Back to Journals » International Medical Case Reports Journal » Volume 19
Left Ventricular Myxoma-Caused Recurrent Stroke in a Middle-Aged Woman: A Case Report
Authors Wu N, Du Y, Li X, Hu L, Li H, Gao A, Dong J, Liu L
Received 13 December 2025
Accepted for publication 19 March 2026
Published 24 March 2026 Volume 2026:19 587217
DOI https://doi.org/10.2147/IMCRJ.S587217
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Na Wu,1 Yinuo Du,1 Xianzheng Li,2 Liting Hu,1 Huhu Li,1 Aimin Gao,1 Jing Dong,1 Li Liu1
1Department of Cardiology, GenerTec Universal Xi’an Beihuan Hospital, The First Hospital of Xi’an Chanba International Port, Xi’an City, Shaanxi Province, People’s Republic of China; 2Department of Radiology, GenerTec Universal Xi’an Beihuan Hospital, The First Hospital of Xi’an Chanba International Port, Xi’an City, Shaanxi Province, People’s Republic of China
Correspondence: Li Liu, Department of Cardiology, GenerTec Universal Xi’an Beihuan Hospital, The First Hospital of Xi’an Chanba International Port, Xi’an City, Shaanxi Province, People’s Republic of China, Email [email protected]
Introduction: Ischemic stroke primarily occurs in older adults, with thromboembolism representing the most common underlying etiology. However, rare causes such as left ventricular (LV) myxomas are frequently overlooked.
Case Presentation: A 53-year-old Chinese woman presented in Emergency Room with acute right-sided hemiparesis and dysarthria. Initial evaluation suggested a cryptogenic stroke, and she underwent thrombolysis (rt-PA) with subsequent clinical improvement. However, she experienced a recurrent ischemic stroke two weeks later, prompting further investigation. Repeat imaging revealed a 20.3 × 13.4 mm pedunculated LV mass attached to the lateral wall - a finding initially missed on prior echocardiography performed by a junior echocardiographer due to suboptimal image quality conducted on an acutely ill, uncooperative patient. The mass’s morphology was consistent with a myxoma and surgical excision was scheduled, however the patient suffered fatal cardiorespiratory arrest before intervention.
Conclusion: LV myxoma is a rare but critical stroke etiology. Echocardiography remains pivotal in identifying cardiac masses. This case highlights the diagnostic challenges posed by LV myxomas and underscores the importance of a comprehensive evaluation by an experienced echocardiologist in embolic stroke, especially in uncooperative patient and with atypical clinical presentation.
Keywords: left ventricular myxoma, stroke, echocardiography, embolic event
Introduction
Ischemic stroke predominantly affects older adults. The underlying causes and risk factors are complex; however, thromboembolism is thought to be the most common etiology.1,2 While thrombus due to atrial fibrillation and ventricular thrombi secondary to myocardial infarction are well-documented sources,2,3 rare causes such as cardiac myxomas are often overlooked, particularly left ventricular (LV) myxoma, which only accounts for 2–3%.4,5 Although histologically benign, myxomas can lead to life-threatening systemic embolization depending on their location, mobility, and morphology. Patients with LV myxoma are typically asymptomatic or present with nonspecific symptoms, which often mimic other cardiovascular diseases, thereby rendering the diagnosis challenging. Herein, we present a fatal case of recurrent stroke due to an initially undiagnosed (LV) myxoma in a middle-aged woman, highlighting the importance of considering rare embolic sources in stroke workup, particularly in younger patients without conventional risk factors.
Case Presentation
A 53-year-old woman presented to emergency room with acute-onset right-sided hemiparesis and dysarthria lasting two hours. Her medical history included cervical cancer, treated with 28 sessions of radiotherapy and three cycles of nedaplatin/paclitaxel chemotherapy. She denied hypertension, diabetes, or familial cardiac disease. Vital signs revealed hypertension (150/105 mmHg) and tachycardia (104 bpm), R 30/min, temperature 36.4°C. Initial ECG showed sinus tachycardia and extensive T waves inversion (Figure 1A) and initial transthoracic echocardiography (TTE) indicated normal chamber size, LV ejection fraction (LVEF 60%), and small amount pericardial effusion. Important laboratory tests at intensive care unit (ICU) were summarized in Table 1. Head MRI with diffusion-weighted imaging (DWI) demonstrated acute infarcts in the frontal, temporal, and parietal lobes (Figure 1B). The patient was diagnosed with cryptogenic stroke and was treated with rt-PA (49.5 mg in total), with partial symptom resolution. Follow-up imaging showed a small amount of corpus callosum hemorrhage (Figure 1C). No other complications were found in the follow-up after the patient was discharged from the hospital.
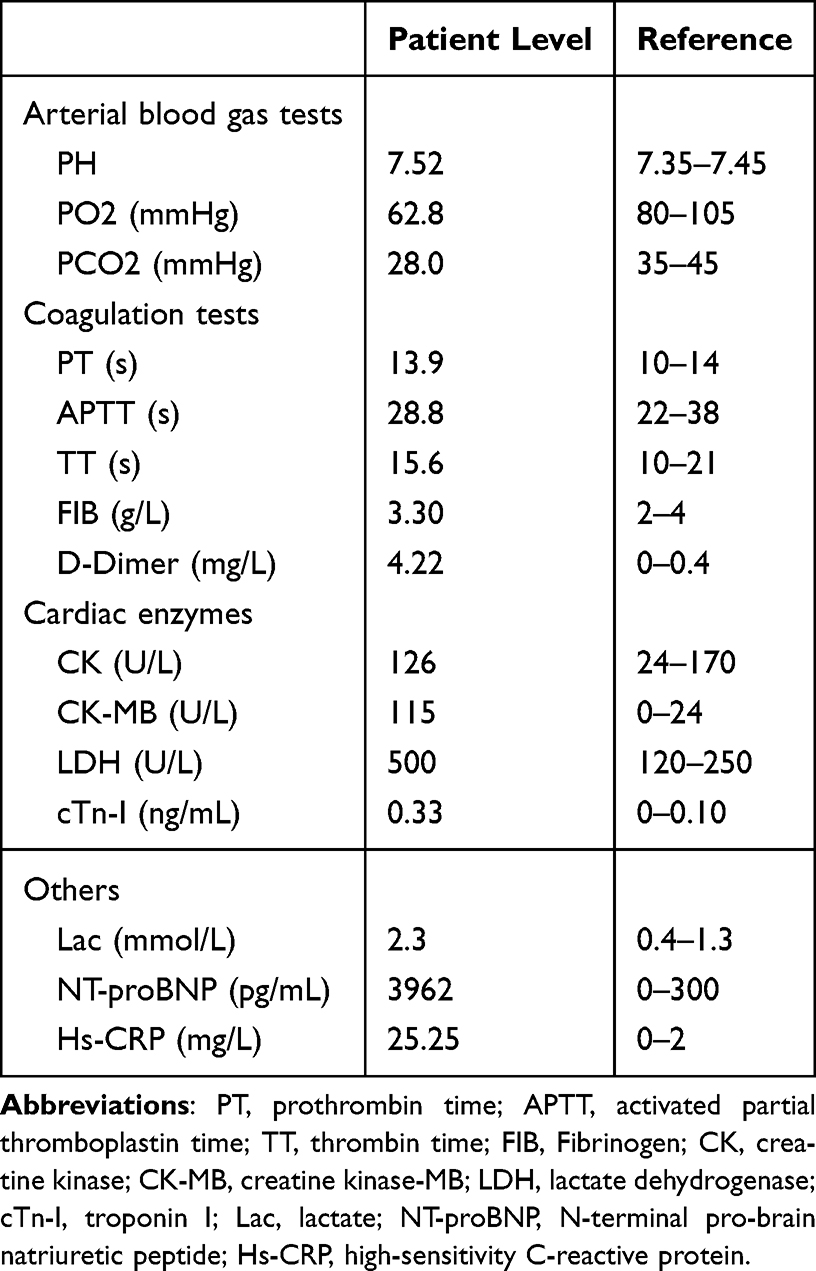 |
Table 1 Laboratory Tests at First Hospitalization |
 |
Figure 1 ECG at emergency room showed sinus rhythm with extensive T waves inversion (A); Head MRI (diffusion-weighted imaging, DWI) revealed focal necrosis of the frontal, temporal, and parietal lobes ((B), red arrow); Head CT showed minor corpus callosum hemorrhage ((C), green arrow). |
Two weeks later, the patient was readmitted to the hospital for syncope and respiratory distress. Examination revealed hypertension (145/105 mmHg), tachycardia (112 bpm), R 31/min, and oxygen saturation 99% (room air). Cardiac and pulmonary examination revealed decreased heart sounds, no murmurs, and clear lungs to auscultation. The abdomen was soft and nontender to palpation, without rebound tenderness. There was no appreciable bilateral lower extremity edema. Laboratory findings included elevated troponin (0.79 ng/mL, reference 0-0-10ng/mL), N-terminal pro-brain natriuretic peptide (NT-proBNP, 7037pg/mL, reference 0–300pg/mL), D-dimer (8.67mg/L, reference 0–0.4mg/L), prothrombin time (PT, 17.2s, reference 10–14s), activated partial thromboplastin time (APTT, 47.7s, reference 22–38s) and deranged hepatic/renal function. ECG showed sinus tachycardia and extensive T waves inversion, which was the same as previous recordings (Figure 2A). Head and chest CT indicated new ischemic necrosis at bilateral basal ganglia (Figure 2B) and small amount of chest effusion (more severe on the left side, Figure 2C). Repeat echocardiography revealed mild mitral and tricuspid regurgitation, normal chamber dimensions, preserved LVEF (56%), and a moderate pericardial effusion. Notably, a 20.3 × 13.4 mm mobile, polypoid mass was visualized in the left ventricle, attached to the lateral wall via a 2–3 mm stalk (Figure 3A–D). The lesion exhibited homogeneous echotexture and high mobility, consistent with a cardiac myxoma. Based on these findings, we established a diagnosis of recurrent ischemic stroke secondary to myxoma-related embolism. Subsequently, the patient was treated with diuretics, antibiotics, and other supportive measures (including hepatoprotective agents) in accordance with imaging findings (indicating chest and pericardial effusion) and laboratory results (elevated NT-proBNP, white blood cell count, creatinine; low albumin, among others). The laboratory parameters gradually improved following treatment. Surgical excision was planned; however, on the morning of the seventh hospital day, the patient abruptly developed cyanosis, shallow breathing, decreased oxygen saturation (78%) despite oxygen supplementation, and hypotension. Secretion suction and assisted ventilation were initiated, followed by cardiopulmonary resuscitation, which ultimately proved unsuccessful.
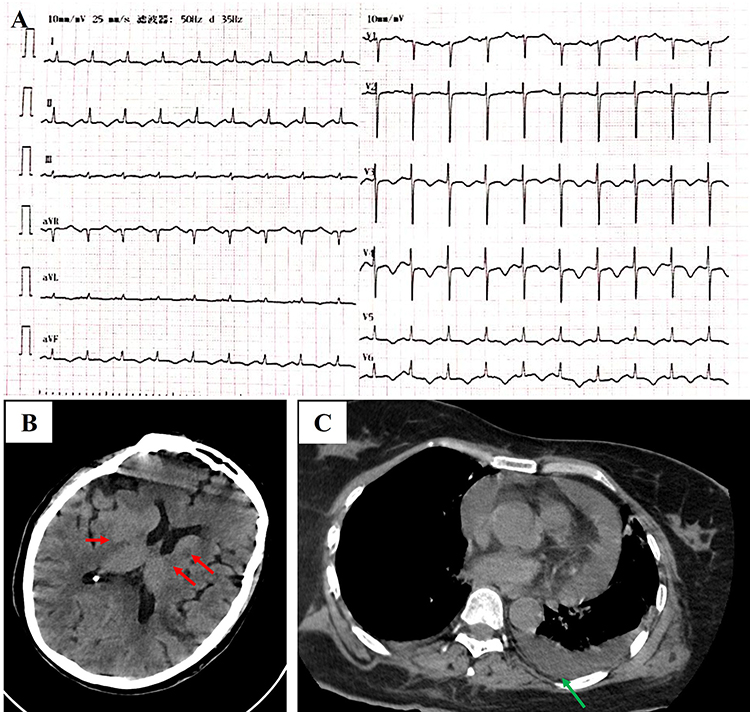 |
Figure 2 ECG showed sinus tachycardia and extensive T wave inversion (A); Head CT revealed new ischemic necrosis at bilateral basal ganglia ((B), red arrow); Chest CT showed bilateral pleural effusion, more severe on the left side ((C), green arrow). |
 |
Figure 3 Echocardiographic evaluation of the cardiac mass. Transthoracic echocardiography (TTE) at parasternal long-axis view (A), short-axis view (B) and four‐chamber view (C) shows a 20.7 mm × 13.4 mm mass (D) which was polyp‐like‐shaped, homogeneous, mobile and solitary centered on the lateral wall of the left ventricle (green arrow), there is a 2–3 mm stalk attached to the lateral wall of left ventricular (red arrow). |
Discussion
Myxoma is a primary cardiac tumor, about 75% of myxomas are found in left atrium, followed by the right atrium (20%). Myxoma located in the left ventricle is rare, only account for 2–3%.4,5 Myxomas can occur at any age, but they are typically identified between 40 and 60 in women.5,6 Most of patients with LV myxoma are asymptomatic, but they can present as chest pain, palpitations, syncope, shortness of breath, arrhythmias, or angina.5,6 Although they are histologically benign, they may lead to life-threatening complications such as hemodynamic disturbances or systemic embolization. Their early diagnosis is difficult since the symptoms and signs may be nonspecific. Most myxoma was diagnosed unexpectedly if they did not cause constitutional symptoms or systemic embolic events.5 About 30% to 40% cases experienced systemic embolism, and most of them are cerebral.6 Myxoma embolization risk is primarily determined by its shape, not size. The left ventricle’s high mobility and pressure make it more susceptible to embolization. Diagnosis is primarily made by transthoracic echocardiography, transoesophageal echocardiography, or magnetic resonance imaging. It allows for a quick and simple evaluation of the morphology, extent, site of attachment, with/without stalk, involvement of valve leaflets, and functional obstruction of the LV outflow tract. Myxomas can be easily misdiagnosed as LV thrombosis. However, the formation of LV thrombosis is usually associated with some substantial situations, such as in patients with ST-segment elevation myocardial infarction (STEMI) (especially with a large anterior MI), dilated cardiomyopathy, severe heart valve disease, or a hypercoagulable state due to underlying medical conditions like inflammatory diseases or certain medications.7,8 Particularly, any situation where there is significant blood stasis within the left ventricle due to poor contractility can lead to thrombus formation, even without a prior MI.7,9,10 In this case, the diagnosis of LV myxoma was established despite the absence of pathological confirmation, primarily based on characteristic echocardiographic features—specifically, a polypoid morphology, homogeneous echotexture, and the presence of a pedunculated stalk—which distinguish it from a thrombus. Although our patient had risk factors for hypercoagulability, including cervical cancer and ongoing chemotherapy, the lack of wall-motion abnormalities or evidence of prior myocardial infarction further supported the diagnosis of a myxoma over a thrombotic lesion. We also investigated the discrepancy in results between the initial and second TTE examinations, which can be attributed to several factors, including the suboptimal acquisition conditions during the initial emergency examination—conducted on an acutely ill, uncooperative patient—coupled with limited operator experience in evaluating embolic stroke etiologies. The first TTE was performed by a junior echocardiographer on duty, whereas the subsequent comprehensive examination was conducted by a senior echocardiologist in the Coronary Care Unit (CCU).
This report underscores the critical importance of a thorough evaluation to determine the etiology of embolic events. Definitive treatment involves prompt surgical resection upon diagnostic confirmation. However, as demonstrated in this case, delayed diagnosis is associated with adverse clinical outcomes.
Conclusion
LV myxoma is a rare but critical stroke etiology. Echocardiography remains pivotal in identifying cardiac masses, and prompt surgical referral is imperative upon diagnosis. A comprehensive evaluation by an experienced echocardiologist, skilled in identifying atypical embolic sources such as LV myxoma, is crucial, especially in uncooperative patient, as it enables prompt surgical intervention - a key determinant for improving outcomes and saving lives.
Ethical Approval
Ethical approval is not required for individual case reports at our institution if the patient has provided informed consent for publication.
Consent for Publication
Written informed consent was obtained from the patient’s legal guardian (her husband) for publication of this case report and any accompanying images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declared that the study received no financial support.
Disclosure
The authors declared no conflicts of interest in this work.
References
1. Campbell BCV, De Silva DA, Macleod MR, et al. Ischaemic stroke. Nat Rev Dis Primers. 2019;5(1):70. doi:10.1038/s41572-019-0118-8
2. Todo K, Okazaki S, Doijiri R, et al. Atrial fibrillation detection and ischemic stroke recurrence in cryptogenic stroke: a retrospective, multicenter, observational study. J Am Heart Assoc. 2024;13(3):e031508. doi:10.1161/JAHA.123.031508
3. Merkler AE, Bartz TM, Kamel H, et al. Silent myocardial infarction and subsequent ischemic stroke in the cardiovascular health study. Neurology. 2021;97(5):e436–6. doi:10.1212/WNL.0000000000012249
4. Swartz MF, Lutz CJ, Chandan VS, Landas S, Fink GW. Atrial myxomas: pathologic types, tumour location, and presenting symptoms. J Card Surg. 2006;21(4):435–440. doi:10.1111/j.1540-8191.2006.00265.x
5. Samanidis G, Khoury M, Balanika M, Perrea DN. Current challenges in the diagnosis and treatment of cardiac myxoma. Kardiol Pol. 2020;78(4):269–277. doi:10.33963/KP.15254
6. Islam AK. Cardiac myxomas: a narrative review. World J Cardiol. 2022;14(4):206–219. doi:10.4330/wjc.v14.i4.206
7. McCarthy CP, Vaduganathan M, McCarthy KJ, et al. Left ventricular thrombus after acute myocardial infarction: screening, prevention, and treatment. JAMA Cardiolo. 2018;3(7):642–649. doi:10.1001/jamacardio.2018.1086
8. Gottdiener JS, Gay JA, VanVoorhees L, et al. Frequency and embolic potential of left ventricular thrombus in dilated cardiomyopathy: assessment by 2-dimensional echocardiography. Am J Cardiol. 1983;52(10):1281–1285. doi:10.1016/0002-9149(83)90588-X
9. Gottdiener JS, Massie B, Ammons SB, et al. Prevalence of left ventricular thrombus in dilated cardiomyopathy: the WATCH trial. J Am J Cardiol. 2003;41(6):202. doi:10.1016/S0735-1097(03)81966-6
10. Cruz Rodriguez JB, Okajima K, Greenberg BH. Management of left ventricular thrombus: a narrative review. Ann Transl Med. 2021;9(6):520. doi:10.21037/atm-20-7839
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.