Back to Journals » Local and Regional Anesthesia » Volume 8
Lidocaine versus ropivacaine for postoperative continuous paravertebral nerve blocks in patients undergoing laparoscopic bowel surgery: a randomized, controlled, double- blinded, pilot study
Authors Ghisi D, Fanelli A, Jouguelet-Lacoste J, La Colla L, Auroux A, Chelly J ![]()
Received 12 March 2015
Accepted for publication 20 April 2015
Published 14 September 2015 Volume 2015:8 Pages 71—77
DOI https://doi.org/10.2147/LRA.S84476
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Stefan Wirz
Daniela Ghisi,1,3 Andrea Fanelli,1,2 Julie Jouguelet-Lacoste,1 Luca La Colla,1,4 Anne-Sophie Auroux,1,5 Jacques E Chelly1
1Department of Anesthesiology, University of Pittsburgh Medical Center, Pittsburgh, PA, USA; 2Anesthesia and Intensive Care Unit, Policlinico S.Orsola-Malpighi, Bologna, Italy; 3Department of Anesthesia and Postoperative Intensive Care, Istituto Ortopedico Rizzoli, Bologna, Italy; 4Department of Anesthesia, Intensive Care and Pain Therapy, Università degli Studi di Parma, Parma, Italy 5Institut des Sciences Pharmaceutiques et Biologiques-Faculté de Pharmacie de Lyon Université Claude Bernard Lyon, France
Background and objectives: Lidocaine could provide many advantages in continuous regional anesthesia techniques, including faster onset, greater titratability, and lower cost than long-acting local anesthetics. This prospective, randomized, double-blinded, pilot study is therefore intended to compare lidocaine to ropivacaine in bilateral continuous paravertebral blocks using a multimodal approach for postoperative pain management following laparoscopic bowel surgery.
Methods: Thirty-five ASA I–III consecutive patients undergoing elective laparoscopic bowel surgery and bilateral thoracic paravertebral continuous blocks were analyzed: bilateral thoracic paravertebral infusions of ropivacaine 0.2% (Group Ropi, n=18) or lidocaine 0.25% (Group Lido, n=17) were started at 7 mL/h in the postanesthesia care unit. For each patient, we collected numerical rating scores (NRS) for pain at rest and during movement at baseline, at postanesthesia care unit discharge, at 24 hours and 48 hours after the end of surgery, as well as hydromorphone patient-controlled analgesia requirements, local anesthetic consumption, side effects, postoperative complications, and functional outcomes.
Results: No effect of group distribution on NRS scores for pain at rest or at movement (P=0.823 and P=0.146), nor on hydromorphone (P=0.635) or local anesthetic consumption (P=0.063) was demonstrated at any analyzed time point. Hospital length of stay and spontaneous ambulation were comparable between groups (P=0.636 and P=0.148). In the context of a multimodal approach, the two drugs showed comparable safety profiles.
Discussion: Lidocaine 0.25% and ropivacaine 0.2% provided similar analgesic profiles after elective abdominal surgeries, without any difference in terms of functional outcomes. The easier titratability of lidocaine together with its lower cost induced our clinical practice to definitely switch from ropivacaine to lidocaine for postoperative bilateral paravertebral continuous infusions.
Keywords: laparoscopic bowel surgery, lidocaine, ropivacaine, continuous paravertebral nerve blocks, pilot study
Introduction
Continuous nerve blocks represent an interesting alternative to single blocks because they allow a longer lasting block and a modulation of the block intensity.1 In this regard, short-acting local anesthetics have been shown to allow faster onset time and quicker titratability when compared to long-acting ones such as ropivacaine and bupivacaine. Furthermore, lidocaine, a short-acting local anesthetic, also offers the advantages: 1) to be safer than ropivacaine and bupivacaine,2,3 2) allows an easier blood concentration monitoring, and 3) costs less than ropivacaine. Although Capdevila et al demonstrated the effectiveness of lidocaine 1% as a local anesthetic solution for continuous femoral nerve blocks,4 Casati et al compared lidocaine and ropivacaine in continuous interscalene brachial plexus blocks after shoulder surgery and demonstrated that lidocaine provided sensory and motor blocks making it less suitable than ropivacaine for continuous peripheral nerve block infusion.5
Recently, we experienced a renewed interest for the use of continuous both unilateral and bilateral paravertebral as an alternative to epidural. Although the local anesthetic solution of choice in this indication is ropivacaine or bupivacaine, the concern for local anesthetic toxicity in the case of bilateral continuous paravertebral blocks raises the possibility of using lidocaine in this indication. Watson et al reported that continuous unilateral paravertebral infusion with bupivacaine and lidocaine for post-thoracotomy pain was equianalgesic.6 This prospective, randomized, double-blinded, study was designed to assess the efficacy, side-effect profile, and safety of lidocaine compared to ropivacaine in bilateral continuous paravertebral nerve blocks for postoperative analgesia following laparoscopic bowel surgery.
Methods
This single-center, double-blinded, randomized pilot study, after Institutional Review Board approval from the University of Pittsburgh, PA (PRO07080230), and signed informed consent, was conducted in 35 (Figure 1) American Society of Anesthesiologists (ASA) physical status I–III consecutive patients undergoing elective laparoscopic bowel surgery and bilateral thoracic paravertebral continuous nerve blocks at the University of Pittsburgh Medical Center Presbyterian-Shadyside Hospitals in Pittsburgh, Pennsylvania. Between the period of October 2009 and August 2011, patients between 18 years and 75 years of age with a body mass index <40 were enrolled. Patients were excluded if unable to express informed consent; if not oriented to place, person, or time; if they presented any contraindication to the placement of bilateral thoracic paravertebral catheters, chronic painful conditions, preoperative opioid use, allergy to the drugs/agents used in the study protocol, personal or family history of malignant hyperthermia, serum creatinine >1.4 g/dL, pregnancy, sepsis, unstable angina, congestive heart disease, valvular heart disease, severe COPD, or respiratory support via ventilator postoperatively; or if they underwent emergency surgery.
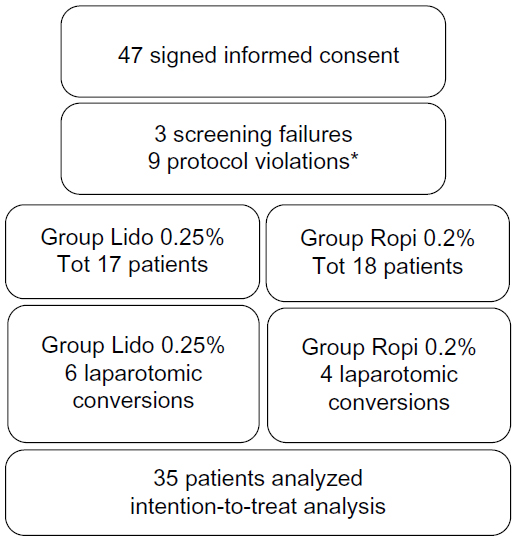 | Figure 1 CONSORT flow diagram of patients screened, included, randomized and evaluated in the intention-to-treat analysis. |
After determining eligibility and obtaining a signed informed consent, subjects were enrolled and randomized to one of the two study groups on the day of surgery using a sealed envelope determined by a computer-generated list that made assignments randomly based on enrollment number. The study groups were defined as: Group Lidocaine (Group Lido; subjects in this group were scheduled to receive a continuous bilateral infusion of 0.25% lidocaine postoperativley through their paravertebral catheters) and Group Ropivacaine (Group Ropi; subjects scheduled to receive a continuous bilateral infusion of 0.2% ropivacaine postoperatively through their paravertebral catheters).
On the day of surgery, the pain score at rest using an 11-point verbal numerical pain scale (numerical rating scale [NRS]) with 0 indicating no pain and 10 indicating the worst pain imaginable.
The patient was then placed in a sitting position for bilateral paravertebral catheter placement between T8 and T9. Standard monitoring for vital signs was registered every 5 minutes (blood pressure via automated cuff, pulse oximetry, and heart rate), supplemental oxygen via a nasal cannula was initiated, and a light sedation (midazolam 1–2 mg and fentanyl 50–100 μg intravenously [IV] titrated to patient comfort) was administered. As previously described, the site of introduction of the needle was marked on the skin, 2.5 cm lateral on each side of the midpoint of the spinous process of T9. The area was then prepared and draped in a sterile fashion, and 1% lidocaine was infiltrated subcutaneously at each point of anticipated needle entry. A sterile 18-G Tuohy needle (Perifix Continuous Epidural Anesthesia Set, Product Code CE18T; B. Braun Medical, Inc., Bethlehem, PA) was introduced perpendicularly to the skin until the transverse process was encountered, and the depth to the skin was noted. The needle was then readjusted in a caudad direction and inserted inferior to the corresponding transverse process to a depth ~1 cm deep to the transverse process. After final needle placement, a hanging drop technique was used to rule out intrapleural placement while the patient inhaled and exhaled deeply. Next, in both groups, 5 mL of 0.5% ropivacaine was injected slowly through each needle after negative aspiration for blood. This was followed by insertion of the nerve block catheter to a depth 5 cm beyond the tip of the needle. An additional 10 mL of 0.5% ropivacaine was then injected in 5 mL increments with negative aspiration for blood, through each catheter. The total volume of local anesthetics was 15 mL of 0.5% ropivacaine on each side or 30 mL of 0.5% ropivacaine total. The catheters were secured with Steri-Strips (3M, St Paul, Minnesota, USA) and a transparent occlusive dressing (Tegaderm, 3M, St Paul).
After routine intraoperative general anesthesia care, once in the postanesthesia care unit (PACU), bilateral paravertebral infusions of either ropivacaine 0.2% (Group 1) or lidocaine 0.25% (Group 2) was started at 7 mL/h on each side, according to the subject randomization. The PACU nurse also titrated intravenous boluses of hydromorphone to patients’ comfort (NRS score ≤4). Then, each subject was given access to patient-controlled analgesia (PCA) of hydromorphone (0.2 mg bolus, 8 minutes lockout, no basal infusion, and no 1-hour limit). Additional pain relief was available via nurse-administered 10 mL/h boluses of local anesthetic solution via the pump to the paravertebral catheters (5 mL/h for each side). In the PACU, a single IV bolus of ketorolac at 7.5 mg was available for additional pain management as rescue medication. NRS scores for pain at rest and during deep breathing immediately before discharge from the PACU and total analgesic requirements were recorded by a blinded research coordinator. In the PACU, each subject was monitored for at least an hour with continuous pulse oximetry, electrocardiography, and regular blood pressure measurements. Once adequate analgesia was established, the patients were transferred to the hospital ward.
After discharge from the PACU, additional pain relief was available via nurse-administered 3 mL/h boluses of local anesthetic via the catheter pumps (3 mL each side). In addition, nurse-administered intravenous boluses of hydromorphone 0.3 mg IV every 30 minutes as needed, up to two doses while the patient had the PCA, and 0.8–1 mg every hour as needed, up to four doses in 2 hours once the patient was taking oral pain therapy. Each subject was assessed daily by members of the acute interventional perioperative pain service blinded to the type of local anesthetic infusion. The infusion rates via the paravertebral catheters were adjusted at the discretion of the pain service up to a rate of 10 mL/h per side. The PCA dose was adjusted as deemed necessary by the acute pain team in order to provide adequate analgesia. In addition, 7.5 mg of IV ketorolac was available as rescue medication every 6 hours for the first 48 hours. Once the patient was able to tolerate oral liquids as determined by the surgeon, the PCA was discontinued, and oxycodone 5 mg po was available to the patient every 4 hours as needed for mild–moderate pain (NRS score 1–6) or oxycodone 10 mg po every 6 hours as needed for severe pain (NRS score 7–10). Pain assessment (0–10 NRS scores) both at rest and during deep breathing was performed postoperatively at 24 hours and at 48 hours after the end of surgery. Daily supplemental analgesic requirements and side effects were blindly recorded at 24-hour and 48-hour timepoints. Ability to ambulate (walking >15 feet) was noted. Hospital lengths of stays were measured in days spent in the hospital postoperatively. The readiness for discharge was determined by each surgeon (blind investigator) when the patient met the following criteria: 1) return of gastrointestinal function as manifested by passing of flatus and tolerating of general diet without nausea or vomiting, 2) hemodynamic stability, 3) normothermia, 4) ability to ambulate without assistance, 5) no clinical evidence of deep vein thrombosis/pulmonary embolism (DVT/PE), and 6) pain controlled by oral agents.
Side effects and complications were recorded during the study period.
Statistical analysis
The primary outcome of the study is the NRS score for pain at rest at 24 hours. Secondary end points are amounts of supplemental PCA and nerve block boluses, time to first flatus/defecation, and hospital length of stay. A total sample size of 64 subjects (32 patients in each arm) is required to detect a difference of 0.5 SD, using an alpha error of 0.05 and a power of 0.8. After enrollment of 47 patients, we decided to complete the present interim analysis, and the study was then interrupted due to equivalence in results between the two groups.
Data are expressed as mean ± SD for normally distributed variables, median (range) for non-normally distributed ones and percentages for categorical variables. Data were compared using the independent sample t-tests, the Mann-Whitney U-test, repeated measures analysis of variance, or Fisher’s exact test, as appropriate. Postoperative NRS scores for pain, hydromorphone consumption, and duration of hospital stay are compared between groups using the general linear model. The null hypothesis was rejected at a level of alpha <0.05. Statistical analysis was performed with SPSS 21 (IBM Corporation, Armonk, NY, USA).
Results
Forty-seven patients were enrolled in this randomized, controlled, double-blinded pilot study. Twelve patients were excluded from the analysis: three prior to randomization because they did not meet all inclusions criteria (screen failure) and nine patients after randomization – one patient required mechanical ventilation postoperatively (Group Ropi), one patient because of changes in the surgical procedures (Group Ropi), two patients for whom the PCA was stopped prematurely because they were either confused or over sedated (one in Group Lido and one in Group Ropi), and five patients because of technical problem with the block (three in Group Ropi [in one patient: one paravertebral catheter could not be infused, one paravertebral catheter removed by the nurse at the request of the patient because of itchiness and finally one paravertebral was dislodged] and two in Group Lido [one paravertebral catheter removed at the request of the patient and one paravertebral catheter removed because it was kinked]).
Therefore, 35 patients were included in the present analysis: 17 patients received lidocaine 0.25% continuous infusion while 18 received ropivacaine 0.2% continuous infusion postoperatively through bilateral paravertebral blocks. Among these patients, six patients in Group Lido and four patients in Group Ropi were converted from laparoscopic to open surgery. These data were included in the present intention-to-treat interim analysis (Figure 1).
Anthropometric and demographic data are shown in Table 1. Surgical procedures lasted 189 (127–521) minutes in Group Lido versus 228 (109–605) minutes in Group Ropi, P=0.351. Surgical procedures were performed by four different teams in both groups; nevertheless, the distribution of surgeons was comparable between groups.
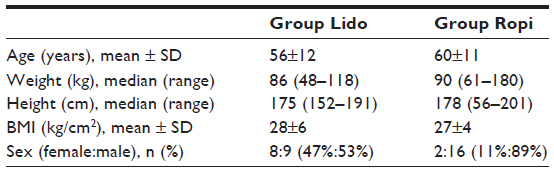 | Table 1 Demographic and anthropometric characteristics of the two groups |
Median NRS score for pain at rest and during movement in Group Lido was 3 (1–8) and 7 (5–9), respectively, at PACU discharge versus 3 (3–8) and 4 (3–8), respectively, in Group Ropi. NRS score for pain at rest and during movement at 24 hours after the end of surgery in Group Lido was 3 (2–6) and 5 (3–6), respectively, versus 3 (3–5) and 5 (3–6), respectively, in Group Ropi, while NRS score for pain at rest and during movement at 48 hours after the end of surgery in Group Lido was 3 (2–5) and 5 (3–6), respectively, versus 3 (2–5) and 4 (3–8), respectively, in Group Ropi. NRS score for pain at rest and during movement decreased significantly in both groups over time but data were comparable between groups, P=0.823 and P=0.146, respectively.
Hydromorphone consumption in the PACU was 1.6 (0–14.4) mg in Group Lido versus 1.1 (0.2–8.3) in Group Ropi, P=0.193. Also hydromorphone consumption at 24 hours postoperatively was comparable between groups: 9.2 (1.2–29.3) mg in Group Lido versus 5.7 (1.4–24.2) in Group Ropi, while hydromorphone consumption at 48 hours postoperatively was 16.1 (1.6–54.7) mg in Group Lido versus 9.6 (2–39.5) in Group Ropi. There was no effect of group on hydromorphone consumption (P=0.635).
Local anesthetic consumption through paravertebral catheters in the PACU was 77.4 (21–242.2) mL in Group Lido versus 50.5 (28–122.5) mL in Group Ropi, P=0.139. Patients in Group Lido received 20 (0–40) mL of boluses in the PACU versus 20 (0–40) mL of boluses in Group Ropi, P=0.318. Local anesthetic consumption was 378.7 (184–594) mL in Group Lido versus 364.8 (330.7–511.6) mL in Group Ropi 24 hours postoperatively and 698 (4–1088) mL in Group Lido versus 778.2 (605.1–946.2) mL in Group Ropi 48 hours postoperatively. There was no effect of group on local anesthetic consumption (P=0.063).
Patients in Group Lido received 0 (0–12) mL of boluses in Group Lido during the first postoperative day in the surgical floor versus 0 (0–30) mL of boluses in Group Ropi, P=0.807 and 0 (0–6) mL of boluses in Group Lido versus 0 (0–18) mL of boluses in Group Ropi during the second postoperative day, P=0.386.
Hospital length of stay was a median of 5 (4–9) days in Group Lido versus 5 (3–22) days in Group Ropi, P=0.636. Spontaneous ambulation took a median of 2 days in Group Lido versus a median of 1 day in Group Ropi, P=0.148.
One patient in Group Ropi requested ketorolac 7.5 mg IV every 6 hours as rescue medication for pain twice on postoperative day 1 and four times on postoperative day 2. No patient in Group Lido required any adjunctive ketorolac dose.
Complications concerned seven patients: two patients showed side effects possibly related to study medications (patient 19 in Group Lido: hypertension on the second postoperative day, patient 34 in Group Ropi: tremors after local anesthetic boluses through paravertebral catheters on the second postoperative day). Five patients reported surgical complications, or complications not related to study drugs (two in Group Lido and three in Group Ropi). These included dehydration with acute renal failure (patient 7) and small bowel obstruction (patient 43) in Group Lido versus rectal bleeding (patient 23), small bowel obstruction (patients 24 and 34), and anastomotic dehiscence with pelvic abscess (patient 34) in Group Ropi.
Discussion
Our interim analysis showed no difference in terms of NRS scores for pain at rest and during movement in any of the analyzed time points nor any difference in hydromorphone or local anesthetic consumptions during the whole study period between the two groups: lidocaine 0.25% and ropivacaine 0.2% provided similar analgesic profiles in this clinical setting after bilateral paravertebral continuous infusions for postoperative analgesia in laparoscopic abdominal surgeries. Moreover, major outcome measures such as time to ambulation and length of hospital stay were also comparable between groups.
To our knowledge, the present study is the first investigating lidocaine efficacy versus ropivacaine through continuous bilateral paravertebral nerve blocks for postoperative analgesia. Nevertheless, lidocaine has been already compared to other long-acting local anesthetics in literature, and our results are in fact consistent with previous literature.6–8 Lidocaine has been already demonstrated to be as effective as bupivacaine for continuous extrapleural intercostal blocks after posterolateral thoracotomies: Watson et al infused 1 mg/kg/h of 1% lidocaine versus 0.5 mg/kg/h of 0.5% bupivacaine in 46 patients with unilateral paravertebral catheters undergoing thoracic surgery, showing equivalent analgesic efficacy.6 Also, Stayer et al showed that lidocaine represents a suitable alternative to bupivacaine for post-thoracotomy pleural continuous infusion in pediatric patients at infusion rates ranging between 20 μg/kg/min and 40 μg/kg/min, without symptoms of systemic toxicity in 96 patients.7 Our choice of lidocaine 0.25% concentration was based on our prior clinical experience with 0.5% lidocaine for continuous paravertebral infusions and the associated high-level plasma concentrations associated with the use of this concentration (≥5 μg/mL) when infusing bilateral paravertebral blocks for >24 hours. In this regard, it is important to recognize that Hsu et al demonstrated that lidocaine plasma levels increase significantly over time despite a constant rate of infusion.9
A wide range of lidocaine doses has been administered in literature both intravenously and at epidural or peripheral sites. A recent systematic review by Vigneault et al pooled data from 29 studies for a total of 1,754 patients receiving continuous IV lidocaine infusion between 1 mg/kg and 6 mg/kg during general anesthesia, therefore, mainly for a limited period of time.10 In particular, one study investigated lidocaine plasmatic concentrations in patients undergoing abdominal surgery and continuous IV lidocaine infusion (1 mg/min infusions in patients <70 kg and 2 mg/min infusions in patients ≥70 kg) versus continuous epidural lidocaine infusion until postoperative return of bowel function. Despite only one patient showing lidocaine plasmatic levels higher than the accepted toxic level of 5 μg/mL, five adverse events in three patients were considered to be clinically significant, including perioral numbness, tachycardia, atrial fibrillation, disorientation, and visual hallucynations.11
Intravenous administration of lidocaine has been previously demonstrated to be significantly effective in preventing hyperalgesia and in treating postoperative pain, even at low doses12 and especially in abdominal procedures.11 Saadawy et al showed improved postoperative analgesia and reduced intraoperative and postoperative opioid requirements in patients undergoing laparoscopic cholecystectomy in patients receiving 2 mg/kg IV at induction of general anesthesia followed by 2 mg/kg/h IV intraoperatively.13 Therefore, it is possible that the therapeutic efficacy of continuous paravertebral infusion is in part mediated via its plasma concentration.14–16
Our investigation presents some limitations. First, we did not completed enrollment: this decision was driven by the present interim analysis that showed no difference between groups in any of the primary or secondary outcomes, leading our clinical practice to switch definitely to lidocaine continuous infusion instead of ropivacaine for paravertebral nerve blocks. Nevertheless, our study is a small-sized single-center randomized controlled trial and further investigations are needed to systematically assess lidocaine efficacy and safety in this setting. Second, a third group receiving intravenous lidocaine continuous infusion might have provided additional information about the treatment drug mechanism of action, whether it is regional or systemic. Third, we did not measure the local anesthetic plasma concentration. Although the determination of lidocaine plasma concentration is standard, the determination of ropivacaine plasma level is not. Fourth, groups are well matched for all demographic and anthropometric characteristics, except for sex distribution: the vast majority of patients in Group Ropi was male. Camorcia et al demonstrated a possible correlation between sex and pregnancy and a reduced ED50 for intrathecally administered 0.5% bupivacaine in a population of 30 men, 30 nonpregnant women, and 30 pregnant women.17 Other authors denied a correlation between sex and clinical effectiveness after buccal infiltration of 2% lidocaine with epinephrine.18 Whether sex distribution may have affected clinical response to lidocaine or ropivacaine paravertebral continuous infusions in the present study setting remains unclear. Fifth, we decided to perform an intention-to-treat analysis that included also those six patients in Group Lido and four patients in Group Ropi who underwent a laparotomic conversion intraoperatively. Although different surgical approaches cause different postoperative pain levels, thus possibly impacting our primary endpoint, the similar distribution of laparotomic cases between groups should have minimized differences in the present interim analysis.
Conclusion
In conclusion, our results show that lidocaine 0.25% and ropivacaine 0.2% provided similar analgesic profiles in patients undergoing after bilateral paravertebral continuous infusions for postoperative analgesia in laparoscopic abdominal surgeries, without any difference in terms of functional outcomes. These findings, associated with the lidocaine established safety profile, its reduced cost versus ropivacaine solution ($18 versus $46, respectively, which represents for our institution a saving of over $1 million, since we use over 36,000 bags annually), and the ability to obtain lidocaine plasma concentration in a matter of hours (versus weeks in the case of ropivacaine), make lidocaine infusion an appropriate alternative to ropivacaine for bilateral continuous paravertebral infusions.
Funding
Department of Anesthesiology, University of Pittsburgh Medical Center, Pittsburgh, PA, USA.
Disclosure
The authors report no conflicts of interest in this work.
References
Bingham AE, Fu R, Horn JL, Abrahams MS. Continuous peripheral nerve block compared with single-injection peripheral nerve block: a systematic review and meta-analysis of randomized controlled trials. Reg Anesth Pain Med. 2012;37:583–594. | |
Groban L, Deal DD, Vernon JC, James RL, Butterworth J. Ventricular arrhythmias with or without programmed electrical stimulation after incremental overdosage with lidocaine, bupivacaine, levobupivacaine, and ropivacaine. Anesth Analg. 2000;91:1103–1111. | |
Groban L, Deal DD, Vernon JC, James RL, Butterworth J. Cardiac resuscitation after incremental overdosage with lidocaine, bupivacaine, levobupivacaine, and ropivacaine in anesthetized dogs. Anesth Analg. 2001;92:37–43. | |
Capdevila X, Barthelet Y, Biboulet P, Ryckwaert Y, Rubenovitch J, d’Athis F. Effects of perioperative analgesic technique on the surgical outcome and duration of rehabilitation after major knee surgery. Anesthesiology. 1999;91:8–15. | |
Casati A, Vinciguerra F, Scarioni M, et al. Lidocaine versus ropivacaine for continuous interscalene brachial plexus block after open shoulder surgery. Acta Anaesthesiol Scand. 2003;47:355–360. | |
Watson DS, Panian S, Kendall V, Maher DP, Peters G. Pain control after thoracotomy: bupivacaine versus lidocaine in continuous extrapleural intercostal nerve blockade. Ann Thorac Surg. 1999;67:825–828. | |
Stayer SA, Pasquariello CA, Schwartz RE, Balsara RK, Lear BR. The safety of continuous pleural lignocaine after thoracotomy in children and adolescents. Paediatr Anaesth. 1995;5:307–310. | |
Sullivan E, Grannis FW Jr, Ferrell B, Dunst M. Continuous extrapleural intercostal nerve block with continuous infusion of lidocaine after thoracotomy. A descriptive pilot study. Chest. 1995;108:1718–1723. | |
Hsu YW, Somma J, Newman MF, Mathew JP. Population pharmacokinetics of lidocaine administered during and after cardiac surgery. J Cardiothorac Vasc Anesth. 2011;25:931–936. | |
Vigneault L, Turgeon AF, Côté D, et al. Perioperative intravenous lidocaine infusion for postoperative pain control: a meta-analysis of randomized controlled trials. Can J Anaesth. 2011;58:22–37. | |
Swenson BR, Gottschalk A, Wells LT, et al. Intravenous lidocaine is as effective as epidural bupivacaine in reducing ileus duration, hospital stay, and pain after open colon resection: a randomized clinical trial. Reg Anesth Pain Med. 2010;35:370–376. | |
Koppert W, Zeck S, Sittl R, Likar R, Knoll R, Schmelz M. Low-dose lidocaine suppresses experimentally induced hyperalgesia in humans. Anesthesiology. 1998;89:1345–1353. | |
Saadawy IM, Kaki AM, Abd El Latif AA, Abd-Elmaksoud AM, Tolba OM. Lidocaine vs magnesium: effect on analgesia after a laparoscopic cholecystectomy. Acta Anaesthesiol Scand. 2010;54:549–556. | |
Frölich MA, McKeown JL, Worrell MJ, Ness TJ. Intravenous lidocaine reduces ischemic pain in healthy volunteers. Reg Anesth Pain Med. 2010;35:249–254. | |
De Oliveira GS Jr, Fitzgerald P, Streicher LF, Marcus RJ, McCarthy RJ. Systemic lidocaine to improve postoperative quality of recovery after ambulatory laparoscopic surgery. Anesth Analg. 2012;115:262–267. | |
De Oliveira GS Jr, Duncan K, Fitzgerald P, Nader A, Gould RW, McCarthy RJ. Systemic lidocaine to improve quality of recovery after laparoscopic bariatric surgery: a randomized double-blinded placebo-controlled trial. Obes Surg. 2014;24:212–218. | |
Camorcia M, Capogna G, Columb MO. Effect of sex and pregnancy on the potency of intrathecal bupivacaine: determination of ED50for motor block with the up-down sequential allocation method. Eur J Anaesthesiol. 2011;28:240–244. | |
Tófoli GR, Ramacciato JC, Volpato MC, Meechan JG, Ranali J, Groppo FC. Anesthetic efficacy and pain induced by dental anesthesia: the influence of gender and menstrual cycle. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103:e34–e38. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.