Back to Journals » International Journal of Nanomedicine » Volume 20
Liposome-Based Nanoparticle Delivery Systems for Lung Diseases: Opportunities and Challenges
Authors Zhang X, Tu S, Tian J, Liang Y, An Y, Zhang T, Guan H, Xiong B, Qin L, Li Y, Gong L ![]()
Received 5 May 2025
Accepted for publication 28 September 2025
Published 14 October 2025 Volume 2025:20 Pages 12485—12509
DOI https://doi.org/10.2147/IJN.S538382
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Krishna Nune
Xi Zhang,1,* Shiju Tu,1,* Jiahua Tian,1,* Yan Liang,1,2 Yiling An,1 Tianyou Zhang,1 Hongyun Guan,1 Bo Xiong,1 Li Qin,1 Yunfei Li,1 Ling Gong1
1Department of Respiratory and Critical Care Medicine, The Third Affiliated Hospital of Zunyi Medical University (The First People’s Hospital of Zunyi), Zunyi, Guizhou, People’s Republic of China; 2School of Laboratory Medicine, College of Medical Laboratory Technology, Harbin Medical University, Daqing, Heilongjiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ling Gong, Department of Respiratory and Critical Care Medicine, The Third Affiliated Hospital of Zunyi Medical University (The First People’s Hospital of Zunyi), Zunyi, Guizhou, People’s Republic of China, Email [email protected]
Abstract: The role of the lungs as one of the most important organs in the body cannot be overstated. When disease occurs in the lungs, due to the special physiological structure and barriers of the lungs, many drugs is often required to maintain the required blood concentration, which brings unbearable adverse drug reactions to the patients, reduces the tolerance of the patients to the drugs, and affects the effect of disease treatment. As a mature delivery system, liposomes are widely used in major fields, and more importantly, liposome-delivered drugs have been utilized in clinical treatments, effectively reducing the side effects of drugs and achieving excellent efficacy. This review describes in detail the physiological structure and barriers of the lungs and the structure of liposomes; then summarizes the application of liposomes in different lung diseases, as well as its drawbacks and advantages. Finally, we suggest that liposome-delivered nucleic acids are expected to be a new trend and approach for the treatment of lung diseases.
Keywords: liposomes, delivery system, lung disease, Lung anatomy
Introduction
The lung is the core organ of the human respiratory system, and its main function is to realize efficient gas exchange between the body and the external environment.1 The lungs are mainly composed of branched airways and billions of alveoli at the ends. Alveoli are the basic functional units of the lungs. Their core role lies in achieving efficient gas exchange, and they also have important structural maintenance and defense functions. More importantly, in addition to the core respiratory function, the lungs also undertake important non-respiratory functions, defending against inhaled pathogens and particulate matter through the mucociliary system and immune cells, and filtering tiny emboli in the blood.2 To sum up, lungs are extremely important organs in the human body.
The lungs are in the thoracic cavity, above the diaphragm, on both sides of the mediastinum, and cover the heart. They are divided into the left lung. The structure of the lungs is precise and efficient. The internal branches form a complex bronchial tree network, with hundreds of millions of thin-walled alveoli connected at the ends, forming a huge gas exchange interface.3 Air enters the left and right main bronchi through the trachea and then branches step by step into the lobar bronchi, segmental bronchi, small bronchi, thin bronchi until the terminal thin bronchi, and finally flows into the respiratory thin bronchi, alveolar ducts and alveolar sacs. The alveoli are the basic units of gas exchange, composed of extremely thin type I alveolar epithelial cells and scattered type II alveolar epithelial cells. Their walls are closely attached to a dense network of capillaries, forming a huge surface area for gas exchange.
The barrier of the lungs is a sophisticated multi-level defense system, with the core objective of protecting the fragile interface of qi and blood exchange and maintaining the stability of the internal environment. As shown in Figure 1B-D, the pulmonary barrier system is primarily categorized into the following components: 1) Physical barriers; 2) Biochemical barriers; 3) Cellular immune defenses; 4) The blood-gas barrier; and 5) Immunomodulatory factors. Then we will make a simple summary of these barriers. The mechanism of the physical barrier mainly involves the secretion of mucus by goblet cells in the airway epithelium to adhere to particulate matter, and the directional movement of cilia to remove foreign substances.4 Meanwhile, a closed barrier is formed between airway epithelial cells through tight junction proteins, preventing pathogens from penetrating. Finally, the foreign object stimulates the airway, triggering a strong exhaled airflow and physically expelling large particles. The biochemical barrier of the lungs mainly works by utilizing antibacterial substances, such as lysozyme, lactoferrin and defensins, etc.5 These antibacterial substances are directly used to kill pathogens, inhibit microbial colonization, regulate immune responses and maintain tissue homeostasis, thus forming a multi-level innate immune defense system. The cellular immune barrier of the lungs is collaboratively maintained by alveolar macrophages that continuously monitor and eliminate pathogens, dendritic cells that initiate adaptive immune responses, neutrophils that rapidly kill microorganisms, and NK cells that precisely target infected cells.6 Together, they form an intricate defense network safeguarding lung tissue homeostasis. The blood-gas barrier of the lungs is composed of an ultrathin structure of alveolar epithelial cells, basement membranes and capillary endothelial cells, which separates the alveolar cavity from the blood flow, allowing for efficient exchange of oxygen and carbon dioxide while preventing the transmembrane diffusion of pathogens and macromolecular substances.7 The immune regulatory barrier of the lungs maintains immune homeostasis by suppressing excessive inflammation through regulatory T cells, balancing immune responses with anti-inflammatory factors (such as IL-10), and transforming the phenotype of alveolar macrophages, achieving a dynamic balance between defense and tolerance.8 Damage to the lung barrier will trigger a vicious cycle: the failure of physical clearance leads to the retention of pathogens and particulate matter, inducing chronic inflammation (such as bronchitis); The disruption of the blood-gas barrier enables bacteria/liquids to invade the alveoli, causing pneumonia, pulmonary edema and even respiratory failure. Long-term damage can lead to irreversible lung tissue lesions (such as pulmonary fibrosis and chronic obstructive pulmonary disease), eventually resulting in progressive loss of respiratory function.
 |
Figure 1 (A) Pulmonary inhalation of material processes and the deposition locations and movement patterns of substances with different particle sizes; (B) Mucus cilia removal; (C) Alveolar macrophages and lung surface-active substances play a scavenging role; (D) Cellular and intracellular barriers. Created in BioRender. Xi, Z. (2025) https://BioRender.com/th2j0ee. |
In recent years, compared with systemic drug administration, research on the use of different delivery systems to deliver drugs to the lungs for the treatment of lung diseases has attracted increasing attention from researchers. The main advantages of drug delivery through the lungs are as follows. First, since the metabolic rate of drugs in the lungs is much lower than that in the liver. Therefore, lung delivery of drugs can avoid the first-pass effect, thereby greatly improving the bioavailability of drugs in vivo. Then, delivering drugs through the lungs can avoid the influence of acidic pH in the gastrointestinal tract, intestinal microorganisms and special enzymes on certain drugs, and will not cause unknown reactions with food in the digestive tract. Therefore, delivering therapeutic drugs through the lungs is a highly promising treatment approach.
Although lung delivery has many advantages. However, there are certain limitations in drug delivery to the lungs, although the direct delivery of drugs to the lungs is limited. The defense mechanism of the respiratory tract can prevent the entry of foreign substances, thus posing certain obstacles to the direct delivery of drugs to the lungs. Then, lung delivery of drugs has relatively strict requirements for the size of the drugs or particles. Therefore, how to ensure that the drug can be accurately delivered to the lesion site. This requires considering the aerodynamics of the particles and their size. Then, we summarized the aerodynamics and deposition sites of particles of different sizes. As shown in Figure 1A, the deposition of inhaled particles in the airways is influenced by multiple mechanisms. Among them, the aerodynamic diameter (AD) of the particles largely determines the deposition mode of the particles.9–11 It mainly falls into the following situations: 1) Larger particles with AD more than 5 µm may be impacted in the upper airway and atmospheric airway.12 This usually leads to the deposition of particles in the oropharynx area, increasing the risk of them entering the gastrointestinal tract rather than the airways. 2) AD particles between 1 and 5 µm will undergo gravitational sedimentation and deposit in the lower airway, terminal bronchioles and alveoli. 3) Nanoscale particles with AD below 1 µm can penetrate deep into the alveoli and randomly diffuse through Brownian motion. Ultrafine particles with AD below 1µm can not only diffuse into the alveolar area but also into the trachea and bronchi area, which promotes the wide distribution of drugs encapsulated by the delivery system throughout the lungs. However, different respiratory diseases affect different locations of the lungs. For instance, asthma mainly affects the upper airway, while COPD mainly affects the distal alveoli.13 Therefore, to successfully deliver drugs to the desired location, particle size is one of the important parameters that determine whether the delivery system can bypass physiological barriers and clearance mechanisms.
Nowadays, an increasing number of researchers are utilizing various drug delivery systems, such as liposomes, hydrogels, and biological carriers, which can address the issues associated with traditional treatment methods. Among them, nano delivery systems are widely used in drug delivery, cancer treatment, and other fields due to their excellent biocompatibility. We compared liposomes, solid lipid nanoparticles, polymer nanoparticles, and extracellular vesicles (Table 1). Detailed comparisons were made in terms of materials, structure, and drug loading types. Comparison shows that due to the unique structure and good drug loading rate of liposomes, they have been widely used in drug delivery systems, and some liposomes have already been launched on the market. Liposomes are also a prominent delivery system in nano delivery systems. Liposomes were proposed in 1964, with a diameter between 100–500 nm, mainly composed of self-assembled phospholipids.14 Phospholipids are composed of polar phosphate head groups and hydrophobic lipid tails.15 With the continuous deepening of research, human interest in liposome delivery drug therapy for diseases is increasing. Recently, due to the official approval of liposomes by the US FDA as a therapeutic carrier for drug delivery, liposomes have continuously entered clinical trials and achieved excellent therapeutic effects (Table 2). Liposomes self-assemble into a unique structure with a lipid membrane and a hydrophilic core, like the structure of cell membranes. As shown in Figure 2, liposome can be used to deliver hydrophobic and hydrophilic molecules and have biocompatibility and biodegradability. Liposomes possess characteristics such as enhancing the solubility of encapsulated substances, reducing the adverse reactions and toxicity of free drugs, flexible charge and size regulation, and the ability to undergo surface modification.16,17 Liposomes can deliver drugs to the lesion site through passive targeting. When inflammation or infection occurs at the lesion site, the endothelial space of the blood vessels will widen, which may cause liposomes to remain at the lesion site and thus achieve therapeutic effects.18 More importantly, unmodified liposomes may be captured by the mononuclear macrophage system and actively accumulate in organs such as the liver and spleen. Meanwhile, since the surface of liposomes is easy to modify, precise delivery can be achieved by modifying specific carriers on the surface.19 Antibodies, polypeptides and sugar chains can be modified on the surface, enabling liposomes to actively recognize and bind to target cells, and then release drugs to achieve therapeutic purposes. At present, due to the unique physical properties and good biocompatibility of liposomes, researchers use liposomes to encapsulate drugs for the treatment of clinical diseases. Excitingly, some liposomes have been successfully marketed and achieved good therapeutic effects. We have summarized the currently marketed liposomes (Table 1).
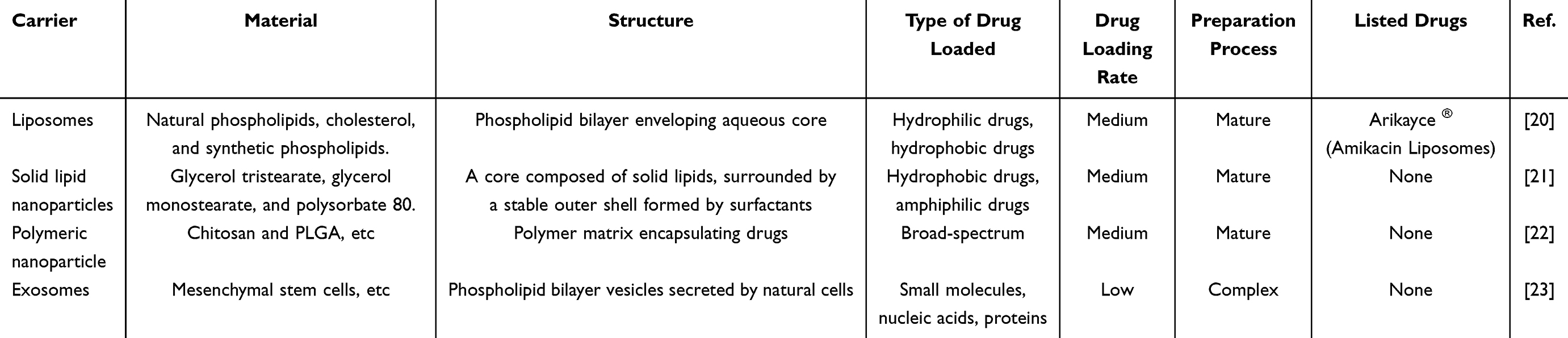 |
Table 1 Comparison of Different Nano Delivery Systems |
 |
Figure 2 Liposomes release drug at diseased alveoli through blood circulation. Created in BioRender. Xi, Z. (2025) https://BioRender.com/zrpched. |
 |
Table 2 Liposomal Delivery of Drugs for the Treatment of Clinical Diseases |
This study focuses on summarizing the structure, pharmacokinetics and liposomes that have entered clinical applications (Table 2). It also provides a detailed insight into the current applications of liposomes in different lung diseases, such as pneumonia, COPD, idiopathic pulmonary fibrosis and lung cancer. We have analyzed the advantages and disadvantages of these therapeutic approaches. More importantly, we conclude with an outlook on liposome-delivered gene therapy and an analysis of the disadvantages that currently exist.
Liposome
Liposomes are nanoscale spherical vesicles composed of phospholipid bilayers that mimic the structure of natural cell membranes, exhibiting excellent biocompatibility and biodegradability. These vesicular carriers enhance therapeutic efficacy by stabilizing the chemical properties of therapeutic agents, overcoming cellular and tissue uptake barriers, and improving biodistribution to target sites in vivo. This targeted delivery mechanism significantly minimizes systemic drug toxicity while optimizing therapeutic outcomes.39 As drug delivery systems, liposomes possess the unique capability to co-encapsulate both hydrophilic and hydrophobic therapeutics. Through surface engineering with targeting moieties such as antibodies, proteins, or ligand-receptor complexes, these nanostructured carriers can either prolong systemic circulation duration or achieve site-specific delivery to designated cellular and tissue targets, demonstrating enhanced therapeutic precision through spatial control of drug release.14,40 Nowadays, liposomes are widely used in anti-tumor drugs, gene delivery and vaccine delivery, etc.41 In this section, the structure of liposomes is introduced first, and the pharmacokinetic characteristics are described in detail. Secondly, summarize in detail the current market applications and potential of liposomes. Finally, the clinical problems existing in liposomes were analyzed to provide corresponding insights.
Liposome Structure and Classification
The main component of liposomes is glycerophospholipids, which are amphiphilic lipids composed of glycerol molecules bound to a phosphate group and two saturated or unsaturated fatty acid chains (Figure 3A). Liposome membranes can be composed of one or more lipid bilayer layers surrounding the internal water nucleation tissue, with polar head bases facing the internal and external water phases.42 This special structure provides liposomes with the ability to load and deliver molecules of different solubilities. Hydrophilic molecules are in the inner water nucleus, hydrophobic molecules in the lipid bilayer, and amphiphilic molecules at the interface of the water/lipid bilayer. The core components of liposomes are mainly phospholipids and cholesterol. Phospholipids are one of the important skeletons of liposomes. Common phospholipid molecules mainly include natural phospholipids and synthetic phospholipids. The proportion of cholesterol is usually 30–50%. It reduces the fluidity of the membrane by filling the gaps in the phospholipid tails, thereby reducing drug leakage and ultimately ensuring that the drug can be better encapsulated within the liposomes.43 As shown in Figure 3B, liposomes can be classified into three types: 1) monolayer liposomes: mainly used for targeted drug delivery; 2) Multilayer liposomes: Containing multiple concentric phospholipid layers (with a layer spacing of approximately 4–6 nm), they are suitable for sustained-release macromolecule drugs; 3) Polycystic liposomes: Non-concentric multi-lumen structure, drug loading capacity can reach over 30%, suitable for the delivery of large quantities of drugs.44 Due to the easy modification of the surface of liposomes, we can modify different antibodies, proteins and targeted peptides on their surfaces according to different usage scenarios to precisely deliver drugs (Figure 3C). The surface of liposomes is modified with monoclonal antibodies or their fragments targeting EGFR or TfR, and at the same time, anti-tumor drugs are loaded. Through receptor-mediated endocytosis, the drugs are efficiently delivered into the interior of cancer cells, enhancing the anti-cancer effect and reducing damage to normal lung tissue.45 At the same time, it is also possible to modify the surface with antibodies that can specifically recognize pathogen surface antigens, aptamers that can bind with high affinity to bacterial surface components, or peptide ligands that can simulate the host receptor binding domain. This type of liposome can actively target and precisely deliver antibiotics to the infection site and the area around the pathogen, significantly increasing the local drug concentration, effectively penetrating the biological membrane, and overcoming the problems of insufficient local concentration and high systemic toxicity in traditional drug administration methods. In conclusion, in the future, different liposomes can be designed based on their specific structures for the delivery of various drugs, ultimately achieving more precise drug delivery goals.
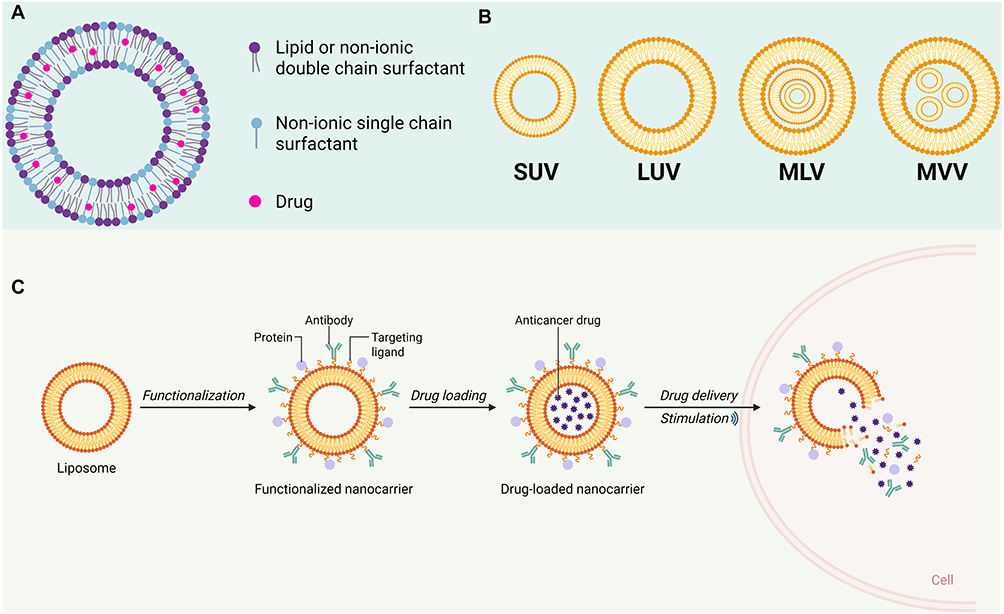 |
Figure 3 (A) The structure of liposomes; (B) Classification of liposomes (C) Liposome drug delivery. Created in BioRender. Xi, Z. (2025) https://BioRender.com/131uux8. |
General Pharmacokinetic Characteristics of Liposomes
Liposomes mainly enter the cell through endocytosis to release drugs. Liposomes have a series of pharmacokinetic advantages, such as specific drug delivery, high metabolic stability, high membrane permeability and improved drug bioavailability, etc. Different administration methods of liposomes and different particle sizes, charges and targeting properties will all affect the pharmacokinetic behavior of liposomes. The size of liposome particle size is one of the key factors determining whether it can effectively perform biological functions in vivo. The latest research indicates that liposomes with a particle size of less than 200 nm are more likely to pass through the vascular endothelial space or follicular epithelial cells (such as M cell), prolonging the circulation time and enhancing tissue penetration, thereby increasing the accumulation of drugs at the target site.46 Liposomes with a particle size more than 500 nm are more easily recognized and rapidly cleared by the reticuloendothelial system, leading to a rapid decrease in blood drug concentration. Therefore, when designing liposomes, the size of the liposomes should be carefully considered to ensure that they can have better therapeutic effects. In practical work, it is usually necessary to design a delivery system suitable for the characteristics of the disease based on the properties of liposomes. For example: In patients with IPF, since the treatment requires a certain blood drug concentration, liposome nanoparticles with larger particle size and faster excretion cannot be used for the treatment of IPF. Liposomes are mainly administered orally or by injection. The main administration methods of liposomes are as follows: 1) Intravenous injection; 2) Oral administration; 3) Inhalation administration.47,48 Different administration methods have different pharmacokinetic characteristics. Liposomes can directly enter the bloodstream through intravenous injection (Table 3). By regulating their particle size between 100 and 200 nm, they can reduce the rapid clearance of the endothelial system to maintain the required blood drug concentration throughout the body.49 The core purpose of inhalation administration is to prolong the retention time of drugs in the alveoli and interstitial lung tissue. Usually, liposomes of 5–10μm are selected to achieve alveolar deposition. However, inhalation administration needs to overcome the dual barriers of mucociliary clearance and macrophage phagocytosis.50 Therefore, researchers considered modifying its surface to enable liposomes to avoid being cleared by liquid cilia and phagocytosed by macrophages. Although oral administration is the most convenient way of drug administration, it is highly challenging. The main reason might be that oral administration will encounter gastrointestinal enzymatic hydrolysis and mucosal absorption disorders. To sum up, in practical applications, the corresponding drug administration methods should be designed based on the characteristics of different lung diseases. However, due to the special barrier system of the lungs and the phagocytosis of macrophages, it is difficult for liposome to maintain the required blood drug concentration in the lungs.51,52 Therefore, how to solve the problem of the residence time of the nano-delivery system in the lungs will become a major challenge.
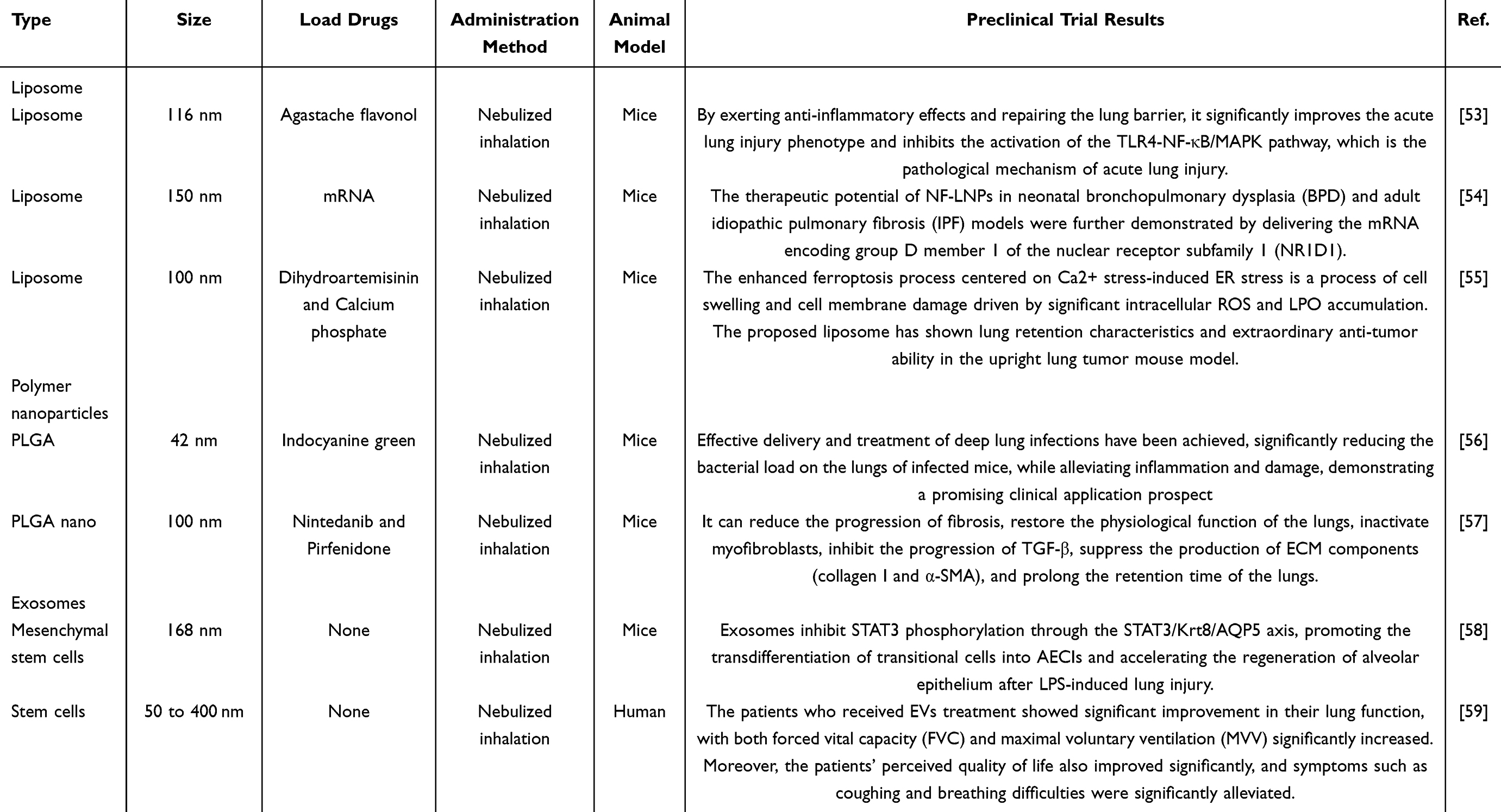 |
Table 3 Different Types of Nano Inhalation Method |
Clinical Potential of Liposomes
The composition of liposomes is very similar to that of the biological membranes of mammals. Most liposomes have excellent biocompatibility and biodegradability. Liposomes, as the first delivery system approved by the US FDA for the treatment of diseases, have been widely used in the treatment of various diseases and achieved excellent results. More importantly, liposome delivery drugs have already been marketed as finished drugs at present. In 1995, the FDA of the United States approved Doxil (liposome doxorubicin) for the treatment of cancer.60 Doxil is an adriamycin-specific agent encapsulated in a monolayer of liposomes covered with PEG called “polyethylene glycol liposomes”, which allow for precise delivery of the drug around the tumor cells through passive targeting. One of the biggest advantages of Doxil is that it significantly reduces the side effects of the medication, especially for the heart and the skin.61 Nowadays, more and more liposome-loaded therapeutic drug products are being marketed due to the excellent biosafety and powerful delivery capabilities of liposomes. Doxorubicin hydrochloride liposome, the world’s first anti-cancer liposome formulation, has sales of more than 5 billion yuan in China by 2021.62 Meanwhile, liposomes loaded with amphotericin have been touted as the “last straw” for patients with invasive fungal infections, with a 20-fold increase in hepatic targeting and a 75% reduction in nephrotoxicity compared to conventional reagents.63,64 Liposomes can deliver not only small molecule drugs, but also mRNA and nucleic acid-based drugs. In 2020, Hong et al65 first used liposomal delivery of miR-34a to treat patients with advanced solid tumors. Although the experiment was prematurely ended due to the death of the patient, it can still be proved that liposomes are feasible for the delivery of nucleic acid drugs to treat diseases. In summary, liposomes have become a mature drug delivery system for disease treatment with a wide range of future market applications.
Inhalation Administration
Inhalation preparations refer to the process where drugs are made into aerosols through special drug delivery devices and are directly deposited in the respiratory tract and lungs by patients through active or passive inhalation.66 Due to the unique physiological structure of the lungs, inhalation preparations can deliver drugs to the lesion site, greatly reducing the side effects of the drugs.48 At the same time, compared with administration methods such as injection, inhalation preparations are more easily accepted by patients. This might be because inhalation administration is a painless operation. We have summarized a table to summarize liposomes, polymer nanoparticles and exosomes. The summaries were made respectively in terms of size, particle size, administration method, animal model and preclinical effect. With the development of science and technology, inhalation drug delivery has become one of the directions that researchers are interested in (Table 4). With the development of science and technology, inhalation drug delivery has become one of the directions that researchers are interested in.67 1) Systemic side effects have been significantly reduced. The dosage of the drug is low, and it mainly takes effect locally, with a small amount of the drug entering the bloodstream.68 2) High local drug concentration enhances therapeutic effect. The drug reaches a high concentration in the target organ, while the concentration in other parts of the body is relatively low.69 3) It takes effect rapidly. The drug directly acts on the smooth muscles, mucous membranes or inflammatory cells of the airways without going through the systemic blood circulation.70 In conclusion, inhalation administration is a highly promising drug delivery method. When combined with liposome therapy for lung diseases, it may achieve better therapeutic effects.
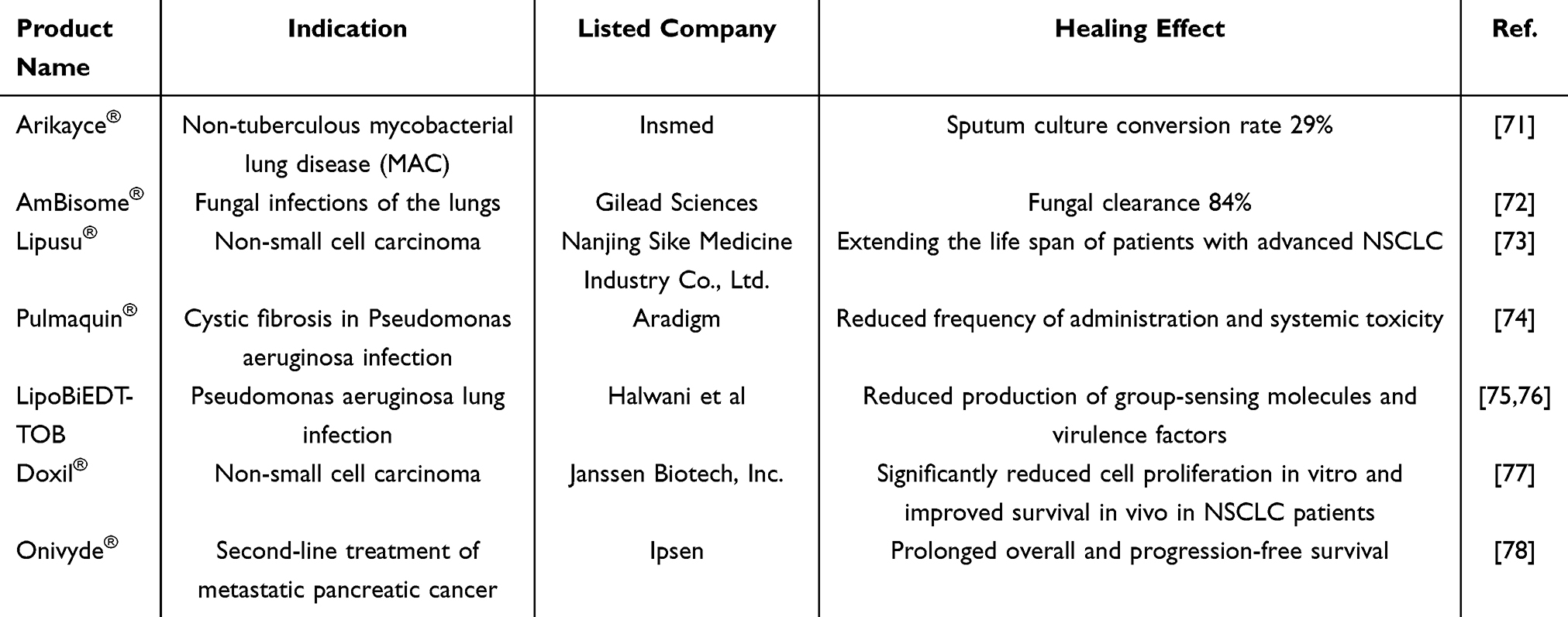 |
Table 4 Clinically Marketed Products for Liposomal Therapy of Diseases |
Liposome Delivery Systems in Lung Disease
Liposomal delivery systems have achieved good therapeutic results in some diseases. However, due to the special barrier effect of the lungs, how to deliver drugs to the lesion site accurately becomes a major challenge. The physiologic barrier of the lungs not only clears inhaled medications as foreign bodies by the regular oscillation of cilia, but also macrophages phagocytose the therapeutic drug and then expel it from the body, both of which prevent the drug from reaching the lungs for therapeutic purposes. At the same time, the diameter and stability of the delivery system indirectly affects whether the drug can be accurately delivered to the lesion. When the diameter of the delivery system is greater than 5 μm, the delivery system tends to get stuck in the throat and cannot finalize the delivery. When the delivery system is less than 1μm, it is easy to be exhaled out of the body and difficult to be accumulated in the body.79 These challenges then contribute to the difficulty of administering liposomal drug delivery systems in the lungs, as well as the difficulty of maintaining the body’s desired blood levels. In this section, we not only summarize the therapeutic role and delivery mechanism of liposomal delivered drugs in different lung diseases, but also the advantages and current problems of liposomes.
Pneumonia
Pneumonia is one of the leading causes of patient death in the world.80 Pneumonia is an inflammation of the lungs triggered by pathogens such as bacterial, viral, and fungal infections, or by non-infectious factors such as inhalation of foreign bodies and noxious gases, mainly involving the alveoli and interstitium of the lungs. Patients often present with fever, cough, chest pain and dyspnea, and in severe cases may be accompanied by confusion or cyanosis of the skin.81 The traditional means of treating pneumonia are usually oral, nebulized inhalation or intravenous administration of appropriate therapeutic drugs. Due to the unique circulatory system of the lungs, large drug concentrations are often required to maintain the blood levels needed for treatment, and large doses can bring about a range of complications and unavoidable damage to the patient’s organism. Liposome delivered drugs can maintain the patient’s desired blood levels by passively or actively targeting the lesion site.
Bacterial Pneumonia
Bacterial pneumonia is mainly categorized into community-acquired pneumonia and hospital-acquired pneumonia, both caused by bacterial infections. The latest surveys show that no less than 2.4 million people of all ages die from lower respiratory infections caused by bacteria.82 Among them, the mortality rates are higher in Africa, Southeast Asia and South Asia.82 However, antibiotics remain a cornerstone in the treatment of bacterial pneumonia, the emergence of bacterial resistance and the potential for drug-induced toxicity pose significant clinical challenges. Liposome-mediated antibiotic delivery has emerged as a promising strategy to enhance therapeutic efficacy while mitigating these limitations. Staphylococcus aureus (S. aureus) is a common pathogen causing pneumonia with a high mortality rate.83 Integrin α5β1 plays a key role in S. aureus invasion of nonphagocytic cells and promotes the development of Staphylococcus aureus pneumonia. The delivered siRNA is designed to specifically target the α5 and β1 subunits of integrin α5β1, which is a key receptor for Staphylococcus aureus to invade respiratory epithelial cells and is only highly expressed on the surface of respiratory system-related cells such as the lungs, enabling siRNA to precisely silence the target protein.84 Based on this, Meng et al85 designed a liposome encapsulated siRNA to treat Staphylococcus aureus pneumonia caused by S. aureus through nebulization inhalation (Figure 4A). The experimental results demonstrated that endotracheal nebulization of siRNA-encapsulated liposomal drugs not only markedly alleviated the severity of S. aureus induced pneumonia (eg, reduction in bacterial load and enhancement of the immune response), but also effectively confined the infection to the pulmonary compartment, thereby preventing systemic dissemination (Figure 4C–E). It mainly adopts endotracheal nebulization for drug administration, which can directly deliver lipid nanoparticles (LNPs) encapsulated with siRNA to the lungs, avoiding drug loss caused by systemic distribution, significantly increasing local drug concentration in the lungs, and achieving targeted delivery to lung infection foci. Zhang et al86 developed a liposome nanoparticle capable of targeting the lungs. It was shown by in vivo studies that liposomal nanoparticles effectively delivered siRNA to the lungs, resulting in a significant downregulation of target mRNA and TNF-α expression levels. Furthermore, this targeted delivery system markedly ameliorated pathological hallmarks of pulmonary inflammation. The liposome nanoparticles provide a novel therapeutic tool and method for the treatment of pneumonia. Liposomal drug delivery represents a highly promising yet imperfect therapeutic strategy for pneumonia treatment. While current studies have primarily evaluated in vitro safety profiles, comprehensive in vivo assessments remain limited. To fully establish the clinical potential of this approach, future research should systematically investigate critical pharmacokinetic parameters, including drug release kinetics and plasma concentration profiles to ensure the effectiveness and safety of the therapeutic measures. Traditional liposomes are usually composed of basic components such as phospholipids, cholesterol and polyethylene glycol (PEG).87 However, traditional liposomes are often preferentially taken up and cleared by the mononuclear phagocyte system (MPS) in the body, especially Kupffer cells in the liver.88 This tendency accumulation severely limits their application in the treatment of diseases related to extrahepatic tissues or organs. Therefore, Lee et al86 developed a lung-targeted amphiphilic liposome that enhanced pulmonary enrichment of small interfering RNA (siRNA) drugs. In vitro and vivo studies showed that the liposome exhibited efficient cellular uptake, robust endosomal/lysosomal escape capabilities, and was able to significantly down-regulate the mRNA and protein levels of TNF-α and improve the pathological features of lung inflammation, which provided a novel strategy for achieving extrahepatic targeted delivery using liposomal systems.
 |
Figure 4 (A) Project diagram; (B) Characterization of LNPs before and after nebulization. LNP preparation. (C and D) Experimental animals were infected with S. aureus with the nebulization equipment (2 × 108 CFU) for 24 h. Total number of intrapulmonary bacteria. (E) Histological examinations of the main organs (lung, liver, and kidney). ns, P > 0.05; *P < 0.05; **P < 0.01; ***P < 0.005. Modified with permission.85 Copyright 2024, BMC. |
Viral Pneumonia
COVID-19, respiratory syncytial virus, rhinovirus, human metapneumovirus, Zika virus, and influenza virus are the most common pathogens of viral pneumonia in both developed and developing countries.89 The 2020 outbreak of New Crown infections killed tens of thousands of people, and in the early stages of treatment, high-dose shock therapy with drugs was necessary to slow the course of the disease,90 however, this high-dose therapeutic regimen induces irreversible damage to healthy organs, potentially compromising long-term patient survival and quality of life. Macrophages are the key immune cells of the lungs and are the most important guardians of the respiratory system; they sense and phagocytose pathogens, release cytokines and participate in tissue repair.91,92 Zhao et al93 reported that a liposomal nanoparticle (surface-modified with macrophage-specific antibodies) can accurately deliver siRNA to macrophages. MacLNP was constructed by coupling the macrophage-specific antibody F4/80 to the surface of lipid nanoparticles (LNPs). F4/80 is a classic marker on the surface of mouse macrophages, which can specifically bind to macrophages, thereby precisely directing LNPs to macrophages. The experimental results demonstrated that siRNA delivery targeting TAK1 significantly reduced pro-inflammatory macrophage expression and ameliorated viral lung injury in vitro and in vivo. The structure of SARS-CoV-2 consists of four structural proteins: spiny protein (S), nucleocapsid (N), membrane (M), and envelope (E) proteins. E proteins are involved in virus assembly and maintenance of viral particles by binding to M proteins.94 The latest research have shown that USP33-protein interaction removes K48-type polyubiquitin chains and enhances E-protein stability, thereby increasing its ability to induce cell death and inflammatory responses, and that knockdown of USP33 expression levels is beneficial in delaying disease progression. Zhou et al95 utilized lipid nanoparticles to encapsulate siUSP33 and successfully delivered siUSP33 to mouse lungs. The experimental results showed that delivery of siRNA targeting USP33 to the lungs of mice using liposomes effectively attenuated the viral replication capacity and virulence in the mouse infection model. Liposome-delivered therapeutics for the treatment of viral pneumonia have achieved remarkable results, but more data supporting their safety and stability are needed to facilitate clinical translation. Tripterin/TP is a natural product with various biological activities, derived from the root bark of the traditional Chinese medicine Lei Gong Teng, which is one of the active ingredients in Lei Gong Teng Tablets and Lei Gong Teng Polyglycolide Tablets used in the treatment of rheumatoid diseases.96 However, TP has disadvantages of low permeability, poor solubility, susceptibility to off targeting, and low oral utilization, factors that limit further clinical use of TP. Thus, Que et al97 reported a TP-loaded liposome used to treat COVID-19. The liposome was prepared mainly by lipid membrane hydration extrusion method. The results of in vitro and vivo experiments showed that this liposome has potent anti-inflammatory properties against severe COVID-19 hyperinflammation.
COPD
COPD is a heterogeneous lung disease characterized by chronic respiratory symptoms (dyspnea, cough, sputum and/or acute exacerbations) due to airway abnormalities (bronchiectasis, bronchiectasis minor) and/or alveolar abnormalities (emphysema) resulting in persistent, usually progressively worsening airflow limitation. The major environmental exposures to COPD are smoking, inhalation of toxic particles and gases from indoor and outdoor air pollution, and other environmental and host factors (including abnormal lung development and accelerated aging) may also contribute to the development of COPD.98 COPD is an incurable disease that places a tremendous psychological and financial burden on the patient and the patient’s family. The main treatment for COPD is still based on preventing infections, reducing inhalation of harmful particles, etc.99 Quercetin holds significant promise as a candidate for COPD treatment due to its anti-inflammatory effects.100 However, quercetin hinders further clinical applications due to poor water solubility and low bioavailability. Yin et al101 utilized liposomal encapsulation of quercetin to treat COPD. The results showed that the liposome significantly enhanced the ability to alleviate lung inflammation and anti-fibrosis by regulating the expression of inflammation-related factors and fibrosis signaling molecules. Berberine is an isoquinoline alkaloid that has shown therapeutic potential in COPD mice. A growing number of studies have focused on the effects of berberine on lung disease and have shown that berberine ameliorates cigarette smoke-induced airway inflammation in mice.102 However, the poor water solubility of berberine limits its clinical application. Liu et al103 reported the study of a chitosanized liposome loaded with berberine for COPD treatment. The results showed that liposome could improve the inflammation score of lung tissues and reduce the levels of neutrophils and inflammatory cytokines (IL-1β, IL-6, IL-17, and TNF-α) in alveolar lavage fluid, which provided a new idea and method for the treatment of COPD. Chinese medicine is a treasure of the Chinese nation, and more and more herbs can be developed for the treatment of COPD in the future. However, herbal medicines suffer from low biological activity and poor solubility. Liposomal delivery systems are well suited to address this difficulty. However, further careful evaluation of safety is still needed when utilizing liposomes to deliver herbal medicines.
Idiopathic Pulmonary Fibrosis
Idiopathic pulmonary fibrosis (IPF) is an interstitial lung disease of uncertain etiology characterized by progressive and irreversible fibrosis of the interstitium of the lungs, which leads to dysfunction of pulmonary ventilation and air exchange, causing respiratory distress in patients. IPF is also known as a carcinoid disease.104 Once a person is diagnosed with IPF, the only way to slow down the progression of the disease is to take medication. In end-stage cases, the only way to save a patient’s life is through a lung transplant. Nidanib and pirfenidone are currently approved and marketed for the treatment of IPF, and patients need to take large amounts of nidanib and pirfenidone to maintain the blood levels needed for treatment. Due to the high side effects of nidanib and pirfenidone, the tolerance of the patients to the drugs is reduced and the development of the disease is accelerated.14 Alveolar type IIepithelial (AT2) cells play a parthenogenetic stem cell role, which promotes alveolar regeneration by proliferating or inducing directed differentiation into alveolar type I epithelial (AT1) cells.105 Considering the critical role of AT2 cells in IPF progression, maintaining AT2 stem cell identity to promote alveolization is considered a promising therapeutic strategy. Wang et al106 reported an inhalable mucus-penetrating lipid nanoparticle (Figure 5A) for co-delivery of dual mRNAs to promote alveolization by restoring dryness of AT2, ultimately leading to the treatment of IPF. SP-A antibody-modified SLNPs were constructed by coupling surface-active substance protein A (SP-A) antibody to the surface of lipid nanoparticles (LNPs). SP-A is highly expressed on the surface of alveolar type II epithelial (AT2) cells. SLNPs can specifically bind to AT2 cells through SP-A antibodies, significantly improving the targeted delivery efficiency to AT2 cells. The uptake efficiency of SLNPS in the lung epithelial cell line MLE12 is significantly higher than that of unmodified LNPs. The liposome nanoparticles were able to reverse mitochondrial dysfunction by improving nicotinamide adenine dinucleotide biosynthesis, thereby inhibiting senescence in AT2 cells. Termination of pathological epithelial remodeling and fibroblast activation induced by damaged AT2 cells promotes alveolar regeneration (Figure 5B–F). SLNPs can efficiently deliver dual mrnas encoding cytochrome b5 reductase 3 (CYB5R3) and bone morphogenetic protein 4 (BMP4) to AT2 cells, achieving precise regulation of AT2 cell function. Breast cancer anti-estrogen resistance protein 3 (Bcar3), originally discovered for its role in estrogen resistance in breast cancer, belongs to the family of proteins of the novel Src homolog 2.107 It was shown that abnormal Bcar3 levels were observed in lung tissue from IPF patients and mice with pulmonary fibrosis, and that Bcar3 expression was positively correlated with fibrotic gene expression. Zeng et al108 reported a self-assembled liposome loaded with Bcar3 siRNA for the treatment of IPF. Experimental results showed that gene therapeutic agents could be delivered precisely to lung macrophages and fibroblasts by intratracheal injection of liposomes containing Bcar3 siRNA, effectively reducing the expression of Bcar3 to 59% of baseline levels. Liposome-delivered drugs for the treatment of IPF have achieved good efficacy in animals. However, no liposome-delivered drug for the treatment of IPF has entered clinical trials to date, which may be related to the rapid disease progression and short median survival of IPF patients. In future work, new liposome-delivered drugs may be explored for the treatment of IPF.
 |
Figure 5 (A) Schematic illustration of inhaled delivery of mRNA-LNPs to AT2 cells reversing epithelial stem cell depletion for the treatment of IPF. (B) Representative images of lung tissue section stained with H&E, Masson’s trichrome, and picrosirius red. Scale bars, 100 μm. (C) Ashcroft scale toward fibrosis on lung sections. Fibrosis scores of the lungs (n= 5). (D) collagen volume fraction (n = 3). (E) lung volume (n = 4). (F) lung wet/dry weight ratios (W/d) (n = 5). (ns, not significant; P ≥ 0.05; *P < 0.05; **P < 0.01; ***P < 0.001; ***P < 0.0001). Modified with permission.106 Copyright 2024, Science. |
Lung Cancer
Lung cancer is one of the malignant tumors with the highest morbidity and mortality rates in the world, with 1.4 million or even 1.6 million deaths per year, accounting for 18% of all malignant tumor deaths.109 Lung cancer is mainly divided into non-small cell lung cancer and small cell lung cancer. Early-stage lung cancer usually has no clinical symptoms. However, when the tumor grows to a certain extent, it is a sign that the disease has entered the intermediate and advanced stages, when obvious clinical symptoms will appear. Unfortunately, once lung cancer reaches the middle or late stage, surgery is no longer indicated in most cases, and the only way to maintain the patient’s life is to seek chemotherapy or radiotherapy. When patients undergo chemotherapy, the side effects of the drugs are often too much for them to bear. Therefore, finding a feasible delivery system to accurately deliver chemotherapeutic drugs to the cancerous area can alleviate patients’ pain to a certain extent. Liposome delivery of drugs for cancer treatment has been clinically effective. In this section, the efficacy of liposomal delivery of different drugs for the treatment of non-small cell lung cancer and small cell lung cancer is described and current problems are presented.
Non-Small Cell Carcinoma
According to global cancer statistics, it is estimated that more than 2 million people are newly diagnosed with lung cancer each year,110 of these, non-small cell lung cancer (NSCLC) accounts for 80–85%. The most common histologic subtype of NSCLC is adenocarcinoma, followed by squamous carcinoma.111 Nearly 70% of NSCLC patients present with locally advanced or systemic metastases at the time of diagnosis.112 As a result, most of the patients have lost the chance of surgery when they are diagnosed and must resort to chemotherapy to keep them alive. Chemotherapy is indicated for many lung cancer patients, and the use of conventional chemotherapeutic agents appears to have reached a therapeutic plateau.113 There is an urgent need for a new treatment for NSCLC. MMP-9 is a protease upregulated in various malignant tumors.114 As shown in Figure 6A, Zhang et al115 constructed an integrated hybridized nanovesicle called cancer cell membrane liposome by fusing cancer cell membrane and charge reversal liposome membrane of MMP-9 switchable peptide. The cancer cell membrane (Cm) coated on the surface of nanoparticles (CLip-PC@CO-LC NPs) retains the surface proteins of protocancer cells (such as Pan-cadherin) and can specifically bind to non-small cell lung cancer (NSCLC) cells through homologous recognition, improving the targeted binding efficiency to tumor cells. It can accurately deliver siRNA to tumor cells with high MMP-9 expression. The highly expressed matrix metalloproteinase 9 (MMP-9) in the tumor microenvironment can clew the MMP-9-sensitive peptides on the surface of nanoparticles, expose the positively charged cell-penetrating peptides (CPP),116 enhance the internalization ability of nanoparticles towards tumor cells, and achieve targeted penetration triggered by TME. The experimental results showed that due to the long blood retention time, homologous targeting ability and accumulation of tumor microenvironment activation properties of this liposome (Figure 6D-F), it could effectively inhibit the growth of tumor cells and provide a new therapeutic idea and method for the treatment of NSCLC. Despite the ability of chemotherapy and molecularly targeted therapies to slow the progression of NSCLC, the life expectancy of patients with advanced NSCLC is still less than 1 year. Abnormal expression of antibodies produced against receptors on the surface of cancer cells has emerged as a new target for cancer treatment, eg, human epidermal growth factor receptor-2 (HER-2), epidermal growth factor receptor (EGFR), heparin A2 receptor (EphA2).117 Ernest Moles et al118 reported a polyethylene glycolated liposomal adriamycin targeting EGFR. It has been shown to effectively target and inhibit the growth of NSCLC tumors in vivo while reducing drug delivery to the heart. More and more products utilizing liposomes to deliver antitumor drugs are now on the market with excellent results, but their long-term safety and stability still have not been accurately evaluated. In subsequent clinical trials, the sample size of the study should be expanded to obtain more accurate and consistent data to support the rationale for liposome delivery of antitumor drugs.
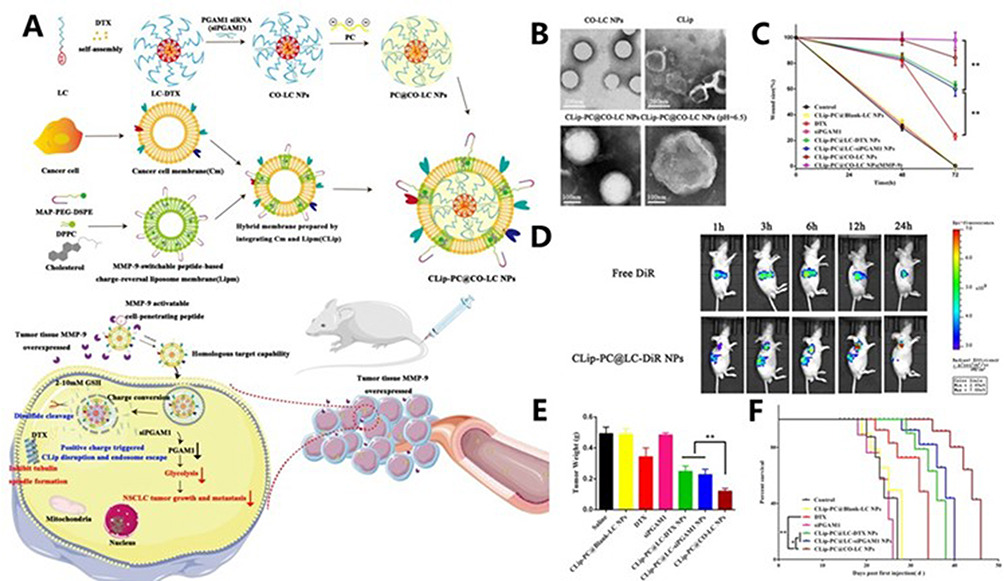 |
Figure 6 (A) A schematic diagram of the synthesis of CLip-PC@CO-LC NPs and the intracellular uptake. (B) Representative transmission electron microscopy (TEM) images of CO-LC NPs, CLip, CLip-PC@CO-LC NPs, and CLip-PC@CO-LC NPs (pH= 6.5) negatively stained with phosphotungstic acid (scale bars= 200 nm and 100 nm). (C) Average hydrodynamic size of CO-LC NPs, PC@CO-LC NPs, and CLip-PC@CO-LC NPs (n= 3). (D) Biodistribution of free DiR and CLip-PC@LC-DiR in A549 cell tumor-bearing nude BALB/c mice at 1, 3, 6, 12, and 24 h after administration. (E) The tumor weights of the A549 tumors excised from all groups after different treatments. Data is expressed as the mean± standard deviation (SD; n= 6). (F) Mice survival rates after different treatments (n= 6). *P < 0.05, **P < 0.01, ***P < 0.001. Modified with permission.115 Copyright 2021, BMC. |
Small Cell Carcinoma
Small cell lung cancer (SCLC) is a highly aggressive neuroendocrine tumor that accounts for approximately 13% of all lung cancer cases. SCLC is characterized by rapid growth and early metastasis. Despite significant improvements in the number and efficacy of current radiotherapy treatment regimens, treatment options and overall survival in SCLC have remained virtually unchanged for nearly three decades.119 The five-year survival rate for SCLC was 7.2%, whereas the five-year survival rates for adenocarcinoma, squamous cell carcinoma, and large cell carcinoma were 29.8%, 22.5%, and 18.6%, respectively.120,121 Although the treatment of SCLC has always been a major challenge, researchers have never stopped exploring. David R Spigel et al27 conducted a clinical trial where they utilized liposomal irinotecan versus topotecan for the treatment of recurrent SCLC in adults, and out of 461 randomly assigned patients, 229 were treated with liposomal irinotecan and 232 with topotecan. The results of clinical trials have shown that the use of liposome-delivered drugs for the treatment of SCLC is effective in reducing the probability of adverse events. More importantly, liposomal delivery of drugs significantly reduces the side effects of the drugs. Because SCLC is prone to recurrence, the current study does not address whether treatment with delivery systems is effective in reducing recurrence rates. Therefore, future studies need to focus on liposomal delivery of drugs in the prognosis of SCLC.
Current Developments
How to effectively treat lung diseases has always been a topic of interest for researchers. Although traditional drug administration methods have achieved remarkable results in treating lung diseases. However, as time went by and technology advanced, the problems with traditional treatment methods became increasingly prominent. Traditional drug administration may cause the following problems. 1) Drug resistance; 2) Drug side effects; 3) Low delivery efficiency.122 Therefore, how to solve these problems has become the goal of the researchers. Nowadays, people have proposed using drug delivery systems to address these issues. Drug delivery systems can be classified into nano-delivery systems, hydrogel delivery systems and biological carrier delivery systems.123 Liposomes, as one of the members of the nano-delivery system, have been widely applied in drug delivery due to their unique structure and excellent biocompatibility124 More importantly, researchers have already used liposomes to load drugs for the treatment of clinical diseases. In recent years, more researchers have utilized delivery systems to deliver drugs to the lungs with good efficacy. Liposomes are widely used in drug delivery, gene delivery, and cosmetic industry as an advantage of possessing good biosafety, strong delivery ability, and easy modification. Liposomes have two cores, a hydrophilic core and a hydrophobic core. For drugs with poor solubility and low bioavailability, the solubility and bioavailability of the drug can be greatly improved by being encapsulated in the hydrophobic core of the liposome, which in turn enhances the therapeutic efficacy of the drug. Due to the lipophilic phospholipid membrane bilayer of liposomes, it avoids being recognized by the body as a foreign substance and reduces the occurrence of a series of immune reactions. In addition, the unique structure of liposomes allows it to more easily cross the physiological barrier of the lungs to accomplish drug delivery. More importantly, in lung delivery, liposomes can be modified by antibodies, targeting peptides and cell shuttle peptides on their surface to enable more precise delivery of liposomes to the lesion site.
The intelligent responsive liposomes can adapt to the changes in the microenvironment of the disease, thereby achieving intelligent drug release, which has attracted extensive attention from researchers. Currently, there are several types of liposomes designed with different stimulus-responsive types according to the environmental changes at the lesion site. For example, pH-responsive, temperature-responsive and enzyme-responsive.
However, liposome delivery of drugs still faces several challenges and limitations.
- The self-stabilization of liposomes still needs to be improved. Liposomes may cause structural damage due to phospholipid oxidation, hydrolysis, or phase transition during storage or in vivo circulation, triggering drug leakage.40 At the same time, long-term preservation of liposomes usually requires freeze-drying, which is a complex process and may affect liposome integrity.
- Preparation methods and quality of liposomes need to be improved. Conventional methods for the preparation of liposomes are difficult to sustain in large quantities, and there is a need to find a simpler method adapted to the generation of liposomes in large quantities. Liposome nanoparticles should be produced with homogeneity and consistency between batches.
- Insufficient targeting efficiency of liposomes. Unmodified liposomes are susceptible to capture by the macrophage phagocytosis system and need to be polyethylene glycolyzed to prolong circulation time but may trigger accelerated blood clearance. Antibody, ligand modifications may improve targeting but may increase immunogenicity and the complex in vivo environment may mask targeting molecules. The poor penetration of liposomes in tumor cells limits, to some extent, the delivery of drugs from liposomes to cancer cells or tissues.125
- Drug release from liposomes is difficult to control precisely. Conventional liposomes rely on passive diffusion or membrane rupture for drug release, which may lead to premature or insufficient release. If smart response liposomes are used, it is difficult to ensure the accuracy and reliability of the stimulation conditions.
- The biosafety of liposomes still needs to be improved. Natural phospholipids are biocompatible, but synthetic phospholipids may cause inflammatory reactions, and the use of natural phospholipids increases the cost of liposome production. Liposomes are difficult to deliver intracellularly and are susceptible to immune clearance by cells, and modification of peptides or cationic lipids is often required to avoid immune clearance; however, introduction of peptides or cationic lipids may increase cytotoxicity.
- Inaccurate deposition location: Even if successfully inhaled, liposomes in aerosols mainly deposit in conductive gases, making it difficult to effectively reach deep lung tissue.126
- Individual differences and disease status impact: The respiratory physiological status of patients has significant individual differences, which significantly affect the deposition, distribution, and clearance of liposomes, making it difficult to predict and standardize treatment outcomes.127
- Regulatory challenges: Regulatory agencies such as FDA and EMA have strict approval requirements for new nanomedicine delivery systems, requiring detailed pharmaceutical, non-clinical, and clinical data, long development cycles, and high risks.15
With the development of science and technology, researchers have further expanded their focus on liposomes to meet future development needs. It may be expanded from the following aspects.
- Design of intelligent responsive liposomes. Pathological microenvironment triggered release: Develop liposomes that are sensitive to the microenvironment of lung diseases, such as decreased pH, increased enzyme activity, oxidative stress, and specific inflammatory factors, to achieve precise drug release at the lesion site.128
- Long term sustained release and release kinetics optimization. Develop new carriers such as phase change liposomes and solid lipid nanoparticles to prolong drug retention time in the lungs (>24 hours) and reduce dosing frequency. Realize constant rapid drug release and avoid sudden release effects.129
- Artificial intelligence guides personalized treatment with liposomes. Algorithm predicts the relationship between lipid composition and drug release behavior, accelerating formula screening. Intelligent inhaler monitors patient usage habits and optimizes medication efficiency.
Inhalation preparations are also a highly promising method of drug administration at present. More scientific researchers have developed a strong interest in this. However, inhalation preparations also have a series of challenges and limitations. Currently, the problems faced in the production of inhaled pulmonary formulations involve multiple aspects such as technology, process, supervision and market. 1) Stability of preparation. Long-term stability issue: Inhalable powder preparations may experience activity loss during storage. For instance, although lactose - leucine formulations can slow down degradation, aerosol performance (FPF) may still decline. 2) High-cost production: The industrial production cost of inhalation preparations is higher than that of traditional dosage forms, mainly due to complex processes and equipment requirements. 3) Drug resistance issue: For inhalation therapy targeting multi-drug-resistant bacteria the problems of cold chain dependence and stability need to be addressed.130
However, delivery of therapeutic drugs to the lungs remains a thorny issue due to the special physiological barrier structure of the lungs.131 Respiratory rate, breath-holding, humidity, wind speed and tidal volume are important factors affecting drug deposition. By understanding the characteristics of drug transport in the lungs, the mechanisms of deposition, the nature of the drug, the nature of the delivery system, the molecular basis of lung disease, and the barriers to drug delivery become the basis for the development of an efficient pulmonary drug delivery system.
Outlook
Overall, the development of liposome to treat lung diseases is an interesting research topic. Liposomes, as a commercially available delivery system, has been marketed in recent years with great economic benefits. Liposome delivery can be used not only for the treatment of lung diseases, but also for other diseases. Examples include bone repair, myocarditis and wound healing. Liposomes have a wide range of clinical applications and have been used in the treatment of various lung diseases. For example, lung cancer, pneumonia and COPD (Table 4). There is no doubt that the potential of liposomes for the treatment of lung diseases is enormous. Nucleic acids are one of the most important biological macromolecules within cells, responsible for carrying and transmitting genetic information and participating in the regulation of cell fate.132 In recent years, nucleic acid drugs have been used in genetic diseases, cancer, viral hepatitis, and new coronavirus infections, and are a highly promising therapeutic agent.133 However, nucleic acid drugs have several problems of their own. For example, poor stability, susceptibility to degradation, risk of immunogenicity, etc.134 The key to the efficacy of nucleic acid drugs is their accurate delivery to diseased tissues and sites. There can be a range of problems in the delivery process.135 These include:1) Obstruction of extracellular barriers: extracellular matrix adsorption, immune clearance, etc.; 2) Difficulty with cellular uptake; 3) Ensure the integrity of nucleic acids. The above difficulties create difficulties for nucleic acid-based drugs to perform their normal therapeutic functions. The emergence of liposomes has provided new ideas and approaches to this challenge. In 2020, Hong et al65 first used liposomal delivery of miR-34a to treat patients with advanced solid tumors, and despite the early termination of the experiment due to the premature death of the patient, it still proved that liposomes are feasible for delivery of nucleic acid-based drugs. Mutations or inactivation of the p53 pathway result in loss of p53 suppressor gene function, present in most human cancers.136 Neil Senzer et al137 reported a liposome nano delivery complex (SCL) for systemic tumor-targeted delivery. They completed the first phase I clinical trial using SCL nanocomplexes (SGT-53) to inhibit the tumor suppressor gene p53. Experimental results showed that minimal side effects of the complex were observed in patients with advanced solid tumors. More importantly, systemically delivered SGT-53 was not only well tolerated but also showed significant anticancer activity. In summary, liposome-delivered nucleic acid analogs have not only made some progress in research but have also achieved good results in clinical treatment. In the future work, if we can realize the efficient delivery of nucleic acid-based drugs and solve the stability problem at the same time, it will provide new ideas and methods for the treatment of different diseases, which will be a major technological innovation.
Liposomes are currently the most mainstream non-viral vectors for nucleic acid delivery, but they still face a series of challenges. For example: in terms of safety, immune response and nucleic acid stability.138
- The potential toxicity of liposomes themselves. Liposome components may be toxic to organs such as the liver, especially when used at high doses or repeatedly. Liposomes are mainly captured by the liver, and drugs may take effect in areas where they should not, causing side effects.
- The self-toxicity of nucleic acid drugs. Foreign mRNA or siRNA may be recognized by the immune system, triggering unnecessary inflammatory responses, which may instead reduce the therapeutic effect.
- The stability of nucleic acid drugs themselves. Exposed mRNA/siRNA is highly prone to rapid decomposition and failure in the blood. Liposome encapsulation provides protection, but incomplete encapsulation or leakage can still lead to degradation, which in turn affects the therapeutic effect.139
- The delivery efficiency still needs to be improved. Most of the encapsulated drugs may still be degraded by lysosomes within the cells, while only a small portion can successfully escape into the cytoplasm where they need to function and exert their effects.
- The storage conditions are extremely strict. Liposome delivery of nucleic acid drugs requires extremely strict transportation and storage conditions. This might have led to a further increase in the difficulty of industrialization.
Aerosol refers to a complex mixed system formed by the stable suspension of tiny solid or liquid particles in a gas.140 Lungs have a huge surface area and rich blood vessels, drugs are absorbed quickly. Delivering drugs to specific locations in the lungs by inhaling aerosols can, to a certain extent, avoid the first-pass effect of drugs.141 The deposition sites of drug particles in the respiratory tract can be controlled by adjusting the physical properties such as the size, density and shape of aerosol particles. The deposition sites of drug particles in the respiratory tract can be controlled by adjusting the physical properties such as the size, density and shape of aerosol particles. For instance, adjusting the particle size of aerosols to 1–5µm can enable drugs to reach the trachea, bronchi and bronchioles. Meanwhile, if the particle size is less than 1µm, the particles can reach the alveoli and may even be exhaled. Shraddha S Ghodke et al142 developed a spray-dried DPI formulation to improve solubility, stability and lung delivery of curcumin-loaded CS-HA double-coated micro colloidal particles for the treatment of lung cancer. The optimized DPI demonstrates excellent aerodynamic characteristics and is suitable for targeted pulmonary drug delivery in non-small cell lung cancer. Primary bronchial cancer accounts for almost 20% of all cancer deaths worldwide. Magnetic aerosol drug targeting is an emerging lung cancer treatment technology with enormous potential. Mohammad K D Manshadi et al143 found that after adding permanent magnets beside tumors, for particles with a diameter of 7µm, the particle deposition rate on the cancer was as high as 49%. Optimizing the magnet size can increase the particle deposition rate by 68%. In conclusion, the method of aerosol targeted drug delivery can effectively treat lung diseases. However, there are also a series of challenges and limitations in using aerosols to treat lung diseases.
- Low deposition efficiency: A large portion of the drug will be lost within the device, in the oropharynx or exhaled. The proportion of drugs reaching the target lung area is limited.
- Safety concerns: Inhaled particles or carriers may cause local irritation, inflammation or immune responses. The long-term pulmonary toxicity of nanomaterials still requires in-depth research.
- Industrialization and regulatory challenges: The development and production processes of inhalation products are complex, and the quality control requirements are strict, resulting in high costs. The bioequivalent evaluation of inhalation products by regulatory authorities is also highly challenging.
To sum up, both liposome delivery of nucleic acids and aerosol targeting of the lungs present opportunities and challenges. In the future, these problems should be addressed in a targeted manner to accelerate clinical transformation.
Data Sharing Statement
The dataset supporting this review article is included within all the cited article.
Consent for Publication
We have included 3 Figs (Figures 4–6) from previously published literature with required copyright permission from the copyright owners. We have mentioned this in the manuscript with appropriate citations.
Acknowledgments
This work was supported by the Science and Technology Fund of Guizhou Provincial Health Commission [gzwkj2023-017], Science and Technology Bureau Project of Zunyi City (Zunshi Kehe HZ [2023]14) and Project of Science and Technology Department of Guizhou Province, Basis of Guizhou Provincial Science and Technology Project [2024] youth 329.
Author Contributions
All authors made a significant contribution to the manuscripts reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the manuscripts; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
These authors declare no conflicts of interest in this work.
References
1. Petersson J, Glenny RW. Gas exchange in the lung. Semin Respir Crit Care Med. 2023;44(5):555–568. doi:10.1055/s-0043-1770060
2. Agusti A, Faner R. Lung function trajectories in health and disease. Lancet Respir Med. 2019;7(4):358–364. doi:10.1016/S2213-2600(18)30529-0
3. Murray JF. The structure and function of the lung. Int J Tuberc Lung Dis. 2010;14(4):391–396.
4. Zheng D, Liu J, Piao H, et al. ROS-triggered endothelial cell death mechanisms: focus on pyroptosis, parthanatos, and ferroptosis. Front Immunol. 2022;13:1039241. doi:10.3389/fimmu.2022.1039241
5. Frank JA, Briot R, Lee JW, et al. Physiological and biochemical markers of alveolar epithelial barrier dysfunction in perfused human lungs. Am J Physiol Lung Cell Mol Physiol. 2007;293(1):L52–9. doi:10.1152/ajplung.00256.2006
6. Hewitt RJ, Lloyd CM. Regulation of immune responses by the airway epithelial cell landscape. Nat Rev Immunol. 2021;21(6):347–362. doi:10.1038/s41577-020-00477-9
7. Zhao R, Ali G, Nie H-G, et al. Plasmin improves blood–gas barrier function in oedematous lungs by cleaving epithelial sodium channels. Br J Pharmacol. 2020;177(13):3091–3106. doi:10.1111/bph.15038
8. Akdis CA, Arkwright PD, Brüggen M-C, et al. Type 2 immunity in the skin and lungs. Allergy. 2020;75(7):1582–1605. doi:10.1111/all.14318
9. Arias-Pérez RD, Taborda NA, Gómez DM, et al. Inflammatory effects of particulate matter air pollution. Environ Sci Pollut Res Int. 2020;27(34):42390–42404. doi:10.1007/s11356-020-10574-w
10. Berg CD, Schiller JH, Boffetta P, et al. Air pollution and lung cancer: a review by international association for the study of lung cancer early detection and screening committee. J Thorac Oncol. 2023;18(10):1277–1289. doi:10.1016/j.jtho.2023.05.024
11. Hua JT, Cool CD, Green FHY. Pathology and mineralogy of the pneumoconioses. Semin Respir Crit Care Med. 2023;44(3):327–339. doi:10.1055/s-0043-1764406
12. Heyder J, Gebhart J, Rudolf G, et al. Deposition of particles in the human respiratory tract in the size range 0.005–15 μm. J Aerosol Sci. 1986;17(5):811–825. doi:10.1016/0021-8502(86)90035-2
13. Jeffery PK. Remodeling in asthma and chronic obstructivelung disease. Am J Respir Crit Care Med. 2001;164(supplement_2):S28–38. doi:10.1164/ajrccm.164.supplement_2.2106061
14. Zhang X, Zhang L, Tian J, et al. The application and prospects of drug delivery systems in idiopathic pulmonary fibrosis. Biomater Adv. 2025;168:214123. doi:10.1016/j.bioadv.2024.214123
15. Liu P, Chen G, Zhang J. A review of liposomes as a drug delivery system: current status of approved products, regulatory environments, and future perspectives. Molecules. 2022;27(4):1.
16. Barenholz Y. Doxil®--the first FDA-approved nano-drug: lessons learned. J Control Release. 2012;160(2):117–134. doi:10.1016/j.jconrel.2012.03.020
17. Sercombe L, Veerati T, Moheimani F, et al. Advances and challenges of liposome assisted drug delivery. Front Pharmacol. 2015;6:286. doi:10.3389/fphar.2015.00286
18. Fang J, Nakamura H, Maeda H. The EPR effect: unique features of tumor blood vessels for drug delivery, factors involved, and limitations and augmentation of the effect. Adv Drug Deliv Rev. 2011;63(3):136–151. doi:10.1016/j.addr.2010.04.009
19. Torchilin VP. Recent advances with liposomes as pharmaceutical carriers. Nat Rev Drug Discov. 2005;4(2):145–160. doi:10.1038/nrd1632
20. Shahid A, Khan MM, Ahmad U, et al. Exploring liposomes for lung cancer therapy. Crit Rev Ther Drug Carrier Syst. 2022;39(4):1–47. doi:10.1615/CritRevTherDrugCarrierSyst.2021037912
21. Omidian H, Gill EJ, Cubeddu LX. Lipid nanoparticles in lung cancer therapy. Pharmaceutics. 2024;16(5):644. doi:10.3390/pharmaceutics16050644
22. Amreddy N, Babu A, Muralidharan R, et al. Polymeric nanoparticle-mediated gene delivery for lung cancer treatment. Top Curr Chem. 2017;375(2):35. doi:10.1007/s41061-017-0128-5
23. Liu Z, Yan J, Tong L, et al. The role of exosomes from BALF in lung disease. J Cell Physiol. 2022;237(1):161–168. doi:10.1002/jcp.30553
24. Verschraegen CF, Gilbert BE, Loyer E, et al. Clinical evaluation of the delivery and safety of aerosolized liposomal 9-nitro-20(s)-camptothecin in patients with advanced pulmonary malignancies. Clin Cancer Res. 2004;10(7):2319–2326. doi:10.1158/1078-0432.CCR-0929-3
25. Lu C, Stewart DJ, Lee JJ, et al. Phase I clinical trial of systemically administered TUSC2(FUS1)-nanoparticles mediating functional gene transfer in humans. PLoS One. 2012;7(4):e34833. doi:10.1371/journal.pone.0034833
26. Xing P, Wang S, Bi M, et al. Phase 2 dose-ranging study to evaluate the efficacy and safety of liposomal irinotecan (LY01610) as a second-line treatment for patients with relapsed small cell lung cancer. EClinicalMedicine. 2024;75:102791. doi:10.1016/j.eclinm.2024.102791
27. Spigel DR, Dowlati A, Chen Y, et al. RESILIENT part 2: a randomized, open-label Phase III study of liposomal irinotecan versus topotecan in adults with relapsed small cell lung cancer. J Clin Oncol. 2024;42(19):2317–2326. doi:10.1200/JCO.23.02110
28. Olivier KN, Griffith DE, Eagle G, et al. Randomized trial of liposomal amikacin for inhalation in nontuberculous mycobacterial lung disease. Am J Respir Crit Care Med. 2017;195(6):814–823. doi:10.1164/rccm.201604-0700OC
29. Zhang J, Pan Y, Shi Q, et al. Paclitaxel liposome for injection (Lipusu) plus cisplatin versus gemcitabine plus cisplatin in the first-line treatment of locally advanced or metastatic lung squamous cell carcinoma: a multicenter, randomized, open-label, parallel controlled clinical study. Cancer Commun. 2022;42(1):3–16. doi:10.1002/cac2.12225
30. Siegel SAR, Griffith DE, Philley JV, et al. Open-label trial of amikacin liposome inhalation suspension in mycobacterium abscessus lung disease. Chest. 2023;164(4):846–859. doi:10.1016/j.chest.2023.05.036
31. Godet C, Couturaud F, Marchand-Adam S, et al. Nebulised liposomal amphotericin-B as maintenance therapy in allergic bronchopulmonary aspergillosis: a randomised, multicentre trial. Eur Respir J. 2022;59(6):2102218. doi:10.1183/13993003.02218-2021
32. Haworth CS, Bilton D, Chalmers JD, et al. Inhaled liposomal ciprofloxacin in patients with non-cystic fibrosis bronchiectasis and chronic lung infection with Pseudomonas aeruginosa (ORBIT-3 and ORBIT-4): two phase 3, randomised controlled trials. Lancet Respir Med. 2019;7(3):213–226. doi:10.1016/S2213-2600(18)30427-2
33. Bilton D, Fajac I, Pressler T, et al. Long-term amikacin liposome inhalation suspension in cystic fibrosis patients with chronic P. aeruginosa infection. J Cyst Fibros. 2021;20(6):1010–1017. doi:10.1016/j.jcf.2021.05.013
34. Clancy JP, Dupont L, Konstan MW, et al. Phase II studies of nebulised Arikace in CF patients with Pseudomonas aeruginosa infection. Thorax. 2013;68(9):818–825. doi:10.1136/thoraxjnl-2012-202230
35. Kneidinger N, Ghiani A, Milger K, et al. Impact of lung function decline on mortality in lung transplant recipients: long-term results from the L-CsA-i study for the prevention of bronchiolitis obliterans syndrome. Front Med. 2022;9:897581. doi:10.3389/fmed.2022.897581
36. Bilton D, Pressler T, Fajac I, et al. Amikacin liposome inhalation suspension for chronic Pseudomonas aeruginosa infection in cystic fibrosis. J Cyst Fibros. 2020;19(2):284–291. doi:10.1016/j.jcf.2019.08.001
37. Mertes P-M, Collange O, Coliat P, et al. Liposomal encapsulation of trans-crocetin enhances oxygenation in patients with COVID-19-related ARDS receiving mechanical ventilation. J Control Release. 2021;336:252–261. doi:10.1016/j.jconrel.2021.06.033
38. Laterre P-F, Colin G, Dequin P-F, et al. CAL02, a novel antitoxin liposomal agent, in severe pneumococcal pneumonia: a first-in-human, double-blind, placebo-controlled, randomised trial. Lancet Infect Dis. 2019;19(6):620–630. doi:10.1016/S1473-3099(18)30805-3
39. Guimarães D, Cavaco-Paulo A, Nogueira E. Design of liposomes as drug delivery system for therapeutic applications. Int J Pharm. 2021;601:120571. doi:10.1016/j.ijpharm.2021.120571
40. Nsairat H, Ibrahim AA, Jaber AM, et al. Liposome bilayer stability: emphasis on cholesterol and its alternatives. J Liposome Res. 2024;34(1):178–202. doi:10.1080/08982104.2023.2226216
41. Large DE, Abdelmessih RG, Fink EA, et al. Liposome composition in drug delivery design, synthesis, characterization, and clinical application. Adv Drug Deliv Rev. 2021;176:113851. doi:10.1016/j.addr.2021.113851
42. Fan Y, Marioli M, Zhang K. Analytical characterization of liposomes and other lipid nanoparticles for drug delivery. J Pharm Biomed Anal. 2021;192:113642. doi:10.1016/j.jpba.2020.113642
43. Akbarzadeh A, Rezaei-Sadabady R, Davaran S, et al. Liposome: classification, preparation, and applications. Nanoscale Res Lett. 2013;8(1):102. doi:10.1186/1556-276X-8-102
44. Euliss LE, DuPont JA, Gratton S, et al. Imparting size, shape, and composition control of materials for nanomedicine. Chem Soc Rev. 2006;35(11):1095–1104. doi:10.1039/b600913c
45. Shah N, Mohammad AS, Saralkar P, et al. Investigational chemotherapy and novel pharmacokinetic mechanisms for the treatment of breast cancer brain metastases. Pharmacol Res. 2018;132:47–68. doi:10.1016/j.phrs.2018.03.021
46. Haddadzadegan S, Dorkoosh F, Bernkop-Schnürch A. Oral delivery of therapeutic peptides and proteins: technology landscape of lipid-based nanocarriers. Adv Drug Deliv Rev. 2022;182:1.
47. Wang W, Hao Y, Liu Y, et al. Nanomedicine in lung cancer: current states of overcoming drug resistance and improving cancer immunotherapy.. Wiley interdisciplinary reviews. Nanomed Nanobiotechnol. 2021;13(1). doi:10.1002/wnan.1654
48. Zheng M, Zhu W, Gao F, et al. Novel inhalation therapy in pulmonary fibrosis: principles, applications and prospects. J Nanobiotechnol. 2024;22(1). doi:10.1186/s12951-024-02407-6
49. Bhattacharjee S. DLS and zeta potential – what they are and what they are not? J Control Release. 2016;235:337–351. doi:10.1016/j.jconrel.2016.06.017
50. Amato-Lourenço LF, Carvalho-Oliveira R, Júnior GR, et al. Presence of airborne microplastics in human lung tissue. J Hazard Mater. 2021;416:126124. doi:10.1016/j.jhazmat.2021.126124
51. Bur M, Henning A, Hein S, et al.Inhalative nanomedicine—Opportunities and challenges. Inhal Toxicol. 2009;(Suppl 21):137–143. doi:10.1080/08958370902962283
52. Mobley C, Hochhaus G. Methods used to assess pulmonary deposition and absorption of drugs. Drug Discov Today. 2001;6(7):367–375. doi:10.1016/S1359-6446(01)01691-9
53. Sun Z-C, Liao R, Xian C, et al. Natural pachypodol integrated, lung targeted and inhaled lipid nanomedicine ameliorates acute lung injury via anti-inflammation and repairing lung barrier. J Control Release. 2024;375:300–315. doi:10.1016/j.jconrel.2024.09.013
54. Zhao Z, Shan X, Ding J, et al. Boosting RNA nanotherapeutics with V-ATPase activating non-inflammatory lipid nanoparticles to treat chronic lung injury. Nat Commun. 2025;16(1):6477. doi:10.1038/s41467-025-61688-z
55. Fu F, Wang W, Wu L, et al. Inhalable biomineralized liposomes for cyclic Ca 2+ -burst-centered endoplasmic reticulum stress enhanced lung cancer ferroptosis therapy. ACS Nano. 2023;17(6):5486–5502. doi:10.1021/acsnano.2c10830
56. Liu M-Y, Liu X, Wang C-Y, et al. Inhalable polymeric microparticles for phage and photothermal synergistic therapy of methicillin-resistant Staphylococcus aureus Pneumonia. Nano Lett. 2024;24(28):8752–8762. doi:10.1021/acs.nanolett.4c02318
57. Lee WT, Lee H, Kim J, et al. Alveolar macrophage phagocytosis-evading inhaled microgels incorporating nintedanib-PLGA nanoparticles and pirfenidone-liposomes for improved treatment of pulmonary fibrosis. Bioact Mater. 2024;33:262–278. doi:10.1016/j.bioactmat.2023.11.005
58. Tang Y, Qian J, Ding M, et al. Nebulized MSC exosomes promote the transdifferentiation of transitional state cells against acute lung injury through STAT3/Krt8/AQP5 axis. Eur J Pharm Biopharm. 2025;214:114792. doi:10.1016/j.ejpb.2025.114792
59. Li M, Huang H, Wei X, et al. Clinical investigation on nebulized human umbilical cord MSC-derived extracellular vesicles for pulmonary fibrosis treatment. Signal Transduct Target Ther. 2025;10(1):179. doi:10.1038/s41392-025-02262-3
60. Gabizon AA, Shmeeda H, Zalipsky S. Pros and cons of the liposome platform in cancer drug targeting. J Liposome Res. 2006;16(3):175–183. doi:10.1080/08982100600848769
61. Farjadian F, Ghasemi A, Gohari O, et al. Nanopharmaceuticals and nanomedicines currently on the market: challenges and opportunities. Nanomedicine. 2019;14(1):93–126. doi:10.2217/nnm-2018-0120
62. Zhu L, Lin M. The synthesis of nano-doxorubicin and its anticancer effect. Anticancer Agents Med Chem. 2021;21(18):2466–2477. doi:10.2174/1871520621666201229115612
63. Laniado-Laborín R, Cabrales-Vargas MN. Amphotericin B: side effects and toxicity. Rev Iberoam Micol. 2009;26(4):223–227. doi:10.1016/j.riam.2009.06.003
64. Groll AH, Rijnders BJA, Walsh TJ, et al. Clinical pharmacokinetics, pharmacodynamics, safety and efficacy of liposomal amphotericin B. Clin Infect Dis. 2019;68(Suppl Supplement_4):S260–s274. doi:10.1093/cid/ciz076
65. Hong DS, Kang Y-K, Borad M, et al. Phase 1 study of MRX34, a liposomal miR-34a mimic, in patients with advanced solid tumours. Br J Cancer. 2020;122(11):1630–1637. doi:10.1038/s41416-020-0802-1
66. Wolff RK. Inhalation pharmacodynamics. J Aerosol Med Pulm Drug Deliv. 2023;36(5):275–280. doi:10.1089/jamp.2023.29092.rkw
67. Jin Z, Gao Q, Wu K, et al. Harnessing inhaled nanoparticles to overcome the pulmonary barrier for respiratory disease therapy. Adv Drug Deliv Rev. 2023;202:115111. doi:10.1016/j.addr.2023.115111
68. Jarai BM, Stillman Z, Attia L, et al. Evaluating UiO-66 metal–organic framework nanoparticles as acid-sensitive carriers for pulmonary drug delivery applications. ACS Appl Mater Interfaces. 2020;12(35):38989–39004. doi:10.1021/acsami.0c10900
69. Fei Q, Bentley I, Ghadiali SN, et al. Pulmonary drug delivery for acute respiratory distress syndrome. Pulm Pharmacol Ther. 2023;79:102196. doi:10.1016/j.pupt.2023.102196
70. Newman SP. Drug delivery to the lungs: challenges and opportunities. Ther Deliv. 2017;8(8):647–661. doi:10.4155/tde-2017-0037
71. Griffith DE, Eagle G, Thomson R, et al. Amikacin liposome inhalation suspension for treatment-refractory lung disease Caused by Mycobacterium avium Complex (CONVERT). A prospective, open-label, randomized study. Am J Respir Crit Care Med. 2018;198(12):1559–1569. doi:10.1164/rccm.201807-1318OC
72. Walsh TJ, Finberg RW, Arndt C, et al. Liposomal amphotericin B for empirical therapy in patients with persistent fever and neutropenia. National Institute of Allergy and Infectious Diseases Mycoses Study Group. N Engl J Med. 1999;340(10):764–771. doi:10.1056/NEJM199903113401004
73. Li R, Liang H, Li J, et al. Paclitaxel liposome (Lipusu) based chemotherapy combined with immunotherapy for advanced non-small cell lung cancer: a multicenter, retrospective real-world study. BMC Cancer. 2024;24(1):107. doi:10.1186/s12885-024-11860-3
74. Cipolla D, Blanchard J, Gonda I. Development of liposomal ciprofloxacin to treat lung infections. Pharmaceutics. 2016;8(1):6. doi:10.3390/pharmaceutics8010006
75. Güngör N, Knaapen AM, Munnia A, et al. Genotoxic effects of neutrophils and hypochlorous acid. Mutagenesis. 2010;25(2):149–154. doi:10.1093/mutage/gep053
76. Forier K, Messiaen A-S, Raemdonck K, et al. Probing the size limit for nanomedicine penetration into Burkholderia multivorans and Pseudomonas aeruginosa biofilms. J Control Release. 2014;195:21–28. doi:10.1016/j.jconrel.2014.07.061
77. Redruello-Guerrero P, Córdoba-Peláez P, Láinez-Ramos-Bossini AJ, et al. Liposomal doxorubicin in vitro and in vivo assays in non-small cell lung cancer: a systematic review. Curr Drug Deliv. 2024;21(10):1346–1361. doi:10.2174/0115672018272162231116093143
78. Yoo C, Kim K-P, Jeong JH, et al. Liposomal irinotecan plus fluorouracil and leucovorin versus fluorouracil and leucovorin for metastatic biliary tract cancer after progression on gemcitabine plus cisplatin (NIFTY): a multicentre, open-label, randomised, phase 2b study. Lancet Oncol. 2021;22(11):1560–1572. doi:10.1016/S1470-2045(21)00486-1
79. Gharse S, Fiegel J. Large porous hollow particles: lightweight champions of pulmonary drug delivery. Curr Pharm Des. 2016;22(17):2463–2469. doi:10.2174/1381612822666160128145356
80. Lanks CW, Musani AI, Hsia DW. Community-acquired pneumonia and hospital-acquired pneumonia. Med Clin North Am. 2019;103(3):487–501. doi:10.1016/j.mcna.2018.12.008
81. Johanson WG, Dever LL. Nosocomial pneumonia. Intensive Care Med. 2003;29(1):23–29. doi:10.1007/s00134-002-1589-7
82. Troeger C, Blacker B, Khalil IA. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis. 2018;18(11):1191–1210. doi:10.1016/S1473-3099(18)30310-4
83. He H, Wunderink RG. Staphylococcus aureus Pneumonia in the community. Semin Respir Crit Care Med. 2020;41(4):470–479. doi:10.1055/s-0040-1709992
84. De Backer L, Cerrada A, Pérez-Gil J, et al. Bio-inspired materials in drug delivery: exploring the role of pulmonary surfactant in siRNA inhalation therapy. J Control Release. 2015;220:642–650. doi:10.1016/j.jconrel.2015.09.004
85. Meng M, Li Y, Wang J, et al. Innovative nebulization delivery of lipid nanoparticle-encapsulated siRNA: a therapeutic advance for Staphylococcus aureus-induced pneumonia. J Transl Med. 2024;22(1):942. doi:10.1186/s12967-024-05711-9
86. Zhang W, Li J, Wang N, et al. Lung-targeted polyzwitterionic lipid nanoparticles for effective treatment of lung inflammation. Sci China Chem. 2025;68(3):1107–1116. doi:10.1007/s11426-024-2295-8
87. El Moukhtari SH, Garbayo E, Amundarain A, et al. Lipid nanoparticles for siRNA delivery in cancer treatment. J Control Release. 2023;361:130–146. doi:10.1016/j.jconrel.2023.07.054
88. Suk JS, Xu Q, Kim N, et al. PEGylation as a strategy for improving nanoparticle-based drug and gene delivery. Adv Drug Deliv Rev. 2016;99(Pt A):28–51. doi:10.1016/j.addr.2015.09.012
89. Ruuskanen O, Lahti E, Jennings LC, et al. Viral pneumonia. Lancet. 2011;377(9773):1264–1275. doi:10.1016/S0140-6736(10)61459-6
90. Pagliano P, Sellitto C, Conti V, et al. Characteristics of viral pneumonia in the COVID-19 era: an update. Infection. 2021;49(4):607–616. doi:10.1007/s15010-021-01603-y
91. Wynn TA, Vannella KM. Macrophages in tissue repair, regeneration, and fibrosis. Immunity. 2016;44(3):450–462. doi:10.1016/j.immuni.2016.02.015
92. Watanabe S, Alexander M, Misharin AV, et al. The role of macrophages in the resolution of inflammation. J Clin Invest. 2019;129(7):2619–2628. doi:10.1172/JCI124615
93. Zhao G, Xue L, Geisler HC, et al. Precision treatment of viral pneumonia through macrophage-targeted lipid nanoparticle delivery. Proc Natl Acad Sci U S A. 2024;121(7):e2314747121. doi:10.1073/pnas.2314747121
94. Wu A, Peng Y, Huang B, et al. Genome composition and divergence of the novel coronavirus (2019-nCoV) originating in China. Cell Host Microbe. 2020;27(3):325–328. doi:10.1016/j.chom.2020.02.001
95. Zhou Y, Liao Y, Fan L, et al. Lung-targeted lipid nanoparticle-delivered siUSP33 attenuates SARS-CoV-2 replication and virulence by promoting envelope degradation. Adv Sci. 2024;11(42):e2406211. doi:10.1002/advs.202406211
96. Kim DH, Shin EK, Kim YH, et al. Suppression of inflammatory responses by celastrol, a quinone methide triterpenoid isolated from celastrus regelii. Eur J Clin Invest. 2009;39(9):819–827. doi:10.1111/j.1365-2362.2009.02186.x
97. Que H, Hong W, Lan T, et al. Tripterin liposome relieves severe acute respiratory syndrome as a potent COVID-19 treatment. Sig Transd Target Ther. 2022;7(1):399. doi:10.1038/s41392-022-01283-6
98. Christenson SA, Smith BM, Bafadhel M, et al. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/S0140-6736(22)00470-6
99. Qian Y, Cai C, Sun M, et al. Analyses of factors associated with acute exacerbations of chronic obstructive pulmonary disease: a review. Int J Chron Obstruct Pulmon Dis. 2023;18:2707–2723. doi:10.2147/COPD.S433183
100. Ghafouri-Fard S, Shabestari FA, Vaezi S, et al. Emerging impact of quercetin in the treatment of prostate cancer. Biomed Pharmacother. 2021;138:111548. doi:10.1016/j.biopha.2021.111548
101. Yin C, Tian Y, Yan A, et al. Mitigating inflammation and fibrosis: the therapeutic potential of quercetin liposomes in COPD. Front Pharmacol. 2024;15:1503283. doi:10.3389/fphar.2024.1503283
102. Wang W, Zha G, Zou -J-J, et al. Berberine attenuates cigarette smoke extract-induced airway inflammation in mice: involvement of TGF-β1/Smads signaling pathway. Curr Med Sci. 2019;39(5):748–753. doi:10.1007/s11596-019-2101-8
103. Liu H, et al. Chitosan-coated solid lipid nano-encapsulation improves the therapeutic antiairway inflammation effect of berberine against COPD in cigarette smoke-exposed rats. Can Respir J. 2022;2022:8509396.
104. Pan Y, Yang H, Quan L, et al. Effects of full-body exercise-based pulmonary rehabilitation in patients with idiopathic pulmonary fibrosis: a systematic review and meta-analysis protocol. BMJ Open. 2022;12(12):e064212. doi:10.1136/bmjopen-2022-064212
105. Dalamaga M, Christodoulatos GS, Mantzoros CS. The role of extracellular and intracellular Nicotinamide phosphoribosyl-transferase in cancer: diagnostic and therapeutic perspectives and challenges. Metabolism. 2018;82:72–87. doi:10.1016/j.metabol.2018.01.001
106. Wang Y, Zhang J, Liu Y, et al. Realveolarization with inhalable mucus-penetrating lipid nanoparticles for the treatment of pulmonary fibrosis in mice. Sci Adv. 2024;10(24):eado4791. doi:10.1126/sciadv.ado4791
107. Arras J, Thomas KS, Myers PJ, et al. Breast Cancer Antiestrogen Resistance 3 (BCAR3) promotes tumor growth and progression in triple-negative breast cancer. Am J Cancer Res. 2021;11(10):4768–4787.
108. Zeng C, Wang Q, Liu X, et al. Localized administration of Bcar3 siRNA via Nano-self-assembly to treat idiopathic pulmonary fibrosis by disrupting macrophage-fibroblast crosstalk. Int J Nanomed. 2024;19:1827–1842. doi:10.2147/IJN.S444470
109. Wu G, Jochems A, Refaee T, et al. Structural and functional radiomics for lung cancer. Eur J Nucl Med Mol Imaging. 2021;48(12):3961–3974. doi:10.1007/s00259-021-05242-1
110. Chen P, Liu Y, Wen Y, et al. Non-small cell lung cancer in China. Cancer Commun. 2022;42(10):937–970. doi:10.1002/cac2.12359
111. Zhang S, Sun K, Zheng R, et al. Cancer incidence and mortality in China, 2015. J Nat Cancer Center. 2021;1(1):2–11. doi:10.1016/j.jncc.2020.12.001
112. Pfister DG, Johnson DH, Azzoli CG, et al. American society of clinical oncology treatment of unresectable non–small-cell lung cancer guideline: update 2003. J Clin Oncol. 2004;22(2):330–353. doi:10.1200/JCO.2004.09.053
113. Molina JR, Yang P, Cassivi SD, et al. Non-small cell lung cancer: epidemiology, risk factors, treatment, and survivorship. Mayo Clin Proc. 2008;83(5):584–594. doi:10.1016/S0025-6196(11)60735-0
114. Bernhard EJ, Gruber SB, Muschel RJ. Direct evidence linking expression of matrix metalloproteinase 9 (92-kDa gelatinase/collagenase) to the metastatic phenotype in transformed rat embryo cells. Proc Natl Acad Sci U S A. 1994;91(10):4293–4297. doi:10.1073/pnas.91.10.4293
115. Zhang W, Gong C, Chen Z, et al. Tumor microenvironment-activated cancer cell membrane-liposome hybrid nanoparticle-mediated synergistic metabolic therapy and chemotherapy for non-small cell lung cancer. J Nanobiotechnol. 2021;19(1):339. doi:10.1186/s12951-021-01085-y
116. Santiago-Sánchez GS, Pita-Grisanti V, Quiñones-Díaz B, et al. Biological functions and therapeutic potential of lipocalin 2 in cancer. Int J Mol Sci. 2020;21(12):4365. doi:10.3390/ijms21124365
117. Makwana V, Karanjia J, Haselhorst T, et al. Liposomal doxorubicin as targeted delivery platform: current trends in surface functionalization. Int J Pharm. 2021;593:120117. doi:10.1016/j.ijpharm.2020.120117
118. Moles E, Chang D, Mansfeld F, et al. EGFR targeting of liposomal doxorubicin improves recognition and suppression of non-small cell lung cancer. Int J Nanomed. 2024;19:3623–3639. doi:10.2147/IJN.S450534
119. Wang WZ, Shulman A, Amann JM, et al. Small cell lung cancer: subtypes and therapeutic implications. Semin Cancer Biol. 2022;86(Pt 2):543–554. doi:10.1016/j.semcancer.2022.04.001
120. Xu L, Zhang G, Song S, et al. Surgery for small cell lung cancer: a Surveillance, Epidemiology, and End Results (SEER) survey from 2010 to 2015. Medicine. 2019;98(40):e17214. doi:10.1097/MD.0000000000017214
121. Wang S, Zimmermann S, Parikh K, et al. Current diagnosis and management of small-cell lung cancer. Mayo Clin Proc. 2019;94(8):1599–1622. doi:10.1016/j.mayocp.2019.01.034
122. Zhang M. Inhaled RNA drugs to treat lung diseases: disease-related cells and nano–bio interactions. Adv Drug Deliv Rev. 2023;203:1.
123. Wan Q, Zhang X, Zhou D, et al. Inhaled nano-based therapeutics for pulmonary fibrosis: recent advances and future prospects. J Nanobiotechnol. 2023;21(1). doi:10.1186/s12951-023-01971-7
124. Zhang Y, Sun C, Wang C, et al. Lipids and lipid derivatives for rna delivery. Chem Rev. 2021;121(20):12181–12277. doi:10.1021/acs.chemrev.1c00244
125. Mangal S, Gao W, Li T, et al. Pulmonary delivery of nanoparticle chemotherapy for the treatment of lung cancers: challenges and opportunities. Acta Pharmacol Sin. 2017;38(6):782–797. doi:10.1038/aps.2017.34
126. Heyder J. Deposition of inhaled particles in the human respiratory tract and consequences for regional targeting in respiratory drug delivery. Proc Am Thorac Soc. 2004;1(4):315–320. doi:10.1513/pats.200409-046TA
127. Yu X-Y, Jin X, Shou Z-X. Surface-engineered smart nanocarrier-based inhalation formulations for targeted lung cancer chemotherapy: a review of current practices. Drug Delivery. 2021;28(1):1995–2010. doi:10.1080/10717544.2021.1981492
128. Pradhan A, Pattnaik G, Das S, et al. Advancements in lung cancer: molecular insights, innovative therapies, and future prospects. Med Oncol. 2025;42(9):383. doi:10.1007/s12032-025-02725-1
129. Ali Zaidi SS, Fatima F, Ali Zaidi SA, et al. Engineering siRNA therapeutics: challenges and strategies. J Nanobiotechnol. 2023;21(1). doi:10.1186/s12951-023-02147-z
130. Bassetti M, Vena A, Russo A, et al. Inhaled liposomal antimicrobial delivery in lung infections. Drugs. 2020;80(13):1309–1318. doi:10.1007/s40265-020-01359-z
131. García-Fernández A, Sancenón F, Martínez-Máñez R. Mesoporous silica nanoparticles for pulmonary drug delivery. Adv Drug Deliv Rev. 2021;177:1.
132. Sun X, Setrerrahmane S, Li C, et al. Nucleic acid drugs: recent progress and future perspectives. Signal Transduct Target Ther. 2024;9(1):316. doi:10.1038/s41392-024-02035-4
133. Wang J, Tan M, Wang Y, et al. Advances in modification and delivery of nucleic acid drugs. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2023;52(4):417–428. doi:10.3724/zdxbyxb-2023-0130
134. Tan X, Jia F, Wang P, et al. Nucleic acid-based drug delivery strategies. J Control Release. 2020;323:240–252. doi:10.1016/j.jconrel.2020.03.040
135. Zhang Y, Luo J, Gui X, et al. Bioengineered nanotechnology for nucleic acid delivery. J Control Release. 2023;364:124–141. doi:10.1016/j.jconrel.2023.10.034
136. Lane DP. On the regulation of the p53 tumour suppressor, and its role in the cellular response to DNA damage. Philos Trans R Soc Lond B Biol Sci. 1995;347(1319):83–87.
137. Senzer N, Nemunaitis J, Nemunaitis D, et al. Phase I study of a systemically delivered p53 nanoparticle in advanced solid tumors. Mol Ther. 2013;21(5):1096–1103. doi:10.1038/mt.2013.32
138. Wang H, Qin L, Zhang X, et al. Mechanisms and challenges of nanocarriers as non-viral vectors of therapeutic genes for enhanced pulmonary delivery. J Control Release. 2022;352:970–993. doi:10.1016/j.jconrel.2022.10.061
139. Wittrup A. Visualizing lipid-formulated siRNA release from endosomes and target gene knockdown. Nat Biotechnol. 2015;33(8):970–993. doi:10.1038/nbt.3298
140. MacLoughlin R, Telfer C, Clark A, et al. Aerosol: a novel vehicle for pharmacotherapy in neonates. Curr Pharm Des. 2018;23(38):5928–5934. doi:10.2174/1381612823666170918122136
141. Labiris NR, Dolovich MB. Pulmonary drug delivery. Part II: the role of inhalant delivery devices and drug formulations in therapeutic effectiveness of aerosolized medications. Br J Clin Pharmacol. 2003;56(6):600–612. doi:10.1046/j.1365-2125.2003.01893.x
142. Ghodke SS, Taylor KMG, Somavarapu S. Spray-dried micellar dry powder inhalation of curcumin for lung-targeted delivery in non-small cell lung cancer therapy. J Microencapsul. 2025;42(5):459–471. doi:10.1080/02652048.2025.2495246
143. Manshadi MKD, Saadat M, Mohammadi M, et al. Magnetic aerosol drug targeting in lung cancer therapy using permanent magnet. Drug Deliv. 2019;26(1):120–128. doi:10.1080/10717544.2018.1561765
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.