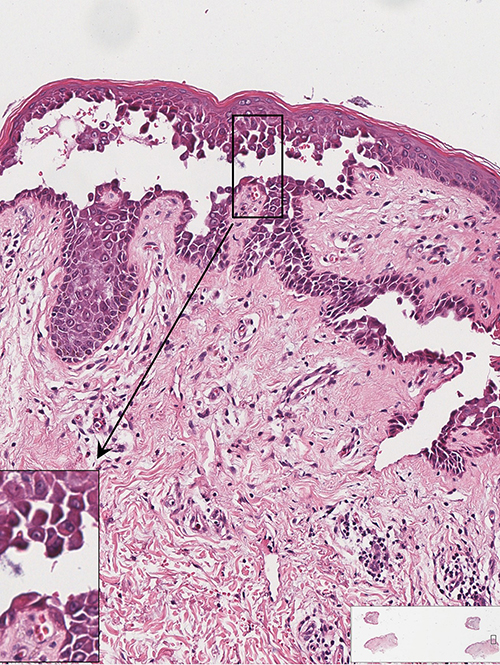 |
Figure 2 Histopathology of the skin lesion showing suprabasal acantholysis with the characteristic “dilapidated brick wall” appearance of Hailey–Hailey disease. |
Methods
Given the long-standing relapsing course, limited and temporary responses to prior systemic and topical therapies, and practical limitations of invasive procedures related to the patient’s occupation, localized infrared hyperthermia was introduced as a non-invasive adjunctive treatment. Baseline topical therapy consisted of halometasone cream, fusidic acid cream, and naftifine-ketoconazole cream, applied twice daily to all affected intertriginous areas to control inflammation and secondary microbial colonization. Infrared hyperthermia was delivered using a device (Model: YY-WRY-V03) emitting wavelengths of 1.0–2.4 μm. The probe was positioned 5.5 cm from the skin, and the surface temperature was maintained at 43 ± 1°C for 30 minutes per session. Treatment was performed in two phases. During Phase 1 (Weeks 1–14), only the right axilla was treated to assess local efficacy and possible remote effects, with twice-weekly sessions for 5 weeks followed by once-weekly sessions. After clearance of the right axilla, Phase 2 (Weeks 15–27) targeted the left groin, which remained the most active residual site.
Results
The patient demonstrated excellent tolerance to the procedure, reporting only a mild, transient sensation of warmth without pain, and no adverse thermal events such as burns or scarring occurred. Clinical improvement followed a rapid and progressive trajectory. By Week 6, significant re-epithelialization and a marked reduction in exudation were noted in the treated right axilla. Most remarkably, a concurrent improvement was observed in the untreated left axilla and bilateral groins, where erythema and erosion were visibly reduced, lowering the PGA score to 3. Figure 3 shows the clinical response after approximately 6 weeks of treatment.
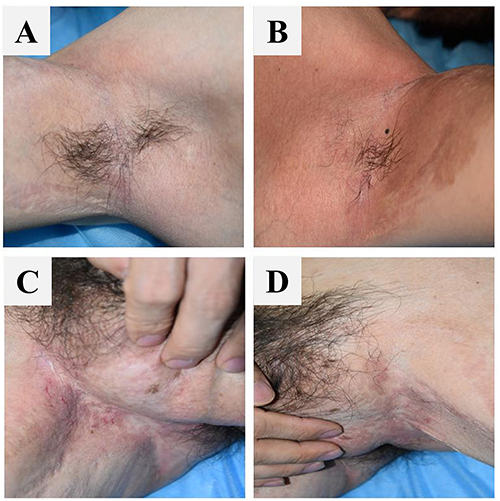 |
Figure 3 Clinical Response During Approximately 6 weeks of Treatment. (A) Right axilla; (B) Left axilla; (C) Right inguinal region; (D) Left inguinal region. |
By the conclusion of Phase 1 at Week 14, the treated right axilla had achieved complete clearance, presenting only post-inflammatory hyperpigmentation. The untreated areas continued to show sustained improvement, with the total BSA reduced to 2%. Figure 4 shows significant improvement and re-epithelialization.
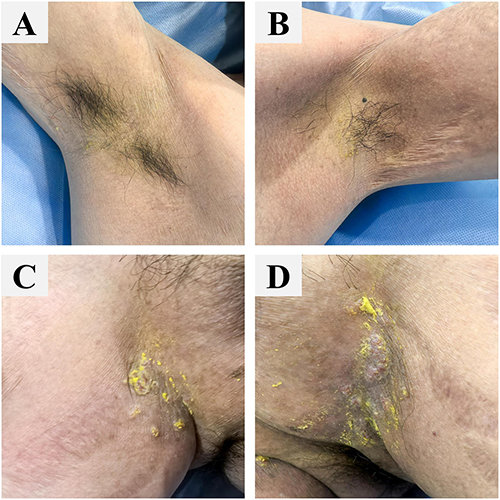 |
Figure 4 Follow-up Assessment at Week 14. (A) Right axilla; (B) Left axilla; (C) Right inguinal region; (D) Left inguinal region. |
Following the targeted treatment of the groin in Phase 2, near-complete remission was achieved across all body sites by Week 27. The inguinal lesions resolved fully, leaving only minimal residual erythema. At the end of the 189-day treatment course, the patient’s clinical metrics had improved dramatically: the PGA score was 1 (almost clear), the BSA was <1%, the DLQI improved to 2/30, and the VAS pain score dropped to 0/10 (Figure 5).
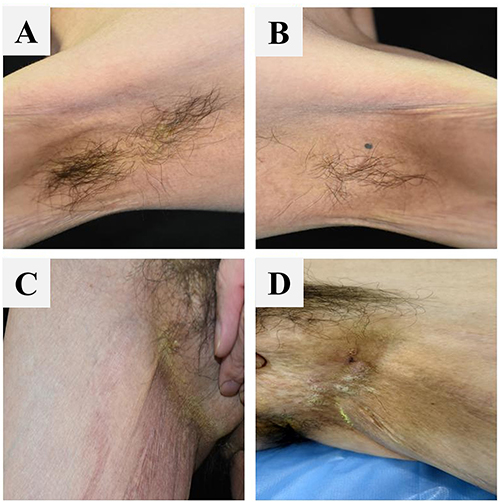 |
Figure 5 Interim Follow-up at 6 Months Post-treatment. (A) Right axilla; (B) Left axilla; (C) Right inguinal region; (D) Left inguinal region. |
A follow-up assessment conducted 11 months after the cessation of treatment confirmed sustained remission with no clinical recurrence, as shown in Figure 6.
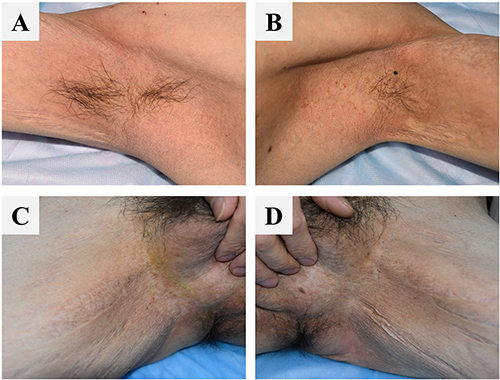 |
Figure 6 Sustained Remission at 11 Months Post-treatment. (A) Right axilla; (B) Left axilla; (C) Right inguinal region; (D) Left inguinal region. |
Discussion
This case suggests that localized infrared hyperthermia may have potential as a non-invasive adjunctive option for selected patients with long-standing, frequently relapsing Hailey–Hailey disease, particularly when lesions are localized to friction-prone intertriginous areas and previous therapies have provided only limited or temporary benefit. At present, this approach should not be considered a replacement for established therapies. Rather, it may be viewed as part of an individualized, stepwise management strategy integrated with standard topical and supportive care.
Despite multiple therapeutic options, long-term disease control in Hailey–Hailey disease remains challenging, especially in patients with chronic, recurrent flexural involvement. Published evidence is heterogeneous, and most recommendations are based on case reports, small series, retrospective studies, and expert opinion rather than large randomized trials. Current reviews therefore support an individualized treatment approach that takes into account disease severity, distribution, triggering factors, prior treatment response, comorbidities, patient preference, and practical feasibility.6
Systemic therapies may be considered for persistent or recurrent disease, but responses are variable and relapse after discontinuation is common. Reported options include tetracycline-class antibiotics, oral retinoids, dapsone, immunomodulatory or immunosuppressive agents, and other adjunctive systemic treatments. Low-dose naltrexone has attracted increasing interest in long-standing Hailey–Hailey disease, although current evidence remains limited to small clinical reports.7 Combination strategies have also been described; for example, alitretinoin combined with onabotulinumtoxinA improved long-standing vulvar disease, suggesting potential benefit from addressing both inflammation and sweating-related aggravation.8 More recently, biologics and small-molecule inhibitors have been explored, but their role remains uncertain because evidence is still largely limited to isolated cases and small series.9
Procedural and device-based therapies may benefit selected patients with localized long-standing lesions when conventional treatments are insufficient. Phototherapy, including narrowband ultraviolet B, has been reported in selected patients, but evidence remains limited, and treatment requires repeated visits, careful exposure of flexural sites, and consideration of recurrence after discontinuation. Photodynamic therapy has also been used, although pain, post-treatment inflammation, and variable durability may reduce its acceptability in flexural or erosive lesions. Botulinum toxin is of particular interest because sweating is a recognized aggravating factor. A systematic review found improvement in many reported cases, although treatment protocols and durability varied substantially.10 A double-blind placebo-controlled study suggested possible benefit of onabotulinumtoxinA in selected patients, although larger studies are needed.11 Ablative laser therapy, dermabrasion, and related energy-based procedures have also been used for localized long-standing disease.12 Carbon dioxide laser resurfacing has shown favorable outcomes in some reports, but pain, wound care, recovery time, dyspigmentation, scarring risk, and practical limitations in flexural areas may restrict its use.13
These therapeutic limitations highlight the need for well-tolerated adjunctive strategies suitable for long-term management. Topical corticosteroids remain useful for short-term inflammatory control, but repeated or prolonged use on intertriginous skin may increase the risk of atrophy, barrier fragility, telangiectasia, striae, and secondary complications.14,15 In this context, a non-invasive modality that may reduce local disease activity or improve the cutaneous microenvironment without increasing corticosteroid burden would be clinically relevant.
In the present patient, the disease was distressing and frequently relapsing but remained relatively localized. Further systemic escalation was not favored at that stage because prior therapies had produced only limited or temporary benefit, relapse after withdrawal was a concern, and additional cumulative adverse effects were undesirable. Narrowband ultraviolet B and photodynamic therapy were considered less practical because of the need for repeated sessions, difficulty exposing involved flexural sites, possible discomfort, and uncertain durability. Ablative laser therapy and dermabrasion were also considered, but the patient’s occupational demands made painful procedures, wound care, and prolonged recovery less acceptable Botulinum toxin was another reasonable option, particularly if sweating was a dominant aggravating factor, but repeated injections, cost, access, and patient preference influenced feasibility. Localized infrared hyperthermia was therefore selected as a pragmatic adjunct to standard topical supportive care rather than as a standalone or replacement therapy.
Clinical improvement was observed in both physician-assessed and patient-reported outcomes. Because no universally accepted Hailey–Hailey disease-specific severity score is routinely used in clinical practice, response was monitored using Physician Global Assessment, body surface area involvement, serial clinical photographs, and the Dermatology Life Quality Index. During treatment and follow-up, the Physician Global Assessment score decreased from 4 to 1, body surface area involvement decreased from 4% to less than 1%, and the Dermatology Life Quality Index improved from 23 to 2. These changes were accompanied by visible reductions in erythema, maceration, erosion, exudation, malodor, pruritus, and pain. No clinically significant recurrence was observed during 11 months of follow-up, findings consistent with near-complete clinical remission and substantial improvement in quality of life.
The mechanism by which localized infrared hyperthermia may have contributed to improvement remains uncertain. Although heat and sweating are recognized aggravating factors in Hailey–Hailey disease, the intervention used here differed from uncontrolled environmental heat exposure because it was localized, time-limited, protocolized, and clinically supervised. One possible explanation is that controlled localized hyperthermia may have helped modify the chronically moist and macerated intertriginous microenvironment, thereby supporting drying, re-epithelialization, symptom relief, and barrier recovery. This effect may have acted alongside topical anti-inflammatory treatment and supportive skin care to interrupt the cycle of friction, sweating, maceration, inflammation, and recurrent epidermal breakdown. Its potential benefit in this setting may therefore relate less to correction of the inherited adhesion defect itself than to modification of external factors that perpetuate disease activity. However, no mechanistic assessments were performed, and tissue-repair, microbiome-related, microcirculatory, or immunomodulatory explanations remain speculative.
An additional observation was that improvement appeared earlier and more prominently at the infrared-treated axillary site, whereas untreated areas improved more gradually. Although this temporal pattern is clinically interesting, it does not establish a remote or systemic effect. Improvement outside the treated area should be interpreted cautiously, as concomitant topical care and the fluctuating natural course of the disease may also have contributed. Intra-patient comparative studies are needed to determine whether localized infrared hyperthermia acts predominantly through local microenvironmental modification or may have broader biologic effects.
Several limitations should be acknowledged. This is a single-case observation without a control condition, and definitive causality cannot be established. Concomitant standard topical and supportive treatment was maintained throughout the treatment course, and spontaneous disease fluctuation or regression to the mean cannot be excluded. In addition, the improvement noted outside the treated area should be interpreted cautiously, and the underlying mechanism remains uncertain. The generalizability of this experience is therefore limited. Although the absence of clinically significant recurrence during 11 months of follow-up is encouraging, longer-term observation remains necessary. Future prospective studies with standardized outcome measures and appropriate controls will help clarify the optimal treatment parameters, safety, durability of benefit, and precise role of localized infrared hyperthermia in the stepwise management of Hailey–Hailey disease.
Conclusion
In summary, this single case suggests that localized infrared hyperthermia may be a safe, well-tolerated, non-invasive adjunctive therapy for selected patients with long-standing, frequently relapsing Hailey–Hailey disease. In our patient, its use was associated with marked clinical improvement and sustained remission during 11 months of follow-up. However, Given the single-case design and concomitant treatment, further studies are needed to clarify its role, optimal parameters, and durability of benefit.
Funding
Sichuan Province Regional Innovation Cooperation Project (22QYCX0191); Chengdu Medical Research Project (2025035).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Deng H, Xiao H. The role of the ATP2C1 gene in Hailey-Hailey disease. Cell Mol Life Sci. 2017;74(20):3687–8. doi:10.1007/s00018-017-2544-7
2. Ben Lagha I, Ashack K, Khachemoune A. Hailey-Hailey disease: an update review with a focus on treatment data. Am J Clin Dermatol. 2020;21(1):49–68.
3. Gisondi P, Sampogna F, Annessi G, et al. Severe impairment of quality of life in Hailey-Hailey disease. Acta Derm Venereol. 2005;85(2):132–135. doi:10.1080/00015550410025462
4. Rogner DF, Lammer J, Zink A, et al. Darier and Hailey-Hailey disease: update 2021. J Dtsch Dermatol Ges. 2021;19(10):1478–1501.
5. Porro AM, Arai Seque C, Miyamoto D, et al. Hailey-Hailey disease: clinical, diagnostic and therapeutic update. An Bras Dermatol. 2024;99(5):651–661. doi:10.1016/j.abd.2023.12.003
6. Sardana K, Bansal A, Muddebihal A, et al. Therapeutic agents for Hailey-Hailey disease: a narrative review. Indian J Dermatol Venereol Leprol. 2025;91(4):462–469.
7. Albers LN, Arbiser JL, Feldman RJ. Treatment of Hailey-Hailey disease with low-dose naltrexone. JAMA Dermatol. 2017;153(10):1018–1020. doi:10.1001/jamadermatol.2017.2446
8. Lemieux A, Funaro D. Recalcitrant vulvar Hailey-Hailey disease treated with alitretinoin and onabotulinumtoxinA: a case report. SAGE Open Med Case Rep. 2020;8:2050313X20905678.
9. Liu W, Xue X, Li S. Treatment of Hailey-Hailey disease with biologics and small molecule inhibitors: a systematic review. Clin Exp Dermatol. 2025;50(1):38–45. doi:10.1093/ced/llae298
10. Zhang H, Tang K, Wang Y, et al. Botulinum toxin in treating Hailey-Hailey disease: a systematic review. J Cosmet Dermatol. 2021;20(5):1396–1402. doi:10.1111/jocd.13963
11. Saal R, Oldfield C, Bota J, et al. Double-blind, placebo-controlled study of onabotulinumtoxinA for the treatment of Hailey-Hailey disease. J Drugs Dermatol. 2023;22(4):339–343. doi:10.36849/JDD.6857
12. Farahnik B, Blattner CM, Mortazie MB, et al. Interventional treatments for Hailey-Hailey disease. J Am Acad Dermatol. 2017;76(3):551–558.e3. doi:10.1016/j.jaad.2016.08.039
13. Faltoizpurua LA, Griffith RD, Yazdani Abyaneh MA, et al. Laser therapy for the treatment of Hailey-Hailey disease: a systematic review with focus on carbon dioxide laser resurfacing. J Eur Acad Dermatol Venereol. 2015;29(6):1045–1052. doi:10.1111/jdv.12875
14. Niculet E, Bobeica C, Tatu AL. Glucocorticoid-induced skin atrophy: the old and the new. Clin Cosmet Investig Dermatol. 2020;13:1041–1050.
15. Gabros S, Nessel TA, Zito PM. Topical corticosteroids. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.