Back to Journals » International Medical Case Reports Journal » Volume 9
Leiomyomatosis peritonealis disseminata in postmenopausal women: a case report with review of literature
Authors Gebresellassie HW ![]()
Received 9 June 2016
Accepted for publication 20 August 2016
Published 6 October 2016 Volume 2016:9 Pages 309—312
DOI https://doi.org/10.2147/IMCRJ.S114655
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Hailu Wondimu Gebresellassie
Department of Surgery, School of Medicine, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Background: Leiomyomatosis peritonealis disseminata is an exceedingly rare benign disorder characterized by multiple vascular leiomyomas growing along the submesothelial tissues of the abdominopelvic peritoneum. It is commonly described in women of reproductive age and is rarely seen in men and postmenopausal women.
Case details: A 65-year-old female patient with a history of abdominal surgery for gastrointestinal stromal tumor presented with abdominal pain, weakness, weight loss, and vomiting. An examination revealed a chronically sick looking, emaciated patient with a long midline abdominal scar, and tenderness on deep palpation all over the abdomen. Ultrasound revealed diffuse intra-abdominal masses and a big liver mass. On laparotomy, innumerable masses were found to arise from the outer walls of whole small intestine and mesentery, and there was a soft, 8×10 cm size liver mass. Histology showed highly cellular interlacing bundles of proliferating smooth muscle cells not associated with nuclear atypia or mitotic figures, and there was no necrosis seen, suggesting cellular leiomyoma.
Conclusion: Leiomyomatosis peritonealis disseminata is a very rare condition, especially in men and postmenopausal women. It should be considered as a differential in patients with disseminated intra-abdominal masses arising in mesentery, peritoneum, and on walls of the intestine.
Keywords: leiomyomatosis, postmenopausal women, leiomyoma, leiomyosarcoma, laparotomy
Introduction
Leiomyomas are histologically benign tumors of the uterus that very rarely occur in extrauterine sites.1 Extrauterine leiomyomas are a diagnostic challenge and are often confused for malignancy during imaging. Their clinical presentation depends on their site of origin, number and size, and rapidity of growth. Their signal intensity is similar to that of smooth muscles in T1- and T2-weighted MR imaging and they have a whorled appearance on ultrasound.2 These extrauterine or atypical leiomyomas include leiomyomatosis peritonealis disseminata (LPD), benign metastasizing leiomyoma, retroperitoneal leiomyoma, etc.3
Factors usually associated with LPD are pregnancy, long-term contraceptive use, and previous surgery for uterine leiomyoma, especially laparoscopic, and it is generally seen in women of reproductive age.4
Knowledge of the presence of such pathologies, their different clinical spectrum, and unusual presentation is helpful for proper management.5 Multiple leiomyomas arising submesothelially in the pelvic and abdominal peritoneum characterize LPD.5
LPD is an exceedingly rare benign disorder characterized by multiple vascular leiomyomas growing along the submesothelial tissues of the abdominopelvic peritoneum.
Case report
A 65-year-old female patient with previous abdominal surgery in a regional hospital in Bahir Dar 6 months prior to this presentation presented with diffuse abdominal pain, weakness, and occasional vomiting of ingested material of 6 months duration. There was no history of abnormal uterine bleeding, oral contraceptive use, or gynecologic operation. The patient gave written informed consent to publish this case report. The biopsy result of her surgery in Bahir Dar was suggestive of gastrointestinal stromal tumor. On examination, she looked chronically sick, was emaciated and slightly pale and had a long midline abdominal scar; there was also mild tenderness all over the abdomen on deep palpation. Investigation revealed a hemoglobin value of 9.3 g/dL and a WBC count of 6,900/μL. She had O +ve blood group and had normal liver and renal function as well as a normal chest X-ray.
Ultrasound showed enumerable hypoechoic intra-abdominal masses of different sizes (Figure 1) and a large hypoechoic liver mass measuring 7.5×4.7 cm2 in the right lobe (Figure 2). Laparotomy later revealed innumerable globular masses arising from the mesentery and walls of whole small bowel, some pedunculated but most sessile (Figures 3 and 4). In addition, there was a large liver mass of approximately 8×10 cm in the right lobe with normal pelvis. Multiple biopsies were taken from the mesenteric and superficial small intestinal masses but not from the liver mass for fear of bleeding and abdomen closure. Biopsy specimens were sent to two centers, and both reported a similar finding of highly cellular interlacing bundles of proliferating smooth muscle cells not associated with nuclear atypia or mitotic figures, and there was no necrosis seen. The overall picture suggests cellular leiomyoma of undetermined biologic behavior. Further surgery was differed as it is impractical to remove all masses.
 | Figure 1 The masses as seen on an ultrasound of the abdomen. |
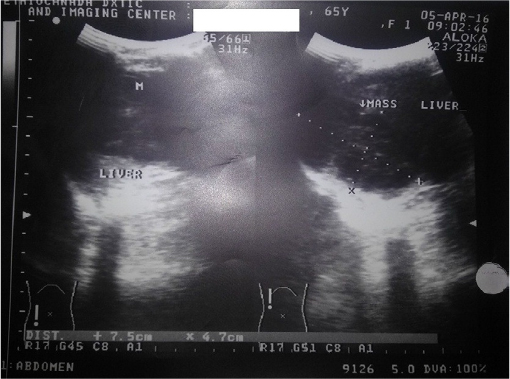 | Figure 2 Ultrasound of abdomen showing a liver mass. |
 | Figure 3 Multiple masses on the wall and mesentery of small bowel. |
 | Figure 4 Masses in the mesentery of the small bowel. |
The patient was discharged with no major complication, and a diagnosis of LPD with possible liver leiomyoma was made. An oncologic consultation was done later. The patient was followed up for 3 months, and she still has some abdominal pain but was doing fine in general.
Discussion
LPD is a rare benign proliferative process that develops from the mesothelial or submesothelial layers of the peritoneum. This disorder is characterized by multiple smooth muscle nodules throughout the peritoneum. It resembles peritoneal carcinomatosis and should be differentiated from other peritoneal tumors.
A differential diagnosis of intra-abdominal carcinomatosis, lymphoma, soft-tissue sarcoma, etc was considered in our patient, but the absence of mitosis, atypia, and necrosis ruled out malignancy. The differential diagnosis should also include those conditions often confused with this such as benign metastasizing leiomyomas, intravenous leiomyomatosis of the uterus, parasitic myoma, or diffuse leiomyomatosis of the uterus.
A finding of highly cellular interlacing bundles of smooth muscles cell proliferation not associated with nuclear atypia or mitotic figure and absence of necrosis as reported by the two centers and the laparotomy finding of subperitoneal nodules varying in size from a few millimeters to several centimeters on the intestine and mesentery confirms the diagnosis of LPD.6
In 1952, Willson and Peale7 reported the first case of LPD. LPD is a specific type leiomyomatosis that is rarely identified by clinical evaluation. To date, only a few hundred cases have been reported in the literature. It is very difficult to reach a diagnosis prior to surgery as diagnosis relies on medical history, observations during surgery, and pathological results.8
Although it commonly occurs in women of reproductive age, few cases have also been reported in postmenopausal women and in men. LPD is benign; however, it exhibits recurrent and malignant tendencies.2,4
LPD generally presents with no symptoms or nonspecific symptoms such as abdominal pain or is suspected at ultrasound or CT scan and after laparotomy for an unrelated problem. This patient also presented with nonspecific symptoms such as abdominal pain, discomfort, nausea, and occasional vomiting of ingested material. The similar ultrasound findings of the intra-abdominal masses and masses in the liver suggest similar pathology. There is a similar report from India, by Tun et al,9 regarding liver leiomyoma in a patient with LPD.
LPD can rarely be associated with leiomyosarcoma. It is postulated that LPD could degenerate into malignancy. Some of the masses not included in the biopsy could have degenerated into leiomyosarcoma that could also be the other explanation of the liver mass found in our patient.10
Conclusion
The patient is postmenopausal with no known risk factors as found in most reports. Her presentation was nonspecific, and the diagnosis was based on operative findings and pathologic report (as is the case with most patients with LPD).
Thus, LPD should be considered as differential diagnosis in patients with disseminated intra-abdominal conditions such as carcinomatosis, lymphoma, tuberculosis, etc.
Disclosure
The author reports no conflicts of interest in this work.
References
Fasih N, Shanbhogue AK, Macdonald DB, et al. RSNA education exhibits leiomyomas beyond the uterus: unusual locations, rare manifestations. Radiographics. 2016;28(7):1–29. | ||
De Vos T, Weyers S, Braems G, et al. Leiomyomatosis peritonealis disseminata associated with ascites and endometriosis: a case report and review of the literature. Acta Chir Belg. 2013;113(5):357–363. | ||
Html F, Kalogiannidis I, Amplianitis I, Grammenou S. Primary mesenteric smooth muscle tumor: an entity with unpredictable biologic behavior. Case Rep Obstet Gynecol. 2016;2013(2013):1–5. | ||
Quade BJ, Mclachlin CM, Soto-wright V, Zuckerman J, Mutter GL, Morton CC. Disseminated peritoneal leiomyomatosis clonality analysis by X chromosome inactivation and cytogenetics of a clinically benign smooth muscle proliferation. Am J Pathology. 1997;150(6):2153–2166. | ||
Yuri T. Leiomyomatosis peritonealis disseminata positive for progesterone receptor. Am J Case Rep. 2015;16:300–304. | ||
Ponsaing LG, Kiss K, Hansen MB. Classification of submucosal tumors in the gastrointestinal tract. World J Gastroenterol. 2007;13(24):3311–3315. | ||
Willson JR, Peale AR. Multiple peritoneal leiomyomas associated with a granulosa-cell tumor of the ovary. Am J Obstet Gynecolo. 1952;64:204–208. | ||
Report C, Lee WY, Noh JH. Leiomyomatosis peritonealis disseminata associated with appendiceal endometriosis: a case report. J Med Case Rep. 2015;9(167):1–4. | ||
Tun AM, Tun NM, Thein KZ, Naing EE, Giashuddin S, Shulimovich M. A rare concurrence of leiomyomatosis peritonealis disseminata, leiomyosarcoma of the pelvis and leiomyomatous nodule of the liver. Case Rep Oncol Med. 2016;2016:3025432. | ||
Manjula J, Vandana P, Anu B. Recurrent diffuse peritoneal leiomyomatosis following leiomyomata uterus. J Obstet Gynecol India. 2014;64(Suppl 1):105–106. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.