Back to Journals » Vascular Health and Risk Management » Volume 22
Lipidomic Profiling and Biological Aging in Patients with Coronary Microvascular Dysfunction
Authors Lu D, Deng L, Wang Z, Hu Y, Pan C, Lu H, Zhou Y ![]()
Received 5 March 2026
Accepted for publication 9 July 2026
Published 17 July 2026 Volume 2026:22 606866
DOI https://doi.org/10.2147/VHRM.S606866
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mirna N Chahine
Danbo Lu,1,* Lixiang Deng,1,* Zhe Wang,1,* Yiqing Hu,2– 5 Congcong Pan,2– 5 Hao Lu,2– 5 You Zhou1
1Department of Cardiology, Shanghai Geriatric Medical Center, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China; 2Department of Cardiology, Zhongshan Hospital, Fudan University, Shanghai Institute of Cardiovascular Diseases, Shanghai, People’s Republic of China; 3State Key Laboratory of Cardiovascular Diseases, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China; 4NHC Key Laboratory of Ischemic Heart Diseases; Key Laboratory of Viral Heart Diseases, Chinese Academy of Medical Sciences, Shanghai, People’s Republic of China; 5National Clinical Research Center for Interventional Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hao Lu, Department of Cardiology, Zhongshan Hospital, Fudan University, Shanghai Institute of Cardiovascular Diseases, Shanghai, People’s Republic of China, Tel +86-21-64041990 ext 2728, Email [email protected] You Zhou, Department of Cardiology, Shanghai Geriatric Medical Center, Zhongshan Hospital, Fudan University, People’s Republic of China, Tel +86-21-51371990, Email [email protected]
Background: Coronary microvascular dysfunction (CMD) was frequently encountered in patients with angina in the absence of epicardial coronary stenosis. CMD was associated with adverse outcomes while the etiology was unclear.
Objective: In this study, we aimed to investigate the association between lipidomic abnormalities, biological aging and CMD.
Methods: We consecutively enrolled 43 patients with angina exhibiting no epicardial coronary stenosis on angiography. CMD was defined by a coronary angiography-derived index of microvascular resistance (caIMR) > 25. Targeted lipidomic profiling quantified 781 lipids. PhenoAge was calculated from clinical parameters. Using machine learning, lipidomic data and clinical characteristics were screened to identify candidate biomarkers.
Results: There were 25 patients having CMD with the mean caIMR of 34.0 (Interquartile range [IQR], 31.0– 36.5), in contrast to 23.0 (IQR, 19.0– 24.5) in the control group. Patients with CMD had substantially older PhenoAge (61 vs 52, p = 0.002). Forty-eight lipid species were dysregulated in patients with CMD, which predominantly belonged to triacylglycerol (TAG). PhenoAge, triglyceride glucose index, hypertension, TAG47:2-FA14:0, TAG48:4-FA18:1 and phosphatidylcholine (18:1/20:3) were independent risk factors of CMD. Incorporating dysregulated lipids significantly improved CMD prediction compared to traditional clinical factors alone (area under the curve, 0.94 vs 0.86, p < 0.05).
Conclusion: PhenoAge acceleration and dysregulated lipidome were associated with CMD. Larger-scale studies and external validation are needed in the future.
Keywords: biological aging, lipidomics, index of microcirculatory resistance, coronary microvascular dysfunction
Introduction
Coronary angiography reveals non-obstructive coronary artery disease (CAD) in nearly half of patients presenting with chest pain.1–3 A significant number of symptomatic patients without flow-limiting coronary lesions have structural or functional abnormalities of the coronary microcirculation, resulting in coronary microvascular dysfunction (CMD).4 Patients with CMD are at substantially elevated risk of future adverse cardiovascular events.5 However, the management of CMD remains challenging due to limited understanding of its etiology and the lack of targeted therapies.
CMD has been invasively assessed using the index of microcirculatory resistance (IMR) through a pressure wire. In recent years, CMD evaluation has been advanced by the development of coronary angiography-derived index of microcirculatory resistance (caIMR), which could conveniently assess CMD based on computational pressure-fluid dynamics and routine coronary angiography.6,7 caIMR enables real-time evaluation of CMD in the catheter room without increasing operation time or radiation exposure.
Lipid metabolism is critical for endothelial cells and coronary microvascular homeostasis.8 Conventional lipid parameters, such as low-density lipoprotein cholesterol (LDL-C) and triglyceride (TG), are insufficient to characterize the complexity of lipid metabolic processes. Modified lipoproteins may be involved in the development of cardiovascular dysfunction.9 The advent of lipidomics allows detailed profiling of lipid species,10 which is a valuable tool for identifying and quantifying potential biomarkers relevant to disease process.11
Moreover, endothelial dysfunction is a recognized hallmark of panvascular diseases, affecting multiple organs within the circulatory system beyond the heart alone.12 Cross-organ interactions could accelerate biological aging through inflammatory processes, secretome alterations, metabolic dysregulation.13 On the other hand, senescence itself was related with deteriorating endothelial function.14 Endothelial senescence, characterized by a shift toward a vasoconstrictive, proinflammatory environment, would cause impaired regulation of vascular homeostasis and microvascular dysfunction.15 The specific association between biological aging and CMD, however, remains unexplored.
In this cross-sectional study, we recruited angina patients without obstructed arteries and assessed coronary microvascular function using caIMR. By integrating machine learning and lipidomic profiling, we investigated the association between lipid metabolic features, biological aging, and CMD. This research aims to enhance the understanding of CMD etiology and identify biomarkers for precise diagnosis and treatment.
Methods
Study Population
A total of 43 patients presenting stable angina pectoris with no coronary stenosis in coronary angiography were consecutively recruited at Shanghai Geriatric Medical Center from 2023 to 2024. Patients were excluded with elevated high-sensitivity cardiac troponin T levels on admission and prior history of percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG). Written informed consent was obtained from all participants or their legal representatives. The study protocol was approved by the Ethics Committee of Shanghai Geriatric Medical Center (B2023-007) and conducted according to the guidelines of the Declaration of Helsinki. This trial was registered with the Chinese Clinical Trial Registry (URL: https://www.chictr.org.cn; Identifier: ChiCTR2500095360).
caIMR Measurements
caIMR was computed using FlashAngio software (Rainmed Ltd, Suzhou, China). The calculation is based on the assumption that mean diastolic coronary flow velocity is proportional to that in hyperemia. First, a three-dimensional mesh model was reconstructed from the coronary ostium to the distal segment, using ≥2 angiographic views separated by ≥30°. Second, angiography-derived FFR (caFFR) was determined through computational pressure-flow dynamics. Finally, caIMR was calculated as:

Pdhyp is the mean distal arterial pressure during simulated maximal hyperemia. Pdhyp = Pahyp − ΔP·Pahyp is derived from mean resting aortic pressure via FlashAngio algorithms. ΔP represents the computed pressure gradient along meshed vessels using computational fluid dynamics. L indicates vessel length from the inlet to the distal segment of the target vessel. Vhyp is the simulated maximal hyperemic flow velocity. Vhyp = K·Vdiatole. K is the constant used to adjust the difference between the resting and hyperemic flow velocity. Vdiatole is the resting diastolic flow velocity calculated by the software. CMD was defined as caIMR >25.
Sample Collection and Lipidomic Analysis
Venous blood samples were collected after at least 8 hours of fasting. Plasma was separated by centrifugation (1500 g, 15 min, 4°C) within 4 hours and stored at −80°C. Blinded to researchers performed lipid extraction and analysis. 20 µL plasma was spiked with 9μL internal standard cocktails (Avanti Lipids Polar) and 350 μL pre-cooled isopropanol (−20°C). After vortex-mixing and 10-min incubation at room temperature, samples were stored at −20°C overnight. After vigorous shaking and centrifugation (12,000 rpm, 20 min), supernatants were transferred, re-centrifuged (12,000 rpm, 10 min), and analyzed in glass tubes via normal-phase liquid chromatography coupled to a QTRAP 5500 mass spectrometer (SCIEX, Framingham, MA, USA) in dual-polarity electrospray ionization mode. 20 µL aliquots of quality control (QC) samples were prepared by pooling identical volumes of the individual plasma samples. Eight pooled plasma QC samples (20 µL each) were evenly distributed across each run. Variables with relative standard deviation >20% were excluded, and internal standard peak heights were monitored to ensure stability.
The Q-Trap was operated to scan precursor/product ion pairs. Each test was repeated thrice. Peak area of each pair was processed with MultiQuant™ software (AB Sciex) for further quantification. Additional parameters had been described previously.16
A total of 781 lipid species were measured in this study including: cholesterol (Cho), cholesterol ester (CE), phosphatidylcholine (PC), lysophosphatidylcholine (LPC), phosphatidylethanolamine (PE), alkylphosphatidylethanolamine [PE(O)], alkenylphosphatidylethanolamine [PE(P)], lysophosphatidylethanolamine (LPE), phosphatidylglycerol (PG), phosphatidylinositol (PI), lysophosphatidylinositol (LPI), phosphatidylserine (PS), ceramide (Cer), GM3 ganglioside, sphingosine (Sph), sphingomyelin (SM), diacylglycerol (DAG) and triacylglycerol (TAG).
Data Preprocessing
Lipid species undetectable in >50% cases were excluded and 691 lipids were left for further analysis. Remaining missing (undetectable) values were replaced by one-fifth of the minimum value of the corresponding lipids in the detected cohort. Then, the lipidomic data was log10 transformed and standardized using Z-score.
PhenoAge Calculation
Biological aging was quantified using PhenoAge adapted from the reported algorithm.17,18 PhenoAge was calculated from clinical biomarkers including albumin (g/L), alkaline phosphatase (U/L), ln(C-reactive protein) (mg/dl), creatine (μmol/L), HbA1c (%), lymphocyte percentage (%), mean corpuscular volume (fl), red blood cell distribution width (%) and white blood cell count (*109/L). PhenoAge advance was defined as PhenoAge minus chronological age. Biological aging acceleration was defined as PhenoAge advance greater than 0.
Model Development and Validation
Three machine learning (ML) models, including Random Forest (RF), Support Vector Machine (SVM) and eXtreme Gradient Boosting (XGBoost) were implemented for CMD prediction. To optimize the prediction models, the final hyperparameters for each model were tuned based on 50 rounds of 5-fold cross-validation with 80% of the population. Then, the models were refitted on the entire dataset with the optimal hyperparameters. Feature contributions were ranked by descending mean absolute SHAP values.
In order to ensure the robustness of significant lipid species selected from the ML models, 200 rounds of Least Absolute Shrinkage and Selection Operator (Lasso) regression were conducted. In each of the 200 rounds, the dataset was randomly divided into a training set (80%) and a validation set (20%). On the training portion, Lasso regression was conducted with 5-fold cross validation to select the best penalty term (λ). Then we recorded which lipid features had non-zero coefficients—meaning they were selected by the model. Lipid species were then ranked by the frequency of inclusion. Orthogonal Partial Least Squares Discriminant Analysis (OPLS-DA) was performed to generate Variable Importance in Projection (VIP) scores.
Lipids meeting all three criteria—top 15 features in ML models (mean SHAP), top 15 selection frequency in Lasso regression, and VIP score >1 in OPLS-DA—were integrated with clinical factors into univariable and multivariable logistic regression models (Figure 1).
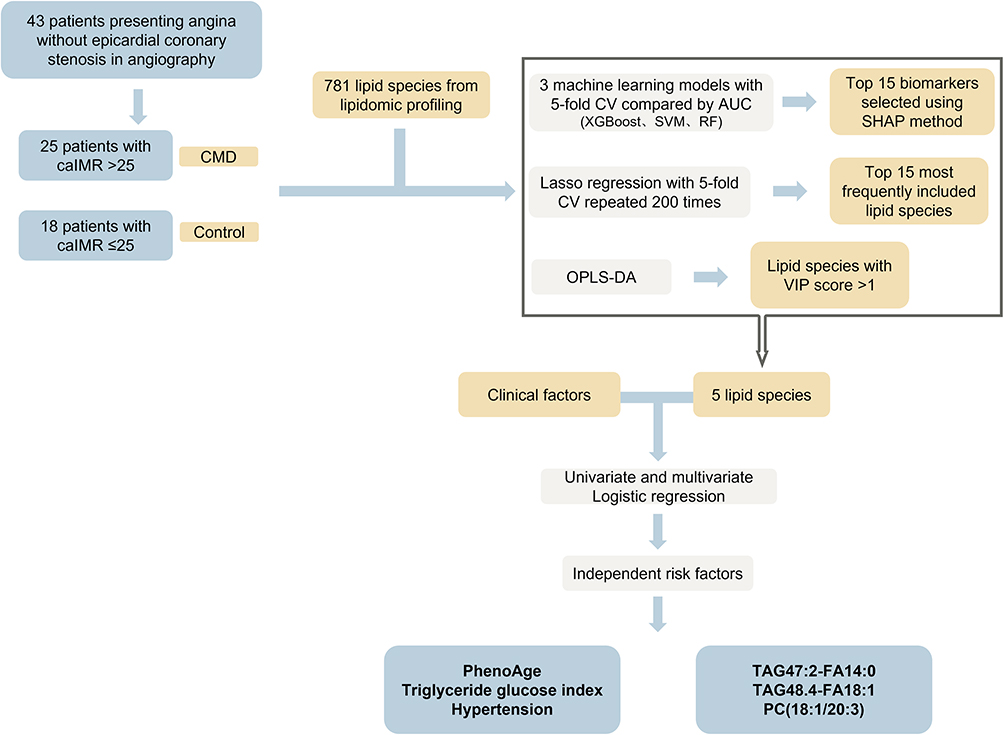 |
Figure 1 Flow chart of the study. Abbreviations: AUC, area under the receiver operating characteristic curve; caIMR, coronary angiography–derived index of microcirculatory resistance; CMD, coronary microvascular dysfunction; CV, cross validation; OPLS-DA, orthogonal partial least squares discriminant analysis; PC, phosphatidylcholine; RF, random forest; SHAP, SHapley Additive exPlanations; SVM, support vector machine; TAG, triacylglycerol; TyG, triglyceride glucose index; VIP, variable importance in projection. |
Statistics
For ML models, model performance was evaluated with area under the receiver operating characteristic (ROC) curve (AUC), sensitivity, specificity and accuracy. AUC comparisons used DeLong’s test. The SHapley Additive exPlanations (SHAP) method ranked the importance of inputted features and was used for ML model explanation.19 Non-linear relationship between the biomarkers and odds ratio of CMD was displayed using restricted cubic splines. Variables with p < 0.05 in the univariable analysis were subsequently included in the multivariable model for further analysis. The discriminating performance of logistic regression models was evaluated by AUC. Calibration plots, showing the predicted probability versus the observed probability of CMD, were internally validated by 1000 bootstrap resampling. Clinical impact curves visualized net clinical benefits at different risk thresholds.
The study was designed as an exploratory lipidomic investigation in patients with angiography-defined coronary microvascular dysfunction. At study initiation, reliable prior estimates were not available for the expected effect sizes of individual lipid species or PhenoAge in caIMR-defined CMD. For that reason, a conventional power calculation for the lipidomic endpoints was not feasible.
Categorical variables are presented as counts (percentages) and continuous variables as mean ± standard deviations (SD) or median with interquartile ranges (IQR), accordingly. Comparisons between categorical variables were made by the Chi-squared test, whereas continuous variables were compared by Student’s t test (normally distributed) or Mann–Whitney U-test (non-normally distributed). The p-values (two-sided) were corrected for multiple comparisons using the Benjamini–Hochberg method,20 after comparing lipid levels between CMD and control groups. A two-tailed P-value < 0.05 was considered statistically significant. Data were analyzed with R software 4.5.1 and SPSS v25.0 (IBM Corp., Armonk, NY, USA).
Result
Baseline Characteristics
The cohort comprised 43 patients, of whom 28 patients were diagnosed with CMD who had caIMR >25 in at least one vessel. Demographic and clinical characteristics are summarized in Table 1. Smoking history, hypertension, diabetes, conventional lipid parameters, and major lipid-lowering medication categories were assessed at baseline. Most baseline variables were similar between the groups. However, patients with CMD were more likely to be male (78.6% % vs 40.0%, p = 0.011) and had higher prevalence of hypertension (60.7% vs 26.7%, p = 0.033) compared to controls. Additionally, fasting glucose levels and triglyceride glucose index (TyG) were significantly elevated in the CMD group than those in the control group (both p < 0.05). No patient was taking omega-3 supplements, fibrates, or PCSK9 inhibitors during the study period. Statin use did not differ significantly between groups, and LDL-C was also comparable between groups (p = 0.610). Details of caIMR are presented in Table 2. In brief, the average caIMR of three vessels was substantially higher in CMD patients (34.0 [IQR, 31.0–36.5]) than in controls (23.0 [IQR, 19.0–24.5]) (p < 0.001).
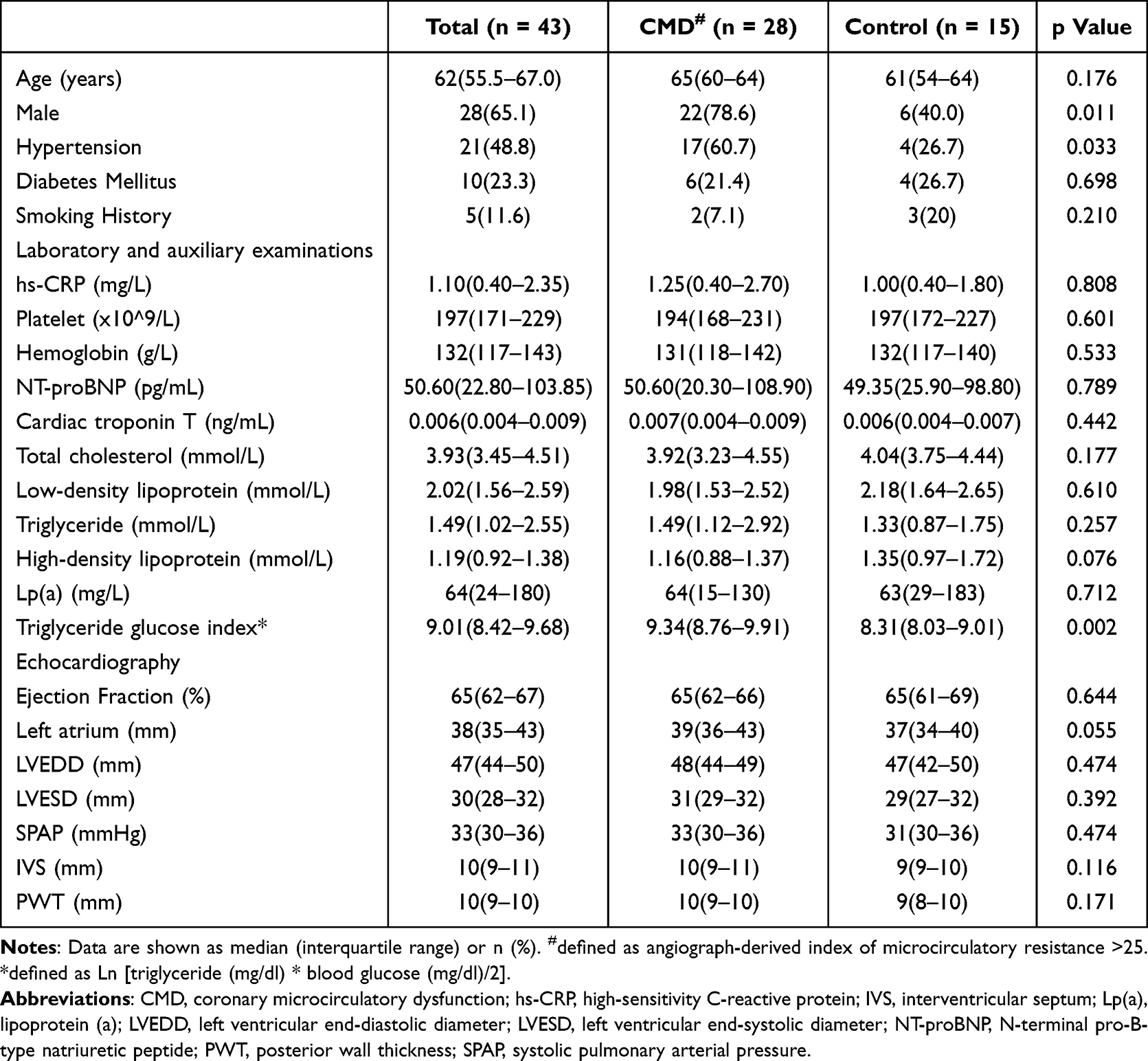 |
Table 1 Baseline Demographics and Clinical Characteristics |
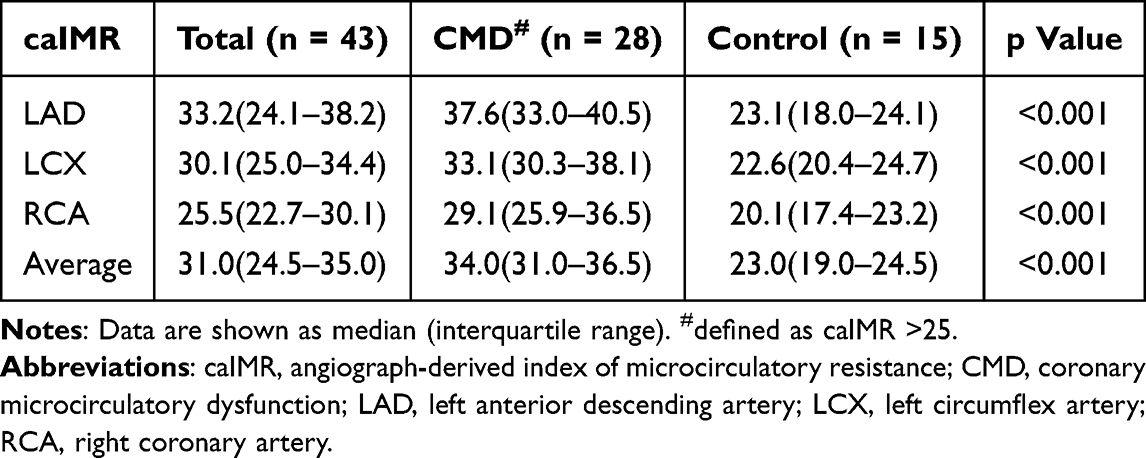 |
Table 2 Angiograph-Derived Index of Microcirculatory Resistance in Coronary Arteries |
Lipidomic Features
After adjustment for multiple comparisons, lipidomic profiling identified 48 lipid species showing differential abundance between the groups (false discovery rate < 0.05. Supplemental Figure 1). Notably, 36 of these dysregulated lipids (75%) were TAG, all of which were significantly elevated in patients with CMD. Conversely, the CMD cohort had substantially lower circulating levels of several other lipids, including 2 in CE, 3 in SM, 3 in PC and 4 in PE(P).
Further investigation into lipid structural characteristics, specifically the total number of carbon atoms and double bonds, revealed significant correlation with CMD risks (Figure 2). DAG and TAG were generally associated with an increased CMD risk, particularly those with longer carbon chains and greater degrees of unsaturation. In contrast, PE(O), PE(P) and SM were broadly related with a reduced risk profile of CMD.
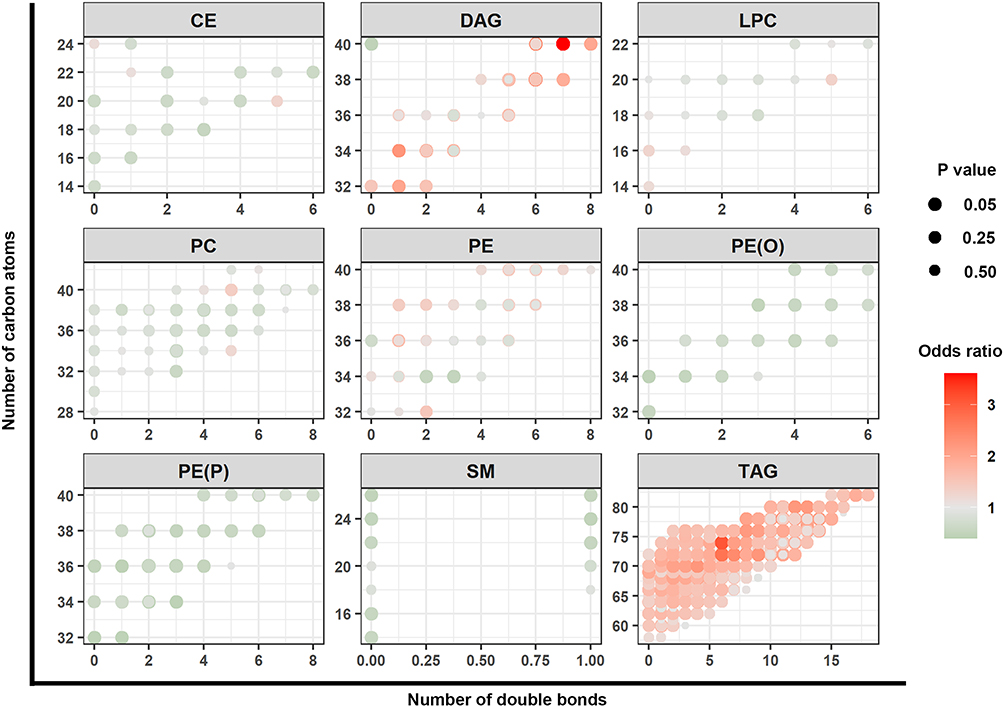 |
Figure 2 Association between number of carbon atoms, double bonds and CMD risk. Individual lipid species are depicted by filled circles and arranged by lipid class in 9 panels according to the number of total carbon atoms (Y axes) and number of double bonds (X axes). Circle color indicates the magnitude of odds ratio (OR) of coronary microvascular dysfunction (CMD), and circle size corresponds to the significance level. Abbreviations: CE, cholesterol ester; DAG, diacylglycerol; LPC, lysophosphatidylcholine; PC, phosphatidylcholine; PE, phosphatidylethanolamine; PE(O), alkylphosphatidylethanolamine; PE(P), alkenylphosphatidylethanolamine; SM, sphingomyelin; TAG, triacylglycerol. |
PhenoAge
Details of PhenoAge and related clinical parameters are shown in Table 3. The median PhenoAge was 61 in the CMD group versus 52 in the control group (p = 0.002) (Figure 3). Of note, PhenoAge advance was significantly greater in patients with CMD. 78.4% of the CMD patients had biological aging acceleration in contrast to none in the control group.
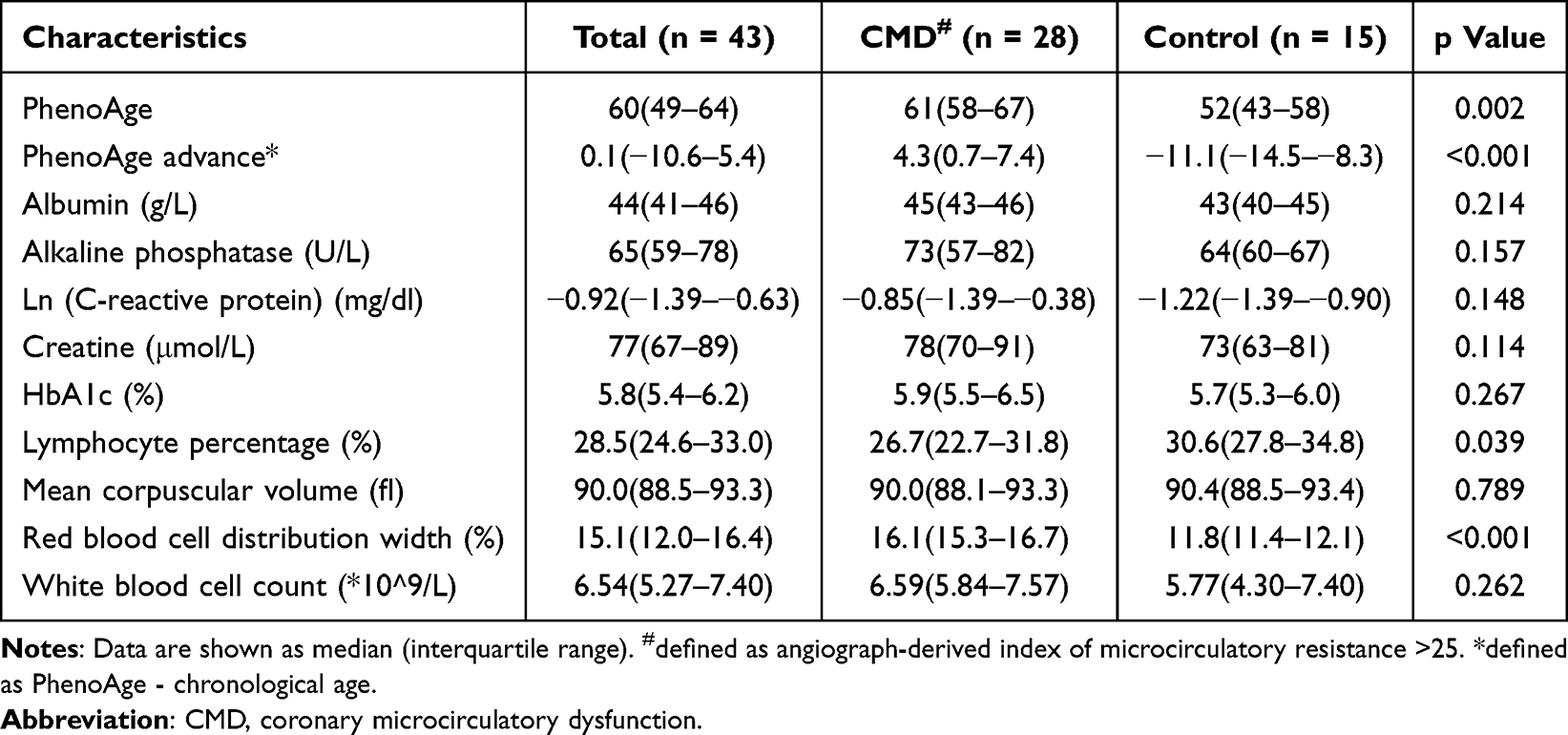 |
Table 3 Features in PhenoAge Calculation |
 |
Figure 3 Study workflow. In this study, we investigated the clinical and lipidomic features of patients with coronary microvascular dysfunction. PhenoAge, triglyceride glucose index, hypertension, TAG47:2-FA14:0, TAG48:4-FA18:1 and phosphatidylcholine (18:1/20:3) were independent risk factors of coronary microvascular dysfunction. The diagnosis of coronary microvascular dysfunction was markedly improved by incorporating lipidomic data with clinical factors. Abbreviations: AUC, area under the receiver operating characteristic curve; CMD, coronary microvascular dysfunction; PC, phosphatidylcholine; TAG, triacylglycerol. |
Selection of Candidate Biomarkers
We performed fifty rounds of 5-fold cross validation to build three ML models. In comparison with SVM and RF models, the XGBoost model demonstrated superior performance in terms of AUC (0.71; 95% confidence interval [CI], 0.68–0.75) and accuracy (0.68; 95% CI, 0.35–0.91) (Supplemental Figure 2). The SHAP method was employed to interpret the XGBoost model’s decision-making process. Feature contributions were ranked by descending mean absolute SHAP values (Figure 4A), revealing PhenoAge, TyG index, lymphocyte counts, high-density lipoprotein cholesterol and 11 lipid species as the fifteen most influential predictors. Furthermore, PhenoAge showed a significant positive correlation with SHAP values (Figure 4B).
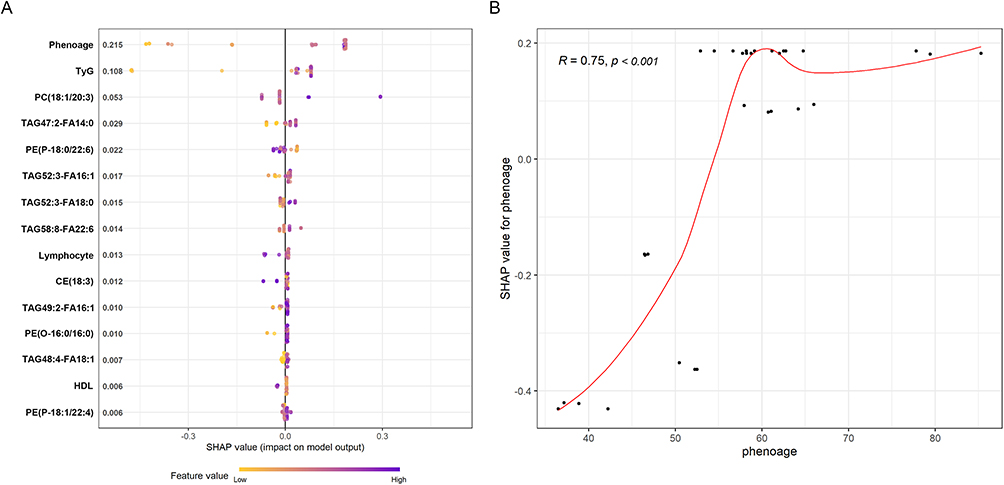 |
Figure 4 SHAP values of features in the XGBoost model. (A) Top 15 features included in the XGBoost model with best discrimination performance. Features are ranked by the importance evaluated through the SHAP method. (B) The positive correlation between SHAP values and PhenoAge. Abbreviations: CE, cholesterol ester; HDL, high-density lipoprotein cholesterol; PC, phosphatidylcholine; PE(O), alkylphosphatidylethanolamine; PE(P), alkenylphosphatidylethanolamine; SHAP, SHapley Additive exPlanations; TAG, triacylglycerol; TyG, triglyceride glucose index. |
Lasso regression with 5-fold cross validation was repeated 200 times, and lipid species were ranked by selection frequency (Supplemental Table 1). OPLS-DA was performed to generate VIP scores for each lipid (Supplemental Figure 3 and Supplemental Table 2). To enhance biomarker robustness, lipids meeting all three criteria—top 15 features in XGBoost (mean SHAP), top 15 selection frequency in Lasso regression, and VIP score >1 in OPLS-DA—were integrated with clinical factors into logistic regression models (Figure 1). Multivariable analyses identified PhenoAge, TyG index, hypertension, PC(18:1/20:3), TAG47:2-FA14:0 and TAG48:4-FA18:1 as independent risk factors of CMD (Table 4). All these factors were associated with elevated risk of CMD except PC(18:1/20:3) showing protective effect. The correlation between PhenoAge, TyG index and the risk of CMD are displayed in Figure 5. The odds ratio of CMD started to be >1 when PhenoAge was over 60 or Tyg index over 8.57.
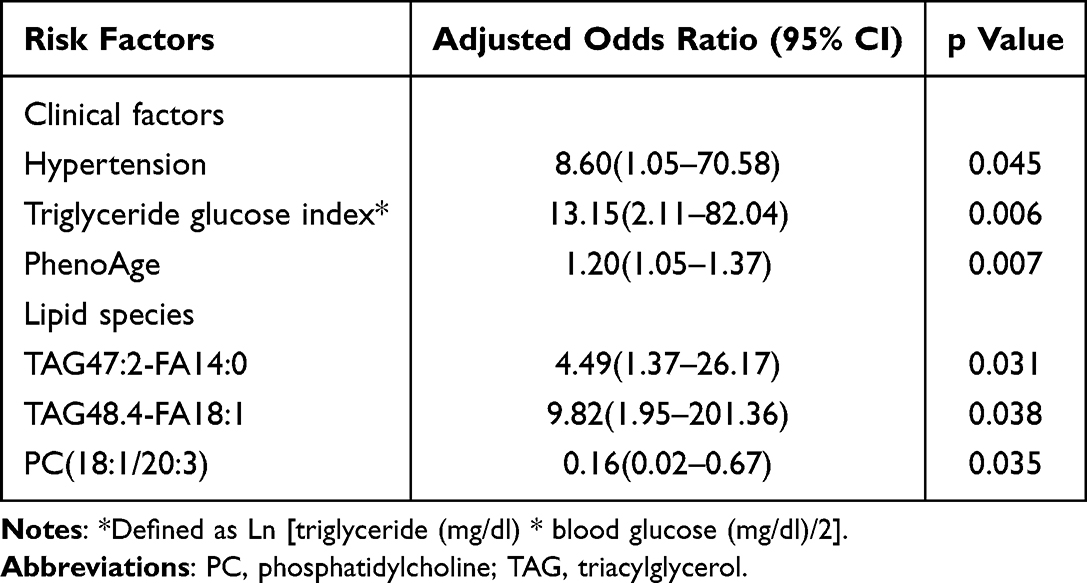 |
Table 4 Predictors of Coronary Microcirculatory Dysfunction in the Logistic Regression Model |
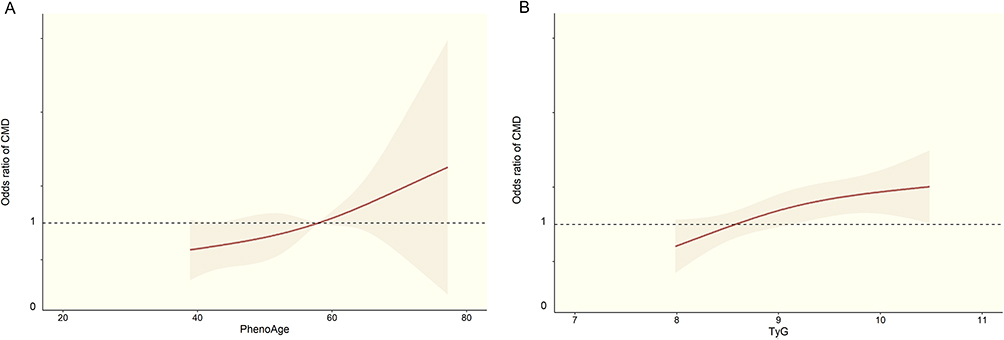 |
Figure 5 Association between PhenoAge, TyG and CMD risks. Restricted cubic spline curves are plotted to demonstrate the association between PhenoAge (A), TyG (B) and the odds ratio of CMD. Abbreviations: CMD, coronary microvascular dysfunction; TyG, triglyceride glucose index. |
Model Performance
The integrated logistic model incorporating both lipid species and clinical factors was compared with a clinical-factor-only model. The combined model demonstrated significantly superior discriminative ability relative to the clinical model (AUC: 0.94 [95% CI, 0.91–0.98] vs 0.86 [95% CI, 0.78–0.96]; p < 0.05) (Figure 6A). As shown in Figure 6B, the combined model exhibited higher consistency between the predicted and observed risks. In clinical impact curves, the model with clinical and lipidomic biomarkers yielded greater net benefits across the entire range of threshold (Figure 6C and D).
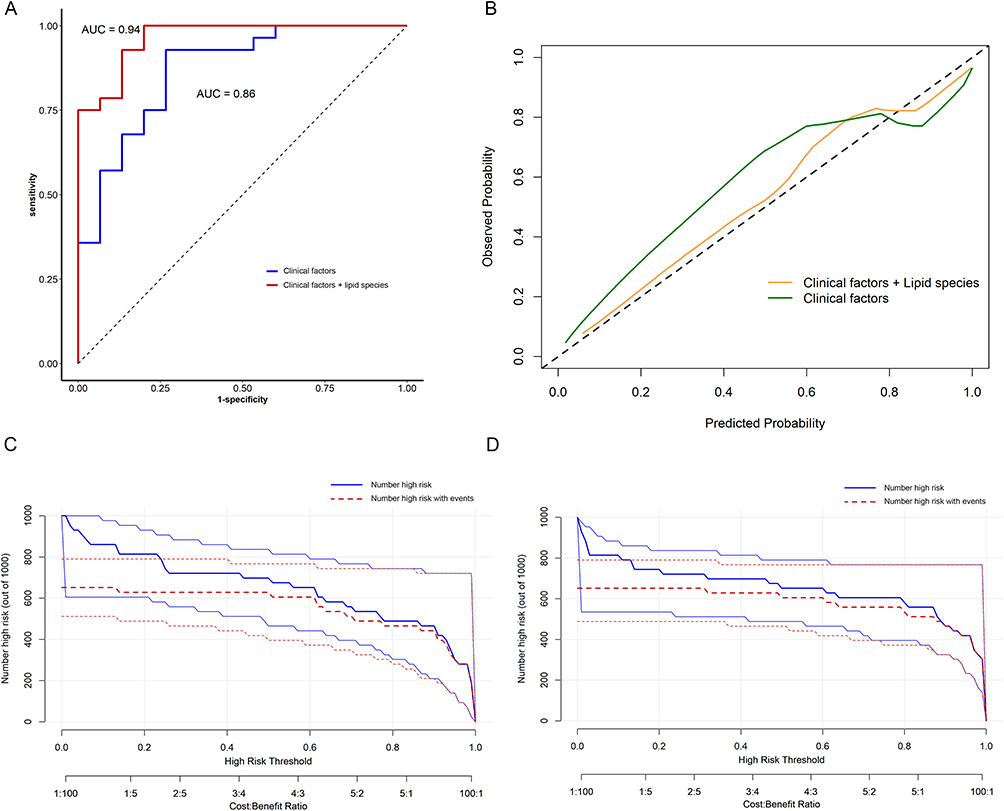 |
Figure 6 Performance of the predicting models. (A) The receiver operating characteristic curve of the clinical and integrated models. AUC was significantly improved in the integrated model (from 0.86 to 0.94, p < 0.05). (B) The calibration curves of the clinical and integrated models. Perfect prediction is shown by the diagonal black dashed line. The model incorporating clinical and lipidomic factors is closer to the observed probabilities indicating better calibration. The clinical impact curves of the clinical and integrated models are shown in (C and D). The integrated model brought better clinical benefits over most of the risk thresholds, as indicated by the number of high-risk patients with CMD closer to the number of high-risk patients. AUC, are under the receiver operating characteristic curve. |
Discussion
In this study, we investigated the lipidomic features of patients with CMD and identified 3 lipids independently associated with CMD. Besides, our findings indicated PhenoAge acceleration was prevalent among CMD patients. PhenoAge, TyG index and hypertension were significant clinical predictors of CMD. Incorporating lipidomic data with clinical factors could provide additional value in the prediction of CMD. These exploratory findings offered novel pathophysiological insights and potential diagnostic strategies for CMD.
Approximately 10% of patients presented non-obstructive coronary arteries despite moderate-to-severe ischemia.21 While ischemia and non-obstructive coronary artery disease (INOCA) was historically considered benign,22 contemporary evidence indicated that patients with INOCA often had CMD and elevated risk of adverse outcomes.5,23,24 The pathophysiology of CMD involved incompletely understood functional and structural alterations. Functional mechanisms encompassed impaired microvascular relaxation and pathological vasoconstriction.25 Structural changes may include luminal narrowing from vascular remodeling, fibrosis and thrombus plugging, while extraluminal compression due to reduced myocardial elasticity or elevated left ventricular end-diastolic pressure may also impair microcirculatory flow.26
Although therapeutic lifestyle modifications and anti-anginal medications may benefit CMD management, robust clinical evidence remained lacking. This was partially limited by the fact that the assessment of CMD predominantly relied on invasive methods and provocative tests. The advent of caIMR reduced the complexity of IMR measurement but it still required angiography. Less-invasive evaluation approaches for microcirculatory function are urgently needed.27 Patients with CMD often experienced functional limitation and anxiety, which could cause frequent clinic visits and healthcare resource consumption. Preliminary studies of endothelial/microvascular-targeted therapies show promising vascular functional improvements.28 However, randomized controlled trials are warranted.
Biological aging can be accessed via telomere length, epigenetic clocks, and composite clinical biomarkers. PhenoAge is a composite biological age derived from routine blood biomarkers, requiring no extra cost or specialized equipment. It integrates inflammation, nutrition, metabolism, and hematopoiesis, thereby capturing systemic aging beyond chronological age. Its superior prediction of mortality and cardiovascular events is well validated. Unlike epigenetic clocks, PhenoAge is accessible even in resource‑limited settings, making it a practical, versatile tool for cardiovascular risk stratification.
This study demonstrated a novel association between PhenoAge acceleration and CMD, which could help to understand the microvascular pathophysiology. Although the chronological age was comparable between the groups, CMD patients had significantly elevated PhenoAge. To our knowledge, this was the first study revealing biological aging acceleration specifically in patients with coronary microcirculatory impairment. These findings aligned with emerging evidence linking cellular senescence to endothelial dysfunction and extended prior researches on vascular aging.29 Exposure to hemodynamic forces of blood flow and circulating stimuli could induce endothelium cellular senescence. Senescent cells accumulated in vascular tissues could release pro-inflammatory cytokines, leading to endothelial barrier disruption and impaired nitric oxide bioavailability, which were core mechanisms in microvascular dysfunction.30,31 The absence of PhenoAge acceleration in non-CMD controls suggested its potential as a sensitive indicator of vascular vulnerability. The systemic aging phenotype may also explain the elevated cerebrocardiovascular risk in CMD patients despite patent epicardial arteries.32–34 However, CMD may also accelerate biological aging through chronic inflammation, oxidative stress, and metabolic dysregulation within the microvasculature. This bidirectional interplay creates a vicious cycle yet remains underexplored. Elucidating this relationship could inform novel therapeutic strategies targeting both CMD and aging pathways.
In this study, control subjects showed no PhenoAge acceleration. Their median PhenoAge advance was substantially negative (−11.1 years), indicating a biologically healthy profile consistent with their clinical status. This reflected the fact that our control group, though symptomatic, comprised patients with genuinely preserved microvascular function. This clear separation implied that accelerated aging was specifically associated with CMD in our cohort, rather than being a common trait in all patients with chest pain. This finding may be limited by the relatively modest sample size and the selective inclusion of symptomatic patients undergoing angiography. Further research is needed to validate this relationship in larger, multi-center cohorts.
Even though traditional lipid parameters were similar between CMD patients and controls, lipidomic analyses revealed profound alterations in the plasma lipidome of CMD patients. 75% of the dysregulated lipids belonged to the TAG class. This TAG predominance was consistent with recent evidence implicating triglyceride-rich lipoproteins (TRL) involvement in vascular inflammation.35–37 Some identified lipid species contained highly unsaturated fatty acids. Unsaturated lipids are prone to oxidative damage. Their oxidized products can trigger endothelial dysfunction and inflammation, which are key drivers of CMD. The abundance of such lipids in our CMD cohort suggests that oxidative lipid injury may contribute to microvascular pathology. Direct measurement of oxidized lipid species is warranted to confirm this pathway. Elevated TRL was a risk factor for both CAD and endothelial dysfunction,38 and demonstrated a causal association with increased mortality risk.39 Reduction of remnant lipoprotein cholesterol could possibly ameliorate endothelial dysfunction.40 Conversely, PE and related lipids were generally associated with a decreased CMD risk. As previously reported, PE and its derivatives were endogenous antioxidant with critical membrane-stabilizing function,41,42 which may prevent the microvasculature from oxidative injury. These lipidomic findings extended beyond conventional lipid metrics (eg, LDL-C and TG) by identifying molecular species that may serve as both biomarkers and therapeutic targets of CMD. These hypothesis-generating lipidomic signatures should be validated in multicenter cohorts before these markers can be considered for clinical use.
Beside the lipidomic alterations, we found that TyG index was also substantially higher in the CMD group. TyG index was regarded as a marker of insulin resistance, which could trigger endothelial damage and vasomotor dysfunction within the microvasculature.43,44 The elevated TyG index and dyslipidemia thus implicated an impaired cardiometabolic milieu which could directly lead to CMD and cardiovascular outcomes.45,46 In patients with chronic coronary syndrome, TyG index was closely correlated with caIMR, and an independent risk predictor for CMD.47 Notably, Zhang et al reported that the TyG-CMD correlation was even stronger in non-diabetic patients and females, which suggested its utility in identifying early microvascular injury prior to overt diabetes Integrating TyG assessment into clinical practice could enhance risk stratification, guide early interventions targeting microvascular injury, and potentially mitigate subsequent adverse events in high-risk cohorts.
A significant imbalance in sex distribution was observed between groups. Sex imbalance was an important limitation, given the known effects of sex hormones and menopausal status on lipid metabolism and vascular biology. The current cohort was too small for reliable sex-stratified analyses. Such analyses would have produced unstable estimates and increased the risk of overfitting. Menopausal status and sex-hormone-related variables were not systematically collected, which prevents us from distinguishing CMD-associated lipidomic differences from sex-related metabolic differences.
Despite its promise, routine clinical implementation of lipidomic profiling would face several hurdles. The need for high‑resolution mass spectrometry and specialized bioinformatics expertise may limit accessibility in most hospital laboratories. Data processing is computationally intensive, and standardized reference ranges across different platforms are lacking. Besides, the turnaround time for lipidomics is often longer than conventional lipid tests, and per‑sample costs remain substantial. Moreover, results require careful interpretation against clinical context. These challenges currently restrict lipidomics to research settings, but targeted panels based on research evidence and streamlined workflows may facilitate future translation.
Limitation
Several limitations must be acknowledged. First, this was an exploratory study of modest sample size. This constrained the statistical power for subgroup analyses. Validation in larger cohorts would be essential. Because both groups were symptomatic, the observed differences may be more specific to CMD, although they may be smaller than differences observed against healthy individuals. The findings should not be generalized to differences between CMD patients and the general healthy population. Second, as a single-center study, selection bias may limit the conclusions’ application to broader populations. Machine learning analyses were not intended to establish a ready-to-use clinical prediction model. Their role was to support exploratory feature screening and to identify lipidomic signals that merit further testing. Feature selection in ML models, while rigorously validated through SHAP, Lasso, and OPLS-DA, still required external validation to ensure generalizability. Third, while caIMR offered practical advantages over invasive IMR, provocative tests were not performed. This made it impossible to confirm whether coronary microvascular spasm coexisted. Fourth, lipidomic profiling relied on a single-timepoint sampling, which precluded the assessment of dynamic lipid changes in response to interventions or disease progression. Additionally, the mechanisms linking specific lipid species to microvascular dysfunction required experimental validation. Fifth, PhenoAge quantification utilized clinical biomarkers rather than direct cellular senescence markers, potentially underrepresenting tissue-level aging mechanisms. Moreover, the cross-sectional design precluded causal inferences regarding observed associations between TyG index, accelerated aging, lipidomic alterations and CMD pathogenesis. Finally, unmeasured confounders such as physical activity patterns, dietary components, and genetic predispositions may further influence the results. The impact of lipid-lowering medications on lipidomic and CMD is still unclear. Future longitudinal work is needed to integrate multi-omics approaches to elucidate mechanistic links between metabolic dysregulation, accelerated aging, and microvascular pathology.
Conclusion
This study demonstrated the association between accelerated biological aging and CMD and delineated a CMD-specific, hypothesis-generating lipidomic signature characterized by TAG enrichment. The integration of lipidomic biomarkers with clinical factors improved CMD diagnosis. Future studies should validate these biomarkers and explore targeted interventions to mitigate microvascular senescence and lipid-mediated endothelial injury.
Data Sharing Statement
The data used in this study would be available upon reasonable request by contacting the corresponding authors (Dr. You Zhou).
Ethical Approval
The study protocol was approved by the Ethics Committee of Shanghai Geriatric Medical Center (B2023-007) and conducted according to the guidelines of the Declaration of Helsinki. This trial was registered with the Chinese Clinical Trial Registry (URL: https://www.chictr.org.cn; Identifier: ChiCTR2500095360).
Funding
This study was supported by the National Natural Science Foundation of China (Grant No: 82370261) and Clinical Special Project of Shanghai Municipal Health Commission (20234Y0105).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Douglas PS, Patel MR, Bailey SR, et al. Hospital variability in the rate of finding obstructive coronary artery disease at elective, diagnostic coronary angiography. J Am Coll Cardiol. 2011;58(8):801–14. doi:10.1016/j.jacc.2011.05.019
2. Sharaf BL, Pepine CJ, Kerensky RA, et al. Detailed angiographic analysis of women with suspected ischemic chest pain (pilot phase data from the NHLBI-sponsored Women’s Ischemia Syndrome Evaluation [WISE] Study Angiographic Core Laboratory). Am J Cardiol. 2001;87(8):937–941. doi:10.1016/S0002-9149(01)01424-2
3. Shaw LJ, Shaw RE, Merz CN, et al. Impact of ethnicity and gender differences on angiographic coronary artery disease prevalence and in-hospital mortality in the American College of Cardiology-National Cardiovascular Data Registry. Circulation. 2008;117(14):1787–1801. doi:10.1161/CIRCULATIONAHA.107.726562
4. Sara JD, Widmer RJ, Matsuzawa Y, Lennon RJ, Lerman LO, Lerman A. Prevalence of Coronary Microvascular Dysfunction Among Patients With Chest Pain and Nonobstructive Coronary Artery Disease. JACC: Cardiovasc Interv. 2015;8(11):1445–1453. doi:10.1016/j.jcin.2015.06.017
5. Jespersen L, Hvelplund A, Abildstrøm SZ, et al. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur Heart J. 2012;33(6):734–744. doi:10.1093/eurheartj/ehr331
6. Ai H, Feng Y, Gong Y, et al. Coronary Angiography-Derived Index of Microvascular Resistance. Front Physiol. 2020;11:605356. doi:10.3389/fphys.2020.605356
7. Huang D, Gong Y, Fan Y, et al. Coronary angiography-derived index for assessing microcirculatory resistance in patients with non-obstructed vessels: the FLASH IMR study. Am Heart J. 2023;263:56–63. doi:10.1016/j.ahj.2023.03.016
8. Wan A, Rodrigues B. Endothelial cell-cardiomyocyte crosstalk in diabetic cardiomyopathy. Cardiovasc Res. 2016;111(3):172–183. doi:10.1093/cvr/cvw159
9. Jakubiak GK, Cieślar G, Stanek A. Nitrotyrosine, Nitrated Lipoproteins, and Cardiovascular Dysfunction in Patients with Type 2 Diabetes: what Do We Know and What Remains to Be Explained? Antioxidants. 2022;11(5):856. doi:10.3390/antiox11050856
10. Han X. Lipidomics for studying metabolism. Nat Rev Endocrinol. 2016;12(11):668–679. doi:10.1038/nrendo.2016.98
11. Wang R, Li B, Lam SM, Shui G. Integration of lipidomics and metabolomics for in-depth understanding of cellular mechanism and disease progression. J Genet Genomics. 2020;47(2):69–83. doi:10.1016/j.jgg.2019.11.009
12. Xu S, Ilyas I, Little PJ, et al. Endothelial Dysfunction in Atherosclerotic Cardiovascular Diseases and Beyond: from Mechanism to Pharmacotherapies. Pharmacol Rev. 2021;73(3):924–967. doi:10.1124/pharmrev.120.000096
13. Sen I, Trzaskalski NA, Hsiao YT, Liu PP, Shimizu I, Derumeaux GA. Aging at the Crossroads of Organ Interactions: implications for the Heart. Circ Res. 2025;136(11):1286–1305. doi:10.1161/CIRCRESAHA.125.325637
14. Camici PG, Crea F. Coronary microvascular dysfunction. N Engl J Med. 2007;356(8):830–840. doi:10.1056/NEJMra061889
15. Li Q, Qian Z, Huang Y, et al. Mechanisms of endothelial senescence and vascular aging. Biogerontology. 2025;26(4):128. doi:10.1007/s10522-025-10279-y
16. Gao D, Zhang L, Song D, et al. Values of integration between lipidomics and clinical phenomes in patients with acute lung infection, pulmonary embolism, or acute exacerbation of chronic pulmonary diseases: a preliminary study. J Transl Med. 2019;17(1):162. doi:10.1186/s12967-019-1898-z
17. Kwon D, Belsky DW. A toolkit for quantification of biological age from blood chemistry and organ function test data: bioAge. Geroscience. 2021;43(6):2795–2808. doi:10.1007/s11357-021-00480-5
18. Levine ME, Lu AT, Quach A, et al. An epigenetic biomarker of aging for lifespan and healthspan. Aging. 2018;10(4):573–591. doi:10.18632/aging.101414
19. Lundberg SM, Lee SI. A unified approach to interpreting model predictions. In:
20. Hochberg Y, Benjamini Y. More powerful procedures for multiple significance testing. Stat Med. 1990;9(7):811–818. doi:10.1002/sim.4780090710
21. Reynolds HR, Diaz A, Cyr DD, et al. Ischemia With Nonobstructive Coronary Arteries: insights From the ISCHEMIA Trial. JACC Cardiovasc Imaging. 2023;16(1):63–74. doi:10.1016/j.jcmg.2022.06.015
22. Lichtlen PR, Bargheer K, Wenzlaff P. Long-term prognosis of patients with anginalike chest pain and normal coronary angiographic findings. J Am Coll Cardiol. 1995;25(5):1013–1018. doi:10.1016/0735-1097(94)00519-V
23. Johnson BD, Shaw LJ, Buchthal SD, et al. Prognosis in women with myocardial ischemia in the absence of obstructive coronary disease: results from the National Institutes of Health-National Heart, Lung, and Blood Institute-Sponsored Women’s Ischemia Syndrome Evaluation (WISE). Circulation. 2004;109(24):2993–2999. doi:10.1161/01.CIR.0000130642.79868.B2
24. Smilowitz NR, Toleva O, Chieffo A, Perera D, Berry C. Coronary Microvascular Disease in Contemporary Clinical Practice. Circ Cardiovasc Interv. 2023;16(6):e012568. doi:10.1161/CIRCINTERVENTIONS.122.012568
25. Ford TJ, Rocchiccioli P, Good R, et al. Systemic microvascular dysfunction in microvascular and vasospastic angina. Eur Heart J. 2018;39(46):4086–4097. doi:10.1093/eurheartj/ehy529
26. Padro T, Manfrini O, Bugiardini R, et al. ESC Working Group on Coronary Pathophysiology and Microcirculation position paper on ‘coronary microvascular dysfunction in cardiovascular disease’. Cardiovasc Res. 2020;116(4):741–755. doi:10.1093/cvr/cvaa003
27. Schindler TH, Fearon WF, Pelletier-Galarneau M, et al. Myocardial Perfusion PET for the Detection and Reporting of Coronary Microvascular Dysfunction: a JACC: cardiovascular Imaging Expert Panel Statement. JACC Cardiovasc Imaging. 2023;16(4):536–548. doi:10.1016/j.jcmg.2022.12.015
28. Bairey Merz CN, Pepine CJ, Shimokawa H, Berry C. Treatment of coronary microvascular dysfunction. Cardiovasc Res. 2020;116(4):856–870. doi:10.1093/cvr/cvaa006
29. Bloom SI, Islam MT, Lesniewski LA, Donato AJ. Mechanisms and consequences of endothelial cell senescence. Nat Rev Cardiol. 2023;20(1):38–51. doi:10.1038/s41569-022-00739-0
30. Donato AJ, Machin DR, Lesniewski LA. Mechanisms of Dysfunction in the Aging Vasculature and Role in Age-Related Disease. Circ Res. 2018;123(7):825–848. doi:10.1161/CIRCRESAHA.118.312563
31. Matsushita H, Chang E, Glassford AJ, Cooke JP, Chiu CP, Tsao PS. Tsao PS. eNOS activity is reduced in senescent human endothelial cells: preservation by hTERT immortalization. Circ Res. 2001;89(9):793–798. doi:10.1161/hh2101.098443
32. Minamino T, Miyauchi H, Yoshida T, Ishida Y, Yoshida H, Komuro I. Endothelial cell senescence in human atherosclerosis: role of telomere in endothelial dysfunction. Circulation. 2002;105(13):1541–1544. doi:10.1161/01.CIR.0000013836.85741.17
33. Liu L, Zhao B, Yu Y, et al. Vascular Aging in Ischemic Stroke. J Am Heart Assoc. 2024;13(15):e033341. doi:10.1161/JAHA.123.033341
34. Sepúlveda C, Palomo I, Fuentes E. Mechanisms of endothelial dysfunction during aging: predisposition to thrombosis. Mech Ageing Dev. 2017;164:91–99. doi:10.1016/j.mad.2017.04.011
35. Bernelot Moens SJ, Verweij SL, Schnitzler JG, et al. Remnant Cholesterol Elicits Arterial Wall Inflammation and a Multilevel Cellular Immune Response in Humans. Arterioscler Thromb Vasc Biol. 2017;37(5):969–975. doi:10.1161/ATVBAHA.116.308834
36. Schnitzler JG, Dallinga-Thie GM, Kroon J. The Role of (Modified) Lipoproteins in Vascular Function: a Duet Between Monocytes and the Endothelium. Curr Med Chem. 2019;26(9):1594–1609. doi:10.2174/0929867325666180316121015
37. Varbo A, Benn M, Tybjærg-Hansen A, Nordestgaard BG. Elevated remnant cholesterol causes both low-grade inflammation and ischemic heart disease, whereas elevated low-density lipoprotein cholesterol causes ischemic heart disease without inflammation. Circulation. 2013;128(12):1298–1309. doi:10.1161/CIRCULATIONAHA.113.003008
38. Nakamura T, Takano H, Umetani K, et al. Remnant lipoproteinemia is a risk factor for endothelial vasomotor dysfunction and coronary artery disease in metabolic syndrome. Atherosclerosis. 2005;181(2):321–327. doi:10.1016/j.atherosclerosis.2005.01.012
39. Wadström BN, Pedersen KM, Wulff AB, Nordestgaard BG. Elevated remnant cholesterol, plasma triglycerides, and cardiovascular and non-cardiovascular mortality. Eur Heart J. 2023;44(16):1432–1445. doi:10.1093/eurheartj/ehac822
40. Nakamura T, Uematsu M, Yoshizaki T, Kobayashi T, Watanabe Y, Kugiyama K. Improvement of endothelial dysfunction is mediated through reduction of remnant lipoprotein after statin therapy in patients with coronary artery disease. J Cardiol. 2020;75(3):270–274. doi:10.1016/j.jjcc.2019.08.006
41. Pohl EE, Jovanovic O. The Role of Phosphatidylethanolamine Adducts in Modification of the Activity of Membrane Proteins under Oxidative Stress. Molecules. 2019;24(24):4545. doi:10.3390/molecules24244545
42. Tasseva G, Bai HD, Davidescu M, Haromy A, Michelakis E, Vance JE. Phosphatidylethanolamine deficiency in Mammalian mitochondria impairs oxidative phosphorylation and alters mitochondrial morphology. J Biol Chem. 2013;288(6):4158–4173. doi:10.1074/jbc.M112.434183
43. Cao BF, Liu K, Chen HW, et al. Impact of baseline and trajectory of the cardiometabolic indices on incident microvascular complications in patients with type 2 diabetes. Atherosclerosis. 2025;407:120407. doi:10.1016/j.atherosclerosis.2025.120407
44. Du T, Yuan G, Zhang M, Zhou X, Sun X, Yu X. Clinical usefulness of lipid ratios, visceral adiposity indicators, and the triglycerides and glucose index as risk markers of insulin resistance. Cardiovasc Diabetol. 2014;13(1):146. doi:10.1186/s12933-014-0146-3
45. Berwick ZC, Dick GM, Tune JD. Heart of the matter: coronary dysfunction in metabolic syndrome. J Mol Cell Cardiol. 2012;52(4):848–856. doi:10.1016/j.yjmcc.2011.06.025
46. Söner S, Aktan A, Kılıç R, et al. Association between the triglyceride-glucose index and contrast-induced nephropathy in chronic total occlusion patients undergoing percutaneous coronary intervention. BMC Cardiovasc Disord. 2025;25(1):31. doi:10.1186/s12872-025-04474-5
47. Zhang W, Liu L, Chen H, et al. Association between the triglyceride-glucose index and the presence and prognosis of coronary microvascular dysfunction in patients with chronic coronary syndrome. Cardiovasc Diabetol. 2023;22(1):113. doi:10.1186/s12933-023-01846-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.