Back to Journals » Hepatic Medicine: Evidence and Research » Volume 16
Liver Dysfunction in Hyperthyroidism
Authors Khongsaengbhak T, Atthakitmongkol T ![]() , Tanwandee T
, Tanwandee T ![]()
Received 11 September 2024
Accepted for publication 5 November 2024
Published 8 November 2024 Volume 2024:16 Pages 81—89
DOI https://doi.org/10.2147/HMER.S487794
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gerry Lake-Bakaar
Thitichaya Khongsaengbhak,1 Thanapat Atthakitmongkol,2 Tawesak Tanwandee2
1Department of Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand; 2Division of Gastroenterology, Department of Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Tawesak Tanwandee, Division of Gastroenterology, Department of Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, 10700, Thailand, Tel +66 2 419 7281-2, Fax +66 2 411 5013, Email [email protected]; [email protected]
Background: Thyrotoxicosis is often associated with abnormal liver tests. This study aimed to characterize the clinical features and laboratory findings in thyrotoxic patients with liver abnormalities and to identify predictive factors for differentiating thyroid storm within this population.
Methods: This is a retrospective review of thyrotoxic patients with hepatic dysfunction between January 2015, and January 2021, at Siriraj Hospital, Thailand. Univariate and multivariate analyses were performed to identify the factors associated with thyroid storm.
Results: Among 771 thyrotoxic patients, 43 revealed abnormal liver tests within six months of diagnosis (5.58%). The mean age was 53.16 ± 15.10 years, with a female predominance (60.5%), and the majority (97.7%) were diagnosed with Graves’ disease. The most common comorbidities were atrial fibrillation, heart failure, and dyslipidemia. Hepatic dysfunction presented as non-specific, with 46.5% showing a cholestatic pattern, 30.2% a mixed pattern, and 20.9% a hepatocellular pattern. The most possible etiologies of hepatic dysfunction were hyperthyroidism-related hepatitis (41.9%) with atrial fibrillation with congestive hepatopathy (38.9%), concomitant with chronic hepatitis C infection (14.0%), and methimazole-induced hepatic dysfunction (9.3%). The younger age, congestive heart failure, and total bilirubin levels ≥ 3.0 mg/dL were independent factors in distinguishing clinical thyroid storm among thyrotoxic patients without thyroid storm.
Conclusion: Liver abnormalities can be observed in patients with thyrotoxicosis. The possible causes are multifactorial, including hyperthyroidism-related hepatitis, atrial fibrillation with congestive hepatopathy, and chronic hepatitis C infection. Younger age, congestive heart failure, and total bilirubin ≥ 3.0 mg/dL were predictive factors for thyroid storm diagnosis among thyrotoxic patients.
Keywords: hepatic dysfunction, hyperthyroidism, liver abnormality, thyrotoxicosis, thyroid storm
Introduction
Thyroid hormones play a crucial role in regulating thermogenesis and human metabolism. These effects are mediated by regulating various cell types, including hepatocytes, influencing hepatic function. Furthermore, liver cells are integral in regulating thyroid hormones, including hormone activation and inactivation, transport, and metabolism. Up to 85% of thyroxine (T4) is converted to triiodothyronine (T3) peripherally by liver cells. Additionally, liver cells synthesize plasma proteins that bind up to 99% of the thyroid hormones present in plasma.1,2
Thyrotoxicosis is a condition caused by excess circulating thyroid hormones, regardless of the underlying cause.2 The global prevalence of thyrotoxicosis ranges from approximately 0.2% to 1.3% in iodine-sufficient regions, with a higher incidence in females.3 Graves’ disease is the most common cause of hyperthyroidism, particularly affecting young to middle-aged individuals, predominantly women, with a female-to-male incidence ratio of approximately 7 to 10:1.4
Gastrointestinal manifestations of thyrotoxicosis include increased gut motility, which can lead to hyperdefecation and malabsorption. Abnormalities in liver function tests have been reported in association with hyperthyroidism, though their frequency varies across studies. Previous studies have found that between 15% and 76% of patients had at least one liver biochemical abnormality at the time of hyperthyroidism diagnosis.5–8 Unexplained jaundice, indicative of hepatic dysfunction, is an important symptom of thyroid storm and is included as a diagnostic criterion in both the Burch-Wartofsky Point Scale and the guidelines of the Japanese Thyroid Association.9,10 The proposed mechanisms of liver dysfunction associated with hyperthyroidism are direct liver toxicity from prolonged excessive thyroid hormone exposure and hepatocyte anoxia with free-radical damage as a result of the hypermetabolic state, hepatocyte degeneration from accelerated liver glycogen and protein breakdown, autoimmune-related liver disease, congestive hepatopathy from concomitant thyrotoxic heart failure, previous underlying liver disease and antithyroid medication-related liver toxicity and injury.7,11–14
In this study, we aimed to characterize hepatic dysfunction and identify potential causes of hepatic dysfunction in Thai patients recently diagnosed with thyrotoxicosis.
Materials and Methods
Study Patients
This study retrospectively reviewed all patients diagnosed with liver test abnormality within 6 months after being diagnosed with thyrotoxicosis at Siriraj Hospital, Bangkok, Thailand, from January 1, 2015, to January 31, 2021. Diagnoses were based on the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) codes E05 concomitant with K701-K754, R17 or B15-B19. The study protocol was approved by the Siriraj Institutional Review Board (certificate of approval number Si 029/2020). The requirement to obtain informed consent was waived due to the retrospective nature of the study.
Eligible patients were over 18 years old and had a diagnosis of hyperthyroidism with thyroid hormone levels [triiodothyronine (T3) and/ or thyroxine (T4)] above the upper normal limit, and thyroid-stimulating hormone (TSH) levels below 0.05 mU/L without prior administration of thyroid hormones. Patients with thyroiditis (acute, subacute, or autoimmune) or those whose clinical features during follow-up were incompatible with thyrotoxicosis were excluded.
Medical Data Collection
Patient medical data were retrieved from electronic medical records. Collected demographic data comprised the age at the time of thyrotoxicosis diagnosis and gender. Comorbidities such as atrial fibrillation, heart failure, dyslipidemia, diabetes mellitus, renal disease, and liver status (chronic hepatitis or cirrhosis) with the etiologies of chronic liver disease were also recorded. Data were collected on clinical history and laboratory test results including TSH, triiodothyronine (T3 or free T3), thyroxine (T4 or free T4), and liver function tests [alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), total bilirubin, direct bilirubin, albumin, and globulin] throughout the clinical course of the disease. Clinical outcomes were also noted.
Statistical Analysis
The age of the patients is presented as mean ± standard deviation. Gender, comorbidities, chronic liver status, and hyperthyroidism diagnoses are expressed as percentage values. Laboratory test results, including initial, peak, and resolution levels, are summarized as median values with interquartile ranges or as means with standard deviations. Univariate analysis was used to identify predictive factors for thyroid storm in patients with thyrotoxicosis. Multivariate analysis was performed to determine independent factors that significantly predict thyroid storm among these patients, using forward stepwise logistic regression. The significant predictors (p < 0.05) in the univariate analysis were included to identify the best multivariate model. A p-value less than 0.05 was considered statistically significant. All statistical calculations were performed using PASW Statistics, version 18 (SPSS Inc., Chicago, IL, USA).
Results
Of the 771 patients with thyrotoxicosis, 43 (5.58%) were found to have abnormal liver function tests within six months of their thyrotoxicosis diagnosis, between January 1, 2015, and January 31, 2021, at Siriraj Hospital, Mahidol University, Bangkok, Thailand. The baseline characteristics are summarized in Table 1. The mean age was 53.16 ± 15.10 years, with a female predominance of 60.5%. Thirty-five patients (81.4%) had comorbidities, including atrial fibrillation (25.6%), heart failure (23.3%), dyslipidemia (23.3%), diabetes (18.6%), and renal disease (4.7%). Chronic liver diseases were present in 18 patients (41.9%), with chronic hepatitis C being the most common etiology, followed by chronic hepatitis B, autoimmune hepatitis, and nonalcoholic fatty liver disease (NAFLD). Only two patients (4.7%) had cirrhosis.
 |
Table 1 Baseline Characteristics of the 43 Patients with Thyrotoxicosis and Liver Dysfunction |
Most patients with thyrotoxicosis were diagnosed with Graves’ disease (97.7%), with only one patient having amiodarone-induced thyrotoxicosis. At the initial presentation, 9 of 43 patients (20.9%) had a clinical diagnosis of thyroid storm. Twenty-three patients (53.5%) had at least one abnormal liver test at the time of thyrotoxicosis diagnosis, while the remaining patients revealed abnormal liver tests at a median of 5.79 weeks (interquartile range [IQR] 4.07–16.57) after the diagnosis of thyrotoxicosis. Abnormal liver tests among patients with thyrotoxicosis were classified according to the R factor for liver injury, which depends on ALT and alkaline phosphatase levels.15 Most patients exhibited a cholestatic pattern (46.5%), followed by a mixed pattern (30.2%) and a hepatocellular pattern (20.9%). Although hepatic outcomes after treatment of thyrotoxicosis largely resolved, with about 76.7% of patients showing improvement, nearly one-fourth of patients had persistent abnormal liver tests.
The laboratory tests, including thyroid hormones, TSH, and liver function tests investigated during the clinical course of thyrotoxicosis treatment, are summarized in Table 2. For thyroid function tests (TSH, T4, FT4, T3, and FT3) the initial laboratory results were nearly similar to the peak values observed during the clinical course. After treatment, all thyroid function tests showed improvement and returned to normal ranges. At the time of thyrotoxicosis diagnosis, the mean TSH level was 0.01 ± 0.02 uIU/mL, which was similar to the maximal level observed during the clinical course, 0.01 ± 0.01 uIU/mL. For liver function tests, Figure 1 demonstrates the trends and levels of liver function tests, including AST, ALT, ALP, total bilirubin, and direct bilirubin, at initial abnormality, peak abnormality, and after resolution among thyrotoxic patients. Patients with hepatocellular and mixed injury showed elevated liver enzymes both at the first liver function abnormality and slightly increased levels at the peak of the clinical course. The median AST levels were 64.5 U/L (IQR, 42.0–110.0) at the initial liver abnormality and 80.0 U/L (IQR, 63.0–172.0) at peak, and the median ALT levels were 70.0 U/L (IQR, 26.0–105.0) at initial liver abnormality and 91.0 U/L (IQR, 52.0–105.0) at peak. In patients with cholestatic or mixed liver injury, ALP levels showed mild elevation both at the initial liver abnormality and at peak levels. The median ALP levels were 137.5 U/L (IQR, 102.0–195.0) at the initial liver abnormality and 164.0 U/L (IQR, 126.5–221.5) at the maximum levels. Albumin levels were similar at the initial liver abnormality and at the peak of the clinical course, with values of 3.28 ± 0.69 g/dL and 3.27 ± 0.75 g/dL, respectively. Finally, all liver function tests declined and became within normal range after resolve of thyrotoxicosis.
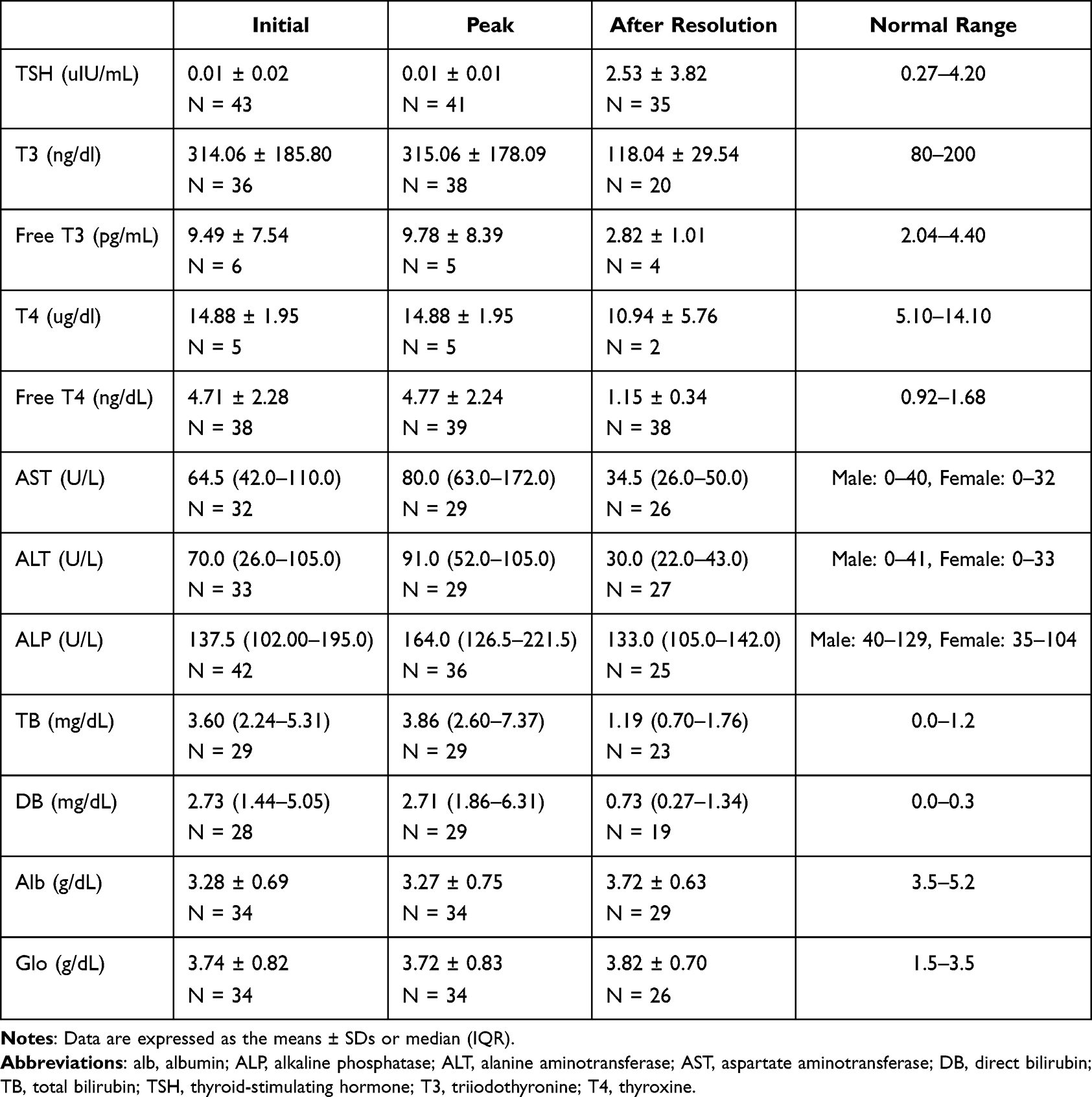 |
Table 2 Thyroid Function Test and Liver Function Test at Initial Abnormalities, Peak Abnormalities, and After Resolution of 43 Patients with Thyrotoxicosis |
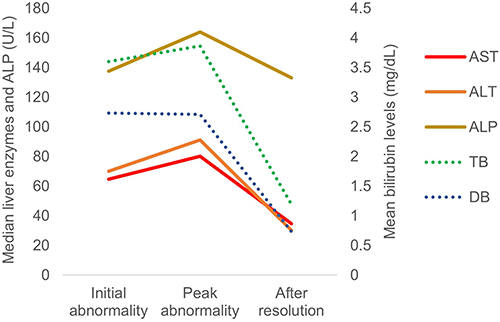 |
Figure 1 Shows the median levels of liver enzymes and bilirubin at initial abnormality, peak abnormality, and after resolution in patients with thyrotoxicosis. Abbreviations: ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; DB, direct bilirubin; TB, total bilirubin. |
Possible causes of liver dysfunction in patients with thyrotoxicosis from our study are shown in Table 3. The most common cause was hyperthyroidism-related hepatitis, found in 18 patients (41.9%). Among these 18 patients, 7 (38.9%) had atrial fibrillation due to hyperthyroidism with congestive hepatopathy. Additionally, there were 2 cases (4.7%) of congestive heart failure not definitively related to hyperthyroidism. Some patients had underlying chronic liver diseases such as chronic hepatitis C (14.0%), autoimmune hepatitis (7.0%), chronic hepatitis B with reactivation (2.3%), and NAFLD (2.3%). As a complication of thyrotoxicosis treatment, methimazole (MMI)-induced hepatic dysfunction occurred in 4 cases (9.3%). The pattern of liver injury varied: 2 patients had hepatocellular injury, while 1 patient each showed cholestatic and mixed injury. All these patients underwent I-131 ablation therapy, and liver function tests normalized in 3 out of the 4 patients. However, the patient with cholestatic liver injury continued to exhibit persistent cholestasis, and a liver biopsy confirmed cholangiopathy consistent with MMI-induced cholestasis. Other drug-induced liver injuries were reported in up to 7.0% of cases, with the culprit drugs including a combination of amoxicillin and clavulanic acid, meropenem, and acetaminophen.
 |
Table 3 Possible Cause of Hepatic Dysfunction in Thyrotoxicosis |
Table 4 shows the univariate and multivariate analysis to identify clinical factors that predicted the clinical thyroid storm among patients with thyrotoxicosis. Several clinical predictors were identified that could differentiate patients with clinical thyroid storm from those with thyrotoxicosis who did not meet the criteria for thyroid storm. In univariate analysis, factors that increased the risk of clinical thyroid storm compared to no clinical thyroid storm included younger age, presence of congestive heart failure, body temperature ≥ 38°C, tachycardia with a heart rate ≥ 130 beats per minute, and total bilirubin level ≥ 3.0 mg/dL. For central nervous system (CNS) involvement, one of the criteria for diagnosing thyroid storm, no patients with thyrotoxicosis who were not diagnosed with thyroid storm had CNS involvement. Therefore, CNS involvement was excluded from this univariate analysis. However, liver function tests other than bilirubin levels, as well as other gastrointestinal symptoms, were not statistically significant in differentiating clinical thyroid storm among patients with thyrotoxicosis. After adjusting for the subdistribution of the predictors in multivariable logistic regression analysis, only three factors: younger age, presence of congestive heart failure, and total bilirubin level ≥ 3.0 mg/dL, remained significant clinical predictors for thyroid storm among these patients.
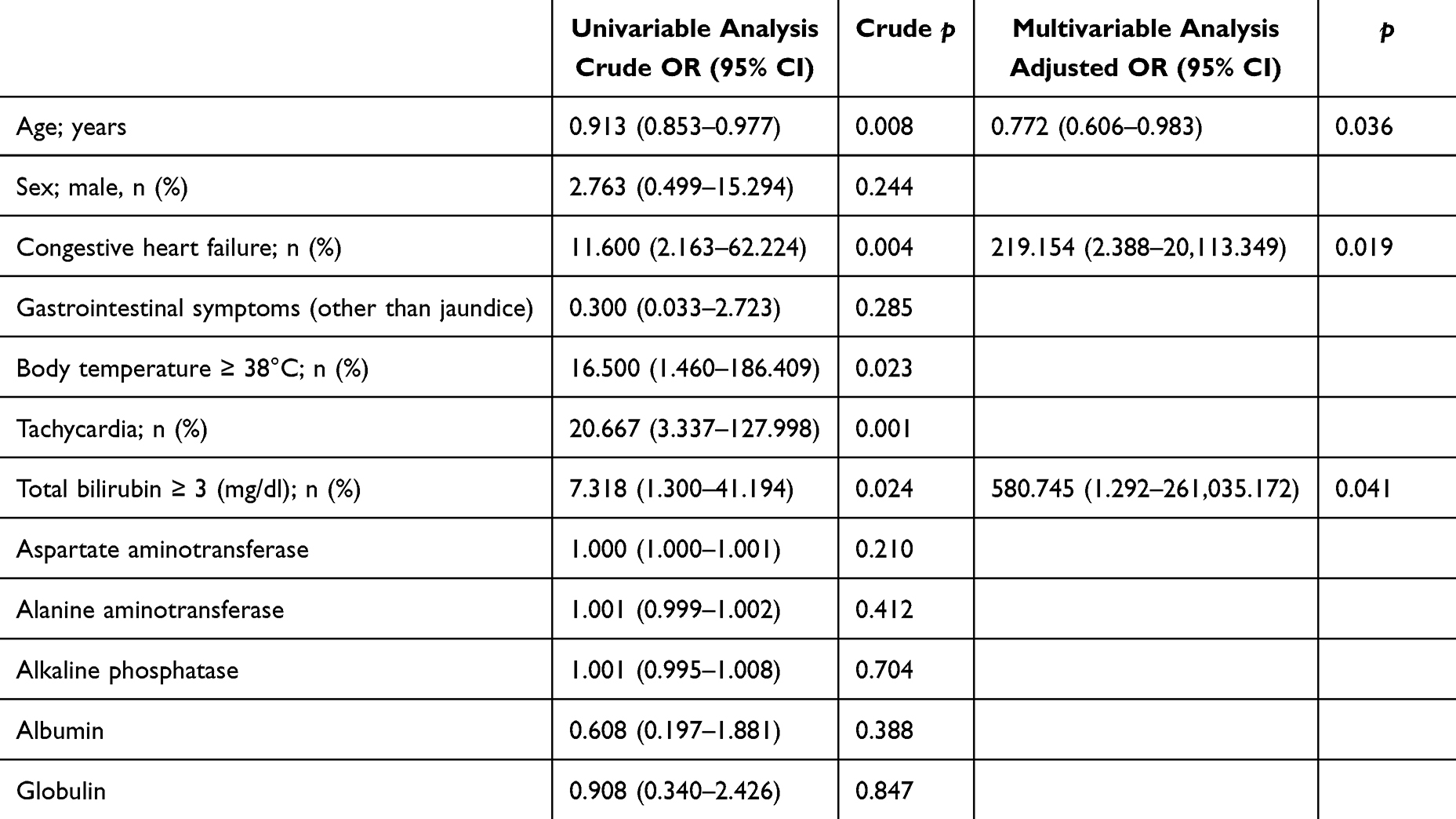 |
Table 4 Univariate and Multivariate Analyses of Predictors Differentiating Patients with Thyroid Storm from Thyrotoxic Patients Without Thyroid Storm |
Discussion
Hepatic dysfunction has been associated with hyperthyroidism either at the initial diagnosis or developed during ongoing treatment. These abnormalities may result from direct injury from thyrotoxicosis, underlying chronic liver diseases, subsequent liver dysfunction caused by thyrotoxicosis, or treatment-related complications.5–8,14 Our study describes the demographic data, laboratory findings, and possible causes of hepatic dysfunction among patients with thyrotoxicosis, as well as the independent clinical predictive factors for clinical thyroid storm, in a tertiary healthcare center in Thailand.
The prevalence of liver biochemical abnormalities among patients with thyrotoxicosis in our study was 5.58%, which is lower compared to previous studies reporting a prevalence range of 15–76%.5–8 This discrepancy may be due to underestimation, as not all patients diagnosed with thyrotoxicosis routinely undergo liver function tests, especially those with mild clinical symptoms, no jaundice, or no suspicion of preexisting liver diseases. Moreover, our data retrieved based on ICD-10-CM codes might miss diagnoses in cases who slightly elevated in laboratory levels and rapidly normalized after initial treatment.
Approximately one-fourth of all our patients had atrial fibrillation, consistent with previous reports indicating that atrial fibrillation occurs in 10 to 25% of patients with hyperthyroidism. Moreover, hyperthyroidism alters hemodynamics and reduces myocardial contractile reserve, precluding further increases in ejection fraction and cardiac output during exertion, which can result in high-output heart failure. Longstanding hyperthyroidism may consequence in decreased cardiac contractility, abnormal diastolic compliance, and pulmonary congestion, ultimately resulting in congestive heart failure.16,17 Additionally, in our study, 18.6% of patients had diabetes, irrespective of the type or glycemic status. The prevalence of thyroid dysfunction regardless of autoimmune antibodies among type 2 diabetes mellitus was up to 16%.18,19 Increased insulin resistance occurs and is the mainly cause of metabolic alterations in patients with thyrotoxicosis because excess thyroid hormone elevates endogenous glucose synthesis, increases insulin requirement, and decreases hepatic insulin sensitivity.20
Our result shows that 41.9% of the patients had preexisting chronic liver diseases, with eight patients (18.6%) having chronic hepatitis C. Previous studies have shown that chronic hepatitis C is associated with autoimmune thyroid disease, both with and without interferon-α (IFN-α) treatment.21,22 The prevalence of patients seropositive for anti-HCV was 21.4%, while the prevalence of hyperthyroidism among patients with chronic hepatitis C is up to 10%.23,24 The proposed mechanisms may involve hepatitis C virus-related extrahepatic manifestations through immunological disorders or the triggering of latent autoimmune thyroiditis by IFN-α.22,25 For another chronic liver comorbidity, although hyperthyroidism is rarely reported to be associated with autoimmune hepatitis, one study has shown that 6% of patients with Graves’ disease also have autoimmune hepatitis.1 Our result revealed that 4.7% of patients with thyrotoxicosis with hepatic dysfunction had autoimmune hepatitis.
A systematic review and meta-analysis have demonstrated the prevalence of abnormal liver tests among patients with hyperthyroidism: 23% for AST, 33% for ALT, 44% for ALP, and 12% for bilirubin.26 Our study classified patients with abnormal liver tests according to the R factor for liver injury. The majority of these patients exhibited cholestatic liver injury (46.5%), characterized by a prominent elevation of alkaline phosphatase levels. This data may overestimate the prevalence of cholestatic liver injury, as elevated alkaline phosphatase is not specific to hepatic sources alone. Although elevated alkaline phosphatase levels have been reported in up to 67% of thyrotoxic patients, these elevations may result from hormone-induced cholestasis as well as increased osteoblast activity.2,27 For hepatocellular injury, our data showed mild elevation of liver enzymes, with median peak levels of AST and ALT being 80 IU/L and 91 IU/L, respectively. The study reported elevations in AST and ALT levels to 50.6 ± 3.5 IU/L and 48.6 ± 4.9 IU/L, respectively.27 Our data showed higher levels of both AST and ALT because we specifically analyzed thyrotoxic patients with either hepatocellular or mixed injury, excluding those with cholestatic injury. However, in severe cases of hepatocellular injury, AST and ALT levels can markedly rise, reaching up to 80.3 and 45 times the upper normal limit, respectively.11 Liver histology predominantly reveals non-specific changes on light microscopy, including mild lobular inflammation, nuclear changes, and Kupffer cell hyperplasia. In a few cases, more extensive hepatic damage is observed, characterized by centrizonal necrosis and perivenular fibrosis.1 Only a few reported cases have presented with fulminant liver failure.28
In thyroid storm, the diagnosis is based on the clinical manifestations and laboratory tests according to the Burch-Wartofsky Point Scale and the guidelines of the Japanese Thyroid Association.9,10 This study identified independent factors for distinguishing clinical thyroid storm from thyrotoxicosis without thyroid storm. These factors include advanced age, the presence of congestive heart failure, and hyperbilirubinemia with total bilirubin levels ≥ 3 mg/dL. Both congestive heart failure and unexplained jaundice are diagnostic criteria for thyroid storm according to established guidelines. Although gastrointestinal symptoms other than jaundice and high body temperature (≥ 38°C) are diagnostic criteria for thyroid storm, they did not prove to be significant predictors after univariate and multivariate analyses. Moreover, liver test abnormalities, except bilirubin levels, did not significantly predict thyroid storm among thyrotoxic patients. However, a few case reports showed that thyroid storm can cause severe fulminant hepatitis or acute liver failure, with AST and ALT levels rising to several hundred to over 1000 IU/L.29,30
There are several limitations in our study. Firstly, it was conducted at a single center, Siriraj Hospital, a tertiary university center, which may not represent the broader Thai population or accurately reflect all regions of Thailand. Secondly, being a retrospective cohort study, it may miss diagnoses in cases with mild liver test abnormalities that spontaneously resolve after thyrotoxicosis treatment. Consequently, the prevalence of abnormal liver tests among patients with thyrotoxicosis may be underestimated. Moreover, some laboratory data may be missing or incomplete due to variations in follow-up duration and decision-making by primary physicians. Finally, most causes of liver dysfunction among thyrotoxic patients in our study are presumed, with neither definitive proof nor biopsy confirmation.
Conclusion
Liver abnormalities in patients with thyrotoxicosis are varied and not specific to any particular pattern of liver injury. The causes are mostly multifactorial, with the main contributors being hyperthyroidism-related hepatitis, atrial fibrillation with congestive hepatopathy, and chronic hepatitis C infection. This study identified independent predictive factors differentiating clinical thyroid storm from thyrotoxicosis without thyroid storm, including younger age, congestive heart failure, and hyperbilirubinemia (total bilirubin ≥ 3.0 mg/dL).
Abbreviations
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; CNS, central nervous system; FT3, free triiodothyronine; FT4, free thyroxine; IFN-α, interferon-α; IQR, interquartile range; MMI, methimazole; NAFLD, nonalcoholic fatty liver disease; T3, triiodothyronine; T4, thyroxine; TSH, thyroid-stimulating hormone.
Ethics Approval and Consent to Participate
The study was reviewed and approved by the Siriraj Institutional Review Board (SIRB) (certificate of approval number Si 029/2020). The requirement for obtaining informed consent was waived due to the retrospective nature of the study, with confirmation that all data were maintained confidentially. All methods were performed in accordance with the Declaration of Helsinki.
Acknowledgments
We thank Khemajira Karaketklang (Department of Medicine, Faculty of Medicine Siriraj Hospital) for assistance in statistical analysis.
Funding
There was no financial support.
Disclosure
The authors declare no conflict of interest.
References
1. Malik R, Hodgson H. The relationship between the thyroid gland and the liver. QJM. 2002;95(9):559–569. doi:10.1093/qjmed/95.9.559
2. Piantanida E, Ippolito S, Gallo D, et al. The interplay between thyroid and liver: implications for clinical practice. J Endocrinol Invest. 2020;43(7):885–899. doi:10.1007/s40618-020-01208-6
3. Taylor PN, Albrecht D, Scholz A, et al. Global epidemiology of hyperthyroidism and hypothyroidism. Nat Rev Endocrinol. 2018;14(5):301–316. doi:10.1038/nrendo.2018.18
4. Nayak B, Hodak SP. Hyperthyroidism. Endocrinol Metab Clin North Am. 2007;36(3):617–656. doi:10.1016/j.ecl.2007.06.002
5. Fong TL, McHutchison JG, Reynolds TB. Hyperthyroidism and hepatic dysfunction. A case series analysis. J Clin Gastroenterol. 1992;14(3):240–244. doi:10.1097/00004836-199204000-00010
6. Aydemir S, Bayraktaroglu T, Demircan N, et al. Effect of hyperthyroidism and propylthiouracil treatment on liver biochemical tests. Int J Clin Pract. 2005;59(11):1304–1308. doi:10.1111/j.1368-5031.2005.00611.x
7. Kubota S, Amino N, Matsumoto Y, et al. Serial changes in liver function tests in patients with thyrotoxicosis induced by Graves’ disease and painless thyroiditis. Thyroid. 2008;18(3):283–287. doi:10.1089/thy.2007.0189
8. Khemichian S, Fong TL. Hepatic dysfunction in hyperthyroidism. Gastroenterol Hepatol. 2011;7(5):337–339.
9. Satoh T, Isozaki O, Suzuki A, et al. 2016 Guidelines for the management of thyroid storm from The Japan Thyroid Association and Japan Endocrine Society (First edition). Endocr J. 2016;63(12):1025–1064. doi:10.1507/endocrj.EJ16-0336
10. Burch HB, Wartofsky L. Life-threatening thyrotoxicosis. Thyroid Storm Endocrinol Metab Clin North Am. 1993;22(2):263–277. doi:10.1016/S0889-8529(18)30165-8
11. de Campos Mazo DF, de Vasconcelos GB, Pereira MA, et al. Clinical spectrum and therapeutic approach to hepatocellular injury in patients with hyperthyroidism. Clin Exp Gastroenterol. 2013;6:9–17. doi:10.2147/CEG.S39358
12. Bhuyan AK, Sarma D, Kaimal Saikia U, Choudhury BK. Grave’s Disease with Severe Hepatic Dysfunction: a Diagnostic and Therapeutic Challenge. Case Rep Med. 2014;2014:790458. doi:10.1155/2014/790458
13. He K, Hu Y, Xu XH, Mao XM. Hepatic dysfunction related to thyrotropin receptor antibody in patients with Graves’ disease. Exp Clin Endocrinol Diabetes. 2014;122(6):368–372. doi:10.1055/s-0034-1375667
14. Yorke E. Hyperthyroidism and Liver Dysfunction: a Review of a Common Comorbidity. Clin Med Insights Endocrinol Diabetes. 2022;15:11795514221074672. doi:10.1177/11795514221074672
15. Benichou C. Criteria of drug-induced liver disorders. Report of an international consensus meeting. J Hepatol. 1990;11(2):272–276. doi:10.1016/0168-8278(90)90124-a
16. Osuna PM, Udovcic M, Sharma MD. Hyperthyroidism and the Heart. Methodist DeBakey Cardiovasc J. 2017;13(2):60–63. doi:10.14797/mdcj-13-2-60
17. Frost L, Vestergaard P, Mosekilde L. Hyperthyroidism and risk of atrial fibrillation or flutter: a population-based study. Arch Intern Med. 2004;164(15):1675–1678. doi:10.1001/archinte.164.15.1675
18. Papazafiropoulou A, Sotiropoulos A, Kokolaki A, Kardara M, Stamataki P, Pappas S. Prevalence of thyroid dysfunction among Greek type 2 diabetic patients attending an outpatient clinic. J Clin Med Res. 2010;2(2):75–78. doi:10.4021/jocmr2010.03.281w
19. Akbar DH, Ahmed MM, Al-Mughales J. Thyroid dysfunction and thyroid autoimmunity in Saudi type 2 diabetics. Acta Diabetol. 2006;43(1):14–18. doi:10.1007/s00592-006-0204-8
20. Kim SY. Diabetes and Hyperthyroidism: is There a Causal Link? Endocrinol Metab. 2021;36(6):1175–1177. doi:10.3803/EnM.2021.602
21. Tran A, Quaranta JF, Benzaken S, et al. High prevalence of thyroid autoantibodies in a prospective series of patients with chronic hepatitis C before interferon therapy. Hepatology. 1993;18(2):253–257. doi:10.1002/hep.1840180205
22. Pateron D, Hartmann DJ, Duclos-Vallee JC, Jouanolle H, Beaugrand M. Latent autoimmune thyroid disease in patients with chronic HCV hepatitis. J Hepatol. 1992;16(1–2):244–245. doi:10.1016/s0168-8278(05)80124-2
23. Leri O, Sinopoli MT, Di Prima MA, Paggi A. Hepatitis C virus antibodies and Graves’ disease. BMJ. 1995;310(6972):128. doi:10.1136/bmj.310.6972.128d
24. Antonelli A, Ferri C, Pampana A, et al. Thyroid disorders in chronic hepatitis C. Am J Med. 2004;117(1):10–13. doi:10.1016/j.amjmed.2004.01.023
25. Ferrari SM, Fallahi P, Mancusi C, et al. HCV-related autoimmune disorders in HCV chronic infection. Clin Ter. 2013;164(4):e305–12. doi:10.7417/CT.2013.1594
26. Scappaticcio L, Longo M, Maiorino MI, et al. Abnormal Liver Blood Tests in Patients with Hyperthyroidism: systematic Review and Meta-Analysis. Thyroid. 2021;31(6):884–894. doi:10.1089/thy.2020.0715
27. Thompson P, Strum D, Boehm T, Wartofsky L. Abnormalities of Liver Function Tests In Thyrotoxicosis. Mil Med. 1978;143(8):548–551. doi:10.1093/milmed/143.8.548
28. Hambleton C, Buell J, Saggi B, Balart L, Shores NJ, Kandil E. Thyroid storm complicated by fulminant hepatic failure: case report and literature review. Ann Otol Rhinol Laryngol. 2013;122(11):679–682. doi:10.1177/000348941312201103
29. Hayat MH, Moazzam Z, Ziogas IA, Yousaf A, Hayat M. Thyroid Storm Presenting as Acute Liver Failure in a Patient with Graves’ Disease. Cureus. 2020;12(9):e10333. doi:10.7759/cureus.10333
30. Sasaki K, Yoshida A, Nakata Y, Mizote I, Sakata Y, Komuro I. A case of thyroid storm with multiple organ failure effectively treated with plasma exchange. Intern Med. 2011;50(22):2801–2805. doi:10.2169/internalmedicine.50.6078
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.