Back to Journals » Journal of Asthma and Allergy » Volume 14
Lipid Profile and IL-17A in Allergic Rhinitis: Correlation With Disease Severity and Quality of Life
Authors Sheha D ![]() , El-Korashi L
, El-Korashi L ![]() , AbdAllah AM, El Begermy MM, Elzoghby DM
, AbdAllah AM, El Begermy MM, Elzoghby DM ![]() , Elmahdi A
, Elmahdi A
Received 12 November 2020
Accepted for publication 8 January 2021
Published 4 February 2021 Volume 2021:14 Pages 109—117
DOI https://doi.org/10.2147/JAA.S290813
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Dina Sheha,1 Lobna El-Korashi,2 Amany M AbdAllah,3 Marwa M El Begermy,4 Doaa M Elzoghby,5 Amira Elmahdi1
1Department of Internal Medicine, Allergy and Clinical Immunology, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 2Department of Medical Microbiology and Immunology, Faculty of Medicine, Zagazig University, Zagazig, Egypt; 3Department of Family Medicine, Faculty of Medicine, Zagazig University, Zagazig, Egypt; 4Department of Otorhinolaryngology, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 5Department of Clinical Pathology, Faculty of Medicine, Ain Shams University, Cairo, Egypt
Correspondence: Dina Sheha
Faculty of Medicine, Ain Shams University, El-Abbassia Street, Cairo, 11566, Egypt
Tel +20 1001525144
Email [email protected]
Background: Recent data display the possible role of cytokines such as interleukin-10 (IL-10), IL-17 and IL-23 as a link between dyslipidemia and atopy; however, the relationship between dyslipidemia, allergic rhinitis (AR), and the underlying mechanisms involved is unclear.
Purpose: To measure the lipid profile and IL-17A level in AR patients in comparison to healthy controls, and correlate serum lipid level with the severity of symptoms and quality of life (QoL) of AR patients.
Patients and Methods: Peripheral blood samples were collected from AR patients (n=70) and a control group (n=80). Samples were analyzed for serum total IgE by ELISA, serum lipid profile, and IL-17A level by ELISA. Severity of AR symptoms was assessed by visual analogue scale (VAS) score and the rhinoconjunctivitis QoL questionnaire.
Results: Serum lipid profile and level of IL-17A in AR patients were significantly higher in comparison to controls (P < 0.001). Positive correlations were found between total cholesterol (TC) and the severity of AR and QoL. IL-17A was positively correlated with triglyceride (TG) level and low-density lipoprotein cholesterol (LDL-C) (P=0.011, r=0.303; P=0.043, r=0.242, respectively). Additionally, IL-17A was negatively correlated with high-density lipoprotein cholesterol (HDL-C) level (P=0.036, r=− 0.251). IL-17A was positively correlated with both age and VAS score with statistical significance (P=0.033, r=0.225; P=0.011, r=0.302, respectively).
Conclusion: Dyslipidemia might play a potential role in the severity of AR symptoms and impairment of patients’ QoL. Highlighting this association might alert physicians to evaluate the lipid profile in AR patients for timely diagnosis and treatment of dyslipidemia in an attempt to improve disease control and improve QoL.
Keywords: allergic rhinitis, cholesterol, dyslipidemia, IgE, interleukin-17, quality of life
Introduction
Allergic rhinitis (AR) is a symptomatic disorder induced by exposure of the nasal mucosa to diverse aeroallergens that is mediated through immunoglobulin E (IgE) hypersensitivity reactions. AR is characterized by four cardinal symptoms of watery rhinorrhea, nasal obstruction, nasal itching and sneezing.1 AR has a wide prevalence, it is estimated to affect 20–30% of adults and up to 40% of pediatrics.2 AR is associated with multiple comorbid disorders, including asthma, conjunctivitis, eczema, rhinosinusitis, adenoid hypertrophy, obstructive sleep apnea, disordered sleep with consequent educational and behavioural effects. These associated comorbidities negatively correlate with the quality of life (QoL), and work performance.3
Dyslipidemia is a major risk for atherosclerosis and cardiovascular diseases especially coronary heart disease (CHD), and may play a major role earlier than other risk factors.4 Dyslipidemia modulates the immune response through the release of pro-inflammatory mediators, activation of immune cells (eg, B-cell, T-cells and dendritic cells),5 promoting polarization of T-helper 2 (Th-2) and Th17 and downregulating interleukin-10 (IL-10) cytokine synthesis.6 Th2 and Th17 release cytokines as IL6, IL-1, IL-4, and IL-17.7 Th2 immune response with an increased production of IL-4 and tumour necrosis factor-α (TNF-α) has been described in AR.8
IL-17 cytokine, produced by Th17 cells, plays a pivotal role in host defense reactions, inflammatory diseases and allergic responses.IL-17 belongs to a family of cytokines that includes six members of different homology and function: IL-l7 (also IL-17A) IL-17B, IL-17C, IL-17D and IL-17 E.9 The role of TNF-α and IL-17 in the pathogenesis and regulation of inflammation in autoimmune diseases such as psoriasis has been described previously.10,11 Serum IL-17A level correlated significantly with clinical and inflammatory markers in patients with persistent moderate to severe AR evaluated during the pollen season. Moreover, studies suggest that serum IL-17A level correlates with symptom scores and with the number of peripheral blood eosinophils, suggesting that Th-17 cells may be involved in the chronic allergic reaction. Authors even proposed IL-17A as a new biomarker of disease progression and allergy.12 Research suggests a link between cholesterol and the adaptive immune system, as both have the same immunological pathways involving Th1 toTh2 switch, an increase in Th2 related IgG1 and IgE release, and elevation of pro-inflammatory Th2 cytokines release such as IL-4.13
Numerous research investigated the association between dyslipidemia and allergic diseases. Fessler et al14 demonstrated the relationship between total cholesterol (TC) level and atopy in children 6–17 years of age. Ouyang et al15 reported increased allergic sensitisation with elevated low-density lipoprotein cholesterol (LDL-C) level. Kusunoki et al16 demonstrated a positive association between TC and LDL-C levels and the allergic sensitization in school-aged children. Similarly, a meta-analysis of ten studies investigated the lipid profile of asthmatics and found higher levels of LDL and low level of high-density lipoprotein (HDL) in asthma patients in comparison to controls.17 Vinding et al18 found higher LDL and triglycerides (TG) were associated with asthma, airway obstruction and higher incidence of aeroallergen sensitization. Elevated HDL was associated with reduction of airway obstruction and lower risk of aeroallergen sensitization. To our knowledge, only a few studies have explored the association of abnormal serum lipids in AR patients and its effect on disease severity.
Since IL-17A could represent a link between AR and dyslipidemia, we aimed to investigate the possible relationship between AR, IL-17A level and dyslipidemia, and correlate level with the severity of AR and QoL of AR patients.
Patients and Methods
Study Design and Setting
Seventy adult AR patients and 80 healthy volunteers as a control group were enrolled in the current case–control study, conducted from March 2019 to August 2019. AR patients were selected by systematic randomization from patients attending the allergy outpatient clinic at Ain Shams University, Cairo and Zagazig University, Zagazig, Egypt. Laboratory Techniques were performed in the Medical Microbiology and Immunology Department, Zagazig University, Zagazig, Egypt. Healthy controls were apparently healthy individuals who were recruited from relatives of patients attending the internal medicine outpatient clinic. They had no chronic diseases or allergic disorders, they were not on regular medications and had no complaints concerning mental or physical health.
AR was diagnosed according to the Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines.19 Inclusion criteria were atopic adult AR with a positive family history of atopy and positive skin prick test (SPT) for at least one inhalant allergen. Patients with asthma, those on statin therapy, patients with acute illness like high-grade fever, first 2 weeks following surgery, non-allergic inflammatory nasal pathology, sleep disorders, diabetics, obese patients, hypothyroid, hypertensive patients, smokers and patients with autoimmune disorders were excluded from the study. No patients received systemic steroids or immunotherapy within 1 month of enrollment. An informed verbal consent was obtained from all participants. The research ethics committee of Zagazig University approved the study (IRB number 6222-25-6-2020) and the procedure outlined for the obtainment of verbal consent. The whole process was documented and the consent was conducted with an impartial witness after which the consent was transcribed. The study procedure complies with the country regulations about subjects’ data protection and maintaining their integrity, and the study was conducted in accordance with the declarations of Helsinki.
Detailed medical history of allergy was collected from each participant including family history of atopy. Clinical examination (ear, nose, throat and chest examination), and SPT to common aeroallergens were performed in the clinic. Venous blood samples for serum lipid profile, serum total IgE and serum level of IL-17A were drawn from all participants.
Assessment of Severity of AR
The severity of AR was measured using the visual analogue scale (VAS) score for global assessment of severity of nasal and non-nasal symptoms. AR patients were asked to rate the combination of the nasal and non-nasal symptoms on a scale (0–10 cm) as follows:
Mild: 0–3; Moderate: 3.1–7; Severe: 7.1–10.19
Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ)
QoL was assessed in the AR group by the RQLQ total score. The instrument has 28 items in seven domains (sleep, non-rhinoconjunctivitis symptoms, practical problems, nasal symptoms, eye symptoms, activity limitations, and emotional function). The overall RQLQ score is the mean of all 28 responses.19
SPT
Skin testing was performed on AR patients according to Bernstein et al.20 A panel for the most common locally encountered inhaled allergens was used including house dust mites, cockroach, cotton, molds mix, ragweed, mugwort, Chenopodium album, hay dust, pigeon feathers, dog hair, cat hair, rabbit hair. Allergen extracts of skin testing were locally prepared at Allergy and Immunology Unit, Department of Internal Medicine, Faculty of Medicine, Ain Shams University. Aqueous allergen extracts (1:100 wt/vol) preparation was done according to allergen extract preparation guidelines developed by the AAAAI/ACAAI/JCAAI and all aqueous allergen extracts were stored at 4 °C.21
The maximum or mean diameter of the wheal to various allergens was read at 15 minutes. A wheal of 3mm or more in diameter was considered positive (indicating sensitization to the allergen).
Sample Collection
Under complete aseptic conditions, 10mL of fasting venous blood was obtained by a clean venipuncture in the early morning from all participants after 9–12 hours of fasting. Patients were on regular average diet 3 days before sampling. The serum was separated by centrifugation (1000× g for 15 minutes) and divided into three tubes. Serum of one tube was immediately assayed for lipid profile (TC, TG, HDL-C and LDL-C), while the serum collected in the other tube was stored at −20°C for subsequent assay of the serum total IgE, IL-17A concentrations. Hemolysed samples were discarded. Repeated freezing and thawing was avoided.
Serum Lipid Profile
Serum TC, triglycerides and HDL-C were assayed on Microlab 300 Semi Automated Clinical Chemistry Analyzer supplied by EliTech clinical system (France,[email protected]).
TC, TG and HDL-C were assayed by (homogenous for HDL-C) enzymatic colorimetric quantitative determination at wavelength (500, 500, and 600/700 nm respectively) using kits provided by Human diagnostics kit (Human Gesellschaft für Biomedica und Diagnostica mbH Max-Planck-Ring 21.6 5205 Wiesbaden-Germany). LDL-C was calculated according to the “Friedwald equation”.22
Dyslipidemia was defined according to the American College of Cardiology/American Heart Association (ACC/AHA) Blood Cholesterol 2013 Guideline, as follows: hypercholesterolemia was defined as total cholesterol (TC) level greater than 200 mg/dL and/or LDL-C level greater than 100 mg/dL, hypertriglyceridemia as TG level greater than 150 mg/dL; and low HDL-C lower than 40 mg/dL in men and 50 mg/dL in women.23
Serum Total IgE
Quantitative measurement of total IgE in the serum was done using a commercially available quantitative enzyme-linked Immunosorbent assay (ELISA) Kit supplied by Calbiotech Inc. (1935 Cordell Ct., El Cajon, CA 92020, USA) according to the manufacturer’s instructions, and the results were expressed in IU/mL.
IL-17A Concentration
Human IL17-A was measured by commercially available quantitative ELISA Kit supplied by Thermo Fisher Scientific (Bender Med Systems gmbH/Campus Vienna Biocenter 2/1030 Vienna, Austria) according to the manufacturer’s instructions and expressed in pg/mL.
Statistical Analysis
Data analysis was performed using the software SPSS (Statistical Package for the Social Sciences) version 20 (SPSS Inc., Chicago, Illinois, USA). Quantitative variables were described using means and standard deviations. Categorical variables were described using absolute frequencies and to compare the proportion of categorical data, chi square test was used when appropriate. Kolmogorov–Smirnov (distribution-type) and Levene (homogeneity of variances) tests were used to verify assumptions for use in parametric tests. To compare the means of two groups, independent sample t-test was used. Mann–Whitney test was used to compare continuous variables between two groups when data were not normally distributed. Pearson correlation and Spearman rank correlation coefficients were used to assess the strength and direction of a linear relationship between two variables. The level of statistical significance was set at 5% (P<0.05). Highly significant difference was present if P≤0.001.
Results
Descriptive data of the study groups are represented in Table 1. Patients and controls were matched regarding age and gender. The mean age of AR patients was 30.74 years (± 7.24) and controls were 32.85 years (± 7.5). Total IgE and IL17-A level were significantly higher in cases in comparison to controls (Table 1). Runny nose, sneezing, nasal obstruction, postnasal drip, itchy nose, cough and eye symptoms prevailed in 60%, 62.9%, 72.9%, 30%, 20%, 38.6% and 10% of the patients within AR group, respectively.
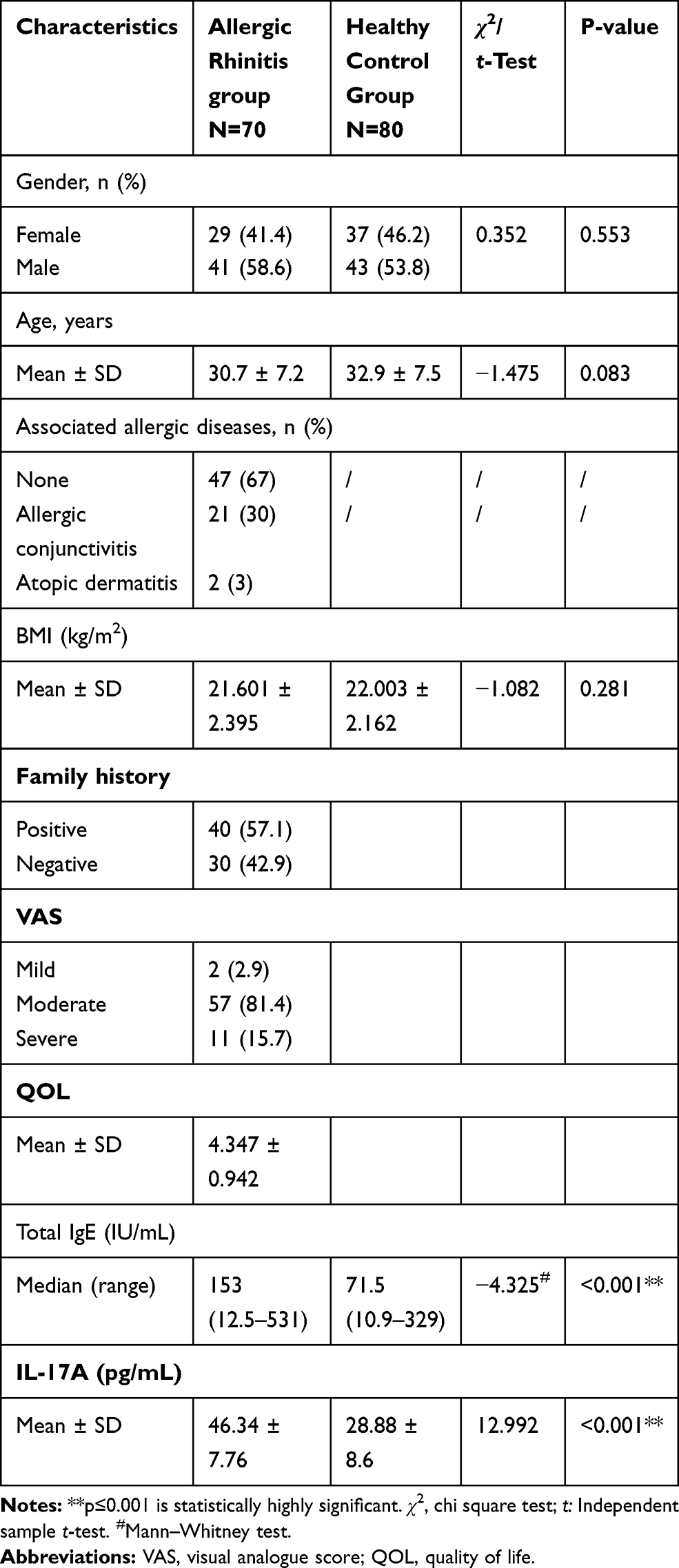 |
Table 1 Demographic and Laboratory Data Characteristics of the Study Groups |
Associated allergic conjunctivitis and atopic dermatitis co-existed in 30% and 3% respectively of those patients (Table 1)
Serum Lipid Profile
Levels of TC and LDL-C were statistically significantly higher in cases than controls. Mean ±SD of TC in cases and controls was 225,65±62.91mg/dl and 187.92±35.24mg/dl, respectively.
Regarding HDL_C, mean±SD in cases was 47.25±5.36 mg/dl and in controls 49.83±4.29 mg/dl, showing statistically significantly lower levels in cases than controls. There was a non-significant difference in serum TG and very-low-density lipoprotein cholesterol (VLDL-C) between the two groups (P=0.79, P=0.175) (Table 2).
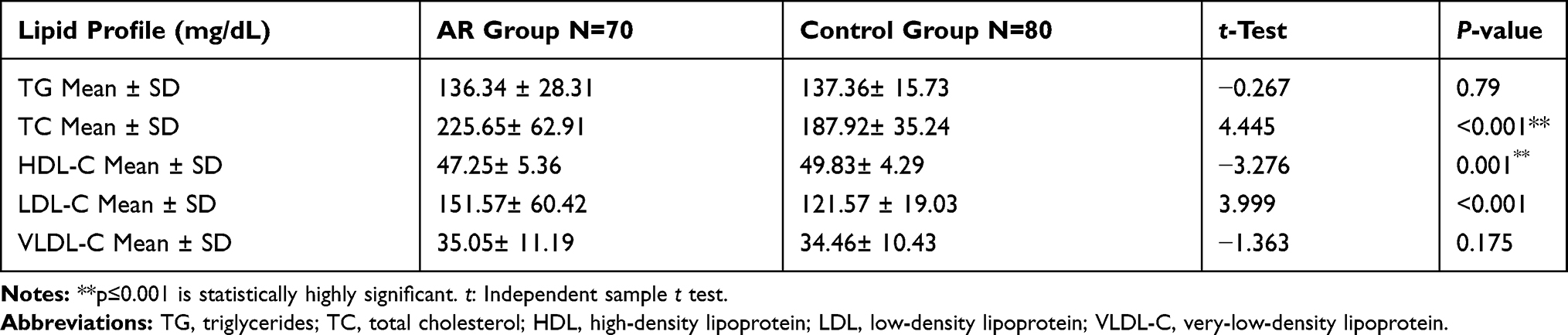 |
Table 2 Serum Lipid Profile of Study Subjects |
Dyslipidemia Among Studied Groups
AR patients had significantly increased risk of dyslipidemia by 6.27-fold (95% confidence interval (CI) of crude odds ratio (COR)=2.71–14.51, P<0.001). Approximately 44% of the patients with AR had dyslipidemia versus 11.2% of the healthy controls.
Correlation Between Serum Lipid Profile and Severity of AR and IL-17A
Correlation studies were performed to assess the relationship between serum lipid profile and the severity of AR assessed by VAS (P=0.039, r=0.31) and RQLQ score (P=0.04, r=0.247). There was a positive correlation between IL-17A and TG and LDL-C levels (P=0.011, 0.043, respectively). IL-17A level was negatively correlated to HDL-C level (P=0.036), while no significant correlation was found for the other correlation studies listed in Table 3.
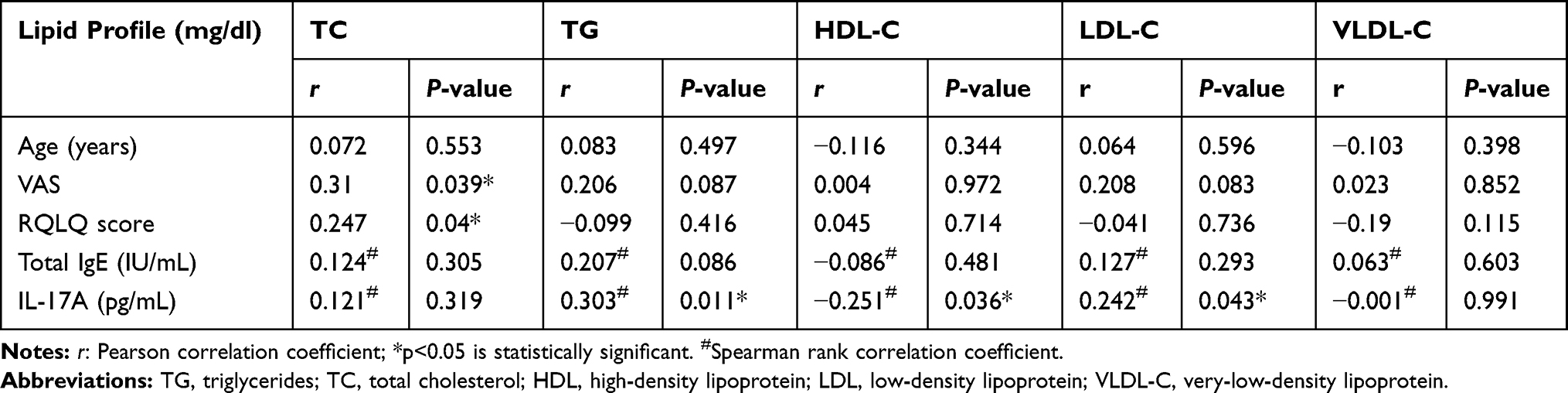 |
Table 3 Correlation Between Serum Lipid Profile and Different Study Parameters |
Correlation Between IL-17A Level and Disease-Specific Characteristics of Patients with AR
There was a statistically significant correlation between IL-17A and both age and VAS score (p=0.033, r=0.225, 0=0.011, r=0.302; 95% CI; 0.078:0.486) and VAS score (95% CI; 0.078:0.486). On the other hand, there was a non-significant correlation between IL-17A and total IgE and RQLQ score (Table 4).
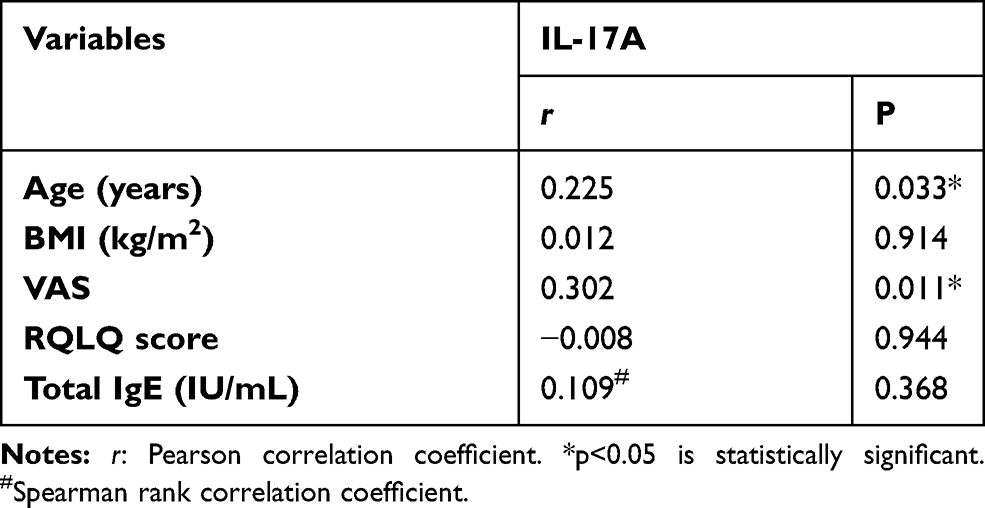 |
Table 4 Correlation Between IL-17A and All of Patients Age, VAS, RQLQ, and Total IgE |
Discussion
Serum lipid levels and their clinical implication in the management and monitoring of cardiovascular diseases or diabetic patients is well established.24,25 On the contrary, the role of dyslipidemia in AR is not fully elucidated.
The current case–control study aimed to investigate the possible relationship between AR, IL-17A level and dyslipidemia and correlate levels with the severity of AR and QoL of AR patients. We included 70 AR patients and 80 healthy controls, and found dyslipidemia in 44% of AR patients versus 11.2% of controls. Levels of TC and LDL-C were significantly higher in AR patients, while HDL-C was significantly lower. Similarly, recent studies have demonstrated a significant association between high serum lipid levels and AR.26,27 Additionally, Schäfer et al investigated the effect of serum cholesterol on atopy and found that elevation of serum cholesterol is associated with an increased incidence of atopic diseases.28 Recent publications suggest the role of dyslipidemia in promoting atopic inflammation, through polarizing Th2 response.7,29 Another proposed theory is the cholesterol trafficking. Cholesterol is a critical microdomain of cell wall lipid rafts that plays an essential role in cell signaling. Changes in these cholesterol rafts trigger the toll-like receptor-signaling pathway of the innate immune reaction, which in turn aggravates the atopic inflammation.30
We report a positive correlation between TC levels and both VAS score, and RQLQ score. Ahmed et al in a recent Egyptian study reported similar results,29 which was also confirmed by regression analysis of Yon et al.31 TC and LDL-C were associated with the severity of AR high TC, which has been reported to increase allergen-specific IgE synthesis thus exacerbating allergic symptoms, which denotes a positive correlation between dyslipidemia and atopy.32 This could be attributed to the impact of dyslipidemia on the immune system where dyslipidemia induces a shift toward an immunologic Th2-oriented response and exacerbates allergic inflammation.26,33 Additionally, hypercholesterolemia is known for being pro-inflammatory, inducing the release of inflammatory cytokines30 and in turn aggravating the symptoms of AR.
We assume the poor QoL is due to the burden of increased AR severity, as well as the socioeconomic and financial burden of treatment costs, and the metabolic burden of dyslipidemia. The inflammatory nature of AR causes nasal obstruction, sleep difficulties, snoring, hypersomnolence, diminished work performance, and finally insomnia that all negatively impact the patients’ QoL.
Several studies have suggested that metabolic factors, such as dyslipidemia, are related to allergic diseases, but the related causal mechanisms remain elusive.34–36 Hence we investigated the role of IL-17A as a link between AR and dyslipidemia, in order to explore one of the cytokines incriminated in the pathogenesis.
We found higher levels of IL-17A in AR patients compared to controls. Similarly, many studies declared this finding.37–43 Moreover, other studies found higher IL-17A positive cells in peripheral blood and nasal mucosa of AR patients compared to healthy controls.44,45 It seems that Th17 cells may be involved in the process of neutrophil infiltration that occurs during the acute phase of allergic reaction.46 Besides, IL-17 induces allergen-specific Th2 cell activation, hence the production of serum IgE and eosinophil accumulation suggesting a regulatory role in Th2-allergic immune response.47
We report a positive correlation between IL-17A level and both TG and LDL-C levels, while IL-17A was negatively correlated to HDL-C level among AR patients. These findings are in line with.26 This could be explained by the fact that dyslipidemia causesTh2 and Th17 polarization and cytokines’ release as (IL-4, IL-17) with decreased production of IL-10. These cytokines’ disturbance is related to chronic inflammation that is common to both atopic predisposition and dyslipidemia6,46,48 Similarly, Vinding et al found that triglyceride levels were associated with increased risk of aeroallergen sensitization, which is one cause of AR.18
Furthermore, we found significant positive correlation between IL-17A and AR severity assessed by VAS score. IL-17 is a pro-inflammatory cytokine which in turn explains its role in increasing the severity of AR symptoms. This is consistent with many other studies.49 Also, Nieminen et al50 showed that serum IL-17A levels and allergen-induced IL-17A messenger RNA expression correlate with symptom severity, as assessed via a VAS score and symptom medication score, respectively. In addition, Lu et al51 reported significant correlations between AR symptoms and the expression of IL-17 in nasal mucosa and peripheral blood.
A study by Shahsavan et al52 found that patients with moderate to severe persistent AR demonstrated significantly greater IL-22 and IL-17A production than healthy controls, suggesting that the development of persistent AR is influenced by these cytokines. A correlation was found between IL-22 and IL-17A serum levels, along with the mean number of IL-22 and IL-17A positive cells in the nasal mucosa, and specific IgE levels, nasal eosinophil count, and total nasal symptom score.
The results of these studies are partially in conflict with Amin et al,53 who found no correlation between IL-17 and the patient’s symptom scores, although AR patients have significant higher serum levels of IL-17 than controls.
In our study, we did not report a correlation between IL-17 and total IgE. Huang et al,45 documented that IL-17 level was positively related to the level of total IgE, and the serum level of IL-17 and IL-23 in the AR patients were markedly higher than those in healthy subjects.
We are aware that one of the limitations of the current study is the small sample size of the study population, and large-scale multicenter studies should be performed to further elucidate the importance of measuring serum lipid profile in AR patients, and including pediatrics where AR is more prevalent. The disease duration of AR was not reported in the current study. In addition, longitudinal studies might aid in a better understanding of the causal relationship between dyslipidemia and AR, to determine whether AR is preceded by dyslipidemia or the other way round. The role of cytokines as IL-17A as a biomarker of AR severity and its role in dyslipidemia should be further elucidated. Furthermore, early detection of dyslipidemia in AR patients may help in the prevention of long-term future cardiovascular morbidity and mortality in AR patients.
Conclusion
Measuring of serum lipid profile and IL-17A in AR patients could be a potential indicator of severe disease, and future research ought to explore the impact of timely treatment of dyslipidemia on severity of AR and QoL of patients.
Ethics Approval and Informed Consent
The research ethics committee of Zagazig University approved the study (IRB number 6222-25-6-2020), and an informed verbal consent was obtained from all participants.
Acknowledgment
We thank all patients who participated in the study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Seidman MD, Gurgel RK, Lin SY, et al. Clinical practice guideline. Otolaryngol Neck Surg. 2015;152(2):197–206. doi:10.1177/0194599814562166
2. Meltzer EO. Allergic rhinitis: burden of illness, quality of life, comorbidities and control. Immunol Allergy Clin North Am. 2016;36(2):235–248. doi:10.1016/j.iac.2015.12.002
3. Cingi C, Gevaert P, Mösges R, et al. Multi-morbidities of allergic rhinitis in adults: European Academy of Allergy and Clinical Immunology Task Force Report. Clin Transl Allergy. 2017;7:17. doi:10.1186/s13601-017-0153-z
4. Lin CF, Chang YH, Chien SC, Lin YH, Yeh HY. Epidemiology of dyslipidemia in the Asia Pacific Region. Int J Gerontol. 2018;12(1):2–6. doi:10.1016/j.ijge.2018.02.010
5. Nus M, Mallat Z. Immune-mediated mechanisms of atherosclerosis and implications for the clinic. Expert Rev Clin Immunol. 2016;12(11):1217–1237. doi:10.1080/1744666X.2016.1195686
6. Yang WQ. Study of the relationship between IL-10 polymorphism and serum lipoprotein levels in Han Chinese individuals. Genet Mol Res. 2016;15(2). doi:10.4238/gmr.15028016
7. Hu X, Wang Y, Hao LY, et al. Sterol metabolism controls TH17 differentiation by generating endogenous RORγ agonists. Nat Chem Biol. 2015;11(2):141–147. doi:10.1038/nchembio.1714
8. Poddighe D, Brambilla I, Licari A, Marseglia GL. Pediatric rhinosinusitis and asthma. Respir Med. 2018;141:94–99. doi:10.1016/j.rmed.2018.06.016
9. Monin L, Gaffen SL. Interleukin 17 family cytokines: signaling mechanisms, biological activities, and therapeutic implications. Cold Spring Harb Perspect Biol. 2018;10(4):a028522. doi:10.1101/cshperspect.a028522
10. Chiricozzi A, Guttman-Yassky E, Suárez-Fariñas M, et al. Integrative responses to IL-17 and TNF-α in human keratinocytes account for key inflammatory pathogenic circuits in psoriasis. J Invest Dermatol. 2011;131(3):677–687. doi:10.1038/jid.2010.340
11. Martin DA, Towne JE, Kricorian G, et al. The emerging role of IL-17 in the pathogenesis of psoriasis: preclinical and clinical findings. J Invest Dermatol. 2013;133(1):17–26. doi:10.1038/jid.2012.194
12. Murdaca G, Colombo BM, Puppo F. The role of Th17 lymphocytes in the autoimmune and chronic inflammatory diseases. Intern Emerg Med. 2011;6(6):487–495. doi:10.1007/s11739-011-0517-7
13. Manti S, Cuppari C, Marseglia L, et al. Association between allergies and hypercholesterolemia: a systematic review. Int Arch Allergy Immunol. 2017;174:67–76. doi:10.1159/000480081
14. Fessler MB, Jaramillo R, Crockett PW, Zeldin DC. Relationship of serum cholesterol levels to atopy in the US population. Allergy. 2010;65(7):859–864. doi:10.1111/j.1398-9995.2009.02287.x
15. Ouyang F, Kumar R, Pongracic J, et al. Adiposity, serum lipid levels, and allergic sensitization in Chinese men and women. J Allergy Clin Immunol. 2009;123:940–8.e10. doi:10.1016/j.jaci.2008.11.032
16. Kusunoki T, Morimoto T, Sakuma M, et al. Total and low-density lipoprotein cholesterol levels are associated with atopy in schoolchildren. J Pediatr. 2011;158:334–336. doi:10.1016/j.jpeds.2010.10.009
17. Peng J, Huang Y. Meta-analysis of the association between asthma and serum levels of high-density lipoprotein cholesterol and low-density lipoprotein cholesterol. Ann Allergy Asthma Immunol. 2017;118(1):61–65. doi:10.1016/j.anai.2016.09.447
18. Vinding RK, Stokholm J, Chawes BLK, Bisgaard H. Blood lipid levels associate with childhood asthma, airway obstruction, bronchial hyperresponsiveness, and aeroallergen sensitization. J Allergy Clin Immunol. 2016;137(1):68–74.e4. doi:10.1016/j.jaci.2015.05.033
19. Klimek L, Bachert C, Pfaar O, et al. ARIA guideline 2019: treatment of allergic rhinitis in the German health system. Allergol Select. 2019;3(1):22–50. doi:10.5414/ALX02120E
20. Bernstein IL, Li JT, Bernstein DI, et al. Allergy diagnostic testing: an updated practice parameter. Ann Allergy Asthma Immunol. 2008;100(3):S1–148.
21. Li JT, Lockey RF, Bernstein IL, Portnoy JM, Nicklas RA; American Academy of Allergy Asthma and Immunology. American College of Allergy, Asthma and Immunology. Joint task force on practice parameters, allergen immunotherapy: a practice parameter. Ann Allergy Asthma Immunol. 2003;90:1–40. doi:10.1016/S1081-1206(10)63600-9
22. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18:499–502. doi:10.1093/clinchem/18.6.499
23. Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults. Circulation. 2013;129(25 suppl 2):S1–45. doi:10.1161/01.cir.0000437738.63853.7a
24. Ference BA, Graham I, Tokgozoglu L, Catapano AL. Impact of lipids on cardiovascular health: JACC health promotion series. J Am Coll Cardiol. 2018;72(10):1141–1156. doi:10.1016/j.jacc.2018.06.046
25. Afshinnia F, Pennathur S. Lipids and cardiovascular risk with CKD. Clin J Am Soc Nephrol. 2020;15(1):57. doi:10.2215/CJN.13531119
26. La Mantia I, Andaloro C, Albanese PG, Varricchio A. Blood lipid levels related to allergic rhinitis: a significant association? EuroMediterranean Biomed J. 2017;12(30):144–147.
27. Alwan A, Alobaidi A. Lipid profile in patients with asthma and allergic rhinitis. Int J Med Sci. 2018;1(2):9–24.
28. Schafer T, Ruhdorfer S, Weigl L, et al. Intake of unsaturated fatty acids and HDL cholesterol levels are associated with manifestations of atopy in adults. Clin Exp Allergy. 2003;33(10):1360–1367. doi:10.1046/j.1365-2222.2003.01780.x
29. Ahmed M, Madian Y, El-Tabbakh M, El-Serafi A, Nasr G, Hessam W. Correlation between dyslipidemia and severity of allergic rhinitis. Egypt J Otolaryngol. 2018;34(2):111. doi:10.4103/ejo.ejo_90_17
30. Ko SH, Jeong J, Baeg MK, et al. Lipid profiles in adolescents with and without asthma: Korea National Health and Nutrition Examination Survey data. Lipids Health Dis. 2018;17(1):158. doi:10.1186/s12944-018-0807-4
31. Yon DK, Lee SW, Ha EK, et al. Serum lipid levels are associated with allergic rhinitis, nasal symptoms, peripheral olfactory function, and nasal airway patency in children. Allergy. 2018;73(9):1905–190828. doi:10.1111/all.13484
32. Craig T, McCann J, GurevichH F, Davies M. The correlation between allergic rhinitis and sleep disturbance. J Allergy Clin Immunol. 2004;114:S139–45. doi:10.1016/j.jaci.2004.08.044
33. Robertson AKL, Zhou X, Strandvik B, Hansson GK. Severe hypercholesterolaemia leads to strong Th2 responses to an exogenous antigen. Scand J Immunol. 2004;59(3):285–293. doi:10.1111/j.0300-9475.2004.01403.x
34. Huang SL, Lin KC, Pan WH. Dietary factors associated with physician-diagnosed asthma and allergic rhinitis in teenagers: analyses of the first Nutrition and Health Survey in Taiwan. Clin Exp Allergy. 2001;31:259–264. doi:10.1046/j.1365-2222.2001.00938.x
35. Lumia M, Luukkainen P, Kaila M, et al. Maternal dietary fat and fatty acid intake during lactation and the risk of asthma in the offspring. Acta Paediatr. 2012;101:e337–43. doi:10.1111/j.1651-2227.2012.02718.x
36. Raj D, Kabra SK, Lodha R. Childhood obesity and risk of allergy or asthma. Immunol Allergy Clin North Am. 2014;34:753–765. doi:10.1016/j.iac.2014.07.001
37. Ciprandi G, Fenoglio D, De Amici M, Quaglini S, Negrini S, Filaci G. Serum IL-17 levels in patients with allergic rhinitis. J Allergy Clin Immunol. 2008;122(3):650–651.e2. doi:10.1016/j.jaci.2008.06.005
38. Ciprandi G, De Amici M, Murdaca G, et al. Serum interleukin-17 levels are related to clinical severity in allergic rhinitis. Allergy. 2009;64(9):1375–1378. doi:10.1111/j.1398-9995.2009.02010.x
39. Huang X, Chen Y, Zhang F, Yang Q, Zhang G. Peripheral Th17/Treg cell-mediated immunity imbalance in allergic rhinitis patients. Braz J Otorhinolaryngol. 2014;80(2):152–155. doi:10.5935/1808-8694.20140031
40. Tang J, Xiao P, Luo X, et al. Increased IL-22 level in allergic rhinitis significantly correlates with clinical severity. Am J Rhinol Allergy. 2014;28(6):e197–201. doi:10.2500/ajra.2014.28.4088
41. Tsvetkova-Vicheva VM, Gecheva SP, Komsa-Penkova R, Velkova AS, Lukanov TH. IL-17 producing T cells correlate with polysensitization but not with bronchial hyperresponsiveness in patients with allergic rhinitis. Clin Transl Allergy. 2014;4(1):3. doi:10.1186/2045-7022-4-3
42. Xuekun H, Qintai Y, Yulian C, Zhang G. Correlation of gammadelta-T-cells, Th17 cells and IL-17 in peripheral blood of patients with allergic rhinitis. Asian Pac J Allergy Immunol. 2014;32(3).
43. Bayrak Degirmenci P, Aksun S, Altin Z, et al. Allergic rhinitis and its relationship with IL-10, IL-17, TGF-β, IFN-γ, IL 22, and IL-35. Dis Markers. 2018;2018:9131432. doi:10.1155/2018/9131432
44. Ba L, Du J, Liu Y, Shang T, Yang F, Bian P. The expression and significance of interleukin-17 and the infiltrating eosinophils in nasal polyps and nasal mucous of allergic rhinitis. L J. 2010.
45. Huang X, Yang Q, Chen Y, Li P, Zhang G, Li Y. Expressions of IL-17, IL-21 and IL-23 in the serum of allergic rhinitis patients. J Med Biochem. 2011;30(4):323–327. doi:10.2478/v10011-011-0025-3
46. Miossec P, Korn T, Kuchroo VK. Interleukin-17 and Type 17 Helper T cells. N Engl J Med. 2009;361(9):888–898. doi:10.1056/NEJMra0707449
47. Oboki K, Ohno T, Saito H, Nakae S. Th17 and Allergy. Allergol Int. 2008;57(2):121–134. doi:10.2332/allergolint.R-07-160
48. Manti S, Leonardi S, Panasiti I, Arrigo T, Salpietro C, Cuppari C. Serum IL-10, IL-17 and IL-23 levels as “bioumoral bridges” between dyslipidemia and atopy. Cytokine. 2017;99:43–49. doi:10.1016/j.cyto.2017.07.002
49. Aly MAG, El Tabbakh MT, Heissam WF, Abbadi SH. The study of a possible correlation between serum levels of interleukin 17 and clinical severity in patients with allergic rhinitis. Allergy Rhinol (Providence). 2017;8(3):126–131. doi:10.2500/ar.2017.8.0207
50. Nieminen K, Valovirta E, Savolainen J. Clinical outcome and IL-17, IL-23, IL-27 and FOXP3 expression in peripheral blood mononuclear cells of pollen-allergic children during sublingual immunotherapy. Pediatr Allergy Immunol. 2010;21(2):e174–e184. doi:10.1111/j.1399-3038.2009.00920.x
51. Lu HG, Peng H, Chen DH, Li TY, Shi JB. [Relationship between allergic symptoms and RORC2 and IL-17 in patients with allergic rhinitis]. Zhonghua ErBi Yan Hou Tou Jing Wai Ke Za Zhi. 2011;46(2):144–148. Chinese.
52. Shahsavan S, Pirayesh A, Samani OZ, et al. The relationship between-17A and IL-22 expression and clinical severity in patients with moderate/severe persistent allergic rhinitis. Am J Otolaryngol. 2019;40(2):173–178. doi:10.1016/j.amjoto.2018.12.009
53. Amin K, Issa SM, Ali KM, et al. Evidence for eosinophil and IL-17 mediated inflammation in allergic rhinitis. Clin Mol Allergy. 2020;18:6. doi:10.1186/s12948-020-00117-6
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.